
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Bioeng. Biotechnol., 14 March 2025
Sec. Biomechanics
Volume 13 - 2025 | https://doi.org/10.3389/fbioe.2025.1533001
This article is part of the Research TopicExoskeleton Gait TrainingView all 10 articles
 Sridevi Nagaraja1,2
Sridevi Nagaraja1,2 Jose E. Rubio1,2
Jose E. Rubio1,2 Junfei Tong1,2
Junfei Tong1,2 Aravind Sundaramurthy1,2Anup Pant1,2
Aravind Sundaramurthy1,2Anup Pant1,2 Meredith K. Owen3
Meredith K. Owen3 Michael A. Samaan4Brian Noehren3
Michael A. Samaan4Brian Noehren3 Jaques Reifman1*
Jaques Reifman1*Active lower-body exoskeleton devices can decrease the energy requirement of the human body by providing mechanical assistance to lower-body muscles. However, they also alter gait kinematics and kinetics, and it is not well understood whether such alterations are detrimental or beneficial to the human body. In this pilot study, we investigated the impact of walking with an ankle exoskeleton device on the biomechanics of men while carrying a heavy load. We collected computed tomography images and motion-capture data for five young, healthy men who walked 5 km (∼60 min) with a 22.7-kg load, with and without an active ankle exoskeleton (the ExoBoot EB60). We developed personalized musculoskeletal models and calculated the joint kinematics and kinetics for each participant under each walking condition. Without the ExoBoot, at 5 km compared to 0 km, on average, the peak trunk flexion angle increased by ∼35% and the stride length increased by ∼3.5%. In contrast, with the ExoBoot, the magnitude of the corresponding increases was smaller (∼16% and ∼2%, respectively). After the 5-km walk, compared to walking without the ExoBoot, its use considerably altered hip-related biomechanical parameters, e.g., it increased hip abduction angle by ∼17%, increased hip flexion moment by ∼3.5%, and decreased hip adduction moment by ∼19%. Finally, irrespective of distance, ExoBoot use significantly increased the stance duration and peak ankle plantarflexion angle (p < 0.001). Overall, the use of the ExoBoot induced beneficial alterations in stride length and trunk-, ankle-, and hip-related parameters for men walking with load carriage. The quantitative analysis provided by this pilot study should help guide future investigations and inform the development of standards for safe and effective use of emerging exoskeleton technologies.
Military operations often require Service members to carry heavy loads, which in the U.S. Army typically range from 22.7 to 31.7 kg (Knapik et al., 2012). Such loads have been associated with musculoskeletal injuries of the lower extremities and lower back, affecting Service members’ health and reducing Force Readiness and Lethality (Knapik et al., 2012; Orr et al., 2015; Orr et al., 2017). In fact, musculoskeletal injuries account for more than 2 million medical visits annually, imposing a considerable cost on the military healthcare system (Department of the Army, 2011). Thus, the U.S. Army is continually exploring ways to reduce the incidence of such injuries. For instance, previous studies have found that during strenuous physical activities, such as walking and running with or without load carriage, reducing the stride length decreases the load to the bones, offering an opportunity to help reduce stress-fracture risk to the tibia for both men and women (Willy et al., 2016; Sundaramurthy et al., 2023). As an alternative to modifying the stride length, which requires a conscious effort by the individual, wearable exoskeleton devices offer the potential to enhance an individual’s strength and endurance (Bogue, 2015), allowing Service members to carry heavier loads for longer distances.
Lower-body exoskeleton devices offer a particularly promising solution because they increase mobility, physical endurance, and load-carrying capacity while counteracting overstress on the lower back and legs, allowing Service members to carry a 90.7-kg load while marching at a speed of 4 km/h for up to 20 km (Bogue, 2015). Exoskeleton devices are typically classified as passive or active based on their mechanism of action. Passive exoskeleton devices usually leverage their mechanical design to store and release energy without powered components, however, their ability to control the amount of the enhanced mechanical power is often limited (Lee et al., 2020; Johnson et al., 2023). In contrast, active exoskeleton devices assist the wearer through powered actuation via electronic control systems and offer a higher degree of mechanical-power modulation under different conditions. Indeed, many emerging active lower-limb exoskeleton devices apply torque at either the ankle joint (Sawicki and Ferris, 2008; Malcolm et al., 2013; Mooney et al., 2014a; 2014b; Jackson and Collins, 2015; Mooney and Herr, 2016; Zhang et al., 2017) or the hip joint (Ding et al., 2017; Panizzolo et al., 2019), and operate in tandem with the wearer to augment their walking capacity while carrying heavy loads. Active exoskeleton devices have demonstrated favorable results, including reductions in metabolic energy requirements by up to 14% (Gordon and Ferris, 2007; Sawicki and Ferris, 2009a; Mooney et al., 2014b; Koller et al., 2015; Ding et al., 2017; Zhang et al., 2017; Panizzolo et al., 2019; Sawicki et al., 2020) and reductions in the activation of different muscle groups, such as the soleus and quadriceps, by ∼35% (Gordon and Ferris, 2007; Zhu et al., 2021).
Nevertheless, there is conflicting evidence in the literature as to whether the biomechanical changes induced by exoskeleton devices are beneficial or detrimental to musculoskeletal-injury risk due to walking with load carriage for long periods of time. For example, preliminary experimental studies suggest that exoskeleton use can also affect walking-gait motion (kinematics) and body forces (kinetics), even during short marching periods without additional load (Gregorczyk et al., 2010). Such gait-related changes could lead to unintended musculoskeletal injuries, such as stress fractures, in the lower extremities (van Herpen et al., 2019) or the lower back (Clansey et al., 2012). To date, existing studies that investigated the potential effects of lower-body exoskeleton use with load carriage on walking kinetics and kinematics only focused on their impact on the human body over very short time periods (e.g., less than 10 min, with a maximum walking distance of 1.8 km) (Gregorczyk et al., 2010; Ding et al., 2017). However, load-carriage activities during military operations may last for many hours (Knapik et al., 2012; Department of the Army, 2022). In addition, the exoskeleton devices investigated in these studies provided mechanical power simultaneously at multiple joints, including the hip, ankle, and knee, which prevents us from isolating the effect of the device on a single joint. Studies that were conducted for slightly longer time periods (i.e., up to 30 min, with a maximum walking distance of 2.25 km) and investigated ankle exoskeleton devices either did not involve load carriage (Gordon and Ferris, 2007; Sawicki and Ferris, 2008; 2009a; Malcolm et al., 2013; Mooney et al., 2014b; Koller et al., 2015; Mooney and Herr, 2016; Ingraham et al., 2022; Medrano et al., 2022; Wu et al., 2024) or did not measure or compute gait-related parameters (Mooney et al., 2014a; Zhang et al., 2017; Panizzolo et al., 2019). Thus, previous studies have not considered the important fact that the human body is more susceptible to injury once it is fatigued, such as during the late stages of load carriage (Clansey et al., 2012), preventing us from understanding the true impact of wearing an exoskeleton device for time periods longer than 30 min. Specifically, we do not know to what extent load carriage and walking distance affect exoskeleton-induced alterations, if any, in gait parameters and whether such alterations are detrimental or beneficial to the human body.
Computational modeling complements experimentation and can be used as a tool to characterize the body’s biomechanical responses under various conditions to identify risk factors and assess potential strategies to reduce the risk of musculoskeletal injuries. For example, by developing individualized musculoskeletal models based on experimental data, our U.S. Department of Defense (DoD) team has previously characterized the effects of stature and load carriage on the risk of stress-fracture injury to the tibia in men and women while running or walking (Xu et al., 2016; Xu et al., 2017; Xu et al., 2020; Unnikrishnan et al., 2021; Rubio et al., 2023; Sundaramurthy et al., 2023). In addition, using computational modeling, we have evaluated the impact of dozens of modifiable gait parameters on stress-fracture risk to identify potential mitigation strategies. For instance, for a simulated 10-week U.S. Army Basic Combat Training regimen, we found that reducing stride length by 10% during running decreases the stress-fracture risk to the tibia in healthy, young women by an average of 60% (Sundaramurthy et al., 2023).
To extend the scope of previous assessments of active ankle exoskeleton devices, we designed a pilot study to characterize the effects of a comparatively longer use of an active, wearable ankle exoskeleton (i.e., the ExoBoot EB60; Dephy, Inc., Boxborough, MA) on the walking biomechanics of adult military-age men with load carriage. Compared to previous works, this study was roughly twice as long in distance (i.e., 5 km) and in time duration (i.e., 60 min). Here, we hypothesized that walking with the ExoBoot for 5 km while carrying a 22.7-kg load will have largely beneficial effects on the joint kinematics and kinetics of the lower leg of young, healthy men compared to walking without the device. Towards this end, we developed individualized musculoskeletal models using newly collected experimental data for five men and investigated the changes in the spatiotemporal parameters, kinematics (i.e., the joint angles), and kinetics (i.e., the joint forces and moments) of the lower-extremity joints (i.e., the hip, knee, and ankle) for these participants during walking on a level treadmill for 5 km carrying a 22.7-kg load, with or without wearing the ExoBoot device.
We enrolled five young, healthy men between the ages of 18 and 25 years, as representative of military recruits in accordance with an anthropometric survey of U.S. Army Soldiers (Department of the Army, 2011; Knapik et al., 2012). All participants reported that they were experienced treadmill walkers and free of injuries that would limit their ability to be physically active for at least 3 months prior to participating in the study. The study protocol was approved by the University of Kentucky Institutional Review Board and by the Office of Human Research Oversight of the U.S. Army Medical Research and Development Command, Fort Detrick, MD. Prior to data collection, we obtained a written informed consent from each participant and recorded their age, mass, height, foot length, body fat percentage, and body mass index (BMI) (Table 1). We also collected quantitative computed tomography (CT) images of each participant’s left tibia and lumbar vertebrae segments L4-L5 using a Siemens CT scanner (Siemens Medical Solutions, Malvern, PA) (Figure 1). The scans had an in-plane pixel resolution of 0.49 × 0.49 mm2 and a slice thickness of 0.60 mm. Each CT scan included a calibration phantom of known calcium hydroxyapatite concentration (QRM, Moehrendorf, Germany) in the field of view (Figure 1).

Table 1. Anthropometric characteristics of 5 young, healthy men.

Figure 1. Summary of the integrated experimental and computational study design. We performed a laboratory study on a level treadmill and collected motion-capture (using 52 reflective markers), ground reaction force (GRF), and electromyography (EMG) data from five participants as they walked 5 km with and without an active ankle exoskeleton device (the ExoBoot EB60), while carrying a 22.7-kg load. We collected EMG, GRF, and motion-capture data for 20 s at the baseline (i.e., 0 km) and at every 1-km mark thereafter. We also collected computed tomography (CT) scans of the tibia and lumbar vertebrae L4-L5 from each participant. To develop the computational model, we first incorporated participant-specific anthropometric, tibial, and lumbar spine data into the musculoskeletal model and performed a parameter identification analysis to personalize the model for each participant. Next, we performed kinematic and inverse dynamics simulations for two conditions, i.e., walking with and without the ExoBoot, while carrying the 22.7-kg load. We used the simulation results to compute the GRFs, joint reaction forces, joint angles, and joint moments for each participant under each walking condition.
Each participant completed four walking trials in the same order spread across four separate days. During each trial, participants walked at a constant speed of 1.34 m/s on a leveled instrumented treadmill (Bertec Corporation, Columbus, OH) in the following order: 1) walking without any additional weight and without wearing the ExoBoot, 2) walking with a 22.7-kg load (50 lb) without the ExoBoot, 3) walking without any additional weight while wearing the ExoBoot EB60, and 4) walking with a 22.7-kg load while wearing the ExoBoot EB60. In addition, prior to the first trial with the ExoBoot (i.e., visit 3), each participant completed a training visit to familiarize themselves with walking while wearing the ExoBoot device. During this visit, we performed alignment and adjustments of the shin pad for each participant. Moreover, to ensure that the participants were acclimated to walking with the ExoBoot on a force-plate instrumented treadmill, we allowed them to walk until they reported being comfortable with the device’s assistance for a minimum of 10 min. We did not collect any data during the training visit.
We chose to evaluate an active ankle exoskeleton because preliminary assessments of the ability of lower-body exoskeletons to enhance user mobility conducted by the U.S. Army and other groups have shown promising results (Sawicki and Ferris, 2008; Gregorczyk et al., 2010; Mooney et al., 2014a). In addition, we selected the walking speed of 1.34 m/s as representative of the various foot marches conducted in the U.S. Army (Department of the Army, 2022). For the trials with a 22.7-kg load carriage, participants wore a vest strapped to their upper body with the load symmetrically distributed between the front and back because during foot marches military personnel carry approximately symmetrical loads >90% of the time (Figure 1) (Knapik et al., 2012). For trials with and without the ExoBoot device, participants wore slightly modified military boots with custom carbon-composite inserts embedded in the lateral side of the soles. For the trials with the device, participants wore the ExoBoot EB60 on the lateral side of each leg and rigidly secured them to the shins via a shank attachment and a strap secured just below the tuberosity of the tibia and whose distal ends were attached to the carbon-composite inserts in the boots (Figure 2A). The ExoBoot had an inversion-eversion joint and a plantar-dorsiflexion joint and used a built-in brushless electric motor and flat cable transmission to provide plantarflexion assistance during walking. Specifically, each side of the ExoBoot applied a torque to the participant’s ankle by tightening a strap between the motor and the boot during the push-off portion of the gait cycle to provide a burst of positive power during the terminal stance phase. In addition to the training visit to acclimatize themselves to walking with the ExoBoot, before each trial involving ExoBoot use, participants underwent a warm-up period to calibrate the device-applied torque. We included this warm-up period to ensure that the torque assistance provided to each participant was appropriate for the specific trial (e.g., with load vs. without load). The warm-up calibration period typically consisted of walking approximately 20–30 steps at a consistent pace on a flat surface to determine the amount of torque to be applied, which was dependent on the participant’s gait. After the calibration was complete, the participant-specific torque was applied by ramping it up over the first 3–5 steps (the maximum torque was set to 35 N·m).
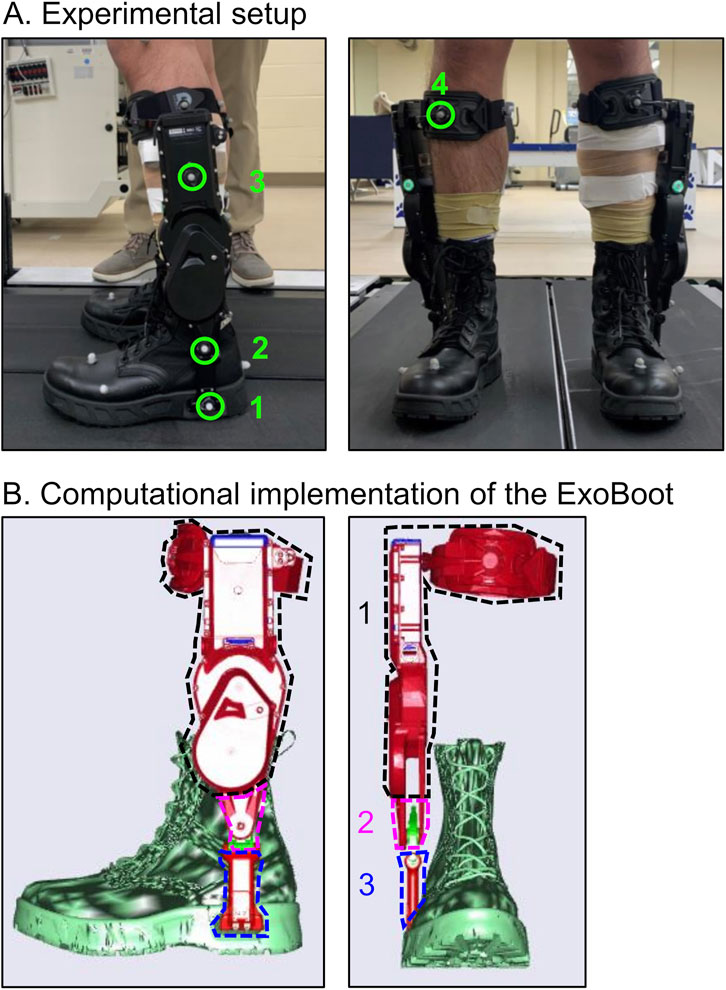
Figure 2. (A) Experimental setup describing the locations of the four optical markers placed on the ExoBoot for motion capture during trials in which participants wore the exoskeleton device: 1) sole where the ExoBoot connected to the boot, 2) ankle joint, 3) below the battery indicator, and 4) anterior part of the shin pad. (B) Implementation of the ExoBoot in the musculoskeletal model as three rigid-body segments. Segment 1 (black dashed line), Segment 2 (pink dashed line), and Segment 3 (blue dashed line) represent the upper, middle, and lower frames of the ExoBoot.
Following warm up for each trial, participants walked 5 km in ∼60 min, during which we collected motion-capture data, ground reaction forces (GRFs), and electromyography (EMG) data for ∼20 s at baseline (i.e., at 0 km) and at each 1-km mark thereafter (Figure 1). In total, we collected 120 s of data during each walking trial. We collected GRF data from the instrumented treadmill (Bertec Corporation, Columbus, OH) and EMG data (Trigno Avanti, Delsys Inc., Natick, MA) from eight major lower-extremity muscles at 2,000 Hz, including the gluteus medius, biceps femoris, vastus lateralis, rectus femoris, vastus medialis, gastrocnemius, soleus, and tibialis anterior. In addition, we continuously collected data from the ExoBoot, including velocity, acceleration, and torque, measured by the device throughout the whole walking trial. We manually flagged the ExoBoot data at every 1-km mark to guarantee synchronization with the force-plate, motion-capture, and EMG data. The data collection length of 20 s provided a sufficient number of strides (∼15–25) to obtain consistent stance and swing durations for all conditions (Rubio et al., 2023; Tong et al., 2023). We collected motion-capture data from 52 reflective markers (Motion Analysis Corporation, Santa Rosa, CA) at a sampling frequency of 200 Hz. We placed the markers bilaterally on anatomical landmarks and segments throughout the body, including the arms, trunk, pelvis, thighs, shanks, and feet. In addition, we placed three tracking markers on the back of each boot to identify the proximal, distal, and lateral heels. We also placed additional tracking markers on the right anterior thigh and shin as well as on the second head of the metatarsal bone to identify the right vs. the left side of the foot (Figure 2). In the trials where participants wore the exoskeleton device, we placed four markers at the following locations on the ExoBoot: 1) on the sole where the ExoBoot connected to the boot, 2) on the ankle joint, 3) below the battery indicator, and 4) on the anterior of the shin pad (Figure 2A). We collected the ExoBoot torque data at 200 Hz.
Similar to our prior studies (Xu et al., 2016; Xu et al., 2017; Xu et al., 2020; Taylor et al., 2021; Unnikrishnan et al., 2021; Rubio et al., 2023; Sundaramurthy et al., 2023), we developed individualized musculoskeletal models using the AnyBody Modeling System (AnyBody Technology, Aalborg, Denmark) to determine the joint kinematics and kinetics for each participant. Briefly, the software provided a generic musculoskeletal model of an average male consisting of rigid segments, including arms, trunk, pelvis, thighs, shanks, and feet, as well as 169 muscles in the lower extremities. To individualize the generic model for each participant, we first morphed the generic tibial and lumbar vertebrae L4-L5 geometry in the AnyBody model to match the participant-specific tibial and lumbar L4-L5 geometry extracted from the CT scan using Mimics (Materialise, Leuven, Belgium). Specifically, we used the automated segmentation in Mimics to segment the bone, followed by a manual refinement to generate a clean tibial and lumbar L4-L5 geometry. Next, we scaled the other segments in the generic musculoskeletal model based on the anthropometric measurements (e.g., mass, height, foot length, and body fat percentage) of each participant. We defined 42 markers in the musculoskeletal model at locations corresponding to where they were placed on the participants during the experimental walking trials.
For trials that involved participants carrying a load or wearing the ExoBoot, we modeled the vest and the ExoBoot as rigid body segments in AnyBody. Specifically, we first modeled the ExoBoot as three rigid body segments (Figure 2B), with a total weight of 12 N, using the material properties (i.e., mass and inertia tensor) provided by the manufacturer. The first segment (Figure 2B, black dashed line) represented the upper frame of the ExoBoot, which we coupled from the center of the knee to the center of the ankle of each leg in the musculoskeletal model. The second and third segments (Figure 2B, pink and blue dashed lines, respectively) represented the lower frames of the ExoBoot, which we coupled from the ankle to the sole of the foot of each leg in the musculoskeletal model. Then, we defined two revolute joints on the ExoBoot, which allowed for ankle rotation around the z-axis (ankle dorsiflexion and plantarflexion) and the x-axis (ankle eversion and inversion) on each foot. Finally, we defined four markers in the musculoskeletal model at locations corresponding to where they were placed on the ExoBoot during the experimental walking trials (Figure 2A).
We applied an optimization scheme that minimized the errors between the markers tracked in the experiment and the markers defined in the model, to further optimize the body segments’ lengths. Once optimized, using the 20-s marker-tracking data collected for each walking trial, we used the participant-specific musculoskeletal model to compute body motion (i.e., the joint angle changes throughout the entire body), including the kinematics of the lower-extremity joints (e.g., hip, knee, and ankle). Finally, we determined the kinetics of the hip, knee, and ankle by performing an inverse dynamics analysis and normalizing the GRFs and joint reaction forces (JRFs) by body weight and the joint moments by body mass. We provided GRFs in the vertical direction relative to the ground because they had by far the highest magnitude.
We used the results of the kinematic and kinetic analyses to determine the impact of two main effects, i.e., walking distance (0 km vs. 5 km) and exoskeleton device use (with ExoBoot vs. without ExoBoot), on the biomechanics of each individual participant. When comparing changes in kinematic and kinetic parameters due to walking distance, both with and without the ExoBoot, we only considered the two trials where participants carried a 22.7-kg load, because the capability to transport heavy loads with ease is one of the potential benefits of exoskeleton devices. For both trials (with and without the ExoBoot), we considered 0 km to be the baseline for comparison purposes. For each participant, using the 20-s GRF data during walking from AnyBody comprising ∼15–20 strides, we first identified the start and end points of each stride (and, hence, the stride duration) at 0 km (i.e., baseline) and at 5 km by using a threshold value of 25 N to identify the peaks in the GRFs. Next, using the start and end points of each stride, we extracted 26 distinct parameters per stride, including spatiotemporal (e.g., stride duration and normalized stride length) as well as joint kinematic and kinetic parameters (e.g., joint angles, moments, and JRFs). Finally, we performed statistical analyses to evaluate changes in these parameters between the different conditions. For these analyses, we resampled the time history of each stride so that strides of different durations (for different participants during different trials) were each represented by 100 values constituting one gait cycle.
Before the study, we performed a power analysis using the G*Power software (v3.1.9.4) to estimate the sample size needed to detect changes in the biomechanical parameters during walking with and without the ExoBoot in young, healthy men. We computed the sample size based on a report by Gregorczyk et al. (2010), which described changes in kinematic and kinetic parameters when participants marched while wearing an exoskeleton suit and carrying a load for 8 min. Because they measured these parameters over a short period compared to ∼60 min in our study, we assumed a larger effect size (ES = 1.00) than the median ES of 0.75 calculated based on their work. Assuming a correlation among repeated measurements of 0.5 and a non-sphericity correction of 1.0, we determined that a sample size of five participants was needed to achieve 80% power at a significance level of 5%.
To determine the impact of walking with the ExoBoot on the biomechanical responses, we first developed linear mixed-effects (LME) models while considering each of the 26 biomechanical parameters as the dependent variable. In the models, we included device use (with ExoBoot or without ExoBoot) and distance (0 km or 5 km) as fixed categorical effects (both with and without a device-distance interaction effect) and the participants as a random effect (intercept only). Next, for each biomechanical parameter (listed in the first column in Table 2), we determined the significance of the interaction effect using the likelihood ratio test. Briefly, for each parameter, we compared the corresponding LME model with and without the device-distance interaction effect. When the interaction effect was not statistically significant, we determined the significance of each fixed effect by comparing the LME model with only one fixed variable (i.e., device or distance) against an LME model without any fixed effect (or an empty model) (Figure 3).
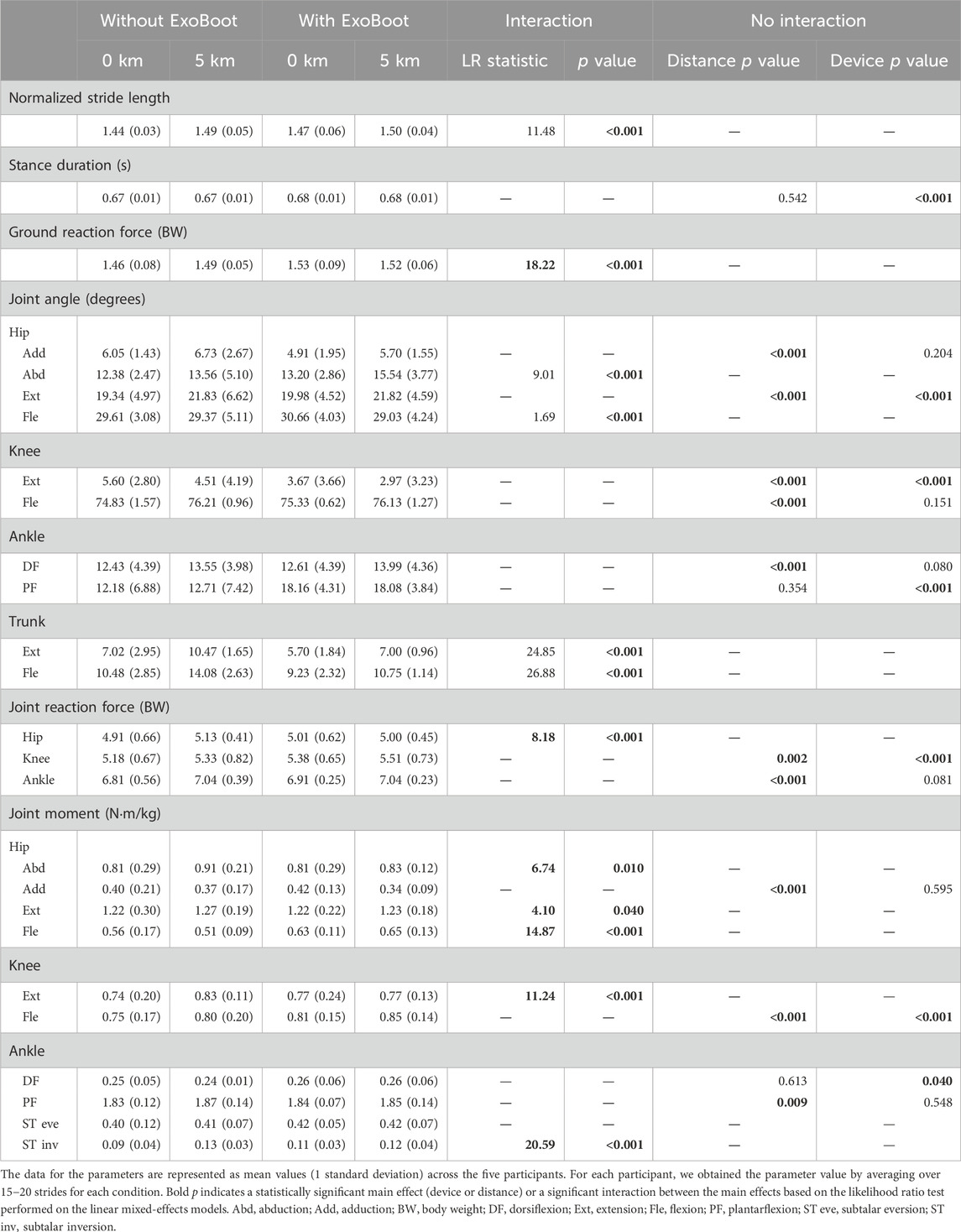
Table 2. Spatiotemporal parameters, peak joint angles, ground reaction force, and joint kinetics.
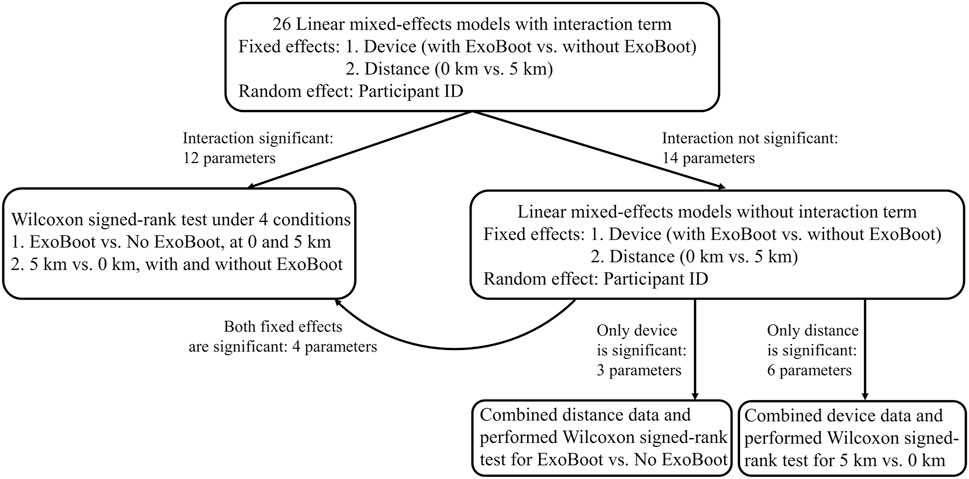
Figure 3. Flowchart of the steps performed to quantitatively assess the impact of wearing the active ankle-powered ExoBoot exoskeleton device on lower-limb biomechanical parameters after walking for 5 km with a 22.7-kg load.
For each of the five participants, using the 20-s data from AnyBody comprising ∼15–20 strides, we first calculated the mean ± standard deviation (SD) of the peak value for each of the 26 computationally derived biomechanical parameters at 0 and 5 km during each of the two walking trials (with and without the ExoBoot device). For the subset of parameters that achieved significance for both the device and distance effects or for their interaction, we performed four pairwise comparisons of their mean values across the five participants using a non-parametric test, the Wilcoxon signed-rank test (Fagerland, 2012), with a Benjamini-Hochberg correction for multiple comparisons (Benjamini and Hochberg, 1995). We compared the two device conditions (i.e., with ExoBoot vs. without ExoBoot) at 0 km and at 5 km and the two distance conditions (i.e., 5 km vs. 0 km) with and without the ExoBoot (Figure 3). For parameters that achieved significance in only one of the fixed effects (device or distance), we grouped the data for the non-significant effect and performed a Wilcoxon signed-rank test to compare the mean values of the significant effect across the five participants. Given the small sample size (N = 5) of our study and that the derived biomechanical parameters included instances of normally and not-normally distributed parameters, we chose to use a non-parametric, distribution-free test to circumvent the possibility of violating the assumption of normality while still having sufficient power to identify differences in each parameter between two dependent samples.
Finally, we also calculated the ES (i.e., Cohen’s d) (Lakens, 2013) to evaluate differences in the means of each of the 26 biomechanical parameters between the two device conditions (i.e., with ExoBoot vs. without ExoBoot) at 0 km and 5 km and between the two distance conditions (i.e., 5 km vs. 0 km) with and without wearing the ExoBoot. We performed the statistical analyses for the LME models using the RStudio v1.4 statistical software, including the lme4, lmerTest, and emmeans packages, with an alpha level of 0.05. We performed the Wilcoxon signed-rank test using the signrank function with an alpha level of 0.05 and calculated Cohen’s d using the meanEffectsize function in MATLAB R2022b (MathWorks, Natick, MA).
To assess the validity of the musculoskeletal models, we qualitatively compared the time courses of the predicted muscle activity with the EMG recordings at 0 km when the participants did not carry any load and did not wear the ExoBoot. We did not perform a quantitative comparison because the model-predicted muscle activity and the experimentally measured EMG do not represent the same quantity. Specifically, the EMG provides a measure of muscle electrical activity in response to a nerve’s stimulation, whereas in the computational model we computed muscle activity as the force generated within a muscle for a particular motion divided by its maximum strength. Thus, while the EMG and muscle activity are distinct quantities, they both indicate the level of muscle activation and can be qualitatively compared. Specifically, we chose to perform the comparison for three muscle groups, i.e., tibialis anterior, rectus femoris, and gluteus medius, to ensure we included different muscle groups that are activated during both the swing and stance phases of a gait cycle. For this comparison, we normalized the EMG and muscle activity values in each stride by their maximum values. This allowed us to qualitatively compare when a particular muscle group was most active during a walking stride as measured by the EMG recordings and as predicted by the musculoskeletal models (Figure 4; blue, EMG measurements; red, model predictions).
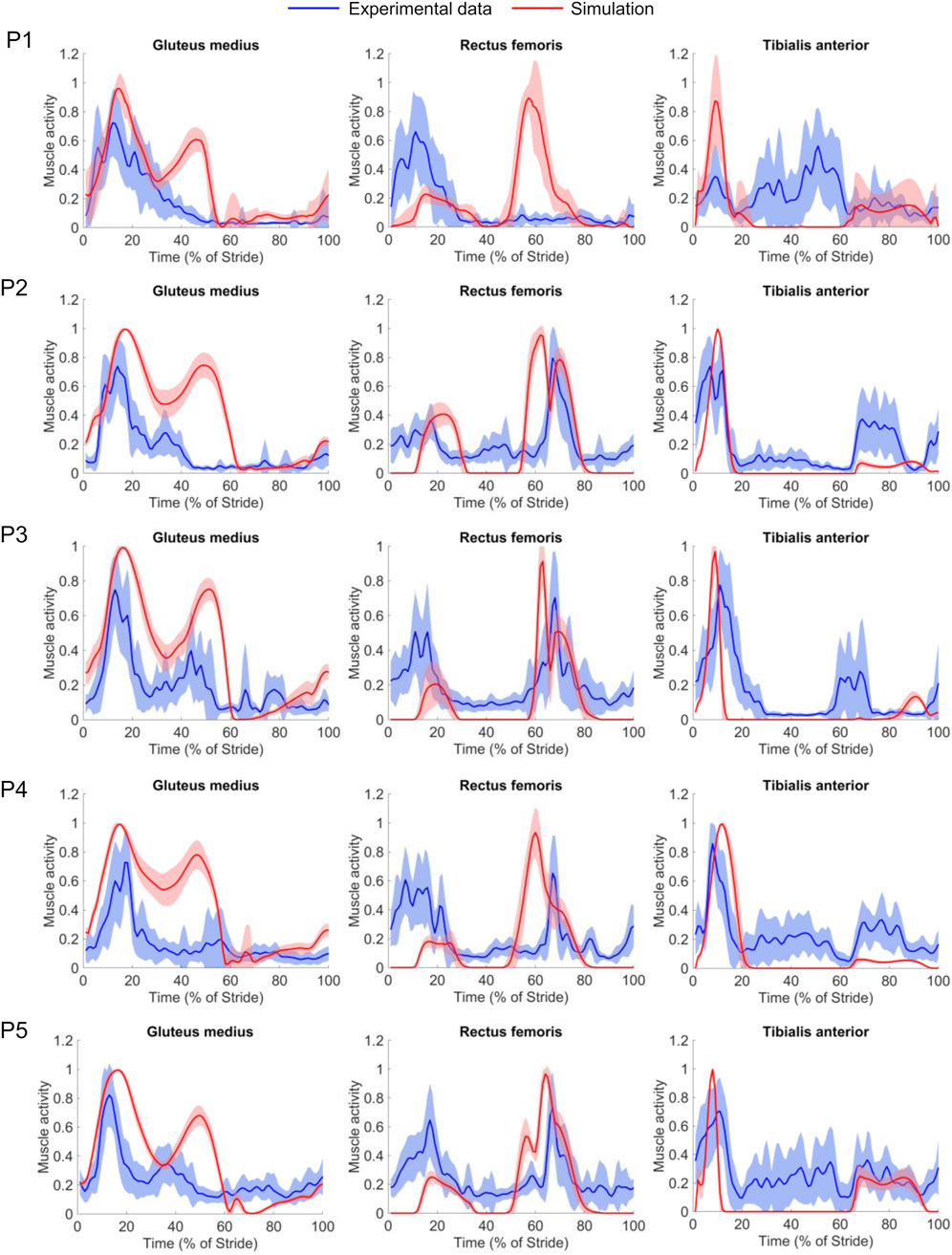
Figure 4. Comparison of muscle activities predicted by the musculoskeletal model (red solid lines) and the electromyography (EMG) data measured in the experiment (blue solid lines) for the gluteus medius, rectus femoris, and tibialis anterior muscles as a function of the percent of the stride for each of the five participants. The shaded areas represent the stride-averaged EMG envelopes (mean ± 1 standard deviation) for each participant (P#). We separately normalized the magnitudes of the muscle activity and the EMG recordings to the maximum of each stride, for each participant.
For certain phases of the stride for participants P2−P5, we observed a reasonable qualitative agreement between the predicted and measured muscle activity profiles after considering the electromechanical delay, which represents the time lag between the onset of muscle activation (measured by EMG) and muscle force generation (predicted by the models) (Cavanagh and Komi, 1979). Specifically, the models correctly predicted activation of the ankle dorsiflexor muscles (tibialis anterior) during the late-swing and early-stance phases. Consistent with the EMG recordings, the models predicted the onset of knee extensor (rectus femoris) activity at mid-stance to absorb shock and the onset of hip abductor (gluteus medius) activity in the early- and mid-stance phases. We did observe some inter-subject variability in the EMG recordings (Figure 4, blue lines). For example, for participant P1, at mid-stance we did not observe activation of the rectus femoris or gluteus medius, both of which were activated in the mid-stance phase for the remaining four participants (P2−P5). In addition, we also observed irregular tibialis anterior activity for this participant during mid-stance, a pattern we did not notice in the EMG recordings of the other four participants.
The average torque provided by the ExoBoot to the participants’ ankle varied between 18 and 24 N·m. For the normalized stride length, we found that the device-distance interaction effect was statistically significant (p < 0.001) (Table 2). However, the mean value of this parameter did not significantly change between the two devices (p ≥ 0.438) or between the two distances (p ≥ 0.125) (Table 3). In terms of ES, the normalized stride length increased considerably at 5 km compared to baseline when the participants walked without the ExoBoot, with an ES of 1.17 (Table 3) [5 km: 1.49 (0.05) vs. 0 km: 1.44 (0.03) (Table 2)]. In contrast, for stance duration, only the device effect was statistically significant (p < 0.001) (Table 2). In fact, compared to without the ExoBoot, walking with the ExoBoot significantly increased the stance duration (p < 0.001), with an ES of 1.12 (Table 4). The stance durations at 5 km and 0 km were the same within a device condition (Table 2).
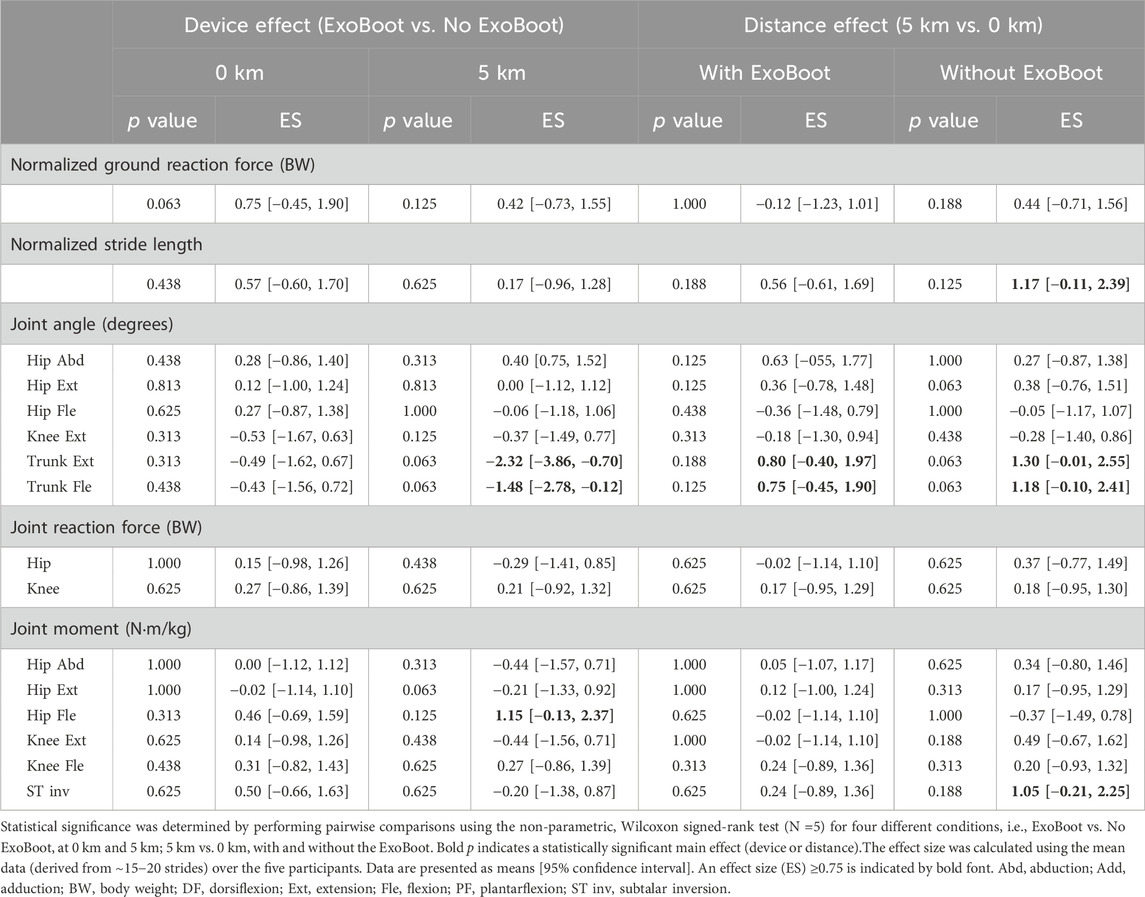
Table 3. Pairwise comparisons of spatiotemporal, joint kinematic, and joint kinetic parameters with significant interaction between device and walking distance.
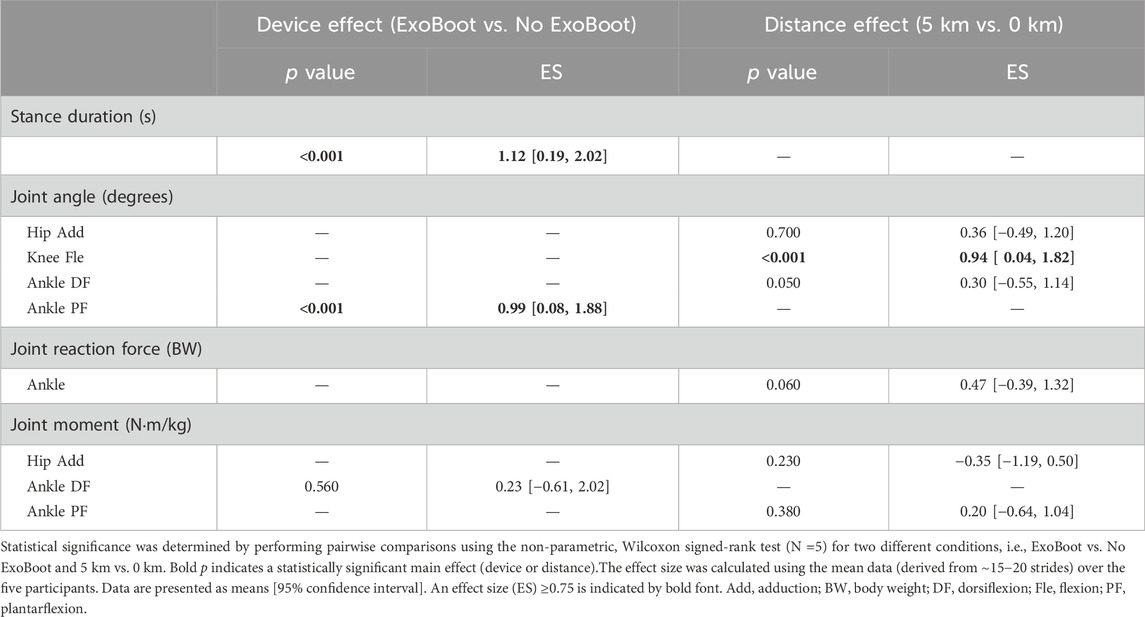
Table 4. Pairwise comparisons of spatiotemporal, joint kinematic, and joint kinetic parameters without significant interaction between device and walking distance.
Among the joint angles, we found that the device-distance interaction effect was statistically significant (p < 0.001) for the peak hip abduction, hip flexion, trunk extension, and trunk flexion angles (Table 2). However, the mean value of each of these four parameters did not significantly change between the two devices or the two distances (Table 3). In terms of ES, compared to baseline, both the peak trunk extension and flexion angles increased at 5 km, with ES values ≥ 0.75, regardless of the ExoBoot condition (Table 3), where the magnitude of the increase in each of these two parameters was smaller when participants walked with the ExoBoot (∼20%) compared to without it (∼42%) (Table 2). In fact, compared to walking without the ExoBoot, walking with it for 5 km considerably reduced the peak trunk extension angle, with an ES of −2.32 (confidence interval = [−3.86, −0.70]), and the peak trunk flexion angle, with an ES of −1.48 (confidence interval = [−2.78, −0.12]), which did not occur at baseline (Table 3).
For the peak ankle plantarflexion angle, we found that only the device effect was statistically significant (p < 0.001) (Table 2). Compared to without the ExoBoot, walking with it significantly increased the ankle plantarflexion angle (p < 0.001) with an ES of 0.99 (Table 4). For the peak knee flexion angle, only the distance effect was statistically significant (Table 2). Indeed, compared to baseline, walking 5 km significantly increased (p < 0.001) this angle with an ES of 0.94 (Table 4). For one of the 26 parameters, the subtalar eversion moment, neither of the two main effects was significant, therefore, we did not perform any pairwise comparisons for this parameter. In summary, while use of the ExoBoot device significantly impacted stance duration and ankle plantarflexion angle regardless of distance, its impact on the peak trunk extension and trunk flexion angles was dependent on the walking distance.
For the GRF and hip JRF, we found that the device-distance interaction effect was statistically significant (p < 0.001) (Table 2). With ExoBoot use, the GRF slightly decreased at 5 km compared to baseline, however, this decrease was not significant (p = 1.000) (Table 3). For the knee JRF, both the device and distance effects were significant, while the interaction effect was not (Table 2). The JRFs at the hip and knee did not change significantly with ExoBoot use or walking distance (Table 3). For the ankle JRF, only the distance effect was significant. While its mean value increased at 5 km compared to baseline with a moderate ES of 0.47, this change was not significant (Table 4).
For five of the 10 joint moments, i.e., the hip abduction, hip extension, hip flexion, knee extension, and subtalar inversion moments, we found that the device-distance interaction effect was significant (p ≤ 0.040) (Table 2). However, none of the mean values of these five parameters changed significantly between the two devices or the two distances (Table 3). In terms of ES, compared to without the ExoBoot, its use increased the mean hip flexion moment by 27% at 5 km with a large ES of 1.15 (Table 3), which was not observed at 0 km. Furthermore, while the hip abduction and hip extension moments consistently increased at 5 km compared to baseline for both device conditions, the magnitude of the increase was considerably smaller when participants wore the ExoBoot (∼2.5% for hip abduction and <1% for hip extension) compared to without it (∼12% for hip abduction and ∼4% for hip extension) (Table 2). When participants walked without the ExoBoot, the subtalar inversion moment increased by 44% at 5 km (Table 2) with an ES of 1.05 (Table 3).
For the peak knee flexion moment, both the device and distance effects were significant (Table 2). However, the pairwise comparison did not show a significant change in the mean values of this parameter between the two devices or the two distances (Table 3). For the ankle dorsiflexion moment, only the device effect was significant (Table 2). Compared to without the ExoBoot, its use increased the mean ankle dorsiflexion moment with a small ES of 0.23, and this increase was not significant (p = 0.560, Table 4). For the hip adduction and ankle plantarflexion moments, only the distance effect was statistically significant (Table 2). We found that the mean values of the hip adduction moment decreased (ES: −0.35) and the ankle plantarflexion moment increased (ES: 0.20) at 5 km compared to 0 km, however, neither of these changes was significant (Table 4). In summary, exoskeleton device use considerably increased the hip flexion moment, moderately increased the ankle dorsiflexion moment, and reduced the magnitude of the increase in hip abduction and hip extension moments after a 5-km walk.
The objective of this pilot study was to characterize the biomechanical responses of the lower extremities of young, healthy men after walking with an active ankle exoskeleton for 5 km. Towards this goal, we collected experimental data for five adult men, developed individualized musculoskeletal models, and computed 26 distinct biomechanical responses, including spatiotemporal, joint kinematic, and joint kinetic parameters, for each participant at two distances (0 km and 5 km) as they walked while carrying a 22.7-kg load with and without wearing an active ankle exoskeleton (the Dephy ExoBoot EB60). We found that, irrespective of the distance walked, ExoBoot use significantly increased the stance duration and peak ankle plantarflexion angle (p < 0.001; Table 4). In addition, at the 5-km distance, we observed considerable decreases in the peak trunk extension (ES: −2.32) and trunk flexion angles (ES:−1.48) with ExoBoot use compared to without it (Table 3). In general, compared to walking without the ExoBoot, its use reduced the magnitude of the increases in peak trunk extension and trunk flexion angles after walking for 5 km compared to baseline. Finally, irrespective of ExoBoot use, we found that the knee flexion angle significantly increased at 5 km compared to baseline (p < 0.001; Table 4).
As expected, we observed large inter-subject variability in certain biomechanical responses of the five participants. For example, at the 5-km distance, compared to without the ExoBoot, its use increased the ankle JRF in two of the participants and decreased it in the other three. Except for a few joint angles, e.g., the peak ankle plantarflexion, trunk extension, and trunk flexion angles, we did not find many parameters that demonstrated the same trend in all five participants when they walked with the ExoBoot. This is consistent with previous studies that have shown an increase in inter-subject variability in gait parameters as individuals become fatigued (Winter et al., 2017; Zandbergen et al., 2023) or when individuals walk with exoskeleton devices compared to unassisted walking (Hybart and Ferris, 2023). Despite the inter-subject variability, we found two parameters that, on average, significantly increased (p < 0.001) with ExoBoot use compared to without it. Consistent with previous studies involving both men and women (Sawicki and Ferris, 2009b; Koller et al., 2015), we observed that in comparison with walking unassisted, walking with the ExoBoot significantly increased the peak ankle plantarflexion angle (p < 0.001; Table 4). In addition, ExoBoot use significantly increased the average stance duration (p < 0.001; Table 4). However, despite being statistically significant, the magnitude of the increase in stance duration was small [with ExoBoot: 0.68 (0.01) s vs. without ExoBoot: 0.67 (0.01) s (Table 2)]. We did not find any previous reports of changes in stance duration due to the use of an exoskeleton device. However, stance duration has been previously shown to decrease in both young and old adults when they walked after becoming fatigued (Zhang et al., 2014; Santos et al., 2019; Halder et al., 2021). Therefore, by increasing the stance duration, exoskeleton use might help mitigate the effect of fatigue.
While previous studies that investigated the impact of active ankle exoskeletons have demonstrated their ability to reduce the energy requirement of walking by ∼8–15%, none of these studies reported any significant changes in the knee or hip joint angles (Sawicki and Ferris, 2008; Malcolm et al., 2013; Mooney et al., 2014b; Koller et al., 2015; Mooney and Herr, 2016; Acosta-Sojo and Stirling, 2022; Gonzalez et al., 2022; Ingraham et al., 2022; Medrano et al., 2022; Wu et al., 2024). In contrast, our results showed that compared to baseline, walking 5 km significantly increased the knee flexion angle regardless of ExoBoot use (p < 0.001; Table 4). In addition, while not statistically significant, our results showed that ExoBoot use considerably altered certain hip and knee joint angles at 5 km, which did not occur when participants walked unassisted. In particular, compared to baseline, the hip flexion angle decreased (ES: −0.36) and the hip abduction angle increased (ES: 0.63) after participants walked 5 km with the ExoBoot (Table 3). It is possible that because of the longer walking time and distance that the participants walked with an active exoskeleton in our study [∼60 min (i.e., 5 km)] compared to previous studies [up to ∼30 min or ∼2 km], we were able to capture changes in hip joint angles that were not previously reported.
On the other hand, some of our findings regarding the effect of the exoskeleton device on joint kinetics are corroborated by previous studies. For example, Mooney and Herr (2016) reported that, compared to unassisted walking, walking with an active ankle exoskeleton for ∼2 km in ∼20 min increased the peak knee flexion and the peak hip flexion moments during late stance and decreased the peak hip extension moment in healthy men, which is consistent with our results (Table 3). In another study, compared to unassisted walking for ∼2 km in ∼30 min, walking with an active ankle exoskeleton increased the average positive hip power (obtained by multiplying the hip angular velocity by the hip torque) in healthy men, implying that an exoskeleton could potentially reduce the effort in the hip muscles during walking (Koller et al., 2015). However, in these studies, participants did not carry a load while walking. Consistent with these two studies, we found that, compared to unassisted walking, on average, wearing the ExoBoot for 5 km also increased the peak hip flexion moment (ES: 1.15) and lowered other moments around the hip joint [i.e., the hip abduction (ES: −0.44) and the hip extension (ES:−0.21) (Table 3)].
In our analysis, we also found eight parameters that, on average, demonstrated the same trend (i.e., an increase or a decrease) at 5 km compared to 0 km both with and without the ExoBoot. We speculate that these increases could be due to fatigue in some, if not all, of the participants because they occurred irrespective of ExoBoot use and because the distance walked in our experiments (i.e., 5 km) was longer than that considered as a mark for fatigue onset (i.e., 3 km) in previous fatigue-inducing running protocols that did not involve load carriage (Winter et al., 2017). Among the spatiotemporal and joint angle parameters, we found that the peak knee flexion angle increased significantly at 5 km compared to 0 km irrespective of ExoBoot use. Indeed, this angle has been previously shown to increase in young, healthy adults during running following fatigue-inducing protocols (Kellis et al., 2011; Bazuelo-Ruiz et al., 2018). Another such parameter, the peak trunk flexion angle, has been previously shown to increase after fatigue onset in running and isokinetic muscle contraction protocols (Granacher et al., 2010; Heiderscheit et al., 2011; Warrener et al., 2021). Interestingly, in our study, although the trunk flexion angle increased both with and without the ExoBoot after 5 km of walking (likely due to fatigue), the magnitude of the increase was smaller when the participants walked with the ExoBoot (16% with ExoBoot vs. 35% without ExoBoot, Table 2). Similarly, the stride length also increased by a smaller magnitude when participants walked for 5 km with the ExoBoot compared to without it (2% with ExoBoot vs. 3.5% without ExoBoot, Table 2). We do know from previous studies that a reduction in stride length when running without load carriage, even for short intervals, is likely to reduce the risk of a stress-fracture injury in healthy, young men and women (Edwards et al., 2009; Sundaramurthy et al., 2023). Therefore, in accordance with our hypothesis, ExoBoot use could be potentially beneficial because a shorter stride length results in a smaller loading to the muscles and bones.
We observed the same trend, i.e., a reduction in the magnitude of the increase with ExoBoot use, in certain hip, knee, and ankle moments: hip abduction (12% without ExoBoot vs. 2% with ExoBoot), hip extension (4% without ExoBoot vs. <1% with ExoBoot), knee extension (12% without ExoBoot vs. <1% with ExoBoot), and subtalar inversion (13% without ExoBoot vs. 9% with ExoBoot). Changes in hip kinetics and kinematics due to fatigue could increase the risk of injury to the lower-leg muscles and joints, especially the knee (Krebs et al., 1998; Williams et al., 2001; Baldon et al., 2009; Ferber et al., 2009; Sangeux, 2019). For example, previous studies have shown that walking after fatiguing the hip abductor muscles increases the knee extension angles and the knee adduction moments in both men and women (Patrek et al., 2011; Tang et al., 2022), and a higher external knee adduction moment has often been observed in patients with pathological knee conditions, such as patellofemoral pain syndrome and knee osteoarthritis (Bolgla et al., 2008; O'Connell et al., 2016). In addition to pathological knee conditions, changes in hip-joint kinematics also contribute to hip muscle strength and the risk of hip-joint injury. For example, an increase in peak hip flexion angle has been associated with a decrease in hip flexor muscle strength (i.e., fatigue) during high-intensity running (Riazati et al., 2020). Thus, with results showing that ExoBoot use, on average, altered the hip joint kinematics and kinetics in a manner potentially associated with lowering injury risk (i.e., decreasing the peak hip flexion angle and increasing the hip abduction angle, as well as lowering the hip abduction and hip extension moments), our study suggests that wearing the ExoBoot could attenuate the negative effects of walking long distances with load carriage, which supports our hypothesis.
Our study has several limitations. First, due to inter-subject variability in the biomechanical responses and the small sample size of this pilot study (N = 5 men), the generalizability of the observed group-level effects is limited. We constrained the study to men because they represent 82% of U.S. Service members (Department of Defense, 2023) and, more importantly, to eliminate sex differences as another source of variability. It is well established that gait biomechanics differ between men and women when walking or running unassisted with load carriage (Bode et al., 2021; Rubio et al., 2023), and we expect such variability to persist with the use of the ExoBoot. Second, we assumed that walking 5 km at 1.34 m/s (i.e., for ∼60 min) is sufficient to induce fatigue, which may not be true for all participants. However, we based our study design on a meta-analysis that included 25 different studies involving both male and female participants where fatigue was assumed to be induced by running without load carriage for at least 3 km or for 30 min (Winter et al., 2017). Third, we conducted the experiments in a controlled laboratory environment using a level treadmill. While this laboratory setup is not fully representative of U.S. Army marching (Department of the Army, 2022), we implemented it to minimize confounding factors and systematically delineate the impact of the ExoBoot on the biomechanical parameters in a controlled environment. Hence, the reported results may differ from those obtained on an uneven terrain, as various studies have reported differences in lower-extremity joint mechanics between unassisted walking on a flat terrain versus an uneven terrain, such as larger flex joint angles and smaller joint extension moments (Lange et al., 1996; Leroux et al., 2002; Lay et al., 2006; McIntosh et al., 2006; Silder et al., 2012; Haggerty et al., 2014). Use of the ExoBoot on an uneven terrain should result in similar differences in hip, knee, and ankle joint angles and moments, which need to be further investigated in a new study.
Fourth, the study participants did not have a history of exoskeleton use, which could have influenced their biomechanics when walking with it for the first time. However, we still consider the participants to be a representative sample of military recruits based on the possibility that new recruits may not have prior experience using active exoskeleton devices that enhance mobility. Furthermore, to minimize the effect of no previous exoskeleton use, participants completed a separate training visit to become acclimated to walking with the ExoBoot. Fifth, we modeled the knee and ankle joints as revolute joints, which only captures their movement in the sagittal plane, because the primary movement of knee and ankle joints occurs in this plane. A study by Marra et al. (2015), which evaluated the performance of revolute and higher-fidelity joints for their ability to represent knee joint biomechanics using musculoskeletal models, found their performance to be comparable. Therefore, we believe that modeling the three-dimensional motion of the knee and ankle joints would not have changed our conclusions. Finally, even though we did not customize muscle strength or explicitly account for muscular fatigue, we individualized the tibial and lumbar (L4-L5) geometry and used each participant’s material properties to individualize the musculoskeletal model. We adjusted the muscle strength based on the height, weight, and fat percentage of each participant. We acknowledge that incorporating participant- and task-specific muscle strengths into musculoskeletal models adds an important dimension of personalization, especially when considering such cases as strenuous military training.
We quantitatively assessed the potential effects of an active ankle exoskeleton device on the lower-limb biomechanics of young, healthy men due to walking with load carriage for 5 km (∼60 min). We found that, compared to without an active exoskeleton device, walking with the ExoBoot while carrying a 22.7-kg load significantly increased the stance duration and peak ankle plantarflexion angle. In addition, walking with the ExoBoot lowered the magnitude of the increases in the trunk flexion angle and stride length compared to unassisted walking. Despite the small sample size of this pilot study, our results suggest that walking with the ExoBoot may mitigate the effects of fatigue-induced changes in certain biomechanical parameters and alter the hip joint angles and moments in a potentially beneficial manner during extended use. By identifying specific gait-related parameters (i.e., stance duration, trunk and knee angles, and hip moments) that are susceptible to change with exoskeleton use, our study offers potential insights into the biomechanical parameters that should be further evaluated for association with lower-leg musculoskeletal injuries due to use of such augmentation devices. In addition, the knowledge gained in this pilot study could provide a benchmark for future studies and inform the development of standards for safe and effective use of emerging exoskeleton technologies.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by the University of Kentucky Institutional Review Board and the Office of Human Research Oversight at the U.S. Army Medical Research and Development Command. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
SN: Formal Analysis, Writing–original draft, Writing–review and editing. JR: Formal Analysis, Writing–original draft, Writing–review and editing. JT: Writing–review and editing, Conceptualization, Data curation, Methodology, Validation. AS: Conceptualization, Data curation, Methodology, Validation, Writing–review and editing. AP: Conceptualization, Data curation, Methodology, Validation, Writing–review and editing. MO: Data curation, Methodology, Writing–review and editing, Investigation. MS: Data curation, Investigation, Writing–review and editing, Methodology. BN: Data curation, Investigation, Writing–review and editing, Methodology, Conceptualization. JR: Conceptualization, Formal Analysis, Funding acquisition, Project administration, Supervision, Writing–original draft, Writing–review and editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was sponsored by the Military Operational Medicine Program Area Directorate of the U.S. Army Medical Research and Development Command (USAMRDC), Fort Detrick, MD. The Henry M. Jackson Foundation was supported by the USAMRDC under Contract No. W81XWH20C0031. In addition, Michael A. Samaan was partly supported by the National Institutes of Health (K01-AG073698).
We acknowledge support from the Department of Defense High Performance Computing Modernization Program. We thank Karen N. Gregorczyk, Chad W. Hearing, Joseph F. Seay, and Andrea J. Taylor from the U.S. Army Combat Capabilities Development Command Soldier Center, Natick, MA, for valuable discussions and providing guidance regarding active exoskeleton devices currently being evaluated by the U.S. Army. We thank Maria Kuhrmann for editorial assistance.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The opinions and assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting the views of the U.S. Army, the U.S. DoD, or The Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc. This paper has been approved for public release with unlimited distribution.
Acosta-Sojo, Y., and Stirling, L. (2022). Individuals differ in muscle activation patterns during early adaptation to a powered ankle exoskeleton. Appl. Ergon. 98, 103593. doi:10.1016/j.apergo.2021.103593
Baldon, R. D. M., Nakagawa, T. H., Muniz, T. B., Amorim, C. F., Maciel, C. D., and Serrao, F. V. (2009). Eccentric hip muscle function in females with and without patellofemoral pain syndrome. J. Athl. Train. 44, 490–496. doi:10.4085/1062-6050-44.5.490
Bazuelo-Ruiz, B., Dura-Gil, J. V., Palomares, N., Medina, E., and Llana-Belloch, S. (2018). Effect of fatigue and gender on kinematics and ground reaction forces variables in recreational runners. PeerJ 6, e4489. doi:10.7717/peerj.4489
Benjamini, Y., and Hochberg, Y. (1995). Controlling the false discovery rate: a practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B Stat. Methodol. 57 (1), 289–300. doi:10.1111/j.2517-6161.1995.tb02031.x
Bode, V. G., Frykman, P. N., Smith, N. I., Fellin, R. E., and Seay, J. F. (2021). Spatiotemporal and kinematic comparisons between anthropometrically paired male and female soldiers while walking with heavy loads. Mil. Med. 186, 387–392. doi:10.1093/milmed/usaa435
Bogue, R. (2015). Robotic exoskeletons: a review of recent progress. Ind. Robot. 42, 5–10. doi:10.1108/IR-08-2014-0379
Bolgla, L. A., Malone, T. R., Umberger, B. R., and Uhl, T. L. (2008). Hip strength and hip and knee kinematics during stair descent in females with and without patellofemoral pain syndrome. J. Orthop. Sports Phys. Ther. 38, 12–18. doi:10.2519/jospt.2008.2462
Cavanagh, P. R., and Komi, P. V. (1979). Electromechanical delay in human skeletal muscle under concentric and eccentric contractions. Eur. J. Appl. Physiol. Occup. Physiol. 42, 159–163. doi:10.1007/BF00431022
Clansey, A. C., Hanlon, M., Wallace, E. S., and Lake, M. J. (2012). Effects of fatigue on running mechanics associated with tibial stress fracture risk. Med. Sci. Sports Exerc 44, 1917–1923. doi:10.1249/MSS.0b013e318259480d
Department of Defense (2023). Demographics: profile of the military community. Available at: https://download.militaryonesource.mil/12038/MOS/Reports/2023-demographics-report.pdf (accessed on January 18, 2025).
Department of the Army (2011). Technical bulletin TB MED 592 prevention and control of musculoskeletal injuries associated with physical training. Washington, DC: Headquarters, Department of the Army.
Department of the Army (2022). Army techniques publication 3-21.18. Foot marches (Washington, DC: Headquarters, Department of the Army).
Ding, Y., Galiana, I., Asbeck, A. T., De Rossi, S. M., Bae, J., Santos, T. R., et al. (2017). Biomechanical and physiological evaluation of multi-joint assistance with soft exosuits. IEEE Trans. Neural Syst. Rehabil. Eng. 25, 119–130. doi:10.1109/TNSRE.2016.2523250
Edwards, W. B., Taylor, D., Rudolphi, T. J., Gillette, J. C., and Derrick, T. R. (2009). Effects of stride length and running mileage on a probabilistic stress fracture model. Med. Sci. Sports Exerc 41, 2177–2184. doi:10.1249/MSS.0b013e3181a984c4
Fagerland, M. W. (2012). T-tests, non-parametric tests, and large studies-a paradox of statistical practice? BMC Med. Res. Methodol. 12, 78. doi:10.1186/1471-2288-12-78
Ferber, R., Hreljac, A., and Kendall, K. D. (2009). Suspected mechanisms in the cause of overuse running injuries: a clinical review. Sports Health 1, 242–246. doi:10.1177/1941738109334272
Gonzalez, S., Stegall, P., Cain, S. M., Siu, H. C., and Stirling, L. (2022). Assessment of a powered ankle exoskeleton on human stability and balance. Appl. Ergon. 103, 103768. doi:10.1016/j.apergo.2022.103768
Gordon, K. E., and Ferris, D. P. (2007). Learning to walk with a robotic ankle exoskeleton. J. Biomech. 40, 2636–2644. doi:10.1016/j.jbiomech.2006.12.006
Granacher, U., Wolf, I., Wehrle, A., Bridenbaugh, S., and Kressig, R. W. (2010). Effects of muscle fatigue on gait characteristics under single and dual-task conditions in young and older adults. J. Neuroeng Rehabil. 7, 56. doi:10.1186/1743-0003-7-56
Gregorczyk, K. N., Hasselquist, L., Schiffman, J. M., Bensel, C. K., Obusek, J. P., and Gutekunst, D. J. (2010). Effects of a lower-body exoskeleton device on metabolic cost and gait biomechanics during load carriage. Ergonomics 53, 1263–1275. doi:10.1080/00140139.2010.512982
Haggerty, M., Dickin, D. C., Popp, J., and Wang, H. (2014). The influence of incline walking on joint mechanics. Gait Posture 39, 1017–1021. doi:10.1016/j.gaitpost.2013.12.027
Halder, A., Nordin, A., Miller, M., Kuklane, K., Nirme, J., and Gao, C. (2021). Effects of leg fatigue due to exhaustive stair climbing on gait biomechanics while walking up a 10° incline – implications for evacuation and work safety. Fire Saf. J. 123, 103342. doi:10.1016/j.firesaf.2021.103342
Heiderscheit, B. C., Chumanov, E. S., Michalski, M. P., Wille, C. M., and Ryan, M. B. (2011). Effects of step rate manipulation on joint mechanics during running. Med. Sci. Sports Exerc 43, 296–302. doi:10.1249/MSS.0b013e3181ebedf4
Hybart, R., and Ferris, D. (2023). Gait variability of outdoor vs treadmill walking with bilateral robotic ankle exoskeletons under proportional myoelectric control. PLoS One 18, e0294241. doi:10.1371/journal.pone.0294241
Ingraham, K. A., Remy, C. D., and Rouse, E. J. (2022). The role of user preference in the customized control of robotic exoskeletons. Sci. Robot. 7, eabj3487. doi:10.1126/scirobotics.abj3487
Jackson, R. W., and Collins, S. H. (2015). An experimental comparison of the relative benefits of work and torque assistance in ankle exoskeletons. J. Appl. Physiol. (1985) 119, 541–557. doi:10.1152/japplphysiol.01133.2014
Johnson, W. B., Young, A., Goldman, S., Wilson, J., Alderete, J. F., and Childers, W. L. (2023). Exoskeletal solutions to enable mobility with a lower leg fracture in austere environments. Wearable Technol. 4, e5. doi:10.1017/wtc.2022.26
Kellis, E., Zafeiridis, A., and Amiridis, I. G. (2011). Muscle coactivation before and after the impact phase of running following isokinetic fatigue. J. Athl. Train. 46, 11–19. doi:10.4085/1062-6050-46.1.11
Knapik, J., Reynolds, K., Santee, W., and Friedl, K. (2012). “Load carriage in military operations: a review of historical, physiological, biomechanical and medical aspects,” in Military quantitative physiology: problems and concepts in military operational medicine (Houston, TX: Office of The Surgeon General Department of the Army, USA and U.S. Army Medical Department Center and School), 303–337.
Koller, J. R., Jacobs, D. A., Ferris, D. P., and Remy, C. D. (2015). Learning to walk with an adaptive gain proportional myoelectric controller for a robotic ankle exoskeleton. J. Neuroeng Rehabil. 12, 97. doi:10.1186/s12984-015-0086-5
Krebs, D. E., Robbins, C. E., Lavine, L., and Mann, R. W. (1998). Hip biomechanics during gait. J. Orthop. Sports Phys. Ther. 28, 51–59. doi:10.2519/jospt.1998.28.1.51
Lakens, D. (2013). Calculating and reporting effect sizes to facilitate cumulative science: a practical primer for t-tests and ANOVAs. Front. Psychol. 4, 863. doi:10.3389/fpsyg.2013.00863
Lange, G. W., Hintermeister, R. A., Schlegel, T., Dillman, C. J., and Steadman, J. R. (1996). Electromyographic and kinematic analysis of graded treadmill walking and the implications for knee rehabilitation. J. Orthop. Sports Phys. Ther. 23, 294–301. doi:10.2519/jospt.1996.23.5.294
Lay, A. N., Hass, C. J., and Gregor, R. J. (2006). The effects of sloped surfaces on locomotion: a kinematic and kinetic analysis. J. Biomech. 39, 1621–1628. doi:10.1016/j.jbiomech.2005.05.005
Lee, H., Ferguson, P. W., and Rosen, J. (2020). “Chapter 11 - lower limb exoskeleton systems—overview,” in Wearable robotics. Editors J. Rosen,, and P. W. Ferguson (Cambridge, MA: Academic Press), 207–229.
Leroux, A., Fung, J., and Barbeau, H. (2002). Postural adaptation to walking on inclined surfaces: I. Normal strategies. Gait Posture 15, 64–74. doi:10.1016/s0966-6362(01)00181-3
Malcolm, P., Derave, W., Galle, S., and De Clercq, D. (2013). A simple exoskeleton that assists plantarflexion can reduce the metabolic cost of human walking. PLoS One 8, e56137. doi:10.1371/journal.pone.0056137
Marra, M. A., Vanheule, V., Fluit, R., Koopman, B. H., Rasmussen, J., Verdonschot, N., et al. (2015). A subject-specific musculoskeletal modeling framework to predict in vivo mechanics of total knee arthroplasty. J. Biomech. Eng. 137, 020904. doi:10.1115/1.4029258
McIntosh, A. S., Beatty, K. T., Dwan, L. N., and Vickers, D. R. (2006). Gait dynamics on an inclined walkway. J. Biomech. 39, 2491–2502. doi:10.1016/j.jbiomech.2005.07.025
Medrano, R. L., Thomas, G. C., and Rouse, E. J. (2022). Can humans perceive the metabolic benefit provided by augmentative exoskeletons? J. Neuroeng Rehabil. 19, 26. doi:10.1186/s12984-022-01002-w
Mooney, L. M., and Herr, H. M. (2016). Biomechanical walking mechanisms underlying the metabolic reduction caused by an autonomous exoskeleton. J. Neuroeng Rehabil. 13, 4. doi:10.1186/s12984-016-0111-3
Mooney, L. M., Rouse, E. J., and Herr, H. M. (2014a). Autonomous exoskeleton reduces metabolic cost of human walking during load carriage. J. Neuroeng Rehabil. 11, 80. doi:10.1186/1743-0003-11-80
Mooney, L. M., Rouse, E. J., and Herr, H. M. (2014b). Autonomous exoskeleton reduces metabolic cost of walking. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2014, 3065–3068. doi:10.1109/EMBC.2014.6944270
O'Connell, M., Farrokhi, S., and Fitzgerald, G. K. (2016). The role of knee joint moments and knee impairments on self-reported knee pain during gait in patients with knee osteoarthritis. Clin. Biomech. 31, 40–46. doi:10.1016/j.clinbiomech.2015.10.003
Orr, R. M., Coyle, J., Johnston, V., and Pope, R. (2017). Self-reported load carriage injuries of military soldiers. Int. J. Inj. Contr Saf. Promot 24, 189–197. doi:10.1080/17457300.2015.1132731
Orr, R. M., Johnston, V., Coyle, J., and Pope, R. (2015). Reported load carriage injuries of the Australian Army soldier. J. Occup. Rehabil. 25, 316–322. doi:10.1007/s10926-014-9540-7
Panizzolo, F. A., Freisinger, G. M., Karavas, N., Eckert-Erdheim, A. M., Siviy, C., Long, A., et al. (2019). Metabolic cost adaptations during training with a soft exosuit assisting the hip joint. Sci. Rep. 9, 9779. doi:10.1038/s41598-019-45914-5
Patrek, M. F., Kernozek, T. W., Willson, J. D., Wright, G. A., and Doberstein, S. T. (2011). Hip-abductor fatigue and single-leg landing mechanics in women athletes. J. Athl. Train. 46, 31–42. doi:10.4085/1062-6050-46.1.31
Riazati, S., Caplan, N., Matabuena, M., and Hayes, P. R. (2020). Fatigue induced changes in muscle strength and gait following two different intensity, energy expenditure matched runs. Front. Bioeng. Biotechnol. 8, 360. doi:10.3389/fbioe.2020.00360
Rubio, J. E., Tong, J., Sundaramurthy, A., Subramani, A. V., Kote, V. B., Baggaley, M., et al. (2023). Differences in running biomechanics between young, healthy men and women carrying external loads. Front. Bioeng. Biotechnol. 11, 1250937. doi:10.3389/fbioe.2023.1250937
Sangeux, M. (2019). “Biomechanics of the hip during gait,” in The pediatric and adolescent hip: essentials and evidence. Editors S. Alshryda, J. J. Howard, J. S. Huntley, and J. G. Schoenecker (Cham, Switzerland: Springer International Publishing), 53–71.
Santos, P., Barbieri, F. A., Zijdewind, I., Gobbi, L. T. B., Lamoth, C., and Hortobagyi, T. (2019). Effects of experimentally induced fatigue on healthy older adults' gait: a systematic review. PLoS One 14, e0226939. doi:10.1371/journal.pone.0226939
Sawicki, G. S., Beck, O. N., Kang, I., and Young, A. J. (2020). The exoskeleton expansion: improving walking and running economy. J. Neuroeng Rehabil. 17, 25. doi:10.1186/s12984-020-00663-9
Sawicki, G. S., and Ferris, D. P. (2008). Mechanics and energetics of level walking with powered ankle exoskeletons. J. Exp. Biol. 211, 1402–1413. doi:10.1242/jeb.009241
Sawicki, G. S., and Ferris, D. P. (2009a). A pneumatically powered knee-ankle-foot orthosis (KAFO) with myoelectric activation and inhibition. J. Neuroeng Rehabil. 6, 23. doi:10.1186/1743-0003-6-23
Sawicki, G. S., and Ferris, D. P. (2009b). Powered ankle exoskeletons reveal the metabolic cost of plantar flexor mechanical work during walking with longer steps at constant step frequency. J. Exp. Biol. 212, 21–31. doi:10.1242/jeb.017269
Silder, A., Besier, T., and Delp, S. L. (2012). Predicting the metabolic cost of incline walking from muscle activity and walking mechanics. J. Biomech. 45, 1842–1849. doi:10.1016/j.jbiomech.2012.03.032
Sundaramurthy, A., Tong, J., Subramani, A. V., Kote, V., Baggaley, M., Edwards, W. B., et al. (2023). Effect of stride length on the running biomechanics of healthy women of different statures. BMC Musculoskelet. Disord. 24, 604. doi:10.1186/s12891-023-06733-y
Tang, Y., Li, Y., Yang, M., Zheng, X., An, B., and Zheng, J. (2022). The effect of hip abductor fatigue on knee kinematics and kinetics during normal gait. Front. Neurosci. 16, 1003023. doi:10.3389/fnins.2022.1003023
Taylor, J. B., Wright, E. S., Waxman, J. P., Schmitz, R. J., Groves, J. D., and Shultz, S. J. (2021). Ankle dorsiflexion affects hip and knee biomechanics during landing. Sports Health 14, 328–335. doi:10.1177/19417381211019683
Tong, J., Subramani, A. V., Kote, V., Baggaley, M., Edwards, W. B., and Reifman, J. (2023). Effects of stature and load carriage on the running biomechanics of healthy men. IEEE Trans. Biomed. Eng. 70, 2445–2453. doi:10.1109/TBME.2023.3248504
Unnikrishnan, G., Xu, C., Baggaley, M., Tong, J., Kulkarni, S., Edwards, W. B., et al. (2021). Effects of body size and load carriage on lower-extremity biomechanical responses in healthy women. BMC Musculoskelet. Disord. 22, 219. doi:10.1186/s12891-021-04076-0
Van Herpen, F. H. M., Van Dijsseldonk, R. B., Rijken, H., Keijsers, N. L. W., Louwerens, J. W. K., and Van Nes, I. J. W. (2019). Case report: description of two fractures during the use of a powered exoskeleton. Spinal Cord. Ser. Cases 5, 99. doi:10.1038/s41394-019-0244-2
Warrener, A., Tamai, R., and Lieberman, D. E. (2021). The effect of trunk flexion angle on lower limb mechanics during running. Hum. Mov. Sci. 78, 102817. doi:10.1016/j.humov.2021.102817
Williams, G. N., Chmielewski, T., Rudolph, K., Buchanan, T. S., and Snyder-Mackler, L. (2001). Dynamic knee stability: current theory and implications for clinicians and scientists. J. Orthop. Sports Phys. Ther. 31, 546–566. doi:10.2519/jospt.2001.31.10.546
Willy, R. W., Willson, J. D., Clowers, K., Baggaley, M., and Murray, N. (2016). The effects of body-borne loads and cadence manipulation on patellofemoral and tibiofemoral joint kinetics during running. J. Biomech. 49, 4028–4033. doi:10.1016/j.jbiomech.2016.10.043
Winter, S., Gordon, S., and Watt, K. (2017). Effects of fatigue on kinematics and kinetics during overground running: a systematic review. J. Sports Med. Phys. Fit. 57, 887–899. doi:10.23736/S0022-4707.16.06339-8
Wu, M. I., Stegall, P., Siu, H. C., and Stirling, L. (2024). Impact of haptic cues and an active ankle exoskeleton on gait characteristics. Hum. Factors 66, 904–915. doi:10.1177/00187208221113625
Xu, C., Reifman, J., Baggaley, M., Edwards, W. B., and Unnikrishnan, G. (2020). Individual differences in women during walking affect tibial response to load carriage: the importance of individualized musculoskeletal finite-element models. IEEE Trans. Biomed. Eng. 67, 545–555. doi:10.1109/tbme.2019.2917415
Xu, C., Silder, A., Zhang, J., Hughes, J., Unnikrishnan, G., Reifman, J., et al. (2016). An integrated musculoskeletal-finite-element model to evaluate effects of load carriage on the tibia during walking. J. Biomech. Eng. 138, 101001. doi:10.1115/1.4034216
Xu, C., Silder, A., Zhang, J., Reifman, J., and Unnikrishnan, G. (2017). A cross-sectional study of the effects of load carriage on running characteristics and tibial mechanical stress: implications for stress-fracture injuries in women. BMC Musculoskelet. Disord. 18, 125. doi:10.1186/s12891-017-1481-9
Zandbergen, M. A., Marotta, L., Bulthuis, R., Buurke, J. H., Veltink, P. H., and Reenalda, J. (2023). Effects of level running-induced fatigue on running kinematics: a systematic review and meta-analysis. Gait Posture 99, 60–75. doi:10.1016/j.gaitpost.2022.09.089
Zhang, J., Fiers, P., Witte, K. A., Jackson, R. W., Poggensee, K. L., Atkeson, C. G., et al. (2017). Human-in-the-loop optimization of exoskeleton assistance during walking. Science 356, 1280–1284. doi:10.1126/science.aal5054
Zhang, J., Lockhart, T. E., and Soangra, R. (2014). Classifying lower extremity muscle fatigue during walking using machine learning and inertial sensors. Ann. Biomed. Eng. 42, 600–612. doi:10.1007/s10439-013-0917-0
Keywords: exoskeleton, individualized models, walking, load carriage, musculoskeletal biomechanics
Citation: Nagaraja S, Rubio JE, Tong J, Sundaramurthy A, Pant A, Owen MK, Samaan MA, Noehren B and Reifman J (2025) Effects of an active ankle exoskeleton on the walking biomechanics of healthy men. Front. Bioeng. Biotechnol. 13:1533001. doi: 10.3389/fbioe.2025.1533001
Received: 22 November 2024; Accepted: 14 February 2025;
Published: 14 March 2025.
Edited by:
Yury Ivanenko, Santa Lucia Foundation (IRCCS), ItalyReviewed by:
Daniele Borzelli, University of Messina, ItalyCopyright © 2025 Nagaraja, Rubio, Tong, Sundaramurthy, Pant, Owen, Samaan, Noehren and Reifman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jaques Reifman, amFxdWVzLnJlaWZtYW4uY2l2QGhlYWx0aC5taWw=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.