 Gaoxiang Zhong
Gaoxiang Zhong
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol. , 18 July 2024
Sec. Quantitative Psychology and Measurement
Volume 15 - 2024 | https://doi.org/10.3389/fpsyg.2024.1378639
Background: Pediatric cancer ranks among the leading causes of mortality in children globally. While serving as primary caregivers, certain parents may experience anxiety, depression, and other related challenges. However, not all parents succumb to such psychological distress. Resilience emerges as a potential protective factor. Assessing parental resilience holds paramount importance for healthcare professionals in identifying issues and offering tailored interventions. Yet, mainland China lacks adequate tools for this assessment. Hence, this study endeavors to translate the Resilience Scale for Parents of Children with Cancer (RSP-CC) into Chinese and scrutinize its psychometric properties.
Methods: From April 2023 to January 2024, a methodological study was conducted in Chengdu, Chongqing, and Jinzhou, China, recruiting 377 eligible parents via convenience sampling for a multicenter cross-sectional survey. The translation process of the RSP-CC adhered rigorously to the Brislin model, involving forward and back-translation, followed by necessary modifications. Item analysis was assessed using the critical ratio and the item-total correlation coefficient. Validity evaluation encompassed content and internal validity assessments. Scale reliability was determined through Cronbach’s α coefficient, retest reliability, and split-half reliability coefficients.
Results: The Chinese version of the RSP-CC comprises 4 dimensions and 24 items, explaining a cumulative variance contribution of 63.58%. In this investigation, the content validity index attained a score of 0.97. Exploratory factor analysis (EFA) yielded four factors consistent with the original scale, while confirmatory factor analysis (CFA) indicated satisfactory fit indices. Both Cronbach’s α coefficient and retest reliability stood at 0.95, with a split-half reliability coefficient of 0.82.
Conclusion: After rigorous translation and verification, the RSP-CC was adapted in China, demonstrating favorable psychometric characteristics. It stands as an effective instrument for parents of children diagnosed with cancer in China. Additionally, this scale could serve as a crucial tool for clinical staff in formulating specific interventions.
Pediatric cancer stands as a leading cause of mortality among children globally, imposing significant burdens on both the afflicted child and their family (Lubega et al., 2021). Global Cancer Statistics indicate an annual diagnosis of approximately 380,000 children worldwide (Sung et al., 2021), with nearly 90% of cases occurring in low to middle-income countries (Cayrol et al., 2022). China, as a developing nation, grapples with a substantial pediatric cancer burden, too. World Health Organization data reveals that nearly 120,000 children in China were diagnosed with cancer between 2015 and 2020, comprising 14% of global juvenile cancer incidences (Ji et al., 2022).
In China, prevalent types of childhood cancer include leukemia, brain and central nervous system malignancies, and lymphomas (Ni et al., 2022). The diagnosis of cancer can inflict profound physical, psychological, social, and behavioral distress upon both the child and their primary family caregivers (Cheng et al., 2023). Throughout the arduous journey of childhood cancer treatment, parents assume the primary caregiving role due to their child’s tender age. Confronted with the treatment’s intricacies and the burden of severe symptoms, parents endure heightened levels of stress compared to their children (Law et al., 2019). Nevertheless, research indicates that despite adversities, a substantial portion of parents actively engage in their child’s treatment, participate in decision-making, and provide both material and emotional support (Van Schoors et al., 2015). Within this context, parental resilience emerges as a pivotal factor.
Resilience denotes an individual’s capacity to adapt effectively when confronted with adversity, trauma, tragedy, threat, or severe stressors (Bajjani-Gebara et al., 2019). Chung et al. (2023) demonstrated a positive correlation between parental resilience in the context of childhood cancer and coping strategies (r = 0.53), while revealing negative correlations with anxiety (r = −0.57) and depression (r = −0.42). Similarly, Mohammadsalehi et al. (2022) found a positive association between parental resilience and self-efficacy (r = 0.37). Parents with high resilience may tend to exhibit superior coping skills and a more positive outlook, facilitating their ability to navigate stressors and adversities effectively. Conversely, parents with low resilience may find themselves more vulnerable to the challenges posed by their child’s cancer diagnosis, with potential repercussions on their quality of life and psychological well-being (Da Silva et al., 2010; Luo et al., 2022). Consequently, bolstering parental resilience emerges as a key strategy for alleviating psychological distress and enhancing overall quality of life. Recognizing the significance of this issue, Prof. Önal (Önal et al., 2023) developed the RSP-CC to assess the resilience of parents. The scale has 4 dimensions and 24 items, with acceptable results in terms of reliability, content validity, and internal validity (Önal et al., 2023).
Currently, the Conner-Davidson Resilience Scale stands as the predominant tool for gaging resilience levels in China (Connor and Davidson, 2003). However, its applicability is limited to general outpatients, psychiatric patients, and those with anxiety disorders, rendering it unsuitable for the specific population of parents of children with cancer. Utilizing this scale in such a context may compromise the validity of the results. Hence, there is a pressing need for a dynamic, multidimensional, and validated Chinese version of the RSP-CC tailored to assess parental resilience and evaluate the efficacy of pertinent interventions.
According to the definition of Patterson’s Family Resilience Theory (Patterson, 2002), factors affecting resilience are generally categorized into protective and risk factors. When experiencing a major crisis, protective and risk factors interact and mutually influence each other. In this study, coping and social support represent protective factors, whereas emotional stress and caregiver burden constitute risk factors. Chronic negative emotions can impede parental coping mechanisms (Koutelekos et al., 2023), while social support has been shown to alleviate such emotions, whereas caregiver burden exacerbates them (Guralnick et al., 2008; Güven Baysal and Çorabay, 2024). Moreover, the presence of social support can mitigate caregiver burden (Adib-Hajbaghery and Ahmadi, 2019). These four factors dynamically interact to influence a parent’s resilience. The purpose of this study was to translate the RSP-CC into Chinese following the Brislin translation model and to assess its psychometric properties through item analysis, content validity analysis, internal validity analysis, internal structural validity analysis, and reliability analysis.
This study adopted a methodological approach. Following comprehensive training and approval from relevant hospitals, two clinicians and one clinical nurse from the Cancer Hospitals of Chengdu, Chongqing, and Jinzhou, China, conducted participant recruitment from April 2023 to January 2024. Inclusion criteria comprised parents of children aged ≤18 years diagnosed with cancer via pathological investigation, serving as primary caregivers, and providing informed consent for research participation. Exclusion criteria encompassed parents of children with additional severe or chronic illnesses, parents of children who received palliative treatment, and parents with communication or cognitive impairments, as determined by language proficiency and cognitive functioning assessments. This study was conducted under the authorization of Prof. Önal and obtained endorsement from the Ethics Committee of Jinzhou Medical University (Ethics Approval No. JZMULL2023129). Prior to survey administration, parents received clear explanations regarding the survey’s objectives, significance, and precautions.
Participant sample size was determined in accordance with factor analysis guidelines. Exploratory factor analysis (EFA) necessitates samples five to ten times the total number of scale items (Knapp and Sawilowsky, 2004), while confirmatory factor analysis (CFA) requires a minimum of 200 cases (Lasmarías et al., 2021). Considering different sample sources for EFA and CFA, and accounting for a 10% invalid questionnaire rate, a minimum of 352 cases was deemed necessary for inclusion. In this study, 400 questionnaires were distributed, with 385 recovered, and 377 deemed valid, yielding a valid recovery rate of 94.25%. Questionnaire completion time averaged 8–10 min, with data collected onsite. Subsequently, a follow-up survey was conducted with a randomly selected subset of 50 parents after a two-week interval to assess retest reliability.
After conducting a thorough review of prior research and consulting with experts, a tailored questionnaire was developed to collect demographic data from both parents and children. The questionnaire encompassed details such as parents’ gender, age, educational background, occupation, economic status, as well as the child’s age, gender, diagnosis, and treatment stage.
The degree of resilience in parents of children with cancer was assessed using the RSP-CC. This scale comprises 4 dimensions and 24 items: coping (12 items), emotional stress (5 items), social support (4 items), and caregiver burden (3 items) (Önal et al., 2023). Responses were measured on a 5-point Likert scale, ranging from “strongly disagree” (1) to “strongly agree” (5), with a total score range of 24–120, where higher scores indicate greater resilience. This scale was validated by 601 parents of children with cancer in Turkey, and the results showed that the overall Cronbach’s α coefficient was 0.99 (Önal et al., 2023).
Following authorization from Prof. Önal, the translation and refinement of the RSP-CC were meticulously conducted in accordance with the Brislin model (Brislin, 1970). Initially, the scale was translated into Chinese by a Ph.D. candidate in oncology proficient in English, alongside an English professor with overseas experience. Subsequently, forward translations were rendered into English by a nursing specialist and a foreign language instructor from the UK, respectively, forming reverse translation versions. Finally, two proficient bilingual specialists compared and deliberated on the translations and the original scale, culminating in the development of a draft Chinese version of the RSP-CC.
A panel of seven experts (comprising two pediatricians, two psychologists, and three oncologists) was convened to refine the draft RSP-CC. Selection criteria mandated a minimum of 6 years of relevant research in pediatric oncology psychology, attainment of at least an attending physician level, and possession of a master’s degree. The expert panel consisted of 5 males and 2 females, with 3 holding master’s degrees and 4 doctorates, and averaging (18.14 ± 6.01) years of professional experience.
After cross-cultural adaptation, a preliminary investigation involving 30 parents was conducted utilizing the revised RSP-CC. This phase aimed to gather feedback on scale comprehension, content relevance, and emotional resonance. Among the participants, one mother suggested revising item 7 from “Having cancer in my life has made me a more understanding and tolerant person” to “In my life, the presence of my child’s cancer has made me a more understanding and tolerant person.” Additionally, she proposed changing item 13 from “The advent of cancer in my life has caused me to become an anxious person” to “In my life, the appearance of my child’s cancer has turned me into an anxious person” to provide a clearer definition of cancer and better alignment with the reading preferences of Chinese people. Similarly, a father suggested changing item 15 from “I have not been sleeping as well since cancer entered my life” to “I have not slept as well since my child was diagnosed with cancer.” The research team reviewed and incorporated these recommendations, and finally, the Chinese version of the RSP-CC was developed.
Data analysis was performed using AMOS 24.0 and SPSS 26.0. Continuous data were expressed as mean ± standard deviation, while categorical data were presented as frequency and percentage (%). Significance was established at p < 0.05.
Item analyses were evaluated by using the critical ratio and correlation coefficient methods. The critical ratio was utilized to assess item differentiation, with a ratio of ≥3 considered indicative of appropriate differentiation (Raykov and Marcoulides, 2016). Additionally, homogeneity was evaluated through calculation of the item-factor correlation coefficient, with a coefficient of ≥0.40 indicating satisfactory homogeneity (Raykov and Marcoulides, 2016).
Seven qualified specialists were engaged in evaluating the relevance of the items for this study. The content validity index of each item (I-CVI) was computed by dividing the number of specialists rating an item with 3 or 4 points by the total number of participating specialists. The content validity index of the scale (S-CVI) was determined by averaging the I-CVI values across all items. Generally, when I-CVI ≥ 0.78 and S-CVI ≥ 0.90, the scale’s content validity is considered satisfactory (Zamanzadeh et al., 2015).
In this study, the internal validity of the Chinese version of the RSP-CC was assessed by exploratory factor analysis (EFA) and confirmatory factor analysis (CFA). The collected samples were randomly divided into two subsamples. Subsample 1 (n = 177) was used to conduct EFA, and subsample 2 (n = 200) was used to conduct CFA.
The EFA was used to delineate the underlying structure of the scale factors (Schreiber, 2021). If the value of the Kaiser-Meyer-Olkin (KMO) is more than 0.60 and Bartlett’s test of sphericity yields a significant result, it indicates that EFA could be conducted (Tobias and Carlson, 1969). The factors were extracted based on the principal axis factoring (PAF), the principle of eigenvalue >1, and the promax rotation method. Four conditions must be met: (1) all of the factor loadings remain greater than 0.40, (2) the absolute value of the difference between the two factor loadings should be at least greater than 0.20, (3) at least three of the extracted items should be attributed to one factor, and (4) the cumulative variance contribution should be >0.40 (Schreiber, 2021).
The CFA was conducted to further validate the rationality of the model’s factor structure. To make the results more robust, the data were analyzed for multivariate normality before choosing the estimation method for CFA. The results indicated a p-value of 0.14 (>0.05), suggesting that the data were multivariate normally distributed. Based on this result, a structural equation model was constructed using the maximum likelihood ratio method, with items as observed variables and factors as latent variables for CFA. In this four-factor model, coping, emotional stress, social support, and caregiver burden encompass the primary psychological and social challenges encountered by parents of children with cancer (Önal et al., 2023). These factors interact and mutually influence each other. By comprehensively studying these four factors, healthcare workers can gain insight into the parents’ psychological adaptation process, laying the groundwork for developing tailored psychological interventions and support measures. The specific numerical requirements are as follows: (1) chi-square degree of freedom (χ2/ν) < 3, (2) root mean square residual (RMSR) < 0.05, (3) Tucker-Lewis index (TLI), comparative fit indices (CFI), and incremental fit indices (IFI) > 0.90, and (4) root mean square error of approximation (RMSEA) < 0.08. In general, when the RMSEA value exceeds 0.08, it suggests a poor model fit; when the RMSEA falls within the range of 0.05–0.08, it indicates an acceptable model fit; and when the RMSEA is below 0.05, it signifies a good model fit (Shi et al., 2022).
The convergent and discriminant validity were evaluated by calculating the average variance extracted (AVE), the combined reliability (CR), and the square root of the AVE. The standards for evaluation are as follows: the AVE must be >0.50, the CR must be >0.70, and the square root of the AVE must exceed the correlation coefficients between the relevant factors (Fornell and Larcker, 1981).
The split-half reliability coefficient and Cronbach’s α coefficient were calculated to assess internal consistency. Subsequently, 50 parents previously identified were reevaluated using the same scale after 2 weeks to determine retest reliability. It is widely acknowledged that for a scale to exhibit good reliability, these indexes must all exceed 0.70 (Chang et al., 2018).
This study involved a total sample of 377 parents, comprising 120 fathers (31.8%) and 257 mothers (68.2%). Among them, 228 (60.5%) were aged between 31 and 40, with an average age of (35.19 ± 5.94) years. Furthermore, 123 (32.6%) had graduated from junior high school, 80 (21.1%) were unemployed, 124 (32.9%) reported a family income ranging from 2,001 to 4,000 yuan per month, and 164 (43.5%) resided in urban areas. Detailed information is available in Table 1.
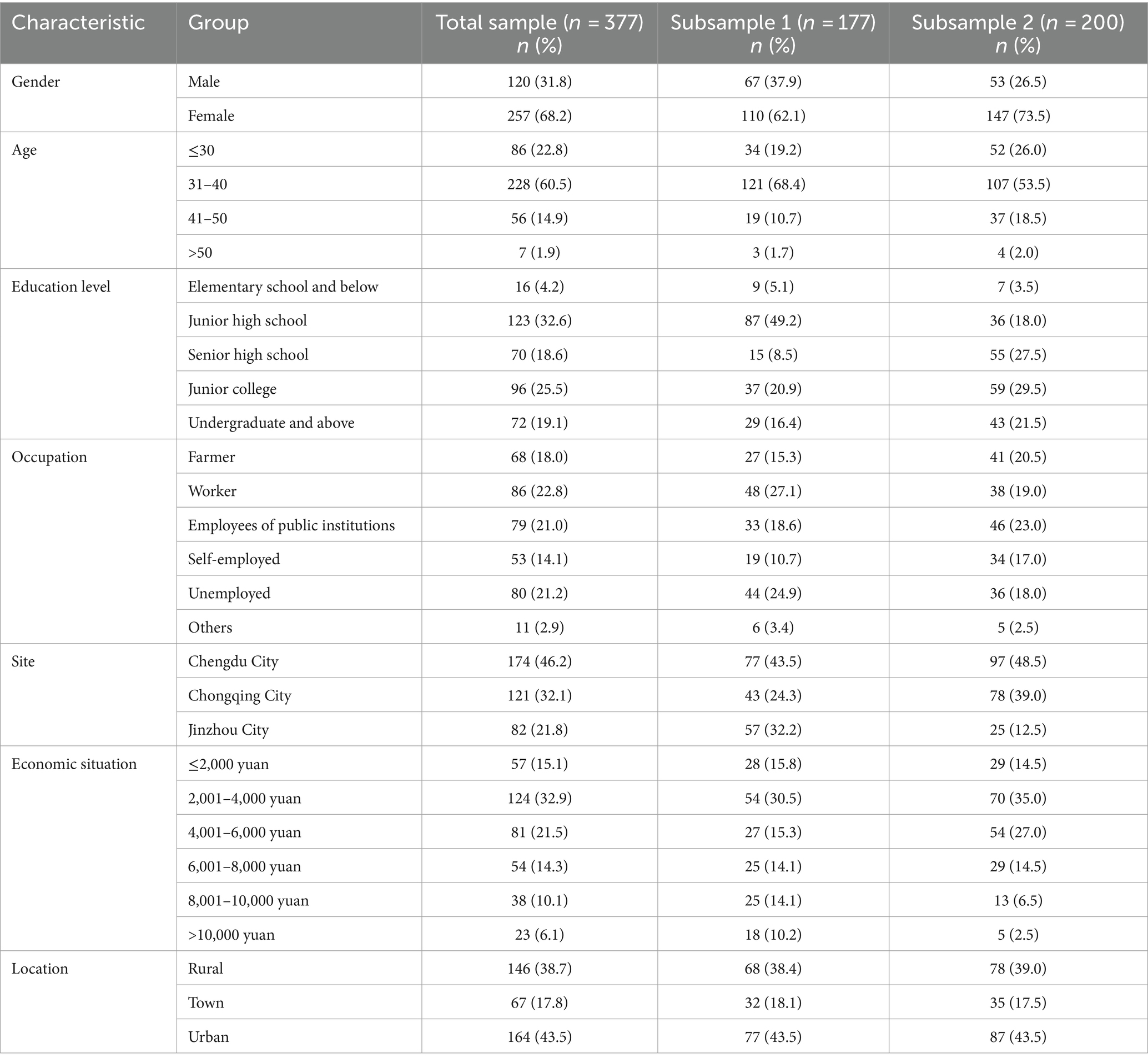
Table 1. The general demographic characteristics of parents.
Regarding the children of participating parents, 241 (63.9%) were male, with 199 (52.8%) aged ≤6 years and an average age of (6.72 ± 4.39) years. Additionally, 145 (38.5%) had acute lymphoblastic leukemia, 72 (19.1%) had other types of leukemia, and 63 (16.7%) had lymphoma. Among them, 286 (75.9%) were undergoing current treatment. Detailed information is provided in Table 2.
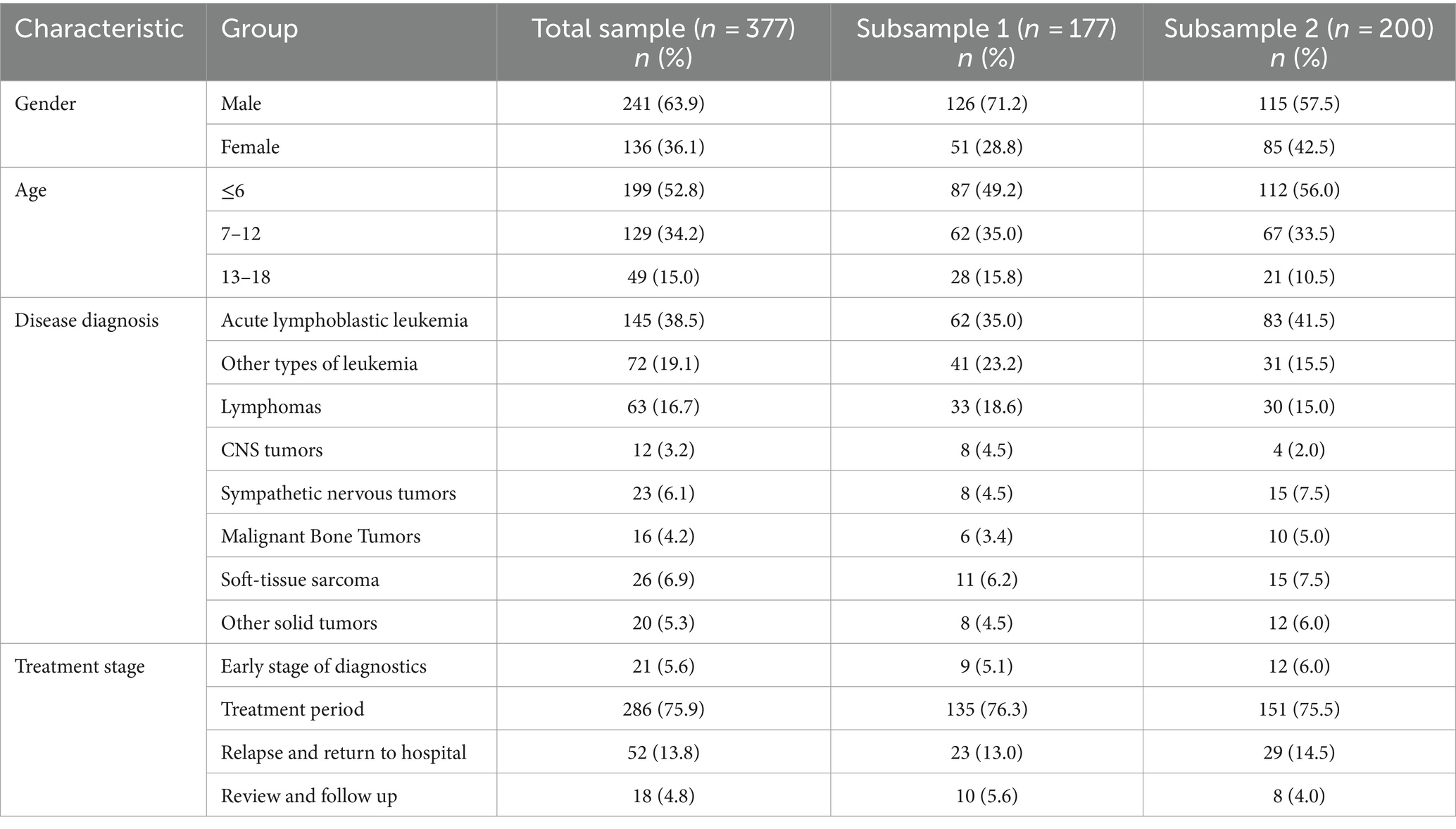
Table 2. The general demographic characteristics of children.
The results of the item analysis revealed critical ratios (t-values) ranging from 10.59 to 22.47, indicating a high level of item differentiation within the scale. Moreover, the correlation coefficients between individual item scores and their corresponding factor scores ranged from 0.71 to 0.89, indicating a high degree of homogeneity among the items of the scale. Furthermore, the Cronbach′s α coefficient of the corresponding factor decreased after deleting any of the item, so all 24 items could be retained. For detailed information, please see Table 3.
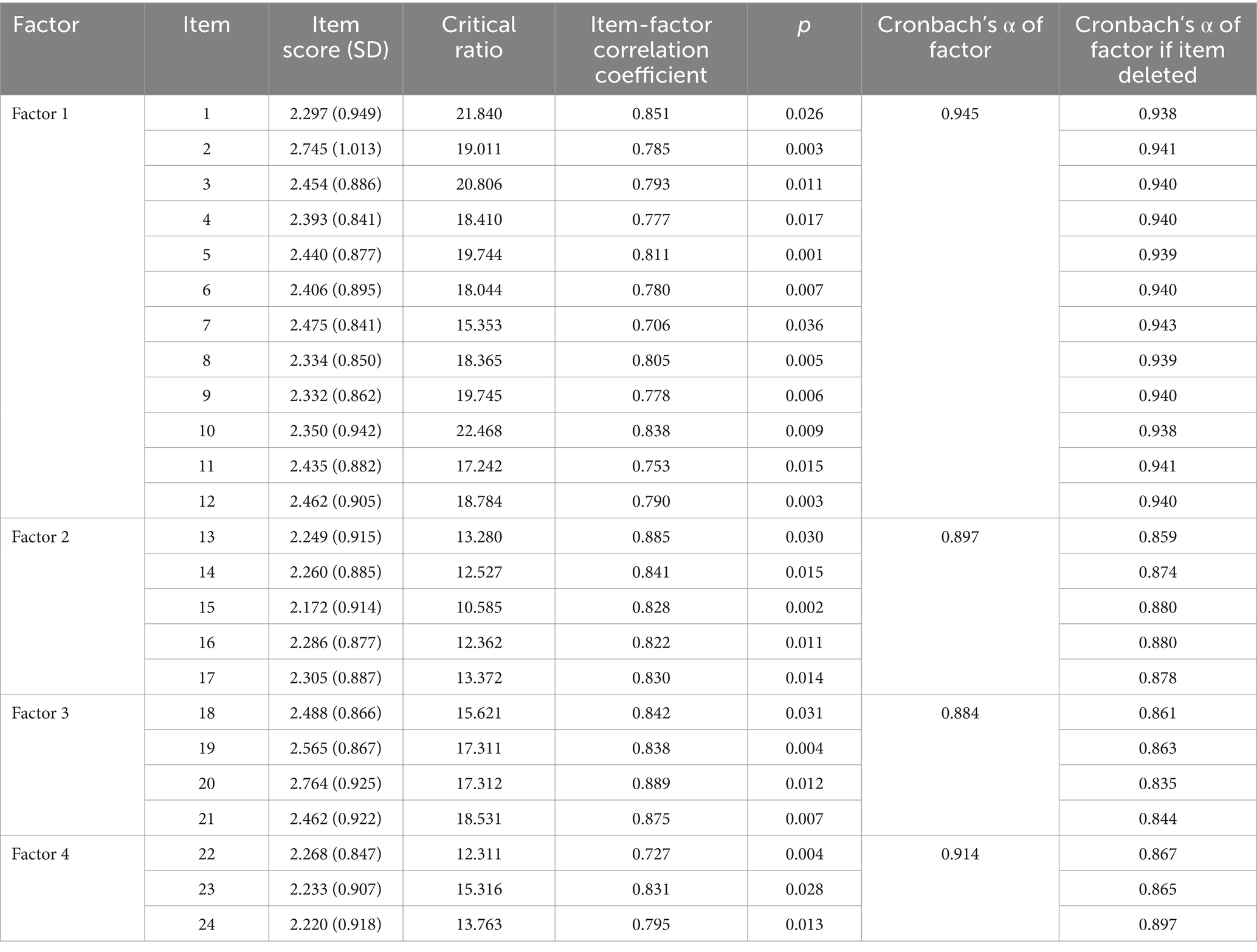
Table 3. Item analysis of the scale.
In this study, a total of seven experts meeting the specified criteria were enlisted to assess the items of the RSP-CC. The results revealed I-CVI values ranging from 0.86 to 1.00, with an S-CVI of 0.97.
The EFA results showed a KMO value of 0.93 and a significant Bartlett’s sphericity test (χ2 = 2785.34, p = 0.004). Four factors were extracted, each comprising a minimum of three items. The factor loadings did not intersect, and all exceeded 0.40. The cumulative variance contribution amounted to 63.58% (> 40%). Refer to Table 4 for detailed information. The results of the CFA indicated favorable model fit indices: χ2/ν = 1.40 (<3); RMSEA = 0.05 (<0.08), RMSEA 90% confidence interval was 0.03–0.06; RMSR = 0.03 (<0.05); CFI = 0.98, TLI = 0.97 and IFI = 0.97. Additional details can be found in Figure 1.
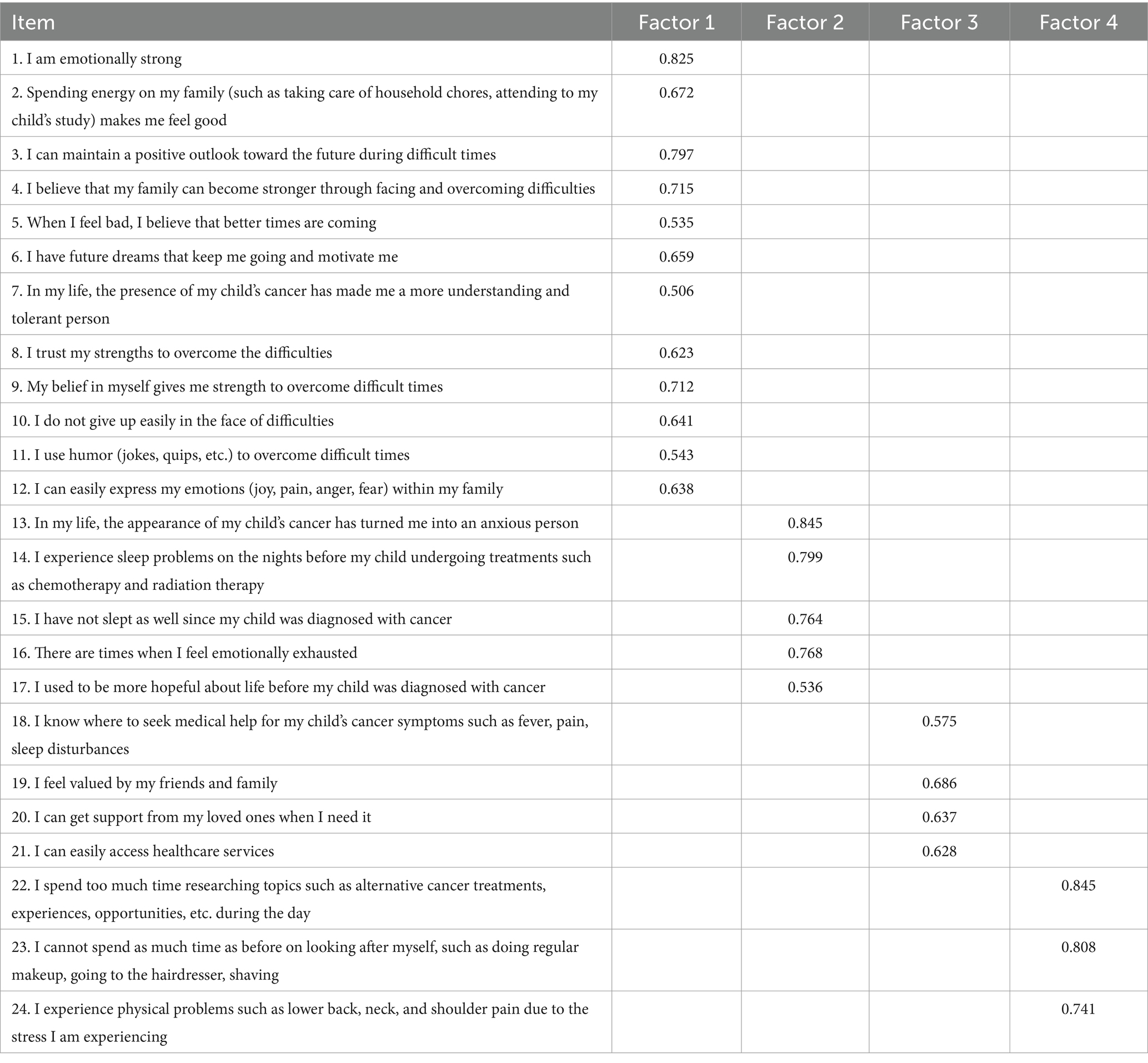
Table 4. Factor loading of each item in the Chinese version of the scale.
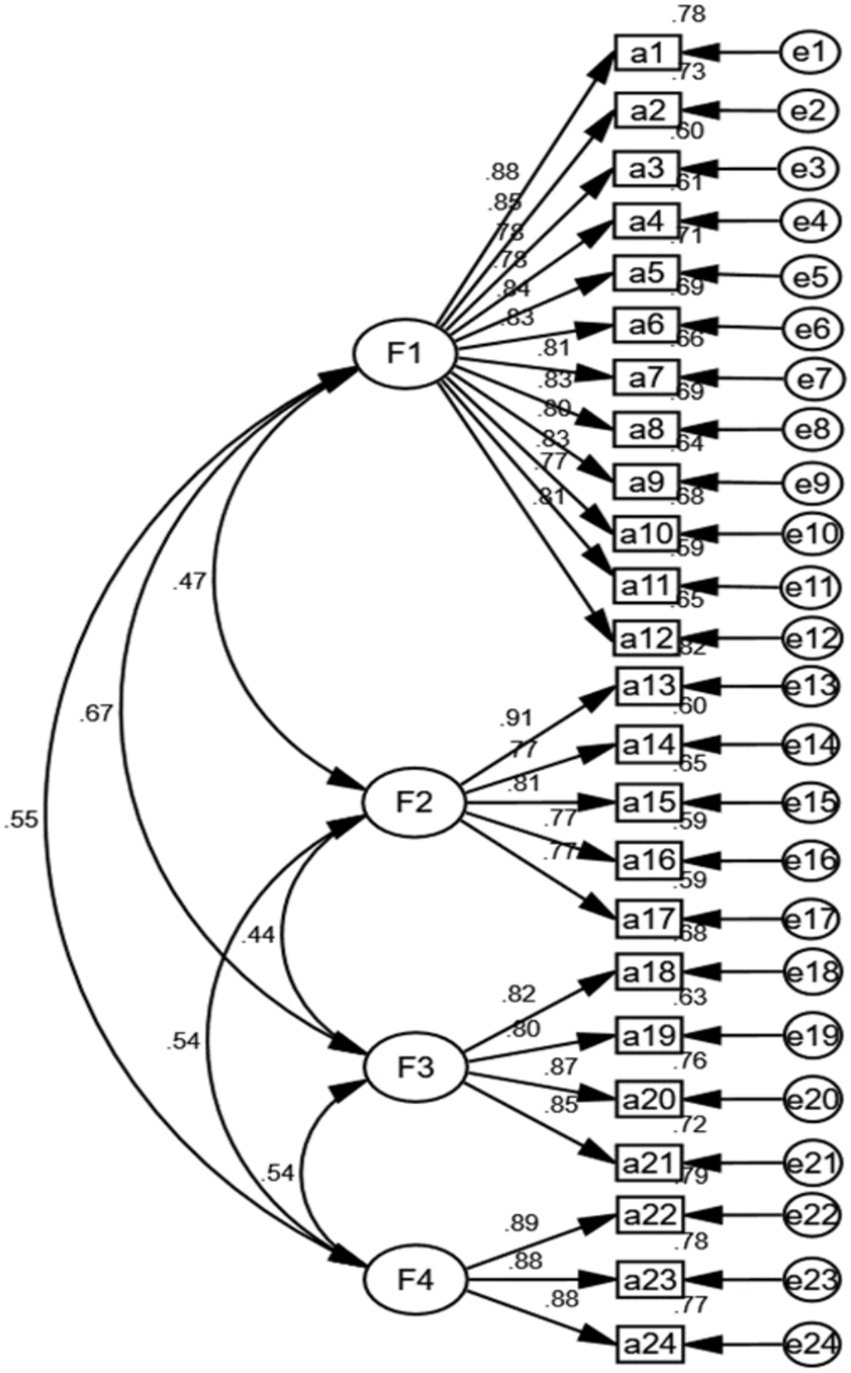
Figure 1. Standardized four-factor model of the.
The AVE values for the four factors ranged from 0.65 to 0.78, and the CR values ranged from 0.90 to 0.96. The square roots of the AVE values ranged from 0.81 to 0.88, all surpassing the correlation coefficients of the relevant components. For more detailed information, please refer to Table 5.
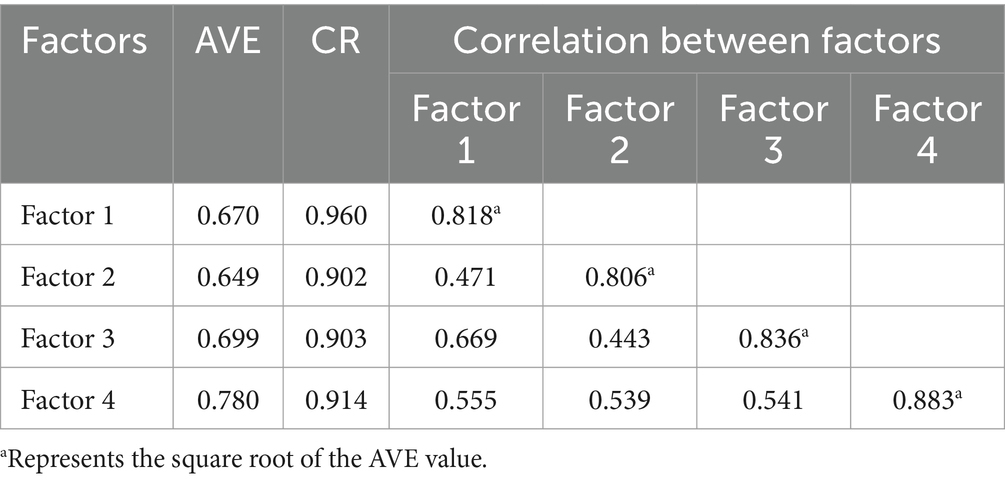
Table 5. Convergent and discriminant validity of the scale.
The results of the reliability analysis indicated that the Cronbach’s α coefficient of the scale was 0.95, with respective coefficients for the four dimensions of 0.95, 0.90, 0.88, and 0.91. The total split-half reliability was 0.82, with corresponding coefficients for the four dimensions of 0.94, 0.90, 0.90, and 0.91. Furthermore, the total retest reliability was 0.95, with coefficients for the four dimensions of 0.93, 0.90, 0.91, and 0.95, respectively.
Compared with family caregivers of children with other common diseases, parents of children with cancer experience greater caregiver burdens and emotional stress (Palacio et al., 2020). The presence of childhood cancer and its accompanying challenges can have significant implications for the physiological and mental health of parents (Shi et al., 2017; Bajjani-Gebara et al., 2019). Resilience, as a defensive strategy, directly impacts an individual’s self-worth, overall contentment, and sense of wellness, aiding in the preservation of both physical and mental health (Merino-Godoy et al., 2022). Studies have indicated that parents with strong resilience exhibit higher levels of hope and employ more proactive coping strategies when confronted with adversity (Rosenberg et al., 2019; Liu et al., 2021). Therefore, resilience training plays a vital role in enhancing parents’ ability to cope with challenges, highlighting the importance of understanding and assessing resilience among parents of children with cancer (Kunzler et al., 2020).
Currently, there remains a need for improved assessment tools to measure the resilience of these parents in China. We expect the introduction of a more dynamic, multidimensional, and tailored instrument to meet these assessment needs. The RSP-CC was developed based on the Resilience Model for Families of Children with Cancer, following an extensive literature review, expert consultation, and pilot study evaluation (Ye et al., 2017). This study was the first to translate the RSP-CC into Chinese and to validate its psychometric properties among these parents. It can serve as a critical tool for clinical staff in formulating specific interventions.
In the items analysis, the critical ratios (t-values) for each item of the scale ranged from 10.59 to 22.47, demonstrating a high level of item differentiation. The correlation coefficients between individual item scores and their corresponding factor scores ranged from 0.71 to 0.89, all exceeding 0.40, indicating extreme homogeneity across the overall scale.
Validity is the degree to which evidence and theory support the interpretations of test scores entailed by proposed uses of tests (AERA, APA, and NCME, 2014). In the original scale, the I-CVI values ranged from 0.88 to 1.00, and the S-CVI was 0.99 (Önal et al., 2023). In this study, the results from expert consultation showed I-CVI values ranging from 0.86 to 1.00, with an S⁃CVI of 0.97. Although these values were slightly lower than those reported for the original scale, they still exceeded the reference standards (I-CVI ≥ 0.78 and S-CVI ≥ 0.90) (Zamanzadeh et al., 2015), indicating good content validity for both versions. Furthermore, EFA extracted a four-factor structure with a cumulative variance contribution of 63.58%, slightly higher than the original scale’s 62.19%. The CFA further confirmed a well-matched four-factor model, indicating satisfactory internal validity. Finally, AVE values for the four factors ranged from 0.65 to 0.78, while CR values ranged from 0.90 to 0.96. The square roots of the AVE values were 0.81 to 0.88, surpassing the relevant components’ correlation coefficients, signifying strong convergent and discriminant validity.
Reliability refers to the ability of an instrument to consistently measure the thing or variable being measured (Koo and Li, 2016). In this study, the Cronbach′s α coefficient and split-half reliabilities for both the overall scale and its dimensions exceeded 0.7, indicating high internal consistency. The retest reliability after 2 weeks was 0.95, with dimensions ranging from 0.90 to 0.95, suggesting better temporal stability for the Chinese version of the RSP-CC.
It is worth noting that there are still certain constraints in this study. First of all, we only examined the content validity and internal structural validity of the scale, omitting investigation into response validity and the construction of criterion validity. In order to further demonstrate the validity of the scale, it is worth considering the addition of more refined validity validation methods. Secondly, predictive validity was not explored, nor was the correlation of the scale’s total score with other potentially relevant measurement variables. Finally, potential biases arising from using the same data source for both exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) were not addressed, potentially introducing method bias and selection bias.
In future studies, it is recommended that researchers in related fields undertake further investigations into the structural validity of the Chinese version of the RSP-CC, and response validity and criterion validity should be incorporated into existing studies to elucidate the significance of the scale scores.
Secondly, exploring correlations between the scale scores and theoretically relevant measurement variables is crucial. For instance, examining predictive relationships between resilience and key variables such as anxiety, depression (van Gils et al., 2022), self-efficacy (Sousa et al., 2023), and coping styles (Koutelekos et al., 2023) could yield valuable insights. An innovative approach could involve exploring the transformation of ordinal scores into linear, equal-interval values using a logistic test model with Rasch methods, thereby demonstrating hierarchical relations among components in the parent caregiver response structure.
Furthermore, to mitigate method bias, future research could provide evidence of known group differences and employ a criterion approach to validity using the obtained parent score distribution. Specifically, researchers should endeavor to establish cross-modal correlations validation studies that validate differences in resilience scores between parents against relevant qualitative markers. These criterion data could be obtained from parent interviews or observer scores. Additionally, consideration of biological and neurological markers is warranted.
Lastly, to address the selection bias resulting from using the same data sources for both exploratory factor analysis (EFA) and confirmatory factor analysis (CFA), future researchers should implement resampling or bootstrapping methods for data collection.
After rigorous translation and verification, the RSP-CC was adapted in China, demonstrating favorable psychometric characteristics. It stands as an effective instrument for parents of children diagnosed with cancer in China. Additionally, this scale could serve as a crucial tool for clinical staff in formulating specific interventions.
The data collected in this investigation can be accessed by contacting the corresponding author upon a reasonable request. Requests to access these datasets should be directed to HC, 1319447367@qq.com.
The studies involving humans were approved by the Ethics Committee of Jinzhou Medical University (Ethics Approval No. JZMULL2023129). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
GZ: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Writing – original draft, Writing – review & editing. ZD: Formal analysis, Investigation, Methodology, Software, Validation, Writing – review & editing. XL: Investigation, Methodology, Supervision, Validation, Writing – review & editing. YQ: Investigation, Methodology, Project administration, Supervision, Validation, Writing – review & editing. XZ: Conceptualization, Formal analysis, Investigation, Methodology, Validation, Writing – review & editing. HC: Formal analysis, Funding acquisition, Methodology, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was funded by the Doctoral Scientific Research Foundation of Wannan Medical College (Grant number: WYRCQD2023043).
The authors extend sincere gratitude to the parents of the children who participated in this study, along with the directors of the nursing department and the invited specialists, for their invaluable assistance. Additionally, we express profound appreciation to Prof. Önal and Prof. Meral Huri for generously providing us with the original materials and granting us permission to use them. We also wish to extend our heartfelt thanks to the reviewers and editors for their insightful comments and suggestions, which significantly enhanced the quality of our manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Adib-Hajbaghery, M., and Ahmadi, B. (2019). Caregiver burden and its associated factors in caregivers of children and adolescents with chronic conditions. Int. J. Commun. Based Nurs. Midwifery 7, 258–269. doi: 10.30476/IJCBNM.2019.73893.0
AERA, APA, and NCME (2014). Standards for educational and psychological testing. Washington, DC: American Psychological Association.
Bajjani-Gebara, J., Hinds, P., Insel, K., Reed, P., Moore, K., and Badger, T. (2019). Well-being, self-transcendence, and resilience of parental caregivers of children in active cancer treatment: where do we go from Here? Cancer Nurs. 42, E41–E52. doi: 10.1097/NCC.0000000000000662
Brislin, R. W. (1970). Back-translation for cross-cultural research. J. Cross-Cult. Psychol. 1, 185–216. doi: 10.1177/135910457000100301
Cayrol, J., Ilbawi, A., Sullivan, M., and Gray, A. (2022). The development and education of a workforce in childhood cancer services in low-and middle-income countries: a scoping review protocol. Syst. Rev. 11:167. doi: 10.1186/s13643-022-02040-0
Chang, Q., Sha, F., Chan, C. H., and Yip, P. S. F. (2018). Validation of an abbreviated version of the Lubben social network scale (“LSNS-6”) and its associations with suicidality among older adults in China. PLoS One 13:e0201612. doi: 10.1371/journal.pone.0201612
Cheng, L., Wu, M., and Yu, L. (2023). Health-related quality of life in Chinese children and adolescents with cancer. Jpn. J. Nurs. Sci. 21:e12564. doi: 10.1111/jjns.12564
Chung, J. O. K., Li, W. H. C., Ho, L. L. K., and Cheung, A. T. (2023). The Association of Resilience with way of coping, psychological well-being and quality of life in parents of children with Cancer. Int. J. Environ. Res. Public Health 20:5765. doi: 10.3390/ijerph20105765
Connor, K. M., and Davidson, J. R. T. (2003). Development of a new resilience scale: the Connor-Davidson resilience scale (CD-RISC). Depress. Anxiety 18, 76–82. doi: 10.1002/da.10113
Da Silva, F. M., Jacob, E., and Nascimento, L. C. (2010). Impact of childhood Cancer on parents’ relationships: an integrative review. J. Nurs. Scholarsh. 42, 250–261. doi: 10.1111/j.1547-5069.2010.01360.x
Fornell, C., and Larcker, D. F. (1981). Structural equation models with unobservable variables and measurement error: algebra and statistics. J. Mark. Res. 18:382. doi: 10.2307/3150980
Guralnick, M. J., Hammond, M. A., Neville, B., and Connor, R. T. (2008). The relationship between sources and functions of social support and dimensions of child-and parent-related stress. J. Intellect. Disabil. Res. 52, 1138–1154. doi: 10.1111/j.1365-2788.2008.01073.x
Güven Baysal, Ş., and Çorabay, S. (2024). Caregiver burden and depression in parents of children with chronic diseases. Turk. Arch. Pediatr. 59, 70–77. doi: 10.5152/TurkArchPediatr.2024.23126
Ji, X., Su, J., Liu, X., Mao, Z., Zhang, W., Zhang, J., et al. (2022). Childhood cancer survivorship in China: an overview of the past two decades. Cancer Med. 11, 4588–4601. doi: 10.1002/cam4.4831
Knapp, T. R., and Sawilowsky, S. S. (2004). Minimizing sample size when using exploratory factor analysis for measurement. J. Nurs. Meas. 12, 95–96; author reply 97-99. doi: 10.1891/jnum.2004.12.2.95
Koo, T. K., and Li, M. Y. (2016). A guideline of selecting and reporting Intraclass correlation coefficients for reliability research. J. Chiropr. Med. 15, 155–163. doi: 10.1016/j.jcm.2016.02.012
Koutelekos, I., Polikandrioti, M., Krokou, P., Dousis, E., Ntafogianni, C., Evagelou, E., et al. (2023). Coping strategies in Greek parents of children with Cancer. Adv. Exp. Med. Biol. 1425, 69–77. doi: 10.1007/978-3-031-31986-0_7
Kunzler, A. M., Helmreich, I., Chmitorz, A., König, J., Binder, H., Wessa, M., et al. (2020). Psychological interventions to foster resilience in healthcare professionals. Cochrane Database Syst. Rev. 2020:CD012527. doi: 10.1002/14651858.CD012527.pub2
Lasmarías, C., Subirana-Casacuberta, M., Mancho, N., and Aradilla-Herrero, A. (2021). Spanish cross-cultural adaptation and psychometric properties of the advance care planning self-efficacy: a cross-sectional study. J. Palliat. Med. 24, 1807–1815. doi: 10.1089/jpm.2020.0653
Law, E., Fisher, E., Eccleston, C., and Palermo, T. M. (2019). Psychological interventions for parents of children and adolescents with chronic illness. Cochrane Database Syst. Rev. 2021:CD009660. doi: 10.1002/14651858.CD009660.pub4
Liu, Q., Petrini, M. A., Luo, D., Yang, B. X., Yang, J., and Haase, J. E. (2021). Parents’ experiences of having a young child with acute lymphoblastic leukemia in China. J. Pediatr. Oncol. Nurs. 38, 94–104. doi: 10.1177/1043454220975463
Lubega, J., Kimutai, R. L., and Chintagumpala, M. M. (2021). Global health disparities in childhood cancers. Curr. Opin. Pediatr. 33, 33–39. doi: 10.1097/MOP.0000000000000984
Luo, Y. H., Li, W. H. C., Cheung, A. T., Ho, L. L. K., Xia, W., He, X. L., et al. (2022). Relationships between resilience and quality of life in parents of children with cancer. J. Health Psychol. 27, 1048–1056. doi: 10.1177/1359105321990806
Merino-Godoy, M. Á., Yot-Domínguez, C., Conde-Jiménez, J., Ramírez Martín, P., and Lunar-Valle, P. M. (2022). The influence of emotional burnout and resilience on the psychological distress of nursing students during the COVID-19 pandemic. Int. J. Ment. Health Nurs. 31, 1457–1466. doi: 10.1111/inm.13046
Mohammadsalehi, N., Asgarian, A., Ghasemi, M., and Mohammadbeigi, A. (2022). Cancer resilience in parents of children with cancer; the role of general health and self-efficacy on resiliency. J. Can. Res. Ther. 18:1119. doi: 10.4103/jcrt.JCRT_464_19
Ni, X., Li, Z., Li, X., Zhang, X., Bai, G., Liu, Y., et al. (2022). Socioeconomic inequalities in cancer incidence and access to health services among children and adolescents in China: a cross-sectional study. Lancet 400, 1020–1032. doi: 10.1016/S0140-6736(22)01541-0
Önal, G., Huri, M., Karakükçü, M., and Demir, H. A. (2023). The resilience scale for parents of children with Cancer: scale development and psychometric evaluation. Psychooncology 32, 951–960. doi: 10.1002/pon.6137
Palacio, G. C., Krikorian, A., Gómez-Romero, M. J., and Limonero, J. T. (2020). Resilience in caregivers: a systematic review. Am. J. Hosp. Palliat. Care 37, 648–658. doi: 10.1177/1049909119893977
Patterson, J. M. (2002). Understanding family resilience. J. Clin. Psychol. 58, 233–246. doi: 10.1002/jclp.10019
Raykov, T., and Marcoulides, G. A. (2016). On the relationship between classical test theory and item response theory: from one to the other and Back. Educ. Psychol. Meas. 76, 325–338. doi: 10.1177/0013164415576958
Rosenberg, A. R., Bradford, M. C., Junkins, C. C., Taylor, M., Zhou, C., Sherr, N., et al. (2019). Effect of the promoting resilience in stress management intervention for parents of children with Cancer (PRISM-P): a randomized clinical trial. JAMA Netw. Open 2:e1911578. doi: 10.1001/jamanetworkopen.2019.11578
Schreiber, J. B. (2021). Issues and recommendations for exploratory factor analysis and principal component analysis. Res. Social Adm. Pharm. 17, 1004–1011. doi: 10.1016/j.sapharm.2020.07.027
Shi, D., DiStefano, C., Maydeu-Olivares, A., and Lee, T. (2022). Evaluating SEM model fit with small degrees of freedom. Multivariate Behav. Res. 57, 179–207. doi: 10.1080/00273171.2020.1868965
Shi, L., Gao, Y., Zhao, J., Cai, R., Zhang, P., Hu, Y., et al. (2017). Prevalence and predictors of posttraumatic stress symptoms in parents of children with ongoing treatment for cancer in South China: a multi-centered cross-sectional study. Support Care Cancer 25, 1159–1167. doi: 10.1007/s00520-016-3506-6
Sousa, L. R. M., Leoni, P. H. T., De Carvalho, R. A. G., Ventura, C. A. A., De Silva, A. C., Reis, R. K., et al. (2023). Resilience, depression and self-efficacy among Brazilian nursing professionals during the COVID-19 pandemic. Ciênc. Saúde Colet. 28, 2941–2950. doi: 10.1590/1413-812320232810.09852023
Sung, H., Ferlay, J., Siegel, R. L., Laversanne, M., Soerjomataram, I., Jemal, A., et al. (2021). Global Cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 71, 209–249. doi: 10.3322/caac.21660
Tobias, S., and Carlson, J. E. (1969). Brief report: BARTLETT’S test of SPHERICITY and chance findings in factor analysis. Multivariate Behav. Res. 4, 375–377. doi: 10.1207/s15327906mbr0403_8
van Gils, Y., Dom, G., Dierckx, E., Van Alphen, S. P. J., and Franck, E. (2022). Resilience, depression and anxiety and hazardous alcohol use behaviour among community dwelling older adults. Aging Ment. Health 26, 56–64. doi: 10.1080/13607863.2020.1870211
Van Schoors, M., Caes, L., Verhofstadt, L. L., Goubert, L., and Alderfer, M. A. (2015). Systematic review: family resilience after pediatric Cancer diagnosis. J. Pediatr. Psychol. 40, 856–868. doi: 10.1093/jpepsy/jsv055
Ye, Z. J., Qiu, H. Z., Li, P. F., Liang, M. Z., Wang, S. N., and Quan, X. M. (2017). Resilience model for parents of children with cancer in mainland China-an exploratory study. Eur. J. Oncol. Nurs. 27, 9–16. doi: 10.1016/j.ejon.2017.01.002
Keywords: childhood cancer, parents, resilience, reliability, validity, psychometric properties
Citation: Zhong G, Ding Z, Li X, Qiao Y, Zhang X and Cui H (2024) Psychometric evaluation of the Chinese version of the resilience scale for parents of children with cancer. Front. Psychol. 15:1378639. doi: 10.3389/fpsyg.2024.1378639
Edited by:
Laura Badenes-Ribera, University of Valencia, SpainReviewed by:
Nikolaus Bezruczko, The Chicago School of Professional Psychology, United StatesCopyright © 2024 Zhong, Ding, Li, Qiao, Zhang and Cui. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Huixia Cui, 1319447367@qq.com
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.