 Dominik Fugmann
Dominik Fugmann- 1Medical Faculty, Clinical Institute of Psychosomatic Medicine and Psychotherapy, Heinrich-Heine-University-Düsseldorf, Düsseldorf, Germany
- 2University Medical Center Rechts der Isar, School of Medicine, Institute of Artificial Intelligence and Informatics in Medicine, Technical University of Munich, Munich, Germany
- 3Department of Medical Psychology, Radboud Institute of Health Sciences, Radboud University Medical Centre, Nijmegen, Netherlands
Introduction: Research on the impact of cancer on close relationships brings up conflicting results. This systematic review collects empirical evidence on the research questions whether a cancer diagnosis in general or the type of cancer affects the divorce rate.
Materials and Methods: This systematic review was conducted according to the guidelines of the Cochrane Collaboration and the PRISMA statement. The following electronic databases were searched: Web of Science, Ovid SP MEDLINE, PsycINFO, PsyINDEX, CINAHL, ERIC. Risk of bias assessment was performed with the preliminary risk of bias for exposures tool template (ROBINS-E tool). The grading of methodological quality was assessed with the Newcastle-Ottawa Scale.
Results: Of 13,929 identified records, 15 were included in the qualitative synthesis. In 263,616 cancer patients and 3.4 million healthy individuals, we found that cancer is associated with a slightly decreased divorce rate, except for cervical cancer, which seems to be associated with an increased divorce rate.
Discussion: According to this systematic review, cancer is associated with a tendency to a slightly decreased divorce rate. However, most of the included studies have methodologic weaknesses and an increased risk of bias. Further studies are needed.
Background
Divorce is a common occurrence around the world, with significant differences between countries. In 2019 there were 1.8 divorces in 1,000 residents in Germany (USA 2019: 2.7 divorces in 1,000 residents) (Centers for Disease Control and Prevention [CDC], 2021; Destatis Statistisches Bundesamt, 2021). A divorce can have harmful consequences: in addition to social and economic impacts, health can also be impaired (Amato, 2000; Sbarra et al., 2011; Sbarra, 2015; Leopold, 2018). A subgroup of divorced people shows significantly increased mortality as a result (Sbarra, 2015). For cancer patients, social and emotional support from close relationships are among the most protective factors (Aizer et al., 2013). In view of 18.1 million cancer diagnoses per year and an increasing tendency worldwide (International Agency for Research on Cancer [IARC], 2020), an effect of cancer on the divorce rate would be of considerable relevance.
Cancer leads to distress in patients but also in their partners in dyadic relationships (Hodges et al., 2005; Hagedoorn et al., 2008). In literature there is evidence that distress increases within one year after diagnosis (Sjövall et al., 2009). The long-term effects of cancer on relationships are less clear (Manne and Badr, 2008; Regan et al., 2012). Furthermore, it is uncertain if there are detrimental effects on the quality of the relationship that can lead to a divorce due to a failure to cope. The literature is inconsistent in this regard: on the one hand, some studies report no higher risk of divorce after a cancer diagnosis of one spouse (Dorval et al., 1999; Joly et al., 2002; Carlsen et al., 2007). On the other hand, some studies provide evidence of a higher risk of divorce after a cancer diagnosis (Kirchhoff et al., 2012; Song et al., 2014).
In addition to known factors such as age at marriage or number of children (Heaton, 1990), the type of cancer could also have an influence on the risk of divorce. In a cohort study, 46,303 patients from the Danish cancer registry were compared to 221,028 matched patients from a Danish administrative registry: A higher divorce rate was only found in patients with cervical cancer (Carlsen et al., 2007). Keeping in mind that interdisciplinary cancer treatment is now organized in cancer type-specific centers, interventions that target unmet needs like maintaining the partnership could be easily implemented in clinical pathways. Targeted support in maintaining the partnership could be provided by all healthcare professionals in oncology, ranging from the provision of information to interventions to improve the quality of the relationship.
This systematic review collects empirical evidence on the research questions whether cancer in general or specific cancer types have an effect on the divorce rate.
In the literature a wide range of definitions of “marriage” and “divorce” can be found. Sometimes the category “divorced” includes both separated and divorced patients (Karraker and Latham, 2015), sometimes cohabitating couples are declared as married and moving into separate places of residence is declared a divorce (Carlsen et al., 2007; Dinh et al., 2018). Yet cohabitating couples separate more often than married couples (Bouchard, 2006). Accordingly, a systematic investigation of divorces following a cancer diagnosis could entail the risk of confounding because the groups compared can be composed differently, so that in the present systematic review only legally married couples and official divorces are considered in order to maximize internal validity.
Materials and Methods
This systematic review was conducted following a protocol that was developed according to the guidelines of the Cochrane Collaboration and the PRISMA statement (Higgins and Green, 2011; Moher et al., 2015).
Objectives, Definitions, Inclusion, and Exclusion Criteria
The primary objective of this systematic review was to collect evidence in as a complete manner as possible, and to extract and synthesis it for changes in the divorce rate after a cancer diagnosis. The secondary objective was analyzing the collected evidence to determine whether diagnoses of different cancer types are associated with changes in the divorce rate.
In terms of the evidence, we only considered married couples for the review, which were defined as a couple relationship between two adults (aged ≥ 18 years), regardless of gender, who are officially married. We included cancer patients with solid or non-solid tumors of all organ systems, who were diagnosed during marriage. A diagnosis prior to marriage did not qualify for our review and such data was excluded. Healthy subjects or those with different types of cancer were studied as a comparison group while comparison groups with diseases other than cancer were excluded. The outcome examined in this review is the divorce rate. A divorce was defined as a certified separation of a former married couple. Studies which included the defined outcome but which were not necessarily restricted to this outcome were included: experimental and/or observational studies, randomized and non-randomized studies, prospective or retrospective cohort studies and descriptive studies. The following study types were excluded: qualitative studies, studies not presenting an outcome including commentaries, letters and editorials, studies not publicized in full-text and not-obtainable in full-text, studies only presenting marital status data within 6 months of the cancer diagnosis.
Search Strategy and Sources
A search strategy was developed to perform a wide search. Before the final search was performed, the Web of Science search strategy was reviewed by a PhD-level information scientist using PRESS: Peer review of Search Strategies model (McGowan et al., 2016).
A MESH term search while testing the search strategy did not yield any additional hits, so it was removed in the final search strategy. The search terms used are listed in Supplementary Material.
To ensure the relevance of the data, only studies released later than 1999 were considered. Only publications in English or German were considered due to the language abilities of the authors.
The following electronic databases were searched on 1st April 2020, a search update was carried out on 3rd June 2021. All studies were retrieved based on that search.
- Web of Science (Web of Science Core Collection, BIOSIS Citation Index, BIOSIS Previews, Current Contents Connect, Data Citation Index, Derwent Innovations Index, KCI-Korean Journal Database, MEDLINE, Russian Science Citation Index, SciELO Citation Index, Zoological Record)
- Ovid SP MEDLINE
- APA PsycINFO
- PsyINDEX
- CINAHL
- ERIC.
A complete sample search in Web of Science can be found in Supplementary Material.
To complete the search the following procedures were performed (hand search and cited-reference searches):
Reviewing the reference lists of the included publications, contacting experts in the examined field of psycho-oncology to gather information about other publications or not-yet published works (i.e., doctoral theses), performing a search for trial- and review registries, performing a citation search in Web of Science to find publications citing the publications included in the review and searching the local library catalog (Heinrich-Heine University Düsseldorf) for further publications.
Study Selection Criteria and Study Selection
Two authors (DF, SH or NS) independently categorized all discovered publications by title and abstract screening to determine whether these were to be included in, or excluded from, the review. If the classification remained unclear after abstract screening or the judgment was not unanimous, the full-text was obtained for a consensus-based decision of the two authors. All publications included at this point were obtained in full-text and reviewed by two authors (DF, SH or NS). Inclusion or exclusion of every publication was discussed by these authors. If no consensus could be achieved the publication in question was reviewed by another author (AK) who decided on inclusion and exclusion. We tracked all results in a Citavi Database (Citavi 6.3 2018). The selection process was recorded to create a PRISMA flow diagram (Figure 1).
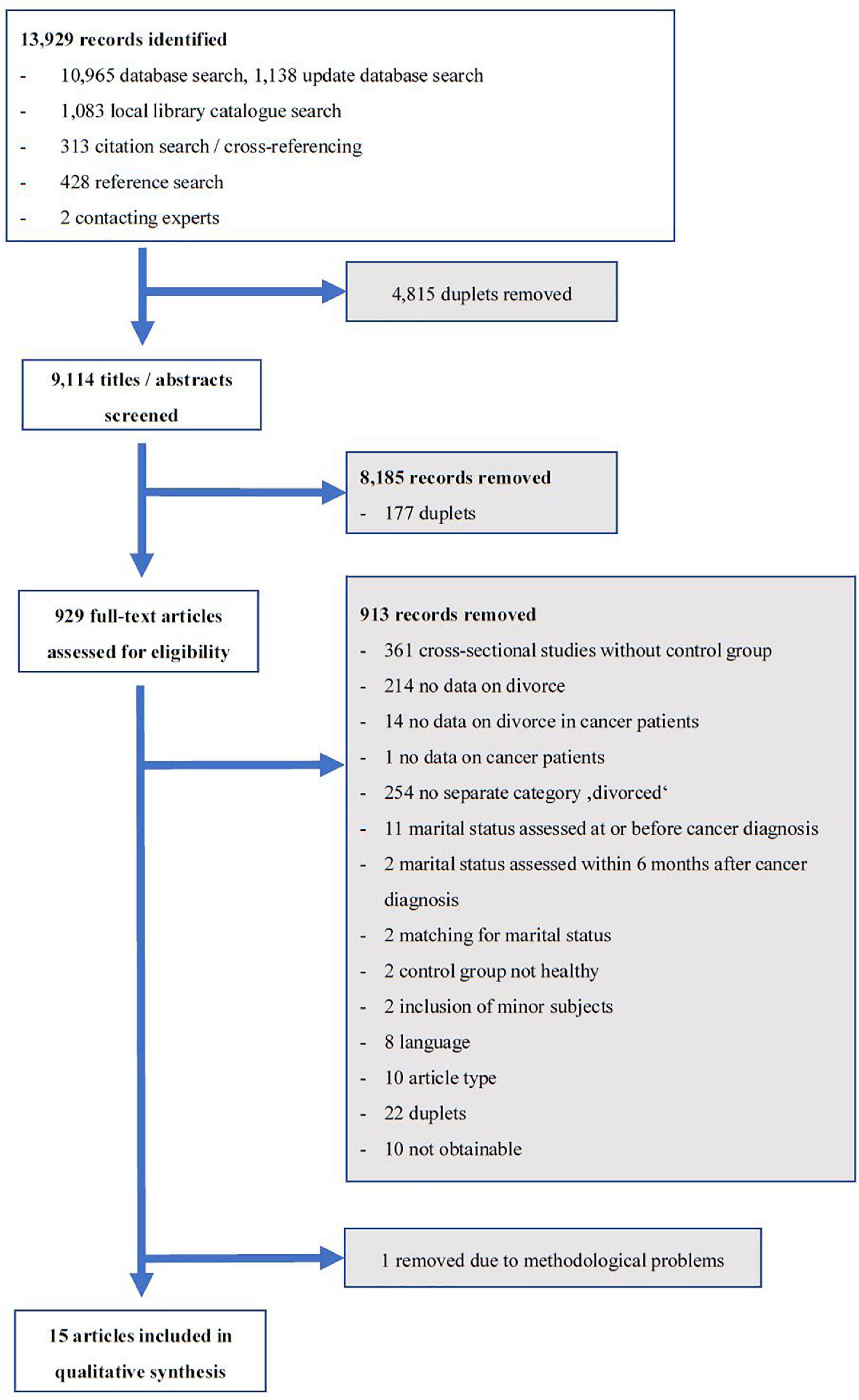
Figure 1. PRISMA flow chart.
Data Extraction Procedures
All publications remaining after this procedure were independently registered in a standardized data extraction form by two authors (DF, SH, or NS). Discrepancies were discussed by at least two authors to reach consensus. Only those parts of the studies dealing with divorce and meeting the inclusion criteria were extracted and evaluated. The following domains were assessed: Source, methods, participants, independent variable, outcome, data analysis, risk of bias, methodological quality, results. A detailed description of the data sheet is available in the Supplementary Material.
Risk of Bias Assessment
Two authors independently assessed the risk of bias and methodological quality in different domains (DF, SH). The overall risk of bias was graded as low, moderate, serious, or critical and the methodological quality was graded as low or high, in each case by two authors (DF, SH) independently. Discrepancies were discussed with another author (AK) to achieve consensus.
The risk of bias assessment of the interventional studies which were included was conducted according to the guidelines of the Cochrane Collaboration. Domains that were assessed are: Selection bias, performance bias, detection bias, attrition bias, reporting bias and other sources of bias.
The risk of bias for non-interventional studies was assessed with the preliminary risk of bias for exposures tool template (ROBINS-E tool) (Preliminary risk of bias for exposures tool template, 2020). The template is subdivided in “Preliminary considerations” and “Risk of bias assessment.” Preliminary considerations in terms of confounding areas regarding the divorce rate assessed for this review were: socio-demographics, marriage details, socio-economic status and country. Preliminary considered co-exposures for this review were co-morbidity, a previous cancer diagnosis, advanced cancer at diagnosis and impairing cancer therapy. Criteria used to determine the accuracy of exposure measurement were security of source and detailed description of cancer diagnoses. Factors to consider when evaluating health outcome assessment were: definition of “married,” definition of “divorce,” contamination of the category “divorced,” time between exposure and outcome assessed. Furthermore, study-specific confounding areas, co-exposures and criteria used to determine the accuracy of exposure measurement in the included studies were identified. The “Risk of bias assessment” includes the domains confounding, selection of participants, classification of exposures, departures from intended exposures, missing data, measurement of outcomes and selection of the reported result. The relative domain and finally the overall bias were graded in the categories low, moderate, serious, critical, and no information.
Assessment of Methodological Quality
The methodological quality of non-randomized studies was assessed with the Newcastle-Ottawa Quality Assessment Scale (NOS), which includes the domains selection, comparability, and exposure/outcome (Wells et al., 2020). For cross-sectional studies, an adapted version was used (Herzog et al., 2013). The overall rating scale goes from zero to nine stars for each study (ten stars for cross-sectional studies). The methodological quality was defined as low if the overall rating was six stars or lower, or if studies were rated with only one star in the domains “selection of cases and controls or cohorts” or “assessment of outcome,” or if studies were rated with zero stars in any domain. The methodological quality of all other studies was defined as high.
Synthesis of Extracted Evidence
The data was analyzed and classified according to the identified primary and secondary outcomes. In systematic qualitative synthesis, evidence was summarized. A summary of the methodology and results of each of the studies included was provided in table form. If possible, the ratio of divorced cancer patients to divorced couples without a cancer diagnosis was calculated for each study group. If groups of studies had similar designs, cohorts, and outcomes and furthermore had low risk of bias and a high methodical quality, a standard test of heterogeneity was planned: In case of low heterogeneity (<25%), studies were set to be included in a meta-analysis.
Results
The search yielded 13,929 publications, of which 15 finally met the inclusion criteria (Figure 1). One study was removed from the analysis because it could not be interpreted due to methodological weaknesses and a critical “risk of bias” rating (Cheng et al., 2018).
Due to the small number of studies and the heterogeneity of the study designs and the investigated groups, no meta-analysis could be performed.
The characteristics of the included studies are shown in Table 1, the corresponding rating of the methodological quality is illustrated in Figure 2.
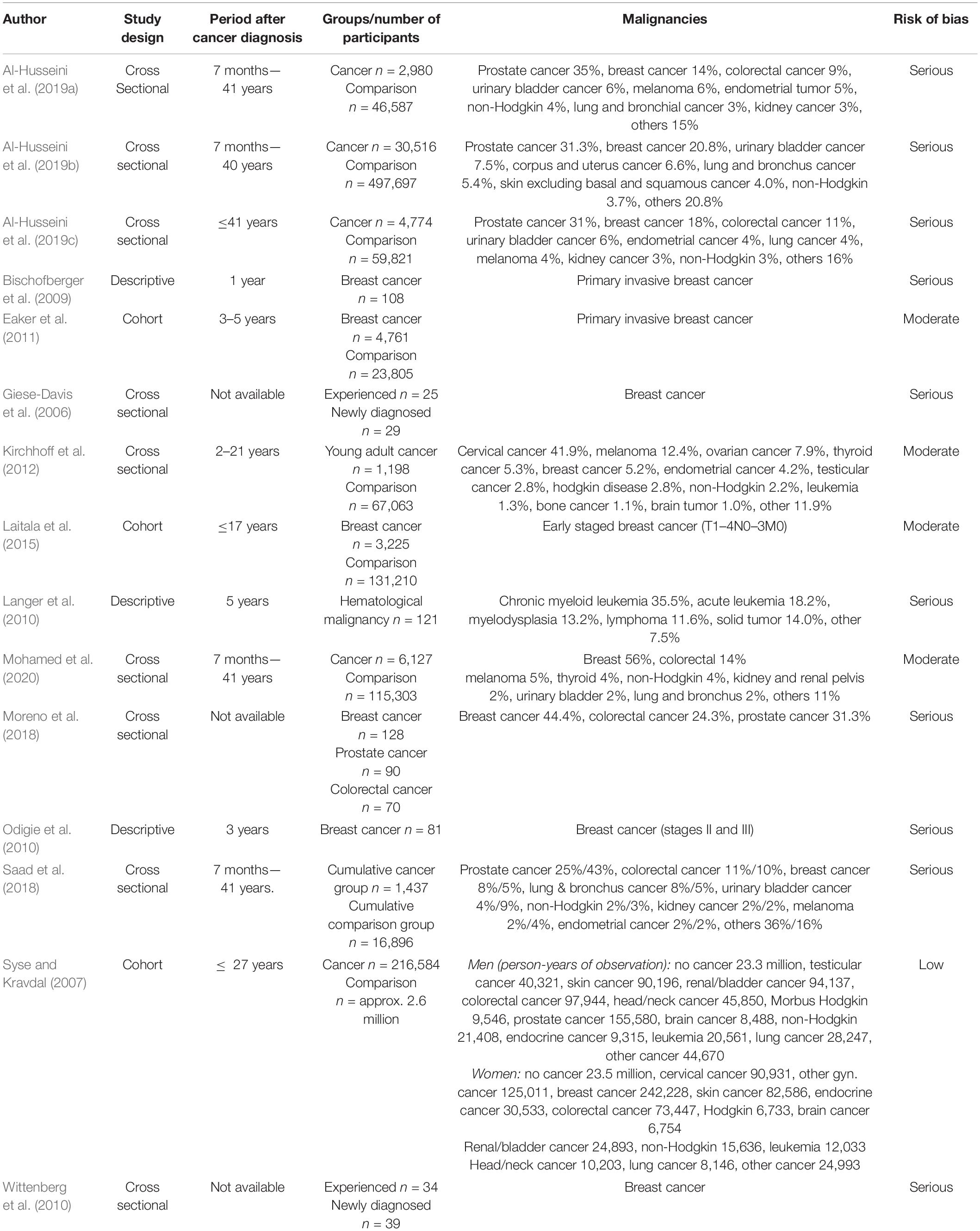
Table 1. Characteristics of the included studies.
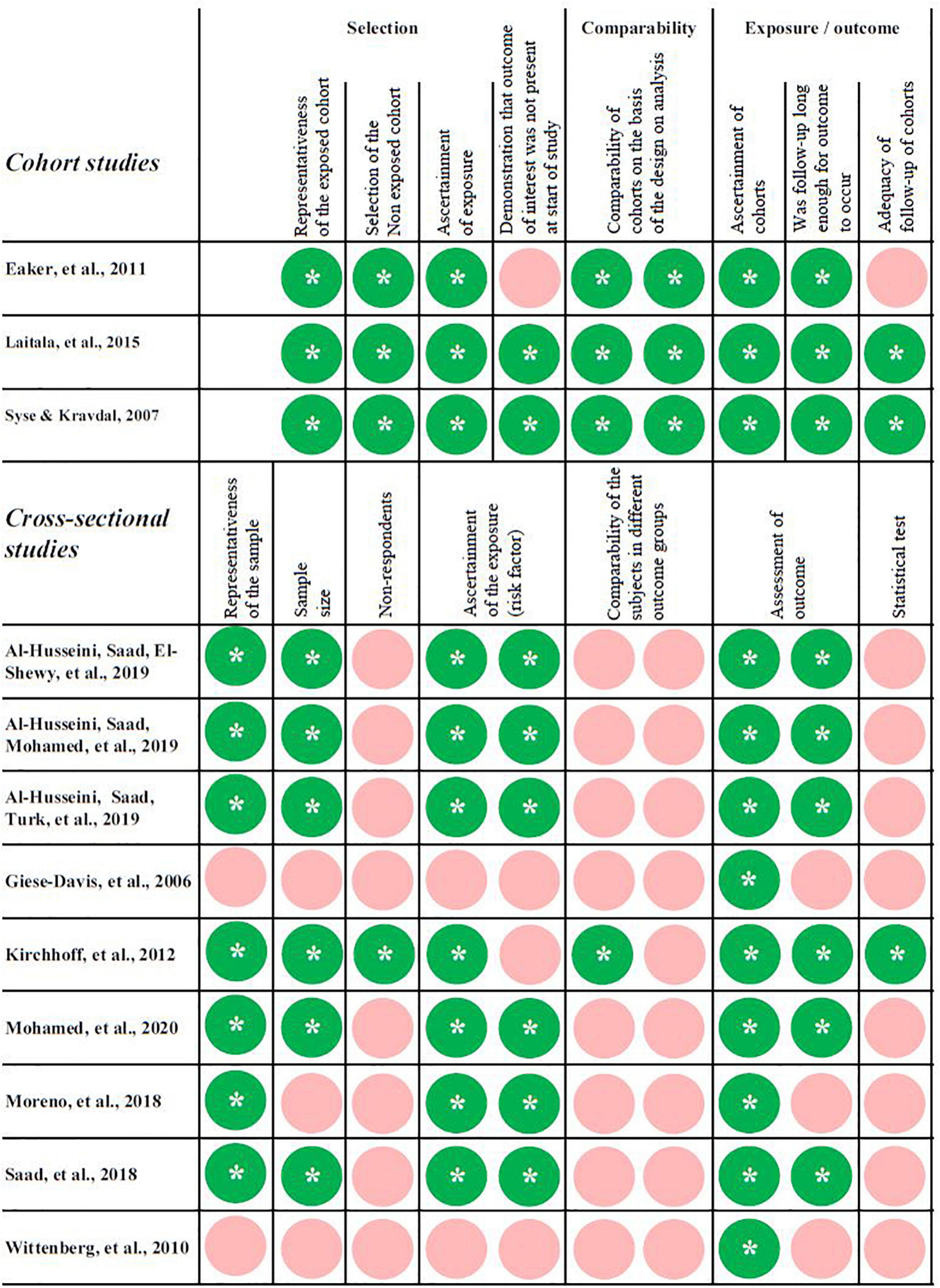
Figure 2. Rating of the methodological quality of the included cohort studies with the NOS (Wells et al., 2020). For the rating of the cross-sectional studies a modified version was used (Herzog et al., 2013). The overall rating scale goes from zero to nine stars (*) for each study (ten stars for cross-sectional studies).
General Cancer Diagnosis
Seven of the studies included present data on the primary question of whether cancer in general affects the divorce rate (Table 2).
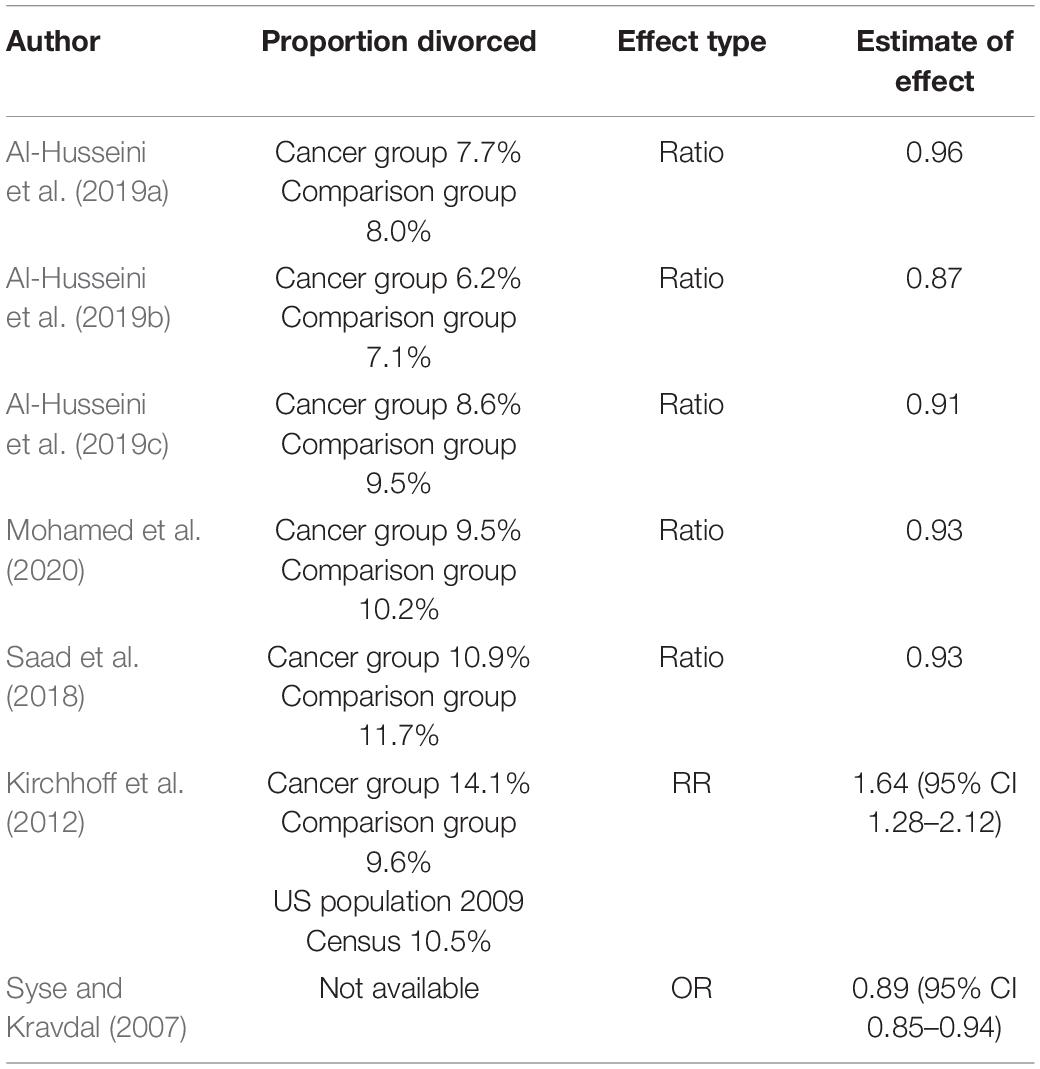
Table 2. Estimate effects of cancer diagnoses in general on the divorce rate.
Five very similar designed cross-sectional studies show marital status data on 739,599 subjects from the U.S. Surveillance, Epidemiology, and End Results database and compare two groups of patients with recent cancer diagnoses: Patients who already had a history of cancer before their recent second cancer diagnosis (n = 45,834) with those who have received their first cancer diagnosis ever (n = 736 304) (Saad et al., 2018; Al-Husseini et al., 2019a,b,c; Mohamed et al., 2020). In all five studies, the proportion of divorced patients in the previous cancer diagnosis group is marginally lower than in the comparison group with a ratio of divorce ranging from 0.87 to 0.96. Since all five studies primarily investigate other issues, the marital status data of the two groups was not adjusted in any way, so that a confounding must be assumed in several domains—the risk of bias was rated serious in all five studies. The methodological quality of the included parts of the studies is low (NOS 6/10 stars).
In a Norwegian registry study by Syse and Kravdal (2007) including 2.8 million subjects over an observation period of 27 years the odds ratio for divorce after a cancer diagnosis in already married subjects of 0.89 (95% CI 0.85–0.94) was calculated. The study was assessed with a low risk of bias and a high methodological quality (NOS 9/9 stars).
However, a cross-sectional study Kirchhoff et al. (2012) shows an increased risk ratio of 1.64 (95% CI 1.28–2.12) for divorce after a cancer diagnosis in one spouse. This study was conducted with 68,261 respondents, who were interviewed in 2009 in a telephone survey. The study was assessed with a moderate risk of bias and a high methodological quality (NOS 8/10 stars).
Cancer Type
Ten of the studies included provided data on the effect of specific cancer types on the divorce rate (Table 3).
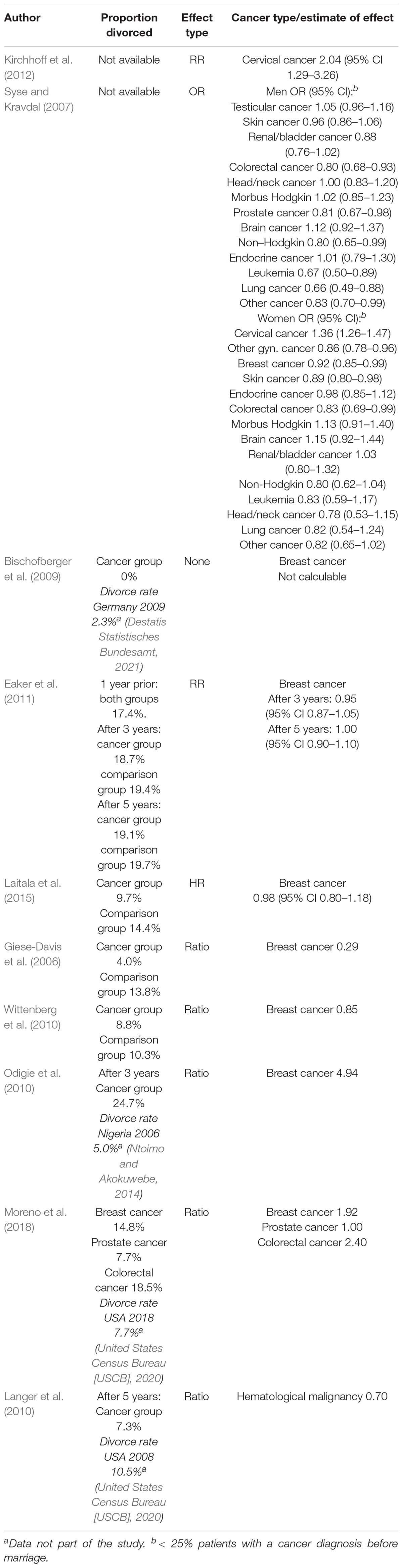
Table 3. Estimate effects of specific cancer types on the divorce rate.
Cervical Cancer
Two studies assessed divorce data on cervical cancer patients. Syse and Kravdal (2007) found an odds ratio for divorce after a cancer diagnosis of 1.36 (95% CI 1.26–1.47), Kirchhoff et al. (2012) found an increased risk of divorce after a cervical cancer diagnosis showing a risk ratio of 2.04 (95% CI 1.29–3.26).
Breast Cancer
Seven studies investigate breast cancer patients within the scope of the inclusion criteria of this systematic review:
In a German longitudinal, descriptive study Bischofberger et al. (2009) examined 108 patients for changes in their relationships one year after the initial diagnosis of breast cancer. During the observation period no divorce occurred. Information is lacking on many potentially confounding domains, so that the risk of bias was assessed as serious.
In a matched cohort study, Eaker et al. (2011) analyzed 4,761 breast cancer patients and 23,805 women matched by birth year and community. Time points were one year prior to the breast cancer patients’ calendar year of diagnosis, at the time of diagnosis, after three, and after 5 years. The risk ratio for divorce for the breast cancer survivors, adjusted for educational level, was 0.95 (95% CI 0.87–1.05) three years after diagnosis and 1.00 (95% CI 0.90–1.10) five years after diagnosis. The risk of bias was graded moderate, the methodological quality high (NOS 8/9 stars).
A total of 3,225 early stage breast cancer patients were compared to 131,210 healthy people in a Finnish registry study by Laitala et al. (2015). There was no significant difference in the divorce rate over a 10-year observation period. Overall, the adjusted hazard ratio for divorce in breast cancer patients was 0.98 (95% CI 0.80–1.18). The study was assessed with a moderate risk of bias and a high methodological quality (NOS 9/9 stars).
Two similar designed studies investigated a peer counseling intervention, in which newly diagnosed breast cancer patients (cumulative n = 68) were accompanied by breast cancer survivors with completed therapy, who were on average 52.20 and 59.56 months away from diagnosis (cumulative n = 59) (Giese-Davis et al., 2006; Wittenberg et al., 2010): Only baseline data in this study included data on divorce, which was extracted and assessed. A lower proportion of divorced patients was found in the more experienced group, compared to the newly diagnosed patients (4.0 vs. 13.8 and 8.8 vs. 10.3%). Accordingly, the divorce ratio is low in both studies. Not least because of the unadjusted group differences, this study was assessed with a serious risk of bias and a low methodological quality (NOS 1/10 stars).
A subgroup analysis in the Norwegian registry study by Syse and Kravdal (2007) showed, that the odds ratio for divorce is slightly lower for breast cancer patients. A limiting factor is that in this calculation, contrary to the review inclusion criteria, some of the subjects were diagnosed with cancer before marriage (< 25%).
Only one Nigerian descriptive study presented a high divorce rate in breast cancer patients within a follow-up period of three years compared to national data that was not part of the study (Odigie et al., 2010; Ntoimo and Akokuwebe, 2014). However, only 86 female patients after mastectomy were examined, most of whom lived in polygamous marriages. The risk of bias was rated serious in this study.
Hematologic Malignancies
Two studies provide divorce data on hematological malignancies:
Langer et al. (2010) examined 121 patients with hematological malignancies after hematopoietic stem cell transplantation, including patients with myelodysplastic syndrome (13.2%), which might not be considered as a malignancy. In a 5-year follow-up period the divorce rate was 7.3% (USA divorce rate 2008: 10.5%) (United States Census Bureau [USCB], 2020). The study was found to have a high risk of bias, partly because of an unclear proportion of subjects that was randomly assigned to an intervention to improve physical and cognitive limitations and manage emotional and family changes associated with hematopoietic stem cell transplantation.
A reduced odds ratio for divorce for leukemia and non-Hodgkin’s lymphomas was assessed by Syse and Kravdal (2007) only with respect to male patients. Again, a < 25% proportion of patients were diagnosed before marriage.
Colo-Rectal, Prostate, and Lung Cancer
In a cross-sectional study, data was divided into three groups: breast cancer (n = 128), prostate cancer (n = 90) and colorectal cancer (n = 70). There were no healthy controls (Moreno et al., 2018). The authors showed that the proportion of divorce was 14.8% for breast cancer patients, 7.7% for prostate cancer patients, and 18.5% for colorectal cancer patients. Since the groups were not adjusted and showed heterogeneity regarding socio-demographics, the risk of bias was assessed as serious and the methodological quality was assessed as low (NOS 4/10 stars).
Syse and Kravdal (2007) found a lower odds ratio of divorce in colorectal and prostate cancer patients compared to the healthy comparison group. A similar result was found in male but not female lung cancer patients.
Discussion
Overall, according to six of the seven included studies on this question, there is evidence for a slightly decreased risk of divorce after a cancer diagnosis in general. The findings of Kirchhoff et al. (2012) differ from this conclusion, which is probably due to the following bias: a large proportion of patients in the cancer group suffered from cervical cancer, who were found to have a significantly increased risk ratio for divorce in the subgroup analysis. Furthermore, only young adult cancer survivors were examined: compared to older patients, younger patients more often are getting divorced after a cancer diagnosis (Syse and Kravdal, 2007). The fact that a cancer diagnosis does not increase the risk of divorce is supported by many studies, that apply a wider definition of separation in addition to official divorces (Dorval et al., 1999; Joly et al., 2002; Carlsen et al., 2007; Karraker and Latham, 2015).
Regarding the effect of a breast cancer diagnosis on the risk of divorce, most of the findings in the included studies are similar: a breast cancer diagnosis appears to have no or a decreasing effect on the risk for divorce. This finding is also consistent with other studies in the field that have examined other types of separations besides official divorces (Dorval et al., 1999; Carlsen et al., 2007).
Remarkably, the risk ratio or the odds ratio of divorce for cervical carcinoma patients is increased in the included studies (Syse and Kravdal, 2007; Kirchhoff et al., 2012). This coincides with the findings of Carlsen et al. (2007), who found an increased risk of divorce in a subgroup analysis for cervical cancer patients. Yet, in this study, the definition of divorce also included moving to different places of residence. Young people in particular are affected by this diagnosis, but the divorce rate is elevated among older individuals, as well (Syse and Kravdal, 2007). It is conceivable that infertility plays a role in this context. However, Syse and Kravdal (2007) did not find any influence of fertility on the odds ratio of divorce after a cancer diagnosis in their analysis, but there is evidence for a negative correlation between infertility distress and relationship satisfaction, which Ussher and Perz (2019) show in a survey of 693 women and 185 men with a cancer diagnosis. This infertility distress is not only persistent long term, but it is also associated with a higher rate of mental health disorders and psychosocial distress (Logan et al., 2019), which is an additional burden for the affected couple. Beyond that, depending on its stage and therapy, a diagnosis of cervical cancer may be associated with long-term changes in sexuality such as a tighter and shorter vagina, dyspareunia, and sexual worries (Lammerink et al., 2012; Wiltink et al., 2020). The resulting changes in sexual relationships are also a central issue for male partners of cervical cancer patients (Oldertrøen Solli et al., 2019). In a cross-sectional study with 113 cervical cancer patients a connection between sexual satisfaction and marital adjustment, partially moderated by body image, was found (do Rosário Ramos Nunes Bacalhau et al., 2020). It is also possible that the group of cervical cancer patients is composed differently than groups suffering from other cancer types because the risk of developing the disease is associated with early sexual intercourse and the number of sexual partners (International Collaboration of Epidemiological Studies of Cervical Cancer, 2009).
Strengths and Limitations
Despite the large number of studies on the topic of separations or divorces after a cancer diagnosis, this is the first systematic review dedicated to this topic. The search strategy and inclusion criteria are very broad, including all countries and cultures, in order to fully reflect the current state of the literature. Thus, a very large number of studies could be found and screened in full-text. The focus on the outcome “divorce” instead of “separation” not only contributes to a high internal validity, but also allows a comparison of the results of the included studies with general divorce statistics.
However, as a result of this limitation exclusively to official divorces, only a few studies could be included. Some of these studies did not primarily investigate marital status in the context of cancer. Among other things, this has led to a more or less significant limitation of the methodological quality of these studies regarding divorce data. The significance of the present study is further diminished by the fact that no meta-analysis could be carried out because of the few and very heterogeneous studies included. Overall, the level of evidence provided by this systematic review is reduced due to the limitations mentioned. Further studies are needed to verify our results.
Time courses after a cancer diagnosis were not in scope of the present systematic review, although these proved to be quite relevant when reviewing the data: For example, Syse and Kravdal (2007) found an increased divorce rate within five years of a testicular cancer diagnosis, whereas the divorce rate is not increased after five years or overall.
What Happens Within the Partnership?
The outcome “divorce” is too general to differentiate between specific positive and negative effects of a cancer diagnosis on a partnership. A well-researched model showing how couples deal with stressors such as a cancer diagnosis is that of dyadic coping (Bodenmann, 1995): Positive coping mechanisms like providing or accepting support maintain or even improve the relationship functioning (Traa et al., 2015). Negative coping behavior such as hiding worries can contribute to increased distress in the partnership (Kayser et al., 2007; Badr et al., 2010; Traa et al., 2015). Thus, there may be subgroups that are heavily distressed by a cancer diagnosis due to failed coping and whose marriages break up in the further course of the disease (Stephens et al., 2016), but which, in regard of the divorce rate, are balanced by subgroups where positive effects of a cancer diagnosis have led to an improved quality of relationships.
We must be cautious to interpret a divorce always as negative. For some couples it could be part of a developmental process. The negative impact of a stressful relationship should not be underestimated. Also being alone and having no social support might have a greater influence on health-related issues than being divorced (Metsä-Simola and Martikainen, 2013). After being divorced there are some cancer patients who will engage after a short time in a new relationship.
Future research has to investigate more closely the longitudinal processes within relationships dealing with cancer and relate individual factors and the dyadic process to health-related outcomes. An important task of such research is to identify risk factors and subgroups of patients and their families who need specific psychosocial support.
Conclusion
Overall, we found evidence that cancer is associated with a slightly decreased divorce rate—an exception may be cervical carcinoma, which is associated with an increased divorce rate. The findings of the present study are limited by the heterogeneity and methodological weaknesses of most of the included studies. Thus, further research is needed, not only to validate the findings, but also to better understand the processes within the partnerships, with the aim of better adapting psychosocial support services to the vulnerable groups.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Author Contributions
AK, DF, and MB contributed to conception and design of the study. DF and MB conducted the protocol and the searches. DF, SH, and NS performed the screening. DF and SH performed the data extraction and rating. DF wrote the first draft of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We would like to thank Carla Fischer for her help in the preparation of the review and Kamila Leszek for her support in the evaluation of the studies.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2022.828656/full#supplementary-material
Abbreviations
CI, confidence interval; HR, hazard ratio; NOS, Newcastle-Ottawa Quality Assessment Scale; OR, odds ratio; RR, risk ratio.
References
Aizer, A. A., Chen, M. H., McCarthy, E. P., Mendu, M. L., Koo, S., Wilhite, T. J., et al. (2013). Marital status and survival in patients with cancer. J. Clin. Oncol. 31, 3869–3876. doi: 10.1200/JCO.2013.49.6489
Al-Husseini, M. J., Saad, A. M., El-Shewy, K. M., Nissan, N. E., Gad, M. M., Alzuabi, M. A., et al. (2019a). Prior malignancy impact on survival outcomes of glioblastoma multiforme; population-based study. Int. J. Neurosci. 129, 447–454. doi: 10.1080/00207454.2018.1538989
Al-Husseini, M. J., Saad, A. M., Mohamed, H. H., Alkhayat, M. A., Sonbol, M. B., and Abdel-Rahman, O. (2019b). Impact of prior malignancies on outcome of colorectal cancer; revisiting clinical trial eligibility criteria. BMC Cancer 19:863. doi: 10.1186/s12885-019-6074-6
Al-Husseini, M. J., Saad, A. M., Turk, T., Tabash, M. A., and Abdel-Rahman, O. (2019c). Impact of Prior Malignancy on Survival Outcomes of Stage IV Pancreatic Adenocarcinoma: SEER-Based Cohort. J. Gastrointest. Cancer 50, 794–800. doi: 10.1007/s12029-018-0158-4
Amato, P. R. (2000). The consequences of divorce for adults and children. J. Marriage Fam. 62, 1269–1287. doi: 10.1111/j.1741-3737.2000.01269.x
Badr, H., Carmack, C. L., Kashy, D. A., Cristofanilli, M., and Revenson, T. A. (2010). Dyadic coping in metastatic breast cancer. Health Psychol. 29, 169–180. doi: 10.1037/a0018165
Bischofberger, B., Mollova, M., Geyer, S., and Neises, M. (2009). [Changes in Partnership Relationships of Women After Breast Cancer Diagnosis]. Geburtshilfe Frauenheilkund. 69, 1091–1096. doi: 10.1055/s-0029-1240640
Bodenmann, G. (1995). A systemic-transactional conceptualization of stress and coping in couples. Swiss J. Psychol. 54, 34–49. doi: 10.1016/j.cpr.2008.10.004
Bouchard, G. (2006). Cohabitation versus marriage: the role of dyadic adjustment in relationship dissolution. J. Divorce Remarriage 46, 107–117.
Carlsen, K., Dalton, S. O., Frederiksen, K., Diderichsen, F., and Johansen, C. (2007). Are cancer survivors at an increased risk for divorce? A Danish cohort study. Eur. J. Cancer 43, 2093–2099. doi: 10.1016/j.ejca.2007.05.024
Centers for Disease Control and Prevention [CDC] (2021). Marriage and Divorce, National Center for Health Statistics, USA. Available Online at: https://www.cdc.gov/nchs/fastats/marriage-divorce.htm. (accessed December 3, 2021)
Cheng, A., Zeng, Y., Liu, X., Liu, S., Cheng, S., Kwok, C., et al. (2018). Cognitive challenges while at work and work output in breast cancer survivors employed in a rapidly evolving economy. J. Cancer Surviv. 12, 753–761. doi: 10.1007/s11764-018-0712-x
Destatis Statistisches Bundesamt (2021). Ergebnis 12631-0001. Available Online at: https://www-genesis.destatis.de/genesis/online?sequenz=tabelleErgebnis&selectionname=12631-0001 (accessed December 3, 2021)
Dinh, K. T., Aizer, A. A., Muralidhar, V., Mahal, B. A., Chen, Y. W., Beard, C. J., et al. (2018). Increased Vulnerability to Poorer Cancer-Specific Outcomes Following Recent Divorce. Am. J. Med. 131, 517–523. doi: 10.1016/j.amjmed.2017.11.039
do Rosário Ramos Nunes Bacalhau, M., Pedras, S., and da Graça Pereira Alves, M. (2020). Attachment style and body image as mediators between marital adjustment and sexual satisfaction in women with cervical cancer. Support. Care Cancer 28, 5813–5819. doi: 10.1007/s00520-020-05423-y
Dorval, M., Maunsell, E., Taylor-Brown, J., and Kilpatrick, M. (1999). Marital stability after breast cancer. J. Natl. Cancer Inst. 91, 54–59. doi: 10.1093/jnci/91.1.54
Eaker, S., Wigertz, A., Lambert, P. C., Bergkvist, L., Ahlgren, J., Lambe, M., et al. (2011). Breast cancer, sickness absence, income and marital status. A study on life situation 1 year prior diagnosis compared to 3 and 5 years after diagnosis. PLoS One 6:e18040. doi: 10.1371/journal.pone.0018040
Giese-Davis, J., Bliss-Isberg, C., Carson, K., Star, P., Donaghy, J., Cordova, M. J., et al. (2006). The effect of peer counseling on quality of life following diagnosis of breast cancer: an observational study. Psychooncology 15, 1014–1022. doi: 10.1002/pon.1037
Hagedoorn, M., Sanderman, R., Bolks, H. N., Tuinstra, J., and Coyne, J. C. (2008). Distress in couples coping with cancer: a meta-analysis and critical review of role and gender effects. Psychol. Bull. 134, 1–30. doi: 10.1037/0033-2909.134.1.1
Herzog, R., Álvarez-Pasquin, M. J., Díaz, C., Del Barrio, J. L., Estrada, J. M., and Gil, Á (2013). Are healthcare workers’ intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health 13:154. doi: 10.1186/1471-2458-13-154
Higgins, J. P. T., and Green, S. (2011). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration. Available Online at: http://handbook.cochrane.org (accessed March 4, 2020)
Hodges, L. J., Humphris, G. M., and Macfarlane, G. (2005). A meta-analytic investigation of the relationship between the psychological distress of cancer patients and their carers. Soc. Sci. Med. 60, 1–12. doi: 10.1016/j.socscimed.2004.04.018
International Agency for Research on Cancer [IARC] (2020). Cancer Today – IARC. Available Online at: https://gco.iarc.fr/today/data/factsheets/cancers/39-All-cancers-fact-sheet.pdf (accessed October 1, 2020).
International Collaboration of Epidemiological Studies of Cervical Cancer (2009). Cervical carcinoma and sexual behavior: collaborative reanalysis of individual data on 15,461 women with cervical carcinoma and 29,164 women without cervical carcinoma from 21 epidemiological studies. Cancer Epidemiol. Biomark. Prev. 18, 1060–1069. doi: 10.1158/1055-9965.EPI-08-1186
Joly, F., Héron, J. F., Kalusinski, L., Bottet, P., Brune, D., Allouache, N., et al. (2002). Quality of life in long-term survivors of testicular cancer: a population-based case-control study. J. Clin. Oncol. 20, 73–80. doi: 10.1200/JCO.2002.20.1.73
Karraker, A., and Latham, K. (2015). In Sickness and in Health? Physical Illness as a Risk Factor for Marital Dissolution in Later Life. J. Health Soc. Behav. 56, 420–435. doi: 10.1177/0022146515596354
Kayser, K., Watson, L. E., and Andrade, J. T. (2007). Cancer as a “we-disease”: examining the process of coping from a relational perspective. Fam. Syst. Health 25, 404–418. doi: 10.1037/1091-7527.25.4.404
Kirchhoff, A. C., Yi, J., Wright, J., Warner, E. L., and Smith, K. R. (2012). Marriage and divorce among young adult cancer survivors. J. Cancer Surviv. 6, 441–450. doi: 10.1007/s11764-012-0238-6
Laitala, V. S., Saarto, T., Einiö, E. K., Martikainen, P., and Silventoinen, K. (2015). Early-stage breast cancer is not associated with the risk of marital dissolution in a large prospective study of women. Br. J. Cancer 113, 543–547. doi: 10.1038/bjc.2015.216
Lammerink, E. A., de Bock, G. H., Pras, E., Reyners, A. K., and Mourits, M. J. (2012). Sexual functioning of cervical cancer survivors: a review with a female perspective. Maturitas 72, 296–304. doi: 10.1016/j.maturitas.2012.05.006
Langer, S. L., Yi, J. C., Storer, B. E., and Syrjala, K. L. (2010). Marital adjustment, satisfaction and dissolution among hematopoietic stem cell transplant patients and spouses: a prospective, five-year longitudinal investigation. Psychooncology 19, 190–200. doi: 10.1002/pon.1542
Leopold, T. (2018). Gender Differences in the Consequences of Divorce: a Study of Multiple Outcomes. Demography 55, 769–797. doi: 10.1007/s13524-018-0667-6
Logan, S., Perz, J., Ussher, J. M., Peate, M., and Anazodo, A. (2019). Systematic review of fertility-related psychological distress in cancer patients: informing on an improved model of care. Psychooncology 28, 22–30. doi: 10.1002/pon.4927
Manne, S., and Badr, H. (2008). Intimacy and relationship processes in couples’ psychosocial adaptation to cancer. Cancer 112, 2541–2555. doi: 10.1002/cncr.23450
McGowan, J., Sampson, M., Salzwedel, D. M., Cogo, E., Foerster, V., and Lefebvre, C. (2016). PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J. Clin. Epidemiol. 75, 40–46. doi: 10.1016/j.jclinepi.2016.01.021
Metsä-Simola, N., and Martikainen, P. (2013). The short-term and long-term effects of divorce on mortality risk in a large Finnish cohort, 1990-2003. Popul. Stud. 67, 97–110. doi: 10.1080/00324728.2012.746386
Mohamed, H. H., Ibrahim Sokkar, M., Afifi, A. M., Saad, A. M., Albarouki, S., and Al-Husseini, M. J. (2020). Does a history of malignancy impact the survival of a subsequent endometrial adenocarcinoma? Should clinical trials eligibility criteria be revisited? J. Obstet. Gynaecol. 40, 233–239. doi: 10.1080/01443615.2019.1621808
Moher, D., Shamseer, L., Clarke, M., Ghersi, D., Liberati, A., Petticrew, M., et al. (2015). Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 4:1. doi: 10.1186/2046-4053-4-1
Moreno, P. I., Ramirez, A. G., San Miguel-Majors, S. L., Fox, R. S., Castillo, L., Gallion, K. J., et al. (2018). Satisfaction with cancer care, self-efficacy, and health-related quality of life in Latino cancer survivors. Cancer 124, 1770–1779. doi: 10.1002/cncr.31263
Ntoimo, L. F. C., and Akokuwebe, M. E. (2014). Prevalence and Patterns of Marital Dissolution in Nigeria. Nigerian J. Sociol. Anthropol. 12, 1–15. doi: 10.36108/NJSA/4102/120210
Odigie, V. I., Tanaka, R., Yusufu, L. M., Gomna, A., Odigie, E. C., Dawotola, D. A., et al. (2010). Psychosocial effects of mastectomy on married African women in Northwestern Nigeria. Psychooncology 19, 893–897. doi: 10.1002/pon.1675
Oldertrøen Solli, K., de Boer, M., Nyheim Solbraekke, K., and Thoresen, L. (2019). Male partners’ experiences of caregiving for women with cervical cancer-a qualitative study. J. Clin. Nurs. 28, 987–996. doi: 10.1111/jocn.14688
Preliminary risk of bias for exposures tool template (2020). The ROBINS-E tool (Risk Of Bias In Non-randomized Studies - of Exposures). England: University of Bristol
Regan, T. W., Lambert, S. D., Girgis, A., Kelly, B., Kayser, K., and Turner, J. (2012). Do couple-based interventions make a difference for couples affected by cancer? A systematic review. BMC Cancer 12:279. doi: 10.1186/1471-2407-12-279
Saad, A. M., Al-Husseini, M. J., Elgebaly, A., Aboshady, O. A., Salahia, S., and Abdel-Rahman, O. (2018). Impact of prior malignancy on outcomes of stage IV esophageal carcinoma: SEER based study. Expert Rev. Gastroenterol. Hepatol. 12, 417–423. doi: 10.1080/17474124.2018.1426458
Sbarra, D. A. (2015). Divorce and health: current trends and future directions. Psychosom. Med. 77, 227–236. doi: 10.1097/PSY.0000000000000168
Sbarra, D. A., Law, R. W., and Portley, R. M. (2011). Divorce and Death: a Meta-Analysis and Research Agenda for Clinical, Social, and Health Psychology. Perspect. Psychol. Sci. 6, 454–474. doi: 10.1177/1745691611414724
Sjövall, K., Attner, B., Lithman, T., Noreen, D., Gunnars, B., Thomé, B., et al. (2009). Influence on the health of the partner affected by tumor disease in the wife or husband based on a population-based register study of cancer in Sweden. J. Clin. Oncol. 27, 4781–4786. doi: 10.1200/JCO.2008.21.6788
Song, H. Y., Kwon, J. A., Choi, J. W., Kim, S. J., and Park, E. C. (2014). Gender differences in marital disruption among patients with cancer: results from the Korean National Health and Nutrition Examination Survey (KNHANES). Asian Pac. J. Cancer Prev. APJCP 15, 6547–6552. doi: 10.7314/apjcp.2014.15.16.6547
Stephens, C., Westmaas, J. L., Kim, J., Cannady, R., and Stein, K. (2016). Gender differences in associations between cancer-related problems and relationship dissolution among cancer survivors. J. Cancer Surviv. 10, 865–873. doi: 10.1007/s11764-016-0532-9
Syse, A., and Kravdal, Ø (2007). Does cancer affect the divorce rate? Demogr. Res. 16, 469–492. doi: 10.4054/DemRes.2007.16.15
Traa, M. J., De Vries, J., Bodenmann, G., and Den Oudsten, B. L. (2015). Dyadic coping and relationship functioning in couples coping with cancer: a systematic review. Br. J. Health Psychol. 20, 85–114. doi: 10.1111/bjhp.12094
United States Census Bureau [USCB] (2020). U.S. Marriage and Divorce Rates by State: 2008 & 2018. Available Online at: https://www.census.gov/library/visualizations/interactive/marriage-divorce-rates-by-state.html (accessed November 30, 2021)
Ussher, J. M., and Perz, J. (2019). Infertility-related distress following cancer for women and men: a mixed method study. Psychooncology 28, 607–614. doi: 10.1002/pon.4990
Wells, G. A., Shea, B., O’Connell, D., Peterson, J., Welch, V., Losos, M., et al. (2020). The Newcastle Ottawa Scale (NOS) for assessing the quality of nonrandomized studies in meta-analysis. Ottawa: The Ottawa Hospital Research Institute.
Wiltink, L. M., King, M., Müller, F., Sousa, M. S., Tang, M., Pendlebury, A., et al. (2020). A systematic review of the impact of contemporary treatment modalities for cervical cancer on women’s self-reported health-related quality of life. Support. Care Cancer 28, 4627–4644. doi: 10.1007/s00520-020-05554-2
Keywords: cancer, oncology, psycho-oncology, divorce, separation, marriage, couple, spouse
Citation: Fugmann D, Boeker M, Holsteg S, Steiner N, Prins J and Karger A (2022) A Systematic Review: The Effect of Cancer on the Divorce Rate. Front. Psychol. 13:828656. doi: 10.3389/fpsyg.2022.828656
Received: 03 December 2021; Accepted: 10 February 2022;
Published: 09 March 2022.
Edited by:
Chiara Acquati, University of Houston, United StatesReviewed by:
Catarina Samorinha, University of Sharjah, United Arab EmiratesBarbara Head, University of Louisville, United States
Copyright © 2022 Fugmann, Boeker, Holsteg, Steiner, Prins and Karger. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dominik Fugmann, dominik.fugmann@med.uni-duesseldorf.de