 Mitra Moodi1†
Mitra Moodi1† Hamid Salehiniya
Hamid Salehiniya Morteza Arab-Zozani
Morteza Arab-Zozani
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Sustain. Food Syst., 15 March 2023
Sec. Nutrition and Sustainable Diets
Volume 7 - 2023 | https://doi.org/10.3389/fsufs.2023.951698
This article is part of the Research TopicFood Systems, Food Insecurity, and Racial and Ethnic Health DisparitiesView all 5 articles
Introduction: The right to food is a human right. Food insecurity refers to the inability to prepare proper and healthy food. Food insecurity is associated with adverse outcomes among households. To determine the prevalence of food insecurity, its level, and the factors affecting it among households covered by health centers in marginalized areas of Birjand city.
Methods: This descriptive-analytical cross-sectional study was performed on 396 households aged 20-60 years covered by health centers in the marginal areas of Birjand in 2019. We used a 9-item Household Food Insecurity Access Scale (HFIAS) questionnaire. Chi-square, Fisher, and logistic regression analyses were performed using SPSS 22 software at a significance level of less than 0.05.
Results: The mean age of the subjects was 34.04 ± 9.41 years. In total, 48% of the subjects had a level of food insecurity, of which 7.6% had severe, 12.6% moderate, and 27.5% mild insecurity. The prevalence of food insecurity in families with low members and higher levels of education is significantly lower (p < 001). Backward Logistic regression showed that illiteracy (OR: 8.26) and primary education (OR: 2.65), rental housing status (OR: 1.69), lower-income levels being covered by support organizations (OR: 3.13), employed members between 3-4 and more than five (OR: 2.73 and 2.93, respectively), and low weight (OR: 2.55) were associated with food insecurity. The prevalence of food insecurity in this study was high.
Conclusion: The high prevalence of insecurity in studied households is an alarm for the authorities, which can be due to poverty and the low level of nutritional literacy of households' heads and mothers. Helping to improve the quality of life of families and food insecurity of households by improving physical and economic access, increasing literacy and nutritional culture, and reducing the burden of non-communicable diseases related to nutrition is a suggested solution.
Food and nutrition are among the basic needs of human society (Alimoradi et al., 2015). Food security is the concept that arises from the availability, affordability, and utilization of food (Gustafson et al., 2016). It is one of the most important health, social, economic, and political issues in different countries, especially in low and middle-income countries (Behzadifar et al., 2016). Iran has been at a moderate risk in terms of food insecurity in the 2013 map (Rezazadeh et al., 2016). Regarding the importance of the issue, food security is considered in the Constitution Vision 1404 Document, Fourth and Fifth Development Plans of Iran (Holben and Pheley, 2006). Also, the US Food and Agriculture Organization (FAO) and the World Bank have identified it as one of the Millennium Development Goals (MDGs) (Drewnowski and Specter, 2004).
Food security is defined as the access of all households at all times to adequate food for a healthy and active life. The major goals of food security are two-fold. The first goal is to provide nutritionally healthy and adequate food. The second is ensuring that decent food is supplied in a way that is acceptable to society (Mohammadzadeh et al., 2011). According to this definition, food security requires better access to a desirable and sufficient food pattern based on the three principles of nutritional adequacy, diversity, and balance (Broussard, 2019).
In general, based on the results of a meta-analysis and regardless of the scale used, the prevalence of food insecurity among households, children, mothers, female-headed households, low-income groups, and elderly households in the country is 49, 67, 61, 75, 86, and 65%, respectively (Behzadifar et al., 2016). According to the Iran's National Food and Nutrition Security Monitoring System, in 2017, fourteen provinces were in a relatively insecure to very insecure food situation (Alimoradi et al., 2015). The results of another study conducted in Iran also indicated that 20% of the society has economic problems to solve abdominal satiety and about 50% to provide cellular satiety (Ghassemi, 1997). According to available data (Ghassemi, 1997), one-fifth of households are deficient in energy and protein, and half of them are deficient in micronutrients (such as Calcium, Vitamin A, and Vitamin B) (Ghassemi, 1997).
Some relationships have been observed between non-communicable diseases (NCDs) such as obesity, overweight and hypertension and food insecurity (Huizar et al., 2020). The reason is that populations with food insecurity consume cheap food with high energy content but low in terms of micronutrients (Drewnowski and Specter, 2004; Mohammadzadeh et al., 2011), fruits, vegetables, milk and dairy products (Pollard and Booth, 2019). These cases are more common in suburban residents who have characteristics such as lack of fundamental infrastructure, high unemployment rate, low water, and environmental health, inadequate housing, insecurity, violence, and poor health indicators (Mutua et al., 2011).
Given that food insecurity is an indicator of household and individual health and inadequate food causes developmental, health, and nutritional problems, monitoring food insecurity and examining its factors are necessary for any society. Also, measuring and monitoring food insecurity and hunger can greatly help policymakers, support organizations, and other institutions to design the necessary programs and interventions, as well as monitoring and evaluating them (Ramesh, 2009; Ramesh et al., 2010). Due to the lack of a study on the prevalence of food insecurity in marginalized areas in Iran, especially in Birjand, the present study aims to determine the prevalence of food insecurity and the factors affecting it among households covered by health centers in marginalized areas around the Birjand city in 2019.
This descriptive-analytical cross-sectional study was performed on 396 households covered by health centers in the marginal areas of Birjand city in 2019. These areas are considered marginal for various reasons. These areas usually exist on the outskirts of the city, and urban developments and facilities are weak in them. Usually poor families who cannot afford proper housing live in these areas because the housing built in these areas is usually illegal.
Individuals were selected according to the population of each center (6 suburban centers). For this purpose, the number of samples for each center was determined proportional to the size, and random sampling was performed in each center based on the list of women 20–60 years in the SIB system (sib.bums.ac.ir). The SIB is an integrated health system that includes all data related to households and type of services.
The valid and reliable questionnaire of Household Food Insecurity Access Scale (HFIAS) consisting of nine questions was used to collect data. The HFIAS consists of two types of related questions. The first question type is called an occurrence question. There are nine occurrence questions that ask whether a specific condition associated with the experience of food insecurity ever occurred during the previous four weeks (30 days). Each severity question is followed by a frequency-of-occurrence question, which asks how often a reported condition occurred during the previous four weeks. Each occurrence question consists of the stem (timeframe for recall), the body of the question (refers to a specific behavior or attitude), and two response options (0 = no, 1 = yes). There is also a “skip code” next to each “no” response option. This code instructs the enumerator to skip the related frequency-of-occurrence follow-up question whenever the respondent answers “no” to an occurrence question. Each HFIAS frequency-of-occurrence question asks the respondent how often the condition reported in the previous occurrence question happened in the previous four weeks. There are three response options representing a range of frequencies (1 = rarely, 2 = sometimes, 3 = often). This tool categorizes households into four levels of household food insecurity (access): food secure, mild, moderately, and severely food insecure using the HFIAP indicator. The higher the score, the more food insecurity (access) the household experienced. The lower the score, the less food insecurity (access) a household experienced (Coates et al., 2007).
One trained employee collected the data regarding anthropometric information. Participants' weight was measured with a digital scale. If the BMI of the participants was less than 18.5 categorized as underweight, if the BMI was 25.0 to <30, it falls within the overweight range, and If the BMI was 30.0 or higher, it falls within the obesity range. Income levels were classified based on the salary of the head of household in three category (low: <50,000,000 Rial, moderate: 50,000,000–1,50,000,000 Rial, and high: >1,50,000,000 Rial)
All participants filled out the informed consent form before entering the study. Also, our study was approved by the ethics committee of Birjand University of Medical Sciences (ethical code: IR.BUMS.REC.1399.284).
Descriptive tests, Chi-square, Fisher, and logistic regression analysis were performed using SPSS 22 software at a significance level of less than 0.05.
In this study, 396 women participants entered the final analysis. The mean age of the subjects was 34.04 ± 9.41 years. Most of the subjects were married (93.9%). Other socio-demographic aspects of the subjects are presented in Table 1.
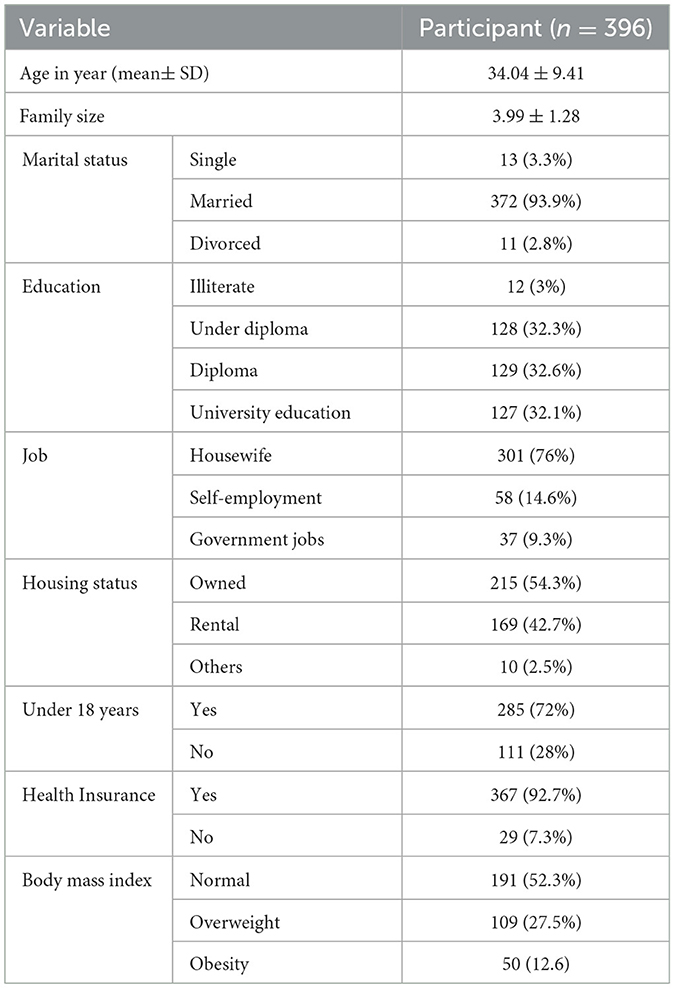
Table 1. Socio-demographic information of the participants.
According to the results, a high percentage of the subjects were overweight (27.5%) or obese (12.6%). About half of the subjects had some degree of food insecurity, of which 7.6% had severe, 12.6% moderate, and 27.5% mild insecurity (Figure 1).
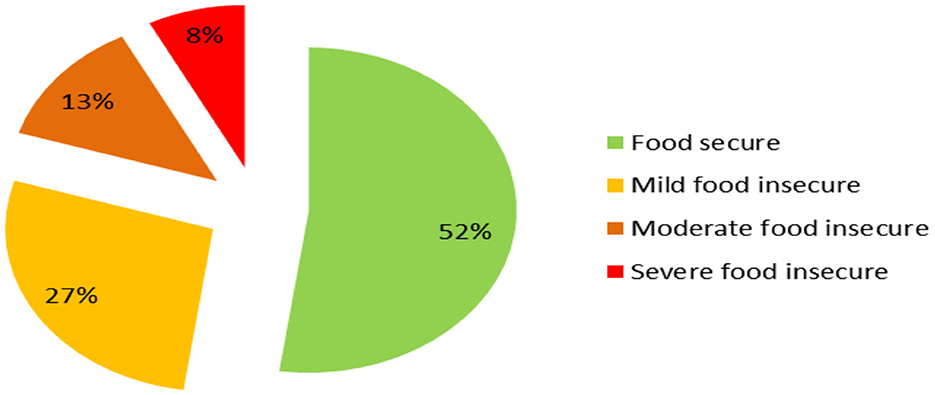
Figure 1. Level of household food insecurity in the selected sample.
There was no significant relationship between family size and the prevalence of food insecurity. However, the prevalence of food insecurity in families with low members and higher levels of education is significantly lower (p < 001) (Table 2). Only 16.8% of households with primary education and 67.7% of households with university education had food security. The prevalence of food security among women in government employment (73%) is higher than that of housewives and women in private employment.
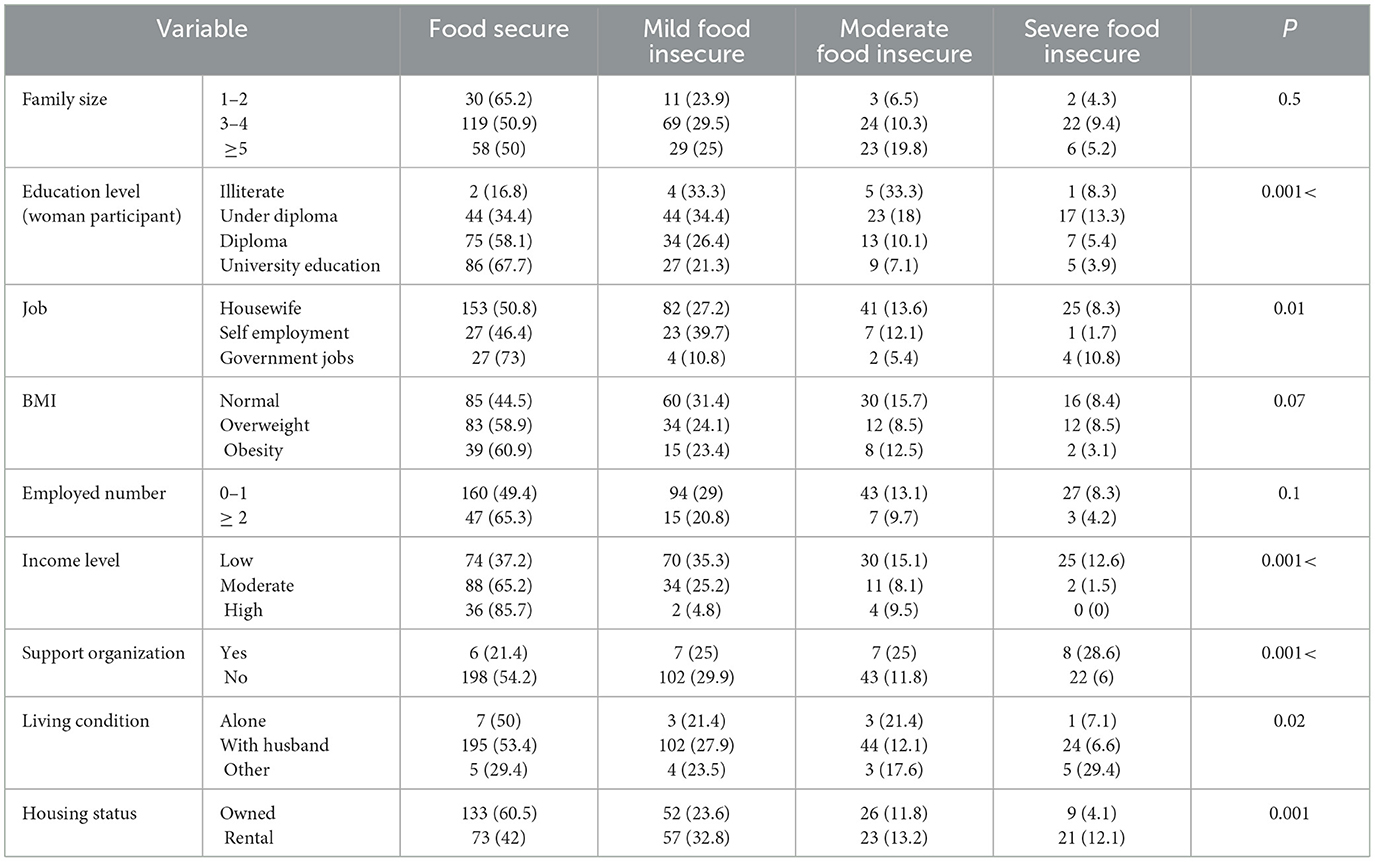
Table 2. Food insecurity levels based on socio-demographic and economic variables.
There was no significant relationship between food insecurity and the number of households working in the family (p = 0.1), but the relationship between the prevalence of food insecurity and income level was statistically significant. Households with low-income had 37.7% food security and households with a good income had 85.7% food security (p > 001). This relationship was also observed between the types of housing such that 42% of tenants had food security compared to 60.5% of households who won a house. Moreover, those who lived with grandchildren or other family members had low food security (29.9%). This relationship is statistically significant (p = 0.02). Also, those who are covered by support organizations have less food security than those who are not covered by support organizations (21.4 vs. 54.2%).
Backward Logistic regression was used to examine the relationship between variables related to food insecurity. Based on this analysis, in the final model, illiteracy (odds ratio: 8.26) and primary education (2.65), rental housing status (1.69), lower-income levels (medium and low), being covered by support organizations (odds ratio: 3.13), employed member between 3 and 4 and more than five (odds ratio: 2.73 and 2.93, respectively), lack of health insurance coverage (odds ratio: 3.13), and low weight (odds ratio: 2.55) were associated with food insecurity (Table 3).
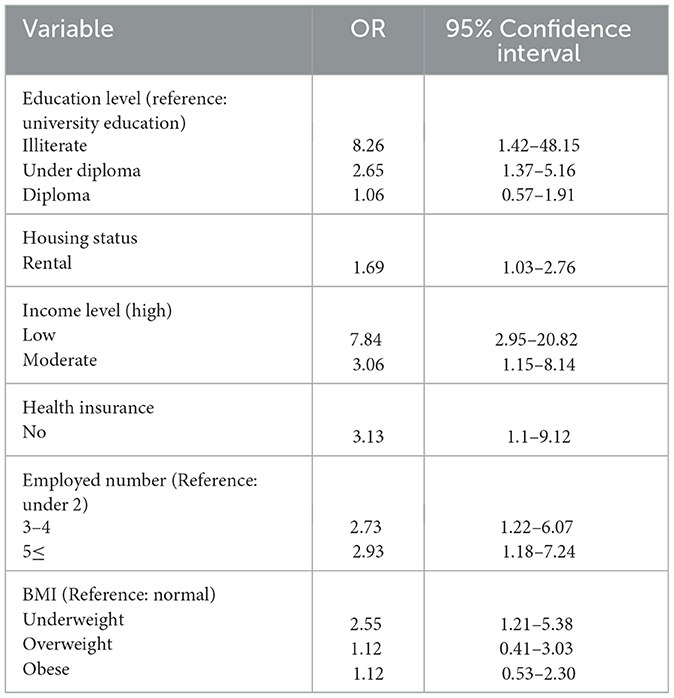
Table 3. Adjusted logistic regression for factors related to food insecurity.
The results of the present study showed that about 48% of the subjects had some degree of food insecurity, of which 7.6, 12.6, and 27.5% had severe, moderate, and mild insecurity, respectively. The results of this study can be the beginning of government support for intervention programs to create food security in the region such that it can lead to the right and informed decisions in this regard.
In line with the results of the present study, it has been reported that food insecurity is evident in small towns, suburbs, and villages (Sharkey et al., 2012). About 48% of the participants had experienced one of the types of food insecurity, which is in line with the study of Abbasi et al. (2016) conducted on suburban households and villages of Alborz province (Abbasi et al., 2016).
Findings have shown that the prevalence of food insecurity has a significant relationship with the number of family members so that food insecurity is less in small families. This finding is consistent with the results of a study by Ramesh et al. (2010), Che and Chen (2001), Willows et al. (2009), Foley et al. (2010), who showed that a significant positive relationship between family size (number of children) and food insecurity (Che and Chen, 2001; Willows et al., 2009; Foley et al., 2010; Ramesh et al., 2010). This important relationship can be explained by the fact that the small size of the families allows providing food and thus food security for family members. As the size of the family increases, the need for food increases as well. Large families are sometimes forced to reduce the amount and number of meals to provide food for family members, resulting in food insecurity. This is related to another finding in the present study that households who lived with grandchildren or other family members had lower food security. This relationship can be attributed to the fact that living with grandchildren or other family members increases the number of family members, so the amount of food required increases, and food security decreases (Sotoudeh et al., 2016).
The results of this study showed that the prevalence of food insecurity is significantly lower at higher education and university levels. This may be because households with higher levels of education have more job opportunities so they can earn more. Following the increase in income, they can provide a variety of foods. As the parents' education level increases, their awareness, attitudes, and actions about family nutrition improve. A high level of education can also increase the level of knowledge about nutrition and affect all stages of purchasing, preparation, cooking, and consumption, and thus provide food security for the family. The results of the present study are consistent with those of Dastgiri et al. (2006), Mohammadzadeh and Eshraghian (2010), Mohammadzadeh et al. (2010), Payab et al. (2012), and Hakim et al. (2011).
However, the results of the current study are inconsistent with those of Shariff and Khor (2005) who reported a relationship between father's education and food insecurity, but no significant relationship between household food insecurity and maternal education (Shariff and Khor, 2005). Also, in 2008, studies in Brazilian and Australian households showed that parents' academic education did not have a significant effect on household food insecurity (Panigassi et al., 2008; Foley et al., 2010).
The prevalence of food security among women who had government jobs was highest. This finding is consistent with the results of Sotoudeh et al. (2016), who showed a significant relationship between food insecurity and maternal job status, and Mohammadzadeh et al. (2010) who reported a significant relationship between food insecurity and job status of the head of the household (Sotoudeh et al., 2016). Dastgiri et al. (2006) also showed that as the job status of the head of the household increases, the level of food insecurity decreases. Kaiser et al. (2004), Che and Chen (2001), and Shariff and Khor (2005) conducted a study on Canadian household heads, rural women in Malaysia, and rural women in California, respectively. They revealed a significant relationship between food insecurity and job status (Che and Chan, 2001; Kaiser et al., 2004; Shariff and Khor, 2005). Payab et al. (2012) identified a statistically significant relationship between job position of the head of the household and food insecurity (Payab et al., 2012), but no significant relationship between the job status of the mother and food insecurity. This finding is similar to the results of a study by Shariff and Khor (2005) on Malaysian households.
In general, employment status is an important predictor of food security because it generates income and provides the power to buy food. Children in low-income families often experience one of the stages of food insecurity more than those of higher-income families. The employment of the mother can lead to food insecurity because the mother has less time to cook and buy food. Also, mothers of families with low-income are forced to work outside the home to help support their family's economic situation.
There was a significant relationship between the prevalence of food insecurity and income level so that 62.8 and 14.3% of food insecurity were reported in low- and high-income households, respectively. Higher-income families have more opportunities to get the food they need. This finding is in line with the results of the study of Sotoudeh et al. (2016) who stated that food insecurity has a significant relationship with household economic status among short and overweight children in Zahedan (Sotoudeh et al., 2016). Ramesh (2009) also reported the household economic status among the main predictors of food insecurity. Another finding of this study is that households covered by support organizations had lower food security than those not covered by support organizations. This important relationship can be justified by the fact that households covered by support organizations are not able to provide a variety of food due to their poor economic situation and low income.
In this study, a significant relationship was observed between the type of housing and food insecurity, with 42% of tenants vs. 60.5% of households living in the estate had food security. Ramesh. (2009), Payab et al. (2012), and Mohammadzadeh et al. (2011) showed a significant inverse relationship between residential home ownership status and household food insecurity (Ramesh, 2009; Mohammadzadeh et al., 2011; Payab et al., 2012). In most studies, homeownership is a part of the household wealth such that in the case of rent and mortgage, an additional economic burden is imposed on the household, which reduces the money for buying food.
Based on our results, a relationship was observed between health insurance coverage and food insecurity, so health insurance coverage reduces food insecurity. In support of our results, several studies showed a significant relationship between health insurance coverage and household food insecurity (Tarasuk et al., 2015; Antabe et al., 2019; Dean et al., 2020). In general, uninsured People are more likely to be food insecure (Garcia et al., 2018). Based on the literature, more than one-half of enrollees in a medical clinic reported an easier time purchasing food after enrollment into public insurance (Patel et al., 2019). Therefore, it seems that the implementation of universal health insurance coverage programs is a suitable solution to reduce food insecurity and its consequences (Johnson et al., 2021; Lee et al., 2022).
About half of the households in marginalized areas of Birjand have food insecurity. Food insecurity among the households in the marginalized Birjand is found to be high and can be attributed to several factors such as education, income, family size, and so on. As there has been no data on the nutritional literacy of the household head (or was any data collected on the knowledge of nutrition of the household head) we cannot attribute the household food insecurity to nutrition literacy. Also, our results showed that households headed by women are more likely to be vulnerable to food insecurity.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Birjand University of Medical Sciences (ethical code: IR.BUMS.REC.1399.284). The patients/participants provided their written informed consent to participate in this study.
MM and MA-Z: idea, design, writing the draft, and approval of the final version. HS: idea, design, analyses, and approval of the final version. SM and ZA: data collection, writing the draft, and approval of the final version. All authors contributed to the article and approved the submitted version.
This research was supported by Birjand University of Medical Sciences (Grant number: 5253; 26.09.2020, ethical code: IR.BUMS.REC.1399.284).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbasi, N., Ghoochani, O., Ghanian, M., and Kitterlin, M. (2016). Assessment of Households' food insecurity through use of a USDA questionnaire. Adv. Plants Agric. Res. 4, 1–8. doi: 10.15406/apar.2016.04.00155
Alimoradi, Z., Kazemi, F., Estaki, T., and Mirmiran, P. (2015). Household food security in Iran: systematic review of Iranian articles. Adv. Nurs. Midwif. 25, 63–76.
Antabe, R., Atuoye, K. N., Sano, Y., Kuuire, V. Z., Galaa, S. Z., and Luginaah, I. (2019). Health insurance enrolment in the Upper West region of Ghana: does food security matter? Int. J. Health Plann. Manage. 34, e1621–e1632. doi: 10.1002/hpm.2857
Behzadifar, M., Abdi, S., Malekzadeh, R., Salmani, M. A., Ghoreishinia, G., Falahi, E., et al. (2016). Prevalence of food insecurity in Iran: A systematic review and meta-analysis. Arch. Iran. Med. 19, 288–294.
Broussard, N. H. (2019). What explains gender differences in food insecurity? Food Policy 83, 180–194. doi: 10.1016/j.foodpol.2019.01.003
Coates, J., Swindale, A., and Bilinsky, P. (2007). Household Food Insecurity Access Scale (HFIAS) for Measurement of Food Access: Indicator Guide: Version 3.
Dastgiri, S., Mahboob, S., Tutunchi, H., and Ostadrahimi, A. (2006). Determinants of food insecurity: a cross–sectional study in Tabriz. J. Ardabil Univ. Med. Sci. 6, 233–239.mQ20
Dean, E. B., French, M. T., and Mortensen, K. (2020). Food insecurity, health care utilization, and health care expenditures. Health Serv. Res. 55, 883–893. doi: 10.1111/1475-6773.13283
Drewnowski, A., and Specter, S. E. (2004). Poverty and obesity: the role of energy density and energy costs. Am. J. Clin. Nutr. 79, 6–16. doi: 10.1093/ajcn/79.1.6
Foley, W., Ward, P., Carter, P., Coveney, J., Tsourtos, G., and Taylor, A. (2010). An ecological analysis of factors associated with food insecurity in South Australia, 2002–7. Public Health Nutr 2010 13, 215–221. doi: 10.1017/S1368980009990747
Garcia, S. P., Haddix, A., and Barnett, K. (2018). Peer reviewed: incremental health care costs associated with food insecurity and chronic conditions among older adults. Prevent. Chron. Dis. 15. doi: 10.5888/pcd15.180058
Ghassemi, H. (1997). Food and nutrition security in Iran: a study on planning and administration. Tehran: Planning and Budget Organization.
Gustafson, D., Gutman, A., Leet, W., Drewnowski, A., Fanzo, J., and Ingram, J. (2016). Seven food system metrics of sustainable nutrition security. Sustainability 8, 196. doi: 10.3390/su8030196
Hakim, S., Dorosty, A., and Eshraqian, M. (2011). Relationship between food insecurity and some of socioeconomic factors with BMI among women in Dezfoul. Iran. J. School Public Health 2, 55–66.
Holben, D. H., and Pheley, A. M. (2006). Peer reviewed: diabetes risk and obesity in food-insecure households in rural Appalachian Ohio. Prevent. Chron. Dis. 3, 3.
Huizar, M. I., Arena, R., and Laddu, D. R. (2020). The Global Food Syndemic: The Impact of Food Insecurity, Malnutrition, and Obesity on the Healthspan Amid the COVID-19 Pandemic. Progress in cardiovascular diseases.
Johnson, K. T., Palakshappa, D., Basu, S., Seligman, H., and Berkowitz, S. A. (2021). Examining the bidirectional relationship between food insecurity and healthcare spending. Health Serv. Res. 56, 864–873. doi: 10.1111/1475-6773.13641
Kaiser, L. L., Townsend, M. S., Melgar-Quinonez, H. R., and Fujii ML., and P. B. C. (2004). Choice of instrument influences relations between food insecurity and obesity in Latino women. Am. J. Clin. Nutr. 80, 1372–1378.
Lee, W. C., Lin, S., Yang, T. C., and Serag, H. (2022). Cross-sectional study of food insecurity and medical expenditures by race and ethnicity. Ethn. Health 1–15. doi: 10.1080/13557858.2022.2161090
Mohammadzadeh, A. D. A, and Eshraghian, M. R. (2010). Relationship between food insecurity and some of socioeconomic factors and status of weight in high school students. Iran. J. Nutri. Sci. Food Technol. 5, 55–62.
Mohammadzadeh, A., Dorosty Motlagh, A., and Eshraghian, M. (2010). The association of food security with socio-economic factors and weight status among adolescents. Iran. J. Nutri. Sci. Food Technol 5, 55–62.
Mohammadzadeh, A., Dorosty, A., and Eshraghian, M. (2011). Household food security status and food consumption among high school students in Esfahan, Iran. Iran. J. Epidemiol. 7, 38–43.
Mutua, M. K., Kimani-Murage, E., and Ettarh, R. R. (2011). Childhood vaccination in informal urban settlements in Nairobi, Kenya: who gets vaccinated? BMC Public Health 11, 6. doi: 10.1186/1471-2458-11-6
Panigassi, G., Segall-Correa, A. M., Marin-Len, L., Perez-Escamillla, R., Sampaio Mde, F., and Maranha, L. K. (2008). Food insecurity as an indicator of inquity: analysis of a population survey. Cad Saude Public 24, 2376–2384. doi: 10.1590/S0102-311X2008001000018
Patel, K. G., Borno, H. T., and Seligman, H. K. (2019). Food insecurity screening: a missing piece in cancer management. Cancer 125, 3494–3501. doi: 10.1002/cncr.32291
Payab, M., Dorosty, A., Eshraghian, M., Siassi, F., and Karimi, T. (2012). Association of food insecurity with some of socioeconomic and nutritional factors in mothers with primary school child in Rey city. Iran. J. Nutri. Sci. Food Technol. 7, 75–84.
Pollard, C. M., and Booth, S. (2019). Food insecurity and hunger in rich countries—It is time for action against inequality. Int. J. Environ. Res. Public Health 16, 1804. doi: 10.3390/ijerph16101804
Ramesh, T. (2009). The Prevalence of Food Insecurity and Some Associated Factors Among Shirazian Households in 2009 [dissertation]. Tehran: Shahid Beheshti University: MC.
Ramesh, T., Dorosty Motlagh, A., and Abdollahi, M. (2010). Prevalence of household food insecurity in the City of Shiraz and its association with socio-economic and demographic factors, 2008. Iran. J. Nutri. Sci. Food Technol. 4, 53–64.
Rezazadeh, A., Omidvar, N., Eini-Zinab, H., Ghazi-Tabatabaie, M., Majdzadeh, R., Ghavamzadeh, S., et al. (2016). Food insecurity, socio-economic factors and weight status in two Iranian ethnic groups. Ethn. Health 21, 233–250. doi: 10.1080/13557858.2015.1061102
Shariff, Z. M., and Khor, G. L. (2005). Obesity and household food insecurity: evidence from a sample of rural households in Malaysia. Eur. J. Clin. Nutr. 59, 1049–1058. doi: 10.1038/sj.ejcn.1602210
Sharkey, J. R., Dean, W. R., and Nalty, C. (2012). Convenience stores and the marketing of foods and beverages through product assortment. Am. J. Prev. Med. 43, S109–S115. doi: 10.1016/j.amepre.2012.05.012
Sotoudeh, M., Safarian, M., Dorosty, A., Dashipour, A., Khodabakhshi, A., and Montazerifar, F. (2016). The association of food insecurity and dietary patterns with simultaneous obesity and stunting in primary school pupils of Zahedan City (Iran). Iran. J. Nutri. Sci. Food Technol. 10, 53–62.
Tarasuk, V., Cheng, J., De Oliveira, C., Dachner, N., Gundersen, C., and Kurdyak, P. (2015). Association between household food insecurity and annual health care costs. CMAJ 187, E429–E436. doi: 10.1503/cmaj.150234
Keywords: food insecurity, household, marginal area, Iran, developing countries
Citation: Moodi M, Salehiniya H, Mohtashaminia S, Amininasab Z and Arab-Zozani M (2023) Prevalence of household food insecurity in the marginal area of Birjand, Iran. Front. Sustain. Food Syst. 7:951698. doi: 10.3389/fsufs.2023.951698
Received: 24 May 2022; Accepted: 22 February 2023;
Published: 15 March 2023.
Edited by:
Kathleen L, Hefferon, Cornell University, United StatesReviewed by:
Shalander Kumar, International Crops Research Institute for the Semi-Arid Tropics (ICRISAT), IndiaCopyright © 2023 Moodi, Salehiniya, Mohtashaminia, Amininasab and Arab-Zozani. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Morteza Arab-Zozani, YXJhYi5odGFAZ21haWwuY29t; bW9ydGV6YS5hcmFiLnpvemFuaUBnbWFpbC5jb20=
†ORCID: Mitra Moodi orcid.org/0000-0002-8877-6609
Hamid Salehiniya orcid.org/0000-0001-7642-5214
Somayeh Mohtashaminia orcid.org/0000-0001-8946-5768
Zahra Amininasab orcid.org/0000-0002-0932-3645
Morteza Arab-Zozani orcid.org/0000-0001-7223-6707
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.