
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Allergy , 22 July 2022
Sec. Skin Allergy
Volume 3 - 2022 | https://doi.org/10.3389/falgy.2022.952079
This article is part of the Research Topic The Complexity of Urticaria View all 10 articles
 Fiorella PetrelliDaiana GianniniSilvia BiliaIsabella Del CorsoValeria Rocchi
Fiorella PetrelliDaiana GianniniSilvia BiliaIsabella Del CorsoValeria Rocchi Paola Migliorini*
Paola Migliorini* Ilaria Puxeddu
Ilaria PuxedduUrticarial vasculitis (UV) is a small-vessel leukocytoclastic vasculitis characterized by different clinical manifestations ranging from long-lasting urticarial lesions to severe and potentially life-threatening multi-organ involvement. Omalizumab (OMA), anti-IgE recombinant humanized IgG1 monoclonal antibody, has been successfully used to treat few cases of severe and/or refractory UV. In this study we report our experience on 6 patients with refractory normocomplementemic UV successfully treated with anti-IgE therapy (OMA), suggesting that this biological therapy may be a safe and effective therapeutic option in UV.
Urticarial vasculitis (UV) is a rare immune-complex mediated small-vessel leukocytoclastic vasculitis, characterized by long-lasting urticarial lesions, persisting more than 24 h. Clinical manifestations may range from itchy and/or burning skin lesions to severe and potentially life-threatening multi-organ involvement, having a substantial impact on patients' life expectancy and quality of life. On the basis of complement levels, UV is classified into two different forms: normocomplementemic (NUV) and hypocomplementemic (HUV). Moreover, the latter form is mainly associated with multi-organ involvement and with the presence of anti-C1q antibodies in more than half of the patients (1). Although most of the forms of UV are defined as idiopathic as the cause of the disease is not identified, some of them can be also associated with autoimmune and/or infectious and/or malignant diseases and can resolve following treatment of the underlying condition. Several drugs or vaccines, including recently those for COVID-19, have been identified as potential triggers for UV (1–3). The therapeutic approach to this disease is currently challenging due to the lack of large randomized controlled trials and approved therapies. Corticosteroids are among the most effective drugs for the treatment of both skin and extracutaneous manifestations, although their long-term administration may lead to serious dose-dependent side effects. In such cases immunosuppressive or immunomodulatory therapies such as azathioprine, cyclophosphamide or cyclosporine may improve disease control and reduce the dosage of corticosteroids. However, side effects, especially in the case of prolonged administration, and/or lack of efficacy often require discontinuation of the treatment (2, 4).
Thus, due to the evident limitations of the current treatment of UV, it is important to identify novel effective and safe therapeutic approaches for patients with diagnosis of UV, able to improve their quality of life and life expectancy. Several biological agents such as etanercept, infliximab, canakinumab, anakinra, rituximab, tocilizumab have been proposed as alternative therapeutic options in severe and/or treatment-refractory UV patients, even though the evidences on their efficacy and safety in the treatment of this condition are currently limited to a few case reports (2, 4).
Omalizumab (OMA) is a recombinant humanized IgG1 monoclonal antibody directed to IgE-specific epitopes within the C3 (FcεRI binding) region of circulating IgE, that reduces IgE/FcεRI binding on mast cells and basophils with consequent down-regulation of cell activation. After being approved in the USA and Europe for the treatment of antihistamine refractory chronic spontaneous urticaria (CSU), severe allergic asthma and severe chronic rhinosinusitis with nasal polyps, its efficacy and safety has been widely demonstrated in real-life experience. Based on the markedly positive impact of OMA in CSU, the use of this drug has been reported in some cases of severe and/or refractory UV either idiopathic or associated with autoimmune diseases (2, 4, 5).
In the Immuno-allergology Unit of Azienda Ospedaliero-Universitaria Pisana (AOUP) 6 patients with diagnosis of severe and/or refractory UV (F/M 5:1) with mean age of 62 years (range 43–74) were treated with OMA at dosage of 300 mg every 4 weeks, according to our experience in CSU (6). Written informed consent for off-label therapy was obtained from all the patients (University Hospital internal protocol, AOUP). Demographic and clinical characteristics were collected, including co-morbidities and current and previous pharmacological treatments for UV. According to the improvement in skin (long-lasting wheels, itch, burning, pain) and systemic (arthralgia, asthenia, abdominal pain, fever and lymphadenopathy) symptoms in response to OMA treatment, the patients were classified as responders, partially responders or not responders and any adverse side effects were recorded. The levels of IgE in the sera of UV patients were also measured before staring OMA treatment.
As reported in Table 1, in all the 6 patients evaluated the results of the immunohystochemistry analysis of skin biopsies were consistent with the diagnosis of UV, mainly revealing a lymphocytic/mononuclear infiltrate. Four out of the 6 patients reported systemic symptoms, including arthralgia, asthenia, abdominal pain, fever and lymphadenopathy, without ocular, renal, or cardiovascular involvement. According to the levels of complement components (C3 and C4), all UV evaluated were classified as NUV and none of them had anti-C1q antibodies. All of the patients had co-morbidities such as infectious diseases and/or malignancies and/or autoimmune diseases, however their UV were un-responsive to the pharmacological treatment for the underlying diseases. Before OMA treatment, all the patients had previously received oral corticosteroids, 5 of them also immunomodulatory and/or immunosuppressive drugs (see Table 1). Only one patient underwent previous biological therapies with anakinra and canakinumab due to severe and refractory disease. Reliever or daily administration of second generation H1-antihistamines were maintained in all the patients during the treatment with OMA. In 4 out of the 6 patients evaluated, a complete resolution of skin symptoms was achieved since the 1st OMA injection. As reported in Table 1, one patient was a partial responder (according to the improvement of skin symptoms) and this was observed after the 3rd injection. In most of our cohort, the improvement of both skin and systemic symptoms was observed since the 1st injection. Among the six patients evaluated, only one did not achieve any improvement in skin symptoms before the 4th OMA injection. She partially improved her long-lasting skin lesions from the 4th to the 6th injection and she was not responder anymore from the 7th injection. According to the clinical history of this patient, the discontinuation of OMA treatment was decided after the 10th injection.
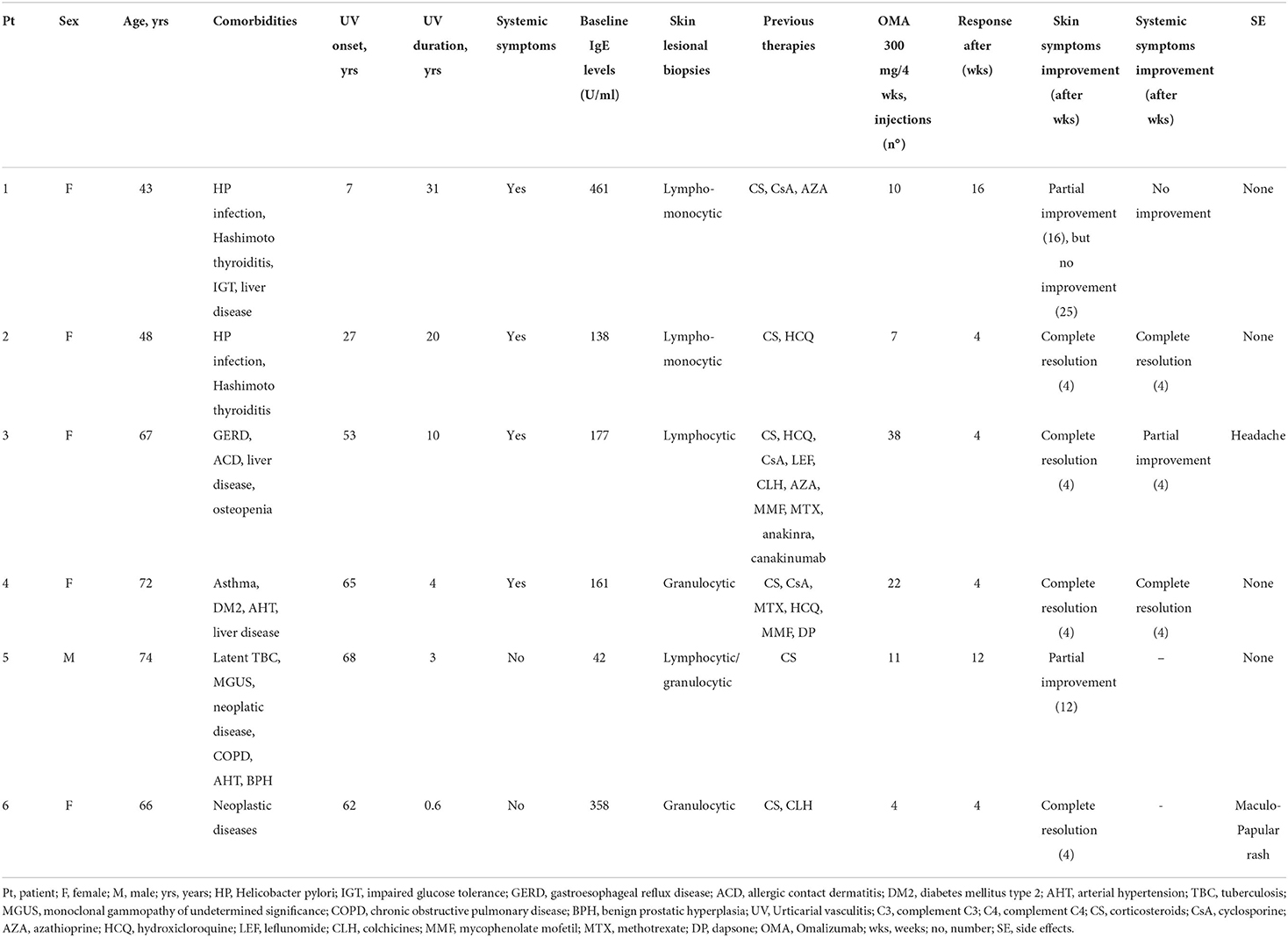
Table 1. Demographic and clinical characteristics of patients with normocomplementemic UV.
During the OMA treatment some common mild/moderate side effects such as headache were reported and in one case a maculo-papular rash occurred after the 4th injection.
In our experience, OMA, used at dosage of 300 mg every 4 weeks, proved to be a safe and effective therapeutic option in severe and/or refractory UV, for which no drugs are currently approved. Thus, the possibility to treat severe and/or refractory UV with manageable drugs such as OMA, that improves the quality of life of these patients, is an important goal for physicians managing UV patients. Few reports have already described the efficacy of OMA in treatment of different forms UV. However, the dosage of OMA and the interval between injections are not concordant among these clinical reports. This is probably due to the heterogenicity of the patients in terms of co-morbidities and/or clinical manifestations and/or laboratory data.
Even though the precise mechanisms of action of this biological agent are still to be clarified, we can postulate that its efficacy in UV treatment is probably due to its ability to reduce circulating IgE, and their binding to membrane of mast cells and basophils, that finally leads to downmodulation of cellular activation and/or inflammatory cells chemotaxis and/or immune complex formation (7).
A limit of our study is that it was a single arm open-label designed and further designed randomized double blind placebo control clinical studies are required. We have to take into account that in further studies large sample groups with different clinical phenotypes of UV should be included. On the whole our report suggests that OMA might be a promising option in the treatment of UV. The major improvement observed during OMA treatment was at skin level and was observed since the 1st injection. It could be interesting to modify dosage and administration frequency of this biological drug in partially or not responders UV patients.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study.
FP, DG, SB, ID, VR, PM, and IP made substantial contributions to conception and design, acquisition of data, interpretation of data, reviewed it critically for important intellectual content, given final approval of the version to be published, and agree to be accountable for all aspects of the work related to its accuracy or integrity. FP, DG, and IP drafted the article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Marzano AV, Maronese CA, Genovese G, Ferrucci S, Moltrasio C, Asero R, et al. Urticarial vasculitis: Clinical and laboratory findings with a particular emphasis on differential diagnosis. J Allergy Clin Immunol. (2022) 149:1137–49. doi: 10.1016/j.jaci.2022.02.007
2. Gu SL, Jorizzo JL. Urticarial vasculitis. Int J Womens Dermatol. (2021) 7:290–7. doi: 10.1016/j.ijwd.2021.01.021
3. Nazzaro G, Maronese CA. Urticarial vasculitis following mRNA anti-COVID-19 vaccine. Dermatol Ther. (2022) 35:e15282. doi: 10.1111/dth.15282
4. Kolkhir P, Grakhova M, Bonnekoh H, Krause K, Maurer M. Treatment of urticarial vasculitis: A systematic review. J Allergy Clin Immunol. (2019) 143:458–66. doi: 10.1016/j.jaci.2018.09.007
5. de Brito M, Huebner G, Murrell D, Bullpitt P, Hartmann K. Normocomplementaemic urticarial vasculitis: effective treatment with omalizumab. Clin Transl Allergy. (2018) 8:37. doi: 10.1186/s13601-018-0222-y
6. Puxeddu I, Petrelli F, Angelotti F, Croia C, Migliorini P. Biomarkers In Chronic Spontaneous Urticaria: Current Targets And Clinical Implications. J Asthma Allergy. (2019) 12:285–95. doi: 10.2147/JAA.S184986
Keywords: urticarial vasculitis, omalizumab, anti IgE, therapy, biological agent
Citation: Petrelli F, Giannini D, Bilia S, Del Corso I, Rocchi V, Migliorini P and Puxeddu I (2022) Efficacy and safety of omalizumab therapy in urticaria vasculitis. Front. Allergy 3:952079. doi: 10.3389/falgy.2022.952079
Received: 24 May 2022; Accepted: 04 July 2022;
Published: 22 July 2022.
Edited by:
George N. Konstantinou, 424 General Military Hospital, GreeceReviewed by:
Andreas Recke, University of Lübeck, GermanyCopyright © 2022 Petrelli, Giannini, Bilia, Del Corso, Rocchi, Migliorini and Puxeddu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Paola Migliorini, cGFvbGEubWlnbGlvcmluaUBtZWQudW5pcGkuaXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.