 Ohoud Mohamad
Ohoud Mohamad Haleama Al Sabbah
Haleama Al Sabbah Linda Smail
Linda Smail Ehab W. Hermena
Ehab W. Hermena Rola Al Ghali1
Rola Al Ghali1
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Sustain. Food Syst., 18 March 2022
Sec. Nutrition and Sustainable Diets
Volume 6 - 2022 | https://doi.org/10.3389/fsufs.2022.792631
This article is part of the Research TopicDietary Change Strategies for Sustainable Diets and their Impact on Human Health - Volume 1View all 44 articles
Background: This study assessed whether perceived stress and depressive symptoms were associated with the frequency of consumption of specific food groups among female university students.
Methods: A cross-sectional study was conducted among female university students using a simple random sampling method. The response rate was 97%, with a total number of 385 participants. The associations between stress levels and most/least-consumed food groups, and between depressive symptoms levels and most/least-consumed food groups were assessed. The questionnaire included a 12-item self-administered food frequency questionnaire, Cohen's Perceived Stress Scale, and the Beck Depression Inventory-II. The study was approved by the University Ethical Committee prior to the data collection. One-way Analysis of Variance (ANOVA) and an independent-sample t-test were performed to test the equality of population means across the categories of each independent variable depending on the number of categories of the independent variable.
Results: Overall, this group of female university students fell under the mild mood disturbance category (depressive symptoms) (BDI-II) and had moderate perceived stress (PSS). Perceived stress was associated with more frequent consumption of salad/raw vegetables and cooked vegetables and less frequent consumption of cake/cookies and meat/sausage products (p < 0.05). Additionally, depressive symptoms were associated with less frequent consumption of fresh fruits and increased consumption of fast food/canned food and soft drinks (p < 0.05).
Conclusions: The data showed that stress and depression were associated with different dietary preferences, which is consistent with the distinctions between stress and depression in human behavior. Specifically, the results revealed associations between soft drinks consumption and higher depressive symptoms and between frequent consumption of salad/raw vegetables and cooked vegetables and higher perceived stress among this group of female university students.
Stress and depression can result in a number of complications, including maladaptive eating behaviors such as overeating or undereating (Oliver et al., 2000; Kramlinger, 2001). These inconsistencies in dietary habits can be caused by stress and other factors, resulting in weight gain or loss in individuals with stress or depression. These changes in eating habits may eventually lead to changes in lifestyle behaviors (Schmidt, 2012). Additionally, undergoing stressful life situations could be a risk factor for developing depression (Kramlinger, 2001).
Over the past few years, the relationship between the type and the frequency of dietary intake has been studied in relation to mental health. This growing field of study concluded that higher consumption of processed and Western food indicates a higher risk of developing poor mental health (Rucklidge and Kaplan, 2016). Prospective studies have relied on causality to explain the nature of this relationship; unhealthy diets at baseline showed a higher risk of depression and poor mental health, whereas healthier diets at baseline showed better mental health and a lower risk of depression (Akbaraly et al., 2009; Jacka et al., 2011; Sánchez-Villegas et al., 2012). In experimental studies, when participants were exposed to a stressful situation, they tended to consume more of high-density foods and sweets (Oliver et al., 2000; Zellner et al., 2006). In addition, cross-sectional studies have suggested that higher perceived stress is positively associated with higher intake of fat, sodium, and carbohydrates (Nastaskin and Fiocco, 2015; Dehghan et al., 2016). However, other studies found that higher levels of stress were not associated with more sweets consumption but it was associated with lower fruit and vegetables intake (El Ansari and Berg-Beckhoff, 2015).
Moreover, systematic reviews have shown that foods rich in antidepressant nutrients, such as folate, iron, and chain omega-3 fatty acids (EPA and DHA), can enhance a person's mental health, and that people who consume these foods more often are less likely to develop depression (LaChance and Ramsey, 2018). The biological link between healthy diets and better mental health can be explained by several factors, including the neurotransmitter precursors, inositol and tryptophan (Grases et al., 2019). People with a higher depression score reported a lower consumption of legumes, fruits and vegetables which are among the foods that contain precursors to inositol and tryptophan which are important to brain health as opposed to people with lower scores (Grases et al., 2019). In line with these findings, cardioprotective diets that are high in fruits and vegetables and low in fat and refined sugar have been found to predict a lower risk of depression (Martínez-González, 2016). Overall, studies examining food choices under stress have found that people, particularly women, consume more types of food than they usually avoid for health reasons (Zellner et al., 2006). Regarding depression and dietary habits, most studies focused on the effects of certain diets on depression. These studies have shown that adherence to certain diets that provide healthier food choices results in improved mental health in depressed individuals (Jacka et al., 2017). Evidence also suggests that certain nutrients can positively affect mood and be used to treat depression, whereas other nutrients can increase the risk of it (Volker and Ng, 2006; Popa and Ladea, 2012). Moreover, it has been reported that poor dietary patterns could promote depressive symptoms (Jacka et al., 2014).
Studies that have sought to map the relationship between mental health symptoms (stress and depressive symptoms) and diet have reported that unhealthy food intake increases with perceived stress and depressive symptoms. Furthermore, unhealthy food consumption was linked to perceived stress in women only; however, depressive symptoms were linked to unhealthy food intake in both males and females (Mikolajczyk et al., 2009; El Ansari et al., 2014). A similar study concluded that levels of perceived stress and depressive symptoms increased with a decrease in fresh food intake and an increase in ready-to-eat food intake, and vice versa (Liu et al., 2007).
College students are vulnerable to vicious cycles in which poor diet choices and mental health symptoms perpetuate each other. Due to their new environment, responsibilities, financial pressure, and time management struggles, students are more prone to experience stress (Schmidt, 2012). Long-lasting stress has been found to be associated with weight gain as it triggers eating more frequently and less healthy (Torres and Nowson, 2007; Roberts, 2008). Depression can also lead to overeating or undereating (Kramlinger, 2001; Volker and Ng, 2006). However, research on the effects of stress and depression on dietary habits and choices in the UAE or the Middle East, specifically in Gulf Cooperation Council (GCC) countries, is limited and outdated. To the best of our knowledge, no studies have been conducted on UAE college students regarding the relationships between dietary habits, depressive symptoms, and perceived stress. Therefore, in this study, the association between frequency of food consumption and two mental health indicators (perceived stress and depressive symptoms) was assessed in female university students in the UAE.
This cross-sectional study was conducted following obtaining ethical clearance. After obtaining written informed consent, the participants were asked to complete a 12-item food frequency questionnaire (FFQ), Beck Depression Inventory, and Cohen's Perceived Stress Scale, which were compiled into a single questionnaire. The details of the study methodology have been described elsewhere (Ali et al., 2021).
The sample was drawn from female students at a national university in the United Arab Emirates (UAE). Several classes were randomly chosen from a list of courses held in spring 2018. The data were collected from April to May 2018. The sample represented ~10% of the target population of 4,000 students and resulting in a total sample size of 389 students. A total of 385 questionnaires were accepted, resulting in a response rate of 98.9%. Before data collection, a pilot study was conducted on a sample of ten students to verify that the questionnaire was well-understood and appropriate for use with the intended sample. Pilot study participants were not included in the final data analysis.
Data were collected through a self-reported questionnaire consisting of three sections: a 12-item food frequency questionnaire, the 10-item Cohen's Perceived Stress Scale (PSS), and the Beck Depression Inventory-II (BDI-II). Weight and height were self-reported, which might have been a potential source of bias.
The Food Frequency Questionnaire (Mikolajczyk et al., 2009) assessed the frequency of consumption of 12 food groups: sweets, cake/cookies, snacks, fast food/canned food, fresh fruits, salad/raw vegetables, cooked vegetables, soft drinks, meat/sausage products, fish/seafood, milk/milk products, and cereal/cereal products. Students were asked to answer the question “How often do you eat the following foods?” on a 5-point scale (several times a day = 5, daily = 4, several times a week = 3, 1–4 times a month = 2, and never = 1). Cronbach's α= 0.68. The FFQ was used in previous studies (Mikolajczyk et al., 2009; El Ansari et al., 2014; El Ansari and Berg-Beckhoff, 2015). Although not formally validated, the FFQ we used contains food groups that are essential for studying dietary behavior, which in line with the contents of other validated FFQs (Mikolajczyk et al., 2009).
The PSS estimates the degree to which situations in a person's life are considered stressful through 10 items (Cohen et al., 1983; Cohen and Williamson, 1988). Students expressed their feelings and thoughts for each item during the past month on a 5-point scale (0 = Never, 1 = Almost never, 2 = Sometimes, 3 = Fairly often, and 4 = Very often). In this study, the Cronbach's α was 0.68.
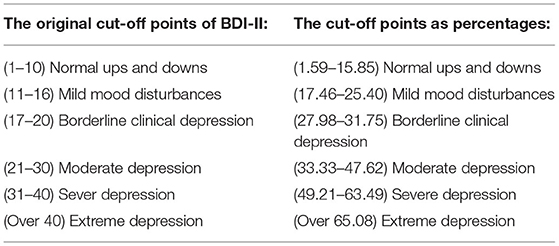
The BDI-II measures the behavioral manifestation of depression (Salkind, 1969; Beck et al., 1996). The BDI-II was created in 1996 in alignment with the DSM-IV's diagnostic criteria for major depressive episode (Wang and Gorenstein, 2013). The BDI-II consists of 21 items with four statements each. Students were asked to choose one statement for each item that best described their feelings over the previous two weeks. The statements were scored on a 4-point scale ranging from 0 to 3. The creators of the BDI-II have enhanced validity compared to the original BDI (Beck et al., 1996). The Arabic version of the BDI-II (Ghareeb, 2000) was validated in 18 Arab countries: Palestine, Lebanon, Syria, Jordan, Saudi Arabia, Kuwait, Qatar, Bahrain, the United Arab Emirates, Oman, Yemen, Egypt, Sudan, Tunisia, Libya, Algeria, and Morocco, with Cronbach's αfalling between 0.82 to 0.93 (Alansari, 2006; Maamria, 2010). To compensate for the removal of item 9 (suicidal thoughts and wishes), the scoring system was adjusted according to the ethical committee's instructions.
As a result, the BDI-II cut-off points were converted to percentages. The original BDI-II had a total score of 63, and the new score after deleting item 9 was 60. The BDI-II percentages were calculated by dividing by 63 and multiplying by 100 (63 was the total of score). The modified version of the BDI-II consists of 20 items, with a Cronbach's αof 0.89.
The FFQ consisted of 12 items, and was measured on a five-point scale (several times a day = 5, daily = 4, several times a week = 3, 1–4 times a month = 2, and never = 1).
To compare the results with those of other studies (Mikolajczyk et al., 2009), and by considering the least moderate correlations (Spearman > 0.2) among the items of each subscale and factor analysis and based on theoretical considerations regarding the content of foods, it was decided to combine some food groups into subscales. The following subscales were used: unhealthy foods subscale that consisting of sweets, cakes/cookies, snacks, and fast food and a fresh food subscale, consisting of fresh fruits, salads/raw vegetables, and cooked vegetables. The remaining food groups were divided into separate subscales. The subscales' scores were calculated as mean scores of the corresponding items.
The BDI-II score (BDI-II sum) was computed by summing the responses to all the 20 items that measured this mental health indicator. The Perceived Stress Score variable (PSS sum) was generated by summing all responses to all items of Cohen's Perceived Stress Scale after reversing scores to the four positively stated items (statements 4, 5, 7, and 8). Reversing was performed by recoding four statements: 0 for 4, 1 for 3, 2 kept as 2, 3 for 1, and 0 for 4.
The normality of all score variables was checked using kurtosis and skewedness, histograms, and Q_Q plots. All variables were normally distributed.
Independent associations between food groups (FFQ), perceived stress (PSS) and depressive symptoms (BDI-II) were examined using univariate and multivariate regression models. The newly created FFQ sum, PSS sum, and BDI-II sum served as dependent variables and were used for the subsequent data analysis. Sociodemographic and anthropometric variables were used as independent variables.
The collected data were coded, entered, and analyzed using the Statistical Package SPSS version 25. Statistical tests with p-values < 0.05 were considered statistically significant. Descriptive statistics was computed to describe all questionnaire items.
Multiple linear regression analysis was performed to predict each outcome variable using the following predictors: Marital status, age, BMI, exercise, stress, and depressive symptoms.
Table 1 shows the participants' sociodemographic characteristics. The study population mainly consisted of Emiratis (97.1%). Their ages ranged from 17 to 24 years old. Regarding self-reported height and weight, 12.7% of the participants were underweight, 16.4% were overweight, and 15.1% were obese.
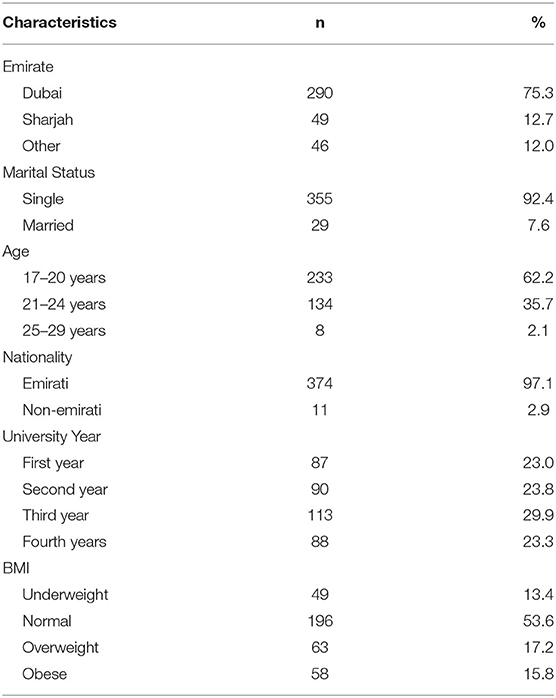
Table 1. Sociodemographic characteristics and weight status (n = 385).
The mean scores were computed for the unhealthy food and fresh food subscales. Among this group of students, both unhealthy food and fresh food subscales had an average consumption (on a scale from 1 to 5). Overall, this group of students fell under the categories of “mild mood disturbances” and “moderate stress” for depressive symptoms and stress respectively.
The associations between the consumption of each food group and perceived stress and depression were assessed separately using a linear regression. Table 2 shows that the significant associations between food groups, perceived stress, and depressive symptoms were not equal, whereas there were four associations for perceived stress and only three for depressive symptoms. Furthermore, negative associations were observed between perceived stress and cake/cookies and meat/sausage products, and between depressive symptoms and fresh fruits. Additionally, positive associations were observed between perceived stress and salad/raw vegetables and cooked vegetables and between depressive symptoms and soft drinks and fast food/canned food.
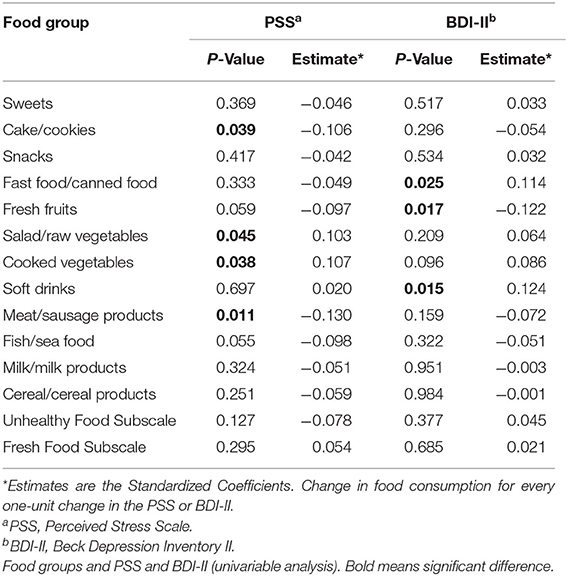
Table 2. Associations between food intake and perceived stress or depressive symptoms.
For every unit increase in PSS, the consumption of cake/cookies will decrease by 0.106, and meat/sausage product consumption will decrease by 0.130. However, salad/raw vegetable consumption will increase by 0.103 and cooked vegetable consumption will increase by 0.107. Regarding depressive symptoms, for every unit increase in the BDI-II, fresh fruits consumption will decrease by 0.122, fast/canned food consumption will increase by 0.114, while soft drink consumption will increase by 0.124 (Table 2).
Multiple linear regressions were used to assess the association between the consumption of all food groups together and both the PSS and BDI-II (Table 3). It was found that the consumption of unhealthy food, fresh food, fish/seafood, milk/milk products, and cereal/cereal products was not significantly associated with perceived stress and depressive symptoms among this group of university students. In addition, increased consumption of soft drinks was significantly associated with higher depressive symptoms, whereas increased consumption of meat/sausage products was significantly associated with lower perceived stress.
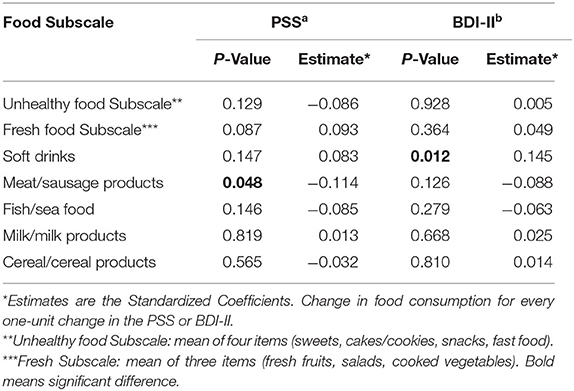
Table 3. Food groups, PSS and BDI-II (multivariable analysis).
Table 4 presents the results of the multiple linear regression model of unhealthy food consumption. This included marital status, age, BMI, exercise, BDI-II sum, and PSS sum. These variables accounted for only ~3% of the variation in the unhealthy food consumption subscale (R2 = 0.028). However, this difference was not statistically significant (p = 0.141). Exercise was the only variable that had a significant effect on the unhealthy food consumption (p < 0.050).
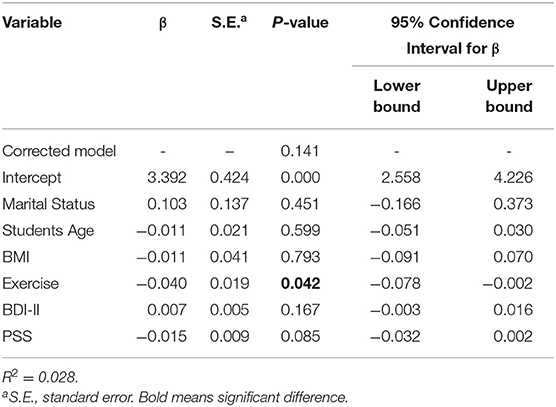
Table 4. General linear model for unhealthy food consumption.
The main objective of this study was to assess the association between perceived stress and depressive symptoms with the frequency of consumption of specific food groups among female university students. Habits formed during youth are likely to be sustained throughout later adulthood (Schmidt, 2012). Therefore, studying the complex relationship between food choice and mental state could help us to understand how the frequency of consumption of certain food groups could be influenced by stress or depression, or vice versa.
The results of this study showed that the consumption of cakes/cookies and meat/sausage products was negatively associated with stress, whereas consumption of salad/raw vegetables and cooked vegetables was positively associated with stress. These results are inconsistent with those of other cross-sectional studies conducted on different populations. Several studies have reported higher consumption of sweets, snacks, and fast food with higher stress levels or higher consumption of fruits and vegetables with lower stress levels (Mikolajczyk et al., 2009; El Ansari and Berg-Beckhoff, 2015). Nevertheless, a study conducted in Palestine reported results similar to those of the present study.
It was found that among females, the consumption of cakes/cookies was negatively associated with stress, and among males, all food groups except cereal/cereal products were negatively associated with stress (Mohamed Yassin, 2016). The latter study suggested that lower consumption of cakes/cookies with higher stress could be linked to the fact that people consume foods high in carbohydrates (CHO) to relieve their stress. This could be explained by the fact that highly palatable foods that are high in CHO and fat, such as cakes/cookies, enhance opioid levels in the brain, which are linked to feelings of pleasure and are eaten as rewards after stress. Hence, students' stress levels were lower when they consumed these foods (Society for the Study of Ingestive Behavior, 2009; Mohamed Yassin, 2016). However, this suggestion is based on the assumption that students with lower stress levels who consumed more cakes and cookies were stressed before, and consumed more of this food group to relieve their symptoms. This assumption could not be confirmed by the current study design. Another possible explanation could be behavioral differences between stress and depression among individuals.
This study found that the consumption of fast food/canned food and soft drinks was positively associated with depressive symptoms whereas, the consumption of fresh fruits was negatively associated with depressive symptoms. These results are consistent with those of similar studies found regarding these food groups and depressive symptoms (Mikolajczyk et al., 2009; El Ansari et al., 2014; Martínez-González, 2016). Previous studies have found that consuming foods such as fruits, vegetables, seafood, and low processed organ meats that are rich in antidepressant nutrients is associated with a lower risk of depression (Martínez-González, 2016). In addition to the fact that highly processed and high-sugar foods are among the foods linked to depression, low-processed organ meats, seafood, and legumes were found to have the highest levels of antidepressants (Martínez-González, 2016). In line with these findings, the current study found a negative association between vegetable consumption and depression; however, no significant effects were found regarding for seafood, organ meat, or legumes consumption. Depression reflects behavioral changes in people with higher levels of depressive symptoms. Thus, individuals with depressive symptoms are more likely isolate themselves from their social networks, which might increase their symptoms. Unlike stress, depression creates feelings of emptiness and hopelessness, pointlessness of efforts and severe reduction in the perception of self-efficacy (Brouwers and Tomic, 2000; Bisschop et al., 2004; Gallagher et al., 2011).
As such, making an effort to eat healthier food for people with depression would not be significant; hence, the tendency we report here to consume more easily accessible foods that fall under the unhealthy food groups in the high-depression group. However, it may still be considered important and possible to eat healthily; hence, there is a positive link between higher levels of stress and healthier eating behaviors. It may be interest in the future to investigate the extent to which there is a discrepancy between the wish to eat healthily and the actual dietary behavior of the high-stress group. Importantly, it would be interesting to determine the extent to which a higher discrepancy (between wish and actual dietary behavior) is linked via dissonance, to the levels of stress reported in this group.
This study found only one significant association between stress and one with depressive symptoms. Consumption of meat/sausage products was negatively associated with stress, whereas the consumption of soft drinks was positively associated with depressive symptoms. These findings are not consistent with findings from other studies that found positive associations between unhealthy food (sweets/snacks/cookies/fast food) and stress and depression, nor with studies that found negative associations between healthy food (fruits and vegetables) and stress and depression (Mikolajczyk et al., 2009; El Ansari et al., 2014). However, Yassin et al. found that stress was negatively associated with unhealthy food consumption among males only, which is similar to the insignificant result found in this study regarding the unhealthy food subscale and stress (Mohamed Yassin, 2016). First, the explanation for the negative association found between meat/sausage product consumption and stress is not known, although it could mean that lower stress leads to an increased consumption of protein. Future studies are needed to further investigate this association. Second, the positive association between soft drink consumption and depressive symptoms could be related to behavioral changes in people with higher depressive symptoms, as previously mentioned.
Finally, the general linear regression model controlling for confounding variables showed that exercise was the only variable that predicted unhealthy food consumption. The results showed that the frequency of exercise decreased with a higher consumption of unhealthy food. Previous studies found that individuals who report higher levels of physical activity have lower levels of stress and depression. Therefore, there may be an indirect association between the two mental health indicators and unhealthy food consumption (Norris et al., 1992; Hassmén et al., 2000). Unhealthy food consumption could be affected more by variables not included in this study, which should be investigated in future studies. The chief among these are socioeconomic variables, variables related to parents' educational level, and other social factors. As this study is cross-sectional, causation could not be derived and was susceptible to bias. Therefore, future studies should focus on clinical and controlled experiments.
This study found associations between stress, and depression, with food consumption among female university students. In contrast to stress, feelings of hopelessness, which are symptomatic of depression, reduce the importance of consuming healthier food. Additionally, eating cakes/cookies was negatively associated with perceived stress. However, assessing the presence of pre-existing stress that affects food consumption was not within the scope of this study. Further studies are required to investigate the relationship between stress and food consumption in this population and to identify the main reasons for this relationship. This study suggests identifying nutritional issues when addressing perceived stress or depressive symptoms among female university students. Moreover, improving the mental state of students could improve their food choice and intake.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Mercedes Sheen Chair of the Research Ethics Committee, Zayed University. The patients/participants provided their written informed consent to participate in this study.
OM wrote the initial draft of the manuscript, compiled the instruments in one questionnaire and performed data collection. HA supervised the project, provided guidance and advice when needed. LS performed data analysis, wrote the initial draft of the statistical analysis and results. EH provided guidance regarding the mental health indicators and the instruments used to assess them in addition to contributing to the discussion. RA provided guidance regarding the food frequency questionnaire and suggested the adjustments of the BDI-II scoring system to compensate for the obligatory removal of one item. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to thank Dr. Walid El Ansari from University of Gloucestershire, Gloucester - United Kingdom, for providing some of the instruments as this study was based on his previous work.
Akbaraly, T. N., Brunner, E. J., Ferrie, J. E., Marmot, M. G., Kivimaki, M., and Singh-Manoux, A. (2009). Dietary pattern and depressive symptoms in middle age. Br. J. Psychiatry 195, 408–413. doi: 10.1192/bjp.bp.108.058925
Alansari, B. M (2006). Internal consistency of an Arabic adaptation of the beck depression inventory-ii with college students in eighteen Arab countries. Soc. Behav. Pers. 34, 25–30. doi: 10.2224/sbp.2006.34.4.425
Ali, A., Hendawy, A., Ahmad, O., Al Sabbah, H., Smail, L., and Kunugi, H. (2021). The Arabic version of the cohen perceived stress scale: factorial validity and measurement invariance. Brain Sci. 11, 419. doi: 10.3390/brainsci11040419
Beck, A. T., Steer, R. A., and Brown, G. K. (1996). Manual for the Beck Depression Inventory-II, 2nd Edn. San Antonio, TX: Psychological Corporation.
Bisschop, M. I., Kriegsman, D. M. W., Beekman, A. T. F., and Deeg, D. J. H. (2004). Chronic diseases and depression: the modifying role of psychosocial resources. Soc. Sci. Med. 59, 721–733. doi: 10.1016/j.socscimed.2003.11.038
Brouwers, A., and Tomic, W. (2000). A longitudinal study of teacher burnout and perceived self-efficacy in classroom management. Teach. Teach. Educ. 16, 239–253. doi: 10.1016/S0742-051X(99)00057-8
Cohen, S., Kamarck, T., and Mermelstein, R. (1983). A global measure of perceived stress. J. Health Soc. Behav. 24, 385–396. doi: 10.2307/2136404
Cohen, S., and Williamson, G. (1988). “Perceived stress in a probability sample of the United States,” in The Social Psychology of Health, eds S. Spacapan and S. Oskamp (Newbury Park, CA: SAGE), 31–67.
Dehghan, P., Pourmoradian, S., Mahdavi, A. M., Sarmadi, B., and Mehralizadeh, S. (2016). Relationship between perceived stress and dietary intakes in type 2 diabetic patients. Curr. Top. Nutraceuticals Res. 14, 199–206. Available online at: https://www.researchgate.net/publication/309557097_RELATIONSHIP_BETWEEN_PERCEIVED_STRESS_AND_DIETARY_INTAKES_IN_TYPE_2_DIABETIC_PATIENTS
El Ansari, W., Adetunji, H., and Oskrochi, R. (2014). Food and mental health: relationship between food and perceived stress and depressive symptoms among university students in the United Kingdom. Cent. Eur. J. Public Health. 22, 90–97. doi: 10.21101/cejph.a3941
El Ansari, W., and Berg-Beckhoff, G. (2015). Nutritional correlates of perceived stress among university students in Egypt. Int. J. Environ. Res. Public Health. 12, 14164–14176. doi: 10.3390/ijerph121114164
Gallagher, D., Mhaolain, A. N., Crosby, L., Ryan, D., Lacey, L., and Coen, R. F. (2011). Self-efficacy for managing dementia may protect against burden and depression in Alzheimer's caregivers. Aging Ment Heal. 15, 663–670. doi: 10.1080/13607863.2011.562179
Ghareeb, G. A (2000). Beck Depression Inventory-II Studies of Instructions, Studies of Reliability and Validity, Standardization and Cut-Off Points. Cairo: The Anglo Egyptian Bookshop.
Grases, G., Colom, M. A., and Sanchis, P. (2019). Possible relation between consumption of different food groups and depression. BMC Psychol. 7, 14. doi: 10.1186./s40359-019-0292-1
Hassmén, P., Koivula, N., and Uutela, A. (2000). Physical exercise and psychological well-being: a population study in Finland. Prev Med (Baltim). 30, 17–25. doi: 10.1006/pmed.1999.0597
Jacka, F. N., Cherbuin, N., Anstey, K. J., and Butterworth, P. (2014). Dietary patterns and depressive symptoms over time: examining the relationships with socioeconomic position, health behaviours and cardiovascular risk. PLoS ONE 9, e87657. doi: 10.1371/journal.pone.0087657
Jacka, F. N., Kremer, P. J., Berk, M., de Silva-Sanigorski, A. M., Moodie, M., Leslie, E. R., et al. (2011). A prospective study of diet quality and mental health in adolescents. PLoS ONE 6, e24805. doi: 10.1371/journal.pone.0024805
Jacka, F. N., O'Neil, A., Opie, R., Itsiopoulos, C., Cotton, S., and Mohebbi, M. (2017). A randomised controlled trial of dietary improvement for adults with major depression (the “SMILES” trial). BMC Med. 15, 1–13. doi: 10.1186/s12916-017-0791-y
Kramlinger, K (2001). Mayo Clinic on Depression: Answers to Help You Understand, Recognize and Manage Depression. Rochester, MN: Mayo Clinic.
LaChance, L. R., and Ramsey, D. (2018). Antidepressant foods: an evidence-based nutrient profiling system for depression. World J Psychiatry 8, 97–104. doi: 10.5498/wjp.v8.i3.97
Liu, C., Xie, B., Chou, C. P., Koprowski, C., Zhou, D., and Palmer, P. (2007). Perceived stress, depression and food consumption frequency in the college students of China seven cities. Physiol. Behav. 92, 748–754. doi: 10.1016/j.physbeh.2007.05.068
Maamria, B (2010). Standardizing Beck Depression Inventory-II on samples from the two genders in the Algerian environment. Arab Ejournal. 25, 92–105. Available online at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3539842/pdf/JMedLife-05-414.pdf
Martínez-González, M. A (2016). Food patterns and the prevention of depression. Proc. Nutr. Soc. 75, 139–146. doi: 10.1017/S0029665116000045
Mikolajczyk, R. T., El Ansari, W., and Maxwell, A. E. (2009). Food consumption frequency and perceived stress and depressive symptoms among students in three European countries. Nutr. J. 8, 1–8. doi: 10.1186/1475-2891-8-31
Mohamed Yassin, M (2016). Food consumption in association with perceived stress and depressive symptoms: a cross sectional study from five universities and three colleges in Gaza Strip, Palestine. Eur. J. Prev. Med. 4, 20. doi: 10.11648/j.ejpm.20160401.14
Nastaskin, R. S., and Fiocco, A. J. (2015). A survey of diet self-efficacy and food intake in students with high and low perceived stress. Nutr. J. 14, 42. doi: 10.1186/s12937-015-0026-z
Norris, R., Carroll, D., and Cochrane, R. (1992). The effects of physical activity and exercise training on psychological stress and well-being in an adolescent population. J Psychosom Res. 36, 55–65. doi: 10.1016/0022-3999(92)90114-H
Oliver, G., Wardle, J., and Gibson, E. L. (2000). Stress and food choice: A laboratory study. Psychosom. Med. 62, 853–865. doi: 10.1097/00006842-200011000-00016
Popa, T. A., and Ladea, M. (2012). Nutrition and depression at the forefront of progress. J. Med. Life. 5, 414–419. Available online at: http://arabpsynet.com/Archives/OP/eJ25-26BachirMaamria.pdf
Roberts, C. J (2008). The effects of stress on food choice, mood and bodyweight in healthy women. Nutr. Bull. 33, 33–39. doi: 10.1111/j.1467-3010.2007.00666.x
Rucklidge, J. J., and Kaplan, B. J. (2016). Nutrition and mental health. Clin. Psychol. Sci. 4, 1082–1084. doi: 10.1177/2167702616641050
Salkind, M. R (1969). Beck depression inventory in general practice. J. R. Coll. Gen. Pract. 18, 267–271.
Sánchez-Villegas, A., Toledo, E., De Irala, J., Ruiz-Canela, M., Pla-Vidal, J., and Martínez-González, M. A. (2012). Fast-food and commercial baked goods consumption and the risk of depression. Public Health Nutr. 15, 424–432. doi: 10.1017/S1368980011001856
Schmidt, M (2012). Predictors of self-rated health and lifestyle behaviours in Swedish university students. Glob. J. Health Sci. 4, 1-14. doi: 10.5539/gjhs.v4n4p1
Society for the Study of Ingestive Behavior (2009). High-fat, High-sugar Foods Alter Brain Receptors. ScienceDaily. Available online at: https://www.sciencedaily.com/releases/2009/07/090727102024.htm (accessed February 13, 2022).
Torres, S. J., and Nowson, C. A. (2007). Relationship between stress, eating behavior, and obesity. Nutrition 23, 887–894. doi: 10.1016/j.nut.2007.08.008
Volker, D., and Ng, J. (2006). Depression: does nutrition have an adjunctive treatment role? Nutr. Diet. 63, 213–226. doi: 10.1111/j.1747-0080.2006.00109.x
Wang, Y. P., and Gorenstein, C. (2013). Psychometric properties of the Beck Depression Inventory-II: a comprehensive review. Rev. Bras. Psiquiatr. 35, 416–431. doi: 10.1590/1516-4446-2012-1048
Keywords: perceived stress, depressive symptoms, university students, dietary behavior, mental health
Citation: Mohamad O, Al Sabbah H, Smail L, Hermena EW and Al Ghali R (2022) Food Consumption Frequency, Perceived Stress, and Depressive Symptoms Among Female University Students in Dubai, United Arab Emirates. Front. Sustain. Food Syst. 6:792631. doi: 10.3389/fsufs.2022.792631
Received: 10 October 2021; Accepted: 07 February 2022;
Published: 18 March 2022.
Edited by:
Alexandru Rusu, Biozoon Food Innovations GmbH, GermanyReviewed by:
Dan Cristian Vodnar, University of Agricultural Sciences and Veterinary Medicine of Cluj-Napoca, RomaniaCopyright © 2022 Mohamad, Al Sabbah, Smail, Hermena and Al Ghali. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Haleama Al Sabbah, aGFsZWVtYWguYWxzYWJhaEB6dS5hYy5hZQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.