
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Sustain. Food Syst. , 30 November 2022
Sec. Agro-Food Safety
Volume 6 - 2022 | https://doi.org/10.3389/fsufs.2022.1058384
This article is part of the Research Topic Food Safety in Low and Middle Income Countries View all 25 articles
 Garima Sharma1,2*
Garima Sharma1,2* Eithne Leahy1
Eithne Leahy1 Ram Pratim Deka1
Ram Pratim Deka1 Bibek R. Shome3
Bibek R. Shome3 Samiran Bandyopadhyay4
Samiran Bandyopadhyay4 Tushar K. Dey1,2,3
Tushar K. Dey1,2,3 Naresh Kumar Goyal5
Naresh Kumar Goyal5 Åke Lundkvist2
Åke Lundkvist2 Delia Grace1,6
Delia Grace1,6 Johanna F. Lindahl1,2,7
Johanna F. Lindahl1,2,7Background: Milk vendors play an important role in India's dairy value chain; however, their food safety practices are poorly understood. From a milk safety perspective, vendor behavior is significant because it has the potential to affect both consumer and producer behavior. This study describes the types of milk vendors in two Indian states, in an attempt to investigate vendors' hygienic knowledge and practices toward safety and antimicrobial resistance (AMR).
Methods: A cross-sectional study was conducted in the states of Assam and Haryana, India. In selected villages, all the milk vendors identified at the time of visit were interviewed. A questionnaire was used to assess the knowledge and practices on antibiotics, milk safety and hygiene. The milk samples were tested for presence of antibiotic resistant bacteria using antibiotic susceptibility testing.
Results: In total, 244 milk vendors were interviewed during the survey. Out of these, 146 (59.8%) of the vendors traded raw milk, while 40.2% traded pasteurized milk. Vendors were categorized depending on whom they supplied milk to. Five categories were identified: (a) those who sold at grocery shops; (b) those who sold on roadside (roadside vendors); (c) those who sold from door to door; (d) those who sold to sweet makers/tea stalls, and (e) those who sold from own home/other entity. The level of training among vendors on milk hygiene was non-existent and the knowledge related to antibiotics was low. Most of them [210/244 (86.07%)] agreed that boiled milk is always safer than raw milk but almost half [119 (48.77%)] of them admitted that sometimes they drink milk without boiling it. Most vendors believed that they could identify whether milk is safe or not for consumption just by its appearance and smell. Out of 124 milk samples collected from surveyed milk vendors and tested for the presence of antibiotic-resistant bacteria, 80 (64.52%) were tested positive.
Conclusion: This study highlights the low levels of knowledge regarding food safety among milk vendors. It shows the predominance of informal milk vendors in the surveyed states and prevalence of AMR bacteria in milk traded by them. Training may be a beneficial strategy for addressing the issue.
India is the world's leading milk producer, currently producing more milk than the European Union or the United Sates (FAO., 2021), with ever-increasing domestic milk consumption (Douphrate et al., 2013; Milk Production in India., 2022). Unlike other countries, where large-scale commercial units dominate dairy production (Douphrate et al., 2013), India's milk production is driven by numerous small dairy holdings (Kumar et al., 2011; Sudhanthiramani et al., 2015). Up to 80% of Indian milk is produced by rural dairy farmers and handled through an unorganized sector with only 20% handled through a regulated, organized industry (Dhanashekar et al., 2012; Sharma et al., 2020).
Milk is responsible for the spread of several foodborne bacterial pathogens from animals to humans in India (Mutua et al., 2020). Antimicrobial-resistant (AMR) bacteria have earlier been found prevalent in milk across India (Kuralayanapalya et al., 2019), which is a significant public health concern given the morbidity and mortality related to AMR infections in humans (Mutua et al., 2020; Sharma et al., 2020). Across India, milk vendors allow consumers to access this highly perishable commodity, transporting it from source to distribution (Sudhanthiramani et al., 2015). A number of laws in India regulate the safety of milk and milk-based products (Mutua et al., 2020). However, it is unclear how successfully these laws are being implemented on the ground mainly in regard to informal dairy sector. Given that animal-sourced foods, including milk, are estimated to be responsible for 70% of India's 100 million yearly cases of foodborne illnesses (FBD) (Smeets Kristkova, 2017), and the way in which vendors handle food has been associated with milk contamination and cross-contamination of other foods (Alimi, 2016), the handling procedures among milk vendors warrant closer examination.
Milk vendors have been found to play a key role in the etiology of foodborne zoonoses (Grwambi, 2020). In India, the infrastructure facilities for milk collection, storage, transportation, and processing raw milk are inadequate (Rajendran and Mohanty, 2004). Given the highly perishable nature of raw milk, handling of raw milk for hours without cooling allows pathogens in milk to multiply, increasing the risk of FBD for the consumer (Roesel Kristina, 2014). In India, research at the dairy-farm level shows poor adoption of hygiene practices in milk handling, while adoption of milk safety practices at vendors' level is poorly understood. Given the lack of studies performed across India to assess the knowledge and attitude of milk vendors related to milk safety, antibiotics, or AMR, we selected this important informal dairy value chain actor for this cross-sectional study. The study explores the hygienic procedures followed by the milk vendors and their awareness level related to basics of safe milk handling, antibiotics, and AMR in two milk producing states of India- Haryana and Assam. The states were chosen based on their strong disparity in regard to dairy production system, processing infrastructure and presence of vegetarian population. Haryana, a state with good dairy production system coupled with better processing infrastructure and predominance of vegetarian population might perform differently in the given areas of this study objectives than in Assam where dairy production, processing and consumption are inferior to Haryana (Kumar et al., 2021).
A cross-sectional study was conducted in the states of Assam and Haryana, India, from October-November 2017, as a follow up on a previous study done in April 2016—March 2017 where farmers were interviewed (Kumar et al., 2021). The farmer survey was based on a multi-stage selection process. In brief, the district selection was guided by Animal Husbandry and Veterinary Department officials regarding the district's potential for dairy development (low, medium, and high). Accordingly, the three districts Kamrup (metropolitan), Golaghat, and Baksa were selected for Assam and Karnal, Kaithal and Bhiwani for Haryana. Figure 1 shows a map of the two states with the three respective districts per state where the study was conducted.
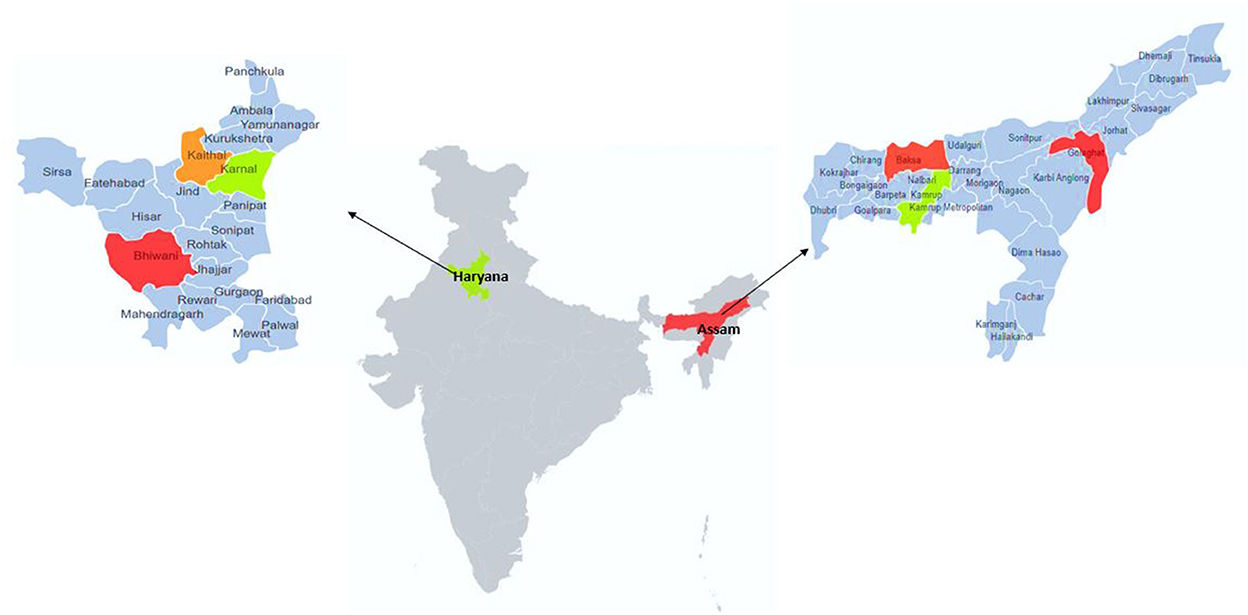
Figure 1. Map of India showing the Haryana and Assam states, with the three districts within each state included in a study on knowledge on food safety and antimicrobial resistance among milk vendors.
From each district, two community development blocks (CDBs), one urban and one rural, had been randomly selected. In case of Assam, the rural CDBs were close to urban (peri-urban) CDBs as the informal milk vendors were more predominant in urban and peri-urban areas. In each CDB, four villages were selected randomly from the list of villages having dairy production and presence of milk vendors. In case of Kamrup Metropolitan district, villages were defined as clusters of milk producers, as they were located only in certain clusters, irrespective of the village boundaries. Other villages were defined to be a cluster based on the official boundaries. Figure 2 gives the scheme that outlines the sampling design used for each state.
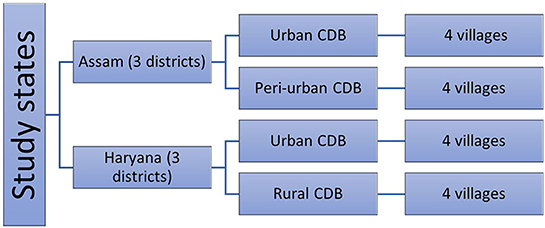
Figure 2. Sampling design for each of the study states specifying the number of districts and villages from each community development block (CDB) in the district.
The same villages were visited for the current vendor survey, and all milk vendors identified at the time of the visit were contacted for the interview. All vendors who agreed to participate were then questioned. A questionnaire was used to assess their knowledge and practices on antibiotics, milk safety and hygiene. If they had milk available, a sample of the milk was purchased at the local going rate for fresh milk.
Knowledge on antibiotics and their usage, milk safety, hygienic measures regarding handling of milk was assessed through a pre-tested vendor questionnaire (Supplementary material). The questions were asked by enumerators in local language and the responses were filled in the questionnaire written in English at the time of the interview.
Milk samples were purchased from vendors and stored in sterile containers maintaining a cold chain, during transportation to the laboratory, and kept at 4°C until further analysis at the National Institute of Veterinary of Epidemiology and Disease Informatics (NIVEDI). The samples were initially inoculated on mannitol salt broth and buffered peptone water and incubated at 37°C for 18–24 h to isolate presumptive pathogenic bacteria. Following their incubation at 37°C for 18–36 h, the culture broth was inoculated on Staphylococcus Agar No. 110 (Hi-media, Maharashtra, India) to grow staphylococci, and MacConkey agar (Hi-media, Maharashtra, India) to grow E. coli, Shigella spp., and Klebsiella spp. Brain Heart Infusion agar (Hi-media, Maharashtra, India) was used for purification and maintenance of cultures. The isolated bacteria's were screened for resistant bacteria using antibiotic disc diffusion testing as per the Kirby Bauer. (2022) method and following the Clinical Laboratory Standard Institute guidelines (Testing, 2013). Gram-positive bacteria were tested against cefoxitin (30 μg), methicillin (5 μg) and oxacillin (1 μg) for screening of methicillin resistance. Gram-negative bacteria were tested against cefoxitin (30 μg), cefotetan (30 μg), cefotaxime (30 μg), ceftazidime (30 μg), imipenem (10 μg) and meropenem (10 μg) was used for screening of beta-lactamases (extended spectrum beta-lactamase, metallo-beta-lactamase, AmpC beta-lactamase). For the purpose of this paper on vendor behavior, any sample that had either a gram-positive or gram-negative bacteria isolated as per above that showed resistance to at least one antibiotic was classified as being positive for AMR, and used as a binary variable in the analyses.
Data was entered in Microsoft Excel and analyzed using STATA 14.0 (STATACorp Ltd., College Station, TX, USA). Firstly, descriptive analyses of all vendors were carried out, followed by ANOVA (analysis of variance) to test for association between different variables for all vendors. Secondly, a descriptive analysis for the vendor milk samples that were analyzed in NIVEDI, Bangalore, for the presence of antibiotic resistant bacteria was carried out and it was combined with laboratory results corresponding to these milk samples. For these vendor samples, univariable analysis was conducted to check for associations between categorical variables like age, gender, education, milk sold, type of vendor and the presence of AMR bacteria in milk samples.
A total of 244 milk vendors were interviewed, 122 in Assam and 122 in Haryana, of these 220 were males (114 in Assam and 106 in Haryana) and 24 were females (8 in Assam and 16 in Haryana). Most, 47.5% (116/244), of the surveyed vendors from Assam and as well as from Haryana were in the age group of 31–45 years.
Only 3.1% (7/226) [18 non-respondents (NR)] had received specific milk hygiene training. In terms of general education levels, 5.7% (14/244) had not received any formal education (1 in Assam and 13 in Haryana), 9.4% (23/244) had received primary education (17 in Assam and 6 in Haryana), 41.8% (102/244) had studied up to 5–10 class (44 in Assam and 58 in Haryana), 29.5% (72/244) had reached higher secondary (41 in Assam and 31 in Haryana) and 13.5% (33/244) were graduates or above (19 in Assam and 14 in Haryana).
Most, 64.8% (158/244), milk vendors sold 2–50 ltrs. of milk/day. And 10.2% (25/244) sold ≤ 5 ltrs./day. Most of the vendors selling <50 ltrs. milk/day were shop owners. Less than half (40.2%, 98/244), vendors sold pasteurized milk while the remaining 59.8% (146/244) traded raw milk. Five categories of milk vendors were identified; vendors who sell milk at a grocery shop (37.3%, 91/244), vendors supplying milk from door to door (16%, 39/244), the vendors who sell on a roadside (6.6%, 16/244), vendors who supply milk to sweet makers/tea stall (17.6%, 43/244), and the ones selling from home/other entity (22.5%, 55/244).
The results from the ANOVA analysis (Table 1) showed that 34.4% (84/244) of the vendors checked milk for dirt, checking of milk was significantly associated with the category of vendor (p < 0.01) with shop owners more likely to check the milk for dirt as compared to other vendors. The quantity of milk sold (ltr/day) differed significantly between vendor categories (p < 0.01). Most, 86.1% (210/244) vendors agreed that boiled milk is always safe but almost half, 48.8% (119/244) of them admitted that they sometimes drink milk without boiling.
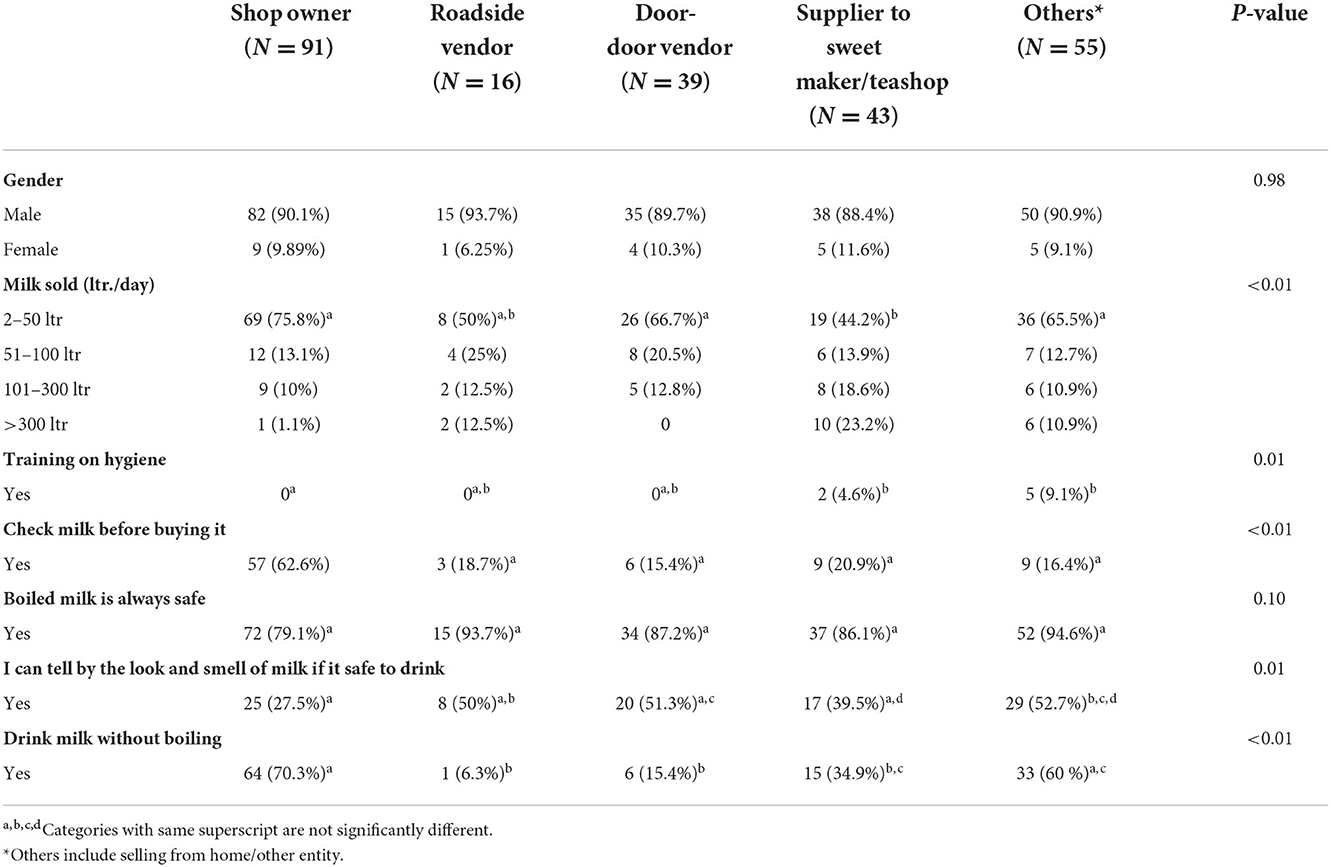
Table 1. Distribution of demographics, knowledge and practice among categories of milk vendors in Assam and Haryana, India.
When vendors were asked if they had ever heard of antibiotics, 34.8% (85/244, confidence interval (CI) 28–41%) vendors answered yes and 65.2% (159/244, CI 58–71%) no. It may be noted here that there was no distinction made between antibiotic for animal or human usage in this question. The majority of those answering what antibiotic is, answered that they kill germs, or they cure diseases. Figure 3 gives various responses of vendors who agreed to know about antibiotics. Out of 85 vendors who had heard about antibiotics, 28.2% (24/85, CI 19–39%), believed that antibiotics stop all diseases. Some (44.7%, 38/85, CI 33.9–55.8%) believed that all diseases need to be treated. Most vendors (55.2%, 47/85, CI 44.1–66%) agreed that more an antibiotic costs, the better it is. Some vendors (20%, 17/85, CI 12–30%) also agreed that the pharmacist is as good as the doctor to decide which antibiotic to use and 40% (34/85, CI 29.5–51.1%) of them agreed that increasing the amount of antibiotic makes it more effective. Only some of them, 45.8% (39/85, CI 35–57%) agreed that if antibiotics are used too often, they become ineffective. Out of 244, only one vendor knew about “withdrawal period” and could describe it correctly.
Figure 3. The various definitions of antibiotics given by milk vendors who agreed to know about antibiotics in Haryana and Assam, India.
Total 124 milk samples were tested in NIVEDI, Bangalore, for the presence of antibiotic resistant bacteria. Out of these tested samples, 85.5% (106/124, CI 78–91%) were raw milk samples and 14.5% (18/124, 8–21%) were pasteurized milk samples. In total, 64.5% (80/124, CI 55–72%) out of these samples tested positive for the presence of antibiotic resistant bacteria (either Staphylococcus or gram-negative bacteria). Out of the samples that tested positive, 83.7% (67/80, CI 73–91%) were from the raw milk vendors and 16.2% (13/80, CI 8–26%) were from the pasteurized milk vendors. The percentage of positive samples from each vendor type is presented in Figure 4. The highest proportion of milk samples with antibiotic resistant bacteria was from the vendors in the other category (selling from home/other entity) where 23/31 (74.19%) were found positive, and similar proportions were found among shop owners, 25/36 (69.44%) and door-to-door vendors, 17/24 (65.38%). Half (50%, 12/24) of the milk samples from suppliers to sweet makers/teashops and 42.86% (3/7) of milk samples from roadside vendors were positive. All six milk vendors who had attended milk hygiene training had resistant bacteria present in their milk. Of the vendors whose milk tested positive for antibiotic-resistant bacteria, 43.75% (35/80, CI 32–55%) believed they could tell if milk is safe to drink just by its look and smell. Only 8.75% (7/80, CI 3–17%) of these 80 vendors kept the milk chilled after purchase; 30% (24/80, CI 20–41%) agreed to know about antibiotics and 70% (56/80, CI 58–79%) answered negative. Only one of them knew about “withdrawal period.”
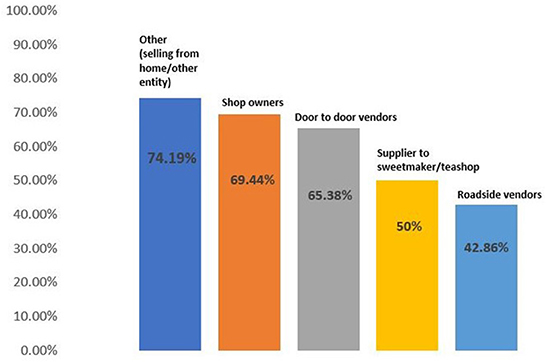
Figure 4. Percentage of milk samples with detected antibiotic-resistant bacteria out of the total milk samples collected from different milk vendor categories in Assam and Haryana, India.
Univariable analyses did not show any significant association (p > 0.05) between age, gender, education level, amount of milk traded or type of trader with the presence of AMR in vendor milk samples.
The results of this study show that milk vendors in Assam and Haryana are predominantly male, are poorly educated, only few vendors receive training on milk hygiene, trade in low daily volumes of milk, and form a very heterogenous group with five major types of vendors identified based on how they sell the milk. Such informal dealers may not appear to pose a serious threat to public health, however, almost sixty percent of these vendors traded exclusively in raw milk. Raw milk may pose a direct risk to the consumer by exposing them to foodborne pathogens through consumption, and indirectly through cross-contamination (Oliver et al., 2005). In this regard, proper boiling of milk before consumption reduce the risk to great extent. The results of this study revealed poor handling and storage of raw milk by the vendors, only 8.2% (12/146, CI 0.04–0.13) of raw milk vendors kept the milk chilled between purchasing from farm and selling, leaving the remaining 91.8% (134/146, CI 0.86–0.95) in breach of regulations of the Food Safety and Standards Authority of India (FSSAI., 2018) which stipulates that all raw milk must be stored at 4–5°C (FSSAI., 2018). Similar results were found in a study among dairy value chain actors in Assam (Lindahl et al., 2019) where milk traders reported never storing milk but delivering it as soon as possible. Considering that at the time this study was conducted, the average daytime weather conditions for the study sites in Assam and Haryana were slight hot and humid with temperature varying from 25 to 35°C (Ministry of Earth Sciences, 2017), a lack of cold chain allows for microbial growth and milk spoilage (Lingathurai and Vellathurai, 2013).
Indeed, milk vendors themselves are also at risk of foodborne disease given that we found that 48.8% (119/244, CI 0.42–0.55) of milk vendors agreed that they sometimes drink raw milk themselves. The majority of the sellers here were shop owners who might be referring to drinking tetra pack milk or pasteurized milk, which is acceptable to consume without boiling, but there were others who concurred on consuming raw milk without boiling. This is in line with earlier findings from other countries where milk vendors and their families consume more milk than the general population, possibly as they consume unsold products (Kirino et al., 2016). Most of the vendors in our study believed that they could recognize if milk is safe to consume by just its sight and smell. This is also in line with the results of a previous study conducted in Assam (Lindahl et al., 2019) where 99.4% of the milk traders agreed on a statement saying, “you can tell if milk is safe by sight or taste.” This highlights that attitudes and practices around milk consumption merit further investigation among key members within these households responsible for food preparation, especially those responsible for preparing food for infants and the elderly.
This study found a high prevalence of antibiotic resistant bacteria in raw milk samples, similar to other studies in India, where raw milk samples were found positive for the presence of antibiotic resistant bacteria (Kumar and Gupta, 2018; Kumar et al., 2021). This is indeed a matter of concern. The simplistic, binary focus of the diagnostic method used in our study give results which show milk samples to be positive or negative for the presence of one or more bacteria resistant to one or more antibiotic, as a first step in scoping out AMR prevalence among vendors of different categories. While other studies focus on identifying specific AMR bacteria, such as a study in southern India showing that raw milk samples collected from local milk vendors had a 39.09% prevalence for the presence of antibiotic resistant Staphylococcus aureus (Sudhanthiramani et al., 2015). For this study, it was decided to focus primarily on the presence or absence of antibiotic resistant bacteria rather than on identifying specific pathogens, given that the cross-cutting measures needed to reduce the risk of AMR bacteria moving along the informal dairy value chain will be overarching, regardless of what specific bacteria or antibiotic resistance involved.
Similar to the research carried out among small-scale dairy farmers in the same study sites in Assam and Haryana, vendors in this study, demonstrate little or no knowledge of the concept of milk withdrawal period, which is similar to farmers, and we have earlier reported the presence of antibiotic residues in the milk from these two states (Kumar et al., 2021), highlighting the lack of appropriate measures taken to prevent such hazards entering the dairy supply chain. If vendors, and indeed farmers, are unaware of such concepts as milk withdrawal periods, then reducing the risk of contamination of milk is very challenging. Our study also showed that 65.2% (CI 0.58–0.71) of all milk vendors did not know what an antibiotic is, and 34.8% (CI 0.28–0.41) of those who said they did know could not give a clear definition of an antibiotic. A previous study on the prevailing practices in the use of antibiotics by dairy farmers in Haryana (Kumar and Gupta, 2018) revealed that the smallholder dairy farmers (7.14%) procured antibiotics from the milk vendors for the treatment of their animals. The fact that milk vendors have so limited awareness of antibiotics while yet being found to be giving antibiotics to dairy farmers raises serious concerns.
The level of formal training received by the milk vendors in our study was very low, only 6 vendors had ever received any training on milk hygiene or safety. The vendors attended training from either a private milk cooperative or by the local veterinary department. This poor level of training is not unique to our study cohort, rather it is very much reflected throughout other parts of India as highlighted by other KAP studies along the informal dairy value chain (Mutua et al., 2020; Sharma et al., 2020). We believed that increased levels of milk hygiene training could impact on food safety practices among vendors as seen in other studies where milk traders and dairy farmers training interventions proved to increase hygiene standards (Lindahl et al., 2018, 2019).
While training may be a beneficial strategy for addressing farmers' and vendors' lack of knowledge regarding food safety practices, antibiotic usage, and the possible harm to public health, it is just one part of a larger solution. Farmers need to be incentivized to produce safe milk, vendors need to demand certain standards when purchasing milk and follow certain hygienic standard, and the consumer needs to also demand safer milk and indeed be willing to pay for a safe product.
A Theory of Change (ToC) approach has helped bring about this shift in mentality among the stakeholders in the informal dairy value chain in other LMICs (Johnson et al., 2015). A ToC approach improves our understanding of how change occurs and outlines what needs to be done to achieve desired outcomes, it requires a number of activities by different entities, to address different objectives to be undertaken, rather than relying on a single intervention (Mutua et al., 2020). Figure 5 is an example of how a ToC approach could be taken, targeting different actors, including consumers, to mitigate milk-borne pathogens in these two states of India.
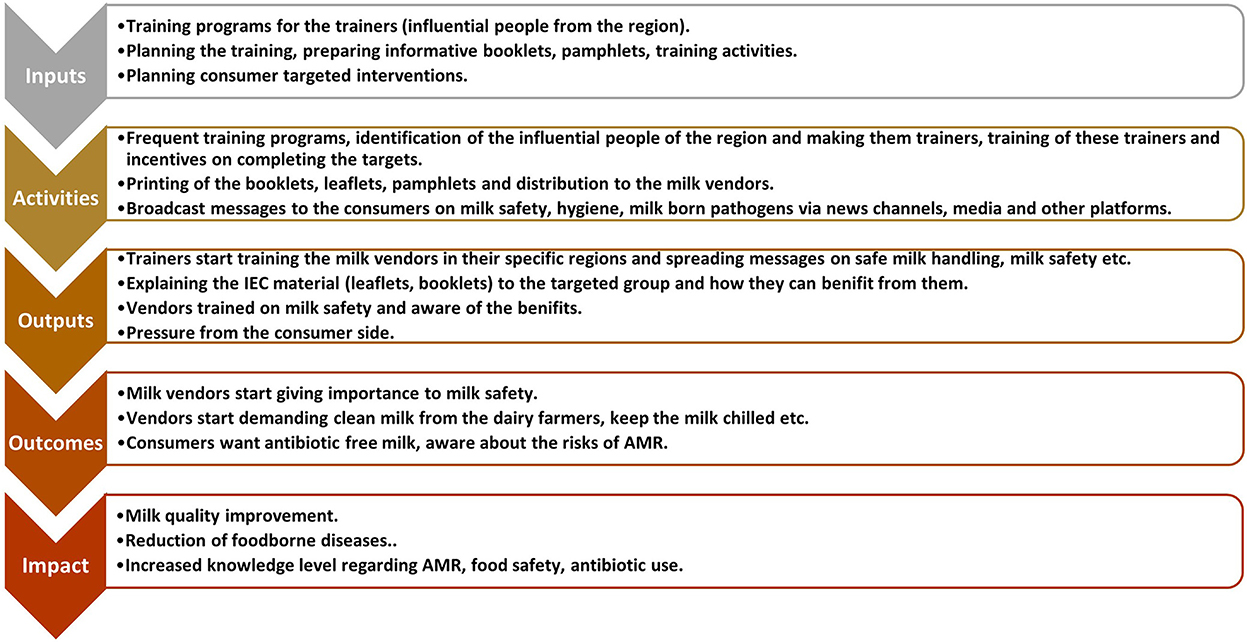
Figure 5. A hypothetical theory of change targeting different actors along the dairy value chain to improve milk safety.
ToC suggests how and why a program works and is a critical reflection on program's strategy, context, and outcomes. It was developed because it is hard to evaluate complex social change programs. The ToC explains the assumptions behind the change process that are written down and tested (Lam et al., 2021). Figure 6 explains the assumptions for the suggested ToC above.

Figure 6. A theory of change for how milk vendor intervention can affect milk safety, including assumptions 1–4 listed on the left, actions, and outcomes flow from the bottom of the diagram upwards.
Many vendors failed to fully answer the questionnaire, making statistical analysis of many variables impossible. Some vendors refused to commit to specific responses; for example, when asked about the type of container used to store milk, interestingly, 26 vendors responded that they did not know what kind of container, open or closed, they used. It is unlikely that a vendor does not know if the container has a lid or not. Also, issues surrounding how the questionnaire was delivered come into play. Did some vendors feel obliged to give a “right answer?” This highlights the challenges involved when carrying out research among economically invested stakeholders who may fear financial repercussion if they do not give the expected answer, they feel the interviewer is looking for. Future studies should include other forms of research techniques beyond the use of a single questionnaire, such as the use of focus groups, to help ease out such complexities.
This study highlights the unsafe ways in which milk vendors handle milk, specifically raw milk. Increased bacterial load might result from the unhygienic ways the informal vendors handle the milk. Many milk samples that were tested for the presence of antibiotic-resistant bacteria were found positive, indicating transmission of AMR along the dairy values chain. There exists a vast knowledge gap when it comes to awareness related to milk hygiene and antibiotics or antimicrobial resistance. The knowledge and attitude of the surveyed vendors related to milk safety; antibiotics were found to be poor, and only a very few vendors had attended any training on hygiene and food safety. Caution must be taken not to demonize the informal nature of this value chain; while risk to human health exist, small-scale food production and processing is an essential pathway out of poverty, existing food safety regulation is often ineffective at the ground level. However, conditions on the ground must be taken into consideration when attempting to implement change. Most of the vendors in this study did not comply with the national milk safety regulation, yet they cannot be blamed if they are unaware of the existence of this legal framework. The policymakers must focus on how these informal vendors can be made aware on the basic safety measures to be followed while handling milk. Also, a monitoring and evaluation mechanism needs to be set up to investigate if the regulations are adhered to at the ground level. The ToC approach could be a useful way of bringing about a change in mindsets of farmers, vendors, and consumers, englobing multiple stakeholders along the value chain with the aim of bringing about sustainable, lasting improvements.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical approval for the study was granted by the Institutional Research Ethics Committee (IREC) of the International Livestock Research Institute (ILRI) on 21 September 2015 (No: ILRI-IREC 2015-12). The patients/participants provided their written informed consent to participate in this study.
JL, BS, SB, NG, and RD: conceptualization, investigation, and resources. JL, BS, SB, and NG: methodology and validation. GS and EL: formal analysis and writing—original draft preparation. GS, JL, and EL: visualization. TD, BS, and JL: laboratory data interpretation. JL and ÅL: supervision. JL and RD: project administration. JL and DG: funding acquisition. All authors contributed to the article and approved the submitted version.
This research was funded by the Indian Council of Agricultural Research (ICAR) and the CGIAR Research Programme on Agriculture for Nutrition and Health.
The authors thankfully acknowledge the administrative support received from the management of the International Livestock Research Institute (ILRI) and the Indian Council of Agricultural Research (ICAR). The authors also thankfully acknowledge the support received from the ICAR-NIVEDI, Bangalore, India and local enumerators and local Animal Husbandry and Veterinary Officials in the state of Assam and Haryana.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fsufs.2022.1058384/full#supplementary-material
Alimi, B. A. (2016). Risk factors in street food practices in developing countries: a review. Food Sci. Hum. Wellness [Internet]. 5, 141–148. doi: 10.1016/j.fshw.2016.05.001
Dhanashekar, R., Akkinepalli, S., and Nellutla, A. (2012). Milk-borne infections. an analysis of their potential effect on the milk industry. Germs [Internet]. 2, 101. doi: 10.11599/germs.2012.1020
Douphrate, D. I., Hagevoort, G. R., Nonnenmann, M. W., Lunner Kolstrup, C., Reynolds, S. J., Jakob, M., et al. (2013). The dairy industry: a brief description of production practices, trends, and farm characteristics around the world. Jama 18, 187–197. doi: 10.1080/1059924X.2013.796901
FSSAI. (2018). Guidance Document Food Safety Management Systems Food Industry Guide To Implement Gmp/Ghp Requirements Milk And M Ilk Products. Available online at: http://www.fssai.gov.in (accessed September 23, 2022).
Grwambi, B. (2020). Food Safety and Food Security in the Informal Sector. Food Secur Africa [Internet]. 14, 23. doi: 10.5772/intechopen.91012
Johnson, N., Mayne, J., Grace, D., and Wyatt, A. (2015). How Will Training Traders Contribute to Improved Food Safety in Informal Markets for Meat and Milk? A Theory of Change Analysis. Available online at: www.ilri.org (accessed September 23, 2022).
Kirby Bauer. (2022). Disc Diffusion Method For Antibiotic Susceptibility Testing [Internet]. Available online at: https://microbenotes.com/kirby-bauer-disc-diffusion/ (accessed September 23, 2022).
Kirino, Y., Makita, K., Grace, D., and Lindahl, J. (2016). Survey of informal milk retailers in Nairobi, Kenya and prevalence of aflatoxin M1 in marketed milk. African J. Food. Agric. Nutr. Dev. 16, 11022–11038. doi: 10.18697/ajfand.75.ILRI05
Kumar, A., Staal, S. J., and Singh, D. K. (2011). Smallholder Dairy farmers' access to modern milk marketing chains in india §. Agric Econ Res Rev. 24:243–53. doi: 10.22004/ag.econ.118232
Kumar, N., Sharma, G., Leahy, E., Shome, B. R., Bandyopadhyay, S., Deka, R. P., et al. (2021). Understanding antibiotic usage on small-scale dairy farms in the indian states of assam and haryana using a mixed-methods approach—outcomes and challenges. Antibiot. 10, 1124. doi: 10.3390/antibiotics10091124
Kumar, V., and Gupta, J. (2018). Prevailing practices in the use of antibiotics by dairy farmers in Eastern Haryana region of India. Vet. World [Internet]. 11, 274. doi: 10.14202/vetworld.2018.274-280
Kuralayanapalya, S. P., Patil, S. S., Hamsapriya, S., Shinduja, R., Roy, P., and Amachawadi, R. G. (2019). Prevalence of extended-spectrum beta-lactamase producing bacteria from animal origin: a systematic review and meta-analysis report from India. PLoS One [Internet]. 14, e0221771. doi: 10.1371/journal.pone.0221771
Lam, S., Nguyen, H. T. T., Tuan, H. N. H., Nguyen, L. T., Nguyen-Viet, H., Toribio, J. A., et al. (2021). Unpacking the theory behind one health food safety programs: a vietnam case study. Front. Vet. Sci. 8, 1402. doi: 10.3389/fvets.2021.763410
Lindahl, J. F., Deka, R. P., Asse, R., Lapar, L., and Grace, D. (2019). Hygiene Knowledge, Attitudes and Practices Among Dairy Value Chain Actors in Assam, North-East India and the Impact of a Training Intervention. Available online at: https://www.tandfonline.com/doi/abs/10.1080/20008686.2018.1555444 (accessed September 23, 2022).
Lindahl, J. F., Deka, R. P., Melin, D., Berg, A., Lundén, H., Lapar, M. L., et al. (2018). An inclusive and participatory approach to changing policies and practices for improved milk safety in Assam, northeast India. Glob. Food Sec. 17, 9–13. doi: 10.1016/j.gfs.2018.03.002
Lingathurai, S., and Vellathurai, P. (2013). Bacteriological quality and safety of raw cow milk in Madurai (South India). Bangladesh J. Sci. Ind. Res. [Internet]. 48, 109–114. doi: 10.3329/bjsir.v48i2.15741
Milk Production in India. (2022). nddb.coop [Internet]. Available online at: https://www.nddb.coop/information/stats/milkprodindia (accessed September 23, 2022).
Ministry of Earth Sciences G.. (2017). Annual Report 2016 India Meteorological Department [Internet]. Available online at: https://metnet.imd.gov.in/imdnews/ar2016.pdf (accessed October 20, 2022).
Mutua, F., Sharma, G., Grace, D., Bandyopadhyay, S., Shome, B., and Lindahl, J. (2020). A review of animal health and drug use practices in India, and their possible link to antimicrobial resistance. Antimicrob. Resist. Infect. Control 9, 1–13. doi: 10.1186/s13756-020-00760-3
Oliver, S. P., Jayarao, B. M., and Almeida, R. A. (2005). Foodborne pathogens in milk and the dairy farm environment: food safety and public health implications. Food 2, 115–129. doi: 10.1089/fpd.2005.2.115
Rajendran, K., and Mohanty, S. (2004). Dairy co-operatives and milk marketing in India: constraints and opportunities. J. Food Distrib. Res. [Internet]. 35, 34–41. doi: 10.22004/ag.econ.2723
Roesel Kristina, G. D. (2014). Food Safety and Informal Markets [Internet]. 1st ed. Food Safety and Informal Markets. London: Routledge. 284. Available online at: https://www.taylorfrancis.com/books/edit/10.4324/9781315745046/food-safety-informal-markets-kristina-roesel-delia-grace (accessed September 23, 2022).
Sharma, G., Mutua, F., Deka, R. P., Shome, R., Bandyopadhyay, S., Shome, B. R., et al. (2020). A qualitative study on antibiotic use and animal health management in smallholder dairy farms of four regions of India. Infect. Ecol. Epidemiol. [Internet]. 10, 85. doi: 10.1080/20008686.2020.1792033
Sudhanthiramani, S., Swetha, C. S., and Bharathy, S. (2015). Prevalence of antibiotic resistant Staphylococcus aureus from raw milk samples collected from the local vendors in the region of Tirupathi, India. Vet. World [Internet]. 8, 478. doi: 10.14202/vetworld.2015.478-481
Keywords: milk vendors, AMR, informal milk supply chain, food safety, milk hygiene, raw milk, antibiotics
Citation: Sharma G, Leahy E, Deka RP, Shome BR, Bandyopadhyay S, Dey TK, Goyal NK, Lundkvist Å, Grace D and Lindahl JF (2022) Antibiotic use, knowledge, and practices of milk vendors in India's informal dairy value chain. Front. Sustain. Food Syst. 6:1058384. doi: 10.3389/fsufs.2022.1058384
Received: 30 September 2022; Accepted: 07 November 2022;
Published: 30 November 2022.
Edited by:
Mary Anne Amalaradjou, University of Connecticut, United StatesReviewed by:
Indranil Samanta, West Bengal University of Animal and Fishery Sciences, IndiaCopyright © 2022 Sharma, Leahy, Deka, Shome, Bandyopadhyay, Dey, Goyal, Lundkvist, Grace and Lindahl. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Garima Sharma, ZHJnYXJpbWExMTFAZ21haWwuY29t; Zy5zaGFybWFAY2dpYXIub3Jn
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.