 Susan Koranyi1*
Susan Koranyi1* Andreas Hinz1
Andreas Hinz1 Julia M. Hufeld1Tim J. Hartung1,2
Julia M. Hufeld1Tim J. Hartung1,2 Leonhard Quintero Garzón1
Leonhard Quintero Garzón1 Uta Fendel3Anne Letsch4,5
Uta Fendel3Anne Letsch4,5 Matthias Rose3,6
Matthias Rose3,6 Peter Esser1
Peter Esser1 Anja Mehnert-Theuerkauf1
Anja Mehnert-Theuerkauf1- 1Department of Medical Psychology and Medical Sociology, University Medical Center Leipzig, Leipzig, Germany
- 2Department of Neurology, Charité - Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin, Berlin, Germany
- 3Department of Psychosomatic Medicine, Charité - Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin, Berlin, Germany
- 4Department of Hematology and Oncology, Campus Benjamin Franklin, Charité -Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Berlin, Germany
- 5Department of Medicine II, Hematology and Oncology, University Hospital Schleswig-Holstein, Kiel, Germany
- 6Department of Quantitative Health Sciences, Medical School, University of Massachusetts, Amherst, MA, United States
Objective: To test the psychometric properties, internal consistency, dimensional structure, and convergent validity of the German version of the Demoralization Scale-II (DS-II), and to examine the association between demoralization, sociodemographic, disease- and treatment-related variables in patients with cancer.
Methods: We recruited adult patients with cancer at a Psychosocial Counseling Center and at oncological wards. Participants completed the 16-item DS-II, Patient Health Questionnaire-9 (PHQ-9), Generalized Anxiety Disorder Screener-2 (GAD-2), Distress Thermometer (DT), and Body Image Scale (BIS). We analyzed internal consistency of the DS-II using Cronbach‘s Alpha (α). We tested the dimensional structure of the DS-II with Confirmatory Factor Analyses (CFA). Convergent validity was expressed through correlation coefficients with established measures of psychological distress. The associations between demoralization, sociodemographic, disease- and treatment-related variables were examined with ANOVAs.
Results: Out of 942 eligible patients, 620 participated. The average DS-II total score was M = 5.78, SD = 6.34, the Meaning and Purpose subscale M = 2.20, SD = 3.20, and the Distress and Coping Ability subscale M = 3.58, SD = 3.45. Internal consistency ranged from high to excellent with α = 0.93 for the DS-II total scale, α = 0.90 for the Meaning and Purpose subscale, and α = 0.87 for the Distress and Coping Ability subscale. The one-factor and the two-factor model yielded similar model fits, with CFI and TLI ranging between 0.910 and 0.933, SRMR < 0.05. The DS-II correlated significantly with depression (PHQ-9: r = 0.69), anxiety (GAD-2: r = 0.72), mental distress (DT: r = 0.36), and body image disturbance (BIS: r = 0.58). High levels of demoralization were reported by patients aged between 18 and 49 years (M = 7.77, SD = 6.26), patients who were divorced/separated (M = 7.64, SD = 7.29), lung cancer patients (M = 9.29, SD = 8.20), and those receiving no radiotherapy (M = 7.46, SD = 6.60).
Conclusion: The DS-II has very good psychometric properties and can be recommended as a reliable tool for assessing demoralization in patients with cancer. The results support the implementation of a screening for demoralization in specific risk groups due to significantly increased demoralization scores.
Introduction
Cancer diagnosis and treatment are frequently associated with psychological distress (Hartung et al., 2017; Mehnert et al., 2018; Pitman et al., 2018; Carlson et al., 2019). Considerable research has shown a wide spectrum of psychological states ranging from subsyndromal psychological distress and mental disorders (Mehnert et al., 2014; Ernst et al., 2021) to existential distress such as demoralization (Robinson et al., 2015; Tang et al., 2015; Robinson et al., 2016c). Prevalence rates of demoralization syndrome range between 13 and 33% depending on the method of measurement used and characteristics of the patient sample (Robinson et al., 2015).
Based on the work of de Figueiredo and Frank (de Figueiredo and Frank, 1982), among others, Kissane and Clark (Kissane et al., 2001) conceptualized demoralization as a state of maladaptive coping characterized by a loss of purpose and meaning in life, low morale, low optimism, as well as helplessness and hopelessness (Clarke and Kissane, 2002; Kissane, 2014; Robinson et al., 2015). Demoralization can influence mood and the ability to cope with threatening life events (Clarke and Kissane, 2002); it also negatively influences social functioning, decision making, and quality of life (Nanni et al., 2018), and causes a feeling of dependence and being a burden on others (Robinson et al., 2015; Vehling et al., 2017). Demoralization is a common presentation of existential distress and is considered a significant mental health concern since it is accompanied with the desire for hastened death and is a risk factor for suicide (Vehling et al., 2017; Nanni et al., 2018; McFarland et al., 2019; Rzeszut and Assael, 2021). It also causes problems in building sustainable and trusting relationships with health care providers (Quintero Garzón et al., 2018) and family caregivers (Bovero et al., 2021).
Kissane and colleagues developed the Demoralization Scale (DS-I; Kissane et al., 2004), a 24-item scale with a five-factorial structure and response options ranging from 0 (“never”) to 4 (“all the time”). The DS-I has been adapted to several languages (Mullane et al., 2009; Hung et al., 2010; Mehnert et al., 2011; Costantini et al., 2013; Grassi et al., 2017), and has been found to have acceptable to excellent psychometric properties. The German version of the DS-I has high internal consistency (α = 0.84) for the total score and good construct validity with other mental health-related measures (Mehnert et al., 2011). Applications of the DS-I have been performed in several oncological studies (Robinson et al., 2015, 2016c).
The DS-II, a more recently developed revised short-version of the DS-I, is a 16-item version of the Demoralization Scale (Robinson et al., 2016a,b) that has fewer items and answer options (three instead of five) making it more user-friendly for patients with advanced cancer and patients in the palliative care period. Initial results for the DS-II scale’s reliability and validity have been published based on an Australian sample of 211 patients receiving palliative care, most of them suffering from cancer (Robinson et al., 2016b). The DS-II demonstrated high internal consistency (α = 0.89 for the total scale; α = 0.84 for the Meaning and Purpose subscale, and α = 0.82 for the Distress and Coping Ability subscale) (Robinson et al., 2016b). Subsequently, a Spanish version of the DS-II was tested in a sample of 150 patients with advanced cancer stages in Spain and a number of Latin American countries (Belar et al., 2019). The Spanish DS-II version also showed a high internal consistency with α = 0.88 (total DS-II scale), α = 0.83 (Meaning and Purpose), and α = 0.79 (Distress and Coping Ability) (Belar et al., 2019). Recently, a Chinese version of the DS-II was used in a cross-sectional study to assess demoralization in Chinese patients with advanced cancer (Wu et al., 2021). The internal reliability of the Chinese DS-II was excellent, with α = 0.91 for the total scale, and α = 0.91 and α = 0.89 for its two subscales (Wu et al., 2021). However, although the DS-II had already been translated and used in various languages, it was not until the present study was conducted that it was translated into German or a psychometric evaluation of that version was carried out. Furthermore, none of the previously conducted studies replicated the proposed two-factor solution of the original DS-II scale (Robinson et al., 2016b) using Confirmatory Factor Analyses.
Previous studies consistently reported a strong positive relationship between demoralization and depression (Katz et al., 2001; Grassi et al., 2004; Kissane et al., 2004; Mullane et al., 2009; Mehnert et al., 2011; Hadnagy et al., 2012; Lee et al., 2012; Vehling et al., 2012, 2013; Costantini et al., 2013) and demoralization and anxiety (Katz et al., 2001; Grandi et al., 2011; Mehnert et al., 2011; Vehling et al., 2011). Recently, the short version of the DS-II scale has also been used to investigate the association between demoralization and other established measures of psychological distress. For example, a strong positive association between DS-II and depression scores were reported (Ignatius and De La Garza, 2019; Wu et al., 2021). Furthermore, various studies across different cancer populations have demonstrated strong associations between depression and body image disturbance, an issue which is known to greatly burden cancer survivors suffering from severe disease- and treatment-related body changes (e.g., body disfigurement, skin changes, weight gain or loss, scars, and hair loss) (Hartung et al., 2021). However, no previous study had investigated whether body image disturbance also goes along with feelings of demoralization.
The relationship between demoralization and disease- and treatment-related factors was frequently studied in previous studies, consistently revealing no association between time since diagnosis (Katz et al., 2001; Boscaglia and Clarke, 2007; Mehnert et al., 2011; Robinson et al., 2016a), stage of disease (Grassi et al., 2004; Boscaglia and Clarke, 2007; Lee et al., 2012; Vehling et al., 2012; Robinson et al., 2016a), type of treatment (Grassi et al., 2004; Vehling et al., 2012), and demoralization scores. However, inconsistent findings were reported with regard to the association between tumor site and demoralization. One study recorded higher demoralization scores in patients with head and neck cancer compared to patients with cervical or gastrointestinal cancer (Lee et al., 2012), whereas other studies found no association (Mehnert et al., 2011; Robinson et al., 2016a).
Regarding sociodemographic factors, consistent evidence was reported for the association between employment and demoralization, with lower demoralization reported by employed patients in comparison to jobless patients (Katz et al., 2001; Lee et al., 2012). Similar results for the relationship between marital status and demoralization were reported by three studies, revealing that living with a partner was associated with lower levels of demoralization (Katz et al., 2001; Grandi et al., 2011; Mehnert et al., 2011). However, mixed evidence was obtained regarding age, gender, and education. In two studies, demoralization was unrelated to age (Katz et al., 2001; Quintero Garzón et al., 2021), whereas, another study demonstrated that older age was related to higher scores of demoralization (Vehling et al., 2011). In contrast, two studies reported a negative correlation between age and demoralization (Mehnert et al., 2011; Vehling et al., 2013). There are also no consistent findings with regard to gender-specific differences in demoralization scores. While some studies indicated that women report higher demoralization scores (Grandi et al., 2011; Mehnert et al., 2011; Vehling et al., 2011, 2013), two other studies reported no gender differences (Grassi et al., 2005; Lee et al., 2012). Additionally, previous studies found no consistent association between education and demoralization (Katz et al., 2001; Lee et al., 2012).
Based on previous evidence, the aims of this study were (1) to examine psychometric properties of the German version of the DS-II scale and to calculate internal consistency in a sample of patients with cancer; (2) to test the two-factor structure of DS-II scale; (3) to verify convergent validity of DS-II scale with established measures of depression, anxiety, mental distress, and body image disturbance; and (4) to determine the relationship between demoralization and sociodemographic and disease- and treatment-related factors.
Materials and Methods
Patient Sample
Participants were adult (≥18 years) patients with a confirmed diagnosis of any cancer type (ICD-10 code C00 - C97) who were recruited consecutively from two study centers, one in Leipzig and the other in Berlin, Germany, between May 2018 and January 2020. In the Leipzig study center, the patients were recruited from the Psychosocial Counseling Center for patients with cancer at the Leipzig University Hospital. In Berlin, the patients were recruited from the wards of two departments, the Department of Radiation Oncology and Radiotherapy, and the Department of Hematology and Oncology, of the Charité University Medical Center (Hartung et al., 2021). After having the aims of the study explained to them, all participants gave informed consent in accordance to the Declaration of Helsinki. Patients were not included in the study if they were not proficient in German or if they were pregnant or breastfeeding. The study was approved by the Ethics Committee of the University of Leipzig (reference number 090/18-ek).
Measures
We collected sociodemographic and disease- and treatment-related variables via standardized patient self-report questionnaires.
Demoralization
The Demoralization Scale DS-II is an established and validated self-report questionnaire with 16 items rated using a three-point Likert scale (0 = “never”; 1 = “sometimes”; 2 = “often”), resulting in a total score ranging from 0 to 32. The DS-II contains two 8-item subscales called Meaning and Purpose and Distress and Coping Ability (see Table 2 for example of items). High scores represent high levels of demoralization (Robinson et al., 2016b). The authors of the original DS-II scale (Robinson et al., 2016b) defined the following cutoff criteria for the total score: low (0–3), moderate (4–10), and high (≥11) demoralization. We translated the DS-II scale from English to German according to state-of-the-art translation procedures (Sousa and Rojjanasrirat, 2011). First, two translators independently performed one German translation each. They then discussed their translations and agreed upon one version. Second, this German version was translated back into English by two other translators who did not know the original English version, and agreed on one final back translation. Third, this back translation was compared with the original questionnaire by an expert in psychosocial oncology. Differences were discussed in the research team, and consensus was reached upon a final German translation.
Depression
The Patient Health Questionnaire-9 (PHQ-9) is a 9-item instrument for measuring depression (Kroenke et al., 2001). Patients rate the symptoms they have experienced over the previous 2 weeks on a four-point Likert scale from 0 = “not at all” to 3 = “almost every day.” The sum score ranges from 0 to 27, and higher scores represent higher depressive symptomatology. The German version of PHQ-9 shows good internal consistencies, with α = 0.89 (Kroenke et al., 2001).
Anxiety
The Generalized Anxiety Disorder Screener-2 (GAD-2) is an ultra-short instrument for measuring anxiety experienced over the past 2 weeks (Löwe et al., 2010). Patients rate their symptoms on a four-point Likert scale from 0 = “not at all” to 3 = “almost every day,” resulting in a sum score ranging from 0 to 6. Higher scores indicate higher levels of anxiety. Cronbach‘s alpha = 0.72 demonstrates acceptable internal consistency (Hinz et al., 2017).
Mental Distress
The NCCN Distress Thermometer (DT) assesses patients’ overall psychological symptom burden during the past week on a visual analog scale (0–10), with higher scores representing higher mental distress (Mehnert et al., 2006).
Body Image Disturbance
The 10-item Body Image Scale (BIS) is a reliable and validated self-report scale to measure body image disturbance (Hopwood et al., 2001). Patients rate how they felt about their appearance during the past week on a four-point Likert scale ranging from 0 = “not at all” to 3 = “very much.” Sum scores range from 0 to 30, with higher scores indicating increased cancer-specific aspects of body image disturbance (e.g., worries about physical and sexual attractiveness and feelings of being permanently disfigured by surgical treatment). The German version of the BIS shows excellent internal consistency with α = 0.92 (Hartung et al., 2021).
Statistical Analysis
The statistical procedures were performed with IBM SPSS, version 25; the Mplus 6.1 version was used for the Confirmatory Factor Analyses.
Missing Values
Patients were included in the statistical calculations if at least 75% of the items were valid on both subscales of the DS-II. In these cases, the missing values were replaced with the rounded mean of the valid items. If on at least one subscale the number of missing items was higher than 25%, the patients were excluded from further analysis.
Internal Consistency and Dimensional Structure of the Demoralization Scale-II
Internal consistency of the DS-II scale and its subscales was assessed with Cronbach’s alpha coefficients (α). Confirmatory Factor Analyses were performed to evaluate whether the proposed two-factor solution of the original DS-II scale (Robinson et al., 2016b) can be replicated with our sample of patients with cancer. Two models were tested: the one-factor model, aggregating across all 16 items, and the two-factor model according to the dimensional structure of two proposed subscales. The goodness-of-fit was evaluated using the Comparative Fit Index (CFI) and the Tucker Lewis Index (TLI) with cutoff values of >0.95 for “good” and >0.90 for an “acceptable” model fit. Badness-of-fit was estimated via Standardized Root Mean Square Residual (SRMR < 0.05 “good,” <0.10 “acceptable” fit) and the Root Mean Square Error of Approximation (RMSEA <0.06 “good,” <0.08 “acceptable” fit) (Hu and Bentler, 1999; Schermelleh-Engel et al., 2003).
Convergent Validity
To assess convergent validity with established measures of psychological distress, we calculated Pearson correlations coefficients between DS-II and PHQ-9 (depression), GAD-2 (anxiety), mental distress (DT) and body image disturbance (BIS). The threshold for convergent validity was determined with r ≥ 0.5 (Cohen, 1977).
Associations Between Demoralization, Sociodemographic, Disease- and Treatment-Related Variables
The relationship between demoralization and sociodemographic (age, gender, employment status, civil status, and education), and disease- and treatment related variables (tumor site, metastases, surgery, chemotherapy, radiotherapy, and hormone therapy) were tested with ANOVAs with the covariables gender and age group.
Results
Sample Characteristics
A total of 942 patients with cancer were eligible for the study, and 677 (response rate: 72%) were willing to participate. Ultimately, 620 patients (n_counseling center = 571, 92%; n_oncological wards = 49, 8%) provided valid data sets (age: M = 60.3 years; 57.7% women). Further sample characteristics are given in Table 1.
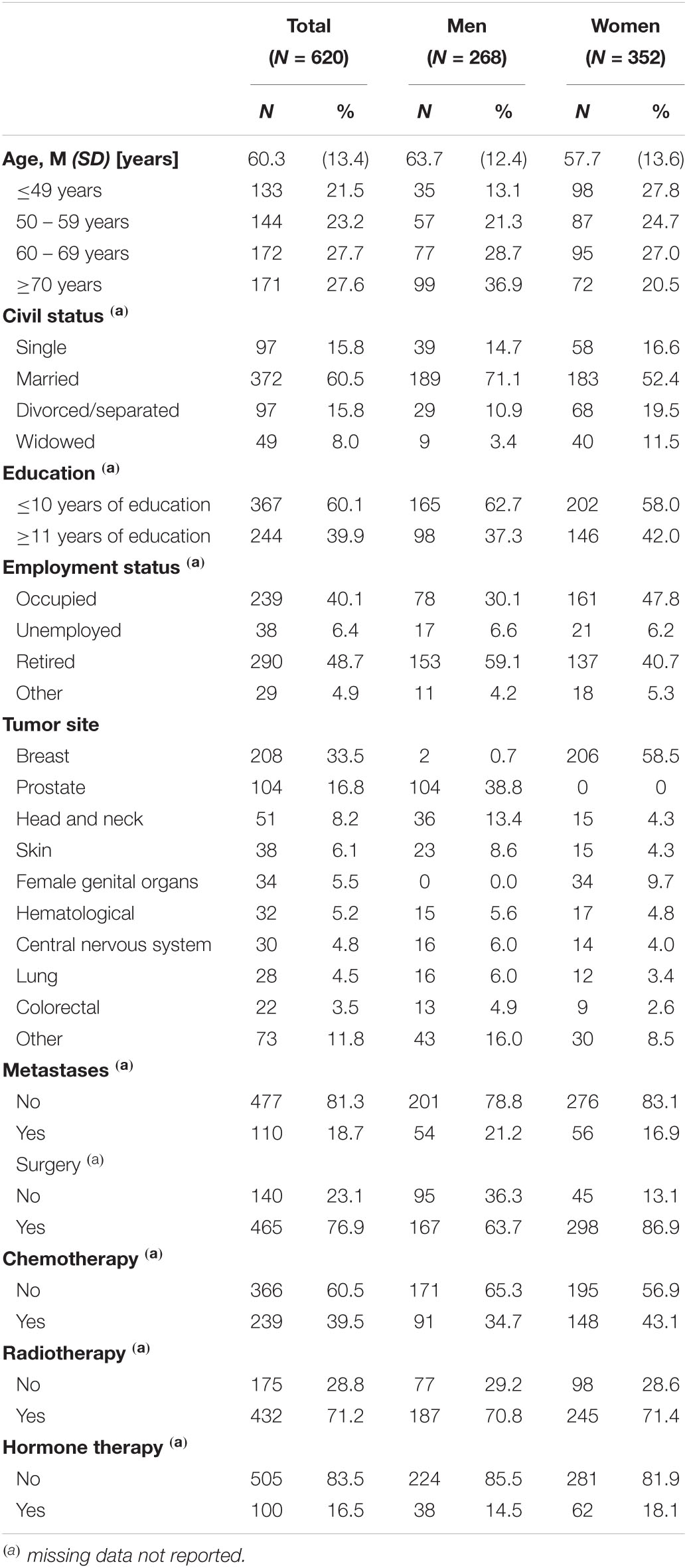
Table 1. Sample characteristics.
Internal Consistency and Psychometric Properties of the Demoralization Scale-II
The Cronbach‘s alpha coefficients were α = 0.93 for the total scale and between α = 0.87 (Distress and Coping Ability) and α = 0.90 (Meaning and Purpose) for the subscales.
Mean scores and standard deviations on a single item level are presented in Table 2. In addition, we calculated the proportion of the patients who responded to the items with at least “sometimes” (summarizing the response codes of 1 = “sometimes” and 2 = “often”), see Table 2. The items with the highest affirmation scores were “I feel distressed about what is happening to me” (M = 0.74, SD = 0.68, 61%) and “I feel irritable” (M = 0.63, SD = 0.66, 52%). The lowest affirmation was given to the items “I am not a worthwhile person” (M = 0.15, SD = 0.39, 14%) and “I would rather not be alive” (M = 0.10, SD = 0.35, 9%).
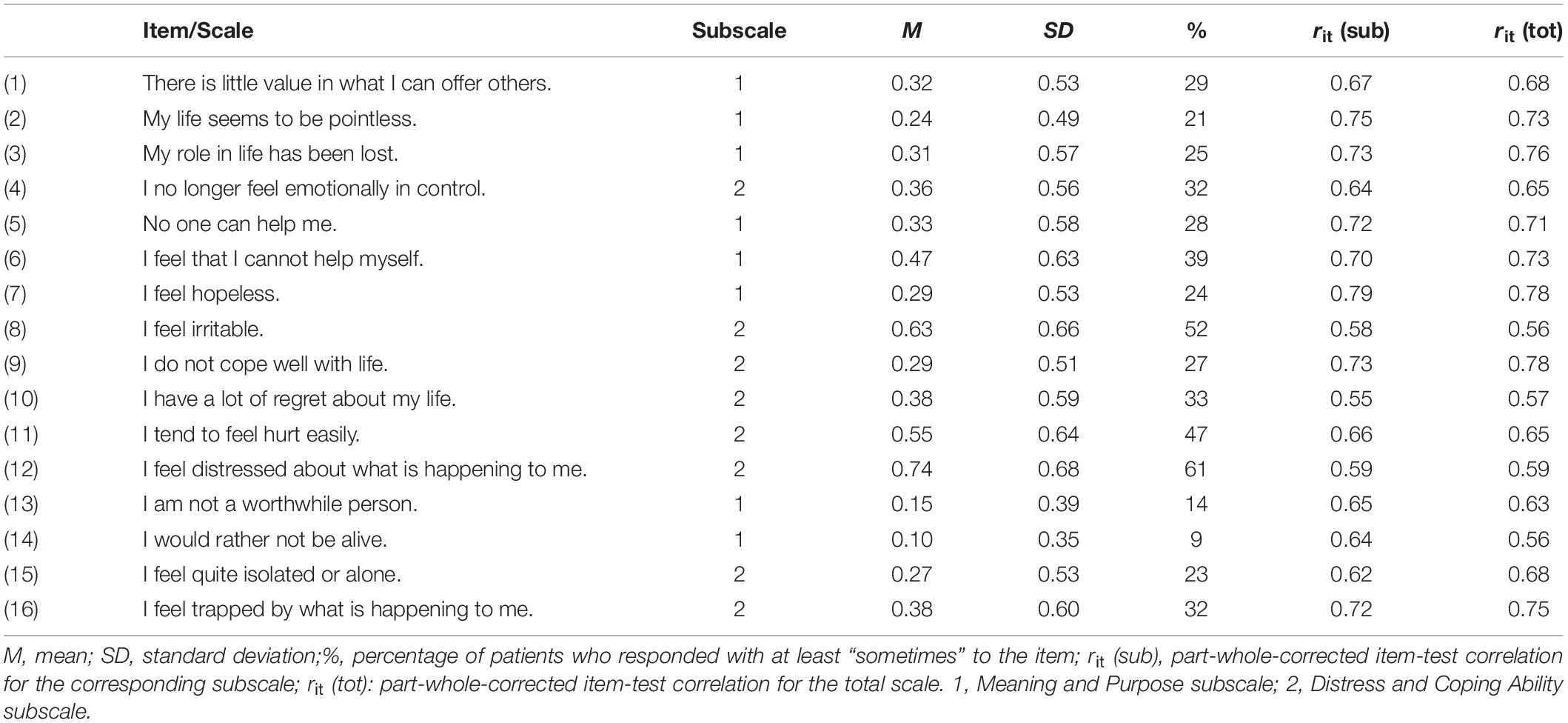
Table 2. Item characteristics of the Demoralization Scale-II (DS-II).
All part-whole-corrected item-test correlations were above 0.50, and the contributions of the items to the assigned subscale were about as high as the contributions to the total scale (Table 2).
The mean scores for the total scale were M = 5.78, SD = 6.34, and for the subscales M = 2.20, SD = 3.20 (Meaning and Purpose) and M = 3.58, SD = 3.45 (Distress and Coping Ability). Using the cutoff criteria for low (0–3), moderate (4–10) and high (≥11) demoralization, the percentages were 50.5% (low), 27.1% (moderate), and 22.4% (high demoralization).
Test of the Dimensional Structure
Table 3 presents the results of the CFA. Both models, the one-factor model and the two-factor model, yielded similar CFA results, with CFI and TLI coefficients between 0.910 and 0.933 and SRMR coefficients <0.05. The correlation between the two subscales of the DS-II was r = 0.82.
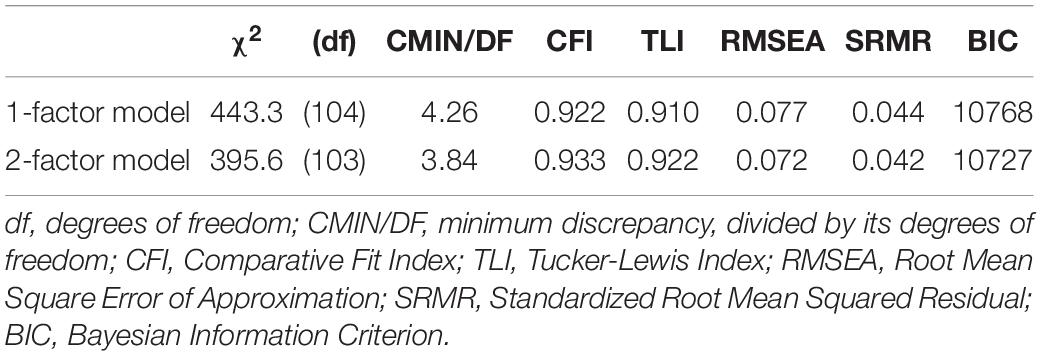
Table 3. Summary of fit indices of the models.
Convergent Validity of the Demoralization Scale-II With Other Measures of Psychological Distress
Table 4 presents associations between the scales of the DS-II and other scales measuring psychological distress. The correlations were highest for anxiety (GAD-2), followed by depression (PHQ-9), with coefficients of about r = 0.70, while the Distress Thermometer score was less strongly associated with demoralization (r = 0.36 for the total scale). In all cases, the correlations between the DS-II subscale Distress and Coping Ability and the other scales was higher than those with the subscale Meaning and Purpose.
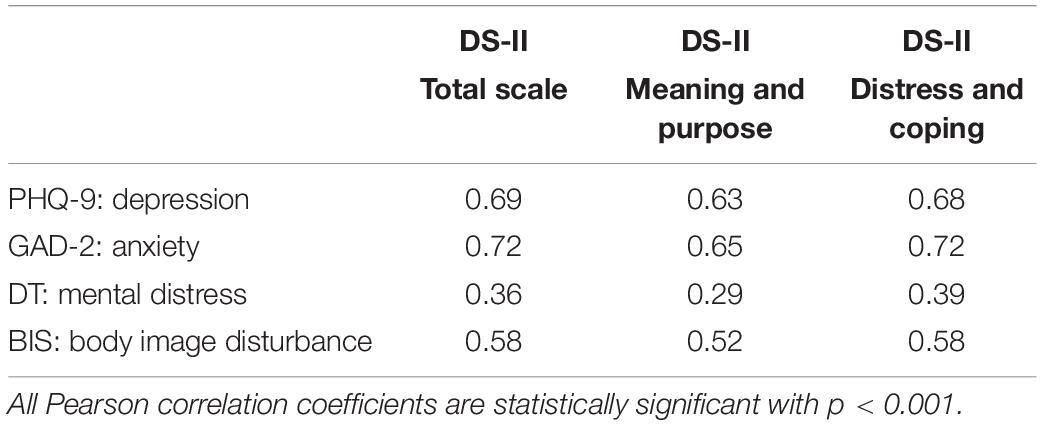
Table 4. Correlations between demoralization and other variables of psychological distress.
Demoralization, Sociodemographic, Disease- and Treatment-Related Variables
The associations between demoralization, sociodemographic, disease- and treatment-related variables are presented in Table 5. Women (M = 5.97, SD = 6.20) reported slightly higher demoralization than men (M = 5.53, SD = 6.53) did, but the effect was far from being statistically significant. Concerning age, the highest demoralization was found in the youngest age group (18–49 years: M = 7.77, SD = 6.26), while the patients of the oldest age group (≥70 years: M = 4.44, SD = 5.65) were least demoralized.
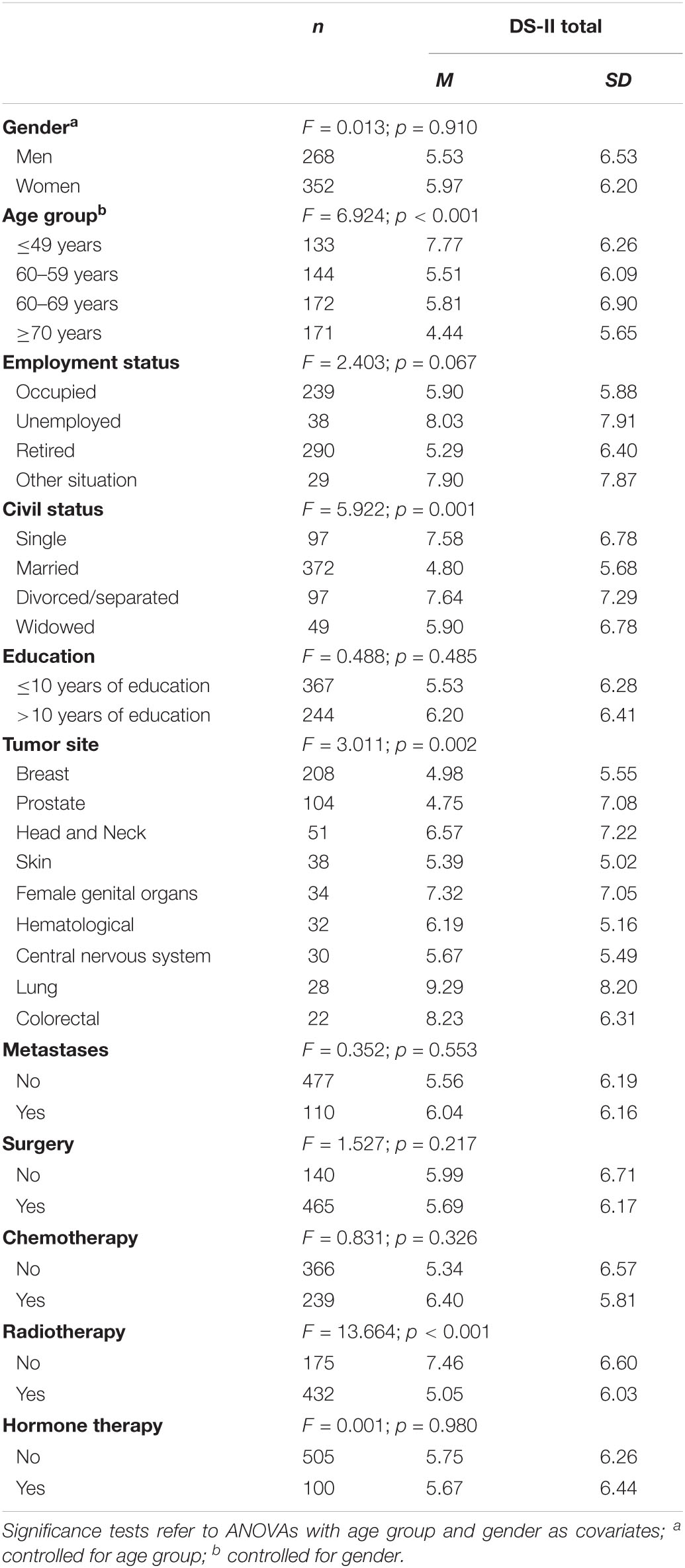
Table 5. Demoralization Scale-II mean scores depending on sociodemographic, disease- and treatment-related variables.
Including age and gender as covariates, ANOVAs revealed high demoralization mean scores for divorced/separated patients (M = 7.64, SD = 7.29). Patient with a diagnosis of lung cancer reported the highest rates of demoralization (M = 9.29, SD = 8.20), while patients with prostate cancer (M = 4.75, SD = 7.08) and patients with breast cancer (M = 4.98, SD = 5.55) being the least demoralized. Patients with metastases (M = 6.04, SD = 6.16) were not significantly less demoralized than patients without metastases (M = 5.56, SD = 6.19).
Treatment conditions were differently associated with demoralization: Patients who had not received radiotherapy reported significantly higher levels of demoralization (M = 7.46, SD = 6.60) compared to patients who received radiotherapy (M = 5.05, SD = 6.03), whereas we found no association between demoralization scores and having received surgery, chemotherapy, or hormone therapy.
Discussion
The first aim of this study was to test the psychometric properties and reliability of the DS-II. All of the items contributed substantially to the total score and to the subscales, and the Cronbach‘s alpha coefficients for the total scale and for the subscales were almost excellent. The coefficients were slightly higher than in the study testing the DS-II in a sample of patients receiving palliative care (Robinson et al., 2016b), and they were also higher than the coefficients obtained in a sample of Spanish patients with advanced cancer (Belar et al., 2019). The higher reliability coefficients may be explained (at least partly) by the fact that our study did not only include patients with advanced stages of cancer, some of whom suffer from cognitive impairment, so coherent item responses may have been somewhat more likely in our sample. The mean score in our sample was lower than that of the sample in the original DS-II study with advanced cancer or other progressive diseases who were receiving palliative care (M = 7.64, SD = 6.43, Robinson et al., 2016b). Interestingly, for the DS-I with 24 items, the Cronbach‘s alpha coefficients of the total scale (α = 0.94), obtained in a general populations sample (Quintero Garzón et al., 2021), was nearly exactly as high as the coefficient (α = 0.93) in our sample.
However, the CFA results for both the one-factor solution and the two-factor solution failed to meet the common criteria for good model fit. Only the SRMR coefficient was within the range of good model fit for both factorial solutions. This means that there is some structure in the items that is not explained by the models. We could have defined factors that would be better suited to our own data set as has been done in previous research on the DS-I scale, however, this would probably not contribute to the comparability of international studies on demoralization. To omit problems with the subscales we believe that, due to the high Cronbach‘s alpha coefficient, it is at least justified to consider the one-dimensional solution of the DS-II.
As expected from previous studies, we also found a strong correlation between demoralization and depression, which demonstrated a close relationship between these concepts. This association is about as high as that reported for outpatients in a psychiatric oncology clinic (Ignatius and De La Garza, 2019) and the relationship between demoralization and depression in the Spanish sample of patients with advanced cancer (Belar et al., 2019). A lower correlation between DS-II and the PHQ-9 score was found for the patients receiving palliative care (r = 0.41) in the study introducing the DS-II (Robinson et al., 2016b), however, in that calculation, the PHQ-9 was only used in two categories.
Despite the positive association between depression and demoralization, both constructs can be distinguished by its core symptoms (depression: loss of pleasure and interest vs. demoralization: a loss of meaning, Robinson et al., 2015) and a dimensional characterization of depressed/demoralized patients indicates possible implications for treatment (Belvederi Murri et al., 2020a). Recent research identified a proportion of patients [17% (Wu et al., 2021) up to 28% (Tang et al., 2020)] with high levels of demoralization but low depression scores to whom special attention must be paid in clinical care. It is possible that these patients will be less likely to respond to antidepressants and are likely to respond best to meaning-centered psychotherapies (Ignatius and De La Garza, 2019).
The association between demoralization and anxiety was even higher than that with depression in our sample. This finding is in line with previous research demonstrating that demoralization is closely linked to the construct of anxiety (Mehnert et al., 2011; Nanni et al., 2018), and especially death anxiety in patients with advanced cancer (An et al., 2018). Anxiety disorders occur in comorbidity with demoralization in about a quarter of medically ill patients, particularly, generalized anxiety disorder, agoraphobia, and panic disorder (Rafanelli et al., 2013). The results also showed a significant association between demoralization and body image disturbance indicating that body-related issues should be addressed and considered in the psychosocial treatment of patients reporting demoralization.
We found a relevant decrease in demoralization with increasing age. This negative correlation confirms the results of two previous studies (Mehnert et al., 2011; Vehling et al., 2013) and was also reported for the Distress and Coping Ability subscale (Robinson et al., 2016a). In addition, multiple studies on depression and anxiety in patients with cancer have shown that, compared with the general population, young patients with cancer are much more affected than older ones (Götze et al., 2020). There are no normative values that could be used for such comparisons for the DS-II. A recent normative study with the DS-I failed to find a linear association between age and demoralization (Quintero Garzón et al., 2021); the highest scores were observed for the age categories <30 years, 50–59 years, and ≥70 years. Because of the lack of normative values for the DS-II scale we cannot assess the extent to which the age effect found in our study is specific for patients with cancer.
In accordance with previous evidence we found no association between demoralization and gender (Robinson et al., 2016a), while in the general population, demoralization (as measured with the DS-I) is higher in females than in males, with an effect size of d = 0.12 (Quintero Garzón et al., 2021).
Our results showed that being divorced/separated is related to higher levels of demoralization, a finding that is in line with the results of four previous studies (Katz et al., 2001; Grandi et al., 2011; Mehnert et al., 2011; Robinson et al., 2016a) and confirms the inverse relation between social support and demoralization.
Our results showed that the presence of metastases had no significant impact on demoralization. This is unlikely to be an indirect age effect since both groups, those with and without metastases, were of similar age (59.2 and 60.5 years, respectively). In addition, this finding is consistent with four other studies showing no association between demoralization and stage of disease (Grassi et al., 2004; Boscaglia and Clarke, 2007; Lee et al., 2012; Vehling et al., 2012). However, we found a significant association between demoralization and tumor site (highest demoralization scores for patients with lung cancer), which has not been reported in previous studies (Mehnert et al., 2011; Robinson et al., 2016a). Moreover, in contrast to previous findings (Robinson et al., 2016a) we obtained a significant association between cancer-specific treatment and demoralization, with significantly higher demoralization scores for patients who had not received radiotherapy compared to patients who had received radiotherapy. However, the lower demoralization scores in patients receiving radiotherapy may be confounded with tumor site. These findings add to the mixed evidence related to the association between demoralization and disease- and treatment-related variables and should be further investigated in future studies.
Several limitations of this study should be mentioned. Most of the patients were recruited in a counseling center. This sample may not be representative of all patients with cancer. These are patients who both perceive a need for help and are able to actively seek professional support. Therefore, we cannot conclude that it is a sample with especially high or especially low levels of burden. In addition, until now, no normative study has been conducted with the DS-II; therefore, the interpretability of the mean scores is limited. In particular, it would be relevant to examine whether age and gender differences obtained in patients with cancer can also be found in general population samples. Furthermore, according to our study design, we are not able to calculate test-retest reliability and sensitivity to change scores.
For future studies, it would be worthwhile to investigate how the DS-II can be used in clinical contexts in which patients do not experience psychological distress associated with cancer, but may still experience feelings of incompetence, and feelings of helplessness and hopelessness in response to a stressful life event. For example, demoralization was assessed with the DS-II scale in a sample of 209 postnatal women admitted with their babies to a residential early parenting program (Bobevski et al., 2018). The authors derived a 14-item revised scale, the Postnatal DS-II, showing good psychometric properties (Bobevski et al., 2018). Moreover, in a recent study with medically ill patients in general hospitals, even shorter versions of the Demoralization Scale with 13- and 6-items were developed, with both versions retaining high correlations with DS-I scores and concordance with the Diagnostic Criteria for Psychosomatic Research-Demoralization module (Belvederi Murri et al., 2020b).
From a clinical perspective, demoralization is a treatable condition and its diagnosis may empower clinicians to provide proper psychological care, something which is especially true with regard to the strong correlation between demoralization and suicidal ideation (Costanza et al., 2020). In this context, it is highly relevant to have access to a short, user-friendly and psychometrically sound measure of demoralization to correctly classify and distinguish the patients’ emotional states. Using the DS-II may guide clinicians’ efforts to provide appropriate interventions as early as possible, e.g., refer patients with high demoralization scores to meaning-centered interventions in order to enhance meaning and purpose and to promote coping abilities while facing existential threats (Breitbart et al., 2015, 2018). The DS-II scale can be easily incorporated into psychosocial, clinical, and palliative care settings as a brief screening measure to identify patients with high levels of demoralization and severe existential distress.
In summary, our study translated the DS-II into German and tested its psychometric properties. The psychometric evaluation demonstrated that the instrument shows satisfactory findings concerning the assessment of demoralization in patients with cancer. Further studies are needed to determine the best item structure of the DS-II scale and to gather normative data to put values from patients with cancer into context. Furthermore, we conclude that the results support the implementation of regular screening for demoralization in certain risk groups, as demoralization scores are significantly increased in patients at a younger age, divorced/separated patients, patients with a lung cancer diagnosis and in patients receiving no radiotherapy.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by the Ethics Committee of the University of Leipzig. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
SK, AH, and AM-T contributed to the conception and design. AM-T, UF, AL, and MR provided the administrative support. TH, AM-T, UF, AL, and MR contributed to the provision of study materials and patients. TH contributed to the collection and assembly of data. SK, AH, JH, LQG, and PE contributed to the data analysis and interpretation. SK and AH were mainly responsible for writing the manuscript, and all authors gave final approval of the manuscript.
Funding
We received funding support from the Leipzig University for Open Access Publishing.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
An, E., Lo, C., Hales, S., Zimmermann, C., and Rodin, G. (2018). Demoralization and death anxiety in advanced cancer. Psycho-Oncology 27, 2566–2572. doi: 10.1002/pon.4843
Belar, A., Arantzamendi, M., Rodríguez-Núñez, A., Santesteban, Y., Martinez, M., López-Saca, M., et al. (2019). Multicenter study of the psychometric properties of the new Demoralization Scale (DS-II) in Spanish-speaking advanced cancer patients. J. Pain Symptom Manage. 57, 627–634. doi: 10.1016/j.jpainsymman.2018.11.016
Belvederi Murri, M., Caruso, R., Ounalli, H., Zerbinati, L., Berretti, E., Costa, S., et al. (2020a). The relationship between demoralization and depressive symptoms among patients from the general hospital: network and exploratory graph analysis. J. Affect. Disord. 276, 137–146. doi: 10.1016/j.jad.2020.06.074
Belvederi Murri, M., Zerbinati, L., Ounalli, H., Kissane, D., Casoni, B., Leoni, M., et al. (2020b). Assessing demoralization in medically ill patients: factor structure of the Italian version of the demoralization scale and development of short versions with the item response theory framework. J. Psychosom. Res. 128:109889. doi: 10.1016/j.jpsychores.2019.109889
Bobevski, I., McKenzie, D. P., Rowe, H., Kissane, D. W., Clarke, D. M., and Fisher, J. (2018). Measuring postnatal demoralisation: adaptation of the Demoralisation Scale-II (DS-II) for postnatal use. J. Reprod. Infant Psychol. 36, 561–577. doi: 10.1080/02646838.2018.1519781
Boscaglia, N., and Clarke, D. M. (2007). Sense of coherence as a protective factor for demoralisation in women with a recent diagnosis of gynaecological cancer. Psycho-Oncology 16, 189–195. doi: 10.1002/pon.1044
Bovero, A., Vitiello, L. P., Botto, R., Gottardo, F., Cito, A., and Geminiani, G. C. (2021). Demoralization in end-of-life cancer patients’ family caregivers: a cross-sectional study. Am. J. Hospice Palliative Care 10499091211023482. doi: 10.1177/10499091211023482 [Epub ahead of print].
Breitbart, W., Pessin, H., Rosenfeld, B., Applebaum, A. J., Lichtenthal, W. G., Li, Y., et al. (2018). Individual meaning-centered psychotherapy for the treatment of psychological and existential distress: a randomized controlled trial in patients with advanced cancer. Cancer 124, 3231–3239. doi: 10.1002/cncr.31539
Breitbart, W., Rosenfeld, B., Pessin, H., Applebaum, A., Kulikowski, J., and Lichtenthal, W. G. (2015). Meaning-centered group psychotherapy: an effective intervention for improving psychological well-being in patients with advanced cancer. J. Clin. Oncol. 33, 749–754. doi: 10.1200/JCO.2014.57.2198
Carlson, L. E., Zelinski, E. L., Toivonen, K. I., Sundstrom, L., Jobin, C. T., Damaskos, P., et al. (2019). Prevalence of psychosocial distress in cancer patients across 55 North American cancer centers. J. Psychosoc. Oncol. 37, 5–21. doi: 10.1080/07347332.2018.1521490
Clarke, D. M., and Kissane, D. W. (2002). Demoralization: its phenomenology and importance. Aust. N. Z. J. Psychiatry 36, 733–742. doi: 10.1046/j.1440-1614.2002.01086.x
Costantini, A., Picardi, A., Brunetti, S., Trabucchi, G., Bersani, F. S., Minichino, A., et al. (2013). La versione italiana della Demoralization Scale: uno studio di validazione [Italian version of Demoralization Scale: a validation study]. Rivista Psichiatr. 48, 234–239. doi: 10.1708/1292.14291
Costanza, A., Baertschi, M., Richard-Lepouriel, H., Weber, K., Berardelli, I., Pompili, M., et al. (2020). Demoralization and its relationship with depression and hopelessness in suicidal patients attending an emergency department. Int. J. Environ. Res. Public Health 17:2232. doi: 10.3390/ijerph17072232
de Figueiredo, J. M., and Frank, J. D. (1982). Subjective incompetence, the clinical hallmark of demoralization. Comp. Psychiatry 23, 353–363. doi: 10.1016/0010-440x(82)90085-2
Ernst, J., Friedrich, M., Vehling, S., Koch, U., and Mehnert-Theuerkauf, A. (2021). Cancer-related distress: how often does it co-occur with a mental disorder? - Results of a secondary analysis. Front. Psychol. 12:660588. doi: 10.3389/fpsyg.2021.660588
Götze, H., Friedrich, M., Taubenheim, S., Dietz, A., Lordick, F., and Mehnert, A. (2020). Depression and anxiety in long-term survivors 5 and 10 years after cancer diagnosis. Support. Care Cancer 28, 211–220. doi: 10.1007/s00520-019-04805-1
Grandi, S., Sirri, L., Tossani, E., and Fava, G. A. (2011). Psychological characterization of demoralization in the setting of heart transplantation. J. Clin. Psychiatry 72, 648–654. doi: 10.4088/JCP.09m05191blu
Grassi, L., Costantini, A., Kissane, D., Brunetti, S., Caruso, R., Piazza, G., et al. (2017). The factor structure and use of the Demoralization Scale (DS-IT) in Italian cancer patients. Psycho-Oncology 26, 1965–1971. doi: 10.1002/pon.4413
Grassi, L., Rossi, E., Sabato, S., Cruciani, G., and Zambelli, M. (2004). Diagnostic criteria for psychosomatic research and psychosocial variables in breast cancer patients. Psychosomatics 45, 483–491. doi: 10.1176/appi.psy.45.6.483
Grassi, L., Sabato, S., Rossi, E., Biancosino, B., and Marmai, L. (2005). Use of the diagnostic criteria for psychosomatic research in oncology. Psychother. Psychosom. 74, 100–107. doi: 10.1159/000083168
Hadnagy, Z., Csikós, A., and Nagy, L. (2012). A demoralizációs skála magyarországi bevezetése, a depresszió és a demoralizáció vizsgálata hospice-betegek körében [Introduction of the demoralization scale in Hungary, a study on demoralization and depression among hospice patients]. Orvosi Hetilap 153, 737–743. doi: 10.1556/OH.2012.29346
Hartung, T. J., Brähler, E., Faller, H., Härter, M., Hinz, A., Johansen, C., et al. (2017). The risk of being depressed is significantly higher in cancer patients than in the general population: prevalence and severity of depressive symptoms across major cancer types. Eur. J. Cancer 72, 46–53. doi: 10.1016/j.ejca.2016.11.017
Hartung, T. J., Friedrich, M., Esser, P., Mehnert, A., Lehmann-Laue, A., Letsch, A., et al. (2021). The German version of the body image scale: validation among a sample of cancer survivors. PsyArXiv [Preprint]. doi: 10.31234/osf.io/wf6q5
Hinz, A., Klein, A. M., Brähler, E., Glaesmer, H., Luck, T., Riedel-Heller, S. G., et al. (2017). Psychometric evaluation of the Generalized Anxiety Disorder Screener GAD-7, based on a large German general population sample. J. Affect. Disord. 210, 338–344. doi: 10.1016/j.jad.2016.12.012
Hopwood, P., Fletcher, I., Lee, A., and Al Ghazal, S. (2001). A body image scale for use with cancer patients. Eur. J. Cancer 37, 189–197. doi: 10.1016/S0959-8049(00)00353-1
Hu, L., and Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 6, 1–55. doi: 10.1080/10705519909540118
Hung, H.-C., Chen, H.-W., Chang, Y.-F., Yang, Y.-C., Liu, C.-L., Hsieh, R.-K., et al. (2010). Evaluation of the reliability and validity of the mandarin version of demoralization scale for cancer patients. J. Int. Med. Taiwan 21, 427–435.
Ignatius, J., and De La Garza, R. (2019). Frequency of demoralization and depression in cancer patients. Gen. Hosp. Psychiatry 60, 137–140. doi: 10.1016/j.genhosppsych.2019.04.013
Katz, R. C., Flasher, L., Cacciapaglia, H., and Nelson, S. (2001). The psychosocial impact of cancer and lupus: a cross validation study that extends the generality of “benefit-finding” in patients with chronic disease. J. Behav. Med. 24, 561–571. doi: 10.1023/a:1012939310459
Kissane, D. W. (2014). Demoralization: a life-preserving diagnosis to make for the severely medically ill. J. Palliative Care 30, 255–258. doi: 10.1177/082585971403000402
Kissane, D. W., Clarke, D. M., and Street, A. F. (2001). Demoralization syndrome-a relevant psychiatric diagnosis for palliative care. J. Palliative Care 17, 12–21.
Kissane, D. W., Wein, S., Love, A., Lee, X. Q., Kee, P. L., and Clarke, D. M. (2004). The Demoralization Scale: a report of its development and preliminary validation. J. Palliative Care 20, 269–276.
Kroenke, K., Spitzer, R. L., and Williams, J. B. (2001). The PHQ-9: validity of a brief depression severity measure. J. Gen. Int. Med. 16, 606–613. doi: 10.1046/j.1525-1497.2001.016009606.x
Lee, C.-Y., Fang, C.-K., Yang, Y.-C., Liu, C.-L., Leu, Y.-S., Wang, T.-E., et al. (2012). Demoralization syndrome among cancer outpatients in Taiwan. Support. Care Cancer 20, 2259–2267. doi: 10.1007/s00520-011-1332-4
Löwe, B., Wahl, I., Rose, M., Spitzer, C., Glaesmer, H., Wingenfeld, K., et al. (2010). A 4-item measure of depression and anxiety: validation and standardization of the Patient Health Questionnaire-4 (PHQ-4) in the general population. J. Affect. Disord. 122, 86–95. doi: 10.1016/j.jad.2009.06.019
McFarland, D. C., Walsh, L., Napolitano, S., Morita, J., and Jaiswal, R. (2019). Suicide in patients with cancer: identifying the risk factors. Oncology 33, 221–226.
Mehnert, A., Brähler, E., Faller, H., Härter, M., Keller, M., Schulz, H., et al. (2014). Four-week prevalence of mental disorders in patients with cancer across major tumor entities. J. Clin. Oncol. 32, 3540–3546. doi: 10.1200/JCO.2014.56.0086
Mehnert, A., Hartung, T. J., Friedrich, M., Vehling, S., Brähler, E., Härter, M., et al. (2018). One in two cancer patients is significantly distressed: prevalence and indicators of distress. Psycho-Oncology 27, 75–82. doi: 10.1002/pon.4464
Mehnert, A., Müller, D., Lehmann, C., and Koch, U. (2006). Die deutsche Version des NCCN Distress-Thermometers [The German version of the NCCN Distress Thermometer: validation of a screening instrument for assessment of psychosocial distress in cancer patients]. Zeitschrift Psychiatr. Psychol. Psychother. 54, 213–223. doi: 10.1024/1661-4747.54.3.213
Mehnert, A., Vehling, S., Höcker, A., Lehmann, C., and Koch, U. (2011). Demoralization and depression in patients with advanced cancer: validation of the German version of the demoralization scale. J. Pain Symptom Manage. 42, 768–776. doi: 10.1016/j.jpainsymman.2011.02.013
Mullane, M., Dooley, B., Tiernan, E., and Bates, U. (2009). Validation of the Demoralization Scale in an Irish advanced cancer sample. Palliative Support. Care 7, 323–330. doi: 10.1017/S1478951509990253
Nanni, M. G., Caruso, R., Travado, L., Ventura, C., Palma, A., Berardi, A. M., et al. (2018). Relationship of demoralization with anxiety, depression, and quality of life: a Southern European study of Italian and Portuguese cancer patients. Psycho-Oncology 27, 2616–2622. doi: 10.1002/pon.4824
Pitman, A., Suleman, S., Hyde, N., and Hodgkiss, A. (2018). Depression and anxiety in patients with cancer. BMJ (Clinical Research Ed.) 361:k1415. doi: 10.1136/bmj.k1415
Quintero Garzón, L., Hinz, A., Koranyi, S., and Mehnert-Theuerkauf, A. (2021). Norm values and psychometric properties of the 24-Item Demoralization Scale (DS-I) in a representative sample of the German general population. Front. Psychol. 12:681977. doi: 10.3389/fpsyg.2021.681977
Quintero Garzón, L., Koranyi, S., Engelmann, D., Philipp, R., Scheffold, K., Schulz-Kindermann, F., et al. (2018). Perceived doctor-patient relationship and its association with demoralization in patients with advanced cancer. Psycho-Oncology 27, 2587–2593. doi: 10.1002/pon.4823
Rafanelli, C., Guidi, J., Gostoli, S., Tomba, E., Porcelli, P., and Grandi, S. (2013). Subtyping demoralization in the medically ill by cluster analysis. Eur. J. Psychiatry 27, 7–17. doi: 10.4321/S0213-61632013000100002
Robinson, S., Kissane, D. W., Brooker, J., and Burney, S. (2015). A systematic review of the demoralization syndrome in individuals with progressive disease and cancer: a decade of research. J. Pain Symptom Manage. 49, 595–610. doi: 10.1016/j.jpainsymman.2014.07.008
Robinson, S., Kissane, D. W., Brooker, J., Hempton, C., Michael, N., Fischer, J., et al. (2016a). Refinement and revalidation of the Demoralization Scale: the DS-II - external validity. Cancer 122, 2260–2267. doi: 10.1002/cncr.30012
Robinson, S., Kissane, D. W., Brooker, J., Michael, N., Fischer, J., Franco, M., et al. (2016b). Refinement and revalidation of the Demoralization Scale: the DS-II - internal validity. Cancer 122, 2251–2259. doi: 10.1002/cncr.30015
Robinson, S., Kissane, D. W., Brooker, J., and Burney, S. (2016c). A review of the construct of demoralization: history, definitions, and future directions for palliative care. Am. J. Hospice Palliative Care 33, 93–101. doi: 10.1177/1049909114553461
Rzeszut, M., and Assael, R. (2021). Differentiating depression from demoralization in organ transplantation recipients. Prog. Transpl. 31, 88–90. doi: 10.1177/1526924820978602
Schermelleh-Engel, K., Moosbrugger, H., and Müller, H. (2003). Evaluating the fit of structural equation models: tests of significance and descriptive goodness-of-fit measures. Methods Psychol. Res. 8, 23–74.
Sousa, V. D., and Rojjanasrirat, W. (2011). Translation, adaptation and validation of instruments or scales for use in cross-cultural health care research: a clear and user-friendly guideline. J. Eval. Clin. Pract. 17, 268–274. doi: 10.1111/j.1365-2753.2010.01434.x
Tang, L., Li, Z., and Pang, Y. (2020). The differences and the relationship between demoralization and depression in Chinese cancer patients. Psycho-Oncology 29, 532–538. doi: 10.1002/pon.5296
Tang, P.-L., Wang, H.-H., and Chou, F.-H. (2015). A systematic review and meta-analysis of demoralization and depression in patients with cancer. Psychosomatics 56, 634–643. doi: 10.1016/j.psym.2015.06.005
Vehling, S., Kissane, D. W., Lo, C., Glaesmer, H., Hartung, T. J., Rodin, G., et al. (2017). The association of demoralization with mental disorders and suicidal ideation in patients with cancer. Cancer 123, 3394–3401. doi: 10.1002/cncr.30749
Vehling, S., Lehmann, C., Oechsle, K., Bokemeyer, C., Krüll, A., Koch, U., et al. (2011). Global meaning and meaning-related life attitudes: exploring their role in predicting depression, anxiety, and demoralization in cancer patients. Support. Care Cancer 19, 513–520. doi: 10.1007/s00520-010-0845-6
Vehling, S., Lehmann, C., Oechsle, K., Bokemeyer, C., Krüll, A., Koch, U., et al. (2012). Is advanced cancer associated with demoralization and lower global meaning? The role of tumor stage and physical problems in explaining existential distress in cancer patients. Psycho-Oncology 21, 54–63. doi: 10.1002/pon.1866
Vehling, S., Oechsle, K., Koch, U., and Mehnert, A. (2013). Receiving palliative treatment moderates the effect of age and gender on demoralization in patients with cancer. PLoS One 8:e59417. doi: 10.1371/journal.pone.0059417
Keywords: psychometrics, validation study, confirmatory factor analysis, demoralization, neoplasm
Citation: Koranyi S, Hinz A, Hufeld JM, Hartung TJ, Quintero Garzón L, Fendel U, Letsch A, Rose M, Esser P and Mehnert-Theuerkauf A (2021) Psychometric Evaluation of the German Version of the Demoralization Scale-II and the Association Between Demoralization, Sociodemographic, Disease- and Treatment-Related Factors in Patients With Cancer. Front. Psychol. 12:789793. doi: 10.3389/fpsyg.2021.789793
Received: 05 October 2021; Accepted: 01 November 2021;
Published: 24 November 2021.
Edited by:
Andreas Dinkel, Technical University of Munich, GermanyReviewed by:
John De Figueiredo, Yale University, United StatesCristiane Decat Bergerot, Cancer Center of Brasilia (CETTRO), Brazil
Copyright © 2021 Koranyi, Hinz, Hufeld, Hartung, Quintero Garzón, Fendel, Letsch, Rose, Esser and Mehnert-Theuerkauf. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Susan Koranyi, c3VzYW4ua29yYW55aUBtZWRpemluLnVuaS1sZWlwemlnLmRl