
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Sustain. Food Syst. , 18 February 2025
Sec. Nutrition and Sustainable Diets
Volume 9 - 2025 | https://doi.org/10.3389/fsufs.2025.1510426
This article is part of the Research Topic Sustainable Diets with Sociocultural and Economic Considerations View all 17 articles
 Khulud Alrougui1
Khulud Alrougui1 Ghedeir M. Alshammari1*
Ghedeir M. Alshammari1* Khalid N. Alrwis2Kholoud B. Alabdulkarem3
Khalid N. Alrwis2Kholoud B. Alabdulkarem3 Mohammed Abdo Yahya1
Mohammed Abdo Yahya1Introduction: Obesity is most common among people with low incomes in high-income countries, although being overweight affects all socioeconomic categories. This study evaluated the nutritional and health status and their associated variables in low-income Saudi females.
Methods: A structured questionnaire was used to collect participants’ (153 women) sociodemographic profiles and other health data (hypertension, diabetes, thyroid, and anemia status). Nutrient intake, anthropometric indices, minimal dietary diversity scores (MDDS), and lipid profiles were also measured. Chi-squared and Student-t tests were used to detect significant variation among groups, and Spearman correlation was used to determine factors affecting the nutritional status of women.
Results and discussion: As their sociodemographic profiles varied greatly, some participants’ nutrient intake was significantly lower (p ≤ 0.01) than their dietary recommended intake (DRI). However, the anthropometric indices differed significantly between the women with high and low MDDS (p ≤ 0.01). The rate of females with obesity outperformed the other groups regarding MDDS, followed by those who are overweight. Furthermore, a significant (p ≤ 0.001) variation in lipid profile was observed between subjects. Despite the majority of participants having normal cholesterol, LDL-C, and triglyceride levels, their HDL-C levels were either at high risk or borderline risk. The majority of the participants showed no signs of anemia, hypertension, diabetes, or thyroid issues. Interestingly, whereas education level was negatively and significantly at (p ≤ 0.05 or p ≤ 0.001) linked with some anthropometric indices, the factors age, family size, source of income, social welfare benefits, and marital status were positively and significantly associated with some of these variables. According to this study, low-income Saudi females face several challenges in adopting a nutritional and healthy lifestyle, as indicated by the parameters evaluated.
Malnutrition and unhealthy diets are major and significant factors that increase the risk of developing and progressing several non-communicable diseases (Branca et al., 2019). Current international policies have recommended increasing the availability of low-cost, high-calorie foods from staple grain crops to reduce hunger worldwide, and accordingly, this has influenced dietary diversity and led to the supplantation of native, often healthier, diets (Branca et al., 2019). However, access to a variety of micronutrient-dense foods, such as fresh fruits, vegetables, legumes, pulses (beans, peas, and lentils), and nuts, has not yet improved equally for all (Scott, 2017). On the other hand, hazardous diets rich in salt, sugar, saturated fats, and trans fats are becoming more widely available and cheap to the general public (Scott, 2017).
Non-communicable diseases are considered one of the most important health concerns in the Kingdom of Saudi Arabia with millions projected to be impacted by 2030 (Gosadi, 2019; Hazazi and Wilson, 2022). In this region of the world, the mortality rate due to non-communicable diseases is estimated to be 73.2% and is considered the leading cause of the overall burden caused by disability (Hazazi and Wilson, 2022). Such high rates were attributed to the subject’s behavioral and lifestyle risk factors, including the over-consumption of an unhealthy diet (Alqunaibet et al., 2021). Several studies have shown that many factors increase the consumption of a healthy diet (Gurewich et al., 2020; Hill-Briggs et al., 2021; Perez-Escamilla et al., 2018; Vilar-Compte et al., 2021). Important components are the social non-medical health determinants such as income, housing, education, and food security (Hill-Briggs et al., 2021). Indeed, the social determinants of health, or differences in health status between socioeconomic groups, are regarded to be the root causes and underlying reasons for health disparities (Gurewich et al., 2020). Nevertheless, the nutrition disparities are reflected as undernutrition, overweight, and obesity, which may occur under inequitable socioeconomic situations in the nutritional context, such as urban poverty (Perez-Escamilla et al., 2018; Vilar-Compte et al., 2021). In this regard, it was shown that an individual’s income is essential in contemporary life to secure a nutritious diet due to the global cost of living crisis (Eskandari et al., 2022). This becomes even more crucial during an emergency, as demonstrated by the COVID-19 pandemic, which placed a double burden on low-income populations (Fitzpatrick et al., 2021). According to a national study on the eating habits of the Saudi population, only a small portion complies with dietary recommendations, and high-income households consume more fruits than low-income households that tend to drink more sugar-sweetened beverages (Moradi-Lakeh et al., 2017). This phenomenon can be explained by the higher consumption of low-income individuals of inexpensive and highly calorie-dense diets with poor micronutrient content (Hamedi-Shahraki et al., 2021). Therefore, financial accessibility is one of the four fundamental pillars of food and nutrition security, including the availability, utilization, and stability of food. This is accomplished when everyone, at all times, has physical, social, and economic access to enough safe and nutritious food to satisfy their dietary needs and food preferences for an active and healthy life (Ryckman et al., 2021). As a result, a lack of affordable nutrition has been connected to several adverse health consequences, such as stress, hypertension, obesity, diabetes, and dyslipidemia (da Silva Miguel et al., 2020).
On the other hand, women remain the most vulnerable group worldwide regarding food-related financial difficulties as they are “disproportionately affected by health and economic crises in several areas of the globe” (Botreau and Cohen, 2020). Women in Saudi Arabia are far more likely than men to suffer infectious diseases. According to a recent study on socioeconomic disparities and related infectious disease variables in Saudi Arabia (Hanawi and Keetile, 2021), obesity and overweight rates were higher among females than males, 67.5 and 63.1%, respectively. Moreover, women with lower education and less income are more likely to develop infectious diseases. Low-income Saudi women receive government and charity assistance such as welfare and food assistance (Kaiser et al., 2019). Despite this, receiving these services does not ensure healthier outcomes. In support, it was shown that food assistance users have higher rates of poor health outcomes (Kaiser et al., 2019). According to the National Supplemental Nutrition Assistance Program (SNAP), Americans, diet-related chronic disease rates and poor dietary habits among recipients remain high despite the dramatically reduced food insecurity rates among low-income (Verghese et al., 2019).
In the Riyadh region, the capital of Saudi Arabia, social assistance beneficiaries counted 135,520 by the end of November 2021, with 39,124 men and 96,396 women (Derbal, 2022). Even more, divorced and widowed women receive welfare despite living with their families and facing fewer financial difficulties than other women (Fadaak, 2010). Also, food relief programs in Saudi Arabia are generally delivered by non-governmental organizations rather than national government programs (Derbal, 2022). Studies on the nutritional status of low-income people, particularly food assistance recipients, are rare in Saudi Arabia. Therefore, this study aimed to evaluate the nutritional and health status of low-income Saudi females in Riyadh who are registered in food assistance programs, as well as to identify factors associated with their nutritional status.
This cross-sectional study focuses on low-income Saudi women (153 women) aged 19 to 58 years old who are receiving governmental food assistance in Riyadh. The Al-Nadah organization assisted in the identification of the participants. Riyadh (the capital city of Saudi Arabia) was chosen due to its large and diverse population, as well as being the location with the highest number of welfare claimants. Inclusion criteria were: Saudi women aged more than 18 years old, residing in Riyadh, and receiving food assistance. The cross-section study’s accuracy and prevalence of satisfaction were considered while calculating the sample size, and participants were chosen using inclusion and exclusion criteria. Women who refused to sign the informed consent form or had particular features, such as pregnancy or a mental or physical handicap, were excluded because they had specific requirements and were more likely to experience additional problems that might interfere with the results. In accordance, 153 women who fit the inclusion criteria were included in the study. The data collection was broken down into three sections: (1) interviewing and measurements of anthropometric parameters; (2) blood sampling and collection; and (3) a health awareness campaign including dietary and health habits by medical professionals.
To detect a median-sized main effect with a statistical power of 1−β = 0.80 (i.e., if the effect exists, there is a 80% chance of detecting a true positive), a two-tailed test with an α of 0.05 (i.e., there is a 5% risk of discovering a false positive) was used. To determine the required N, the three main parameters (anticipated d, target power, and α) were entered into G*Power, which utilized the following formula (Faul et al., 2007)
Where Z(1-α/2 = 0.025) = 1.96 and Z(1-β = 0.80) = 0.84 are the critical Z values associated with a two-tailed test with α = 0.05 and 1 − β = 0.80, d = 0.50, respectively. We simply assumed that the intervention worked as expected, and a sample size of 125 participants gave us a 80% probability of observing the median-sized (or larger) effect of the condition with p < 0.05.
A structured questionnaire and face-to-face interviews were delivered to all participants to collect information about age, family size, educational level, marital status, monthly income, social welfare benefits received, and/or any other financial assistance obtained. The questionnaire was also used to collect participants’ history of any chronic disorders such as hypertension, diabetes, thyroid, and anemia and compare it with the existing medical report. All data were gathered by certified researchers.
A multiple-frequency ACCUNIQ BC360 body composition analyzer (SELVAS Healthcare Inc., Daejeon, Korea) was used to measure anthropometric parameters as per the manufacturers’ instructions. Parameters analyzed were such as the percentage body fat (PBF), BMI, and visceral fat (VF) (in duplicate). A non-stretchable meter was used to gauge each subject’s height (H), hip circumference (HC), and waist circumference (WC). The waist-to-height ratio (WHtR) was computed by dividing WC over H, and the waist-to-hip ratio (WHR) by dividing WC over HC. BMI was computed as a weight-to-height ratio in Kg/m2. The classifications of the BMI, WHtR, and WHR were performed following previous studies (Ashwell et al., 2012; WHO, 2000, 2008).
A venous blood sample (10 mL) was drawn from each participant at 8 to 12 h fasting. Samples were taken at two different times between 11 a.m. and 1 p.m. to eliminate the effects of timing and dietary intake on the measured biochemical parameters and to ensure consistent fasting duration at both times. All samples were transported to the laboratory in sterile capped tubes and put in an ice container. Thereafter, they were centrifuged (3,000 rpm/15 min) to collect serum. The collected serum samples were preserved at −80°C until biochemical analysis. Serum levels of cholesterol, HDL-C, LDL-C, and triglyceride were assessed using Roche Cobas 6,000 equipment (model c 501/Germany) according to the manufacturer’s instructions.
Because it has been found to predict appropriate nutrient intake (Kennedy et al., 2011) and can be used as a proxy indicator for determining nutrient adequacy among pregnant females (Wen et al., 2010), the minimum dietary diversity for women (MDD-W) was used to assess the overall dietary quality of participants. The MDD-W indicator is based on the WDDS-10, a 10-food-group women’s dietary diversity score. Starch staples (grains, roots, and tubers), pulses/legumes, nuts and seeds, dairy, flesh foods (meat, fish, and poultry), eggs, dark leafy greens and vegetables, vitamin A-rich fruits and vegetables, other vegetables, and other fruits were among these food groups. The WDDS (Wen et al., 2010), based on a 24-h dietary recall period, was used to define the average normal food intake of pregnant women in the research area. The women were asked to recall all foods consumed from the above food groups on the previous day. Responses were recorded as “yes” or “no.” A “yes” response was scored as 1, and a “no” response was scored as 0. The scores were summed up to indicate the women’s DD score. Based on the MDD-W, the dietary scores were considered as low or high diversity. Women with a diversity score of less than 5 were classed as having low dietary variety, whereas women with scores of 5–10 were classified as having high dietary diversity (FAO, 2016.).
For 1 day, 24-h dietary recall (24HDR) was completed by face-to-face interviews for all items consumed the previous day, including breakfast, lunch, dinner, and snacks, using an authorized structured questionnaire. Dietitians and trained researchers recorded dietary intake, assisting participants in reporting accurate serving size measurements using standard measures, such as a teaspoon, tablespoon, cup, gram, or liter, and encouraging participants to provide detailed information about food types, cooking methods, food product brand names, and food additives. Following each interview, the data were examined to establish adequacy and to identify any missing or confused information. According to AlZoubi et al. (2021), the dietary data were analyzed using a software application for nutritional research and therapeutic purposes (ESHA’s Food Processor® Nutrition Analysis). The resulting energy and nutritional values were compared to the DRI using a Student two-tail t-test as defined by Meyers et al. (2006).
The statistical analysis was carried out using the Statistical Package for Social Sciences (SPSS, version 25) (SPSS Inc., Chicago, IL, United States). The sociodemographic variables, anthropometric indices, and blood parameters of research participants were reported as frequencies and percentages. A chi-squared test was conducted to determine if there were significant differences within the group. The mean and standard deviation (SD) of continuous data were calculated. The subjects’ dietary intake and DRI mean values were compared using a one-sample Student’s two-tailed t-test. The cutoff for significance was set at p ≤ 0.05 or p ≤ 0.001. The Fisher exact test was calculated to test the association between MDD-W food group consumption and MDD-W score. To determine the risk factors for low-income Saudi females, bivariate analysis was used. The relationship between anthropometric measurements (BMI, PBF, VF, WHR, and WHtR) and sociodemographic factors (age, family size, monthly income, source of income, social welfare benefits, education, and marital status) was investigated using Spearman correlation.
Table 1 shows the sociodemographic characteristics of the participants. A real positive statistical power has an 80% probability of being detected, according to a G-power study of 125 individuals. However, 153 eligible participants agreed to be involved in this study after being approached. Sociodemographic factors generally differed significantly (p ≤ 0.01) between participants. Females aged 39 to 48 (45.8%) outnumbered those aged 29 to 38 (37.3%). Families with 5–7 members were the most common (45.8%), followed by those with 2 to 4 members (28.1%).
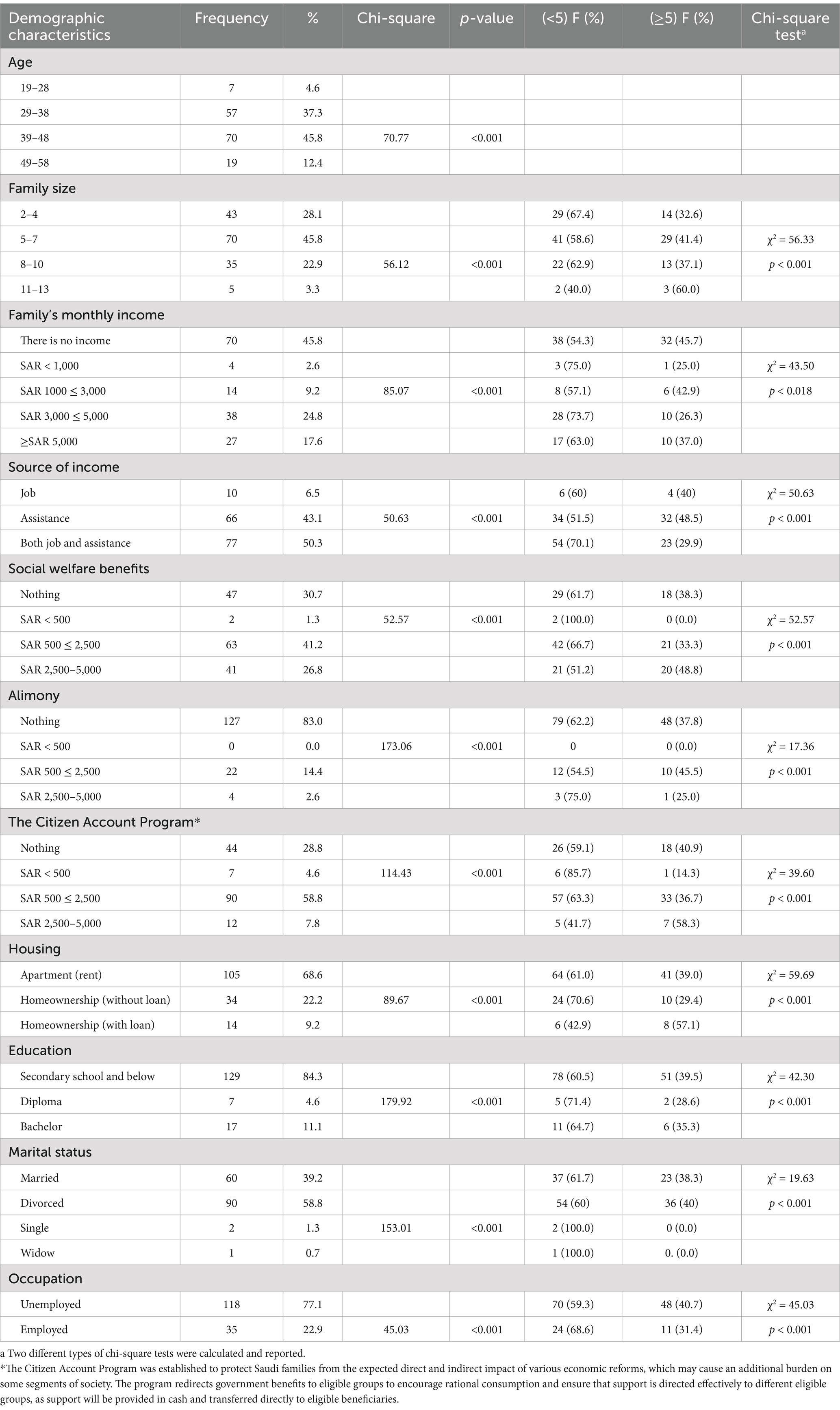
Table 1. Demographic characteristics of participants (n = 153) and bivariate analyses of factors associated with women’s minimum dietary diversity (MDD-W).
The majority of females have temporary occupations and rely on assistance for income (50.33%), followed by those with no monthly income (45.8%), those who exclusively get assistance (43.14%), and those with incomes ranging from 3,000 to 5,000 SR (24.8%). The participants’ social welfare benefits varied, with the majority (41.18%) receiving 500–2,500 SR, 83.01% receiving no alimony, and more than half enrolling in The Citizen Account Program. Most females (68.63%) reside in rented apartments, while the remaining (22.22%) live in their own homes free of debt, and 9.15% do so with debt. A high school diploma or lower is the level of education held by 84.31% of females, while a bachelor’s degree is held by 11.11%. Women who were married (39.22%) and divorced (58.82%) represent the two major groups. Only 22.88% of women were employed, compared to 77.12% who were unemployed. According to Table 1, the bivariate analysis revealed a significant (p ≤ 0.001) association between participants’ dietary diversity for women and the sociodemographic factors. It revealed that the proportion of women with lower dietary diversity scores significantly increased with decreased socioeconomic benefits. It was high in the women who have no monthly income, hold temporary employment or receive assistance, are not receiving Alimony, are enrolled in The Citizen Account Program, live in an apartment (rent), have a low education level, and are divorced and unemployed.
The average nutritional consumption is compared to the DRIs in Table 2. The results demonstrated that the low-income Saudi female’s overall real intake of macro- and micronutrients fell short of the recommended dietary requirement. Protein, fiber, minerals, vitamins, cholesterol, and thiamin intake were significantly (p ≤ 0.01 or p ≤ 0.05) lower than the daily essential quantity. However, calories, carbohydrates, and total fat were significantly higher than the DRI, while unsaturated fat intake was high but did not differ significantly from the DRI.

Table 2. Average daily intake of nutrients as compared to the dietary requirement intake (DRI).
The females’ anthropometric indices (BMI, PBF, VF, WHR, and WHtR) were calculated, and the results are displayed in Table 3. According to the statistics, there was a significant (p ≤ 0.01) difference in BMI categories among the individuals. Females with obesity, whether I, II, or III (62.8%), outperformed the other groups, followed by those with overweight (24.18%). Bivariate analysis revealed a significant (χ2 = 45.37; p < 0.05) positive connection between BMI categories and women’s minimum dietary diversification. Because the distribution of adipose tissue varies between individuals, BMI as a measure of a respondent’s obesity may not always precisely indicate the degree of a respondent’s visceral fat level. As a result, in this study, in addition to using BMI as an indicator, PBF, VF, WHR, and WHtR were measured to provide a comprehensive assessment of a female’s nutritional status. In terms of PBF, there was a significant (p ≤ 0.01) variance in PBF categories across participants, with more than half of the participants (50.3%) having a very high PBF, followed by those with a high PBF (31.8%). The findings revealed a strong and positive relationship between the PBF, VF, WHR, and WHtR categories and women’s mini-mum dietary diversity. However, the data showed that 64.1% of participants had normal VF, whereas 30.1% had high VF.
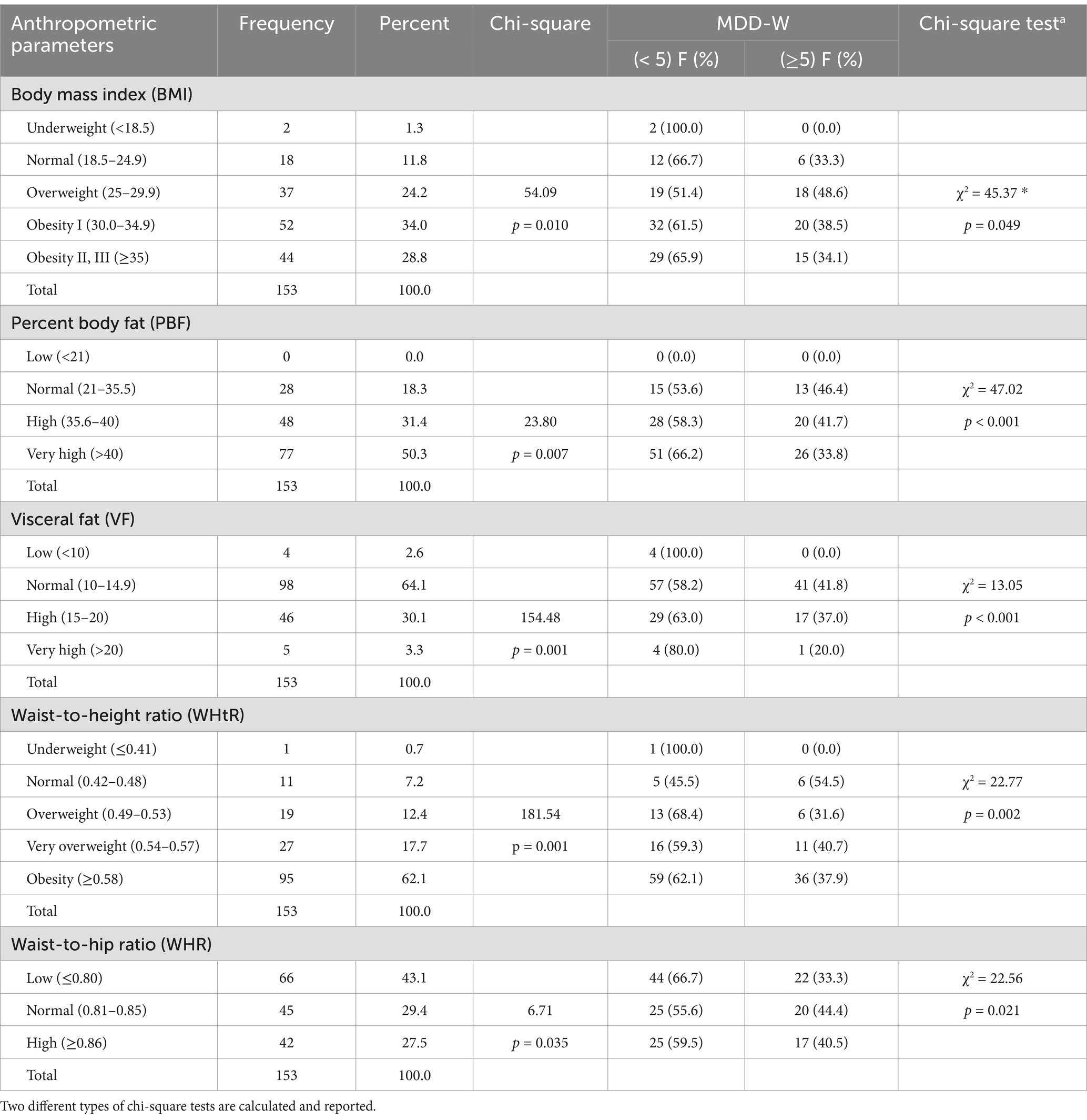
Table 3. Distribution frequency of anthropometric parameters (BMI, WC, WHR, FM, VF), and bivariate analyses of factors associated with women’s minimum dietary diversity (MDD-W).
Table 4 shows the MDD-W food group intake by BMI category as well as the total MDD-W score. Each participant’s consumption of 10 food groups was measured to establish an MDD-W score. Low-income Saudi females with MDD-W scores ≥5 consumed more vegetables and fruits than women with MDD-W scores <5 (Table 4). Overall, 52.8% of participants did not meet the minimal dietary variety requirement, and only 47.2% had MDD-W scores. With few exceptions, the majority of obese female participants did not consume pulses, such as beans, peas, lentils, nuts, and seeds, as well as dark leafy greens and vegetables, various fruits and vegetables high in vitamin A, and other meals. Pulses were consumed by only 8.5% of participants with minimum dietary diversity and 5.8% with poor nutritional diversity scores. Meat, fish, and poultry were more popular than eggs. Figure 1 depicts multiple regression analyses between WHR and WHtR and participants’ BMI, PBF, and VF. Multiple regression analyses of BMI, WHR, and WHtR (Figure 1A) revealed a positive connection (R2 = 0.738), indicating that an increase in WHR or WHtR is associated with an increase in BMI. Furthermore, a relationship between PBF, WHR, and WHtR (Figure 1B) revealed that a rise in WHR or WHtR increased PBF (R2 = 0.512), as well as an increase in VF (R2 = 0.697).
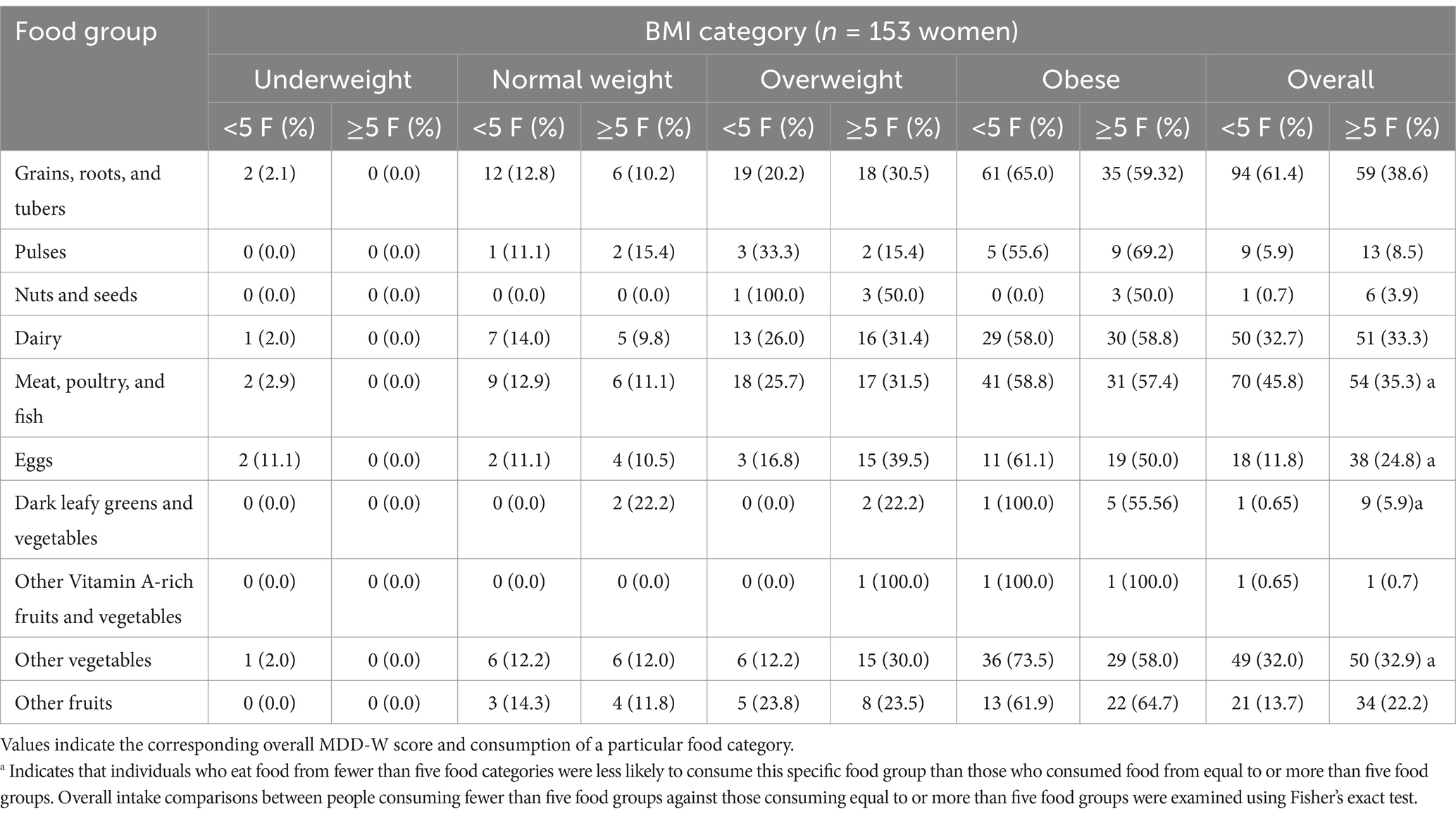
Table 4. MDD-W food group consumption according to total MDD-W score.

Figure 1. Multiple regression analyses between BMI and WHR and WHtR (A), R2 = 0.738; PBF and WHR and WHtR (B), R2 = 0.512; and VF and WHR and WHtR (C), R2 = 0.697.
Table 5 depicts the basic hematological features of low-income Saudi females. According to the findings, a significant (p ≤ 0.001) variance in cholesterol levels was noted across participants. The majority of participants (61.4%) had normal cholesterol, whereas 4.6% had high cholesterol. HDL-C levels were either high (47.7%) or normal (47.1%), with a significant (p ≤ 0.001) difference between groups. However, most females (70.6%) had normal LDL-C levels, and those with normal levels (24.2%) came in second. There was also a significant (p ≤ 0.001) difference between categories. There was a significant (p ≤ 0.001) difference in the triglyceride levels of the subjects. Most participants (83.0%) had low levels, while 11.76% had normal levels. The majority of participants (88.9%) did not have hypertension, diabetes, thyroid problems (96.1%), or anemia (93.5%).
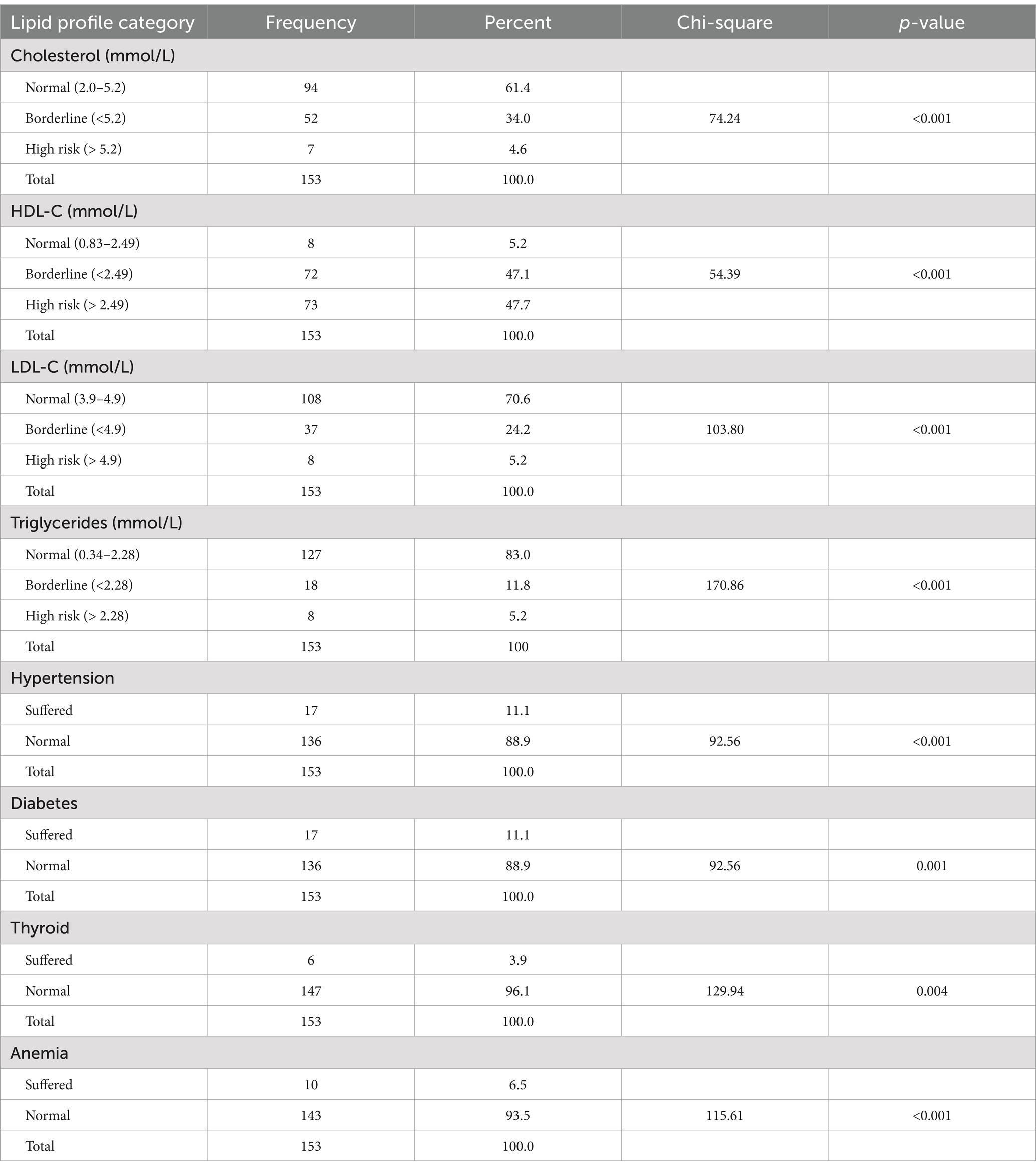
Table 5. Frequency distribution of lipid profiles and health information of participants.
Table 6 highlights some of the associated parameters expected to influence the nutritional state of low-income Saudi females. The data analysis using Spearman correlation coefficient analysis revealed positive or negative correlations between female anthropometric proxies as dependent variables and demographic factors as independent variables. As proxies, females’ nutritional status was assessed using BMI, PBF, VF, WHR, and WHtR. Females’ age was shown to be positively and strongly (p ≤ 0.05 or p ≤ 0.001) related to all anthropometric indices. All anthropometric indicators except PBF are positively and significantly (p ≤ 0.05) linked with participant family size. The participants’ source of income and social welfare benefits were positively and significantly (p ≤ 0.05) linked with BMI, WHR, and WHtR. Females education level was found to be significantly (p ≤ 0.05 or p ≤ 0.001) and inversely related to BMI, VF, WHR, and WHtR. Females’ marital status was found to be positively and significantly (p ≤ 0.05) related to BMI, WHR, and WHtR. On the other hand, females’ occupation was related to all dependent variables, although the relationship was not statistically significant.
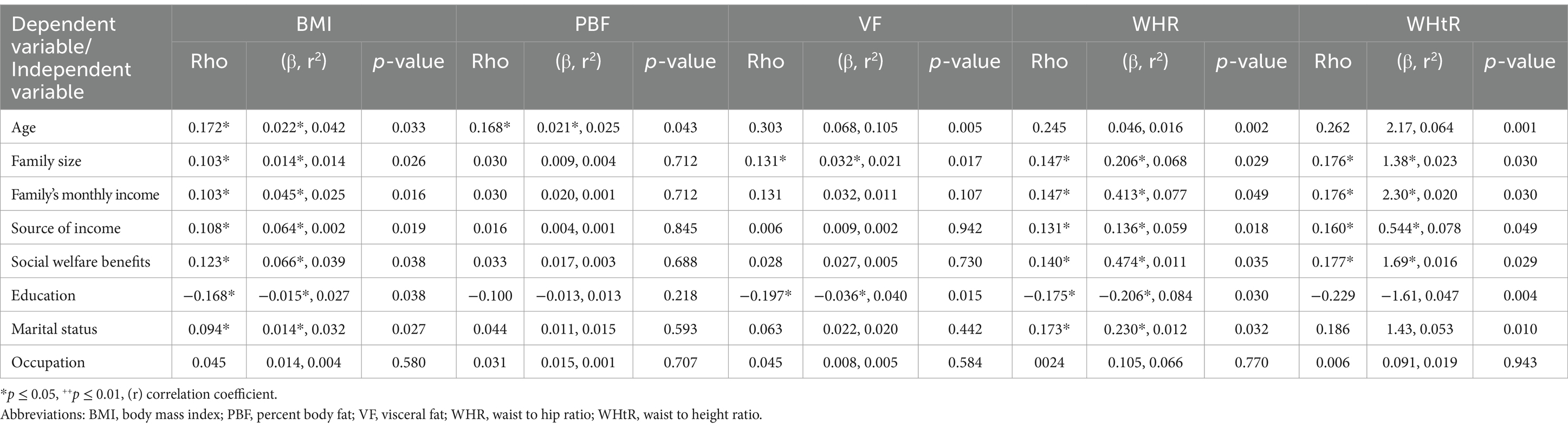
Table 6. Spearman correlation coefficients between sociodemographic factors and anthropometric indices of participants.
In this study, we have explored the nutritional and health status and associated characteristics of low-income Saudi females participating in food assistance programs in Riyadh. According to the data, the frequency distribution of low-income Saudi females based on sociodemographic factors revealed that the rates of participants differed in all categories, as evidenced by the chi-square test. The results showed that the majority of women between the ages of 39 and 48 had more than 5 family members, a reasonable monthly income from either direct labor or donations, or both. The majority of them were also divorced and had poor education (secondary education or lower). These sociodemographic variations might be explained by variations in tribes and living conditions. Bivariate analysis revealed a significant and positive relationship between participants’ dietary diversity scores and women’s sociodemographic traits.
It was found that the proportion of women with lower dietary diversity scores increased significantly with decreased socioeconomic benefits because the majority of the population now obtains food commercially through markets due to a decline in smallholder agriculture, and as a result, most poor communities are at high risk of micronutrient deficiency due to a lack of fruits and vegetables. Furthermore, due to high unemployment, rising food prices, and agricultural abandonment, such participants are unable to consume a more varied diet, leaving them overly dependent on market purchases, resulting in low-nutrient diets that silently contribute to hidden hunger (Otunchieva et al., 2022). According to Jayawardena et al. (2013), dietary diversity is connected with numerous sociodemographic factors and obesity among Sri Lankan adults. Moreover, Olatona et al. (2021) found that healthy dietary habits and a high nutritional diversity score were associated with low parity and a higher socioeconomic status among Nigerian women. A Chinese study also showed that dietary diversity is connected with general and central obesity in adults, excessive energy intake, and the micronutrient deficits of diversified diets. Although dietary diversity is widely advocated, public health communications should emphasize improving moderate and balanced dietary diversity in specific food categories (Zhang et al., 2017).
The findings of this study revealed a low level of nutrient intake compared to DRI, which is consistent with the results of the recent findings of Alageel et al. (2023). Those authors concluded that maintaining a healthy lifestyle is heavily influenced by both social and physical barriers, such as the high cost of maintaining a healthy lifestyle and time constraints. The low-income women’s inadequate nutritional consumption is comparable with previous related studies. In this context, a recent Saudi health survey indicated that only 7% of Saudi women have the recommended fruit and vegetable servings in their diet (Bakhsh et al., 2021). In addition, low-income women are less likely than males to meet the recommended dietary limit for most macronutrients and micronutrients (Ma et al., 2021). In order to explain this, Sawyer et al. (2021) found that a number of socio-ecological factors influence dietary determinants. These factors include resources, household finances, geographic accessibility, and other individual, societal, and cultural influences that interact with the food environment of low-income populations. Furthermore, a study conducted on low-income women in Jeddah City, Saudi Arabia, discovered that participants who are receiving financial and food assistance might struggle to secure a balanced diet, with half of the study sample being food insecure (Hanbazaza and Mumena, 2022). The majority of women who were included in this study live in leased homes or pay housing mortgages and other living expenses, which further limit food affordability. This is in the same line with other previous findings (Fafard St-Germain and Tarasuk, 2020). A systematic review and meta-analysis were conducted to investigate the relationships between anemia risk and food insecurity; the results revealed that particular sub-groups (adult women, infants, and toddlers) in food-insecure households are at a higher risk of anemia (Moradi et al., 2018). Furthermore, being a woman, food insecure, living alone, and other influencing factors were discovered to place women at a higher risk of malnutrition (Ganhão-Arranhado et al., 2018). Another study that examined the relationship between poverty, calcium/vitamin D consumption, and osteoporosis discovered that being poor increased the likelihood of insufficient calcium intake in all participants with a higher risk of inadequacy among both men and women (Marshall et al., 2020).
In terms of anthropometric measurements, the participants’ BMI, PBF, and WHtR were all higher than the normal range in our study population. These results are consistent with previous reports, which showed that low-income women were significantly more likely to have obesity as compared to aged-match males (Ma et al., 2021). According to Park and Strauss (2020), the association between food insecurity and body weight has been extensively studied. However, there is no consensus on this link, and research suggests that food insecurity may be a risk factor for obesity. A systematic review and meta-analysis of 31 studies from 14 different countries revealed a severe level of household food insecurity might be related to the risk of being overweight or obese among adults, with women having a higher risk of obesity than men (Moradi et al., 2018). In contrast, Alazzeh et al. (2018) found that lower-income individuals were less likely to be obese.
Dover and Lambert (2016) reviewed the literature on social determinants of health concerning food security, obesity, and food intake to address the intricacy of decision-making in health behavior. They asserted that there are always restrictions and limited choices regarding food consumption. They attributed this to numerous uncontrollable factors such as food availability, food system equity, and the availability of food and nutrition interventions and policies. Along the same line, Caamaño et al. (2019) investigated the effect of eating valuation and satiation on food insecurity, diet, obesity, and cardiometabolic disease. They emphasized that in developing countries, where energy-dense meals that are low in nutrient content are widely available, there is a desire to prolong satiation due to a fear of feeling hungry. This data underscores the complexities of the food insecurity experience and the significance of designing public health policies that include a deeper knowledge of the reasons, behaviors, and feelings associated with food insecurity. For example, a study discovered that psychological stress modulates the association between neighborhood poverty and increases in central adiposity over time (Kwarteng et al., 2017).
The findings of this study also revealed a significant and positive link between the PBF, VF, WHR, and WHtR categories and women’s minimum dietary diversity. According to the study by Kornatowski and Comstock (2018), women who did not reach the requisite dietary diversity were less likely to consume fruits and vegetables than women who did meet the necessary dietary diversity (Azadbakht and Esmaillzadeh, 2011). They also consumed low nutrient-density items. In contrast to these findings, Azadbakht and Esmaillzadeh (Azadbakht and Esmaillzadeh, 2011) discovered an inverse relationship between dietary diversity score and obesity. In general, dietary diversity is regarded as a problem for women in poor and middle-income countries (Chakona and Shackleton, 2017). However, different approaches to analyzing food patterns yield similar results from different datasets (Liese et al., 2015). The MDD-W score, an established way of assessing dietary consumption at the population level, reduces participant and researcher burden.
According to the current findings, the majority of the participants had normal cholesterol levels, low levels of HDL-C, normal LDL-C, and triglycerides. Interestingly, the majority of them showed no signs of hypertension, diabetes, thyroid problems, or anemia. In addition to obesity-linked poverty, dyslipidemia was found to be relative in this study, with lipid cholesterol being within the healthy range but HDL-C being significantly either at the borderline or high risk. These data correspond with other recent studies that reported a positive association between low income and HDL-C levels in adults and women (Liese et al., 2015). Research on Korean men and women found that the lower-income group had a higher prevalence of low HDL-C levels for both genders (Cho, 2022). In addition, this study revealed that women have a stronger direct link between poverty and low HDL-C levels than men due to a variety of variables, including aging (Cho, 2022). This link could be related to exercise and eating habits, as lower socioeconomic groups are less likely to exercise consistently and more likely to consume fast foods due to financial restrictions. In support, lifestyle has been linked to reduced HDL-C levels and an increased risk of metabolic syndrome (Bahadoran et al., 2013). A thorough review, however, showed no link between food insecurity and dyslipidemia (Arenas et al., 2022).
The significant positive correlation between the independent variables (sociodemographic variables) and the dependent variables (anthropometric indices) of participants indicates that independent factors such as age, family size, monthly income, source of income, social welfare benefits, and marital status are positively correlated with some or all anthropometric characteristics (BMI, PBF, VF, WHR, and WHtR). However, the participants’ education level was inversely correlated with women’s anthropometric characteristics, primarily because the females’ education level was poor. Vajdi and Farhangi (2020) discovered that education is more likely associated with a healthier eating pattern, although age was positively connected with “healthy” dietary patterns. A study found a negative relationship between education and obesity, indicating that the burden of obesity is common among individuals with less education (Sakboonyarat et al., 2020). On the other hand, Mohajeri et al. (2020) discovered an inverse connection between education and general and abdominal obesity in Ardabil–Iran adults. Furthermore, compared to their counterparts, women with a higher level of education are more likely to engage in preventative health behaviors such as regular exercise and having a healthy diet and are less likely to have high parity, which is connected with overweight and obesity (Cooper et al., 2021). However, Otunchieva et al. (2022) showed no statistically significant link between dietary diversity and women’s education, as well as a very slight negative correlation between specific nutrient adequacy ratios and education. They also stated that the results relate to income. This is mostly because educated women are more likely to work and receive better compensation, which may have a negative impact on their diet.
Among other socioeconomic factors, the results of this study revealed a significant and negative relationship between education level and obesity parameters, as reported by Witkam et al. (2021). Salem et al. (2022) found similar results in the relationship between education level and obesity in Saudi women, as well as in both Saudi genders (Mosli et al., 2020) and non-Saudi women (Chung and Lim, 2020). This can be explained by the impact of education on living and working conditions as well as social and community networks, which in turn impact individual lifestyle factors and health. Therefore, the educational level is a significant predictor of socioeconomic position and life chances throughout adulthood (Witkam et al., 2021). Supporting these data, Schvey et al. (2019) studied the association between age and BMI. They discovered that while BMI increases with age until the seventh and eighth decades of life, the average gains are the largest in younger persons. According to Basto-Abreu et al. (2018), BMI increases in adolescence and decreases in the elderly. Moreover, Lawson et al. (2016) discovered that high income increases females’ BMI and other anthropometrics, especially in wealthy countries due to high caloric intake and reduced physical activity. Because the study participants have lower nutrient intake, greater rates of obesity, and lower HDL levels, they are more likely to develop diet-related diseases. In terms of income, for example, a study discovered an elevated risk of sudden cardiac mortality and nonfatal myocardial infarction in low-income cohorts that persisted even after adjusting for smoking and alcohol characteristics (Simoni et al., 2022).
Low-income people may have the motivation and knowledge to improve their lives, but change is hindered by modifiable social factors (Alageel et al., 2023). According to Alageel et al. (2023), women are at higher risk of dietary disparities, which motivates us to address this issue through a holistic intersectionality strategy, which has been applied and demonstrates promising results. Furthermore, a recent study concluded that traditional food security methods might be insufficient to reduce inequities if gender is viewed as a variable rather than a foundation to describe inequities because gendered-centered examination helps identify most underprivileged groups and inform policies to target existing inequities (Kassie et al., 2014). Innovative thinking and implementation approaches would be useful when exploring and treating Saudi women concerning their health.
Because this study used a cross-sectional design, the comparison of nutritional status and related features between high and low-income groups was difficult; thus, cohort studies should be considered in future relevant studies. Another weakness of the study is its small sample size, which was due to its focus on a specific Saudi Arabian region; it was not easy to cover the entire country due to its large size. Self-reported data for sociodemographic characteristics and dietary intake might include an error, which we assume is marginal. A 24-h recall is a standard method for assessing nutritional intake in target populations. However, it has limitations, as it may not accurately reflect a respondent’s regular food intake especially when done for 1 day due to time and fund problems. Additionally, all participants were chosen from a Saudi Arabian organization that helps low-income women by providing them with food assistance. It is also challenging to locate the same number of low-income women who match the same requirements as those located by the organization. The nutritional status measurements in this study were not all-inclusive, but future research might examine additional variables such as blood pressure, blood serum glucose, vitamins, and other important nutrients for this population.
This study found that low-income Saudi females had a variety of sociodemographic, health, and anthropometric features. Despite some of them having minimal nutritional intake, obesity and overweight were common. The vast majority of participants did not acquire MDDS. The participants’ education level was negatively correlated with some or all anthropometric indices, whereas females’ age, family size, and source of income were positively correlated with all or some of these variables.
National initiatives and policies that permit and support healthy living are also required. Saudi Arabia has taken steps toward this goal, such as establishing a food security authority to handle all areas of food security and adopting associated international interventions to reduce health inequities, such as via an all-policies approach. As a result, there is a need to guide and inform these connected policies and government activities and reduce the associated health implications. Further research into this group of Saudi women is required.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by King Saud University, Subcommittee of the Ethics on Human, Ref. No. KSU- 22/0951/IRB. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
KA: Conceptualization, Methodology, Writing – original draft. GA: Conceptualization, Funding acquisition, Methodology, Supervision, Writing – review & editing. KNA: Conceptualization, Supervision, Writing – original draft. KBA: Data curation, Resources, Writing – review & editing. MY: Investigation, Project administration, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This research was funded by the Researchers Supporting Project, King Saud University, Riyadh, Saudi Arabia (grant number RSP2025R84).
The authors extend thanks to the Researchers Supporting Project number (RSP2025R84), King Saud University, Riyadh, Saudi Arabia. Also, the authors extend thanks to the Saudi National Center for Social Studies, Al-Nadah Organization, AlGhowairi Charitable Foundation, and Enayah Organization for their contributions to the success of this work.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Alageel, S., Alhujaili, M., Altwaijri, Y., Bilal, L., and Alsukait, R. (2023). Barriers and facilitators to adopting healthier lifestyle among low-income women in Saudi Arabia: A qualitative study. Health Expect. 26, 1202–1212. doi: 10.1111/hex.13735
Alazzeh, A. Y., AlShammari, E. M., Smadi, M. M., Azzeh, F. S., AlShammari, B. T., Epuru, S., et al. (2018). Some socioeconomic factors and lifestyle habits influencing the prevalence of obesity among adolescent male students in the hail region of Saudi Arabia. Children 5:39. doi: 10.3390/children5030039
Alqunaibet, A., Herbst, C. H., El-Saharty, S., and Algwizani, A. (2021). Noncommunicable diseases in Saudi Arabia: Toward effective interventions for prevention (English). International Development in Focus Washington, DC: The World Bank.
AlZoubi, K. M., Alshammari, G. M., Al-Khalifah, A. S., Mohammed, M. A., Aljuhani, H. E., and Yahya, M. A. (2021). Nutritional status and associated risk factors of Syrian children’s residents in the Kingdom of Saudi Arabia. Children 8:1053. doi: 10.3390/children8111053
Arenas, D. J., Beltrán, S., Pharel, M., Lopez-Hinojosa, I., Vilá-Arroyo, G., and DeLisser, H. M. (2022). A systematic review and Meta-analysis of food insecurity and dyslipidemia. J. Am. Board Family Med. 35, 656–667. doi: 10.3122/jabfm.2022.04.210413
Ashwell, M., Gunn, P., and Gibson, S. (2012). Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: systematic review and meta-analysis. Obes. Rev. 13, 275–286. doi: 10.1111/j.1467-789X.2011.00952.x
Azadbakht, L., and Esmaillzadeh, A. (2011). Dietary diversity score is related to obesity and abdominal adiposity among Iranian female youth. Public Health Nutr. 14, 62–69. doi: 10.1017/S1368980010000522
Bahadoran, Z., Mirmiran, P., Hosseini-Esfahani, F., and Azizi, F. (2013). Fast food consumption and the risk of metabolic syndrome after 3-years of follow-up: Tehran lipid and glucose study. Eur. J. Clin. Nutr. 67, 1303–1309. doi: 10.1038/ejcn.2013.217
Bakhsh, M. A., Khawandanah, J., Naaman, R. K., and Alashmali, S. (2021). The impact of COVID-19 quarantine on dietary habits and physical activity in Saudi Arabia: a cross-sectional study. BMC Public Health 21:1487. doi: 10.1186/s12889-021-11540-y
Basto-Abreu, A., Barrientos-Gutiérrez, T., Zepeda-Tello, R., Camacho, V., Ruiz, G., de Porras, D., et al. (2018). The relationship of socioeconomic status with body mass index depends on the socioeconomic measure used. Obesity 26, 176–184. doi: 10.1002/oby.22042
Botreau, H., and Cohen, M. J. (2020). Gender inequality and food insecurity: A dozen years after the food price crisis, rural women still bear the brunt of poverty and hunger. Adv. Food Sec. Sustain. 5, 53–117. doi: 10.1016/bs.af2s.2020.09.001
Branca, F., Lartey, A., Oenema, S., Aguayo, V., Stordalen, G. A., Richardson, R., et al. (2019). Transforming the food system to fight non-communicable diseases. BMJ 364:l296. doi: 10.1136/bmj.l296
Caamaño, M. C., García, O. P., Parás, P., Palacios, J. R., and Rosado, J. L. (2019). Overvaluation of eating and satiation explains the association of food insecurity and food intake with obesity and cardiometabolic diseases. Food Nutr. Bull. 40, 432–443. doi: 10.1177/0379572119863558
Chakona, G., and Shackleton, C. (2017). Minimum dietary diversity scores for women indicate micronutrient adequacy and food insecurity status in south African towns. Nutrients 9:812. doi: 10.3390/nu9080812
Cho, K.-H. (2022). The current status of research on high-density lipoproteins (HDL): a paradigm shift from HDL quantity to HDL quality and HDL functionality. Int. J. Mol. Sci. 23:3967. doi: 10.3390/ijms23073967
Chung, W., and Lim, S. (2020). Factors contributing to educational differences in obesity among women: evidence from South Korea. BMC Public Health 20:1136. doi: 10.1186/s12889-020-09221-3
Cooper, A. J., Gupta, S. R., Moustafa, A. F., and Chao, A. M. (2021). Sex/gender differences in obesity prevalence, comorbidities, and treatment. Curr. Obes. Rep. 10, 458–466. doi: 10.1007/s13679-021-00453-x
da Silva Miguel, E., Lopes, S. O., Araújo, S. P., Priore, S. E., Alfenas, R., and Hermsdorff, H. H. M. (2020). Association between food insecurity and cardiometabolic risk in adults and the elderly: a systematic review. Journal of. Glob. Health 10:402. doi: 10.7189/jogh.10.020402
Derbal, N. (2022). Charity in Saudi Arabia: Civil society under authoritarianism. Cambridge: Cambridge University Press.
Dover, R. V., and Lambert, E. V. (2016). “Choice set” for health behavior in choice-constrained settings to frame research and inform policy: examples of food consumption, obesity and food security. Int. J. Equity Health 15:48. doi: 10.1186/s12939-016-0336-6
Eskandari, F., Lake, A. A., Rose, K., Butler, M., and O'Malley, C. (2022). A mixed-method systematic review and meta-analysis of the influences of food environments and food insecurity on obesity in high-income countries. Food Sci. Nutr. 10, 3689–3723. doi: 10.1002/fsn3.2969
Fadaak, T. (2010). Poverty in the kingdom of Saudi Arabia: an exploratory study of poverty and female-headed households in Jeddah city. Soc. Policy Adm. 44, 689–707. doi: 10.1111/j.1467-9515.2010.00738.x
Fafard St-Germain, A.-A., and Tarasuk, V. (2020). Homeownership status and risk of food insecurity: examining the role of housing debt, housing expenditure and housing asset using a cross-sectional population-based survey of Canadian households. Int. J. Equity Health 19, 5–12. doi: 10.1186/s12939-019-1114-z
Faul, F., Erdfelder, E., Lang, A.-G., and Buchner, A. (2007). G* power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 39, 175–191. doi: 10.3758/BF03193146
Fitzpatrick, K. M., Harris, C., Drawve, G., and Willis, D. E. (2021). Assessing food insecurity among US adults during the COVID-19 pandemic. J. Hunger Environ. Nutr. 16, 1–18. doi: 10.1080/19320248.2020.1830221
Ganhão-Arranhado, S., Paúl, C., Ramalho, R., and Pereira, P. (2018). Food insecurity, weight and nutritional status among older adults attending senior centres in Lisbon. Arch. Gerontol. Geriatr. 78, 81–88. doi: 10.1016/j.archger.2018.06.004
Gosadi, I. M. (2019). National screening programs in Saudi Arabia: overview, outcomes, and effectiveness. J. Infect. Public Health 12, 608–614. doi: 10.1016/j.jiph.2019.06.001
Gurewich, D., Garg, A., and Kressin, N. R. (2020). Addressing social determinants of health within healthcare delivery systems: a framework to ground and inform health outcomes. J. Gen. Intern. Med. 35, 1571–1575. doi: 10.1007/s11606-020-05720-6
Hamedi-Shahraki, S., Mir, F., and Amirkhizi, F. (2021). Food insecurity and cardiovascular risk factors among Iranian women. Ecol. Food Nutr. 60, 163–181. doi: 10.1080/03670244.2020.1812596
Hanawi, M. K., and Keetile, M. (2021). Socio-economic and demographic correlates of non-communicable disease risk factors among adults in Saudi Arabia. Front. Med. 8:605912. doi: 10.3389/fmed.2021.605912
Hanbazaza, M. A., and Mumena, W. A. (2022). Food security status, coping strategies, and health of women’s welfare society beneficiaries in Jeddah, Saudi Arabia: a facility-based study. Ecol. Food Nutr. 61, 43–55. doi: 10.1080/03670244.2021.1926244
Hazazi, A., and Wilson, A. (2022). Noncommunicable diseases and health system responses in Saudi Arabia: focus on policies and strategies. A qualitative study. Health Res. Policy Syst. 20:63. doi: 10.1186/s12961-022-00872-9
Hill-Briggs, F., Adler, N. E., Berkowitz, S. A., Chin, M. H., Gary-Webb, T. L., Navas-Acien, A., et al. (2021). Social determinants of health and diabetes: a scientific review. Diabetes Care 44, 258–279. doi: 10.2337/dci20-0053
Jayawardena, R., Byrne, N. M., Soares, M. J., Katulanda, P., Yadav, B., and Hills, A. P. (2013). High dietary diversity is associated with obesity in Sri Lankan adults: an evaluation of three dietary scores. BMC Public Health 13, 1–8. doi: 10.1186/1471-2458-13-314
Kaiser, M. L., Dionne, J., and Carr, J. K. (2019). Predictors of diet-related health outcomes in food-secure and food-insecure communities. Soc. Work Public Health 34, 214–229. doi: 10.1080/19371918.2019.1575313
Kassie, M., Ndiritu, S. W., and Stage, J. (2014). What determines gender inequality in household food security in Kenya? Application of exogenous switching treatment regression. World Dev. 56, 153–171. doi: 10.1016/j.worlddev.2013.10.025
Kennedy, G., Ballard, T., and Dop, M. (2011). Guidelines for measuring household and individual dietary diversity. Food and Agriculture Organization of the United Nations, Rome.
Kornatowski, B. M., and Comstock, S. S. (2018). Dietary diversity is inversely correlated with pre-pregnancy body mass index among women in a Michigan pregnancy cohort. PeerJ 6:e5526. doi: 10.7717/peerj.5526
Kwarteng, J. L., Schulz, A. J., Mentz, G. B., Israel, B. A., and Perkins, D. W. (2017). Independent effects of neighborhood poverty and psychosocial stress on obesity over time. J. Urban Health 94, 791–802. doi: 10.1007/s11524-017-0193-7
Lawson, R. A., Murphy, R. H., and Williamson, C. R. (2016). The relationship between income, economic freedom, and BMI. Public Health 134, 18–25. doi: 10.1016/j.puhe.2016.01.020
Liese, A. D., Krebs-Smith, S. M., Subar, A. F., George, S. M., Harmon, B. E., Neuhouser, M. L., et al. (2015). The dietary patterns methods project: synthesis of findings across cohorts and relevance to dietary guidance. J. Nutr. 145, 393–402. doi: 10.3945/jn.114.205336
Ma, C., Ho, S. K., Singh, S., and Choi, M. Y. (2021). Gender disparities in food security, dietary intake, and nutritional health in the United States. Offic. J. Am. Coll. Gastroenterol. 116, 584–592. doi: 10.14309/ajg.0000000000001118
Marshall, K., Teo, L., Shanahan, C., Legette, L., and Mitmesser, S. H. (2020). Inadequate calcium and vitamin D intake and osteoporosis risk in older Americans living in poverty with food insecurities. PLoS One 15:e0235042. doi: 10.1371/journal.pone.0235042
Meyers, L. D., Hellwig, J. P., and Otten, J. J. (2006). Dietary reference intakes: The essential guide to nutrient requirements : National Academies Press.
Mohajeri, M., Houjeghani, S., Ghahremanzadeh, M., Borghei, M. H., Moradi, F., and Barzegar, A. (2020). Some behavioral risk factors of obesity in Ardabil–Iran adults. Obesity Med. 18:100167:100167. doi: 10.1016/j.obmed.2019.100167
Moradi, S., Arghavani, H., Issah, A., Mohammadi, H., and Mirzaei, K. (2018). Food insecurity and anaemia risk: a systematic review and meta-analysis. Public Health Nutr. 21, 3067–3079. doi: 10.1017/S1368980018001775
Moradi-Lakeh, M., El Bcheraoui, C., Afshin, A., Daoud, F., AlMazroa, M. A., Al, S. M., et al. (2017). Diet in Saudi Arabia: findings from a nationally representative survey. Public Health Nutr. 20, 1075–1081. doi: 10.1017/S1368980016003141
Mosli, H. H., Kutbi, H. A., Alhasan, A. H., and Mosli, R. H. (2020). Understanding the interrelationship between education, income, and obesity among adults in Saudi Arabia. Obes. Facts 13, 77–85. doi: 10.1159/000505246
Olatona, F. A., Olowu, O. J., Goodman, O. O., and Amu, E. O. (2021). Dietary habits, diversity, and predictors among pregnant women attending primary health care centers for antenatal care in Lagos, Nigeria. J. Family Med. Prim. Care 10, 3076–3083. doi: 10.4103/jfmpc.jfmpc_397_21
Otunchieva, A., Smanalieva, J., and Ploeger, A. (2022). Dietary quality of women of reproductive age in low-income settings: a cross-sectional study in Kyrgyzstan. Nutrients 14:289. doi: 10.3390/nu14020289
Park, S. H., and Strauss, S. M. (2020). Food insecurity as a predictor of metabolic syndrome in US female adults. Public Health Nurs. 37, 663–670. doi: 10.1111/phn.12781
Perez-Escamilla, R., Bermudez, O., Buccini, G. S., Kumanyika, S., Lutter, C. K., Monsivais, P., et al. (2018). Nutrition disparities and the global burden of malnutrition. BMJ 361:k2252. doi: 10.1136/bmj.k2252
Ryckman, T., Beal, T., Nordhagen, S., Chimanya, K., and Matji, J. (2021). Affordability of nutritious foods for complementary feeding in eastern and southern Africa. Nutr. Rev. 79, 35–51. doi: 10.1093/nutrit/nuaa137
Sakboonyarat, B., Pornpongsawad, C., Sangkool, T., Phanmanas, C., Kesonphaet, N., Tangthongtawi, N., et al. (2020). Trends, prevalence and associated factors of obesity among adults in a rural community in Thailand: serial cross-sectional surveys, 2012 and 2018. BMC Public Health 20, 850–859. doi: 10.1186/s12889-020-09004-w
Salem, V., AlHusseini, N., Abdul, R. H., Naoum, A., Sims, O. T., and Alqahtani, S. A. (2022). Prevalence, risk factors, and interventions for obesity in Saudi Arabia: A systematic review. Obes. Rev. 23:e13448. doi: 10.1111/obr.13448
Sawyer, A. D., van Lenthe, F., Kamphuis, C. B., Terragni, L., Roos, G., Poelman, M. P., et al. (2021). Dynamics of the complex food environment underlying dietary intake in low-income groups: a systems map of associations extracted from a systematic umbrella literature review. Int. J. Behav. Nutr. Phys. Act. 18, 96–21. doi: 10.1186/s12966-021-01164-1
Schvey, N. A., Marwitz, S. E., Mi, S. J., Galescu, O. A., Broadney, M. M., Young-Hyman, D., et al. (2019). Weight-based teasing is associated with gain in BMI and fat mass among children and adolescents at-risk for obesity: a longitudinal study. Pediatr. Obes. 14:e12538. doi: 10.1111/ijpo.12538
Scott, P. (2017). Global panel on agriculture and food systems for nutrition: food systems and diets: facing the challenges of the 21st century. London, UK: Springer.
Simoni, A. H., Frydenlund, J., Kragholm, K. H., Bøggild, H., Jensen, S. E., and Johnsen, S. P. (2022). Socioeconomic inequity in incidence, outcomes and care for acute coronary syndrome: a systematic review. Int. J. Cardiol. 356, 19–29. doi: 10.1016/j.ijcard.2022.03.053
Vajdi, M., and Farhangi, M. A. (2020). A systematic review of the association between dietary patterns and health-related quality of life. Health Qual. Life Outcomes 18, 337–315. doi: 10.1186/s12955-020-01581-z
Verghese, A., Raber, M., and Sharma, S. (2019). Interventions targeting diet quality of supplemental nutrition assistance program (SNAP) participants: A scoping review. Prev. Med. 119, 77–86. doi: 10.1016/j.ypmed.2018.12.006
Vilar-Compte, M., Burrola-Méndez, S., Lozano-Marrufo, A., Ferré-Eguiluz, I., Flores, D., Gaitán-Rossi, P., et al. (2021). Urban poverty and nutrition challenges associated with accessibility to a healthy diet: a global systematic literature review. Int. J. Equity Health 20, 40–19. doi: 10.1186/s12939-020-01330-0
Wen, L. M., Flood, V. M., Simpson, J. M., Rissel, C., and Baur, L. A. (2010). Dietary behaviours during pregnancy: findings from first-time mothers in Southwest Sydney, Australia. Int. J. Behav. Nutr. Phys. Act. 7, 13–17. doi: 10.1186/1479-5868-7-13
WHO (2000). Obesity: Preventing and managing the global epidemic: Report of a WHO consultation. Geneva: WHO.
Witkam, R., Gwinnutt, J. M., Humphreys, J., Gandrup, J., Cooper, R., and Verstappen, S. M. (2021). Do associations between education and obesity vary depending on the measure of obesity used? A systematic literature review and meta-analysis. SSM Popul. Health 15:100884. doi: 10.1016/j.ssmph.2021.100884
Keywords: low-income women, nutritional status, questionnaire, malnutrition, sociodemographic
Citation: Alrougui K, Alshammari GM, Alrwis KN, Alabdulkarem KB and Yahya MA (2025) Nutritional status and associated socioeconomic factors among low-income Saudi females. Front. Sustain. Food Syst. 9:1510426. doi: 10.3389/fsufs.2025.1510426
Edited by:
Elliot Berry, Hebrew University of Jerusalem, IsraelReviewed by:
Predner Duvivier, University of Haiti, HaitiCopyright © 2025 Alrougui, Alshammari, Alrwis, Alabdulkarem and Yahya. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ghedeir M. Alshammari, YWdoZWRlaXJAa3N1LmVkdS5zYQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.