 Monica Chande1Happiness Muhimbula1Ruth Mremi1Yasinta C. Muzanila2Nelson C. Kumwenda3John Msuya1Harry Msere3
Monica Chande1Happiness Muhimbula1Ruth Mremi1Yasinta C. Muzanila2Nelson C. Kumwenda3John Msuya1Harry Msere3 Mateete Bekunda4
Mateete Bekunda4 Patrick Okori3
Patrick Okori3 Wanjiku N. Gichohi-Wainaina3*
Wanjiku N. Gichohi-Wainaina3*- 1Department of Food Technology, Nutrition and Consumer Studies, Sokoine University of Agriculture, Morogoro, Tanzania
- 2Department of Biosciences, Solomon Mahlangu College of Science and Education, Sokoine University of Agriculture, Morogoro, Tanzania
- 3International Crops Research Institute for the semi-arid Tropics, Lilongwe, Malawi
- 4Africa Rising Program, International Institute for Tropical Agriculture, Arusha, Tanzania
Background: Iron and zinc deficiency are common public health problems in low-income countries largely due to poor consumption of iron and zinc rich foods. It has previously been observed that 57% of school aged children (SAC) in Tanzania suffer from anemia. In addition, estimates indicate that over 25% of the population have inadequate zinc intake. Pearl millet is an example of a nutrient dense, resilient cereal crop, that can be promoted to diversify diets and combat iron and zinc deficiency. This study overall aim was to increase pearl millet consumption among school aged (5 – 12 years) children. As part of the study, we investigated, the drivers of food choice relating to pearl millet consumption.
Methods: The study was a cross-sectional study of randomly selected households in Kongwa district, Dodoma region of Tanzania. In total, 128 women of reproductive age (20 – 49 years) were randomly selected for the study. A study questionnaire consisting of 66 items, was developed and validated. The constructs in the questionnaire were categorized in two groups: internal and external factors. Respondents were asked to indicate their level of agreement or disagreement with statements read to them by interviewers. The scores on intention and behavior constructs were based on the number of times caregivers intended to, or had fed their school going children with pearl millet in the referent month. Intention was considered high if it was higher than the median intention score of the group, and low if it was equal to or lower than the median scores. Correlations and multiple linear regressions were performed to measure association between constructs and to identify predictive constructs. The Mann-Whitney U test was used for score comparison.
Results: There was a significant difference between intention and behavior among those who did not consume pearl millet (P = 0.003), and those who consumed pearl millet two or more times a week, in the same month (P = 0.01). Knowledge was significantly correlated with behavior identity (ρ = 0.58, P = 0.001), while health behavior identity was significantly correlated with intention (ρ = 0.31, P = 0.001). Intention of caregivers was significantly and positively correlated (ρ = 0.44, P = 0.001) with and predicted consumption of pearl millet (ρ = 0.87, P = 0.067).
Conclusion: Increasing knowledge or awareness on nutritional benefits of pearl millet among caregivers may increase consumption of pearl millet by children of school going age.
Introduction
Iron and zinc deficiency are common public health problems in low-income countries largely due to poor consumption of iron and zinc rich foods (Bouis, 2002; Brown et al., 2004; Nestel et al., 2006). Anemia is one of the many consequences of iron deficiency (Lopez et al., 2016). Among school aged children (SAC) specifically, a study conducted in 2001, indicated that 57% of SAC in Tanzania suffered from anemia (Hall et al., 2001). Anemic school-children have decreased motor activity, social inattention, and decreased school performance (Grantham-McGregor and Ani, 2001). In Tanzania, estimates indicate that over 25% of the population have inadequate zinc intake (Wessells et al., 2012). In terms of consequences of zinc deficiency, observational studies among school-age children, have shown hair zinc to be associated with reading ability, suggesting that zinc deficiency interfered with academic performance (Butrimovitz and Purdy, 1978; Cavan et al., 1993). Addressing these deficiencies is therefore crucial not only for the aforementioned consequences on growth and health but also for economic development (Zimmermann and Hurrell, 2007). Food based strategies to combat micronutrient deficiencies present a sustainable and accessible solution (FAO, 2011). Pearl millet (PM) is an example of a nutrient dense, resilient cereal crop, that can be promoted to diversify diets and combat iron and zinc deficiency (Rao et al., 2006; Kanatti et al., 2014). It is grown mostly in marginal environments in the arid and semi-arid tropical regions of Asia and Africa (Jukanti et al., 2016). In terms of dietary contribution, it is a major contributor of dietary protein, iron, and zinc intake in a variety of rural populations in sub-Saharan Africa (Agte et al., 1999; Kodkany et al., 2013).
This study was embedded within a wider program that aimed to link agriculture production to nutrition to address malnutrition in the semi-arid agro ecologies of Kongwa district, Dodoma Region, Tanzania, Although pearl millet is already consumed in Dodoma region of Tanzania (Rohrbach and Kiriwaggulu, 2007), we aimed to increase its consumption to a wider group beyond pre-school children. The results presented herein elucidate via a combination of two psychosocial theories-the Theory of Planned Behavior (TPB) and Health Belief Model (HBM); the factors that drive pearl millet consumption among their school going children (5 – 12 years).
Methods
Ethical Approvals and Consent
This study did not seek for ethical approval from an ethical review board because it did not involve blood collection, any invasive procedure or anthropometry. Approvals from district administrative officials as well as traditional authorities were obtained as part of the study preparation. Prior to questionnaire administration, all respondents had the study explained to them in the local language Kiswahili, assured of confidentiality and offered the opportunity to ask questions. Respondents were also informed that they were free to decline participation at any point during the questionnaire administration. Study participants then indicated their approval by giving written informed consent or thumb print.
Study Site
This cross-sectional study of randomly selected households was conducted in Kongwa district, Dodoma region of Tanzania. Kongwa district is one of the action districts of the Africa Research in Sustainable Intensification for the Next Generation (Africa RISING) program. The program aims to create opportunities for smallholder farm households to move out of hunger and poverty through sustainably intensified farming systems that improve food, nutrition, and income security, particularly for women and children (Africa RISING, 2021). In Kongwa the study was conducted in, Laikala, the driest village in the district and largest producer of pearl millet. Laikala village receives about 357 mm of rainfall annually, with annual ambient temperatures ranging between 18 and 34°C. The main economic activity in the area is integrated crop and livestock farming (NBS, 2013).
Sampling and Study Participants
In total, 128 caregivers who were women of reproductive age (20 – 49 years) were randomly selected for the study. According to Francis et al. (2004) it is reasonable to assume at least a moderate effect size with a sample size of 80 – 160 individuals for Theory of Planned Behavior studies using a multiple regression. Households with school aged children (5 – 12 years) were intentionally selected using the random walk sampling method (Wei et al., 2004), and all caregivers from selected households were listed. From this list, one caregiver was randomly selected in each household for questionnaire administration. The main selection criteria were willingness to participate, presence of a school aged child (SAC) within the household and previous or current consumption of pearl millet. When a selected woman did not fulfill the selection criteria, she was replaced with another woman in the same household that met the inclusion/exclusion criteria. All selected women met the selection criteria.
Questionnaire Development and Validation
The study questionnaire consisted of 66 items, identified from literature. The items were characterized into 12 constructs based on the combined model of TPB and HBM as was undertaken in several studies (Sun et al., 2006; Fanou-Fogny et al., 2011; Macharia-Mutie et al., 2011; Abizari et al., 2013; Talsma et al., 2013) (Table 1). The following constructs were used: knowledge of iron and zinc deficiency and pearl millet, perceived susceptibility to iron and zinc deficiency, perceived severity of iron and zinc deficiency, health value attached to anemia or zinc deficiency in the SAC, health behavior identity attached to giving pearl millet to address iron deficiency, anemia or zinc deficiency, perceived barriers to give pearl millet, attitudes toward pearl millet consumption, subjective norms, external control beliefs and cues to action influencing (lack of) consumption of pearl millet by school aged children, intention to give pearl millet to the SAC, and behavior or pearl millet consumption among school aged children. In detail the constructs assessed the following (Table 1):
1. Knowledge assessed the caregivers understanding on the relationship between pearl millet and health, and specifically its' relationship to iron deficiency or anemia and zinc deficiency
2. Perceived susceptibility assessed caregiver's feeling about her school aged child being exposed to iron deficiency or anemia and zinc deficiency
3. Perceived severity assessed caregiver's feeling that her school aged child being exposed to iron deficiency or anemia and zinc deficiency is serious
4. Health value assessed the importance caregiver places on the outcome of her school aged child being anemic or zinc deficient
5. Health behavior identity assessed caregiver's evaluation of the effectiveness of giving pearl millet or iron rich food in reducing the perceived threat-that is iron deficiency anemia and zinc deficiency
6. Perceived barriers assessed caregiver's evaluation of various complications that hinder her in giving pearl millet to the school aged child
7. Attitude toward behavior assessed caregiver's evaluation of sensory and nutrient content attributes of pearl millet and how these influenced giving this to the SAC
8. Cues to action assessed surrounding situation that cause a caregiver to change her health behavior in feeding pearl millet to her school aged child
9. Control belief assessed a caregiver's perceived ability to make a decision on feeding pearl millet to their school aged child
10. Subjective norms assessed a caregiver's perceived social influencers to give, or not to give, pearl millet to their school aged child. In detail, this assessed who is important for the giving pearl millet to the SAC and the value of that persons opinion
11. Behavioral intention indicated how much effort a caregiver is planning to make, in order to give pearl millet to school aged child
12. Behavior assessed the giving pearl millet to SAC by caregivers

Table 1. Functioning explanation of constructs used to examine internal and external factors predicting intention of caregivers to give pearl millet to school aged children.
Examples of item statements are provided in Table 5.
To assess nutrition related behavior of individuals, constructs were further categorized in two groups that is, internal and external factors. The internal factors were further grouped into “background and perception,” “beliefs and attitudes” and “intention.” “Background and perception” consisted constructs such as knowledge, perceived susceptibility, perceived severity and health value while “beliefs and attitudes” contained health behavior identity, attitude toward behavior and perceived barriers. External factors were subjective norms, cues to action and control belief.
Respondents were asked to indicate their level of agreement or disagreement with statements read to them by interviewers. Prior to administration, the questionnaire was verified in focus group discussions and pre-tested among caregivers in a site similar to Laikala village. Changes to the questionnaire were them made after pretesting and validation. The questionnaire was subsequently translated into the local language (Swahili) and correctness checked with back translation into English.
Scale Measurements and Analysis
Knowledge, perceived susceptibility, perceived severity, health value, health behavior identity, perceived barriers, cues to action and control belief constructs were rated using a five-point likert scale that ranged from strongly disagree, disagree, neutral, agree and strongly agree. The reason that odd numbered scales were chosen was so that a central neutral response and an equal number of positive and negative responses above and below the neutral middle response were provided (Emerson, 2017). The score for each construct was computed as the sum of individual item scores. The scores for the constructs “Attitudes toward behavior” and “Subjective norms” were sums of products of paired items; attitudes × evaluation of attitudes, and normative beliefs × motivation to comply, respectively. To show negative, neutral or positive influences, item scores of attitudes and normative beliefs ranged from −2 to 2 and the scores of the evaluation of attitudes and motivation to comply ranged from +1 to +5. This resulted in a paired-item score range of −10 to 10. For intention and behavior, the rating scale ranged from not consumed, four or less times per month and two or more times per month. The scores on intention and behavior constructs were based on the number of times caregivers intended to, or had fed their school going pearl millet in the refereed month, respectively. Intention was considered high if it was higher than the median intention score of the group, and low if it was equal to or lower than the median scores as it was in previous studies (Sun et al., 2006; Fanou-Fogny et al., 2011; Macharia-Mutie et al., 2011; Abizari et al., 2013; Talsma et al., 2013).
Statistical Analyses
Descriptive statistics were performed to describe the caregivers and children. Multiple sentence constructs were tested for reliability of the questionnaire and internal consistency using Cronbach alpha and sentence-total correlation. The items within a construct were regarded as consistent when Cronbach alpha was ~0.75 or higher and the corrected sentence-total correlation of all sentences in a construct were higher than 0.30 (Field, 2005). The Mann-Whitney U test was used to examine differences in construct items between high and low intenders as the variables were on the ordinal scale (Karadimitriou et al., 2018). Spearman's rank correlation was used to test for bivariate associations within the combined model of TPB and HBM as the variables were on the ordinal scale (Schober et al., 2018). Three multiple linear regression models were used to examine the contribution of constructs to health behavior identity, intention and behavior. The first model was designed to identify constructs within background and perception that were associated with health behavior identity (Model 1). To identify constructs associated with intention, the second model combined internal factors (Perceived barrier, Health behavior identity, and Attitudes toward behavior) and external factors (Subjective norms, Control beliefs, and Cues to action) as predictor variables (Model 2). Finally, to identify constructs associated with pearl millet consumption among SAC, we included constructs that were significantly associated with intention (Health behavior identity, Attitudes toward behavior, Subjective norms, Cues to action) as well as intention. We included perceived barriers despite the fact that it was not a construct significantly associated with intention because of the importance of considering the role barriers to consumption may play. An interaction term between perceived barriers and intention was also included in this model to investigate how perceived barriers modulated the association between intention and behavior. All models were corrected for age of the child, education and interviewer effect.
The three models were therefore constructed as follows:
Model 1: Health behavior identity = f (Knowledge, Perceived susceptibility, Perceived severity, Health value, Age of child, Education and Interview effect).
Model 2: Intention = f (Perceived barrier, Health behavior identity, Attitudes toward behavior, Subjective norms, Control beliefs, Cues to action, Age of child, Education and Interview effect).
Model 3: Behavior = f (Health behavior identity, Attitudes toward behavior, Subjective norms, Cues to action, Perceived barrier, Intention, Perceived barriers * behavioral intention, Age of child, Education and Interview effect).
Overall, statistical tests were 2-tailed, and p-values < 0.10 were considered statistically significant. We used this P-value cut off due to the finite sample size of our study and because this study was prone to random errors (Thiese et al., 2016). All analyses were performed using IBM SPSS Statistics for Windows (Version 20.0. IBM Corp, 2011, Armonk, NY).
Results
Characteristics of the Study Participants
A total of 128 caregivers with a similar number of children participated in the study (Table 2). Majority of the school aged children included in the study were female (59.4%). The age of the children ranged from 6 to 12 years, with more than 60% in the age groups 7–8 years and 9–10 years. The majority of the respondents were married (82.0%). Only 40.7% of the caregivers had attained primary or secondary school education. The respondents were majorly from the Kaguru ethnic group (96.9%), the predominant tribe in Laikala. Agriculture and farming in particular were the predominant income generating occupation for most of the caregivers (89.1%). We then conducted preliminary analyses that investigated the associations between intention and behavior related to pearl millet consumption among the school aged children.
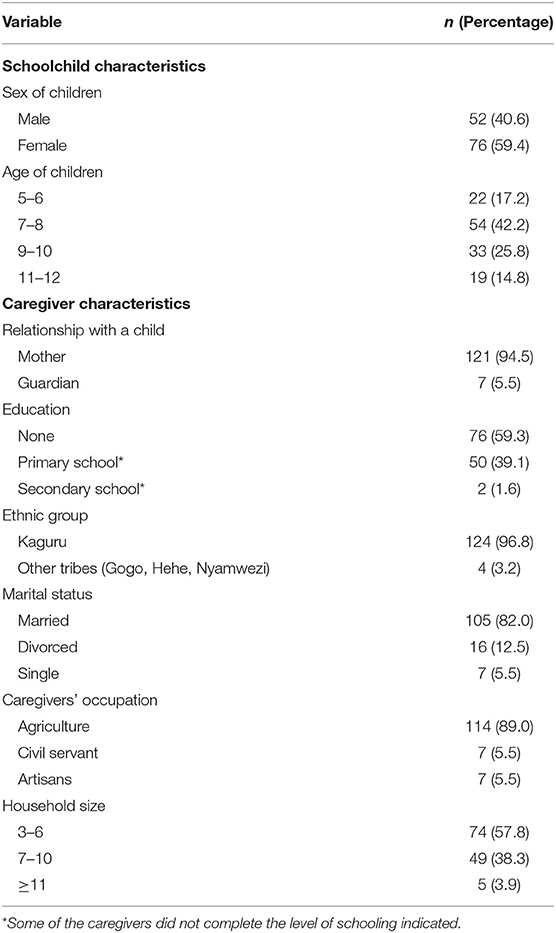
Table 2. Socio-demographic characteristics of school aged children and their caregivers in Kongwa (n = 128).
There Was a Significant Difference Between Intention and Behavior Among Those Who Did Not Consume Pearl Millet and Those Who Consumed Pearl Millet Two or More Times a Week in the Referent Month
There was significant difference between intention and behavior when consumption was two or more times per week (53.1 vs. 32.8; P = 0.001) or where there was no intention to or consumption taking place (30.5 vs. 13.3%; P = 0.003). No significant difference was observed between intention and behavior among respondents who were classified as consuming or intending to consume pearl millet four or less times per month (Figure 1). We further investigated knowledge, attitudes and perceptions of caregivers related to feeding pearl millet to SAC to elucidate internal factors influencing pearl millet consumption.

Figure 1. Comparison of pearl millet consumption between behavioral intention and behavior (n = 128). P-value obtained using chi-square test comparisons of per cent of intention and behavior. Significant difference between intention and behavior P ≤ 0.10.
Caregivers Have Low Knowledge on the Nutritional Content and Benefits of Pearl Millet Consumption
In assessing knowledge of the nutrient composition of pearl millet, 22.7 and 29.0% of caregivers were aware that pearl millet contained zinc and iron, respectively. In terms of their importance of zinc and iron in supporting growth, 25.8 and 34.3% of caregivers, respectively, were aware of this role (Table 3). Majority of respondents however perceived pearl millet as tasty (92.3%) and nutritious (82.9%) with significantly higher positive perception among high intenders compared to low intenders for taste and nutritive value (P = 0.044 and P = 0.01, respectively; Tables 3, 4). Interestingly, respondents attributed positive health outcomes to consumption of pearl millet despite not being aware of its micronutrient composition. In detail, majority agreed that pearl millet can improve intelligence (73.2%), health (82.9%) and survival (80.6%) of their children. When comparisons for high and low intenders were made, high intenders had significantly higher scores and therefore agreement on these benefits compared to low intenders (intelligence; P = 0.041, health; P = 0.005 and survival; P = 0.015).
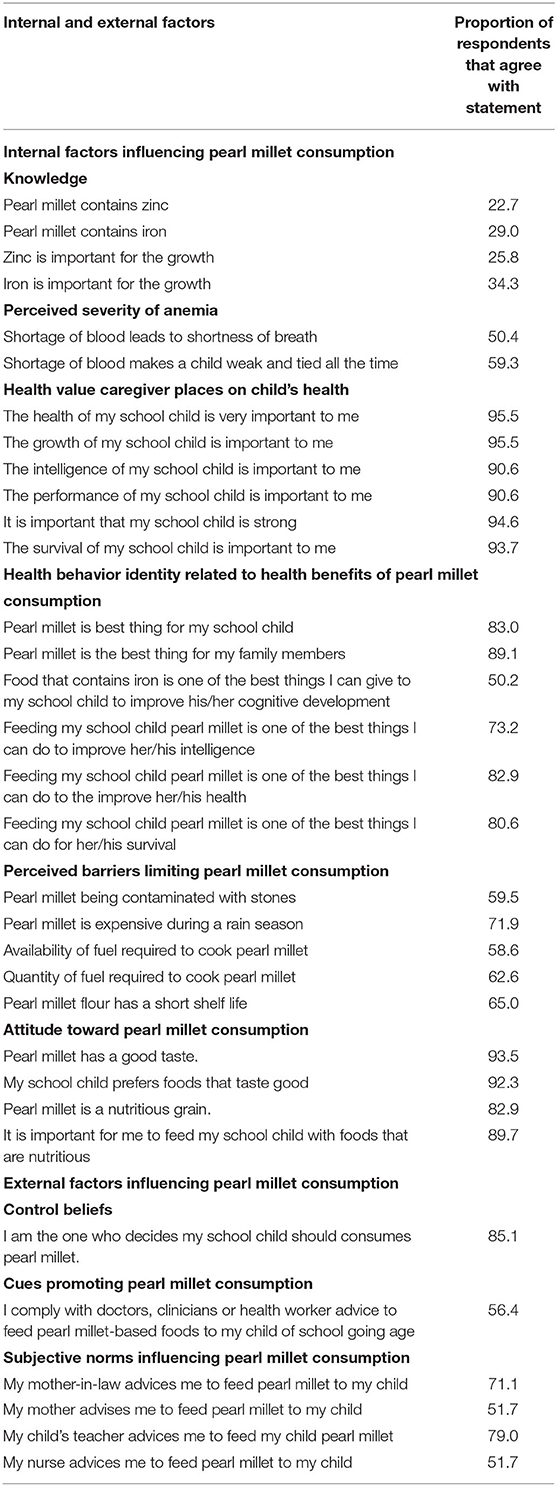
Table 3. Internal and external factors influencing pearl millet consumption.
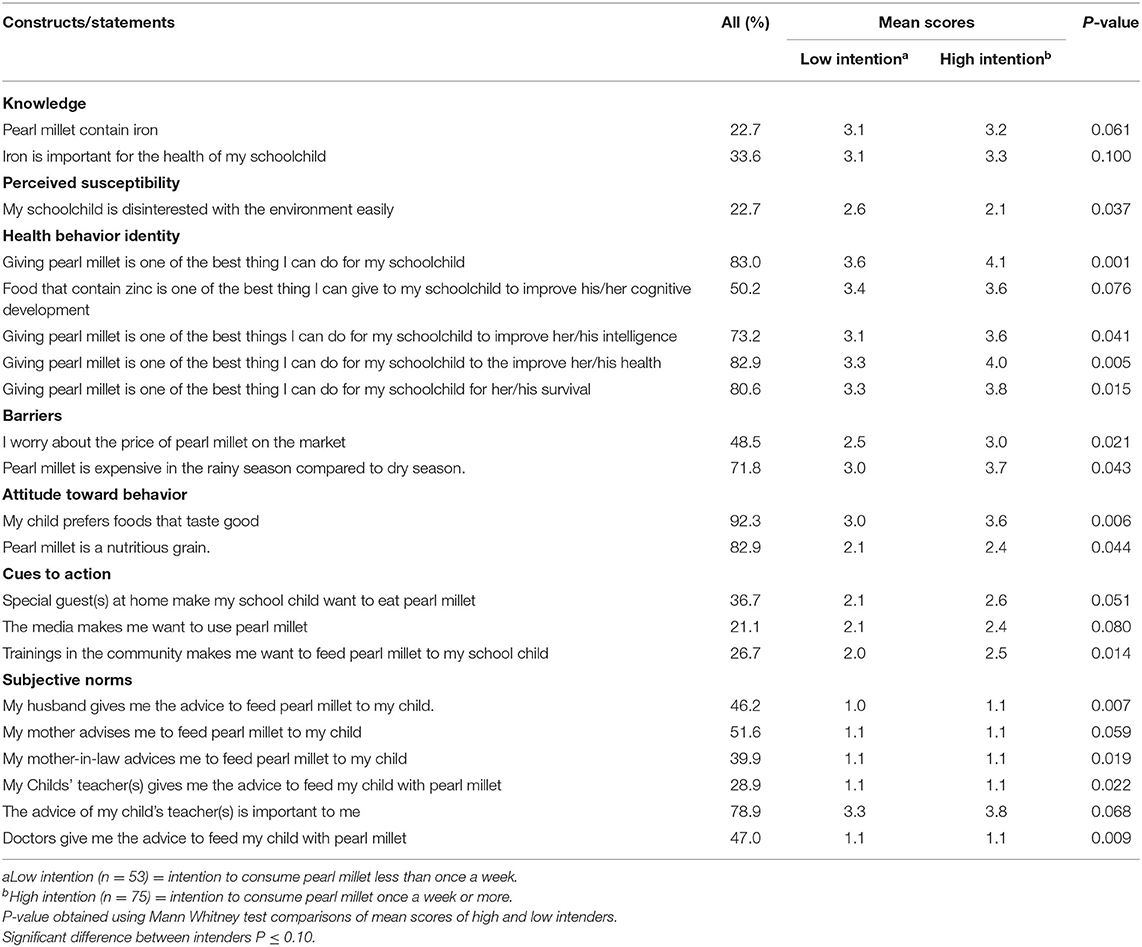
Table 4. Comparison between high and low intenders of pearl millet consumption.
Majority of Caregivers View Their Child's Health as Important but a Lower Proportion Connect Specific Health Outcomes of Their SAC to Consumption of Pearl Millet
Over 90% caregivers reported the health, growth, intelligence, school performance, strength and survival of their SAC as important to them, that is they placed a high health value on these attributes (Table 3). Interestingly, when we assessed the caregiver's evaluation of the effectiveness of giving pearl millet or iron rich food to the various health value attributes, the proportion of caregivers that agreed with the statements reduced. In fact when we particularly considered the relationship between consuming iron rich foods and cognition, the proportion of caregivers that agreed with this association was 50.2%. There was a higher appreciation for pearl millet consumption (P = 0.0001) and the role of iron rich foods in cognition (0.076), intelligence (P = 0.041), health (P = 0.005), and survival (P = 0.015) among SAC when high and low intenders were compared.
Various barriers limiting pearl millet consumption were identified though investigating attitudes toward pearl millet consumption by SAC as well as other perceived barriers by respondents.
Attitudes Toward Consumption of Pearl Millet Are Positive Though Price, Seasonality, Availability, and Quantity of Fuel Required for Pearl Millet Preparation Limit Consumption
Over 90% of respondents indicated that pearl millet had good taste (93.5%), is nutritious (82.9%) and that they valued feeding their children with nutritious foods (89.7%). High intenders had a more positive attitude toward the taste of pearl millet grain (P = 0.006) and it's nutrient value (P = 0.044) compared to low intenders. Respondents indicated several barriers to pearl millet consumption among school aged children. Majority of respondents (71.9%) indicated price increases during rainy seasons as a barrier to consumption. When analyses were stratified according to high and low intention groups, high intention groups worried more about the high price of pearl millet in general (P = 0.021) especially during the rainy season (P = 0.043; Table 4). Other barriers identified by majority of the respondents include: contamination with stones (59.5% quantity of fuel required for preparation (62.6%), short shelf life of pearl millet flour (65.0%; Table 3).
The Role of Mothers, Teachers, and Nurses Is Crucial in Promoting Increased Pearl Millet Consumption Among School Aged Children
Caregivers indicated that mothers-in-law (71.1%), mothers (51.6%), teachers (78.9%) and nurses (51.6%) were influential in their decision on whether to give pearl millet to their school aged children (Table 3). In addition, community trainings were viewed as important in positively influencing consumption of pearl millet in the high intention group compared to the low intention group (P = 0.014; Tables 3, 4).
To elucidate associations of individual constructs with intention, we assessed various constructs reliability as well as their correlations with each other and eventually with intention.
There Was High Reliability of the Multiple Constructs and Correlations Between Various Constructs Were Observed
Cronbach-α scores ranged from 0.7 to 0.8, which demonstrating a medium reliability for most of the constructs, median scores of the constructs ranged from 3 to 30 (Table 5). Median scores of health value, attitude toward behavior, control belief, subjective norms and intention constructs were high compared to the range values. This showed that caregivers tended to agree with the statements in those constructs. Low medians values were found for knowledge, susceptibility, severity, health behavior identity, barriers, cues to action and behavior construct when compared to their range scores. This indicated that most caregivers tended to disagree with the statements. Control belief, behavioral intention, and behavior constructs consisted of only one item each, and therefore their reliability analyses were not carried out.
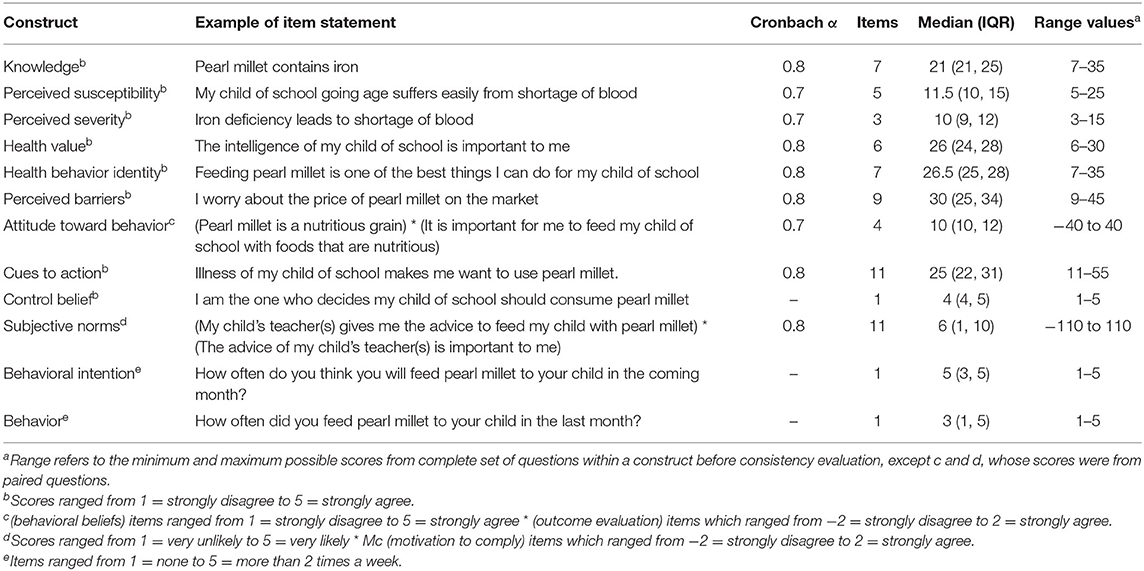
Table 5. Internal consistency and median scores of the constructs.
In investigating associations between constructs, knowledge was significantly and positively associated with health behavior identity (ρ = 0.58, P = 0.001). Within Beliefs and attitudes constructs, health behavior identity was significantly and positively correlated with attitude toward behavior (ρ = 0.46, P = 0.001) and behavioral intention (ρ = 0.31, P = 0.001). Finally, health behavior identity was significantly and positively correlated with intention (ρ = 0.31, P = 0.001, respectively). In investigating external factors associated with intention, subjective norms (ρ = 0.27, P = 0.002) and cues to action (ρ = 0.30, P = 0.001) were significantly and positively correlated with intention. A statistically significant positive correlation between intention and consumption of pearl millet among school aged children was observed (ρ = 0.44, P = 0.001, Figure 2 and Supplementary Table 1).

Figure 2. A combined model of the theory of planned behavior and health belief model with Spearman correlation coefficients between related constructs **P ≤ 0.01 and ***P ≤ 0.001 (2-tailed).
To identify a combination of factors that are associated with intention and behavior, regression analyses were utilized.
Intention Is a Significant Predictor of Pearl Millet Consumption Among School Aged Children
Model 1 had predictors as knowledge, perceived susceptibility, perceived severity, health value and the outcome as health behavior identity. The control variables included were age of child, interviewer effect and caregivers' education. Knowledge was a significant predictor of health behavior identity (β = 0.53, P = 0.001) with an increase in knowledge resulting in a more positive evaluation of the effectiveness of giving pearl millet or iron rich foods to reduce iron deficiency or anemia and zinc deficiency. Perceived susceptibility (P = 0.271), perceived severity (P = 0.342), health value (P = 0.291), age of child (P = 0.624), interviewer effect (P = 0.693) and caregivers' education (P = 0.532) were not significant predictors. This model explained 34% of the variance in health behavior identity.
Model 2 had both internal factors (perceived barriers, health behavior identity and attitudes toward behavior) and external factors (subjective norms, control beliefs and cues to action) as predictors of intention. Age of child, interviewer effect and caregivers' education were included as control factors. We observed that intention to give pearl millet to the SAC increased as the caregiver's evaluation of the effectiveness of giving pearl millet or iron rich food to reduce iron deficiency anemia and zinc deficiencies increased (Health behavior identity, β = 0.09, P = 0.021). Similarly, caregivers' attitude toward pearl millet consumption was also positive (Attitude toward behavior β = 0.17, P = 0.010) their intention to give pearl millet to the SAC increased. When considering the control variables, as the age of the SAC child (β = 0.39, P = 0.005) and caregivers' education (β = 0.48, P = 0.048) increased, so did the intention to give pearl millet. Interestingly, as the mother asserted more control on what the school aged child was fed (Control belief, β = −0.30, P = 0.041), the effort she was intending to make toward giving her child pearl millet (intention) decreased, indicating she was less likely to feed pearl millet to the SAC. This model explained 27% of the variation in intention to give pearl millet to the SAC.
Model 3 investigated predictors of pearl millet consumption among SAC. We observed that as the caregiver's evaluation of the effectiveness of giving pearl millet or iron rich food to reduce iron deficiency or anemia and zinc deficiencies became more positive (Health behavior identity, β = 0.08, P = 0.051) or the effort that the caregiver planned to make in. order to give pearl millet to their SAC increased (Intention, β = 0.87, P = 0.067) or the caregivers' education increased (Caregivers' education β = 0.74, P = 0.008), the SAC was more likely to be fed pearl millet. Attitude toward behavior, Control belief, Perceived barriers, age of child and interviewer effect were not significantly associated with giving pearl millet to the SAC (P > 0.10). The interaction term investigating how perceived barriers influence the association between intention and behavior was also not significant (Barriers*intention, β = −0.01, P = 0.409). This model explained 28% of the variation in pearl millet consumption among school aged children. Details of all models are provided in Table 6.

Table 6. Constructs associated with health behavior identity, intention to feed pearl millet to children of school going age and feeding pearl millet to school aged children.
Discussion
The study herein presents an investigation aimed at identifying factors influencing consumption of the nutrient dense cereal crop-pearl millet among school aged children. We observed that there was a significant difference between intention and behavior among the children who did not consume pearl millet (P = 0.003) and those who consumed millet two or more times a week (P = 0.013). Additionally, caregivers did not have adequate knowledge on the nutritional content and benefits of pearl millet consumption although the health of their school aged child was important to them. The barriers identified as limiting pearl millet consumption were price, seasonality, availability and quantity of fuel required for preparation. In terms of external factors, influencing consumption, the role of mothers, teachers and nurses was observed as crucial in promoting increased pearl millet consumption among school aged children. Using the combined TPB and HBM model we observed that knowledge significantly predicted health behavior identity (β = 0.60, P = 0.001) while health behavior identity significantly predicted intention (β = 0.09, P = 0.021). Intention of caregivers was significantly correlated (ρ = 0.44, P < 0.001) and predicted consumption of pearl millet (β = 0.87, P = 0.067).
Our current study is in concordance with several studies that have observed a positive relationship between caregiver knowledge, nutritional behavior and nutritional status (Zeng et al., 2012; Christian et al., 2016; Oly-Alawuba and Ihedioha, 2018; Oduor et al., 2019). Caregivers with improved knowledge and skills are more likely to ensure proper composition of foods. However, when passing on knowledge, subjective norms that are the social pressures the individual experiences to adopt or avoid the desired behavior should be considered. This could explain why we observed that when the caregivers assertion of giving pearl millet increased, the likelihood that the SAC consumed pearl millet decreased. It may be possible that other reinforcing actors are crucial. For example, we observed that the role of female grandparents, teachers and nurses is crucial in promoting increased pearl millet consumption among school aged children. The impact of grandparental caregiving on child feeding becomes more direct and influential as their caregiving role with grandchildren increases. Previous research has shown that parent attitudes, beliefs and feeding practices have a significant influence on child dietary intake and weight status (Contento et al., 1993; Appoh and Krekling, 2005; Burchi, 2010; Fadare et al., 2019a,b). As grandparents take responsible roles in the lives of their grandchildren, it can be assumed that their attitudes, beliefs and feeding practices may have a similarly significant impact on child dietary intake and weight status as those of parents. This is additionally important in cultures where the role of grandparents in the family is valued and respected. While a large number of studies have examined the influence of various familial factors on child dietary intake or weight status, the vast majority of these have focused primarily on parents and on pre-school children. There is however now growing evidence to suggest that grandparents play an increasingly important role in influencing their grandchildren's feeding practices (Mukuria et al., 2016; Negin et al., 2016; Karmacharya et al., 2017; Young et al., 2018). Many of these studies observe that grandparents are important in influencing the diets of pre-school children. More studies are however required to investigate whether the grandparents influence on diets and nutrition statue extends beyond early childhood. That notwithstanding, our results buttress the observation that for a successful nutrition behavior change program in Kongwa, the role of female grandparents would have to be factored into interventions. Such an approach could involve nurses, who were also observed to be influential in our study. Indeed, a study on the role of nurses in Sub Saharan Africa has observed that they are often required to provide health education to the communities in which they serve (Ugochukwu et al., 2013). Expanding actors involved in disseminating nutrition knowledge is crucial especially because it has previously been observed that there is low coverage of nutrition education in Central Tanzania (Bundala et al., 2020). For nurses' involvement to be effective, they need to be trained to give in-depth nutrition education, a skill they often lack (DiMaria-Ghalili et al., 2014). For example, a study by Davis et al. (2017) among Ghanian nurses reported a lack of in-depth nutrition knowledge and young child feeding (YCF) education as a barrier to effective nutrition education. Perhaps incorporating other influential actors may also make up for this gap in nutrition education. Teachers also have an important role as health promoters (Pickett et al., 2015). It is important that it is however noted that a successful nutrition education program involving teachers also depends on their training and following of a standardized protocol to ensure fidelity (Murimi et al., 2018). Other factors that have been observed to be vital for success of a nutrition education program include an intervention period of at least 6 months and use of age-appropriate activities (Murimi et al., 2018). Based on these observations, Agriculture for nutrition programs that seek to promote pearl millet consumption therefore need to have a multi actor approach that are age appropriate, be of adequate duration and ensure fidelity and proper alignment between the stated objectives, the intervention, and the desired outcomes to ensure success. In addition, such program should include the use of appropriate media channels to encourage utilization. In our study, we did observe that respondents mentioned that the media had a positive effect on their consumption of pigeon pea.
It is important to take into account that though nutrition knowledge is necessary, it may not be a sufficient factor for changes in food consumption. Education interventions, which are expected to be effective in influencing dietary behaviors or choice, need to consider external influencing factors as well. For example, respondents in our study identified price, seasonality, availability and quantity of fuel required for pearl millet preparation as barriers to consumption, which interestingly has been observed in India too (Amarender Reddy et al., 2013; Singh et al., 2018). A previous study conducted in Tanzania indicates that virtually all of the pearl millet production is carried out on a subsistence basis (Rohrbach and Kiriwaggulu, 2001). In fact, <2% of the harvest is available in the formal market; with the bulk of the harvest consumed by farm households. These limited quantities of grain traded may explain the issues of seasonality, availability and price experienced by our respondents. As various programs begin to promote consumption of pearl millet, the production and functionality of the entire pearl millet grain value chain will need to be simultaneously improved to meet the growing demand and ensure affordability.
Our results confirm the mediating role of health behavior identity between background and perception constructs and intention in the combined TPB and HBM model. This indicates that the knowledge of caregivers about pearl millet together with the health values they hold for pearl millet consumption by their children resulted in a positive health behavior identity. This positive health behavior identity influenced attitude to feeding pearl millet to school aged children positively that subsequently predicted intention of caregivers to give pearl millet to their children. For programs and efforts to promote pearl millet consumption, it is imperative that pearl millet should be promoted as a nutrient dense crop to combat iron and zinc deficiency among school aged children since this what caregivers value.
Intention was utilized in our study as a predictor of previous behavior, which in turn is a surrogate for future behavior. We observed that though the internal reliability of our constructs was good, our model had low predictive ability. Three other studies in Africa that have utilized these predictive models have shown similar trends in low predictive abilities of models on intention (Fanou-Fogny et al., 2011; Macharia-Mutie et al., 2011; Abizari et al., 2013). The fact that pearl millet is consumed in combination with maize flour may explain the low contribution of the constructs to the prediction of intention in this study. Since the TPB requires participants to describe their cognitions, this requirement is based on the assumption that the answers given will reveal pre-existing states of mind (Armitage and Conner, 2001). Thus, if the behavior investigated is uncommon, in this case consumption of pearl millet alone, it is possible that the cognitions may be created simply by completing a questionnaire (Ogden, 2003). We sought to reduce the effect of unfamiliarity by setting certain requirements for participation such as, knowing and having consumed pearl millet. However, though majority of the respondents had consumed pearl millet in the past, they had not consumed it regularly and had consumed it as a blend with maize flour. Predictive ability may have been improved if reference to a specific food was made.
In summary, though pearl millet consumption presents a viable option to combat iron and zinc deficiency several considerations need to be made. Firstly, increasing awareness about iron and zinc deficiencies and nutritional benefits of pearl millet as well as health consequences of consuming pearl millet (health behavior identity) such as pearl millet improves cognitive development, intelligence, health and survival should be targeted. In addition, value chain factors such as price, seasonality and availability that present barriers should be addressed. For example, programs aiming to increase pearl millet consumption should not only invest in its increased production but also on new technologies, including processing machines, packaging and storage to influence growth of local markets. These strategies may not only promote pearl millet consumption among school aged children at household level but also at scale in school feeding programs.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available upon approval by the funder.
Ethics Statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
MC: questionnaire validation and administration, data analyses, interpretation of results, visualization, writing—original draft, and writing final draft—review and editing. HMu: data analyses, interpretation of results, visualization, writing—original draft, and writing final draft—review and editing. RM, YM, NK, JM, and HMs: questionnaire development and validation, administration, and review of final draft. MB and PO: supervision and review of final draft. WG-W: project administration, conceptualization, methodology, interpretation of results, visualization, writing—original draft, writing—review and editing, and supervision. All authors contributed to the article and approved the submitted version.
Funding
This research publication was made possible with support from the United States Agency for International Development (USAID) through the Africa Research in Sustainable Intensification for the Next Generation (Africa RISING) program as part of the US Government's Feed the Future Initiative. The funders had no role in the design and/or implementation of the study or the preparation of the manuscript thereof.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors wish to thank the administrative and local authorities as well as all caregivers/respondents from Laikala village that participated in the study. The support of Mr. Peter Ngowi in identifying potential respondents for the survey is appreciated. Additionally, we thank the interviewers for their work in the field. Furthermore, we are grateful to Tanzania Agricultural Research Institute (TARI) Hombolo for all the logistical support. The Authors also acknowledge various contributions by the International Institute for Tropical Agriculture (IITA).
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fsufs.2021.694160/full#supplementary-material
References
Abizari, A. R., Pilime, N., Armar-Klemesu, M., and Brouwer, I. D. (2013). Brouwer. Cowpeas in Northern Ghana and the factors that predict caregivers' intention to give them to schoolchildren. PLoS ONE 8:e72087. doi: 10.1371/journal.pone.0072087
Africa RISING. (2021). Africa Research in Sustainable Intensification for the Next Generation. Africa RISING. Available online at: https://africa-rising.net/ (accessed January 4, 2021).
Agte, V. V., Khot, S., Girigosavi, S. T., Paknikar, K. M., and Chiplonkar, S. A. (1999). Comparative performance of pearl millet- and sorghum- based diets vs. wheat- and rice-based diets for trace metal bioavailability. J. Trace Elements Med. Biol. 13, 215–219. doi: 10.1016/S0946-672X(99)80038-8
Amarender Reddy, A., Dharm Pal Malik, O. Y., Singh, I. P., Ardeshna, N. J., Kundu K. K Gupta, S. K., et al. (2013). Utilization pattern, demand and supply of pearl millet grain and fodder in Western India. Working Paper Series no. 37. Patancheruvu: International Crops Research Institute for the Semi Arid Tropics, 24. Available online at: http://oar.icrisat.org/6694/1/WPS_37_MIP.pdf
Appoh, L. Y., and Krekling, S. (2005). Maternal nutritional knowledge and child nutritional status in the Volta region of Ghana. Matern. Child Nutr. 1, 100–110. doi: 10.1111/j.1740-8709.2005.00016.x
Armitage, C. J., and Conner, M. (2001). Efficacy of the theory of planned behaviour: a meta-analytic review. Br. J. Soc. Psychol. 40, 471–499. doi: 10.1348/014466601164939
Bouis, H. E. (2002). Plant breeding: a new tool for fighting micronutrient malnutrition. J. Nutr. 132, 491S−4S. doi: 10.1093/jn/132.3.491S
Brown, K. H., Rivera, J. A., Bhutta, Z., Gibson, R. S., King, J. C., Lönnerdal, B., et al. (2004). International Zinc Nutrition Consultative Group (IZiNCG) technical document #1. Assessment of the risk of zinc deficiency in populations and options for its control. Food Nutr. Bull. 25, S99–203.
Bundala, N., Kinabo, J., Jumbe, T., Bonatti, M., Rybak, C., and Sieber, S. (2020). Gaps in knowledge and practice on dietary consumption among rural farming households; a call for nutrition education training in Tanzania. Int. J. Food Sci. Nutr. 71, 341–351. doi: 10.1080/09637486.2019.1655533
Burchi, F. (2010). Child nutrition in Mozambique in 2003: the role of mother's schooling and nutrition knowledge. Econ. Hum. Biol. 8, 331–345. doi: 10.1016/j.ehb.2010.05.010
Butrimovitz, G. P., and Purdy, W. C. (1978). Zinc nutrition and growth in a childhood population. Am. J. Clin. Nutr. 31, 1409–1412. doi: 10.1093/ajcn/31.8.1409
Cavan, K. R., Gibson, R. S., Grazioso, C. F., Isalgue, A. M., Ruz, M., and Solomons, N. W. (1993). Growth and body composition of periurban Guatemalan children in relation to zinc status: a longitudinal zinc intervention trial. Am. J. Clin. Nutr. 57, 344–352. doi: 10.1093/ajcn/57.3.344
Christian, A. K., Marquis, G. S., Colecraft, E. K., Lartey, A., Sakyi-Dawson, O., Ahunu, B. K., et al. (2016). Caregivers' nutrition knowledge and attitudes are associated with household food diversity and children's animal source food intake across different agro-ecological zones in Ghana. Br. J. Nutr. 115, 351–360. doi: 10.1017/S0007114515004468
Contento, I. R., Basch, C., Shea, S., Gutin, B., Zybert, P., Michela, J. L., et al. (1993). Relationship of mothers' food choice criteria to food intake of preschool children: identification of family subgroups. Health Educ. Q. 20, 243–259. doi: 10.1177/109019819302000215
Davis, J. N., Brown, H., and Ramsay, S. A. (2017). Gaps in international nutrition and child feeding guidelines: a look at the nutrition and young child feeding education of Ghanaian nurses. Public Health Nutr. 20, 2215–2224. doi: 10.1017/S1368980017000908
DiMaria-Ghalili, R. A., Mirtallo, J. M., Tobin, B. W., Hark, L., Van Horn, L., and Palmer, C. A. (2014). Challenges and opportunities for nutrition education and training in the health care professions: intraprofessional and interprofessional call to action. Am. J. Clin. Nutr. 99, 1184S−1193S. doi: 10.3945/ajcn.113.073536
Emerson, R. W. (2017). Likert scales. J. Vis. Impair. Blindness 111:488. doi: 10.1177/0145482X1711100511
Fadare, O., Amare, M., Mavrotas, G., Akerele, D., and Ogunniyi, A. (2019a). Correction: mother's nutrition-related knowledge and child nutrition outcomes: empirical evidence from Nigeria. PLoS ONE 14:e0215110. doi: 10.1371/journal.pone.0215110
Fadare, O., Amare, M., Mavrotas, G., Akerele, D., and Ogunniyi, A. (2019b). Mother's nutrition-related knowledge and child nutrition outcomes: empirical evidence from Nigeria. PLoS ONE 14:e0212775. doi: 10.1371/journal.pone.0212775
Fanou-Fogny, N., van Dam, B., Koreissi, Y., Dossa, R. A., and Brouwer, I. D. (2011). Factors predicting consumption of fonio grain (Digitaria exilis) among urban Malian women of reproductive age. J. Nutr. Educ. Behav. 43, 219–228. doi: 10.1016/j.jneb.2010.03.008
Field, A. (2005). Discovering Statistics Using SPSS. 2nd ed. London, United Kingdom: SAGE Publications.
Francis, J., Eccles, M. P., Johnston, M., Walker, A. E., Grimshaw, J. M., Foy, R., et al. (2004). Constructing Questionnaires Based on the Theory of Planned Behaviour: A Manual for Health Services Researchers. N: Newcastle: Centre for Health Services Research, University of Newcastle, UK.
Grantham-McGregor, S., and Ani, C. (2001). A review of studies on the effect of iron deficiency on cognitive development in children. J. Nutr. 131, 649S−666S. doi: 10.1093/jn/131.2.649S
Hall, A., Bobrow, E., Brooker, S., Jukes, M., Nokes, K., Lambo, J., et al. (2001). Anaemia in schoolchildren in eight countries in Africa and Asia. Public Health Nutr. 4, 749–756. doi: 10.1079/PHN2000111
Jukanti, A. K., Gowda, C. L., Rai, K. N., Manga, V. K., and Bhatt, R. K. (2016). Bhatt Crops that feed the world 11. Pearl Millet (Pennisetum glaucum L.): an important source of food security, nutrition and health in the arid and semi-arid tropics. Food Secur. 8, 307–329. doi: 10.1007/s12571-016-0557-y
Kanatti, A., Rai, K. N., Radhika, K., Govindaraj, M., Sahrawat, K. L., and Rao, A. S. (2014). Grain iron and zinc density in pearl millet: combining ability, heterosis and association with grain yield and grain size. SpringerPlus 3:763. doi: 10.1186/2193-1801-3-763
Karadimitriou, S. M., Marshall, E., and Knox, C. (2018). Mann Whitney U-test. Sheffield: Sheffield Hallam University.
Karmacharya, C., Cunningham, K., Choufani, J., and Kadiyala, S. (2017). Grandmothers' knowledge positively influences maternal knowledge and infant and young child feeding practices. Public Health Nutr. 20, 2114–2123. doi: 10.1017/S1368980017000969
Kodkany, B. S., Bellad, R. M., Mahantshetti, N. S., Westcott, J. E., Krebs, N. F., Kemp, J. F., et al. (2013). Biofortification of pearl millet with iron and zinc in a randomized controlled trial increases absorption of these minerals above physiologic requirements in young children. J. Nutr. 143, 1489–1493. doi: 10.3945/jn.113.176677
Lopez, A., Cacoub, P., Macdougall, I. C., and Peyrin-Biroulet, L. (2016). Iron deficiency anaemia. Lancet 387, 907–916. doi: 10.1016/S0140-6736(15)60865-0
Macharia-Mutie, C. W., Van de Wiel, A. M., Moreno-Londono, A. M., Mwangi, A. M., and Brouwer, I. D. (2011). Sensory acceptability and factors predicting the consumption of grain amaranth in Kenya. Ecol. Food Nutr. 50, 375–392. doi: 10.1080/03670244.2011.604584
Mukuria, A. G., Martin, S. L., Egondi, T., Bingham, A., and Thuita, F. M. (2016). Role of social support in improving infant feeding practices in Western Kenya: a quasi-experimental study. Glob. Health Sci. Pract. 4, 55–72. doi: 10.9745/GHSP-D-15-00197
Murimi, M. W., Moyeda-Carabaza, A. F., Nguyen, B., Saha, S., Amin, R., and Njike, V. (2018). Factors that contribute to effective nutrition education interventions in children: a systematic review. Nutr. Rev. 76, 553–580. doi: 10.1093/nutrit/nuy020
NBS (2013). 2012 Population and Housing Census: Population Distribution by Administrative Areas. Dare es Salaam and Office of Chief Government Statistician President's Office, Zanzibar, United Republic of Tanzania.
Negin, J., Coffman, J., Vizintin, P., and Raynes-Greenow, C. (2016). The influence of grandmothers on breastfeeding rates: a systematic review. BMC Pregnancy Childbirth 16:91. doi: 10.1186/s12884-016-0880-5
Nestel, P., Bouis, H. E., Meenakshi, J. V., and Pfeiffer, W. (2006). Biofortification of staple food crops. J. Nutr. 136, 1064–1067. doi: 10.1093/jn/136.4.1064
Oduor, F. O., Boedecker, J., Kennedy, G., Mituki-Mungiria, D., and Termote, C. (2019). Caregivers' nutritional knowledge and attitudes mediate seasonal shifts in children's diets. Matern. Child Nutr. 15:e12633. doi: 10.1111/mcn.12633
Ogden, J. (2003). Some problems with social cognition models: a pragmatic and conceptual analysis. Health Psychol. 22, 424–428. doi: 10.1037/0278-6133.22.4.424
Oly-Alawuba, N. M. A., and Ihedioha, S. (2018). Nutritional knowledge of mothers/caregivers in relation to the anthropometric indices of children(2–5 years) in Obowu Local Government Area, Imo State, Nigeria. FASEB J. 31, 957–913. doi: 10.1096/fasebj.31.1_supplement.957.13
Pickett, K., Byrne, J., Rietdijk, W., Shepherd, J., Roderick, P., and Grace, M. (2015). Teachers as health promoters: a longitudinal study of the effect of a health education curriculum for trainee teachers on their practice in schools. Lancet. 386:S63. doi: 10.1016/S0140-6736(15)00901-0
Rao, P. P., Birthal, P. S., Reddy, B. V. S., Rai, K. N., and Ramesh, S. (2006). Diagnostics of sorghum and pearl millet grains-based nutrition in India. Int. Sorghum Millets Newslett. 47, 93–96.
Rohrbach, D. D., and Kiriwaggulu, J. A. B. (2001). Commercialization prospects for Sorghum and Pearl Millet in Tanzania. SAT e J. 3, 1–28.
Rohrbach, D. D., and Kiriwaggulu, J. A. B. (2007). Commercialization prospects for Sorghum and Pearl Millet in Tanzania. ICRISAT e J. 3, 1–28.
Schober, P., Boer, C., and Schwarte, L. A. (2018). Correlation coefficients: appropriate use and interpretation. Anesth. Analg. 126, 1763–1768. doi: 10.1213/ANE.0000000000002864
Singh, N., Singh, S. P., Kumar, M., Kanhiya, K., and Kumar, A. (2018). Nutri cereal pearlmillet: way forward. Int. J. Curr. Microbiol. Appl. Sci. 7, 578–581. doi: 10.20546/ijcmas.2018.706.066
Sun, X., Guo, Y., Wang, S., and Sun, J. (2006). Predicting iron-fortified soy sauce consumption intention: application of the theory of planned behavior and health belief model. J. Nutr. Educ. Behav. 38, 276–285. doi: 10.1016/j.jneb.2006.04.144
Talsma, E. F., Melse-Boonstra, A., de Kok, B. P., Mbera, G. N., Mwangi, A. M., and Brouwer, I. D. (2013). Biofortified cassava with pro-vitamin A is sensory and culturally acceptable for consumption by primary school children in Kenya. PLoS ONE 8:e73433. doi: 10.1371/journal.pone.0073433
Thiese, M. S., Ronna, B., and Ott, U. (2016). P value interpretations and considerations. J. Thorac. Dis. 8, E928–E931. doi: 10.21037/jtd.2016.08.16
Ugochukwu, C. G., Uys, L. R., Karani, A. K., Okoronkwo, I. L., and Diop, B. N. (2013). Roles of nurses in Sub-Saharan African region. Int. J. Nurs. Midwifery 5, 117–131. doi: 10.5897/IJNM2013.0104
Wei, W., Erenrich, J., and Selman, B. (2004). Towards Efficient Sampling: Exploiting Random Walk Strategies. Ithaca, NY: Department of Computer Science, Cornell University.
Wessells, K. R., Singh, G. M., and Brown, K. H. (2012). Estimating the global prevalence of inadequate zinc intake from national food balance sheets: effects of methodological assumptions. PLoS ONE 7:e50565. doi: 10.1371/journal.pone.0050565
Young, K. G., Duncanson, K., and Burrows, T. (2018). Tracy burrows influence of grandparents on the dietary intake of their 2-12-year-old grandchildren: a systematic review. Nutr. Dietetics 75, 291–306. doi: 10.1111/1747-0080.12411
Zeng, R., Luo, J. Y., Tan, C., Du, Q. Y., Zhang, W. M., and Li, Y. (2012). Relationship between caregivers' nutritional knowledge and children's dietary behavior in Chinese rural areas. J. Cent. South Univ. 37, 1097–1103. doi: 10.3969/j.issn.1672-7347.2012.11.003
Keywords: pearl millet, theory of planned behavior, health belief model, drivers of food choice, school aged children and Tanzania
Citation: Chande M, Muhimbula H, Mremi R, Muzanila YC, Kumwenda NC, Msuya J, Msere H, Bekunda M, Okori P and Gichohi-Wainaina WN (2021) Drivers of Millet Consumption Among School Aged Children in Central Tanzania. Front. Sustain. Food Syst. 5:694160. doi: 10.3389/fsufs.2021.694160
Received: 12 April 2021; Accepted: 28 June 2021;
Published: 06 August 2021.
Edited by:
Taku Tsusaka, Ostrom, ThailandReviewed by:
Daniela Spina, University of Catania, ItalyGiulia Maesano, University of Catania, Italy
Copyright © 2021 Chande, Muhimbula, Mremi, Muzanila, Kumwenda, Msuya, Msere, Bekunda, Okori and Gichohi-Wainaina. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wanjiku N. Gichohi-Wainaina, d25naWNob2hpQGdtYWlsLmNvbQ==; dy5naWNob2hpQGNnaWFyLm9yZw==