 Yomali Ferreyra1
Yomali Ferreyra1 Gina Rosas2Alicia M. Cock-Rada3Jhajaira Araujo4Leny Bravo5Franco Doimi6Jhoysi Casas6María de los Ángeles Clavo7
Gina Rosas2Alicia M. Cock-Rada3Jhajaira Araujo4Leny Bravo5Franco Doimi6Jhoysi Casas6María de los Ángeles Clavo7 Joseph A. Pinto4*
Joseph A. Pinto4* Carolina Belmar-López5,6
Carolina Belmar-López5,6- 1Departamento de Bioingeniería, Universidad de Ingenieria y Tecnología, Lima, Peru
- 2Departamento de Patología, Insituto Nacional de Enfermedades Neoplásicas, Lima, Peru
- 3Departmento de Oncología Médica, Instituto de Cancerología Las Américas - Auna, Medellín, Colombia
- 4Centro de Investigación Básicas y traslacional, Auna Ideas, Lima, Peru
- 5Escuela Profesional de Medicina Humana-Filial Ica, Universidad Privada San Juan Bautista, Ica, Peru
- 6Oncogenomics, Auna, Lima, Peru
- 7Facultad de Medicina Humana, Universidad Nacional San Luis Gonzaga, Ica, Peru
Background: There is an increasing amount of data from Latin America on the characterization of BRCA variants; however, there is limited information from Peru. We conducted a retrospective study to describe germline pathogenic/likely pathogenic(P/LP) variants and variants of uncertain/unknown significance (VUS) in the BRCA1 and BRCA2 genes in Peru, in patients with breast and ovarian cancer, candidates for treatment with poly (adenosine diphosphate–ribose) polymerase (PARP) inhibitors.
Methods: The patients were evaluated during the period 2019-2021. Genomic DNA was isolated from peripheral blood samples and targeted sequencing was performed using the Ampliseq BRCA panel. Genetic variant interpretation was carried out in accordance with the recommendations of the American College of Medical Genetics and ClinVar. During this period, 525 patients (143 with breast cancer and 382 with ovarian cancer) were studied.
Results: We found that 14.7% (21/143) of breast cancer patients and 20.7% (79/382) of ovarian cancer patients were carriers of P/LP variants in BRCA1/2. The most frequent pathogenic variants detected in BRCA1 were c.2105dupT (BIC: 2224insT, n=12, 18.75%), c.68_69delAG (BIC: 185delAG, n=6, 9.38%), c.140G>T and c.815_824dupAGCCATGTGG (n=5, 7.81%), while in BRCA2 were c.8023A>G (n=6, 16.67%), c.6024dupG (BIC: 6252insG, n=4, 11.11%), and c.9235delG (BIC: 9463delG, n=3, 8.33%). Regarding VUS, we found that 6.99% (10/143) of breast cancer patients and 7.33% (28/382) of ovarian cancer patients were carriers of a VUS in BRCA1/2. For BRCA1, the most frequent VUS was c.93C>G (n=2), and for BRCA2, c.5465A>T (n=4), c.3101T>C (n=3), c.205C>A and c.437T>C (n=2).
Conclusion: We found a frequency of 14.7% germline mutations in breast cancer patients and 20.7% in ovarian cancer patients. The most recurrent mutations were BRCA1 c.2105dupT and BRCA2 c.8023A>G. We found that BRCA2 c.8023A>G, c.6024dupG, and c.9235delG were not previously reported in Peruvian patients. BRCA1 c.2344dupA is a novel mutation that has not been previously reported in any database. The frequency of VUS in our cohort was 7.2%.
Background
Breast and ovarian cancer are highly prevalent malignancies in Latin America, where more than 50 thousand patients die yearly from these pathologies. It is estimated that 5-10% of breast cancer (BC) and 10-15% of ovarian cancer (OC) are attributed to hereditary breast and ovarian cancer (HBOC). Mutations in the BRCA1 and BRCA2 genes are the best-known genetic risk factors for breast and ovarian cancer (1–3).
Detecting BRCA1/2 mutations allows crucial and challenging decisions regarding cancer prevention or risk reduction, early detection and pharmacological management. Germline BRCA1/2 variants cause hereditary breast and ovarian cancer syndrome and confer a lifetime risk of 38-87% of developing breast cancer in women and 16.5-63% of developing ovarian cancer (4). Germline BRCA1/2 mutations are present in approximately 5% of all breast patients and 15% of all ovarian cancer patients (5, 6). Breast tumors with BRCA1/2 mutation carriers are more frequently HER2 negative, and triple-negative tumors (TNBC) account for approximately 68% of BRCA1 tumors (7). High-grade serous ovarian cancers are more commonly associated with BRCA1/2 mutations (8).
BRCA1/2 are tumor suppressor genes that participate in the homologous recombination repair of double-strand DNA damage. BRCA1/2 defective cells are more sensitive to Poly(ADP-ribose) polymerase (PARP), an enzyme involved in base excision repair, a vital component of single-strand break repair (SSB). PARP inhibitors can increase SSB, which are converted to double-strand DNA breaks (DSBs) during replication. In defective BRCA1/2 cells, these DSBs are not effectively repaired, leading to chromosomal instability, cell cycle arrest, and subsequent apoptosis, a mechanism known as synthetic lethality (9)
Several PARP inhibitors have been developed to treat patients with breast, ovarian, pancreatic, and prostate cancer with BRCA1/2 mutations. OlympiAD, a phase III randomized, controlled, open-label study trial, compared Olaparib, a PARP inhibitor, with non-platinum chemotherapy (CT) in metastatic breast cancer patients with germline BRCA1/2 mutations. Progression-free survival (PFS) was higher in patients receiving Olaparib than in those receiving CT (7.0 vs 2.2 months). The hazard ratio (HR) for disease progression or death was 0.58 (95% CI 0.43-0.80: P< 0.001). The response rate was 59.9% in the Olaparib group and 28.8% in the CT group. An improvement in PFS was observed in all subtypes and was higher in TNBC patients (10).
The randomized phase III trial, EMBRACA, compared another PARP inhibitor, Talazoparib, with single-agent CT in patients with advanced breast cancer with BRCA1/2 mutations. The median PFS was longer in the Talazoparib group than in the control group (8.6 months [95% CI, 7.2-9.3] vs 5.6 months [95% CI, 4.2-6.7]; HR=0.54 [95% CI 0.41-0.71; P < 0.001] for disease progression or death. Based on these two trials, the FDA approved Olaparib and Talozaparib for HER2-negative patients with BRCA1/2 mutations, and the NCCN guidelines recommend testing for BRCA1/2 mutations in all patients with TNBC or metastatic breast cancer to identify candidates for PARP inhibitor therapy (11).
For ovarian cancer, germline testing for BRCA1/2 is informative for selecting patients for PARP inhibitor therapy. Around 50% of ovarian tumors are homologous recombination deficient (HRD) and 20% are associated with BRCA1/2 mutations, germline (14%) or somatic (6%) (6). PARP inhibitor treatment is recommended for maintenance therapy for stage II-IV disease or persistent or recurrent disease in BRCA1/2 mutated ovarian cancer (12). The SOLO-1 phase III trial showed an improvement in 3-year PFS with Olaparib versus Placebo as maintenance therapy for patients with a germline variant BRCA1/2, who had a complete or partial response (CR/PR) after platinum-based first-line chemotherapy (60% vs. 27%; P<0.0001); HR=0.30 [95% CI, 0.23-0.41] (13). Other phase III studies with PARP inhibitor, PAOLA-1: Olaparib + Bevacizumab versus Placebo + Bevacizumab for maintenance therapy for patients with advanced disease who had CR/PR after platinum-based first-line chemotherapy, or PRIMA: Niraparib versus Placebo as maintenance therapy for patients with CR/PR after platinum first-line chemotherapy showed a notable improvement in median PFS, especially in patients with a germline BRCA1/2 mutation or HRD (22.1 vs 16.6 months and 21.9 months vs 10.4 months, respectively) (14, 15).
There is increasing information on the molecular epidemiology of BRCA1/2 genes in Latin America and several founder mutations have been identified (16). Founder mutations in Latin America have been reported in Mexico (BRCA1 del exons 9-12), Brazil (BRCA1 5382insC and BRCA2 c.156_157insAlu), and Colombia (BRCA1 3450del4, A1708E and BRCA2 3034del4) (17).
Unfortunately, there is a gap in information about the genetic epidemiology of breast and ovarian cancers in Peru. A limited number of publications describe the frequency of BRCA1 and BRCA2 mutations in Peru with studies with small sample sizes and in a particular group of patients (18). Here, we describe the frequency and spectrum of genetic variants (pathogenic/likely pathogenic P/LP and VUS) in the BRCA1/2 genes in patients with BC and/or OC, profiled during 2019-2021 in a reference laboratory in Peru, for the identification of PARP inhibitor candidates.
Methods
Study population
The study included all BC and OC patients, referred to Oncogenomics Laboratory (Lima, Peru) from 2019 to 2021, to identify candidates for PARP inhibitors treatment. The histological tumor types, hormone receptor and human epidermal growth factor receptor 2 (HER2) statuses were recorded.
BRCA1/2 mutation screening
Peripheral blood samples were taken to assess mutations in the BRCA1/2 genes. DNA was extracted using the ReliaPrep Blood gDNA Miniprep System or the ReliaPrep FFPE gDNA Miniprep System (Promega, Madison, USA) according to the manufacturer’s protocol. DNA concentration was determined by fluorometric quantitation using a Qubit 4.0 fluorimeter with Qubit dsDNA HS ASSAY KIT (Invitrogen, USA). The panel targets single nucleotide variants (SNVs) and insertion/deletions (indels) in all exonic regions of the BRCA1 and BRCA2 genes and flanking intronic sequences. A commercial reference standard, Horizon Quantitative Multiplex Reference Standard HD810 was tested to validate the performance of NGS that detect mutations. Libraries were prepared using the Ampliseq BRCA Panel and Ampliseq Library PLUS (Illumina, San Diego, USA) following the manufacturer’s protocol without modifications using 10 ng of input DNA per sample. The multiplex polymerase chain reaction (PCR) was performed in 18 cycles. Sequencing adapters with unique indexes (AmpliSeq CD Indexes Set A for Illumina) were ligated to the amplification products and purified using Agencourt AmpureXP beads (Beckman Coulter, CA, USA) according to the manufacturer’s instructions. Libraries with 2nM molarities were subjected to clustering using a standard flow cell and sequenced on the Illumina MiSeq platform using the MiSeq Reagent Micro Kit v2 (300 cycles). Raw data were processed automatically in the BaseSpace Sequence Hub (Illumina) and aligned with the hg19 reference genome. An average of 95.7% (91.7– 99.8%) on-target reads, 96.6% (94.7 – 98.6%) read uniformity and 50X average coverage per sample were obtained.
Mutation nomenclature and classification
BaseSpace Variant Interpreter (Illumina) annotated and interpreted genetic variants. Genetic variants were annotated under the nomenclature of the Human Genome Variation Society (HGVS). Interpretation was made using the single nucleotide polymorphism database (dbSNP), breast cancer information core (BIC) and Clinvar database. The Integrative Genomics Viewer was applied to visualize the variants. All identified variants were checked with Varsome (Saphetor, Swiss).
Interpreting the pathogenicity of the variants followed the latest recommendations of the American College of Medical Genetics (ACMG) and ClinVar. In cases of conflicting interpretations of pathogenicty (classified as pathogenic by at least one database and benign, likely benign, or VUS by others) between ACMG and ClinVar, ACMG classification was used. All new variants (missense, in frame and splicing) not yet reported in the databases consulted, were also considered VUS. Benign variants were not reported.
Statistical analysis
We conducted a descriptive analysis. The frequency of variants identified in the BRCA1/2 genes was calculated using RStudio. Packages such as sf, ggplot2 and ggrepel were installed to obtain geographical maps of Peru, to observe the distribution of pathogenic variants according to the place of birth of the patients.
Results
General characteristics of patients
A total of 525 patients were included in this study (143 with BC and 382 with OC). Most of the patients were born in metropolitan Lima (58.1%), followed by patients from the coast (excluding metropolitan Lima, 28.0%), highlands (11.6%) and jungle (2.1%). Regarding the clinical characteristics of BC patients, 21.7% (n=31) had HER2-negative and hormone receptor positive tumors, while 78.3% (n=112) of the patients had HER2-negative and hormone receptor negative tumors (TNBC). Most of the OC (90.8%) were high-grade serous carcinomas. The frequency of clinical stage III was 33.6% and 50%, and clinical stage IV was 66.4% and 50% for BC and OC, respectively (Table 1). The prevalence of patients with P/LP germline variants in BRCA1/2 was 19.0% (n=100/525). No patient had more than one P/LP variant. The percentage of BC patients who carried germline BRCA1/2 P/LP variants was 14.7% (n=21/143) with 61.9% (n=13/21) of them carrying variants in BRCA1 and 38.1% (n=8/21) in BRCA2 (Figure 1). In total, 81% (n=17/21) of patients with BRCA1/2 P/LP variants were TNBC and 19.1% (n=4/21) were positive for hormone receptors. Furthermore, 38.1% (n=8/21) were reported in clinical stage III and 61.9% (n=13/21) in clinical stage IV. Although we had no information about their age at the time of diagnosis, the mean age at molecular diagnosis was 48.63 years (range: 30-74 years).On the other hand, 20.7%(n=79/382) of OC patients had germline BRCA1/2 P/LP variants with 64.8% (n=51/79) of them in BRCA1 and 35.44% (n=28/79) in BRCA2. Regarding the histological subtypes of BRCA1/2 OC patients, it was observed that 91.1% (n=72/79) were characterized by high-grade serous carcinoma, followed by endometrioid carcinoma (n=5/79, 6.3%) and clear cell carcinoma (n=2/79, 2.53%). The clinical stages were distributed in 49.4% (n=39/79) stage III and 50.6% (n=40/79) stage IV. Furthermore, only 77 patients had their age at molecular diagnosis available, so the mean age was 54.36 years (range: 34-77).
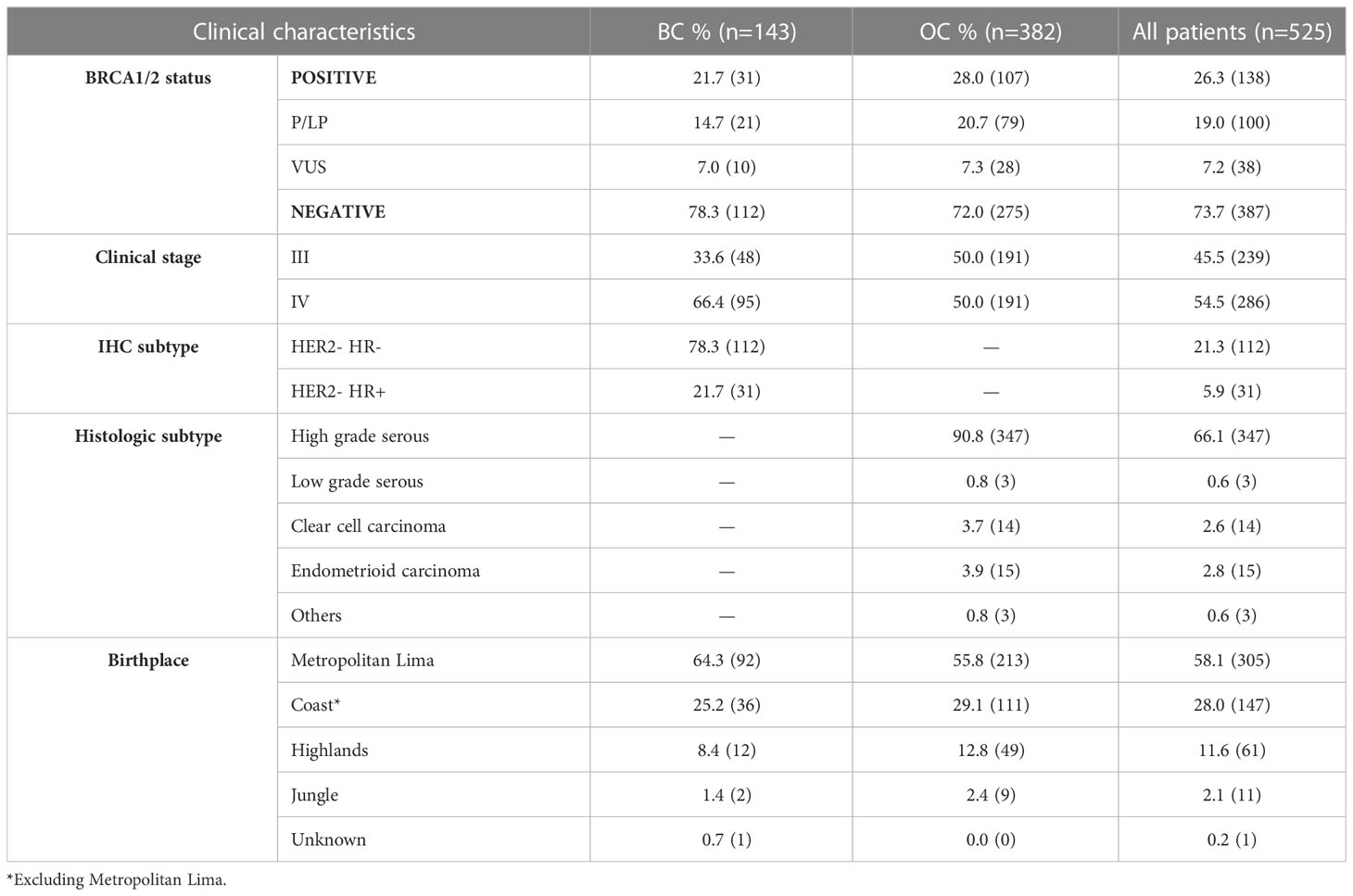
Table 1 Clinicopathological characteristics of the general population.
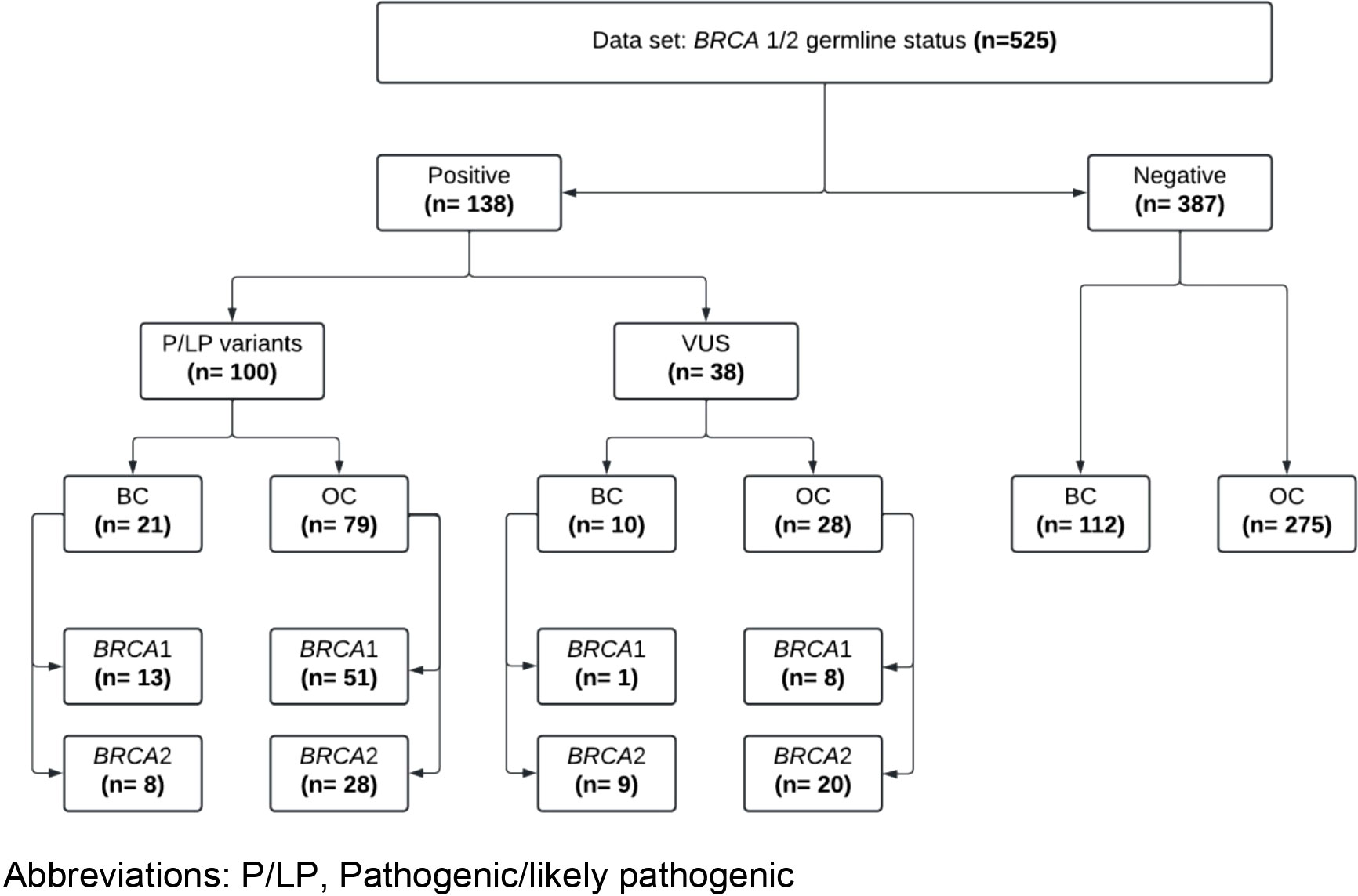
Figure 1 Flowchart showing results and characteristics of patients with breast and ovarian cancer included in this study. P/LP, Pathogenic/likely pathogenic.
Germline BRCA1 pathogenic/likely pathogenic variants
The study identified 33 different P/LP germline variants in BRCA1 gene in 64 patients, finding 20.3% (n=13/64) in BC and 79.9% (n=51/64) in OC. The most frequent variants in BRCA1 were c.2105dupT (BIC: 2224insT, n=12, 18.75%), c.68_69delAG (BIC: 185delAG, n=6, 9.38%), c.140G>T and c.815 _824dupAGCCATGTGG (n=5, 7.81%) (Table 2). Most variants were previously reported, except BRCA1 c.2344dupA (n=2, 2.74%), which was not reported in any database. These patients were born in Lima and Arequipa.

Table 2 Pathogenic/likely pathogenic germline BRCA1 variants found in our study.
Furthermore, BRCA1 P/LP variants were observed mainly in exon 10 (n=20/33), exon 19 (n = 3/33), and exon 2 and 4 (n=2/33). Most of the P/LP variants were missense (n=13/33) and in frame deletion variants (n=12/33), followed by frame insertions (n=6/33) and stop gained variants (n=1/33) (Table 2). There was only one case with a large deletion, specifically a deletion of exon 11 (n=1/33). Patients with P/LP variants in the BRCA1 gene were born primarily in Metropolitan Lima (n=37/64), the coast (n=21/64) and the highlands (n=6/64). The most frequent P/LP variants in BRCA1, c.2105dupT (n=11) and c.68_69delAG (n=5) were found predominantly in patients born in Metropolitan Lima (Figure 2A). The position of P/LP variants in relation to the Brca1 protein is shown in Figure 3A.
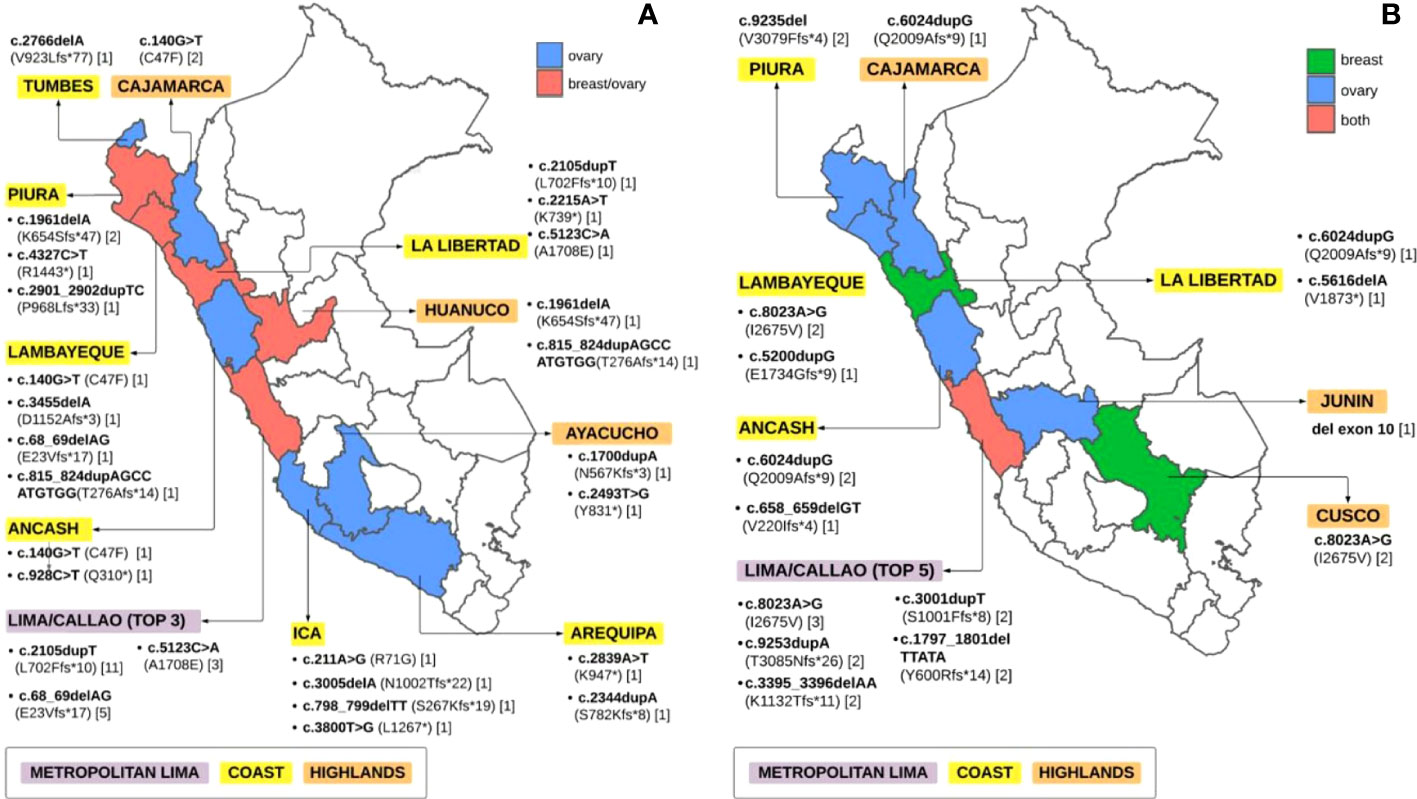
Figure 2 Pathogenic/likely pathogenic germline BRCA1/2 variants according to the place of birth (A) Germline BRCA1 LP/P variants (B) Germline BRCA2 LP/P variants.
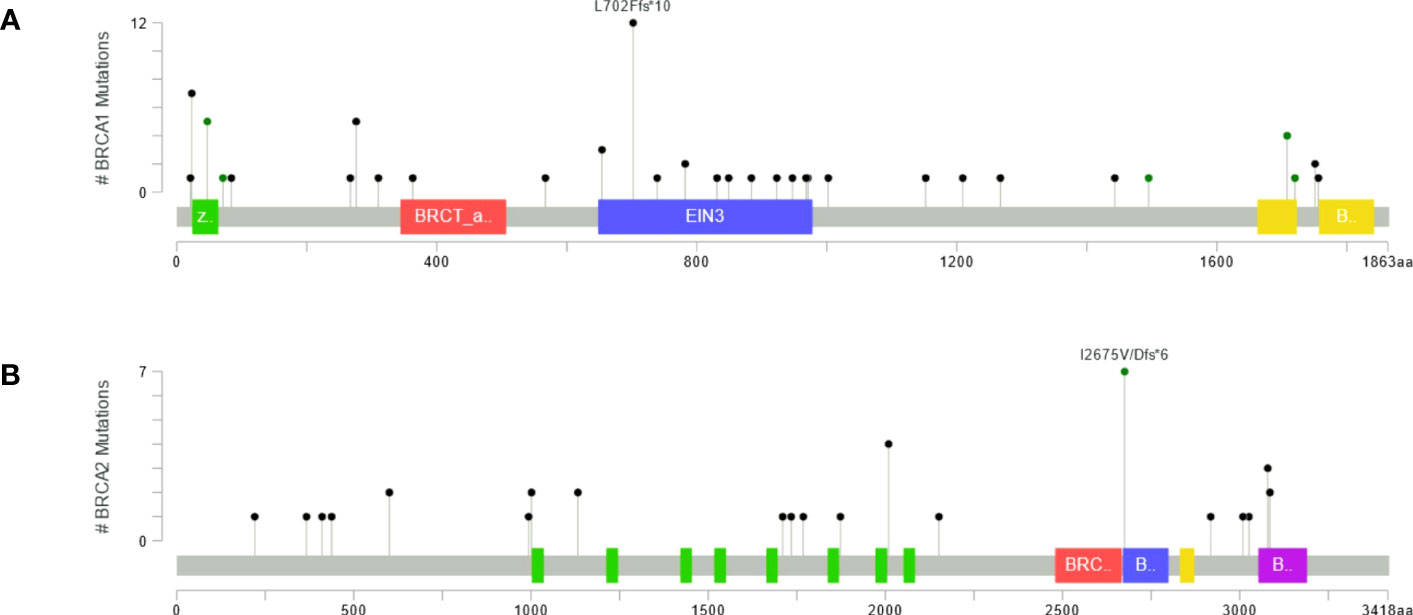
Figure 3 Maps presenting counts of pathogenic and likely pathogenic variants sites in (A) Brca1 and (B) Brca2 proteins.
Germline BRCA2 pathogenic/likely pathogenic variants
We found 22 different P/LP variants in BRCA2 among 36 patients, 22.2% (n=8/36) in BC and 77.8% (n=28/36) in OC. The most frequent mutations in BRCA2 were c.8023A>G (n=6, 16.67%), c.6024dupG (BIC: 6252insG, n=4, 11.11%), and c.9235delG (BIC: 9463delG, n=3, 8.33%) (Table 3). Likewise, most of the BRCA2 P/LP variants were found only in OC patients (n=14/22, 63.63%), followed by both OC and BC patients (n=4/22, 18.18%) and only BC patients (n=4/22, 18.18%). Furthermore, BRCA2 variants were mainly reported in exon 11 (n=9/22, 40.91%), predominantly inframe deletions (n=10/22), followed by inframe insertions (n=6/22) and missense variants (n=5/22) (Table 3). Only one large deletion was identified in exon 10. Patients with P/LP variations in BRCA2 were born in Metropolitan Lima (n = 24/36), on the coast (n=9/36) and in the highlands (n=3/36) (Figure 2B). The position of P/LP variants in relation to the Brca2 protein is shown in Figure 3B.
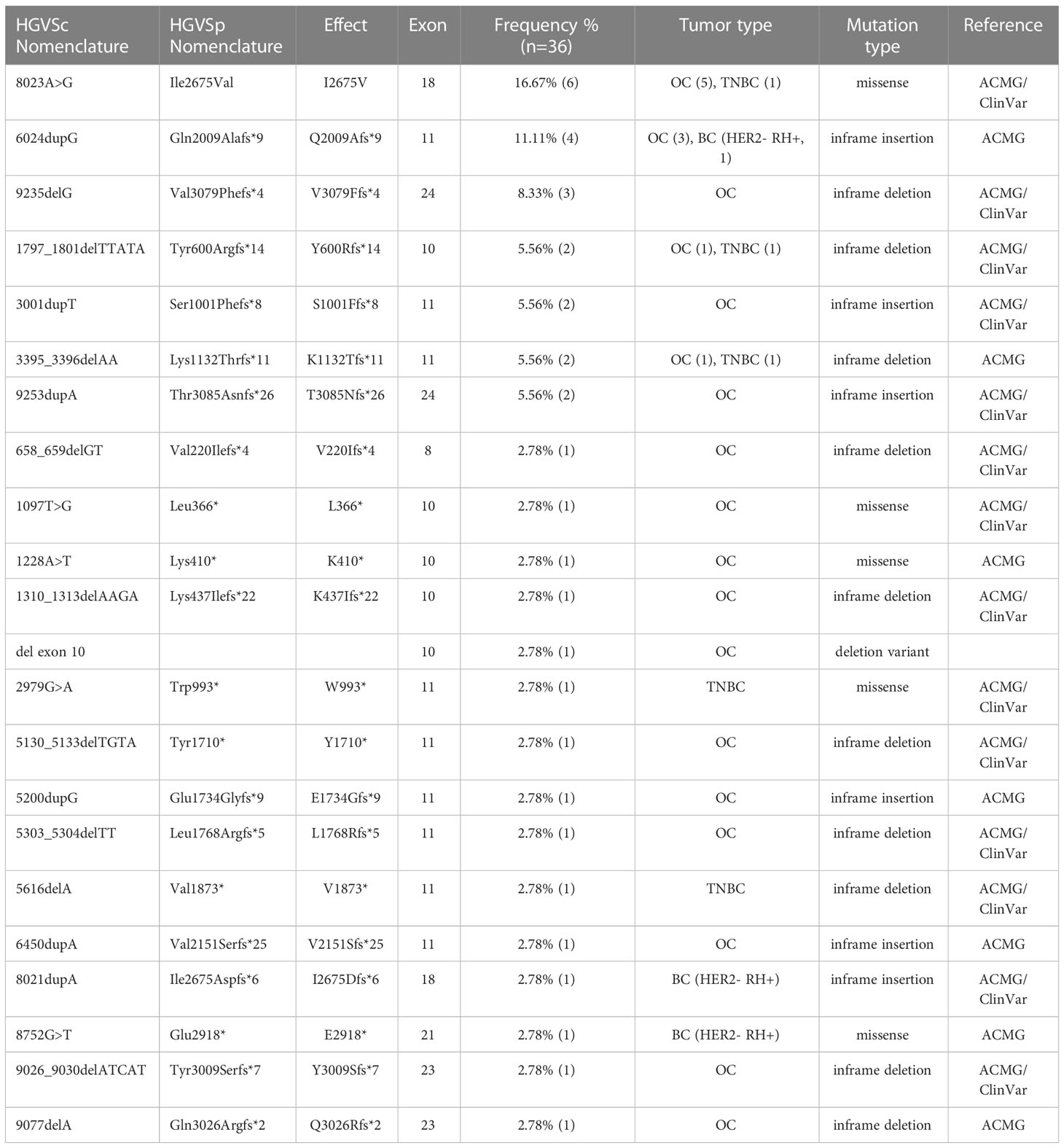
Table 3 Pathogenic/likely pathogenic germline BRCA2 variants found in our study.
BRCA1/2 germline VUS
BRCA1/2 variants classified as VUS were found in 7.23% (n=38/525) of the total study population. Regarding BRCA1, eight different VUS were found, with an overall frequency in patients of 1.71% (n = 9/525). Most VUS were reported only in patients with OC (n= 7/8, 87.5%) with a low frequency per variant (n=1/9, 1.1%) and most of them occurred in exon 10. Two VUS had conflicting classifications between ClinVar and the ACMG guidelines: BRCA1 c.93C>G (n = 2/9, 2.22%) and BRCA1 c.287A>G (Table S1). The overall frequency of VUS in BRCA2 was 5.52% (n=29/525). We identified 21 different VUS in BRCA2 and the most frequent were c.5465A>T (n = 4, 13.79%), followed by c.3101T>C (n = 3, 10.34%), c.205C>A and c.437T>C (n = 2, 6.89%). Similarly, many of the VUS occurred in exon 11 (n = 9/21, 42.86%) and were reported only in patients with OC (n = 14/21, 66.67%). Variants c.2274T>G, c.3509C>T, c.7617 + 6T>C, c.7759C>T, and c.8462T>C had conflicting classifications between the ACMG guidelines and ClinVar (Table S1). In addition the pathogenic scores of VUS founds in this study are also presented in Table S1.
Discussion
Breast and ovarian cancers are malignancies with a high incidence and prevalence in Latin American women. Costs of treatment and disability adjusted life years directly impact public health systems and society. The management of BC and OC is rapidly evolving with the discovery of new treatments that offer an improved survival advantage, as seen in recent years with PARP inhibitors in BRCA1/2 mutation carriers (19)
There is limited information on the molecular epidemiology of BRCA1/2 in Peru. Although a third of the Peruvian population lives in Lima, there are economic and geographic barriers that make it difficult for patients to access adequate cancer care, including molecular tests and genetic counseling (20). Our work has some limitations, for example, the underrepresentation of patients from several regions of Peru, which have socioeconomic and ancestry differences with respect to Lima. Another limitation that could cause bias is that the study population was selected for possible treatment with PARP inhibitors (e.g., advanced-stage cancer, HER2-negative breast cancer).
The study of BRCA1/2 variants in these patients is crucial to identify candidates for these treatments, but is also important to manage their future cancer risks. Patients with BRCA1/2 mutations and their families can benefit from cancer risk reduction or early cancer detection strategies, such as double mastectomy or high-risk follow-up for BC and bilateral salpingo-oophorectomy for OC (12).
Latin American countries usually have less infrastructure and resources for genetic testing and treatment of patients with BRCA1/2 than developed countries, and many of the cancer drugs approved in other countries are not available (21). Therefore, genetic testing is not always performed when needed. The interpretation of genetic variants can be more difficult in less-studied populations, and there are no specific open databases for variants in cancer-predisposing genes in Hispanic patients.
BRCA1 c.2105dupT was the most frequently found variant in this study. It is located in the coding exon 10 and causes a translational frameshift with a predicted alternate stop codon. This alteration is expected to result in loss of function, according to ClinVar. Until now, this variant was previously reported in 6 of 44 (13.6%) mutated patients with ovarian cancer belonging to the Peruvian population. Furthermore, it was reported only once in the Canadian population. A similar variant, BRCA1 c.2105dup, was identified in Caucasian and Hispanic individuals in a study that included only female carriers with pathogenic variants in BRCA1/2 (22)
In our cohort, we observed the BRCA1 c.68_69delAG mutation (185delAG), which occurs in exon 2 and creates a stop codon at position 39. This alteration leads to premature translation termination and significant protein truncation (23). Regarding its origin, it constitutes one of the primary founder mutations in the Ashkenazi Jewish population that arose 61 generations ago and was introduced into the Hispanic population 650 years ago (24). Currently, it has been reported among several other non-Jewish ethnic groups, such as Peruvians, Mexicans, Colombians, and Brazilians (25–28). A study in Peruvian patients diagnosed with breast cancer showed that 185delAG was the most common mutation found, observed in 7 of 13 carriers (54%). They also noted that two mutation carriers identified as of indigenous ancestry had the BRCA1 185delAG mutation (28). Unlike that study, we found that the mutation was observed in people born in Lima and Lambayeque. While it has not been determined whether they share an indigenous or Jewish ancestry, it is known that although the 185delAG mutation resides in a common haplotype among Ashkenazi Jews, it also arose independently in at least two non-Jewish populations, such as those in Malaysia and the United Kingdom. On the other hand, the BRCA1 c.140G>T mutation is a missense variant, which occurs within exon 5 and the RING domain. It was previously reported as a VUS in Peruvian families with hereditary breast and ovarian cancer (18, 24). However, it was also identified in the Norwegian population as a pathogenic and non-founder mutation (29).
The BRCA1 c.815_824dupAGCCATGTGG variant is located in exon 10 and is the most common pathogenic variant reported in African Americans (30). This pathogenic variant results in a frameshift and a spurious stop codon of 14 amino acids downstream. Due to its African origin, the variant was found in inherited patients with BC from Senegal and its allele frequency was 27.7%. In that study, the variant was also detected in a control population of sporadic BC cases and healthy controls without cancer (allele frequency estimated at 5% and 0.55%, respectively) (31). This variant was also found in Latin American populations, such as Colombian, Peruvian and Mexican (18, 32, 33). In Table 4, we summarize and compare our findings with those of other populations. Because we evaluated a very specific group of patients, comparison of prevalence of P/LP variants with other populations it would not be appropriate.
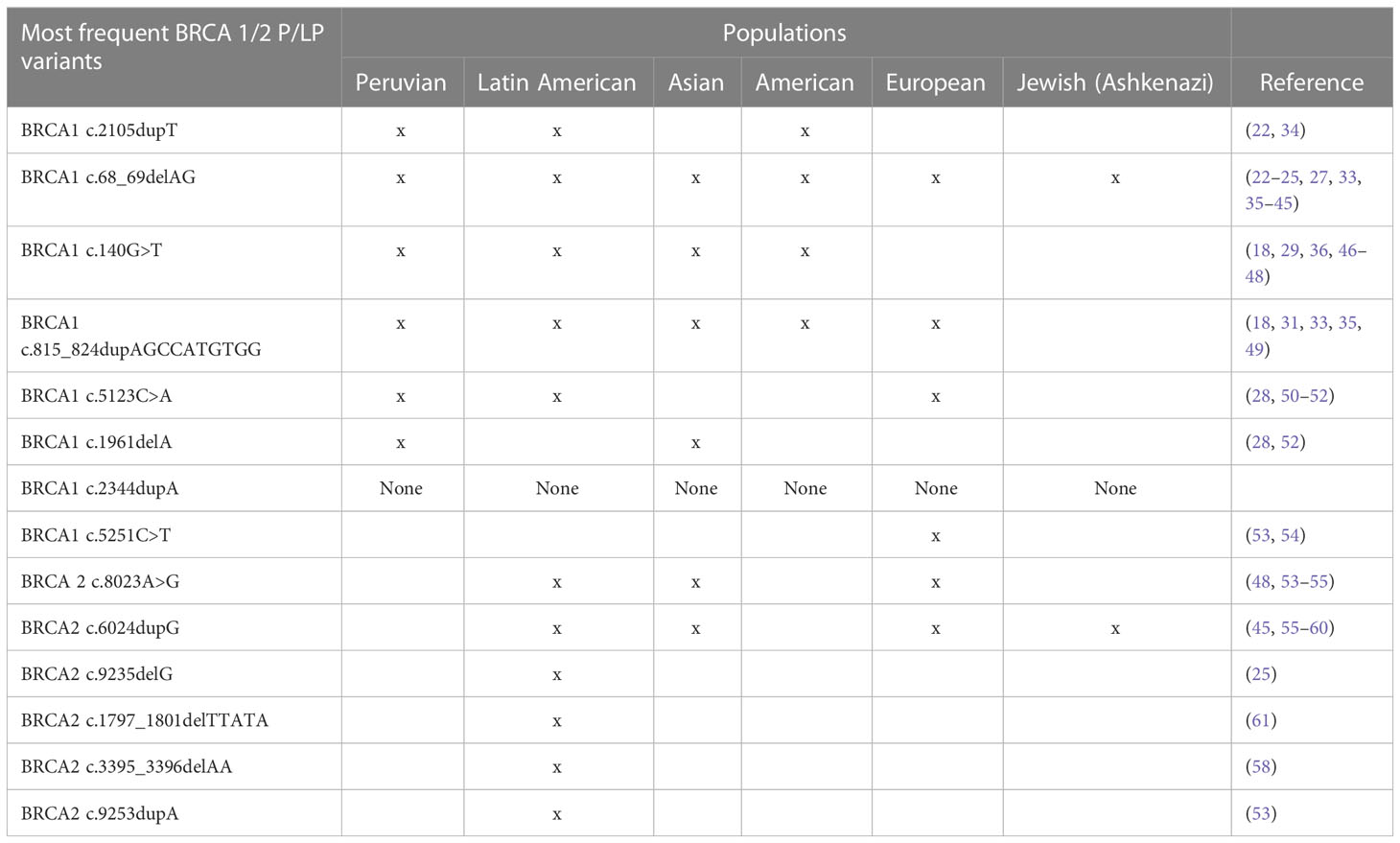
Table 4 Previous reports of BRCA1/2 variants found in this study in different populations.
In conclusion, in this selected Peruvian population, we found a frequency of 14.7% BRCA1/2 germline mutations in BC and 20.7% in OC. The most recurrent mutations were BRCA1 c.2105dupT and BRCA2 c.8023A>G. On the other hand, BRCA2 c.8023A>G, c.6024dupG and c.9235delG were not previously reported in Peruvian patients. BRCA1 c.2344dupA is a novel mutation that has not been previously reported in any database.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary Material.
Ethics statement
The study was approved by the Institutional Review Board of the Universidad Privada San Juan Bautista (418-2021-CIEI-UPSJB) and conducted in compliance with all relevant ethical guidelines. Due to the retrospective nature of the study, the informed consent was waived.
Author contributions
CB-L, JC, and FD conducted molecular assays and collected the data. CB-L, FD, YF, GR, and AC-R conducted analysis of variants. YF, GR, JA, LB, and JP conducted statistical analysis. MC conducted the bioinformatic analysis. YF, GR, JA, LB, and JP prepared Tables 1, 2. YF, GR, JA, LB, and JP prepared Figures 1-3. All authors wrote the manuscript. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1227864/full#supplementary-material
Abbreviations
VUS, Variants of Uncertain/Unknown Significance; PARP, Poly (Adenosine Diphosphate–Ribose) Polymerase; BC, Breast Cancer; OC, Ovarian Cancer; HBOC, Hereditary Breast and Ovarian Cancer; SSB, single-strand break repair, DSBs, Double-Strand DNA Breaks; CT, Chemotherapy; PFS, Progression-free survival; TNBC, Triple Negative Patients; CR/PR, Complete or Partial Response; HRD, Homologous Recombination Deficient; HER2, Human Epidermal Growth Factor Receptor 2; P/PL, Pathogenic/Likely Pathogenic; SNVs, Single Nucleotide Variants; PCR, Polymerase Chain Reaction; HGVS, Human Genome Variation Society (HGVS); dbSNP, Single Nucleotide Polymorphism Database; BIC, Breast Cancer Information Core; ACMG, American College of Medical Genetics.
References
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin (2021) 71(3):209–49. doi: 10.3322/caac.21660
2. Yoshida R. Hereditary breast and ovarian cancer (HBOC): review of its molecular characteristics, screening, treatment, and prognosis. Breast Cancer (2021) 28(6):1167–80. doi: 10.1007/s12282-020-01148-2
3. Saleem M, Ghazali MB, Wahab MAMA, Yusoff NM, Mahsin H, Seng CE, et al. The BRCA1 and BRCA2 genes in early-onset breast cancer patients. Adv Exp Med Biol (2020) 1292:1–12. doi: 10.1007/5584_2018_147
4. Petrucelli N, Daly MB, Pal T. BRCA1- and BRCA2-Associated Hereditary Breast and Ovarian Cancer (2022). GeneReviews®. Available at: https://www.ncbi.nlm.nih.gov/books/NBK1247/ (Accessed cited 2023 Jul 11).
5. Malone KE, Daling JR, Doody DR, Hsu L, Bernstein L, Coates RJ, et al. Prevalence and predictors of BRCA1 and BRCA2 mutations in a population-based study of breast cancer in white and black American women ages 35 to 64 years. Cancer Res (2006) 66(16):8297–308. doi: 10.1158/0008-5472.CAN-06-0503
6. Konstantinopoulos PA, Ceccaldi R, Shapiro GI, D’Andrea AD. Homologous recombination deficiency: exploiting the fundamental vulnerability of ovarian cancer. Cancer Discovery (2015) 5(11):1137–54. doi: 10.1158/2159-8290.CD-15-0714
7. Mavaddat N, Barrowdale D, Andrulis IL, Domchek SM, Eccles D, Nevanlinna H, et al. Pathology of breast and ovarian cancers among BRCA1 and BRCA2 mutation carriers: results from the Consortium of Investigators of Modifiers of BRCA1/2 (CIMBA). Cancer Epidemiol Biomarkers Prev (2012) 21(1):134–47. doi: 10.1158/1055-9965.EPI-11-0775
8. Song H, Cicek MS, Dicks E, Harrington P, Ramus SJ, Cunningham JM, et al. The contribution of deleterious germline mutations in BRCA1, BRCA2 and the mismatch repair genes to ovarian cancer in the population. Hum Mol Genet (2014) 23(17):4703–9. doi: 10.1093/hmg/ddu172
9. Farmer H, McCabe H, Lord CJ, Tutt AHJ, Johnson DA, Richardson TB, et al. Targeting the DNA repair defect in BRCA mutant cells as a therapeutic strategy. Nature (2005) 434(7035):917–21. doi: 10.1038/nature03445
10. Robson M, Im SA, Senkus E, Xu B, Domchek SM, Masuda N, et al. Olaparib for metastatic breast cancer in patients with a germline BRCA mutation. N Engl J Med (2017) 377(6):523–33. doi: 10.1056/NEJMoa1706450
11. Litton JK, Rugo HS, Ettl J, Hurvitz SA, Gonçalves A, Lee KH, et al. Talazoparib in patients with advanced breast cancer and a germline BRCA mutation. New Engl J Med (2018) 379(8):753–63. doi: 10.1056/nejmoa1802905
12. Gradishar WJ, Moran MS, Abraham J, Aft R, Agnese D, Allison KH, et al. Breast cancer, version 3.2022, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw (2022) 20(6):691–722. doi: 10.6004/jnccn.2022.0030
13. Moore K, Colombo N, Scambia G, Kim BG, Oaknin A, Friedlander M, et al. Maintenance olaparib in patients with newly diagnosed advanced ovarian cancer. N Engl J Med (2018) 379(26):2495–505. doi: 10.1056/NEJMoa1810858
14. Ray-Coquard I, Pautier P, Pignata S, Pérol D, González-Martín A, Berger R, et al. Olaparib plus bevacizumab as first-line maintenance in ovarian cancer. New Engl J Med (2019) 381(25):2416–28. doi: 10.1056/nejmoa1911361
15. González-Martín A, Pothuri B, Vergote I, DePont Christensen R, Graybill W, Mirza MR, et al. Niraparib in patients with newly diagnosed advanced ovarian cancer. New Engl J Med (2019) 381(25):2391–402. doi: 10.1056/NEJMoa1910962
16. Zavala VA, Serrano-Gomez SJ, Dutil J, Fejerman L. Genetic epidemiology of breast cancer in Latin America. Genes (Basel) (2019) 10(2). doi: 10.3390/genes10020153
17. Ossa CA, Torres D. Founder and recurrent mutations in BRCA1 and BRCA2 genes in Latin American countries: state of the art and literature review. Oncologist (2016) 21(7):832–9. doi: 10.1634/theoncologist.2015-0416
18. Buleje J, Guevara-Fujita M, Acosta O, Huaman FDP, Danos P, Murillo A, et al. Mutational analysis of BRCA1 and BRCA2 genes in Peruvian families with hereditary breast and ovarian cancer. Mol Genet Genomic Med (2017) 5(5). doi: 10.1002/mgg3.301
19. Shao F, Duan Y, Zhao Y, Li Y, Liu J, Zhang C, et al. PARP inhibitors in breast and ovarian cancer with BRCA mutations: a meta-analysis of survival. Aging (2021) 13(6):8975–88. doi: 10.18632/aging.202724
20. Pinto JA, Pinillos L, Villarreal-Garza C, Morante Z, Villarán MV, Mejía G, et al. Barriers in Latin America for the management of locally advanced breast cancer. Ecancermedicalscience (2019) 13. doi: 10.3332/ecancer.2019.897
21. Horgan D, Mia R, Erhabor T, Hamdi Y, Dandara C, Lal JA, et al. Fighting cancer around the world: A framework for action. Healthc (Basel) (2022) 10(11). doi: 10.3390/healthcare10112125
22. Rebbeck TR, Friebel TM, Friedman E, Hamann U, Huo D, Kwong A, et al. Mutational spectrum in a worldwide study of 29,700 families with BRCA1 or BRCA2 mutations. Hum Mutat (2018) 39(5):593–620. doi: 10.1002/humu.23406
23. Hartwig M, Janiszewska H, Bak A, Pilarska M, Heise M, Junkiert-Czarnecka A, et al. Prevalence of the BRCA1 c.68_69delAG (BIC: 185delAG) mutation in women with breast cancer from north-central Poland and a review of the literature on other regions of the country. Contemp Oncol (Pozn) (2013) 17(1):34–7. doi: 10.5114/wo.2013.33767
24. Laitman Y, Feng BJ, Zamir IM, Weitzel JN, Duncan P, Port D, et al. Haplotype analysis of the 185delAG BRCA1 mutation in ethnically diverse populations. Eur J Hum Genet (2013) 21(2):212–6. doi: 10.1038/ejhg.2012.124
25. Villarreal-Garza C, Alvarez-Gómez RM, Pérez-Plasencia C, Herrera LA, Herzog J, Castillo D, et al. Significant clinical impact of recurrent BRCA1 and BRCA2 mutations in Mexico. Cancer (2015) 121(3):372–8. doi: 10.1002/cncr.29058
26. Cock-Rada AM, Ossa CA, Garcia HI, Gomez LR. A multi-gene panel study in hereditary breast and ovarian cancer in Colombia. Fam Cancer (2018) 17(1):23–30. doi: 10.1007/s10689-017-0004-z
27. Dillenburg CV, Bandeira IC, Tubino TV, Rossato LG, Dias ES, Bittelbrunn AC, et al. Prevalence of 185delAG and 5382insC mutations in BRCA1, and 6174delT in BRCA2 in women of Ashkenazi Jewish origin in southern Brazil. Genet Mol Biol (2012) 35(3):599–602. doi: 10.1590/S1415-47572012000400009
28. Abugattas J, Llacuachaqui M, Allende YS, Velásquez AA, Velarde R, Cotrina J, et al. Prevalence of BRCA1 and BRCA2 mutations in unselected breast cancer patients from Peru. Clin Genet (2015) 88(4):371–5. doi: 10.1111/cge.12505
29. Heramb C, Wangensteen T, Grindedal EM, Ariansen SL, Lothe S, Heimdal KR, et al. BRCA1 and BRCA2 mutation spectrum - an update on mutation distribution in a large cancer genetics clinic in Norway. Hered Cancer Clin Pract (2018) 16(1):1–15. doi: 10.1186/s13053-017-0085-6
30. Scheuner MT, McNeel TS, Freedman AN. Population prevalence of familial cancer and common hereditary cancer syndromes. The 2005 California Health Interview Survey. Genet Med (2010) 12(11):726–35. doi: 10.1097/GIM.0b013e3181f30e9e
31. Ndiaye R, Diop JPD, Bourdon-Huguenin V, Dem A, Diouf D, Dieng MM, et al. Evidence for an ancient BRCA 1 pathogenic variant in inherited breast cancer patients from Senegal. NPJ Genom Med (2020) 5(1). doi: 10.1038/s41525-020-0114-7
32. Vargas E, Torres Lopez DM, Deugd R, Gil F, Nova A, Mora L, et al. Low prevalence of the four common Colombian founder mutations in BRCA1 and BRCA2 in early-onset and familial afro-Colombian patients with breast cancer. Oncologist (2019) 24(7):e475–9. doi: 10.1634/theoncologist.2018-0346
33. Herzog JS, Chavarri-Guerra Y, Castillo D, Abugattas J, Villarreal-Garza C, Sand S, et al. Genetic epidemiology of BRCA1- and BRCA2-associated cancer across Latin America. NPJ Breast Cancer (2021) 7(1). doi: 10.1038/s41523-021-00317-6
34. Molina J, Fernandez OOC, Lim M, Mas L, Veliz IF, Vargas C. BRCA 1/2 mutations in high-grade serous ovarian cancer (HGS-OC) patients of three Latin American countries: Report of 412 cases. J Clin Oncol (2019) 37(15_suppl):e14288–8. doi: 10.1200/JCO.2019.37.15_suppl.e14288
35. Jara L, Morales S, de Mayo T, Gonzalez-Hormazabal P, Carrasco V, Godoy R. Mutations in BRCA1, BRCA2 and other breast and ovarian cancer susceptibility genes in Central and South American populations. Biol Res (2017) 50(1). doi: 10.1186/s40659-017-0139-2
36. Solano AR, Mele PG, Jalil FS, Liria NC, Podesta EJ, Gutiérrez LG. Study of the genetic variants in BRCA1/2 and non- BRCA genes in a population-based cohort of 2155 breast/ovary cancer patients, including 443 triple-negative breast cancer patients, in Argentina. Cancers (Basel) (2021) 13(11). doi: 10.3390/cancers13112711
37. Bhaskaran SP, Huang T, Rajendran BK, Guo M, Luo J, Qin Z, et al. Ethnic-specific BRCA1/2 variation within Asia population: evidence from over 78 000 cancer and 40 000 non-cancer cases of Indian, Chinese, Korean and Japanese populations. J Med Genet (2021) 58(11):752–9. doi: 10.1136/jmedgenet-2020-107299
38. Kluz T, Jasiewicz A, Marczyk E, Jach R, Jakubowska A, Lubiński J, et al. Frequency of BRCA1 and BRCA2 causative founder variants in ovarian cancer patients in South-East Poland. Hered Cancer Clin Pract (2018) 16(1). doi: 10.1186/s13053-018-0089-x
39. Kechin A, Boyarskikh U, Barinov A, Tanas A, Kazakova S, Zhevlova A, et al. A spectrum of BRCA1 and BRCA2 germline deleterious variants in ovarian cancer in Russia. Breast Cancer Res Treat (2023) 197(2):387–95. doi: 10.1007/s10549-022-06782-2
40. Gabaldó Barrios X, Sarabia Meseguer MD, Marín Vera M, Sánchez Bermúdez AI, Macías Cerrolaza JA, Sánchez Henarejos P, et al. Molecular characterization and clinical interpretation of BRCA1/BRCA2 variants in families from Murcia (south-eastern Spain) with hereditary breast and ovarian cancer: clinical-pathological features in BRCA carriers and non-carriers. Fam Cancer (2017) 16(4):477–89. doi: 10.1007/s10689-017-9985-x
41. Nguyen-Dumont T, Karpinski P, Sasiadek MM, Akopyan H, Steen JA, Theys D, et al. Genetic testing in Poland and Ukraine: should comprehensive germline testing of BRCA1 and BRCA2 be recommended for women with breast and ovarian cancer? Genet Res (Camb) (2020) 102. doi: 10.1017/S0016672320000075
42. Manzanares Campillo M, Muñoz Atienza V, Sánchez Tapia EM, Martín Fernández J. Portadoras de mutaciones en BRCA1 y 2 en familias de alto riesgo del área de Ciudad Real (España): prevalencia mutacional y características clínico-patológicas del cáncer de mama y ovario. Rev Senol Y Patol Mamaria J Breast Sci (2018) 31(2):59–66. doi: 10.1016/j.senol.2018.04.002
43. Kang PCE, Phuah SY, Sivanandan K, Kang IN, Thirthagiri E, Liu JJ, et al. Recurrent mutation testing of BRCA1 and BRCA2 in Asian breast cancer patients identify carriers in those with presumed low risk by family history. Breast Cancer Res Treat (2014) 144(3):635–42. doi: 10.1007/s10549-014-2894-x
44. Gallardo-Rincón D, Montes-Servín E, Alamilla-García G, Montes-Servín E, Bahena-González A, Cetina-Pérez L, et al. Clinical benefits of olaparib in mexican ovarian cancer patients with founder mutation BRCA1-del ex9-12. Front Genet (2022) 13. doi: 10.3389/fgene.2022.863956
45. Fernandes GC, Michelli RAD, Galvão HCR, Paula AE, Pereira R, Andrade CE, et al. Prevalence of BRCA1/BRCA2 mutations in a Brazilian population sample at-risk for hereditary breast cancer and characterization of its genetic ancestry. Oncotarget (2016) 7(49):80465–81. doi: 10.18632/oncotarget.12610
46. Jarhelle E, Riise Stensland HMF, Mæhle L, Van Ghelue M. Characterization of BRCA1 and BRCA2 variants found in a Norwegian breast or ovarian cancer cohort. Fam Cancer (2017) 16(1):1–16. doi: 10.1007/s10689-016-9916-2
47. Parsons MT, Tudini E, Li H, Hahnen E, Wappenschmidt B, Feliubadaló L, et al. Large scale multifactorial likelihood quantitative analysis of BRCA1 and BRCA2 variants: An ENIGMA resource to support clinical variant classification. Hum Mutat (2019) 40(9):1557–78. doi: 10.1002/humu.23818
48. Ponce J, Vigil C, Araujo J, Castañeda C, Calderon G, Buleje J, et al. Abstract P5-09-08: Molecular evaluation of Peruvian patients with hereditary breast cancer reveals a novel germline mutation in BRCA1. Cancer Res (2017) 77(4_Supplement):P5-09-08. doi: 10.1158/1538-7445.SABCS16-P5-09-08
49. Pal T, Bonner D, Cragun D, Monteiro ANA, Phelan C, Servais L, et al. A high frequency of BRCA mutations in young black women with breast cancer residing in Florida. Cancer (2015) 121(23):4173–80. doi: 10.1002/cncr.29645
50. Díez O, Osorio A, Durán M, Martinez-Ferrandis JI, de la Hoya M, Salazar R, et al. Analysis of BRCA1 and BRCA2 genes in Spanish breast/ovarian cancer patients: a high proportion of mutations unique to Spain and evidence of founder effects. Hum Mutat (2003) 22(4):301–12. doi: 10.1002/humu.10260
51. Iyevleva AG, Suspitsin EN, Kroeze K, Gorodnova TV, Sokolenko AP, Buslov KG, et al. Non-founder BRCA1 mutations in Russian breast cancer patients. Cancer Lett (2010) 298(2):258–63. doi: 10.1016/j.canlet.2010.07.013
52. Vidal AF, Ferraz RS, El-Husny A, Silva CS, Vinasco-Sandoval T, Magalhães L, et al. Comprehensive analysis of germline mutations in northern Brazil: a panel of 16 genes for hereditary cancer-predisposing syndrome investigation. BMC Cancer (2021) 21(1). doi: 10.1186/s12885-021-08089-9
53. Rogoża-Janiszewska E, Malińska K, Cybulski C, Jakubowska A, Gronwald J, Huzarski T, et al. Prevalence of recurrent mutations predisposing to breast cancer in early-onset breast cancer patients from Poland. Cancers (Basel) (2020) 12(8):1–10. doi: 10.3390/cancers12082321
54. Szwiec M, Jakubowska A, Górski B, Huzarski T, Tomiczek-Szwiec J, Gronwald J, et al. Recurrent mutations of BRCA1 and BRCA2 in Poland: an update. Clin Genet (2015) 87(3):288–92. doi: 10.1111/cge.12360
55. Blay P, Santamaría I, Pitiot AS, Luque M, Alvarado MG, Lastra A, et al. Mutational analysis of BRCA1 and BRCA2 in hereditary breast and ovarian cancer families from Asturias (Northern Spain). BMC Cancer (2013) 13. doi: 10.1186/1471-2407-13-243
56. Kim JH, Park S, Park HS, Park JS, Lee ST, Kim SW, et al. Analysis of BRCA1/2 variants of unknown significance in the prospective Korean Hereditary Breast Cancer study. Sci Rep (2021) 11(1). doi: 10.1038/s41598-021-87792-w
57. Sakamoto I, Hirotsu Y, Nakagomi H, Ouchi H, Ikegami A, Teramoto K, et al. BRCA1 and BRCA2 mutations in Japanese patients with ovarian, fallopian tube, and primary peritoneal cancer. Cancer (2016) 122(1):84–90. doi: 10.1002/cncr.29707
58. Yamaguchi-Kabata Y, Yasuda J, Tanabe O, Suzuki Y, Kawame H, Fuse N, et al. Evaluation of reported pathogenic variants and their frequencies in a Japanese population based on a whole-genome reference panel of 2049 individuals. J Hum Genet (2017) 63(2):213–30. doi: 10.1038/s10038-017-0347-1
59. Tokunaga H, Iida K, Hozawa A, Ogishima S, Watanabe Y, Shigeta S, et al. Novel candidates of pathogenic variants of the BRCA1 and BRCA2 genes from a dataset of 3,552 Japanese whole genomes (3.5KJPNv2). PloS One (2021) 16(1). doi: 10.1371/journal.pone.0236907
60. Hirotsu Y, Nakagomi H, Sakamoto I, Amemiya K, Mochizuki H, Omata M. Detection of BRCA1 and BRCA2 germline mutations in Japanese population using next-generation sequencing. Mol Genet Genomic Med (2015) 3(2):121–9. doi: 10.1002/mgg3.120
Keywords: breast cancer, ovarian cancer, BRCA1, BRCA2, germline mutation
Citation: Ferreyra Y, Rosas G, Cock-Rada AM, Araujo J, Bravo L, Doimi F, Casas J, Clavo MdlÁ, Pinto JA and Belmar-López C (2023) Landscape of germline BRCA1/BRCA2 variants in breast and ovarian cancer in Peru. Front. Oncol. 13:1227864. doi: 10.3389/fonc.2023.1227864
Received: 23 May 2023; Accepted: 27 July 2023;
Published: 17 August 2023.
Edited by:
Charles Theillet, Institut du Cancer de Montpellier (ICM), FranceReviewed by:
Ekaterina Kuligina, N.N. Petrov National Medical Research Center of Oncology, RussiaAlvaro Galli, National Research Council (CNR), Italy
Copyright © 2023 Ferreyra, Rosas, Cock-Rada, Araujo, Bravo, Doimi, Casas, Clavo, Pinto and Belmar-López. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Joseph A. Pinto, anBpbnRvQGdlY29wZXJ1Lm9yZw==