 Nanine Wyma
Nanine Wyma Christi Niesing
Christi Niesing- Africa Unit for Transdisciplinary Health Research, North-West University, Potchefstroom, South Africa
The reduction of meat consumption in health systems is a high-impact pathway for healthcare decarbonization. Effects including changes in greenhouse gas emissions are rarely calculated following interventions, such as the implementation of plant-forward menus in hospitals, and the results of these changes are rarely published in peer-reviewed literature. In this perspective, we discuss the decarbonization outcomes of plant-rich dietary shifts across five health systems worldwide, gathered from peer-reviewed and gray literature. In each case, the implementation of a plant-rich approach reduced food-related greenhouse gas emissions. Health co-benefits are also commonly reported. The measurement of greenhouse gas emissions of plant-rich dietary shifts in future health system interventions is encouraged, with the results published in peer-reviewed journals.
1 Introduction
The need for health systems to reduce their carbon footprint is becoming increasingly urgent. Following the United Nations Framework Convention on Climate Change (UNFCCC) Conference of Parties (COP) 26 Health Programme, the World Health Organization (WHO) established the Alliance for Transformative Action for Climate and Health (ATACH) to support a transition toward climate-resilient and low-carbon health systems. As of 2024, ATACH has gathered low-carbon commitments from 75 countries and net-zero commitments from 36 [World Health Organization (WHO), 2024].
The baseline climate impact of healthcare was calculated at 4.4% of global greenhouse gas (GHG) emissions in 2014, measured in carbon dioxide equivalent (CO2e) (Health Care Without Harm and Arup, 2019). The great majority of healthcare’s GHG emissions, over 70%, originate from the supply chain, known as “Scope 3” emissions. Food, catering, and accommodation are a supply chain category that make up 7.2% of total healthcare GHG emissions (Health Care Without Harm and Arup, 2021a).
The Global Road Map for Health Care Decarbonization (Health Care Without Harm and Arup, 2021a) identified seven high-impact actions for emissions reduction. Providing healthy and sustainable food from climate-resilient agriculture is the fourth high-impact action, projecting a cumulative emissions savings of 0.9 Gt CO2e by 2050 (Health Care Without Harm and Arup, 2021a). A key component of this action is reducing the amount of meat served and creating plant-forward menus (Health Care Without Harm and Arup, 2021b). A plant-forward recommendation is echoed in a scoping review of sustainable food system procurement strategies in health systems (Alberdi and Begiristain-Zubillaga, 2021) and a systematic review of sustainable hospital food services across the supply chain, which found meatless meals to have the lowest carbon footprint (Carino et al., 2020).
Plant-rich dietary shifts are crucial to climate change mitigation. The Intergovernmental Panel on Climate Change (IPCC) (2019) estimates the GHG mitigation potential of healthy dietary shifts at 2.7–6.4 Gt CO2eq yr.−1 by 2050. They further explain that the carbon emissions of dietary composition are primarily driven by the amount of livestock and associated products consumed. A range of sustainable dietary scenarios and their technical GHG mitigation potential is calculated by the Intergovernmental Panel on Climate Change (IPCC) (2019), demonstrating a step-wise increase in technical GHG mitigation potential when removing animal products from the diet, with vegan diets offering the greatest technical GHG mitigation potential.
Prioritizing health co-benefits is important for all mitigation pathways, especially in healthcare. Major public health benefits of plant-forward dietary patterns include protection against chronic non-communicable diseases (NCDs), the world’s leading cause of death and the target of Sustainable Development Goal 3.4 (Bennet et al., 2020). The Lancet Countdown on health and climate (Romanello et al., 2023) monitors dietary and health co-benefits as indicator 3.3.2 and states that balanced, low-emission diets can address 12.2 million deaths, of which 7.8 million are attributable to insufficient plant-based food consumption and 1.9 million to overconsumption of dairy produce and red and processed meats.
Studies support the idea that healthy, climate-friendly dietary patterns are plant-forward. Storz (2020) questioned whether plant-based meals should be the law in hospitals, with several hospitals across the United States of America (USA) having mandated the availability of meat-free meals. Despite an appetite for change, literature on the decarbonization potential of plant-rich dietary shifts in health systems remains limited. It is important to examine the health system context as unique from other large-scale kitchens, whereby health systems are positioned as beacons of health for communities. This article provides a perspective on decarbonizing healthcare using plant-rich dietary shifts.
2 Methods
The perspective includes a subset of literature gathered for a master’s dissertation at North-West University, South Africa, titled Plant-based food interventions in hospitals and their co-benefits: A scoping review. Scoping reviews typically map literature on emerging concepts where little is known (Arksey and O’Malley, 2007). The aim of the dissertation was to capture a broad overview and explore transdisciplinarity through the health, environmental, and economic co-benefits of plant-based food interventions in the context of hospitals. Consistent with scoping review methodologies, such as outlined by the JBI Institute (Peters et al., 2015), peer-reviewed and gray literature was included in the search strategy with reiterations of the keywords “plant-based” or “vegetarian” or “vegan” and “food” and “hospital” across databases, search engines, key websites, and professional networks. The protocol was approved by the North-West University Ethics Review Board (NWU-00019-23-A1) in 2023 and is further discussed in the Supplementary material.
The literature subset includes only those that measured GHG emissions as outcomes of interventions. The scoping review included 83 sources, of which only five sources (one peer-reviewed article, two blog posts, one project report, and one report) measured GHG emissions. The rationale for presenting this perspective is to illuminate cases of plant-rich dietary shifts mitigating GHG emissions in health systems that exist outside of peer-reviewed literature. These cases would be excluded from systematic reviews and may be pivotal in advancing the understanding and further investigation of healthcare decarbonization.
3 Findings
The decarbonization outcomes of plant-rich dietary shifts of five health systems were reported across Austria (n = 1), the USA (n = 3), and Taiwan (n = 1), mapped in Table 1. The types of interventions and their impact on food-related GHG emissions are discussed in this section.
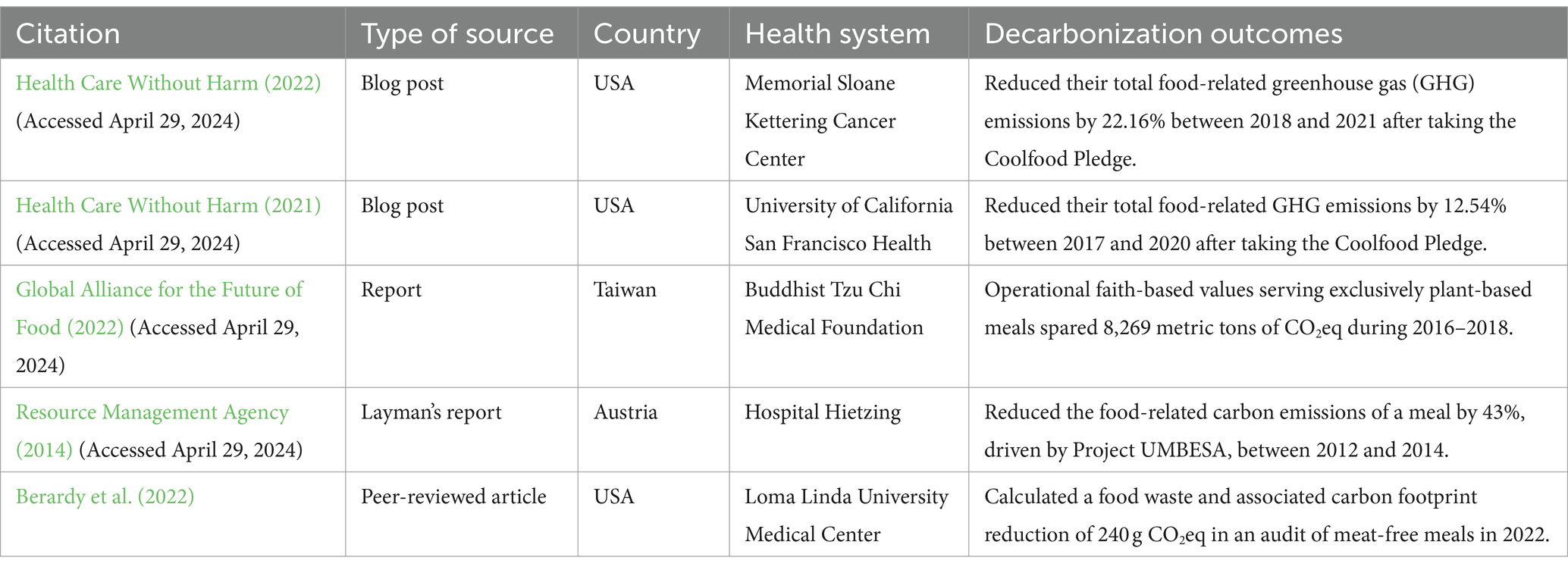
Table 1. Overview of data demonstrating decarbonization outcomes of plant-based dietary shifts in health systems.
3.1 Health systems take the Coolfood Pledge
The aim of the Coolfood Pledge is to reduce food-related GHG emissions by 25% by 2030 from a 2015 baseline. According to their 2022 Progress Report (World Resource Institute, 2022), the Coolfood Pledge has members in several settings, including 26 identified healthcare members. Health Care Without Harm (2022) reported that 97% of the Coolfood Pledge healthcare cohort had reduced their food-related GHG emissions, collectively reducing per-plate emissions by 13.09%.
In blog posts, Health Care Without Harm (2021, 2022) details the progress of the Coolfood Pledge in selected US health systems. Memorial Sloane Kettering Cancer Center, a health system based in New York City, United States, applied a plant-forward philosophy to its menu and reduced total food-related GHG emissions by 22.16% over four years (2018–2021) (Health Care Without Harm, 2022). A key component of their menu included serving plant-based alternatives to traditional dishes, such as swapping a “BLT” sandwich, containing bacon, lettuce and tomato, with a mushroom-based “MLT” (Health Care Without Harm, 2022).
Similarly, another Coolfood Pledge member, University of California San Francisco Health, measured a 12.54% reduction in total food-related emissions over 4 years (2017–2020) (Health Care Without Harm, 2021). Annually, this environmental impact is equivalent to taking 455 cars off the road. Strategies driving this outcome at the University of California San Francisco Health included launching a new plant-based menu concept, reducing the number of beef dishes offered, and replacing beef burgers with a 70/30 mushroom “blended” burger (Health Care Without Harm, 2021).
3.2 Buddhist Tzu Chi Medical Foundation exclusively serves plant-based meals
The Buddhist Tzu Chi Medical Foundation (Tzu Chi) in Taiwan operates based on faith-based principles of health, environmental stewardship and compassion (Global Alliance for the Future of Food, 2022). Tzu Chi exclusively serves plant-based vegetarian options with organic local produce in their medical facilities. As leaders of food systems transformation in health systems, Tzu Chi has also published a number of peer-reviewed population-based studies examining the health benefits of plant-based dietary patterns in Taiwan. According to their calculations, between 2016 and 2018 Tzu Chi “prevented 8,269 metric tons of CO2eq from entering the atmosphere” because they served meat-free meals across seven medical facilities (Global Alliance for the Future of Food, 2022).
3.3 Project UMBESA promotes sustainable food in large-scale European kitchens
Project UMBESA was a European initiative between 2012 and 2014, enabling transitions to sustainable menus in several contexts, such as schools, prisons, corporate environments, and a single hospital. Evaluation of the overall project was based on multidimensional components of sustainability, including economic, health, ecological, and societal impacts. It was reported that from 40 optimized meals, an 88% reduction in CO2 emissions is possible, primarily from the reduction of meat portions. Interestingly, the UMBESA project report (Resource Management Agency, 2014) showed that swapping a convenient vegetable schnitzel for a freshly prepared vegetable patty cut the cost of the meal in half (−51%).
The Hospital Hietzing, Neurological Center Rosenhügel in Austria, participated in Project UMBESA and reportedly reduced a meal’s carbon footprint by 43% when swapping a potato-cured meat casserole with a vegetarian moussaka (Resource Management Agency, 2014).
3.4 An audit of plant-based meals in a US hospital
At Loma Linda University Medical Center in the USA, all patients are served a lacto-ovo-vegetarian meal by default upon admission (Berardy et al., 2022). After 24 h, patients have the option to choose standard menu options that include meat. To examine food waste and GHG emissions, Berardy et al. (2022) performed a plate waste audit of vegetarian and meat-based meals across seven consecutive days. They found that the total food waste and associated GHG emissions were lower for vegetarian meals. Total GHG emissions of meat-based meals were significantly greater (604.20 ± 643.45 g CO2eq) than vegetarian meals (356.66 ± 376.98 g CO2eq).
4 Discussion
We present cases of plant-rich dietary shifts across five health systems, each of which successfully reduced food-related GHG emissions. This supports the implementation of plant-forward menus as a high-impact intervention pathway for healthcare decarbonization. An added strength to the study is the sociocultural diversity of approaches spanning three continents, reflecting aspects of US, European, and Taiwanese cultures and cross-continental beliefs of health, environmentalism, and compassion. Inclusivity of local culture, knowledge, and consumption patterns is a component of sustainable, healthy dietary shifts [World Health Organization (WHO) and Food and Agriculture Organization (FAO), 2019].
Data on the decarbonization potential of plant-rich dietary shifts in health systems remain limited. Including gray literature in the review, such as project reports and blog posts, advances understanding of the concept and allows the sharing of evidence that would be omitted from systematic reviews. However, the decarbonization outcomes found in gray literature are less reliable, with insufficient information provided on calculation methods. The reporting methods also differ, creating uncertainties and limiting the comparability of outcomes.
The methods and processes used to evaluate decarbonization outcomes, as mean total GHG emissions (g CO2eq), at Loma Linda University Medical Center are described by Berardy et al. (2022). These involved collecting data from meals and using life-cycle assessment software. Methods used for calculations must be clearly reported in future publications, as these may differ by context and resources available. There is an opportunity to access standardized longitudinal data on GHG emissions from the Coolfood Pledge healthcare cohort. A systematic review of such data would provide valuable insight for health systems worldwide.
Faith-based cohorts also provide valuable opportunities to explore the health co-benefits of plant-forward dietary patterns. Tzu Chi conducted a number of observational studies on traditionally plant-forward Buddhist populations (including the Tzu Chi Vegetarian Study cohort), and their publications support that Taiwanese vegetarian diets are protective against NCDs such as diabetes (Chiu et al., 2018), depression (Shen et al., 2021), cardiovascular disease (Chiu et al., 2020), and dementia (Tsai et al., 2022) while also reducing medical expenditure (Lin et al., 2019). Another case of faith-based values shaping plant-based dietary choices can be found among Seventh-Day Adventists, who similarly abstain from meat products, based on compassion. The Adventist Health Study (Orlich and Fraser, 2014) is well-known for demonstrating the NCD protective benefits of plant-based dietary patterns among a large cohort of about 90,000 members. There are over 100 hospitals associated with the Adventist health system worldwide serving plant-rich foods (Banta et al., 2018). Interestingly, the headquarters of the International Adventist Health System is in Loma Linda, where the audit of hospital meals took place (see 3.4).
While GHG emissions are an important indicator of climate impact, the cases described in this perspective integrate several other aspects of sustainable healthy diets. Future interventions should be guided by the 16 principles of sustainable healthy diets of the World Health Organization (WHO) and Food and Agriculture Organization (FAO) (2019), to maximize co-benefits and avoid unintended consequences. These principles state that healthy diets include abundant plant-based foods and only small amounts of meat. In addition to GHG emissions, the environmental impacts of water and land use, biodiversity loss, and food waste must be factored in. Sociocultural aspects must also be protected and maintained by enforcing accessible and desirable dietary patterns built on local culture, knowledge, and consumption patterns.
5 Conclusion
Plant-rich dietary shifts are a high-impact pathway for healthcare decarbonization. There is limited peer-reviewed literature on practical cases of plant-forward interventions and their GHG outcomes in the context of health systems. This article presents diverse cases from five health systems across the globe, in which each case successfully reduces food-related GHG emissions as a result of a plant-rich dietary shift. Decarbonization outcomes emerging from gray literature, such as project reports, are limited in terms of reliability and comparability. The further measurement of GHG emissions from plant-forward interventions in health systems is encouraged, with the results published in peer-reviewed journals.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: the dataset may be available in the Institutional Repository of the North-West University (NWU-IR) after 2026. Requests to access these datasets should be directed to Nanine Wyma, bmFuaW5lLnd5bWFAcGFuLXNhLm9yZw==.
Ethics statement
Written informed consent was not obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article because the data was sourced from public information.
Author contributions
NW: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Visualization, Writing – original draft, Writing – review & editing. CN: Conceptualization, Funding acquisition, Resources, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The Physicians Association for Nutrition South Africa provided funding for the language editing of this manuscript. North-West University funded the article processing charges of this manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fsufs.2024.1432103/full#supplementary-material
References
Alberdi, G., and Begiristain-Zubillaga, M. (2021). Identifying a sustainable food procurement strategy in healthcare systems: a scoping review. Sustain. For. 13:2398. doi: 10.3390/su13042398
Arksey, H., and O’Malley, L. (2007). Scoping studies: towards a methodological framework. Int. J. Soc. Res. Methodol. 8, 19–32. doi: 10.1080/1364557032000119616
Banta, J. E., Lee, J. W., Hodgkin, G., Yi, Z., Fanica, A., and Sabate, J. (2018). The global influence of the seventh-day Adventist church on diet. Religions 9:251. doi: 10.3390/rel9090251
Bennet, J. E., Kontis, V., Mathers, C. D., Guillot, M., Rehm, J., Chalkidou, K., et al. (2020). NCD countdown 2030: pathways to achieving sustainable development goal target 3.4. Lancet 396, 918–934. doi: 10.1016/S0140-6736(20)31761-X
Berardy, A., Egan, B., Birckfield, N., Sabaté, J., and Lynch, H. (2022). Comparison of plate waste between vegetarian and meat-containing meals in a hospital setting: environmental and nutritional considerations. Nutrients 14:1174. doi: 10.3390/nu14061174
Carino, S., Porter, J., Malekpour, S., and Collins, J. (2020). Environmental sustainability of hospital food services across the food supply chain. J. Acad. Nutr. Diet. 120, 825–873. doi: 10.1016/j.jand.2020.01.001
Chiu, T. H. T., Change, H. R., Wang, L. Y., Chang, C. C., Lin, M. N., and Lin, C. L. (2020). Vegetarian diet and incidence of total, ischemic, and hemorrhagic stroke in 2 cohorts in Taiwan. Neurology. 94 (11), e 1121 94, e1112–e1121. doi: 10.1212/WNL.0000000000009093
Chiu, T. H. T., Pan, W. H., Lin, M. N., and Lin, M. N. (2018). Vegetarian diet, change in dietary patterns, and diabetes risk: a prospective study. Nutr. Diabetes 8:12. doi: 10.1038/s41387-018-0022-4
Global Alliance for the Future of Food. (2022). Creating better health for people, animals, and the planet: Food systems insights for health professionals. Available at: https://futureoffood.org/insights/creating-better-health/ (Accessed April 29, 2024).
Health Care Without Harm. (2021). How one health system increased plant-forward options and saw its climate impact drop. Available at: https://noharm.medium.com/how-one-health-system-increased-plant-forward-options-and-saw-its-climate-impact-drop-6c7d771f2958 (Accessed April 29, 2024).
Health Care Without Harm. (2022). Cool food participants serve up solutions, chopping dishes’ GHG emissions. Available at: https://noharm.medium.com/cool-food-participants-serve-up-solutions-chopping-dishes-ghg-emissions-66dd138ee1ec (Accessed April 29, 2024).
Health Care Without Harm and Arup. (2019). Healthcare’s climate footprint: How the health sector contributes to the global climate crisis and opportunities for action. Health Care Without Harm Climate-Smart Health Care Green Paper Number One. Available at: https://noharm-global.org/sites/default/files/documents-files/5961/HealthCaresClimateFootprint_092319.pdf (Accessed April 29, 2024).
Health Care Without Harm and Arup. (2021a). Global roadmap for health care Decarbonization: A navigational tool for achieving zero emissions with climate resilience and health equity. Health Care Without Harm Climate-Smart Health Care Green Paper Number Two. Available at: https://healthcareclimateaction.org/sites/default/files/2021-08/Global%20Road%20Map%20for%20Health%20Care%20Decarbonization.pdf (Accessed April 29, 2024).
Health Care Without Harm and Arup. (2021b). Global road map for health care Decarbonization. Annex C: Recommended interventions for implementing the seven high-impact actions. Available at: https://healthcareclimateaction.org/sites/default/files/2021-06/Health%20Care%20Without%20Harm%20Road%20Map%20for%20Health%20Care%20Decarbonization%20Annex%20C_final.pdf (Accessed April 29, 2024).
Intergovernmental Panel on Climate Change (IPCC). (2019). Food security: Special report on climate Change and land. Available at: https://www.ipcc.ch/srccl/chapter/chapter-5/ (Accessed April 29, 2024).
Lin, C. L., Wang, J. H., Chang, C. C., Chiu, T. H. T., and Lin, M. N. (2019). Vegetarian diets and medical expenditure in Taiwan—a matched cohort study. Nutrients 11:2688. doi: 10.3390/nu11112688
Orlich, M. J., and Fraser, G. E. (2014). Vegetarian diets in the Adventist health study 2: a review of initial published findings. Am. J. Clin. Nutr. 100, 353S–358S. doi: 10.3945/ajcn.113.071233
Peters, M. D. J., Godfrey, C. M., McInerney, P., Khalil, H., Parker, D., and Soares, C. B. (2015). Guidance for conducting systematic scoping reviews. Int. J. Evd. Based Healthc. 13, 141–146. doi: 10.1097/XEB.0000000000000050
Resource Management Agency. (2014). Layman’s report: UMBESA. Available at: http://umbesa.rma.at/sites/new.rma.at/files/Projekt%20UMBESA%20-%20Layman´s%20report%20(Vers%201.0)_2.pdf (Accessed April 29, 2024).
Romanello, M., di Napoli, C., Green, C., Kennard, H., Lampard, P., and Scamman, D. (2023). The 2023 report of the lancet countdown on health and climate change: the imperative for a health-centred response in a world facing irreversible harms. Lancet 402, 2346–2394. doi: 10.1016/S0140-6736(23)01859-7
Shen, Y. C., Change, C. E., Lin, M. N., and Lin, C. L. (2021). Vegetarian diet is associated with lower risk of depression in Taiwan. Nutrients 13:1056. doi: 10.3390/nu13041059
Storz, M. A. (2020). Should plant-based hospital meals be the law? An American experience. Hosp. Prac. 48, 241–243. doi: 10.1080/21548331.2020.1807756
Tsai, J. H., Huang, C. F., Lin, M. N., Chang, C. E., Chang, C. C., and Lin, C. L. (2022). Taiwanese vegetarians are associated with lower dementia risk: a prospective cohort study. Nutrients 14:588. doi: 10.3390/nu14030588
World Health Organization (WHO). (2024). Alliance for transformative action on climate and health (ATACH). Available at: https://www.who.int/initiatives/alliance-for-transformative-action-on-climate-and-health (Accessed April 29, 2024).
World Health Organization (WHO) and Food and Agriculture Organization (FAO). (2019). Sustainable healthy diets: Guiding principles. Available at: https://www.who.int/publications/i/item/9789241516648 (Accessed April 29, 2024).
World Resource Institute. (2022). Cool food Progress report 2022. Available at: https://issuu.com/wricoolfood/docs/22_psh_0049_impact_report_issuu1 (Accessed April 29, 2024).
Keywords: healthcare decarbonization, plant-based diets, health promotion, transdisciplinarity, sustainable diets
Citation: Wyma N and Niesing C (2024) Perspectives on healthcare decarbonization through plant-rich dietary shifts: cases from the US, Austria and Taiwan. Front. Sustain. Food Syst. 8:1432103. doi: 10.3389/fsufs.2024.1432103
Edited by:
Travis Idol, University of Hawaii, United StatesReviewed by:
Gidon Eshel, Bard College, United StatesCopyright © 2024 Wyma and Niesing. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence:Nanine Wyma, bmFuaW5lLnd5bWFAcGFuLXNhLm9yZw==