 Melissa B. Manus1,2
Melissa B. Manus1,2- 1Manitoba Interdisciplinary Lactation Centre (MILC), Children’s Hospital Research Institute of Manitoba (CHRIM), Winnipeg, MB, Canada
- 2Department of Pediatrics and Child Health, University of Manitoba, Winnipeg, MB, Canada
Breastfeeding supplies infant gut bacteria with human milk oligosaccharides (HMOs) as a nutrient source. HMO profiles are influenced by the FUT2 gene, which encodes an enzyme affecting the fucosylation of milk sugars. 20 to 40% of individuals have a “non-secretor” polymorphism that inactivates the FUT2 gene, resulting in variable HMO proportions in milk. This has engendered a concerning, yet unfounded, perception that non-secretor milk is “inferior.” To address this untested hypothesis, we re-analyzed two datasets in which we previously showed that breastfeeding was protective against early life asthma and excessive infant weight gain in the Canadian CHILD Cohort Study. Using stratified regression models, we found that the protective association of exclusive breastfeeding and infant asthma was not modified by maternal secretor status (secretors aOR: 0.53, 95% CI 0.31 to 0.92; non-secretors aOR: 0.36, 95% CI 0.12 to 1.04; p for interaction = 0.50, N = 2086 children). Similarly, the association of breastfeeding with lower infant BMI and weight gain velocity did not vary by maternal secretor status (infant BMI: secretors aβ −0.47, 95% CI −0.66 to −0.29; non-secretors aβ −0.46, 95% CI −0.78 to −0.13; p for interaction = 0.60; N = 1971 infants). Our results indicate that secretor and non-secretor mothers can equally promote infant growth and respiratory health through breastfeeding. These findings run contrary to the idea that non-secretor milk is an inferior food source, and instead reify the importance of breastfeeding for all infants. The results of this study can inform feeding recommendations that are applicable to all infants, regardless of maternal secretor status.
Introduction
Breastfeeding provides myriad benefits to infants, including supplying infant gut bacteria with human milk oligosaccharides (HMOs) as a nutrient source (1). HMO profiles are strongly influenced by the FUT2 gene, which encodes an enzyme that affects the fucosylation of milk sugars (2). Globally, 20% to 40% of individuals (3) have a “non-secretor” polymorphism that inactivates the FUT2 gene. These individuals display altered enzymatic activity and a distinct milk profile that is enriched with certain HMOs, yet contains lower proportions of others (4). One HMO in particular, 2′-fucosyllactose (2’FL), is virtually absent in the milk of non-secretors (4). In contrast, 2’FL is typically the most abundant HMO in secretor milk.
Alongside growing interest in HMOs and their role in infant development, there is a concerning and largely unfounded perception that non-secretor milk is somehow “inferior (5).” In one study, the consumption of non-secretor milk was associated with delayed infant gut colonization by HMO-utilizing bacteria that are critical for immune system development (6), though other studies have failed to find associations between maternal secretor status and infant gut bacterial communities (7). Alongside variation in the gut microbiome based on maternal secretor status, evidence of a relationship between 2’FL exposure and infant cognitive development (8) has led to the speculation that non-secretor milk is “deficient.” However, the hypothesis that non-secretor milk is an inferior food source for infants has not been fully tested. These data are essential to informing public health messaging and research priorities related to maternal secretor status, infant feeding, and health. To address this gap, we re-analyzed two datasets in which we previously showed that breastfeeding was protective against early life asthma and excessive infant weight gain. The current analysis was motivated by the central question: are the benefits of breastfeeding dependent on maternal secretor status?
Methods
Study population
We leveraged data from two previously published studies that explored associations between infant feeding mode and asthma at 3 years (9), as well as BMI z score and weight gain velocity at 1 year (10) in the Canadian CHILD Cohort Study. This research was approved by the Human Research Ethics Boards at McMaster University and the Universities of Manitoba, Alberta, Toronto, and British Columbia.
Secretor status, asthma diagnosis, and infant body mass index
Secretor status was defined using the methods in Moossavi et al. (11), for genotyping of the rs601338 and rs1047781 single nucleotide polymorphism in the fucosyl-transferase 2 (FUT2) gene. Asthma at 3 years of age was diagnosed (as possible or probable) by a healthcare professional, using medical history and physical examination (9). The diagnosis of “possible or probable asthma” reflects the fact that a firm asthma diagnosis is generally not possible until later in childhood. Body mass index was determined from weight and length measured by CHILD Study staff at the 12-month clinical assessment (10). Since measures of underweight, including stunting and wasting, are not common in this infant population (as evidence by the positive median z-scores), lower z-scores (i.e., closer to zero) in the current study indicate healthier body composition and weight gain trajectories. Weight gain velocity was calculated as the change in weight for age z-score during the period from birth to 12 months.
Statistical analysis
We used base packages in R to clean and subset the data, allowing model stratification by maternal secretor status. The glm function within the stats package (12) was used to stratify regression models that included infant feeding mode as the exposure and either asthma diagnosis, BMI z score, or weight gain velocity as the outcome. We also formally tested for interactions between maternal secretor status and infant feeding mode for asthma at 3 years (logistic regression) and BMI z score and weight gain velocity at 1 year (linear regression). All models were adjusted for the same covariates used in the original studies (9, 10). Unadjusted model results are presented in Supplementary Figures S1, S2. All plots were generated using the ggplot2 package (13). The figures display frequency data within the CHILD study, where participants represent a sample of the Canadian population. Since error bars help to visualize the (un)certainty in this estimate, they were calculated and included in the figures as a representation of the confidence intervals associated with sub-sampling from a larger population (9).
Results
We found no evidence of an interaction between infant feeding mode and maternal secretor status for any of the health outcomes. The protective association of exclusive breastfeeding with asthma was not modified by maternal secretor status (p for interaction = 0.50; N = 2086 children) (Figure 1). Adjusting for covariates, infants exclusively breastfed by secretor mothers showed a 47% reduction in the risk of asthma at 3 years (aOR: 0.53, 95% CI 0.31 to 0.92) compared to infants who received only formula. Similarly, exclusively breastfed infants of non-secretor mothers displayed a 64% reduction in the risk of asthma at 3 years (aOR: 0.36, 95% CI 0.12 to 1.04). The unadjusted models produced similar results (secretor mothers: OR: 0.48, 95% CI 0.29 to 0.77; non-secretor mothers: OR: 0.56, 95% CI 0.23 to 1.40) (Supplementary Figure S1).
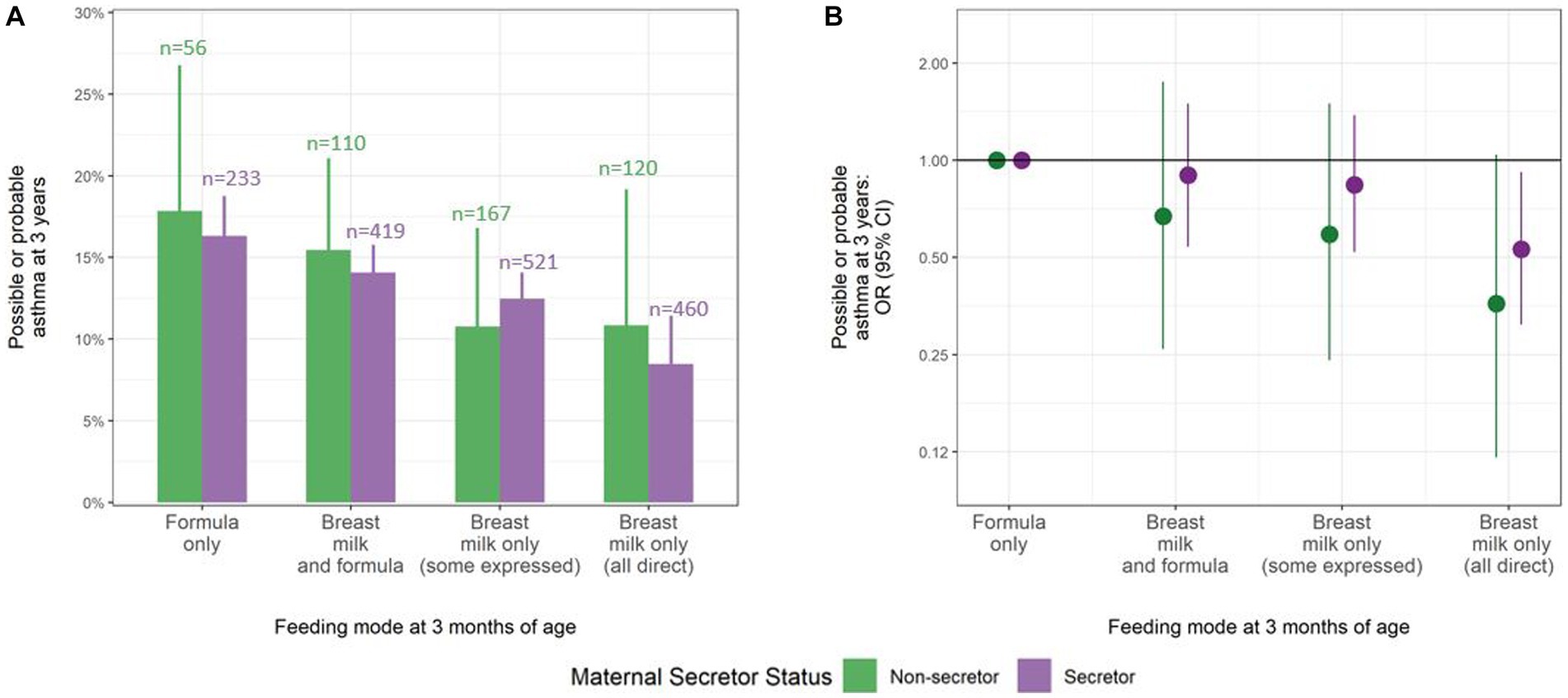
Figure 1. Consistent protective association between breastfeeding at 3 months and possible or probable asthma at 3 years, regardless of maternal secretor status. (A) Frequency of possible or probable asthma at 3 years by feeding mode at 3 months (total N = 2086). The values above the bars indicate the number of children in each feeding group, stratified by maternal secretor status. (B) Adjusted odds ratios (ORs) of possible or probable asthma at 3 years by feeding mode at 3 months. ORs adjusted for infant sex, maternal asthma, ethnicity, method of birth, daycare attendance, and gestational age, with multiple imputation of missing data. Lines represent 95% confidence intervals that display the (un)certainty in sub-sampling study participants from a larger population.
Similarly, the association of breastfeeding with healthier (lower) infant BMI and weight gain velocity did not vary by maternal secretor status (p for interaction = 0.60 and 0.81; N = 1971 and 1955 infants, respectively) (Figure 2). For example, in covariate-adjusted models, infants exclusively breastfed by a secretor mother had a 0.47 SD lower BMI z-score (aβ −0.47, 95% CI −0.66 to −0.29) compared to formula fed infants; virtually identical to the effect estimate for those exclusively breastfed by a non-secretor mother (aβ −0.46, 95% CI −0.78 to −0.13). The unadjusted models showed similar results (secretor mothers: β −0.59, 95% CI −0.77 to −0.42; non-secretor mothers: β −0.51, 95% CI −0.83 to −0.19) (Supplementary Figure S2).
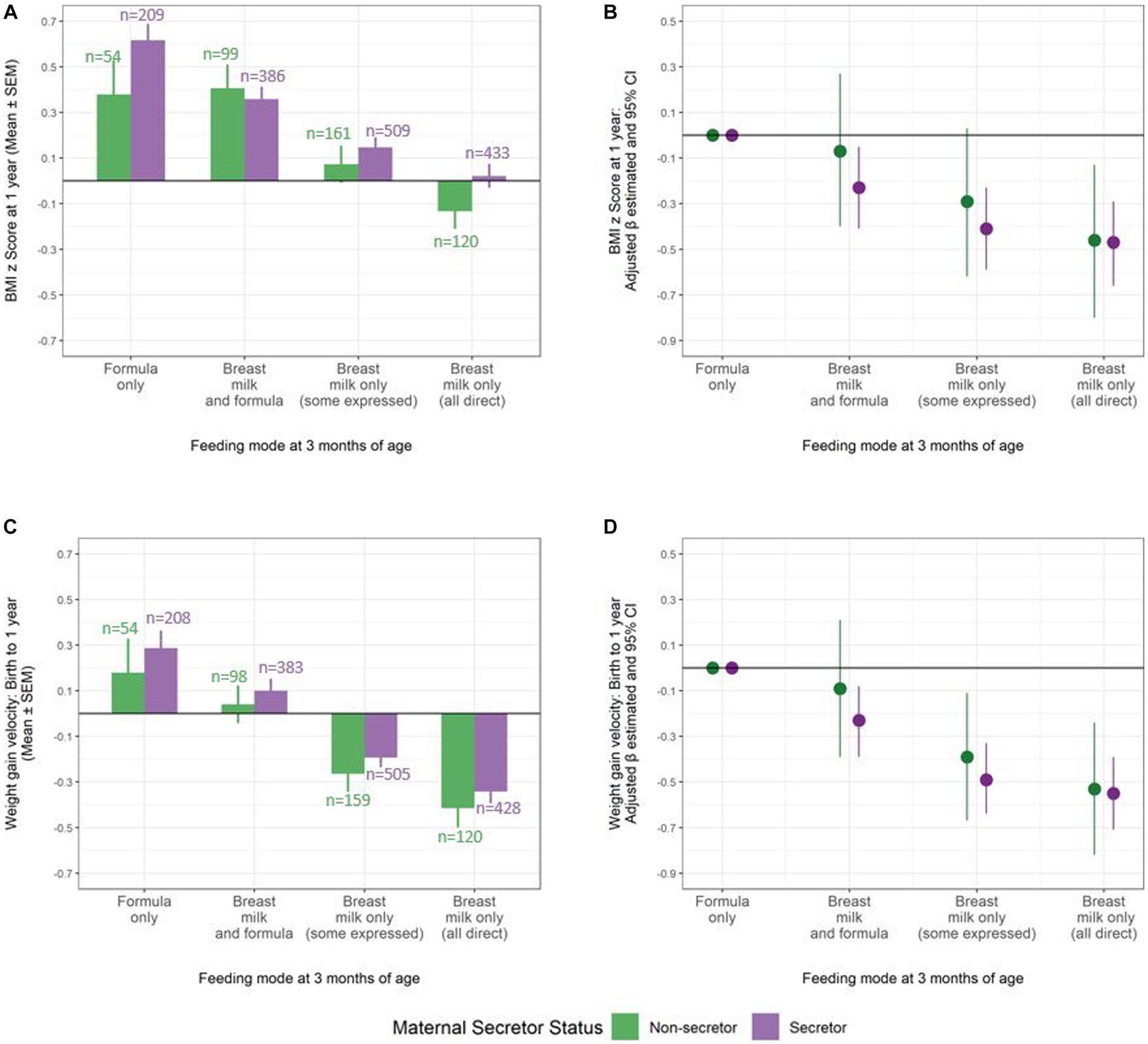
Figure 2. Consistent beneficial association of breastfeeding at 3 months with BMI z score and infant weight gain velocity at 1 year, regardless of maternal secretor status. (A) Mean BMI z score and (B) adjusted β estimates for BMI z score by infant feeding mode at 3 months (N = 1971 dyads). (C) Mean weight gain velocity and (D) adjusted β estimates for weight gain velocity by infant feeding mode at 3 months (N = 1955 dyads). Models adjusted for study site, maternal age, pre-pregnancy BMI, ethnicity, education, marital status, smoking during pregnancy, mode of delivery, parity, infant sex, gestational age, and birth weight. Lines represent 95% confidence intervals that display the (un)certainty in sub-sampling study participants from a larger population.
Discussion
We provide new evidence that the benefits of breastfeeding related to infant weight gain, body composition, and early childhood asthma are not dependent on maternal secretor status. Compared to receiving secretor milk, the consumption of non-secretor milk appears to provide a similar degree of dose-dependent protection against asthma and infant overweight. These data run contrary to the idea that non-secretor milk is an inferior food source for infants, and instead reify the importance of breastfeeding, regardless of maternal secretor status.
Further research should explore these associations in relation to other health outcomes and feeding scenarios. For example, data from the UK ALSPAC cohort suggest potentially enhanced protective effects of non-secretor milk against infant diarrhea (14). It will be particularly important to explore this relationship in contexts where infant mortality due to infectious disease remains high, as infections may provide selection pressure on the non-secretor polymorphism in these settings. Additionally, studies should further explore the connections between specific HMOs, the infant gut microbiome, and health outcomes in early life. Key bacterial colonizers, such as Bifidobacterium, may be able to utilize a range of HMOs beyond 2’FL (11). If so, then the benefits of breastfeeding that are likely mediated by the infant gut microbiome— including those explored in the current study (15, 16)— may extend to all breastfeeding infants, regardless of maternal secretor status and the associated abundance of 2’FL in milk.
Maternal secretor status may also be relevant to human donor milk, where the HMO profile of the pregnant person may not match the HMO profile of donor milk consumed postnatally. With evidence of fetal exposure to HMOs, including 2’FL, in amniotic fluid (17), infants may be primed to receive a specific amount or profile of HMOs in utero. While additional research is needed to understand the mechanisms and consequences of fetal exposure to HMOs, evidence of this phenomenon is in line with the Developmental Origins of Health and Disease literature, which posits that intrauterine exposure to bioactive molecules has a profound impact on birth outcomes and infant physiology (18). In the context of maternal secretor status, it may be that HMOs in amniotic fluid provide a “signal” of the composition of milk to which the infant will be exposed postnatally. Additional research on potential discordance between HMO exposure before and after birth is warranted. Future research should also consider the influence of infant secretor status on health outcomes (19), including the potential biological impacts of “mismatched” maternal–infant secretor status.
Overall, our current results indicate that secretor and non-secretor mothers can equally promote infant growth and protect against asthma through breastfeeding. These findings can inform feeding recommendations that are applicable to all infants, independent of maternal secretor status.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: data will be made available upon request from the CHILD Cohort Study as described at https://childstudy.ca/for-researchers/data-access/. Requests to access these datasets should be directed to child@mcmaster.ca.
Ethics statement
The studies involving humans were approved by The Human Research Ethics Boards at McMaster University and the Universities of Manitoba, Alberta, Toronto, and British Columbia. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
MA conceptualized and designed the study, and critically reviewed and revised the manuscript. MM drafted the initial manuscript and critically reviewed and revised the manuscript. SG carried out the initial analyses and critically reviewed and revised the manuscript. All authors contributed to the article and approved the submitted version.
Funding
The CHILD Cohort Study was funded by the Canadian Institutes of Health Research and supported by the Allergy, Genes and Environment Network of Centres of Excellence (AllerGen NCE). No additional funding was received for this secondary analysis. MA is supported by the Canada Research Chairs program and is a Fellow of the Canadian Institute for Advanced Research (CIFAR) Humans and the Microbiome Program.
Conflict of interest
MA receives research funding from the Canadian Institutes of Health Research, Research Manitoba, the Canada Foundation for Innovation, the Bill and Melinda Gates Foundation, the Manitoba Children’s Hospital Foundation, Prolacta Biosciences, Mitacs, CIFAR and the Garfield G. Weston Foundation. She regularly speaks at conferences and workshops on infant nutrition, some sponsored by Medela, the Institute for the Advancement of Breastfeeding & Lactation Education and Prolacta Biosciences. She has contributed without remuneration to online courses on breast milk and the infant microbiome produced by Microbiome Courses.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2023.1203552/full#supplementary-material
References
1. Lyons, KE, Ryan, CA, Dempsey, EM, Ross, RP, and Stanton, C. Breast Milk, a source of beneficial microbes and associated benefits for infant health. Nutrients. (2020) 12:1039. doi: 10.3390/nu12041039
2. Castanys-Muñoz, E, Martin, MJ, and Prieto, PA. 2′-fucosyllactose: an abundant, genetically determined soluble glycan present in human milk. Nutr Rev. (2013) 71:773–89. doi: 10.1111/nure.12079
3. Totten, SM, Zivkovic, AM, Wu, S, Ngyuen, U, Freeman, SL, Ruhaak, LR, et al. Comprehensive profiles of human Milk oligosaccharides yield highly sensitive and specific markers for determining secretor status in lactating mothers. J Proteome Res. (2012) 11:6124–33. doi: 10.1021/pr300769g
4. Azad, MB, Robertson, B, Atakora, F, Becker, AB, Subbarao, P, Moraes, TJ, et al. Human Milk oligosaccharide concentrations are associated with multiple fixed and modifiable maternal characteristics, environmental factors, and feeding practices. J Nutr. (2018) 148:1733–42. doi: 10.1093/jn/nxy175
5. Hao, H, Zhu, L, and Faden, HS. The milk-based diet of infancy and the gut microbiome. Gastroenterol Rep (Oxf). (2019) 7:246–9. doi: 10.1093/gastro/goz031
6. Lewis, ZT, Totten, SM, Smilowitz, JT, Popovic, M, Parker, E, Lemay, DG, et al. Maternal fucosyltransferase 2 status affects the gut bifidobacterial communities of breastfed infants. Microbiome. (2015) 3:13. doi: 10.1186/s40168-015-0071-z
7. Lewis, ZT, Sidamonidze, K, Tsaturyan, V, Tsereteli, D, Khachidze, N, Pepoyan, A, et al. The Fecal microbial Community of Breast-fed Infants from Armenia and Georgia. Sci Rep. (2017) 7:40932. doi: 10.1038/srep40932
8. Berger, PK, Plows, JF, Jones, RB, Alderete, TL, Yonemitsu, C, Poulsen, M, et al. Human milk oligosaccharide 2′-fucosyllactose links feedings at 1 month to cognitive development at 24 months in infants of normal and overweight mothers. PLoS One. (2020) 15:e0228323. doi: 10.1371/journal.pone.0228323
9. Klopp, A, Vehling, L, Becker, AB, Subbarao, P, Mandhane, PJ, Turvey, SE, et al. Modes of infant feeding and the risk of childhood asthma: a prospective birth cohort study. J Pediatr. (2017) 190:192–199.e2. doi: 10.1016/j.jpeds.2017.07.012
10. Azad, MB, Vehling, L, Chan, D, Klopp, A, Nickel, NC, JM, MG, et al. Infant feeding and weight gain: separating breast Milk from breastfeeding and formula from food. Pediatrics. (2018) 142:e20181092. doi: 10.1542/peds.2018-1092
11. Moossavi, S, Atakora, F, Miliku, K, Sepehri, S, Robertson, B, Duan, QL, et al. Integrated analysis of human Milk microbiota with oligosaccharides and fatty acids in the CHILD cohort. Front Nutr. (2019) 6:58. doi: 10.3389/fnut.2019.00058
12. R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. (2022). Available at: https://www.R-project.org/)
13. Wickham, H. ggplot2: Elegant graphics for data analysis. Springer-Verlag New York. (2016). Available at: http://ggplot2.org.
14. Muthumuni, D, Miliku, K, Wade, KH, Timpson, NJ, and Azad, MB. Enhanced protection against Diarrhea among breastfed infants of nonsecretor mothers. Pediatr Infect Dis J. (2021) 40:260–3. doi: 10.1097/INF.0000000000003014
15. Dai, DLY, Petersen, C, Hoskinson, C, Del Bel, KL, Becker, AB, Moraes, TJ, et al. Breastfeeding enrichment of B. longum subsp. infantis mitigates the effect of antibiotics on the microbiota and childhood asthma risk. Med clinical. Advances. (2023) 4:92–112. doi: 10.1016/j.medj.2022.12.002
16. Granger, CL, Embleton, ND, Palmer, JM, Lamb, CA, Berrington, JE, and Stewart, CJ. Maternal breastmilk, infant gut microbiome and the impact on preterm infant health. Acta Paediatr. (2021) 110:450–7. doi: 10.1111/apa.15534
17. Wise, A, Robertson, B, Choudhury, B, Rautava, S, Isolauri, E, Salminen, S, et al. Infants are exposed to human Milk oligosaccharides already in utero. Frontiers. Pediatrics. (2018):6. doi: 10.3389/fped.2018/00270
18. Gluckman, PD, Hanson, MA, and Buklijas, T. A conceptual framework for the developmental origins of health and disease. J Dev Orig Health Dis. (2010) 1:6–18. doi: 10.1017/S2040174409990171
Keywords: infant feeding, human milk, maternal secretor status, infant asthma, infant weight gain
Citation: Manus MB, Goguen SK and Azad MB (2023) The protective associations of breastfeeding with infant overweight and asthma are not dependent on maternal FUT2 secretor status. Front. Nutr. 10:1203552. doi: 10.3389/fnut.2023.1203552
Edited by:
Daniel W. Sellen, University of Toronto, CanadaReviewed by:
Martin Frederik Laursen, Technical University of Denmark, DenmarkSercan Karav, Çanakkale Onsekiz Mart University, Türkiye
Copyright © 2023 Manus, Goguen and Azad. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Meghan B. Azad, Meghan.Azad@umanitoba.ca