 Rosalia Facendola
Rosalia Facendola Giovanni Ottomano Palmisano
Giovanni Ottomano Palmisano Annalisa De Boni
Annalisa De Boni Claudio Acciani
Claudio Acciani Rocco Roma
Rocco Roma- Department of Soil, Plant and Food Science, University of Bari Aldo Moro, Bari, Italy
The transition to sustainable food systems and the achievement of SDGs 2 and 12 entails the adoption of sustainable consumption and production patterns, such as the Mediterranean diet. The Mediterranean diet and its impact on nutritional status and health have been the focus of recent research. The aim of this study was to investigate the associations between adherence to the Mediterranean diet, lifestyle, socioeconomic status, BMI (kg/m2), and age of children. The geographical area is the Metropolitan City of Bari (Apulia region, southern Italy), which is involved in the development of an effective food policy aimed at ensuring a sustainable food transition. An online survey was filled out by parents or guardians responsible for the dietary patterns of children between 2 and 15 years of age to collect data about their Mediterranean diet adherence through the Mediterranean Diet Quality Index (KIDMED) and sociodemographic features, food habits and lifestyles, and anthropometric variables. Descriptive statistics and k-means cluster analysis were applied for profiling children, contributing to identifying the main factors that might affect individual Mediterranean diet adherence. Four clusters were characterized, taking into account food habits and lifestyle index, socioeconomic index, children’s age, and body mass index (BMI). Results showed an association between low adherence to the Mediterranean diet and high prevalence of overweight and obesity in children. The factors positively associated with following an optimal Mediterranean diet adherence were the mother’s education level and level of income; skipping breakfast is linked to low adherence to the Mediterranean diet. Therefore, targeted strategies should be put in place to improve Mediterranean diet adherence among children, promoting healthy dietary habits.
1 Introduction
The concept of food security has deeply evolved over time, starting from the first generally acknowledged definition by the World Bank (1986), “secure access at all times to sufficient food for a healthy life” (Allen, 1987). This concept has evolved to a more holistic approach (Fardet and Rock, 2014), involving nutritional aspects related to adequate intake of protein (Burd et al., 2019), energy, vitamins, and minerals (Livingstone et al., 2022) for all people over time (Fardet and Rock, 2014). The term “Food Security and Nutrition” takes into account, besides food availability and accessibility, the use and utilization of food (Clapp et al., 2022). Namely, food availability relates to physical affordability, quality, and assortment of food and access to retail (Durao et al., 2015); accessibility is related to financial resources, transportation facilities, and distances (Rajasooriar and Soma, 2022); use and utilization of food refers to variables strongly influenced by the socioeconomic status and lifestyles of consumers (Monterrosa et al., 2020; Amin et al., 2021) (e.g., level of knowledge about nutrition facts, food preferences and rejection, and time devoted to purchasing and preparation of foods) (Godrich et al., 2017). Several studies (Burchi and De Muro, 2016; Bertoni et al., 2023) highlighted the importance of considering the broader meaning of food security; the acknowledgment of a strong tie between food and health requirements led to consider nutrition as an essential component of food security, merging both notions in the term “food security and nutrition” (FAO, 2021). However, a bunch of recent events threatened food and nutrition security worldwide, such as the COVID-19 pandemic (Zollet et al., 2021), the current Russia–Ukraine war (Ben Hassen and El Bilali, 2022; Nasir et al., 2022), and the Israeli–Palestinian conflict (Bar-Nahum et al., 2020), worsening food insecurity and nutrition (Lin et al., 2022). However, current agri-food systems have to shift toward sustainable food systems and diets to tackle this stress scenario (Agriculture and Economic Development Analysis Division, 2006; Hwalla et al., 2016). Furthermore, the efficiency of agri-food systems plays a major role in guaranteeing food security and nutrition (Ruiz-Almeida and Rivera-Ferre, 2019).
On this matter, the Mediterranean diet (MD) is considered a strategic resource to deal with the challenges affecting the Mediterranean region (Antonelli and Donelli, 2022) and to achieve SDGs 2 (Zero Hunger) and 12 (Responsible Consumption and Production) (Barros and Delgado, 2022) because it is widely recognized as a lever for sustainable consumption and production and for the adoption of healthy and sustainable lifestyle (Biasini et al., 2021; FAO, 2021) due to its emphasis on consumption of local, seasonal, and minimally processed food products favoring biodiversity (Mattas et al., 2023), traditional, and eco-friendly food products (Donini et al., 2016; Truzzi et al., 2020). The term Mediterranean diet pattern was initially defined in 1975 by Ancel Keys based on the traditional eating habits of people after the Second World War from countries of the Mediterranean basin (Keys et al., 1986); it was specific to Crete, a significant area of Greece and Southern Italy (Caprara, 2023). The MD is characterized by a nutritional model based on a high intake of fresh or dried fruits, vegetables, and cereals and a low-to-moderate intake of fish, meat, and dairy products (Davis et al., 2015; Serra-Majem et al., 2019); extra-virgin olive oil is mainly used as a condiment (Mazzocchi et al., 2019). It has been demonstrated that these dietary components are beneficial for countering the risk of developing several diseases, improving physical and mental health (Cena and Calder, 2020), and increasing life expectations (Martínez-González and Sánchez-Villegas, 2003; Bach-Faig et al., 2011).
Recent studies have confirmed numerous benefits of MD for children and adolescents (Rosi et al., 2019). In light of this evidence, a growing number of studies (Riolo et al., 2022; Arangia et al., 2023) have suggested the importance of implementing health promotion interventions in primary school settings (Aureli and Rossi, 2022). Despite these recognized benefits, there was a gradual abandonment of the Mediterranean diet (Cavaliere et al., 2018) among “vulnerable population” (Papadaki et al., 2023), such as children and adolescents (Leidy and Gwin, 2020; Aureli and Rossi, 2022; Zielińska et al., 2022); indeed, in this period, many factors influenced their eating habits (De Santi et al., 2020). This has been partly attributed to the globalization process through the widespread diffusion of Western-type dietary models (Azzam, 2021). The transition towards a Western diet has led to a high prevalence of overweight and obesity in countries supposed to adopt a traditional MD (Tsakiraki et al., 2011; Lacirignola et al., 2015; Grosso et al., 2017; Archero et al., 2018). On this matter, this phenomenon has affected not only the non-Mediterranean countries (Fernando et al., 2013; Sedaghat et al., 2019) but also those of the Mediterranean (Van Stralen et al., 2014; Beets et al., 2015; Pietrobelli et al., 2017; Arcila-Agudelo and Torres-Fernàndez, 2019; Mounayar et al., 2019; Grassi et al., 2020; El Hajj and Julien, 2021; Spinelli et al., 2021; Bibiloni et al., 2022), including the Italian young (Schröder et al., 2013; Rangelov et al., 2018; Maher et al., 2019).
In recent decades, the adherence to the Mediterranean diet (AMD) of adolescents has been adopted in Europe as a criterion for assessing their diet pattern (Mohammadi et al., 2022). Many scientific studies in several Mediterranean countries (Grams et al., 2022) have applied the “Mediterranean Diet Quality Index for Children and Adolescents” (KIDMED) as an effective approach to evaluate the adherence to MD in people between 2 and 24 years of age and developed by Serra-Majem et al. (2004).
Thus, the current study aimed to investigate the associations among children’s MD adherence, lifestyle, socioeconomic status, BMI (kg/m2), and age in a convenience sample of Apulian children aged 2 to 15 years. MD adherence was evaluated through the implementation of the KIDMED score index. The lifestyle index included components concerning physical activity status and sedentary behavior, eating at the school canteen, and food rejection. The socioeconomic index considered aspects concerning family income, parental education, and household composition. A k-means cluster analysis was applied to a set of indexes for profiling children and adolescents concerning their dietary behaviors and lifestyles, contributing to identifying the main factors that might affect individual MD adherence.
The geographical area considered in this research is the Metropolitan City of Bari (MCB), Apulia region (southern Italy), which is one of the cities involved in the FoodShift 2030 EU project (FoodSHIFT 2030, 2016) funded by the EU Horizon 2020. The innovative project’s approach focuses on supporting innovation toward a fast transition of the European food system by 2030 to address the pressing challenges for food and nutrition security, as well as to promote sustainable food diets (FoodSHIFT 2030, 2023). The Metropolitan city of Bari has drafted the “Manifesto for Sustainable Food Transition” (Ciba, 2023) as part of the FoodShift 2030 EU project toward the achievement of these targets and to foster the institutionalization of an effective food policy of the MCB.
This is the first study, to the best of our knowledge, attempting to classify children into different groups based on their food habits, sociodemographic characteristics, and lifestyle. The segmentation and profiling of these children could provide tangible actions to guide policymakers toward an effective food policy of the MCB and to advise effective long-term measures aimed at ensuring safe, healthy, sustainable, and nutritious food for vulnerable populations, such as children and adolescents.
This study adds to this field of research by exploring the relationship between healthy behaviors and adherence to MD in children and adolescents in a specific urban area. In addition, based on recent evidence, it emphasizes the crucial role of socioeconomic, anthropometric, and lifestyle variables in affecting food choices. The analysis sheds light on the role of unhealthy dietary behavior acquired during infancy that often consolidates into adulthood, generating overweight, inappropriate intake of key nutrients, and health issues.
2 Materials and methods
2.1 Data collection
Data were collected through a voluntary online survey administered from September to December 2022, addressed to parents or guardians responsible for the dietary patterns of children between 2 and 15 years of age living in the Metropolitan City of Bari (MCB). The validity and reliability of the survey were preliminarily tested according to a pilot study coordinated by the research group and involving a small group of children’s parents or their guardians. The survey was disseminated through social networks (e.g., WhatsApp, Facebook, and LinkedIn) and took approximately 15 min to fill out. Written informed consent was collected by participants in accordance with the national ethical requirement “Personal Data Protection Code” (D.L. no. 196/2003). The survey included a preface to inform about the objective of the study and the benefits of the MD on human health. The first part of the survey aimed to investigate MD adherence through the KIDMED questionnaire, while in the second part, the respondents were asked about their sociodemographic features, food and lifestyle habits, and children’s anthropometric information. Participants were recruited among parents or their guardians who were asked to share the empty questionnaire with acquaintances dealing with children and to fill in all fields. Through the snowball techniques, a convenience sample was obtained: it is not representative of the whole Italian population, but the method was considered effective in collecting a relevant amount of data in a brief period of time (Victoria-Montesinos et al., 2023). Moreover, data collection is less expensive than data detection carried out through other sampling methods (Bimbo et al., 2022). The final eligible sample consisted of 196 participants.
2.2 Questionnaire
The questionnaire was divided into two segments: the first part of the survey aimed to assess the MD adherence of children; meanwhile, the second part aimed to collect information on sociodemographic characteristics, food and lifestyle habits, and anthropometric measures. The KIDMED was applied to assess the MD adherence of the study sample. Indeed, this is a tool widely used to measure MD adherence in children and young people (Serra-Majem et al., 2004). It can be self-administered or conducted by interviewers (e.g., pediatricians and dietitians) (López-Gajardo et al., 2022). KIDMED consisted of 16 questions, 12 of which denoted positive connotations with respect to MD adherence, and 4 denoted negative aspects. Questions with a negative connotation were assigned a score of –1 (e.g., “takes sweets and candy several times every day”), while those with a positive connotation were assigned a score of +1 (e.g., “takes a fruit or fruit juice every day”) (Table 1). The index of MD adherence was calculated as the sum of each answer and ranged from −4 to 12 (Kontogianni et al., 2010), and it enabled to classify the adherence to MD as follows: i) ≤3, poor MD adherence; ii) 4 – 7, medium MD adherence; and iii) ≥ 8, high MD adherence. The second part of the survey aimed to collect information about the sociodemographic features of children and their families, including children’s age and gender (Maher et al., 2019), household monthly income, and whether both parents are employed (Marventano et al., 2018; Cardamone et al., 2023). Then, this survey gained information concerning the food and lifestyle habits of children. In particular, the items concerning food habits (Archero et al., 2018) were consumption frequency of cured meat (Hemeryck et al., 2022), carbonated and soft drinks (Lopez et al., 2012), street food, as well as the frequency of meals at restaurants or pizzerias (Archero et al., 2018; Penne and Goedemé, 2021; Bimbo et al., 2022; López-Gajardo et al., 2022). Further food habits explored were the occurrence of lunch at the school canteen (Lopez et al., 2012; Hemeryck et al., 2022), the presence of food intolerances or allergies, and food rejection. Finally, this survey collected information about the lifestyle habits (Hoffmann et al., 2018; Jia et al., 2021). In particular, the practice of sports and outdoor group activities was investigated by asking parents if their child did these activities for at least 60 min in the previous week (NeffatRIi et al., 2004; Penne and Goedemé, 2021). Other lifestyle habits explored were daily hours watching TV (including YouTube or similar services on smart TV, DVDs, and other types of entertainment) (Cohen et al., 2021; Penne and Goedemé, 2021) and family’s knowledge about the health benefits arising from the adoption of MD (Au et al., 2018; Spinelli et al., 2021).
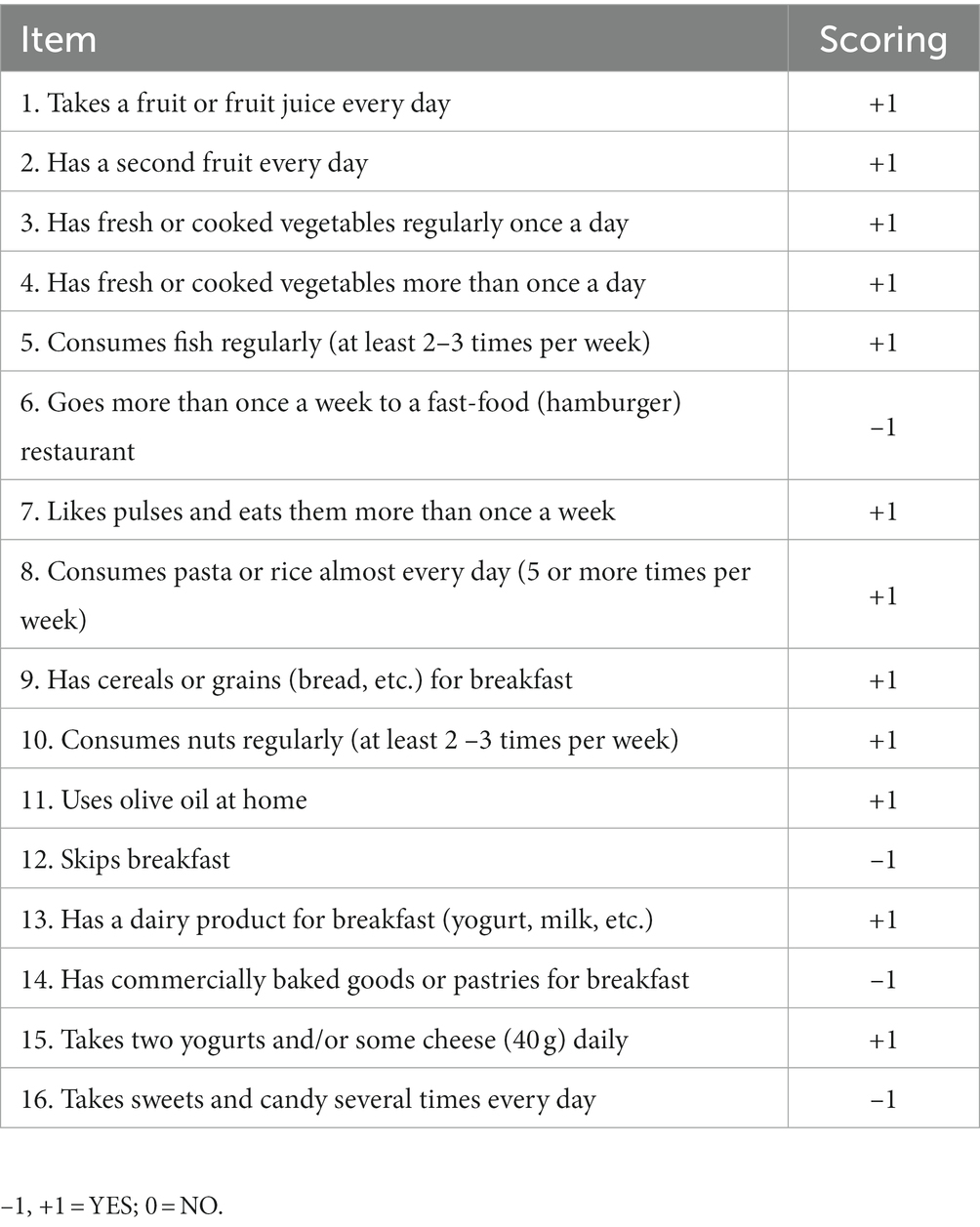
Table 1. KIDMED questions to assess the MD adherence.
2.3 Survey design
A healthy lifestyle index, i.e., the KIDMED score index, was established through the total scores of KIDMED questions to evaluate the MD. KIDMED score index was assigned to KIDMED-score ≥ 8, suggesting an optimal adherence to the MD; score 1 to KIDMED score 4–7, suggesting an average adherence to the MD and score 0 to KIDMED-score ≤ 3, suggesting a low adherence to the MD adherence (Serra-Majem et al., 2004; Katsagoni et al., 2020). A socioeconomic index was generated through the average sum of the total scores of the following variables: gender, father’s age, mother’s age, father’s education level, mother’s educational level, both parents’ employment, and monthly household income. Then, the socioeconomic index was evaluated through the assignment of three classes: low (score = 1), medium (score = 2), and high (score = 3). A lifestyle index was generated through the average sum of the total scores of the following variables: regularly playing sports, no. of hours daily spent watching TV, no. of hours daily using pc and videogames, outdoor group activities, informed on the benefits of the MD, food rejection, school canteen, purchase frequency of carbonated and soft drinks, consumption frequency of ready-to-eat food, and frequency of meals at restaurants or pizzeria. Then, the lifestyle index was evaluated through the assignment of four classes: inadequate (score = 1), low (score = 2), appropriate (score = 3), and optimum (score = 4). The anthropometric measurements, including weight and height, were measured and carried out by parents. Body mass index (BMI) was calculated by dividing weight (kg) by height squared (m2) for all children. Then, children were classified as normal weight, overweight, and obese based on the World Health Organization (WHO) age and sex-standardized BMI percentiles (De Onis, 2007; Mohammadi et al., 2022).
2.4 Statistical analysis
Data were submitted to two types of analyzes using IBM/SPSS software (version 21). First, a descriptive analysis was carried out to describe the sample. Data were expressed as means ± standard deviations (SD) for continuous variables and as numbers/percentages for categorical variables. Then, a multivariate analysis, K-means clustering based on the indices described above, BMI (kg/m2), and age class was carried out. In this research, four clusters proved to be the optimal number to avoid drawbacks (Callieris et al., 2016). Furthermore, the following variables: “monthly household income,” “mother’s education,” and father’s education” concerning the socioeconomic index, and the following variables: “food rejection,” “school canteen,” and “regularly play sport” concerning lifestyle index were considered for the k-means cluster analysis. Indeed, these variables influenced MD adherence, as highlighted in recent scientific literature.
Cluster analysis was frequently used in exploratory data analysis as data mining techniques (Vandeginste et al., 1998). Specifically, there are various techniques through which clusters have been produced, such as K-mean (Herman et al., 2022). K-mean cluster analysis was applied in this research; it is a typology of a hard partitioning algorithm (Weatherill and Burton, 2009). According to Duda and Hart (Duda and Hart, 1973), this specific algorithm splits the data set into K-clusters, so that K-clusters are as separated as possible in which each observation belongs to the cluster with the nearest mean. This aggregation occurs through an iterative process (Javadi et al., 2017). Furthermore, the distances between the current data vector and each of the centroids are computed, identifying the cluster whose centroid is closest to the current data vector (Javadi et al., 2017). The first step of this method is based on the calculation of the centroids for each cluster (K rows chosen at random) (Jain and Dubes, 1988; Park and Choi, 2022; Das et al., 2023). Subsequently, the randomly selected K objects from the data set occur as the initial cluster centers, and each data point is given to its closest centroid through the Euclidean distance. Furthermore, for each of the K clusters, the cluster centroid is updated by calculating the new mean values of all the data points in the cluster. Finally, it should iterate the last steps until the cluster assignments stop changing or the maximum number of iterations is reached (Miolla et al., 2023).
3 Results
3.1 Sample description
Table 2 displays the characteristics of the participants, relying on the following variables concerning their sociodemographic characteristics: age, gender, monthly household income, both parents employed, one child, parental education, and parental age. Additional, food habits than those already considered, lifestyle, and healthy variables were described. Finally, weight, height, and body mass index were described. Regarding the sociodemographic characteristics, more than half of respondents (64.8%) were 6–10 years old and male (53.6%). Moreover, respondents were almost equally distributed into the low-middle level of monthly household income, specifically between 1,000 and 2,000 € (38.8%) and 2,100 and 3,200 € (38.8%). Most of the respondents (72.4%) declared to have more than one child in the household. Furthermore, fathers were almost equally distributed into medium-high education levels, specifically between education high school 43.4 and 45.4% graduate or postgraduate. Additionally, most of the respondents declared that more than half of mothers (57.7%) were graduates, and less than half of respondents (36.7%) declared to have mothers with a high school degree. Finally, most of the respondents (73.6%) declared that only one parent was employed. As far as food habits, most of the respondents (69.6%) declared the consumption of cured meat at least once a week; instead, only 10.2% of respondents claimed they never consumed this foodstuff. Moreover, respondents showed an almost equal distribution of consumption of carbonated and soft drinks between never (44.9%) and less than once a week (44.9%). Furthermore, 41.5% of respondents declared to eat street food less than once a week. In addition, about half of the children (51.0%) did not have lunch at the school canteen. Less than half of respondents (41.3%) declared consuming meals at restaurants or pizzerias less than once a week. Finally, 87.8% of children did not show food intolerance or allergies, but 63.7% declared food rejection. The results about the lifestyle indicators showed that 75.0% of children did both outdoor group activities and sports regularly. Moreover, about half of respondents (53.4%) declared that their children watch TV between 1.5 and 3 h daily, while 41.5% up to 1 h daily. Finally, most of the respondents (91.2%) declared their knowledge of the health benefits of the MD. Moreover, the mothers’ age was on average of 39.8 ± 8.6 years and the fathers’ age was on average of 43.6 ± 9.3 years. As far as anthropometric assessments, the height (cm) of children was on average 129.0 ± 20.0; furthermore, the weight (kg) of children was on average approximately 31.4 ± 12.3 and body mass index BMI was on average 20.4 ± 3.8.
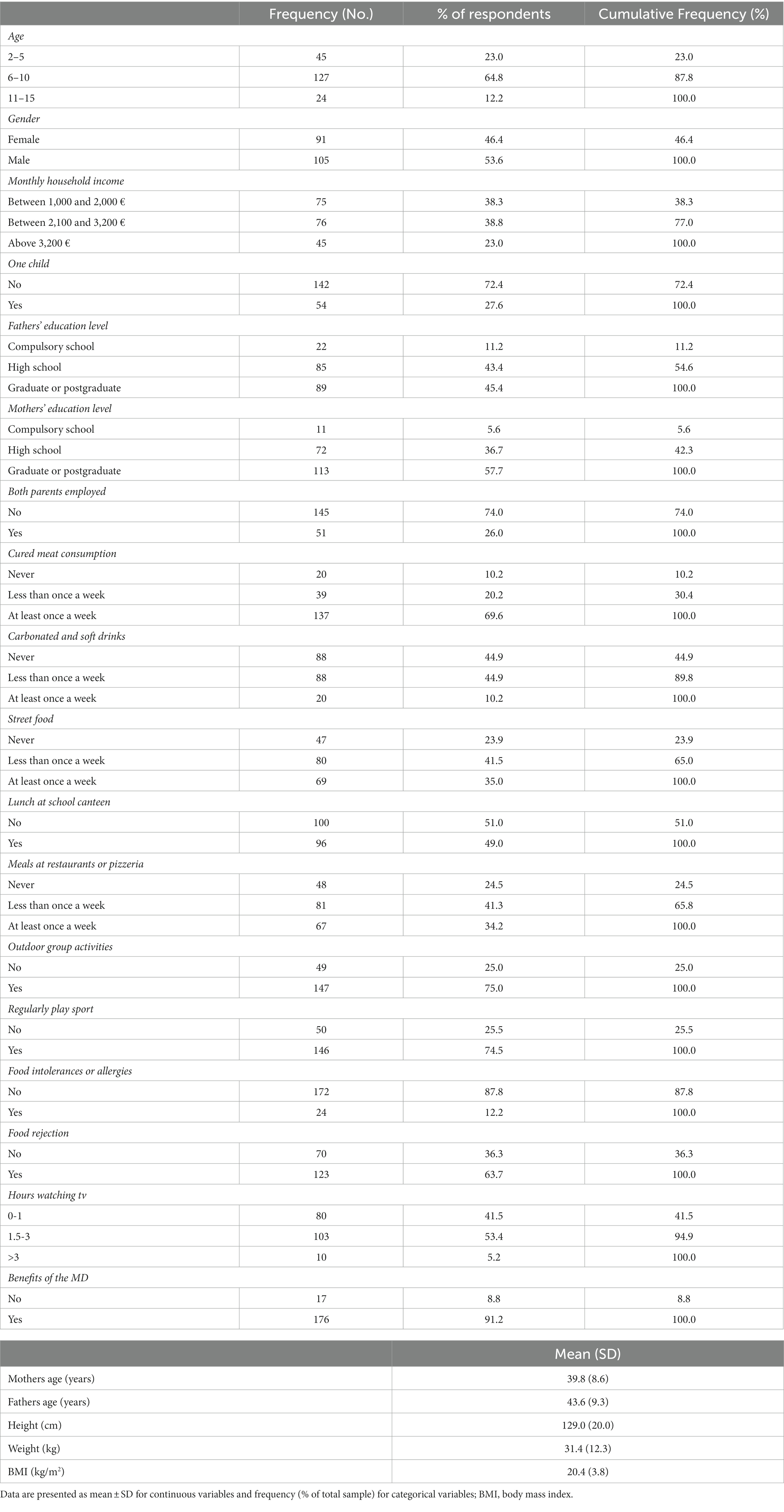
Table 2. Descriptive statistics of the participants according to sociodemographic characteristics, further food habits and lifestyle variables, and body mass index (BMI).
MD adherence was calculated through the KIDMED questionnaire (Table 1). Table 3 shows the responses to the questions considered by KIDMED and the subsequent classification into three classes of MD adherence. More than half of respondents (57.5%) showed a medium adherence. Regarding food habits concerning plant-based food and vegetables, a good share of respondents (83.4%) declared that their children are used to consuming one fruit or fruit juice every day, but more than half of children (51.0%) declared not to eat a second serving of fruit; moreover, most children (89.8) declared not to consume fresh or cooked vegetables more than once a day; a substantial share of participants (91.3) declared that their children not attended fast food less than weekly. Furthermore, most respondents (81.6%) declared that their children eat pulses more than once a week, and 92.9% said they eat pasta or rice five or more times per week. A substantial share of respondents (86.7%) declared that their children do not skip breakfast; additionally, commercially baked goods or pastries for breakfast are preferred by 76.5%. Most respondents (72.0%) declared that children are not accustomed to consuming nuts regularly; the most frequent habit was the use of olive oil for seasoning meals at home by 96% of respondents, and the frequent consumption of sweets and candy is declared by 60.6% of parents.

Table 3. Responses to the KIDMED questionnaire (Mediterranean Diet Quality Index in Children and Adolescents) for the total sample.
Figure 1 displays the distribution by age of participants into three categories of degree of adherence to the MD, according to the score obtained on the KIDMED index. A significant share of toddlers (from 2 to 5 years old), 75%, showed a medium adherence to the MD, compared to kids (53%) and children (46%). Furthermore, children (from 6 to 10 years old) showed poor adherence to the MD, a higher proportion of the sample (37%), than kids (23%) and toddlers (4%). Additionally, kids (from 11 to 15 years old) showed a high adherence to the MD, a higher share of proportion (24%), than children (17%) and toddlers (21%). Finally, more than half of the participants (57%) showed a high adherence to the MD, and the rest of the sample was distributed almost equally between poor adherence (20%) and high adherence (22%).
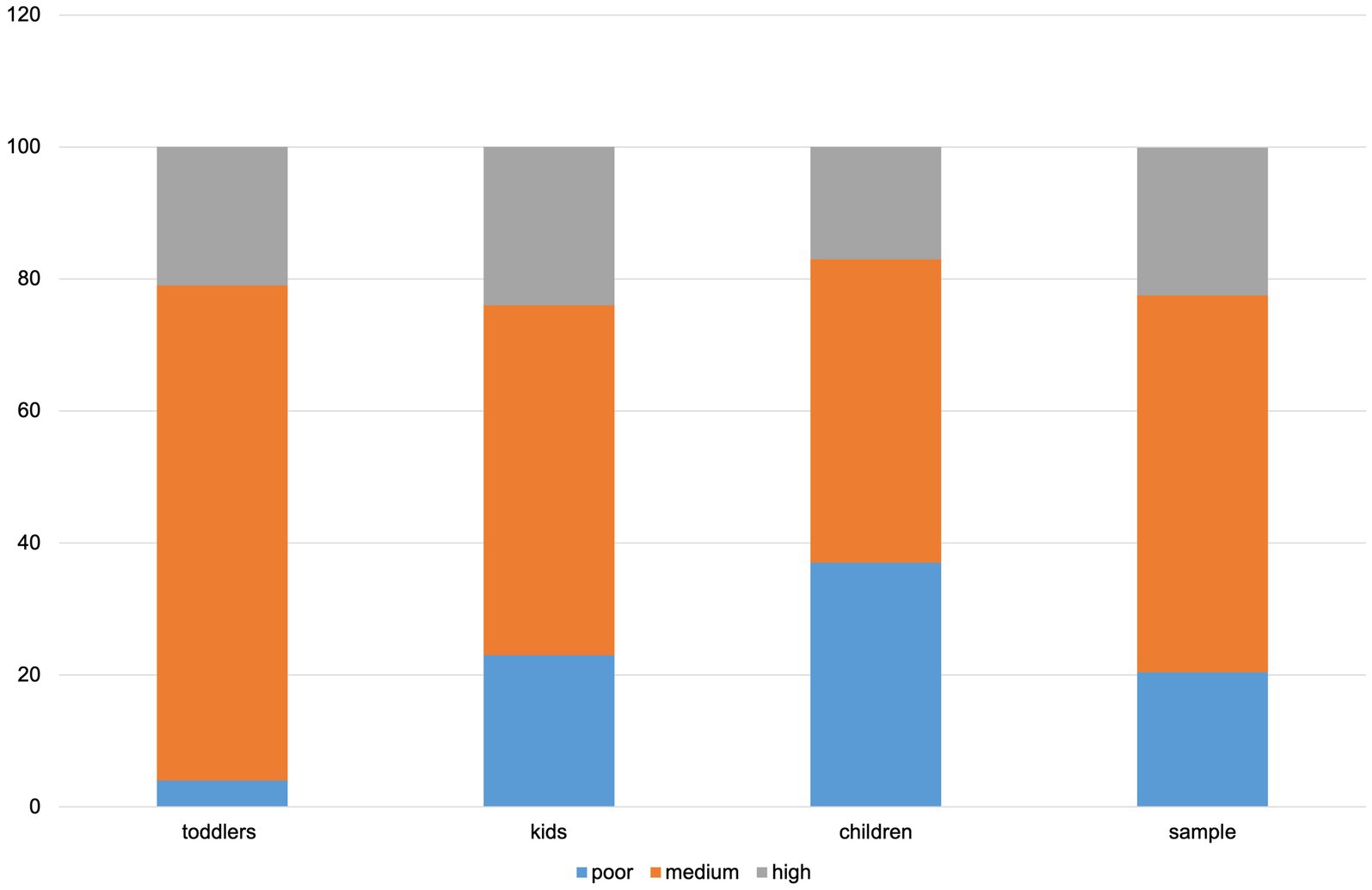
Figure 1. Adherence to MD by age class (children from 2 to 15 years old). toddlers, from 2 to 5 years old; kids, from 6 to 10 years old; children, from 11 to 15 years old.
3.2 Cluster analysis
According to the KIDMED score index, Lifestyle index, Socioeconomic index, BMI (kg/m2), and age, a four-cluster solution emerged as the optimum for k-means clustering. Table 4 displays the variables taken into account in the analysis and their distance from the final cluster centers; indeed, the final centroid values enabled us to determine the “labeling” of the clusters and thus the assignment of the children to a specific cluster. The following four clusters were identified: (2) the “normal weight and healthy”; (1) the “obese and unhealthy”; (3) “the overweight and lazy”; and (4) “the underweight and picky.” Cluster 1 was represented by MCB children with high adherence to MD (score ≥ 8 = high MD adherence); indeed, they showed the highest average score (8.0). In accordance, they showed a lifestyle index ranging from appropriate to optimum, with the highest score (3.2) compared to the other clusters. Indeed, MCB children of this cluster proved a medium-to-high socioeconomic status (2.4) and BMI (kg/m2), with an average score of 16.5. Finally, children had an average age of 7 years. Cluster 2, instead, was represented by MCB children with low adherence to MD; however, it presented an optimal lifestyle, with a medium-to-high score (3.0) and medium-to-high socioeconomic status (2.3). In line with their score of poor adherence, they showed a high BMI (kg/m2) (31.4). Finally, cluster 2 children presented an average age of 9 years.

Table 4. Variable and their distance from the final cluster centers.
Cluster 3 was represented by MCB children with a medium adherence to MD (4), optimal lifestyle (2.3), and medium-to-high socioeconomic status (2.3) as for cluster 2 children. However, they showed a BMI (kg/m2) average score of 19.2 and an average age of 10.1 years. Finally, cluster 4 was represented by MCB children with a medium adherence to MD (5.0), an appropriate lifestyle index (2.7). Moreover, they showed a medium-to-high socioeconomic status (2.4) for Cluster 1, but BMI (kg/m2) was definitely low, particularly an average score of 14.9; finally, cluster 4 children presented an average age of 6.4 years.
Four clusters of MCB children were profiled according to food habits and lifestyle index, socioeconomic index, children’s age, and BMI. Figures 2–5 display the profiles of children according to each cluster concerning the indices listed above and show the average of the scores for each index, categorized by classes. Table 5 shows the profile of consumption of each cluster, considering every compound of the KIDMED. Moreover, Table 6 displays the differences in terms of sociodemographic characteristics and physical and lifestyle measures between the four cluster solutions.
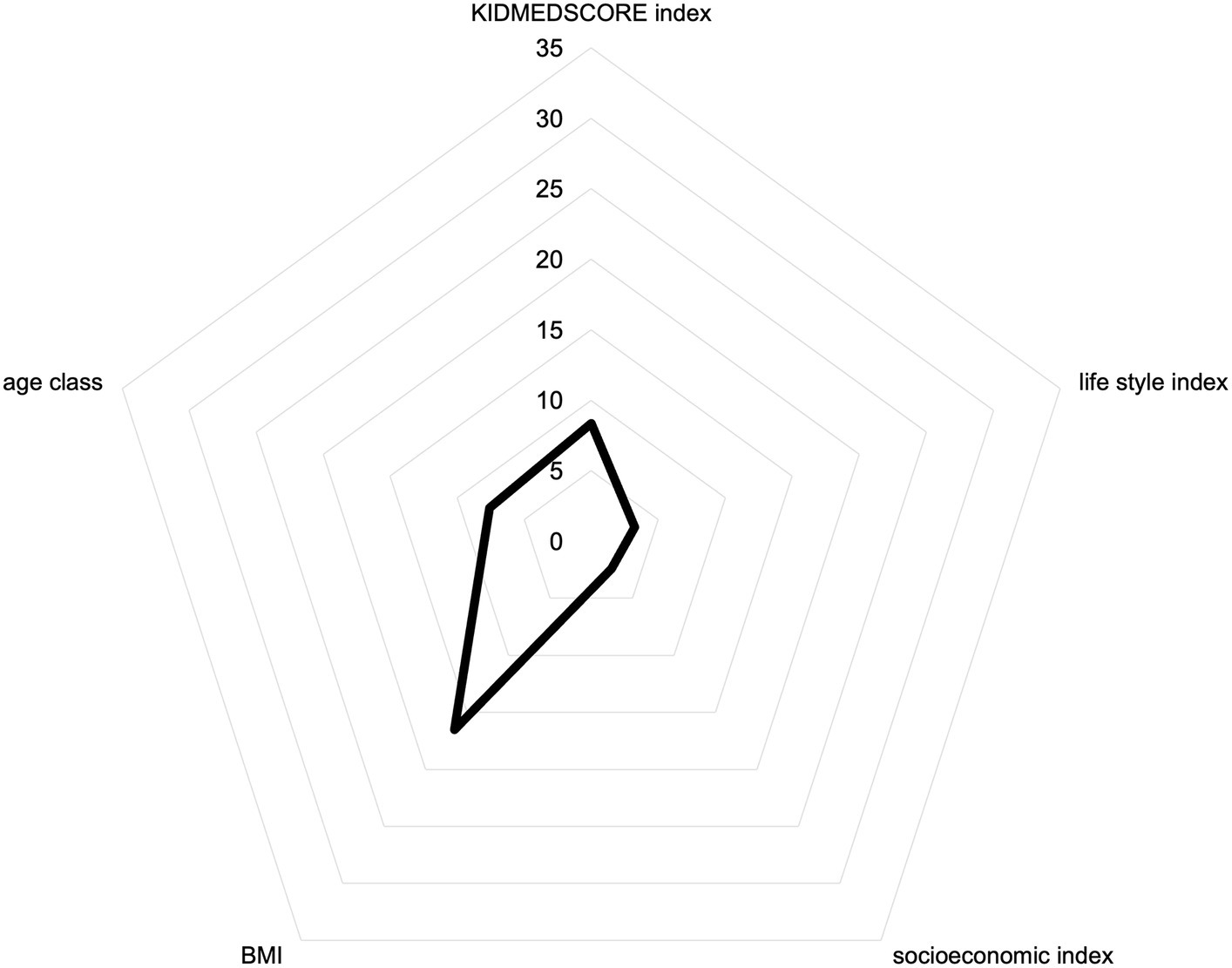
Figure 2. Radar chart showing the scores of “the Normal weight and healthy.”
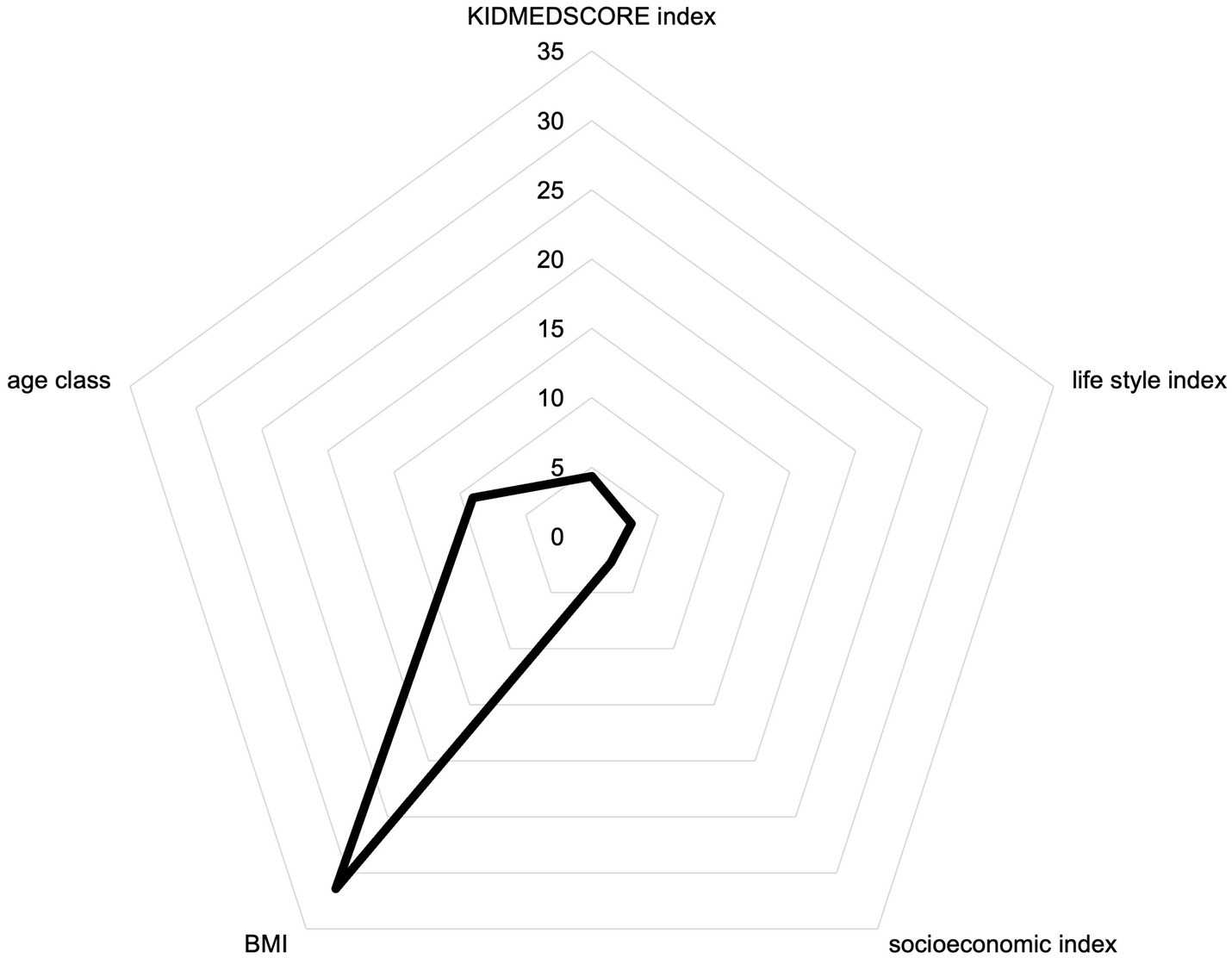
Figure 3. Radar chart showing the scores of “the Obese and unhealthy.”
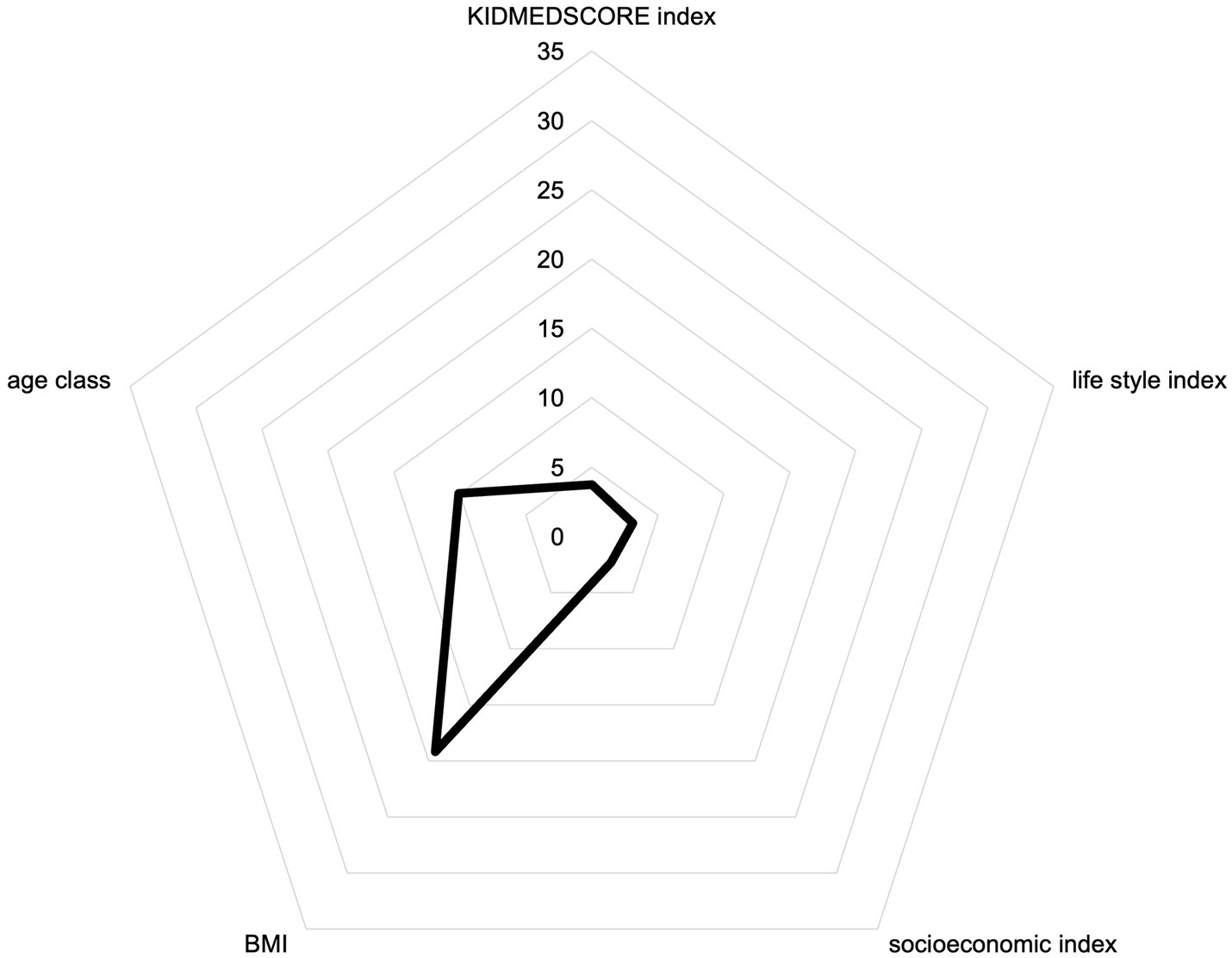
Figure 4. Radar chart showing the scores of “the Overweight and lazy.”
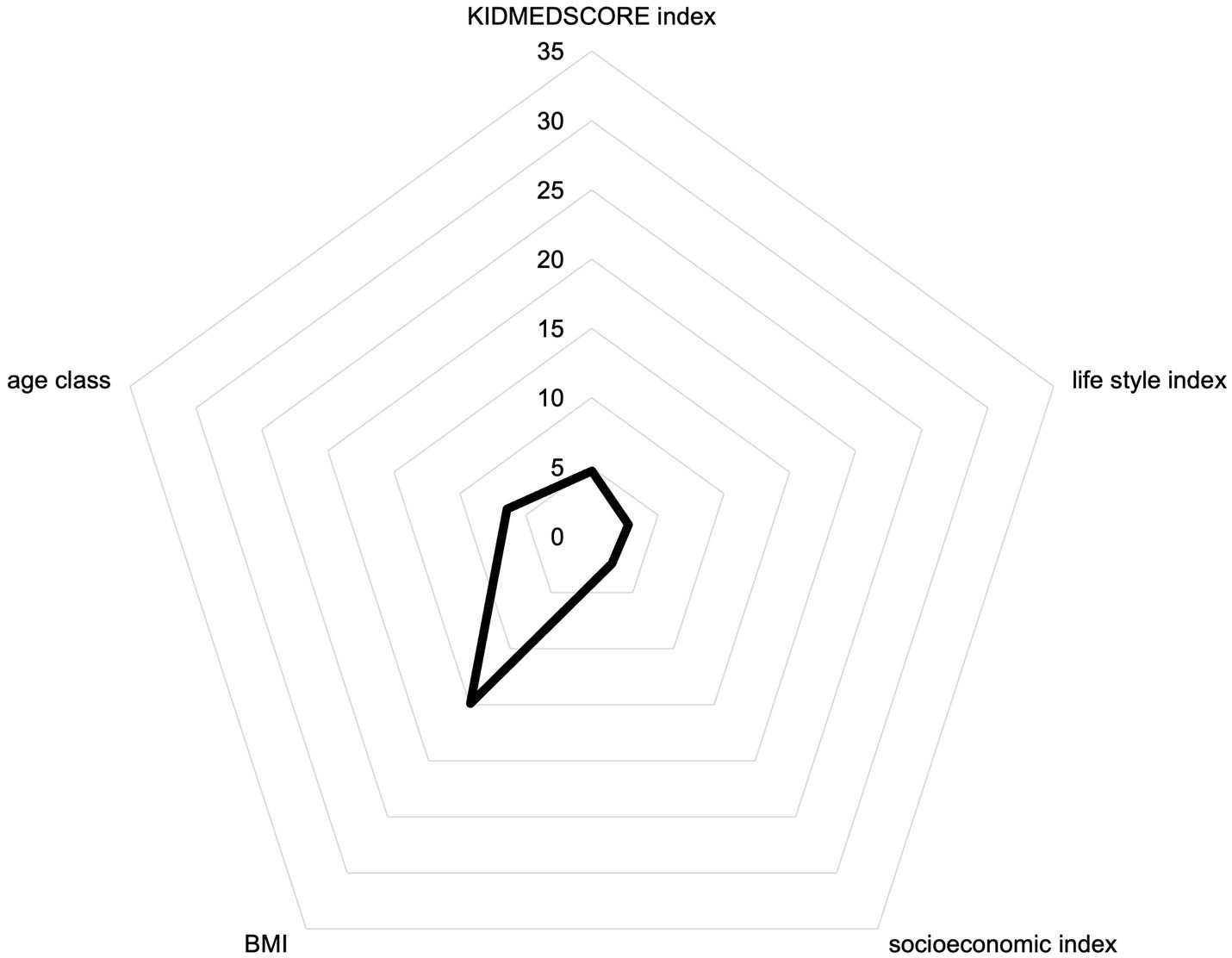
Figure 5. Radar chart showing the scores of “the Underweight and picky.”

Table 5. Percentage of individuals who answered affirmatively to the different items of the Mediterranean Diet Quality Index in children and adolescents (KIDMED) by cluster.
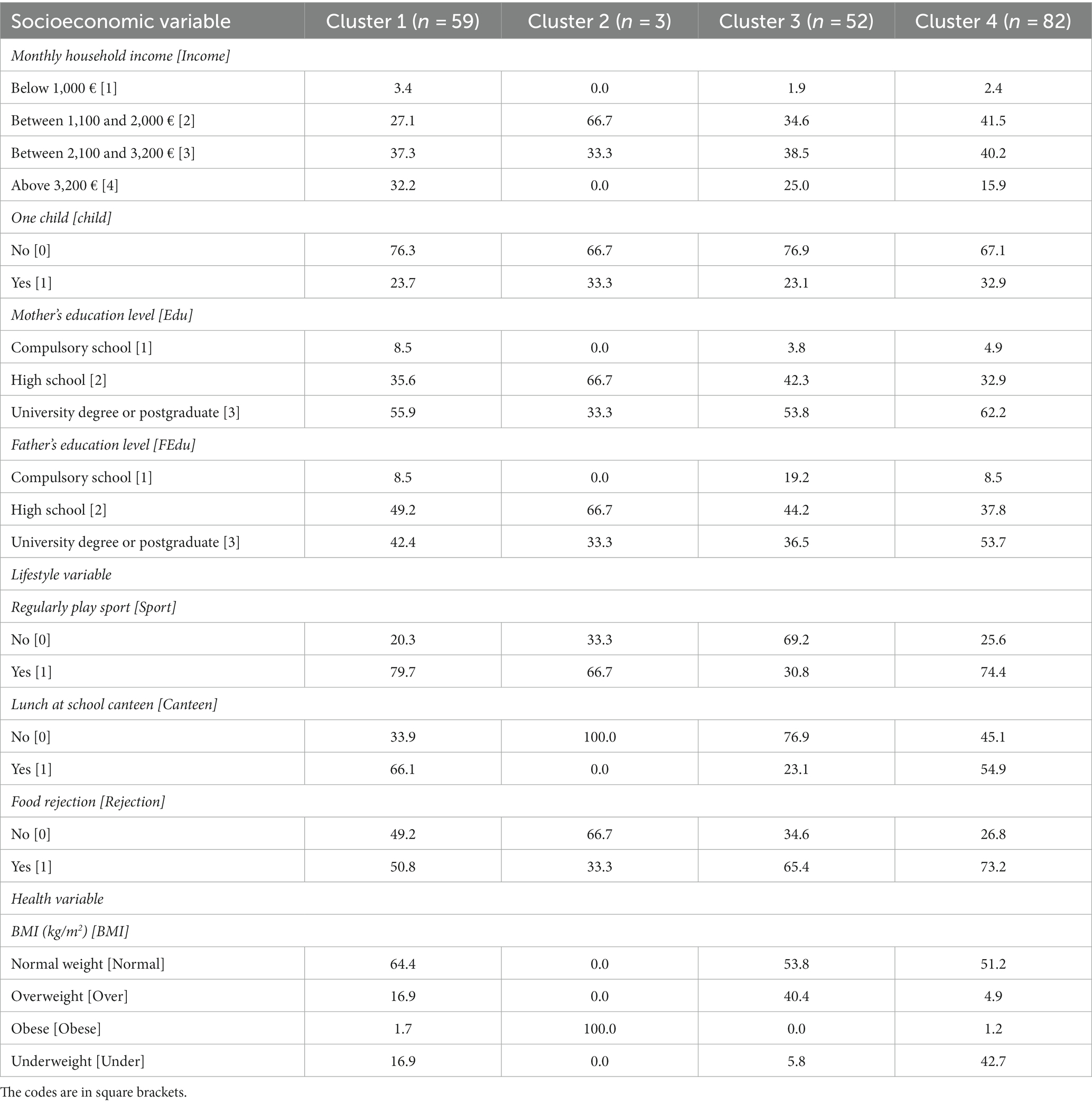
Table 6. Percentage of individuals who answered the different variables concerning socioeconomic index and lifestyle index.
3.2.1 The normal weight and healthy
The first group of children, identified as Cluster 1 and labeled as “the normal weight and healthy,” is composed of 59 children. It includes mainly children with an average age of approximately 7 years. According to established cutoffs of the KIDMED, Cluster 1 would have a high adherence to the MD; indeed, it showed the highest KIDMED score (Amin et al., 2021). The definition of “healthy” is mainly due to the tendency to observe the MD and optimal lifestyle. These aspects are reflected in the BMI (kg/m2) value; indeed, 64.4% of children are normal weight and only approximately 17% of them are overweight. Cluster 1 showed the highest proportion of individuals who consumed plant-based food, especially fruits daily (97 %) and vegetables daily (75 %). Furthermore, the highest proportion of children (93%) consumed pulses regularly, and seafood dishes (80%) and pasta or rice almost daily (95%). Finally, Cluster 1 showed the lowest proportion of children (3%) who skipped breakfast; indeed, more than half of children (57%) stated eating dairy products for breakfast. Furthermore, most of the children (69.5%) showed a high monthly household income (above 3,200 €/monthly), and less than half of individuals (23.7%) declared that the household included only one child. Moreover, children of cluster 1 have both highly educated parents; indeed, most of half of the children (55%) have a mother and father (42 %) with a high education level (graduate or postgraduate). Children of Cluster 1 declared that they regularly play sports (80%); finally, more than half of the children (66%) declared to consume meals at the school canteen, and about half of the children of Cluster 1 (50%) not declared to show food rejection.
3.2.2 The obese and unhealthy
The second group of children, identified as Cluster 2 and labeled as “the obese and unhealthy,” is composed of three children. It includes mainly children with an average age of approximately 9 years. According to established cutoffs of the KIDMED, Cluster 2 showed poor adherence to the MD; indeed, the resulting KIDMED score is the lowest (Livingstone et al., 2022). The socioeconomic index demonstrated a favorable situation regarding household composition and income and parents’ education, but the lifestyle index resulted in excellent only for one child and low or adequate for the others. The label “unhealthy” is mainly due to the unwillingness to adhere to the MD. Cluster 2 showed the lowest proportion of individuals who consumed plant-based food, notably fruits daily (33%) and vegetables daily (33%). Moreover, all children in Cluster 2 declared consuming seafood dishes at least 2–3/week (100%) and pulses >1/week (100%); over half of the children (67%) consumed pasta or rice almost regularly while displaying a low adherence to the MD. Moreover, Cluster 2 showed the highest proportion of children (67%) who attended fast-food restaurants more than once a week and skipped breakfast (67%). Finally, the “the obese and unhealthy” included the highest proportion of children (67%) who consume sweets and candy several times a day. Moreover, children of cluster 2 (66.7%) showed a medium monthly household income (between 2,100 and 3,200 € monthly), and more than half of individuals (66.7%) declared that the household included more than one child. Moreover, children of cluster 2 have both medium-educated parents; indeed, almost half of the children (66.7%) have a mother and father with medium education level (high school). Furthermore, more than half of the children (66.7%) declared that they regularly play sports, contrary to their unhealthy food habits. Finally, all children of Cluster 2 declared that they do not attend school canteen, and food rejection occurs in one-third of the children (33%).
3.2.3 The overweight and lazy
The third group of children, identified as Cluster 3 and labeled “the overweight and lazy,” is composed of 52 children. It includes children with an average age of approximately 10 years. According to established cutoffs of the KIDMED, Cluster 3 showed poor adherence to the MD; indeed, the resulting KIDMED score is the lowest (Livingstone et al., 2022) as Cluster 2. Moreover, children of Cluster 3 resulted in normal weight for 53.8%, overweight for 40.4%, and underweight for 5.8%. The socioeconomic index demonstrated a favorable situation as Cluster 2; indeed, Figure 3 displays a socioeconomic index score of 3 (between medium and high levels) and the lowest lifestyle index score (2.4). The label “the lazy” is mainly due to their lack of constancy to playing sports, compared to children from the other clusters; this group showed a higher proportion of individuals who consumed plant-based food, notably fruits daily (69%), and the lowest proportion of children who consumed second serving fruit daily (29%) and vegetables >1/day (6%). Moreover, Cluster 3 showed the lowest proportion of children who consumed seafood dishes at least 2–3/week (25%) and pulses >1/week (75%); Cluster 3 showed the highest proportion of children who consumed pasta or rice almost regularly (90%). Moreover, Cluster 3 showed the highest proportion of children (60%) as Cluster 2, who attended fast-food restaurants more than once a week; furthermore, it showed the lowest proportion of children as Cluster 2, who skipped breakfast (21%). Finally, the “lazy” included the highest proportion of children (85%) who consume commercially baked goods or pastries for breakfast. Moreover, less than half of children (38.5%) showed a medium monthly household income (between 2,100 and 3,200 € monthly), and more than half of individuals (76.9%) declared that the household includes more than one child. Moreover, children of cluster 3 have both medium-to-high educated parents; indeed, more than half of the children (53.8%) have a mother with a high education level (graduate or postgraduate) and a father with a medium education level (high school) for 44.2% of children. Furthermore, less than half of children (30.8%) declared that they regularly play sports. Finally, less than half of the children (23.1%) of Cluster 3 declared that they would attend school canteen, and food rejection occurs in more than half of the children (65.4%).
3.2.4 The underweight and picky
The fourth group of children, identified as Cluster 4 and labeled as “the underweight and picky,” is composed of 82 children. It includes mainly children with an average age of approximately 6 years. According to established cutoffs of the KIDMED, Cluster 4 would have a medium adherence to the MD; indeed, it showed a KIDMED score of 5.
The definition of “picky” is mainly due to the tendency of children of Cluster 4 to food rejection. This aspect is reflected in BMI (kg/m2) value; indeed, more than half of the children (51.2%) were in normal weight; but a significant proportion of children (42.7%) were underweight; only approximately 4.9% of them were overweight and obese (1.2%). Cluster 4 showed the highest proportion of individuals who consumed plant-based food, especially fruits daily (97%) and vegetables daily (44%) as Cluster 1. Furthermore, more than half of children (77%) consumed pulses regularly, but less than half of children (38%) consumed seafood dishes, and almost all children (95%) consumed pasta or rice almost daily; moreover, more than half of children (57%) attended fast-food restaurants more than once a week. Cluster 4 showed the highest proportion of children (87%) who skipped breakfast, and more than half of the children (80%) stated eating commercially baked goods or pastries for breakfast. Finally, half of the children (50%) in Cluster 4 declared consuming sweets and candy several times a day. Moreover, less than half of children (41.5%) showed a low monthly household income (between 1,100 and 2,000 €) and medium monthly household income (between 2,100 and 3,200 € monthly) for 40.2% of children; more than half of individuals (67.1%) declared that the household includes more than one child. Moreover, children of cluster 4 have both highly educated parents; indeed, more than half of the children (53.7%) have a father with a high education level (graduate or postgraduate) and 62.2% of children have a mother with a high education level. Furthermore, almost all children (74.4%) declared that they regularly play sports. Finally, more than half of the children (54.9%) in Cluster 4 declared to attend school canteen, and food rejection occurs in almost all children (74.4%).
4 Discussion
In the present study, we investigated the association between overall adherence to MD and its components with a health indicator as BMI (kg/m2), as well as socioeconomic and lifestyle indexes. To the best of our knowledge, this is the first study to analyze the association of adherence to the MD and these components in MCB children using K-means cluster analysis. The indexes were developed as a tool based on several lifestyle and socioeconomic factors that could effectively assess the associations with adherence to MD; however, our results highlighted that higher adherence was not associated with the socioeconomic and lifestyle indexes with the single variables considered. The findings for the MCB children confirm the need to increase adherence to the MD pattern in this study population: 57.6 and 20.4% of children showed poor and medium adherence, respectively. This result is in line with some research in Italy (Rosi et al., 2020) that obtained medium levels of adherence in the children population. In detail, the overall results confirm that poor MD adherence is greater in older children; indeed, they are less inclined than younger to follow the dietary pattern correctly, in accordance with several studies conducted among the Italian population (Germani et al., 2014; Benedetti et al., 2016; Roma et al., 2020; Biasini et al., 2021; Antonelli and Donelli, 2022; Scarpato et al., 2022). Such results are aligned with other studies focused on adolescents (Leone et al., 2017; Dinu et al., 2021) and even younger individuals (Binkin et al., 2010; Roccaldo et al., 2014). In particular, a tendency to reduce fruit consumption in favor of more processed and less healthy foods is observed with increasing age due to the increase in the phenomenon of Western dietary patterns (Vitale and Getzin, 2019; Chung et al., 2021). Furthermore, the results showed that children of families with high levels of monthly income showed a high MD adherence in line with the previous research (Cavaliere et al., 2019), which found that this level of income is correlated to high adherence to the MD. In the same way, a recent study (Rubini et al., 2022) highlighted that low income was combined with poor MD adherence. Moreover, children with high adherence play sports regularly; indeed, these findings are in line with the previous research (Aine et al., 2022) since they highlighted the association between a good dietary pattern and proper time spent doing physical exercise. Furthermore, the results showed a high percentage of children who skipped breakfast; on the other hand, several studies performed on the Italian and foreign population highlighted various percentages, in particular around 14 and 20% (Deshmukh-Taskar et al., 2010; Lazzeri et al., 2014; Ferranti et al., 2016; Rosi et al., 2020). In line with our results, previous studies found an inverse association between adherence to the MD and the prevalence of overweight and obesity in children from the Mediterranean countries of the European Union (Agnoli et al., 2018; Kanellopoulou et al., 2021), but one early study showed a different outcome (Bučan Nenadić et al., 2021). Furthermore, such findings are aligned with other investigations focused on Spanish adolescents that observed a BMI of children and adolescents equal to underweight (17%) and normal weight (69%); however, national data showed different results; indeed, 3 and 81% of adolescents are underweight and normal weight, respectively (Lazzeri et al., 2014). In line with our results, maternal maximum educational level was positively associated with an optimal adherence to MD in children and adolescents (Bibiloni et al., 2022). As reported above for the sample of children with poor MD adherence, the scientific literature suggests that a higher level of income fosters a better adherence to MD. In this regard, the reduction of socioeconomic inequalities and the development of focused policies favoring the affordability of healthy foods for every social class may foster the adoption of healthier food behavior and sustainable food transition (Kontogianni et al., 2008; Grao-Cruces et al., 2014). Previous studies showed a strong association between diet adequacy and socioeconomic features (Martínez et al., 2010). In agreement with this evidence, some scholars found that 15 out of 20 studies providing appropriate data observed a significant correlation between higher MD adherence and socioeconomic features (Iaccarino Idelson et al., 2017). Regarding physical activity, our results were in contrast with the literature that showed a positive association between physical activity and other healthy lifestyle habits, such as an adequate diet and good BMI (Patrick and Nicklas, 2005; Wittmeier et al., 2008; Llargues et al., 2011; Arcila-Agudelo and Torres-Fernàndez, 2019; Bibiloni et al., 2022), as well as adherence to the MD (Iaccarino Idelson et al., 2017). Moreover, the results showed an association between poor adherence and the number of meals eaten outside of the home (e.g., street food) and at pizzerias or restaurants, which are potential factors for an increase in body weight, in line with some scholars (Marventano et al., 2018). This finding was also in agreement with other studies that showed that children and adolescents who regularly ate meals at home had healthier eating (La Fauci et al., 2020). Moreover, in accordance with the results of some scholars (Grassi et al., 2020), Italian children consume, on average, few portions of pulses as well as high quantities of sweet drinks and red or processed meat. Finally, our results showed greater adherence to MD and attendance at the school canteen. In line with the results of some scholars (Rico-Sapena et al., 2019), the percentage of students with optimal diets was higher than those who did not consume healthy meals at the school canteen (Lawlis et al., 2017). Finally, the overall findings support the need to implement actions that contribute to increasing adherence to MD in children and adolescents who live in MCB.
5 Conclusion
The results and reflections of this study are intended to contribute to the academic debate on the phenomena of food security and nutrition in MCB. The present research investigated MD adherence in a convenience sample of children residing in the Metropolitan City of Bari (MCB), in association with food and lifestyle habits and anthropometric and sociodemographic variables, and shows the relationship between health indicators, such as BMI and adherence to MD. The cluster analysis showed the characterization of children, taking into account the indexes and variables considered into four clusters with different features. The overall results showed an association between low adherence to MD and high prevalence of overweight and obesity in children. The factors positively associated with following optimal MD adherence were the mother’s education level and level of income; furthermore, skipping breakfast is linked to low adherence to MD. Furthermore, the overall results showed a medium adherence to MD, which demonstrates that this dietary pattern is still recognized in Italian as a model of dietary sustainability. However, the results also display a transition of children to unhealthy and unsustainable diet patterns.
This study is a contribution to identifying effective measures for the institutionalization of Food Policy 2030 of the Metropolitan City of Bari (MCB). The results of this research support the need to design food education activities and implement interventions for promoting healthy habits and lifestyles through a multilevel approach involving the family and school. The proposed approach may also be used by municipal policymakers to identify target strategies to direct public funding in increasing MD adherence and improving food security and nutrition in urban areas.
However, this study is not free of some limitations. The main shortcoming is related to socioeconomic and lifestyle indexes. The construction of these indexes was not effective in profiling children through the k-means technique; indeed, the consideration of multiple variables in a single index has led to a balance between the values of the individual variables. However, the current indexes are limited by subjectivity in selecting components and scoring systems. Furthermore, another limitation of the present study is the relatively small sample size recruited in an urban restrictive area that is not deemed representative of Italian children. Additionally, it is worth considering the particularly low participation rate; under this circumstance, the sample size might have returned false negative results due to the lack of statistical power; indeed, the results cannot be generalized to the Italian population.
Further long-term research must first concern the extension of the analysis to a wider audience of consumers appropriately differentiated to grasp the different dynamics that characterize different geographical areas. Moreover, it would be worthy to further study the deepening of how and to what extent healthy eating habits acquired in childhood may result in more aware food consumption habits lasting in adulthood. The results of the analyzes will provide the basis for defining policy interventions for fostering children’s adherence to the Mediterranean diet model, as it is demonstrated to be healthy and sustainable.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Ethical approval was not required for the study involving human samples in accordance with the local legislation and institutional requirements because [reason ethics approval was not required]. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin. Written informed consent was obtained from the individual(s), and minor(s)’ legal guardian/next of kin, for the publication of any potentially identifiable images or data included in this article.
Author contributions
RF: Conceptualization, Data curation, Formal analysis, Investigation, Resources, Visualization, Methodology, Writing – original draft, Writing – review & editing. GP: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Visualization, Writing – original draft. AB: Conceptualization, Data curation, Methodology, Project administration, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing. CA: Conceptualization, Data curation, Methodology, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing. RR: Conceptualization, Data curation, Methodology, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was funded under the NextGenerationEU Programme “MUR-Fondo Promozione e Sviluppo—DM 737/2021,” Project “Sistemi agroalimentari, nutrigenomica e alimentazione: regole dell’agricoltura e dell’informazione ai consumatori (SANA),” Horizon Europe Seeds, Project Code: S45 (CUP H99J21017750005).
Acknowledgments
Project funded under the National Recovery and Resilience Plan (NRRP), Mission 4 Component 2 Investment 1.3—Call for proposals No. 341 of 15 March 2022 of the Italian Ministry of University and Research, funded by the European Union—NextGenerationEU; Award Number: Project code PE00000003, Concession Decree No. 1550 of 11 October 2022, adopted by the Italian Ministry of Universities and Research, CUP D93C22000890001, project title “ON Foods—Research and innovation network on food and nutrition Sustainability, Safety and Security—Working ON Foods.”
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Agnoli, C., Sieri, S., Ricceri, F., Giraudo, M. T., Masala, G., Assedi, M., et al. (2018). Adherence to a Mediterranean diet and long-term changes in weight and waist circumference in the EPIC-Italy cohort. Nutr. Diabetes 8:22. doi: 10.1038/s41387-018-0023-3
Agriculture and Economic Development Analysis Division (2006). The State of Food and Agriculture, 2006: Food aid for food security? Rome, Italy. Available at: https://www.fao.org/documents/card/en/c/80a57cb8-da7e-5cf4-a767-afb9b2a1fed5 (Accessed October 5, 2023).
Aine, A., Muhonen, J., and Toivonen, V. (2022). Children’s right to play sports in a safe and healthy environment. Int Sports Law J 22, 93–104. doi: 10.1007/s40318-022-00217-2
Allen, G. (1987). Poverty and hunger issues and options for food security in developing countries. Food Policy 12:397. doi: 10.1016/0306-9192(87)90014-5
Amin, M. D., Badruddoza, S., and McCluskey, J. J. (2021). Predicting access to healthful food retailers with machine learning. Food Policy 99:101985. doi: 10.1016/j.foodpol.2020.101985
Antonelli, M., and Donelli, D. Protective role of the Mediterranean diet against the development of age-related cognitive disorders: an umbrella review of Meta-analyzes. IECN 2022. MDPI (2022) Basel
Arangia, A., Marino, Y., Impellizzeri, D., D’Amico, R., Cuzzocrea, S., and Di Paola, R. (2023). Hydroxytyrosol and its potential uses on intestinal and gastrointestinal disease. IJMS 24:3111. doi: 10.3390/ijms24043111
Archero, F., Ricotti, R., Solito, A., Carrera, D., Civello, F., Di Bella, R., et al. (2018). Adherence to the Mediterranean diet among school children and adolescents living in northern Italy and unhealthy food behaviors associated to overweight. Nutrients 10:1322. doi: 10.3390/nu10091322
Arcila-Agudelo, F.-S., and Torres-Fernàndez, F.-C. (2019). Determinants of adherence to healthy eating patterns in a population of children and adolescents: evidence on the Mediterranean diet in the City of Mataró (Catalonia, Spain). Nutrients 11:854. doi: 10.3390/nu11040854
Au, L. E., Gurzo, K., Gosliner, W., Webb, K. L., Crawford, P. B., and Ritchie, L. D. (2018). Eating school meals daily is associated with healthier dietary intakes: the healthy communities study. J. Acad. Nutr. Diet. 118, 1474–1481.e1. doi: 10.1016/j.jand.2018.01.010
Aureli, V., and Rossi, L. (2022). Nutrition knowledge as a driver of adherence to the Mediterranean diet in Italy. Front. Nutr. 9:804865. doi: 10.3389/fnut.2022.804865
Azzam, A. (2021). Is the world converging to a ‘Western diet’? Public Health Nutr. 24, 309–317. doi: 10.1017/S136898002000350X
Bach-Faig, A., Berry, E. M., Lairon, D., Reguant, J., Trichopoulou, A., Dernini, S., et al. (2011). Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 14, 2274–2284. doi: 10.1017/S1368980011002515
Bar-Nahum, Z., Finkelshtain, I., Ihle, R., and Rubin, O. D. (2020). Effects of violent political conflict on the supply, demand and fragmentation of fresh food markets. Food Sec. 12, 503–515. doi: 10.1007/s12571-020-01025-y
Barros, V. C., and Delgado, A. M. (2022). Mediterranean diet, a sustainable cultural asset. Encyclopedia 2, 761–777. doi: 10.3390/encyclopedia2020053
Beets, M. W., Shah, R., Weaver, R. G., Huberty, J., Beighle, A., and Moore, J. B. (2015). Physical activity in after-school programs: comparison with physical activity policies. J. Phys. Act. Health 12, 1–7. doi: 10.1123/jpah.2013-0135
Ben Hassen, T., and El Bilali, H. (2022). Impacts of the Russia-Ukraine war on global food security: towards more sustainable and resilient food systems? Foods 11:2301. doi: 10.3390/foods11152301
Benedetti, I., Laureti, T., and Secondi, L. (2016). Exploring the Italians’ food habits and tendency towards the Mediterranean diet. Italian. Rev. Agric. Econ. 71, 218–228. doi: 10.13128/REA-18641
Bertoni, E., Fontana, M., Gabrielli, L., Signorelli, S., and Vespe, M. eds. Handbook of computational social science for policy. Cham: Springer International Publishing (2023).
Biasini, B., Rosi, A., Menozzi, D., and Scazzina, F. (2021). Adherence to the Mediterranean diet in association with self-perception of diet sustainability, anthropometric and sociodemographic factors: a cross-sectional study in Italian adults. Nutrients 13:3282. doi: 10.3390/nu13093282
Bibiloni, M. D. M., Gallardo-Alfaro, L., Gómez, S. F., Wärnberg, J., Osés-Recalde, M., González-Gross, M., et al. (2022). Determinants of adherence to the Mediterranean diet in Spanish children and adolescents: the PASOS study. Nutrients 14:738. doi: 10.3390/nu14040738
Bimbo, F., Viscecchia, R., De Devitiis, B., Seccia, A., Roma, R., and De Boni, A. (2022). How do Italian consumers value sustainable certifications on fish?—an explorative analysis. Sustainability 14:3654. doi: 10.3390/su14063654
Binkin, N., Fontana, G., Lamberti, A., Cattaneo, C., Baglio, G., Perra, A., et al. (2010). A national survey of the prevalence of childhood overweight and obesity in Italy. Obes. Rev. 11, 2–10. doi: 10.1111/j.1467-789X.2009.00650.x
Bučan Nenadić, D., Kolak, E., Selak, M., Smoljo, M., Radić, J., Vučković, M., et al. (2021). Anthropometric parameters and Mediterranean diet adherence in preschool children in Split-Dalmatia County, Croatia—are they related? Nutrients 13:4252. doi: 10.3390/nu13124252
Burchi, F., and De Muro, P. (2016). From food availability to nutritional capabilities: advancing food security analysis. Food Policy 60, 10–19. doi: 10.1016/j.foodpol.2015.03.008
Burd, N. A., McKenna, C. F., Salvador, A. F., Paulussen, K. J. M., and Moore, D. R. (2019). Dietary protein quantity, quality, and exercise are key to healthy living: a muscle-centric perspective across the lifespan. Front. Nutr. 6:83. doi: 10.3389/fnut.2019.00083
Callieris, R., Rocco, R., and Brahim, S. (2016). Different consumer behaviours for organic food in Tunisia. A cluster analysis application. New Medit 15, 53–62.
Caprara, G. (2023). “The Mediterranean diet” in Nutritional health. Nutrition and health. eds. N. J. Temple, T. Wilson, D. R. Jacobs, and G. A. Bray (Cham: Springer International Publishing), 201–213.
Cardamone, E., Di Benedetto, R., Lorenzoni, G., Gallipoli, S., Ghidina, M., Zobec, F., et al. (2023). Adherence to Mediterranean diet in Italy (ARIANNA) cross-sectional survey: study protocol. BMJ Open 13:e067534. doi: 10.1136/bmjopen-2022-067534
Cavaliere, A., De Marchi, E., and Banterle, A. (2018). Exploring the adherence to the Mediterranean diet and its relationship with individual lifestyle: the role of healthy behaviors, pro-environmental behaviors, income, and education. Nutrients 10:141. doi: 10.3390/nu10020141
Cavaliere, A., De Marchi, E., Donzelli, F., and Banterle, A. (2019). Is the Mediterranean diet for all? An analysis of socioeconomic inequalities and food consumption in Italy. BFJ 121, 1327–1341. doi: 10.1108/BFJ-06-2018-0373
Cena, H., and Calder, P. C. (2020). Defining a healthy diet: evidence for the role of contemporary dietary patterns in health and disease. Nutrients 12:334. doi: 10.3390/nu12020334
Chung, L. M. Y., Fong, S. S. M., and Law, Q. P. S. (2021). Younger adults are more likely to increase fruit and vegetable consumption and decrease sugar intake with the application of dietary monitoring. Nutrients 13:333. doi: 10.3390/nu13020333
Ciba (2023). The manifesto for sustainable food transition. Available at: https://www.ciba2030.it/ (Accessed April 24, 2023).
Clapp, J., Moseley, W. G., Burlingame, B., and Termine, P. (2022). Viewpoint: the case for a six-dimensional food security framework. Food Policy 106:102164. doi: 10.1016/j.foodpol.2021.102164
Cohen, J. F. W., Hecht, A. A., McLoughlin, G. M., Turner, L., and Schwartz, M. B. (2021). Universal school meals and associations with student participation, attendance, academic performance, diet quality, food security, and body mass index: a systematic review. Nutrients 13:911. doi: 10.3390/nu13030911
Das, D., Kayal, P., and Maiti, M. (2023). A K-means clustering model for analyzing the bitcoin extreme value returns. Decis. Anal. J. 6:100152. doi: 10.1016/j.dajour.2022.100152
Davis, C., Bryan, J., Hodgson, J., and Murphy, K. (2015). Definition of the Mediterranean diet; A Literature Review. Nutrients 7, 9139–9153. doi: 10.3390/nu7115459
De Onis, M. (2007). Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 85, 660–667. doi: 10.2471/BLT.07.043497
De Santi, M., Callari, F., Brandi, G., Toscano, R. V., Scarlata, L., Amagliani, G., et al. (2020). Mediterranean diet adherence and weight status among Sicilian middle school adolescents. Int. J. Food Sci. Nutr. 71, 1010–1018. doi: 10.1080/09637486.2020.1751089
Deshmukh-Taskar, P. R., Nicklas, T. A., O’Neil, C. E., Keast, D. R., Radcliffe, J. D., and Cho, S. (2010). The relationship of breakfast skipping and type of breakfast consumption with nutrient intake and weight status in children and adolescents: the National Health and nutrition examination survey 1999-2006. J. Am. Diet. Assoc. 110, 869–878. doi: 10.1016/j.jada.2010.03.023
Dinu, M., Lotti, S., Pagliai, G., Pisciotta, L., Zavatarelli, M., Borriello, M., et al. (2021). Mediterranean diet adherence in a sample of Italian adolescents attending secondary school—the “#facciamoComunicAzione” project. Nutrients 13:2806. doi: 10.3390/nu13082806
Donini, L. M., Dernini, S., Lairon, D., Serra-Majem, L., Amiot, M.-J., Del Balzo, V., et al. (2016). A consensus proposal for nutritional indicators to assess the sustainability of a healthy diet: the Mediterranean diet as a case study. Front. Nutr. 3:37. doi: 10.3389/fnut.2016.00037
Durao, S., Schoonees, A., Ramokolo, V., Oliveira, J. M. D., and Kristjansson, E. (2015). Community-level interventions for improving access to food in low- and middle-income countries. Cochrane Database Syst. Rev. 7:CD011504. doi: 10.1002/14651858.CD011504
El Hajj, J. S., and Julien, S. G. (2021). Factors associated with adherence to the Mediterranean diet and dietary habits among university students in Lebanon. J. Nutr. Metab. 2021, 1–7. doi: 10.1155/2021/6688462
FAO; CIHEAM. Food systems transformation – Processes and pathways in the Mediterranean. FAO; CIHEAM International Centre for Advanced Mediterranean Agronomic Studies; UfM Union for the Mediterranean ; (2021). FAO. Rome, Italy
Fardet, A., and Rock, E. (2014). Toward a new philosophy of preventive nutrition: from a reductionist to a holistic paradigm to improve nutritional recommendations. Adv. Nutr. 5, 430–446. doi: 10.3945/an.114.006122
Fernando, R. R., Ángela Romo, B., Daniela Escobar, B., and Aragú, B. (2013). Hábitos Alimentarios, Actividad Física Y Nivel Socioeconómico En. Nutricion Hospitalaria 28, 447–455. doi: 10.3305/nh.2013.28.2.6230
Ferranti, R., Marventano, S., Castellano, S., Giogianni, G., Nolfo, F., Rametta, S., et al. (2016). Sleep quality and duration is related with diet and obesity in young adolescent living in Sicily, Southern Italy. Sleep Science 9, 117–122. doi: 10.1016/j.slsci.2016.04.003
FoodSHIFT 2030 (2016). Transforming the European food system towards a low carbon, circular and plant-based future. FoodSHIFT 2030. Available at: https://foodshift2030.eu/ (Accessed June 5, 2023).
FoodSHIFT 2030 (2023) Project | FAO. Available at: http://www.fao.org/agroecology/database/detail/en/c/1469622/ (Accessed November 28, 2023)
Germani, A., Vitiello, V., Giusti, A. M., Pinto, A., Donini, L. M., and Del Balzo, V. (2014). Environmental and economic sustainability of the Mediterranean diet. Int. J. Food Sci. Nutr. 65, 1008–1012. doi: 10.3109/09637486.2014.945152
Godrich, S., Lo, J., Davies, C., Darby, J., and Devine, A. (2017). Prevalence and socio-demographic predictors of food insecurity among regional and remote Western Australian children. Aust. N. Z. J. Public Health 41, 585–590. doi: 10.1111/1753-6405.12716
Grams, L., Nelius, A.-K., Pastor, G. G., Sillero-Quintana, M., Veiga, Ó. L., Homeyer, D., et al. (2022). Comparison of adherence to Mediterranean diet between Spanish and German school-children and influence of gender, overweight, and physical activity. Nutrients 14:4697. doi: 10.3390/nu14214697
Grao-Cruces, A., Fernández-Martínez, A., and Nuviala, A. (2014). Association of Fitness with Life Satisfaction, health risk behaviors, and adherence to the Mediterranean diet in Spanish adolescents. J. Strength Cond. Res. 28, 2164–2172. doi: 10.1519/JSC.0000000000000363
Grassi, T., Bagordo, F., Panico, A., De Giorgi, M., Idolo, A., Serio, F., et al. (2020). Adherence to Mediterranean diet of children living in small southern Italian villages. Int. J. Food Sci. Nutr. 71, 490–499. doi: 10.1080/09637486.2019.1679725
Grosso, G., Marventano, S., Yang, J., Micek, A., Pajak, A., Scalfi, L., et al. (2017). A comprehensive meta-analysis on evidence of Mediterranean diet and cardiovascular disease: are individual components equal? Crit. Rev. Food Sci. Nutr. 57, 3218–3232. doi: 10.1080/10408398.2015.1107021
Hemeryck, L. Y., Goethals, S., Van Meulebroek, L., Van Hecke, T., Vossen, E., Van Camp, J., et al. (2022). Are red and processed meats bad for our health? Front. Young Minds 10:720495. doi: 10.3389/frym.2022.720495
Herman, E., Zsido, K.-E., and Fenyves, V. (2022). Cluster analysis with K-mean versus K-Medoid in financial performance evaluation. Appl. Sci. 12:7985. doi: 10.3390/app12167985
Hoffmann, D., Marx, J., Burmeister, J., and Musher-Eizenman, D. (2018). Friday night is pizza night: a comparison of Children’s dietary intake and maternal perceptions and feeding goals on weekdays and weekends. IJERPH 15:720. doi: 10.3390/ijerph15040720
Hwalla, N., El Labban, S., and Bahn, R. A. (2016). Nutrition security is an integral component of food security. Front. Life Sci. 9, 167–172. doi: 10.1080/21553769.2016.1209133
Iaccarino Idelson, P., Scalfi, L., and Valerio, G. (2017). Adherence to the Mediterranean diet in children and adolescents: a systematic review. Nutr. Metab. Cardiovasc. Dis. 27, 283–299. doi: 10.1016/j.numecd.2017.01.002
Jain, A. K., and Dubes, R. C. Algorithms for clustering data. Prentice-Hall, Inc. (1988). Hoboken, NJ
Javadi, S., Hashemy, S. M., Mohammadi, K., Howard, K. W. F., and Neshat, A. (2017). Classification of aquifer vulnerability using K-means cluster analysis. J. Hydrol. 549, 27–37. doi: 10.1016/j.jhydrol.2017.03.060
Jia, P., Luo, M., Li, Y., Zheng, J., Xiao, Q., and Luo, J. (2021). Fast-food restaurant, unhealthy eating, and childhood obesity: a systematic review and meta-analysis. Obes. Rev. 22:e12944. doi: 10.1111/obr.12944
Kanellopoulou, A., Giannakopoulou, S.-P., Notara, V., Antonogeorgos, G., Rojas-Gil, A. P., Kornilaki, E. N., et al. (2021). The association between adherence to the Mediterranean diet and childhood obesity; the role of family structure: results from an epidemiological study in 1728 Greek students. Nutr. Health 27, 39–47. doi: 10.1177/0260106020952600
Katsagoni, C. N., Psarra, G., Georgoulis, M., Tambalis, K., Panagiotakos, D. B., and Sidossis, L. S. (2020). High and moderate adherence to Mediterranean lifestyle is inversely associated with overweight, general and abdominal obesity in children and adolescents: the MediLIFE-index. Nutr. Res. 73, 38–47. doi: 10.1016/j.nutres.2019.09.009
Keys, A., Mienotti, A., Karvonen, M. J., Aravanis, C., Blackburn, H., Buzina, R., et al. (1986). The diet and 15-year death rate in the seven countries study. Am. J. Epidemiol. 124, 903–915. doi: 10.1093/oxfordjournals.aje.a114480
Kontogianni, M. D., Farmaki, A.-E., Vidra, N., Sofrona, S., Magkanari, F., and Yannakoulia, M. (2010). Associations between lifestyle patterns and body mass index in a sample of Greek children and adolescents. J. Am. Diet. Assoc. 110, 215–221. doi: 10.1016/j.jada.2009.10.035
Kontogianni, M. D., Vidra, N., Farmaki, A.-E., Koinaki, S., Belogianni, K., Sofrona, S., et al. (2008). Adherence rates to the Mediterranean diet are low in a representative sample of Greek children and adolescents. J. Nutr. 138, 1951–1956. doi: 10.1093/jn/138.10.1951
La Fauci, V., Alessi, V., and Assefa, D. (2020). Mediterranean diet: knowledge and adherence in Italian young people. Clin. Ter., 171, 437–443. doi: 10.7417/CT.2020.2254
Lacirignola, C., Capone, R., Bottalico, F., El Bilali, H., and Debs, P. (2015). Sustainability of typical quality products for food and nutrition security in the Mediterranean: lessons from the case of Apulia region in Italy. Feeding Expo Milano with Mediterranean Perspectives, Paris: CIHEAM 32, 40–44.
Lawlis, T., Eckley, D., Jamieson, M., and Knox, M. (2017). Scoping study investigating stakeholder perceptions and use of school canteens in an Australian city. Nutr. Dietetics 74, 502–508. doi: 10.1111/1747-0080.12363
Lazzeri, G., Giacchi, M. V., Spinelli, A., Pammolli, A., Dalmasso, P., Nardone, P., et al. (2014). Overweight among students aged 11–15 years and its relationship with breakfast, area of residence and parents’ education: results from the Italian HBSC 2010 cross-sectional study. Nutr. J. 13:69. doi: 10.1186/1475-2891-13-69
Leidy, H. J., and Gwin, J. A. (2020). Growing up strong: the importance of physical, mental, and emotional strength during childhood and adolescence with focus on dietary factors. Appl. Physiol. Nutr. Metab. 45, 1071–1080. doi: 10.1139/apnm-2020-0058
Leone, A., Battezzati, A., De Amicis, R., De Carlo, G., and Bertoli, S. (2017). Trends of adherence to the Mediterranean dietary pattern in northern Italy from 2010 to 2016. Nutrients 9:734. doi: 10.3390/nu9070734
Lin, T. K., Kafri, R., Hammoudeh, W., Mitwalli, S., Jamaluddine, Z., Ghattas, H., et al. (2022). Pathways to food insecurity in the context of conflict: the case of the occupied Palestinian territory. Confl. Heal. 16:38. doi: 10.1186/s13031-022-00470-0
Livingstone, K. M., Ramos-Lopez, O., Pérusse, L., Kato, H., Ordovas, J. M., and Martínez, J. A. (2022). Precision nutrition: a review of current approaches and future endeavors. Trends Food Sci. Technol. 128, 253–264. doi: 10.1016/j.tifs.2022.08.017
Llargues, E., Franco, R., Recasens, A., Nadal, A., Vila, M., Perez, M. J., et al. (2011). Assessment of a school-based intervention in eating habits and physical activity in school children: the AVall study. J. Epidemiol. Community Health 65, 896–901. doi: 10.1136/jech.2009.102319
Lopez, N. V., Ayala, G. X., Corder, K., Eisenberg, C. M., Zive, M. M., Wood, C., et al. (2012). Parent support and parent-mediated behaviors are associated with Children’s sugary beverage consumption. J. Acad. Nutr. Diet. 112, 541–547. doi: 10.1016/j.jand.2011.11.013
López-Gajardo, M. A., Leo, F. M., Sánchez-Miguel, P. A., López-Gajardo, D., Soulas, C., and Tapia-Serrano, M. A. (2022). KIDMED 2.0, an update of the KIDMED questionnaire: evaluation of the psychometric properties in youth. Front. Nutr. 9:945721. doi: 10.3389/fnut.2022.945721
Maher, C., Virgara, R., Okely, T., Stanley, R., Watson, M., and Lewis, L. (2019). Physical activity and screen time in out of school hours care: an observational study. BMC Pediatr. 19:283. doi: 10.1186/s12887-019-1653-x
Martínez, E., Llull, R., Del Mar, B. M., Pons, A., and Tur, J. A. (2010). Adherence to the Mediterranean dietary pattern among Balearic Islands adolescents. Br. J. Nutr. 103, 1657–1664. doi: 10.1017/S0007114509993576
Martínez-González, M. Á., and Sánchez-Villegas, A. (2003). Review: the emerging role of Mediterranean diets in cardiovascular epidemiology: monounsaturated fats, olive oil, red wine or the whole pattern? Eur. J. Epidemiol. 19, 9–13. doi: 10.1023/B:EJEP.0000013351.60227.7b
Marventano, S., Godos, J., Platania, A., Galvano, F., Mistretta, A., and Grosso, G. (2018). Mediterranean diet adherence in the Mediterranean healthy eating, aging and lifestyle (MEAL) study cohort. Int. J. Food Sci. Nutr. 69, 100–107. doi: 10.1080/09637486.2017.1332170
Mattas, K., Raptou, E., Alayidi, A., Yener, G., and Baourakis, G. (2023). Assessing the interlinkage between biodiversity and diet through the Mediterranean diet case. Adv. Nutr. 14, 570–582. doi: 10.1016/j.advnut.2023.03.011
Mazzocchi, A., Leone, L., Agostoni, C., and Pali-Schöll, I. (2019). The secrets of the Mediterranean diet. Does [only] olive oil matter? Nutrients 11:2941. doi: 10.3390/nu11122941
Miolla, R., Ottomano Palmisano, G., Roma, R., Caponio, F., Difonzo, G., and De Boni, A. (2023). Functional foods acceptability: a consumers’ survey on bread enriched with oenological by-products. Foods 12:2014. doi: 10.3390/foods12102014
Mohammadi, S., Lotfi, K., Mirzaei, S., Asadi, A., Akhlaghi, M., and Saneei, P. (2022). Adherence to Mediterranean diet and its association with metabolic health status in overweight and obese adolescents. Int. J. Clin. Pract. 2022, 1–11. doi: 10.1155/2022/9925267
Monterrosa, E. C., Frongillo, E. A., Drewnowski, A., De Pee, S., and Vandevijvere, S. (2020). Sociocultural influences on food choices and implications for sustainable healthy diets. Food Nutr. Bull. 41, 59S–73S. doi: 10.1177/0379572120975874
Mounayar, R., Jreij, R., Hachem, J., Abboud, F., and Tueni, M. (2019). Breakfast intake and factors associated with adherence to the Mediterranean diet among Lebanese high school adolescents. J. Nutr. Metab. 2019, 1–10. doi: 10.1155/2019/2714286
Nasir, M. A., Nugroho, A. D., and Lakner, Z. (2022). Impact of the Russian–Ukrainian conflict on global food crops. Foods 11:2979. doi: 10.3390/foods11192979
NeffatRIi, L., Ridha, H., Kolsteren, P., and Hilderbrand, K. (2004). Street food among children: a study in North Tunisia. Sante 14, 43–48.
Papadaki, S., Carayanni, V., Notara, V., and Chaniotis, D. (2023). Adherence to the Mediterranean diet in Greek adolescents during COVID-19: exploring determining factors through cross-sectional study. NFS 53, 700–713. doi: 10.1108/NFS-12-2022-0419
Park, J., and Choi, M. (2022). A K-means clustering algorithm to determine representative operational profiles of a ship using AIS data. JMSE 10:1245. doi: 10.3390/jmse10091245
Patrick, H., and Nicklas, T. A. (2005). A review of family and social determinants of Children’s eating patterns and diet quality. J. Am. Coll. Nutr. 24, 83–92. doi: 10.1080/07315724.2005.10719448
Penne, T., and Goedemé, T. (2021). Can low-income households afford a healthy diet? Insufficient income as a driver of food insecurity in Europe. Food Policy 99:101978. doi: 10.1016/j.foodpol.2020.101978
Pietrobelli, A., and Agosti, M., the MeNu Group (2017). Nutrition in the first 1000 days: ten practices to minimize obesity emerging from published science. IJERPH 14:1491. doi: 10.3390/ijerph14121491
Rajasooriar, D., and Soma, T. (2022). Food access, mobility, and transportation: a survey and key informant interviews of users of non-profit food hubs in the City of Vancouver before and during the COVID-19 crisis. BMC Public Health 22:6. doi: 10.1186/s12889-021-12434-9
Rangelov, N., Marques-Vidal, P., and Suggs, L. S. (2018). Reporting children’s food consumption: a comparison of reliability between a 2-day food record and a 7-day food diary. Forum Nutr. 43:24. doi: 10.1186/s41110-018-0083-0
Rico-Sapena, N., Galiana-Sanchez, M. E., Bernabeu-Mestre, J., Trescastro-López, E. M., and Vasallo, J. M. (2019). Efectos de un programa alternativo de promoción de la alimentación saludable en comedor escolar. Ciênc saúde coletiva 24, 4071–4082. doi: 10.1590/1413-812320182411.02482018
Riolo, R., De Rosa, R., Simonetta, I., and Tuttolomondo, A. (2022). Olive oil in the Mediterranean diet and its biochemical and molecular effects on cardiovascular health through an analysis of genetics and epigenetics. IJMS 23:16002. doi: 10.3390/ijms232416002
Roccaldo, R., Censi, L., D’Addezio, L., Toti, E., Martone, D., D’Addesa, D., et al. (2014). Adherence to the Mediterranean diet in Italian school children (the ZOOM8 study). Int. J. Food Sci. Nutr. 65, 621–628. doi: 10.3109/09637486.2013.873887
Roma, R., Ottomano Palmisano, G., and De Boni, A. (2020). Insects as novel food: a consumer attitude analysis through the dominance-based rough set approach. Foods 9:387. doi: 10.3390/foods9040387
Rosi, A., Giopp, F., Milioli, G., Melegari, G., Goldoni, M., Parrino, L., et al. (2020). Weight status, adherence to the Mediterranean diet, physical activity level, and sleep behavior of Italian junior high school adolescents. Nutrients 12:478. doi: 10.3390/nu12020478
Rosi, A., Paolella, G., Biasini, B., Scazzina, F., Alicante, P., De Blasio, F., et al. (2019). Dietary habits of adolescents living in North America, Europe or Oceania: a review on fruit, vegetable and legume consumption, sodium intake, and adherence to the Mediterranean diet. Nutr. Metab. Cardiovasc. Dis. 29, 544–560. doi: 10.1016/j.numecd.2019.03.003
Rubini, A., Vilaplana-Prieto, C., Flor-Alemany, M., Yeguas-Rosa, L., Hernández-González, M., Félix-García, F. J., et al. (2022). Assessment of the cost of the Mediterranean diet in a low-income region: adherence and relationship with available incomes. BMC Public Health 22:58. doi: 10.1186/s12889-021-12433-w
Ruiz-Almeida, A., and Rivera-Ferre, M. G. (2019). Internationally-based indicators to measure Agri-food systems sustainability using food sovereignty as a conceptual framework. Food Sec. 11, 1321–1337. doi: 10.1007/s12571-019-00964-5
Scarpato, D., Rotondo, G., and Simeone, M. (2022). Healthy and sustainable food: a cross-cultural study among Spanish and Italian consumers. Foods 11:1941. doi: 10.3390/foods11131941
Schröder, H., Mendez, M. A., Gomez, S. F., Fíto, M., Ribas, L., Aranceta, J., et al. (2013). Energy density, diet quality, and central body fat in a nationwide survey of young Spaniards. Nutrition 29, 1350–1355. doi: 10.1016/j.nut.2013.05.019
Sedaghat, F., Naja, F., Darand, M., Beyzai, B., and Rashidkhani, B. (2019). Adherence to a Mediterranean dietary pattern and overweight and obesity among female adolescents in Iran. Int. J. Adolesc. Med. Health 31:9925267. doi: 10.1515/ijamh-2016-0160
Serra-Majem, L., Ribas, L., Ngo, J., Ortega, R. M., García, A., Pérez-Rodrigo, C., et al. (2004). Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean diet quality index in children and adolescents. Public Health Nutr. 7, 931–935. doi: 10.1079/PHN2004556
Serra-Majem, L., Román-Viñas, B., Sanchez-Villegas, A., Guasch-Ferré, M., Corella, D., and La Vecchia, C. (2019). Benefits of the Mediterranean diet: epidemiological and molecular aspects. Mol. Asp. Med. 67, 1–55. doi: 10.1016/j.mam.2019.06.001
Spinelli, A., Buoncristiano, M., Nardone, P., Starc, G., Hejgaard, T., Júlíusson, P. B., et al. (2021). Thinness, overweight, and obesity in 6- to 9-year-old children from 36 countries: the World Health Organization European childhood obesity surveillance initiative—COSI 2015–2017. Obes. Rev. 22:e13214. doi: 10.1111/obr.13214
Truzzi, M. L., Ballerini Puviani, M., Tripodi, A., Toni, S., Farinetti, A., Nasi, M., et al. (2020). Mediterranean diet as a model of sustainable, resilient and healthy diet. Prog. Nutr. 22, 388–394. doi: 10.23751/pn.v22i2.8632
Tsakiraki, M., Grammatikopoulou, M. G., Stylianou, C., and Tsigga, M. (2011). Nutrition transition and health status of Cretan women: evidence from two generations. Public Health Nutr. 14, 793–800. doi: 10.1017/S1368980010003010
Van Stralen, M. M., Yıldırım, M., Wulp, A., Te Velde, S. J., Verloigne, M., Doessegger, A., et al. (2014). Measured sedentary time and physical activity during the school day of European 10- to 12-year-old children: the ENERGY project. J. Sci. Med. Sport 17, 201–206. doi: 10.1016/j.jsams.2013.04.019
Vandeginste, B. G. M., Massart, D. L., Buydens, L. M. C., De Jong, S., Lewi, P. J., and Smeyers-Verbeke, J. “Cluster analysis,” Data Handling in Science and Technology, Elsevier (1998). p. 57–86: Amsterdam
Victoria-Montesinos, D., Tárraga-Marcos, A., Brazo-Sayavera, J., Jiménez-López, E., Gutiérrez-Espinoza, H., Panisello Royo, J. M., et al. (2023). Adherence to the Mediterranean diet and health-related quality of life during the COVID-19 lockdown: a cross-sectional study including preschoolers, children, and adolescents from Brazil and Spain. Nutrients 15:677. doi: 10.3390/nu15030677
Vitale, K., and Getzin, A. (2019). Nutrition and supplement update for the endurance athlete: review and recommendations. Nutrients 11:1289. doi: 10.3390/nu11061289
Weatherill, G., and Burton, P. W. (2009). Delineation of shallow seismic source zones using K -means cluster analysis, with application to the Aegean region. Geophys. J. Int. 176, 565–588. doi: 10.1111/j.1365-246X.2008.03997.x
Wittmeier, K. D. M., Mollard, R. C., and Kriellaars, D. J. (2008). Physical activity intensity and risk of overweight and adiposity in children. Obesity 16, 415–420. doi: 10.1038/oby.2007.73
Zielińska, M., Łuszczki, E., Michońska, I., and Dereń, K. (2022). The Mediterranean diet and the Western diet in adolescent depression-current reports. Nutrients 14:4390. doi: 10.3390/nu14204390
Keywords: food and nutrition security, Mediterranean diet, children, KIDMED, cluster analysis
Citation: Facendola R, Ottomano Palmisano G, De Boni A, Acciani C and Roma R (2024) Determinants of the adherence to Mediterranean diet: application of the k-means cluster analysis profiling children in the Metropolitan City of Bari. Front. Sustain. Food Syst. 7:1329090. doi: 10.3389/fsufs.2023.1329090
Edited by:
Giuseppe Antonio Di Vita, University of Messina, ItalyReviewed by:
Francesco Bimbo, University of Foggia, ItalyLucia Rocchi, University of Perugia, Italy
Copyright © 2024 Facendola, Ottomano Palmisano, De Boni, Acciani and Roma. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Giovanni Ottomano Palmisano, Z2lvdmFubmkub3R0b21hbm9wYWxtaXNhbm9AdW5pYmEuaXQ=