 Ainoa García-Fernández1,2,3
Ainoa García-Fernández1,2,3 Clara Martínez-Cao1,2,3
Clara Martínez-Cao1,2,3 Alberto Sánchez-Fernández-Quejo4*
Alberto Sánchez-Fernández-Quejo4* Teresa Bobes-Bascarán2,3,5,6
Teresa Bobes-Bascarán2,3,5,6 Jorge Andreo-Jover7,8
Jorge Andreo-Jover7,8 Wala Ayad-Ahmed9Ana Isabel Cebriá10,11,12Marina Díaz-Marsá4,9,10
Wala Ayad-Ahmed9Ana Isabel Cebriá10,11,12Marina Díaz-Marsá4,9,10 Nathalia Garrido-Torres10,13,14,15
Nathalia Garrido-Torres10,13,14,15 Sandra Gómez10,16,17,18
Sandra Gómez10,16,17,18 Ana González-Pinto10,19,20,21
Ana González-Pinto10,19,20,21 Iria Grande10,16,17,18
Iria Grande10,16,17,18 Noelia Iglesias22Katya B. March7,8Diego J. Palao10,11,23Iván Pérez-Díez10,24
Noelia Iglesias22Katya B. March7,8Diego J. Palao10,11,23Iván Pérez-Díez10,24 Natalia Roberto10,16,17,18Miguel Ruiz-Veguilla10,13,14,15
Natalia Roberto10,16,17,18Miguel Ruiz-Veguilla10,13,14,15 Alejandro de la Torre-Luque4,10Iñaki Zorrilla10,19,20,21Víctor Pérez25,26,27SURVIVE Group
Alejandro de la Torre-Luque4,10Iñaki Zorrilla10,19,20,21Víctor Pérez25,26,27SURVIVE Group Pilar A. Sáiz1,2,3,5,10†María Paz García-Portilla1,2,3,5,10†
Pilar A. Sáiz1,2,3,5,10†María Paz García-Portilla1,2,3,5,10†- 1Department of Psychiatry, Universidad de Oviedo, Oviedo, Spain
- 2Instituto de Investigación Sanitaria del Principado de Asturias (ISPA), Oviedo, Spain
- 3Instituto Universitario de Neurociencias del Principado de Asturias (INEUROPA), Oviedo, Spain
- 4Department of Legal Medicine, Psychiatry, and Pathology, Universidad Complutense de Madrid (UCM), Madrid, Spain
- 5Servicio de Salud del Principado de Asturias (SESPA), Oviedo, Spain
- 6Department of Psychology, Universidad de Oviedo, Oviedo, Spain
- 7Hospital La Paz Institute for Health Research (IdiPAZ), Madrid, Spain
- 8Department of Psychiatry, Universidad Autónoma de Madrid (UAM), Madrid, Spain
- 9Hospital Clínico San Carlos, Madrid, Spain
- 10CIBER de Salud Mental, Instituto de Salud Carlos III, Madrid, Spain
- 11Mental Health Service, Hospital Universitari Parc Taulí, Unitat Mixta de Neurociència Traslacional (I3PT-INc-UAB), Sabadell, Barcelona, Spain
- 12Department of Clinical and Health Psychology, Faculty of Psychology, Universitat Autònoma de Barcelona, Cerdanyola del Vallès, Spain
- 13Institute of Biomedicine of Seville (IBiS), Sevilla, Spain
- 14Hospital Virgen del Rocío, Sevilla, Spain
- 15Department of Psychiatry, University of Seville, Sevilla, Spain
- 16Departament de Medicina, Facultat de Medicina i Ciències de la Salut, Institut de Neurociències, Universitat de Barcelona (UB), Barcelona, Spain
- 17Bipolar and Depressive Disorders Unit, Hospìtal Clinic de Barcelona, Barcelona, Spain
- 18Institut d’Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Barcelona, Spain
- 19Department Psychiatry, UPV/EHU, Vitoria, Spain
- 20BIOARABA, Vitoria, Spain
- 21Hospital Universitario de Alava, Vitoria, Spain
- 22Department of Psychiatry, Clinical Psychology and Mental Health, La Paz University Hospital, Madrid, Spain
- 23Department of Psychiatry and Forensic Medicine, Faculty of Medicine, Universitat Autònoma de Barcelona, Cerdanyola del Vallès, Spain
- 24Department of Psychiatry, Universidad Autónoma de Madrid (UAM), Madrid, Spain
- 25Institute of Neuropsychiatry and Addictions, Hospital del Mar, Barcelona, Spain
- 26Department of Psychiatry and Forensic Medicine, Autonomous University of Barcelona, Barcelona, Spain
- 27Hospital del Mar Medical Research Institute, Barcelona, Spain
Background: Child maltreatment is associated with a higher probability of mental disorders and suicidal behavior in adolescence. Therefore, accurate psychometric instruments are essential to assess this.
Objective: To validate the Spanish version of the Childhood Trauma Questionnaire-Short Form (CTQ-SF) in adolescents with suicide attempts.
Methods: Multisite cohort study of 208 adolescents with suicide attempts using data from the following scales: Mini International Neuropsychiatric Interview (MINI), Columbia Suicide Severity Rating Scale (C-SSRS), Patient Health Questionnaire (PHQ-9), and CTQ-SF. Statistical analysis: CTQ-SF scores analyzed by descriptive statistics. Internal consistency: McDonald’s omega and Cronbach’s alpha. Concurrent validity with PHQ-9 and C-SSRS scores: Spearman correlation coefficient. Structural validity: Confirmatory factor analysis.
Results: Floor and ceiling effects: Physical abuse and neglect as well as sexual abuse demonstrated high floor effects (50.0, 35.1, and 61.1% of adolescents, respectively). No ceiling effects were found. The CTQ-SF had excellent internal consistency (McDonald’s omega = 0.94), as did the majority of its subscales (Cronbach’s alpha 0.925–0.831) except for physical neglect (0.624). Its concurrent validity was modest, and the emotional neglect subscale had the lowest Spearman correlation coefficients (0.067–0.244). Confirmatory factor analysis: Compared with alternative factor structures, the original CTQ-SF model (correlated 5-factor) exhibited a better fit [S-B χ2 = 676.653, p < 0; RMSEA (90% CI = 0.076–0.097) = 0.087; SRMR = 0.078; CFI = 0.980; TLI = 0.978].
Conclusion: The Spanish CTQ-SF is a reliable, valid instrument for assessing traumatic experiences in adolescents at high risk of suicide. It appears appropriate for use in routine clinical practice to monitor maltreatment in this group.
1 Introduction
Child maltreatment encompasses all forms of physical and emotional ill-treatment, sexual abuse, neglect, and exploitation that result in actual or potential harm to the child’s health, development, or dignity (World Health Organization, 2022). Exposure to such traumatic experiences in childhood may affect proper neurobiological, cognitive, and affective development in these individuals (Pérez-Balaguer et al., 2022). This unfortunate reality makes them part of a vulnerable group, increasing their susceptibility to developing psychosocial problems if they are not adequately protected (Georgieva et al., 2021). Additionally, childhood maltreatment is linked to a variety of mental disorders as well as an increase in suicide attempts (Chen et al., 2021). Except for emotional neglect, all childhood maltreatment subtypes are associated with non-suicidal self-injury (NSSI) (Liu et al., 2018). Therefore, accurate detection and evaluation of these experiences is essential to understanding and preventing the negative consequences that can arise as a result of exposure to traumatic situations.
Among the available instruments for the retrospective assessment of childhood maltreatment, the Childhood Trauma Questionnaire-Short Form (CTQ-SF) is one of the most widely used and validated instruments to measure and assess traumatic experiences during childhood and adolescence (Saini et al., 2019; Georgieva et al., 2021). Originally developed from an initial 70-item version by Bernstein et al. (1994) and Bernstein and Fink (1998), this self-report questionnaire measures several types of traumatic experiences quantitatively. Furthermore, Bernstein et al. (1997) replicated their previous results in the adolescent psychiatric population and provided initial support for the validity of the CTQ in this population as well. Five years later, Bernstein et al. (2003) developed a short form of the CTQ (the CTQ-SF), providing a briefer approach to measuring trauma. Additionally, it is supported by strong evidence and has been translated into multiple languages and applied across diverse populations worldwide (Saini et al., 2019; Malan-Muller et al., 2022). Some investigators, such as Hernandez et al. (2013), have referred to it as the “gold standard” for the assessment of maltreatment in childhood. The evidence for the CTQ-SF factorial structure is controversial. While several research groups confirmed the standard 5-factor structure of the CTQ-SF (Dovran et al., 2013; Karos et al., 2014; Charak et al., 2017; Sacchi et al., 2018; He et al., 2019; Petrikova et al., 2021), others supported it only partially or suggested alternative models to the original structure (Gerdner and Allgulander, 2009; Kim et al., 2011; Grassi-Oliveira et al., 2014; Kongerslev et al., 2019; Aloba et al., 2020; Behn et al., 2020). Remarkably, the physical neglect subscale is problematic in these studies. Given these inconclusive research results, further efforts to examine its factor structure are essential.
CTQ-SF internal consistency was good, ranging from 0.79 to 0.94, and comparable across previously published studies (Gerdner and Allgulander, 2009; Kim et al., 2011; He et al., 2019; Kongerslev et al., 2019; Petrikova et al., 2021). Again, the physical neglect subscale had the poorest internal consistency of all five scales in most studies. Moreover, some studies also tested and demonstrated measurement invariance based on sex (Charak et al., 2017; He et al., 2019; Aloba et al., 2020), age (Grassi-Oliveira et al., 2014) and population type, e.g., substance abuse, inmate, psychiatric, and adolescent samples (Dovran et al., 2013).
Hernandez et al. (2013) conducted an initial validation of the Spanish version of the CTQ-SF in an adult female clinical sample (mean age 41.6 years) undergoing psychiatric outpatient (48%) or inpatient treatment. They demonstrated adequate psychometric properties and a good fit of the 5-factor structure, replicating the original study’s findings. As in the CTQ-SF English version, the physical neglect scale showed the lowest internal consistency and factor loadings. However, no studies have used this questionnaire to examine childhood maltreatment in the Spanish adolescent population at high risk of suicide and the relation of these adverse experiences with suicidal behaviors. Therefore, this study aims to validate the Spanish version of the self-reported CTQ-SF and assess its psychometric properties, including reliability, validity, and factorial structure, in a clinical sample of adolescents with suicide attempts.
2 Materials and methods
2.1 Participants
In all, 208 adolescents who had completed the Spanish version of the CTQ-SF (Hernandez et al., 2013) were included in the study. All patients were recruited at the psychiatric emergence department from seven University Hospitals across Spain: Hospital Clinic (n = 49) and Corporació Sanitària Parc Taulí (n = 38) in Barcelona; Hospital Clínico San Carlos (n = 18) and Hospital Universitario La Paz (n = 49) in Madrid; Hospital Universitario Central de Asturias (n = 34) in Oviedo; Hospital Universitario Araba-Santiago (n = 19) in Vitoria, and Hospital Universitario Virgen del Rocío (n = 1) in Seville. Inclusion criteria were: (1) females or males, (2) between 12 and 18 years old, (3) informed consent of the patient who made the suicide attempt, (4) informed consent of their parents or legal guardians, and (5) undergoing outpatient care (Psychiatrist and/or Clinical Psychologist) in the Child and Youth Mental Health Centers or Child and Youth Day Hospital. Exclusion criteria were: (1) incapacity to give informed consent, (2) lack of fluency in Spanish, and (3) currently participating in another clinical study likely to interfere with this study.
2.2 Instruments
Trained psychologists assessed the participants within 10 days following the adolescents’ admission to the emergency department due to a suicide attempt. The assessment included an ad hoc questionnaire for collecting socio-demographic (age, sex, current academic year) and clinical data (psychiatric diagnosis, depressive symptoms and medical treatment). The Spanish versions of the following instruments were also used: the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID; Sheehan et al., 2010) to assess the presence of psychiatric diagnosis in children and adolescents, and the Columbia Suicide Severity Scale (C-SSRS) (Posner et al., 2011; Al-Halabí et al., 2016) to assess the suicide risk severity.
In addition, the adolescents completed the following self-report scales: Patient Health Questionnaire (PHQ-9) (Diez-Quevedo et al., 2001; Kroenke et al., 2001) to assess depressive symptoms and CTQ-SF.
The CTQ-SF is an instrument designed to explore childhood abuse history. It consists of 28 items, of which 25 are grouped into five subscales: emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect. The remaining items constitute a validity scale (items 10, 16, and 22). Each item is rated on a 5-point Likert-type scale from 1 (never) to 5 (almost always). Some of the items are written in reverse (shown in Table 1 as item number followed by “R”), so those must be recoded before calculating the scores (5 = 1 and 1 = 5). There is a total score and independent scores for the five subscales. Therefore, the total score ranges from 25 to 125 and the subscale scores from 5 to 25. According to the original manual, the cut-off values of the CTQ-SF subscales classify severity into four levels, from “none” to “extreme” (Bernstein et al., 2003).
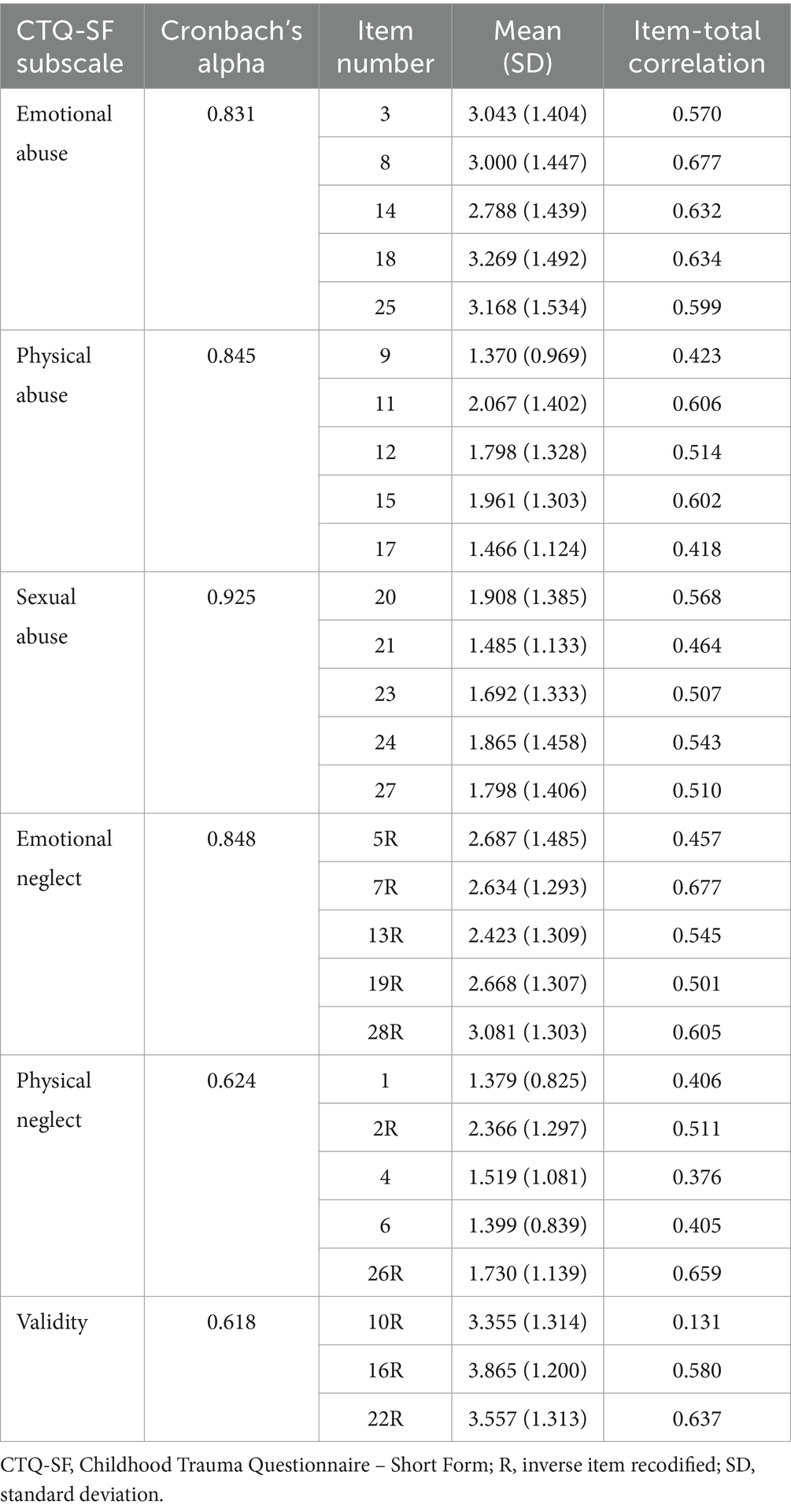
Table 1. Reliability characteristics of CTQ-SF subscales.
2.3 Procedure
This secondary analysis for validating a self-assessment instrument for childhood trauma is part of a larger nationwide project called SURVIVE (Survive Prevention and Intervention: cohort study and nested randomized controlled trials of secondary prevention programs for suicide attempts). The SURVIVE project, described in detail by Pérez et al. (2023), encompasses a multi-site cohort study conducted by several research groups across Spain. The recruitment period was from January 2021 to March 2023.
Participants were recruited from psychiatric emergency departments due to a suicide attempt in the 10 days prior to evaluation. All eligible participants were invited to complete an assessment administered by trained psychologists. Both participants and their parents were required to be willing and able to comply with the study procedures and to provide informed consent.
It was approved by the Clinical Research Ethics Committee at each of the participating sites [Hospital Clinic, IDIBAPS (PI19/000954), Hospital Universitario Parc Taulí (PI19/01484), Hospital Clínico San Carlos (PI19/01256), La Paz Institute for Health Research (PI19/00941), Hospital Universitario Central de Asturias (HUCA) (IP19/01027), Hospital Universitario Araba-Santiago (PI19/00569), and Hospital Universitario Virgen del Rocío (PI19/00685)]. It follows national and international guidelines: the latest version of the World Medical Association (2013), developed as ethical principles for medical research involving human subjects, and the International Council for Harmonization (ICH) Good Clinical Practice Guideline, GCP Directive 2005/28/EC. This study also complies with current Spanish legislation: Organic Law 3/2018 of December 5 on the Protection of Personal Data and Guarantee of Digital Rights and Regulation (EU) 2016/679 of the European Parliament and of the Council, version of April 27, 2016, known as the General Data Protection Regulation (GDPR). All participants and their parents or legal guardians gave their written informed consent before enrolment.
2.4 Data analysis
The statistical analysis was done using SPSS 27.0 and the software R (version 4.2.1). All tests were two-tailed and the significance level was set at 0.05.
To measure the shape of the distributions, skewness (asymmetry) and kurtosis (peakedness or flatness) were computed. Values of ±1 were considered good. The coefficient of variation (standard deviation/mean) and ceiling and floor effects were also determined [floor and ceiling effects were calculated for each subscale, and the widely used 15% threshold was adopted for patients achieving the highest and lowest scores (Terwee et al., 2007)]. All data were checked for normal distribution with the Kolmogorov–Smirnov test. The data did not meet the normality assumption; thus, non-parametric statistical methods were used for the analyses.
Regarding validity, we assessed concurrent and structural validities. The criterion validity could not be evaluated since no established gold standard is available for comparison with the instrument under evaluation.
An exploratory factor analysis and a principal component analysis was performed in addition, which can be found in the Supplementary material.
Structural validity of the CTQ-SF was tested using confirmatory factor analysis (CFA) with the following packages: psych (Revelle, 2023) and lavaan (Rosseel, 2012).
Given the inconclusive results for the factor structure of the CTQ-SF reported by Sacchi et al. (2018), three competitive factor models were tested: a unifactorial model, a correlated 5-factor model, and an uncorrelated 5-factor model. Prior to the CFA, the 3 validity items (10, 16, 22) were excluded. To evaluate the fit of these models, the weighted least squares (WLS) estimation method was used, as the items were ordinal Likert scale and non-normally distributed data. For these CFA models, factor loadings were freely estimated, the factor variances were fixed to 1, and correlations between factors were allowed. The model fit was evaluated with the Satorra-Bentler Scaled Chi-Square test (S-B χ2) and associated degrees of freedom (df). A good fit is indicated by non-significant S-B χ2 values and χ2/df coefficients lower than 2 (Newcomb, 1994). Since the S-B χ2 test is susceptible to sample size, robust versions of fit indices were used to evaluate the different models, including the Comparative Fit Index (CFI), Tucker-Lewis Index (TLI), the root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR). According to Hooper et al. (2008), appropriate criteria for these indices are as follows: RMSEA <0.08, CFI > 0.95, SRMR <0.08, and TLI > 0.95.
Concurrent validity was examined using the Spearman’s Rho correlation coefficient between the CTQ-SF subscale scores and the PHQ-9 total score as well as the following items of the C-SSRS: number of NSSI and number of suicide attempts (total, interrupted, and aborted attempts).
Concerning reliability, the internal consistency of the overall CTQ-SF was measured using MacDonald’s omega value (ω), which was more appropriate for multidimensional scales (Crutzen and Peters, 2017). Additionally, Cronbach’s alpha coefficients were calculated to evaluate the internal consistency of each subscale.
3 Results
3.1 Sample
A total of 208 adolescents with suicide attempts were included. The mean age was 15.03 (SD = 1.49), and 87.0% were female. Table 2 shows the demographic and clinical characteristics of the adolescents.
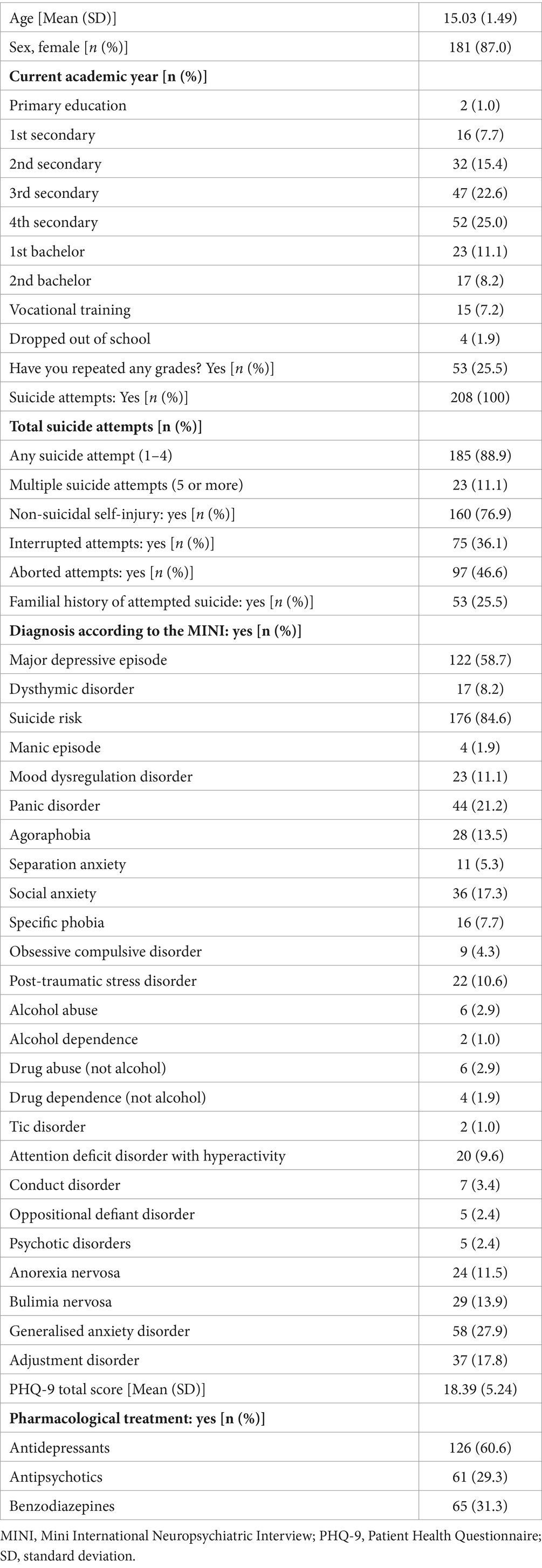
Table 2. Demographic and clinical characteristics.
3.2 Psychometric properties of the CTQ-SF
3.2.1 Distribution characteristics and descriptive statistics of CTQ-SF scores
The distribution characteristics of the CTQ-SF are shown in Table 3. In all cases, the mean scores exhibit no normality of distribution (Kolmogorov–Smirnov test <0.05). Only two subscales (emotional abuse and emotional neglect) show symmetrical distributions and platykurtic kurtosis, with more scattered values and fewer data in the central region. The other three subscales show an asymmetric distribution, with values >1, and a more concentrated data distribution around the mean. The physical abuse and neglect subscales and the sexual abuse subscale demonstrate a striking floor effect (50.0, 35.1, and 61.1% of adolescents, respectively). On the contrary, none of the subscales show a ceiling effect (values between 0.0 and 9.1% of adolescents).
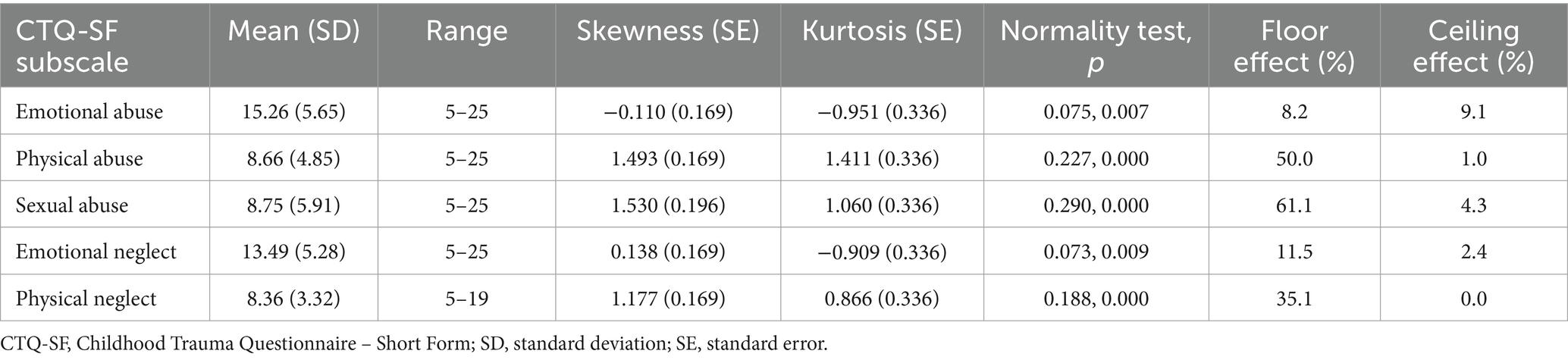
Table 3. Descriptive analysis of CTQ-SF subscale scores.
3.2.2 CTQ-SF validity
3.2.2.1 Structural validity
Results of the CFA show that the classic correlated 5-factor model provides a good fit with the observed data [S-B χ2 = 676.653, p < 0; RMSEA (90% CI: 0.076–0.097) = 0.087; SRMR = 0.078; CFI = 0.980; TLI = 0.978]. Although the χ2 statistic is significant and the χ2/df ratio is above 2, these outcomes might be influenced by the limited sample size (Kenny and McCoach, 2003). On the contrary, the other 2-factor solutions resulted in unsatisfactory models, suggesting that modifications of the original 5-factor structure were not necessary (see Table 4).

Table 4. Fit indices for CTQ-SF models.
All items had factor loadings higher than 0.6 with the exception of items 4 and 6 (0.589 and 0.578, respectively) (see Table 5). Therefore, the results of this analysis support an underlying structure of five components in this sample (Figure 1). On the other hand, as expected, these five components are intercorrelated, with correlation coefficients ranging from 0.857 between emotional neglect and physical neglect to 0.346 between emotional neglect and sexual abuse (see Supplementary Table S2).

Table 5. Standardized factor loadings for CTQ-SF based on confirmatory factor analysis.
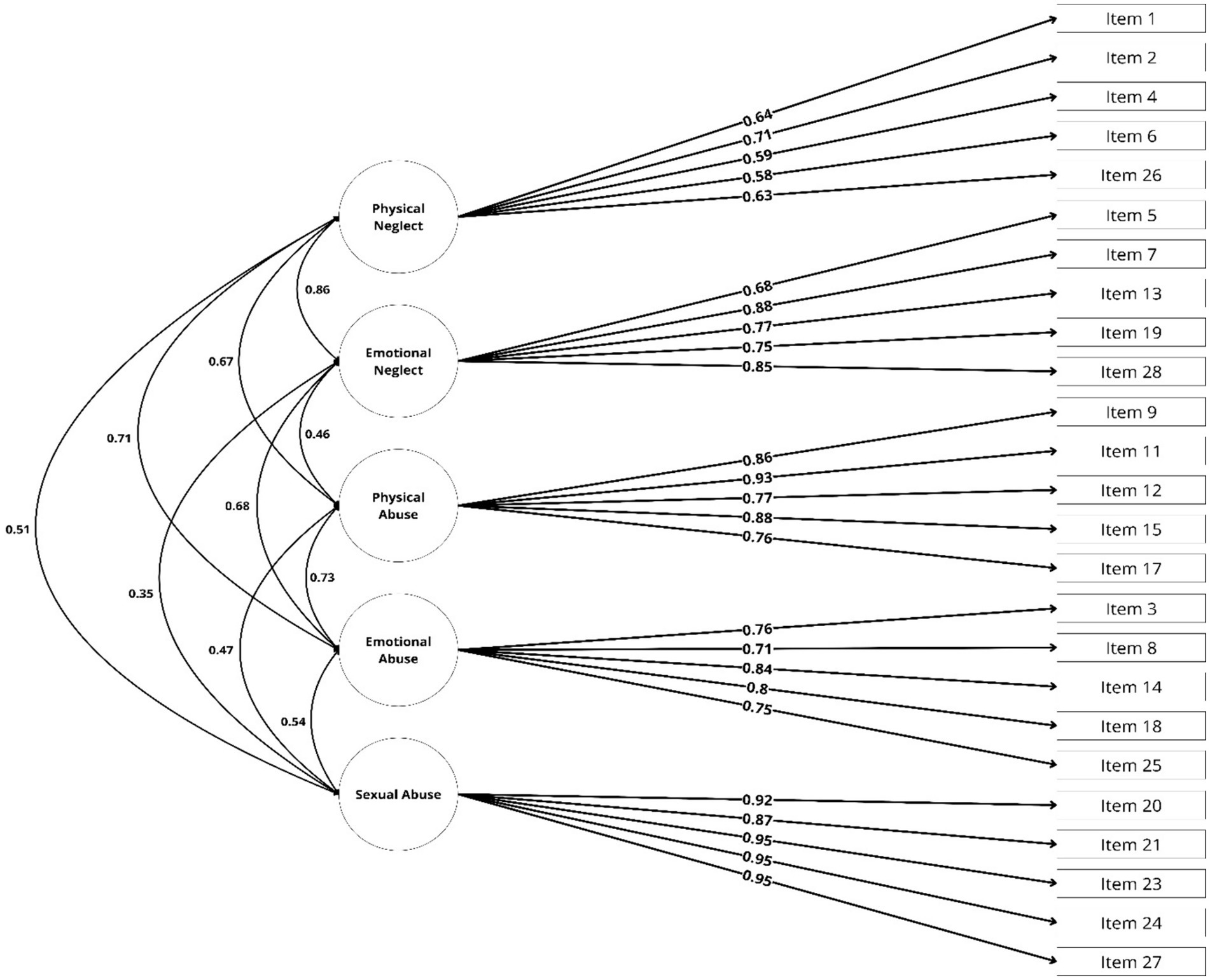
Figure 1. Confirmatory factor analysis of the original structure of CTQ-SF with items distributed into five standard subscales. CTQ-SF, Childhood Trauma Questionnaire – Short Form.
3.2.2.2 Concurrent validity
Table 6 shows the correlation coefficients between the original five CTQ-SF subscale scores with the PHQ-9 total score and the C-SSRS items: number of NSSI and number of suicide attempts (total, interrupted, and aborted attempts). Additionally, we are showing the correlation coefficients using our new CTQ-SF subscales. As seen in Table 6, depression scores and the number of suicide attempts significantly correlate with almost all types of maltreatment. In contrast, the number of self-injuries and the subtypes of suicidal behaviors correlate with the CTQ-SF subscales to a lesser extent.
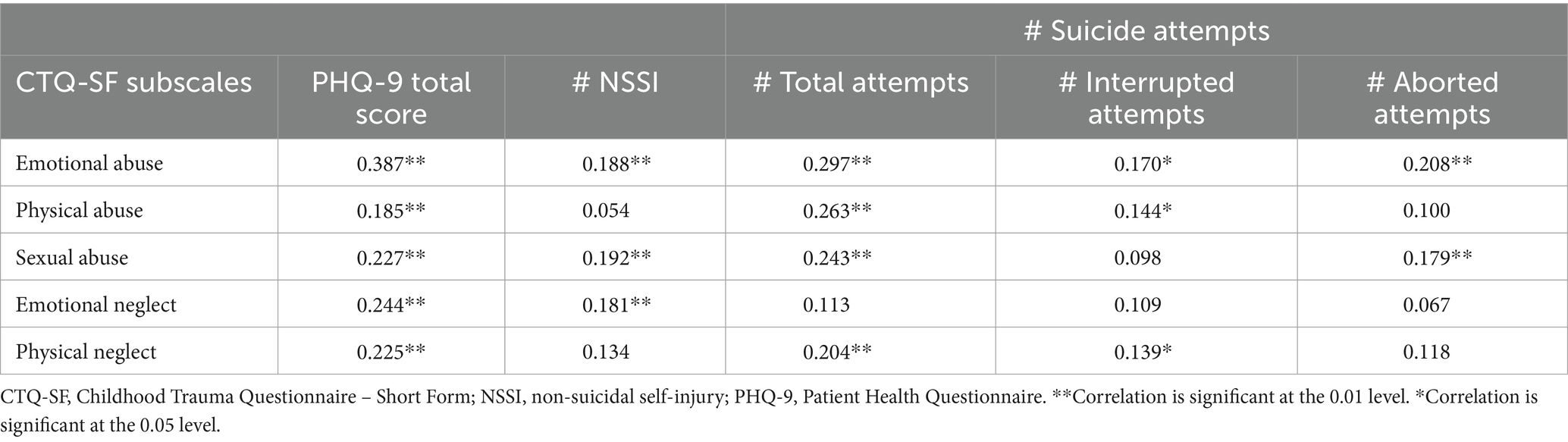
Table 6. Correlations among CTQ-SF subscales and other measures.
3.2.3 CTQ-SF reliability
The CTQ-SF scale demonstrates excellent internal consistency in adolescents with suicide attempts, with a total Omega of (ωT) = 0.94. On the other hand, all subscales showed good internal consistency, except for physical neglect and the validity items where it is moderate (Cronbach’s alpha of 0.624 and 0.618, respectively) (see Table 1). All but item 10R has corrected item-total correlation values >0.3, ranging from 0.376 (item 4) to 0.677 (items 7R and 8) (see Table 1).
4 Discussion
This study investigated the psychometric properties of the Spanish version of the CTQ-SF in Spanish adolescents who made at least one suicide attempt. The results confirm that this version has acceptable psychometric properties.
Regarding the descriptive analysis of its subscale scores, the distribution on three subscales (physical abuse and neglect subscales and sexual abuse subscale) is positively skewed, meaning that higher values are scattered on the right-hand side of the distribution. It should be noted that none of the subscales presented a ceiling effect; however, physical abuse and neglect and sexual abuse showed an enormous floor effect, so the discriminative capacity of these items is limited in that range. Moreover, we found that emotional abuse and emotional neglect were the most common types of traumatization reported by our adolescents, while physical neglect had the lowest occurrence. In other words, almost 70% (n = 140) of our sample reported a history of moderate to extreme emotional abuse. This proportion is nearly 50% (n = 71) for emotional neglect. In contrast, physical neglect had a higher proportion of participants at lower severity levels (none to minimal). These same results were previously obtained in a similar cultural environment (Reus, Spain) but in an adult female clinical sample (Hernandez et al., 2013).
We explored both the classic and alternative structures of the CTQ-SF in a sample of Spanish adolescents. In comparison with competitive factor models, the classic CTQ-SF model exhibited the best fit to the data, and the original 5-factor model showed reasonable fit (Bernstein et al., 1997).
Additionally, our confirmatory factor analysis results indicated adequate loadings of all items. However, the items belonging to the physical neglect subscale obtained the lowest values. As observed in previous validation studies, the physical neglect subscale has been the most controversial of the instrument. According to Grassi-Oliveira et al. (2014), neglect is a challenging construct to operationalize, as most definitions rely on personal perceptions of a lack of care. More specifically, child rearing practices exhibit considerable variations across cultures. Consequently, it is crucial to investigate whether the interpretation of the items differs among cultures (Grassi-Oliveira et al., 2014) and varies depending on the language spoken.
The directions of the correlations between the CTQ-SF and other study instruments were modest in magnitude but consistent with the expected patterns, confirming its concurrent validity and usefulness as a clinical tool to assess the impact of different types of child maltreatment. Compatible with previous evidence (Aloba et al., 2020), all types of child maltreatment were correlated with the severity of depressive symptoms. This highlights the direct relationship between adverse childhood experiences and the development of mental health problems throughout life, particularly depressive symptoms (Grossberg and Rice, 2023). Additionally, four of the five subscales of the CTQ-SF positively correlated with total suicide attempts. This finding suggests that different types of child maltreatment have a substantial impact on the risk of suicidal behaviors, emphasizing the need to identify and support individuals with a history of child maltreatment to prevent tragic outcomes. Emotional neglect was the sole subscale not associated with any suicidal events (interrupted, aborted, or suicide attempts), but significantly correlated with NSSI. In contrast, emotional abuse was the sole subscale significantly correlated with all suicidal behaviors and with NSSI. The fact that emotional neglect is not associated with suicide attempts but is associated with NSSI suggests that different types of maltreatment may have different effects on mental health outcomes. On the other hand, emotional abuse shows a strong correlation with both suicidal behaviors and NSSI, indicating that this type of mistreatment may have a more profound impact on mental health. Taken together, child maltreatment significantly contributes to increasing the risk of suicide (Duprey et al., 2023), and specifically, the various forms of traumatic experiences could differentially affect different suicidal behaviors.
Finally, the internal consistency of the overall scale was excellent; all the inter-item correlations (except item 10, which belongs to the validity subscale) had values >0.3. Four of the five subscales obtained alpha values >0.8. However, the physical neglect factor had an alpha below 0.7, reflecting moderate internal homogeneity as reported in previous studies (Gerdner and Allgulander, 2009; Kim et al., 2011; Hernandez et al., 2013; Grassi-Oliveira et al., 2014; Karos et al., 2014; Charak et al., 2017; He et al., 2019; Behn et al., 2020; Petrikova et al., 2021). The most robust internal consistency was found for the sexual abuse subscale, in accordance with the existing literature (Gerdner and Allgulander, 2009; Dovran et al., 2013; Hernandez et al., 2013; Charak et al., 2017; Sacchi et al., 2018; Kongerslev et al., 2019; Behn et al., 2020; Petrikova et al., 2021).
A primary strength of this study lies in its clinical significance and immediate practical relevance. Our research emphasizes how the CTQ-SF can play a vital role in clinical settings, aiding in the identification and understanding of childhood maltreatment among adolescents with suicide attempts. “Another strong aspect of this study is the representativeness of our sample, as the patients were recruited in seven different regions of Spain, comprising most of the national territory. Furthermore, the non-restrictive inclusion and exclusion criteria allowed the inclusion of patients with diverse clinical and demographic characteristics.” However, subsequent studies could be performed in different populations to further increase the validity and utility of the CTQ-SF. Some limitations should be taken into consideration. Firstly, the present study does not provide information about the convergent validity of the Spanish CTQ-SF. However, we did not find a suitable option available in Spanish to assess convergent validity. Second, child maltreatment explored through a self-report questionnaire was not contrasted with other objective evidence (such as pediatric or legal reports), leading to the possibility of participant memory and response bias. Third, a notable limitation of this study is the significant sex imbalance within the participant sample, with 87.0% of the adolescents being female. While this sex distribution may align with the specific context of the study population, the overrepresentation of females limits the extent to which the study’s results can be applied to a more sex-balanced population. Furthermore, although the sample size is representative, it is only fair for confirmatory factor analysis.
In conclusion, the Spanish version of the CTQ-SF is reliable and valid for measuring traumatic experiences in Spanish adolescents with at least one suicide attempt. As a self-reported instrument, it appears suitable for identifying childhood maltreatment in this population in routine clinical practice. Such identification can benefit patients and clinicians when making treatment plans, including assessment, treatment alternatives, and prognosis. Moreover, it is a feasible option as it does not require much time to administer, and the information obtained should be considered complementary to the clinician’s point of view.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Clinical Research Ethics Committee at each of the participating sites [Hospital Clinic, IDIBAPS (PI19/000954), Hospital Universitario Parc Taulí (PI19/01484), Hospital Clínico San Carlos (PI19/01256), La Paz Institute for Health Research (PI19/00941), Hospital Universitario Central de Asturias (HUCA) (PI19/01027) (PI23/01277). Hospital Universitario Araba-Santiago (PI19/00569), and Hospital Universitario Virgen del Rocío (PI19/00685)]. It follows national and international guidelines: the latest version of the World Medical Association (2013), developed as ethical principles for medical research involving human subjects, and the International Council for Harmonization (ICH) Good Clinical Practice Guideline, GCP Directive 2005/28/EC. This study also complies with current Spanish legislation: Organic Law 3/2018 of December 5 on the Protection of Personal Data and Guarantee of Digital Rights and Regulation (EU) 2016/679 of the European Parliament and of the Council, version of April 27, 2016, known as the General Data Protection Regulation (GDPR). All participants and their parents or legal guardians gave their written informed consent before enrolment. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
AG-F: Conceptualization, Methodology, Visualization, Writing – original draft, Writing – review & editing. CM-C: Formal analysis, Methodology, Writing – review & editing. AS-F-Q: Data curation, Formal analysis, Methodology, Software, Visualization, Writing – original draft, Writing – review & editing. TB-B: Supervision, Writing – review & editing. JA-J: Visualization, Writing – review & editing. WA-A: Visualization, Writing – review & editing. AC: Visualization, Writing – review & editing. MD-M: Visualization, Writing – review & editing. NG-T: Visualization, Writing – review & editing. SG: Visualization, Writing – review & editing. AG-P: Visualization, Writing – review & editing. IG: Visualization, Writing – review & editing. NI: Visualization, Writing – review & editing. KM: Visualization, Writing – review & editing. DP: Visualization, Writing – review & editing. IP-D: Visualization, Writing – review & editing. NR: Visualization, Writing – review & editing. MR-V: Visualization, Writing – review & editing. AT-L: Visualization, Writing – review & editing. IZ: Visualization, Writing – review & editing. VP: Visualization, Writing – review & editing. PS: Conceptualization, Supervision, Visualization, Writing – review & editing. MPG-P: Conceptualization, Formal analysis, Methodology, Validation, Visualization, Writing – review & editing.
SURVIVE Group members
Íñigo Alberdi-Páramo, Margarita Alcami, Lorenzo Bracco, Maria Fe Bravo-Ortiz, Manuel Canal Rivero, Laura Comendador, Benedicto Crespo-Facorro, Cristina Diaz, Fernando Corbalán, Jennifer Fernández-Fernández, Eduardo Fernández-Jiménez, Veronica Fernandez-Rodrigues, Adriana Garcia-Ramos, Luis Jiménez-Treviño, Elvira Lara, Itziar Leal-Leturia, Maria Purificación Lopez-Peña, Lorea Mar-Barrutia, Julen Marin, Pablo Mola, Marta Navas, Luis Olivares, Angela Palao-Tarrero, Joaquín Punti, Pablo Reguera, Julia Rider, Carlamarina Rodríguez-Pereira, Maria Dolores Saiz Gónzalez, Yolanda Sanchez-Carro, Elisa Seijo-Zazo, Mireia Vázquez, Emma Vidal Bermejo, Eduard Vieta.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was supported by the Spanish Ministry of Science and Innovation (MCIN) (PI19/01027, PI19/00236, PI19/00569, PI19/00685, PI19/00941, PI19/00954, PI19/01027, PI19/01256, PI19/01484, PI20/00229, PI23/01277) integrated into the Plan Nacional de I + D + I and co-financed by the ISCIII-Subdirección General de Evaluación and co-financed by the European Union (FEDER, FSE, Next Generation EU/Plan de Recuperación Transformación y Resiliencia_PRTR), the Instituto de Salud Carlos III, the Government of the Principality of Asturias PCTI-2021-2023 IDI/2021/111, the Fundación para la Investigación e Innovación Biosanitaria del Principado de Asturias (FINBA), and Centro de Investigación Biomédica en Red de Salud Mental (CIBERSAM). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript. AG-F thanks Instituto de Salud Carlos III for its PFIS grant (FI20/00318), and CM-C also thanks the Ministry of Science, Innovation and Universities for its FPU grant (FPU19/01231). IG thanks the following for their support: the Spanish Ministry of Science and Innovation (MCIN) (PI19/00954) integrated into the Plan Nacional de I + D + I and co-financed by the ISCIII-Subdirección General de Evaluación and co-financed by the European Union (FEDER, FSE, Next Generation EU/Plan de Recuperación Transformación y Resiliencia_PRTR); the Instituto de Salud Carlos III; the CIBER of Mental Health (CIBERSAM); and the Secretaria d’Universitats i Recerca del Departament d’Economia i Coneixement (2021 SGR 01358), CERCA Program/Generalitat de Catalunya as well as the Fundació Clínic per la Recerca Biomèdica (Pons Bartran 2022-FRCB_PB1_2022). AG-P thanks the Instituto de Salud Carlos III for its support, cofinanced by the European Union (FEDER, FSE, Next Generation EU/Plan de Recuperación Transformación y Resiliencia_PRTR) (PI21/00713), and the Basque Government (2022111054).
Acknowledgments
The authors wish to thank Sharon Grevet for her English assistance.
Conflict of interest
IG has received grants and served as consultant, advisor or CME speaker for the following entities: ADAMED, Angelini, Casen Recordati, Esteve, Ferrer, Gedeon Richter, Janssen Cilag, Lundbeck, Lundbeck-Otsuka, Luye, SEI Healthcare, and Viatris outside the submitted work. She also receives royalties from Oxford University Press, Elsevier, and Editorial Médica Panamericana. EV has received grants and served as consultant, advisor, or CME speaker for the following entities: AB-Biotics, AbbVie, Angelini, Biogen, Biohaven, Boehringer-Ingelheim, Celon Pharma, Compass, Dainippon Sumitomo Pharma, Ethypha Gedeon Richter, GH Research, Glaxo- Smith Kline, Idorsia, Janssen, Lundbeck, Medincell, Novartis, Orion Corporation, Organon, Otsuka, Rovi, Sage, Sanofi-Aventis, Sunovion, Takeda, and Viatris outside the submitted work. AG-P has received grants and served as consultant, advisor or CME speaker for the following entities: Janssen-Cilag, Lundbeck, Otsuka, Alter, Angelini, Novartis, Rovi, Takeda, the Spanish Ministry of Science and Innovation (CIBERSAM), the Ministry of Science (Carlos III Institute), the Basque Government, and the European Framework Program of Research. IZ has received grants and served as consultant, advisor or CME speaker for the following entities: Janssen-Cilag, Lundbeck, Otsuka, Angelini, Rovi and Takeda. MPG-P has been a consultant to and/or has received honoraria/grants from Alter, Angelini, Cassen-Recordati, Janssen- Cilag, Idorsia, Lundbeck, Otsuka, Rovi, and SAGE Therapeutics. PS has been a consultant to and/or has received honoraria or grants from Adamed, Alter Medica, Angelini Pharma, CIBERSAM, Ethypharm Digital Therapy, European Commission, Government of the Principality of Asturias, Instituto de Salud Carlos III, Johnson & Johnson, Lundbeck, Otsuka, Pfizer, Plan Nacional Sobre Drogas, and Servier.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2024.1378486/full#supplementary-material
References
Al-Halabí, S., Sáiz, P. A., Burón, P., Garrido, M., Benabarre, A., Jiménez, E., et al. (2016). Validation of a Spanish version of the Columbia-suicide severity rating scale (C-SSRS). Spanish J. Psychiatry Ment. Health 9, 134–142. doi: 10.1016/j.rpsm.2016.02.002
Aloba, O., Opakunle, T., and Ogunrinu, O. (2020). Childhood trauma questionnaire-short form (CTQ-SF): dimensionality, validity, reliability and gender invariance among Nigerian adolescents. Child Abuse Negl. 101:104357. doi: 10.1016/j.chiabu.2020.104357
Behn, A., Vöhringer, P. A., Martínez, P., Domínguez, A. P., González, A., Carrasco, M. I., et al. (2020). Validation of the childhood trauma questionnaire-short form in Chile. Rev. Med. Chile 148, 336–343. doi: 10.4067/S0034-98872020000300336
Bernstein, D. P., Ahluvalia, T., Pogge, D., and Handelsman, L. (1997). Validity of the childhood trauma questionnaire in an adolescent psychiatric population. J. Am. Acad. Child Adolesc. Psychiatry 36, 340–348. doi: 10.1097/00004583-199703000-00012
Bernstein, D. P., and Fink, L. (1998). Childhood Trauma Questionnaire: A Retrospective Self-Report. Manual. Orlando: Psychological Corporation.
Bernstein, D. P., Fink, L., Handelsman, L., Foote, J., Lovejoy, M., Wenzel, K., et al. (1994). Initial reliability and validity of a new retrospective measure of child abuse and neglect. Am. J. Psychiatry 151, 1132–1136. doi: 10.1176/ajp.151.8.1132
Bernstein, D. P., Stein, J. A., Newcomb, M. D., Walker, E., Pogge, D., Ahluvalia, T., et al. (2003). Development and validation of a brief screening version of the childhood trauma questionnaire. Child Abuse Negl. 27, 169–190. doi: 10.1016/S0145-2134(02)00541-0
Charak, R., de Jong, J. T. V. M., Berckmoes, L. H., Ndayisaba, H., and Reis, R. (2017). Assessing the factor structure of the childhood trauma questionnaire, and cumulative effect of abuse and neglect on mental health among adolescents in conflict-affected Burundi. Child Abuse Negl. 72, 383–392. doi: 10.1016/j.chiabu.2017.09.009
Chen, H., Li, W., Cao, X., Liu, P., Liu, J., Chen, X., et al. (2021). The association between suicide attempts, anxiety, and childhood maltreatment among adolescents and young adults with first depressive episodes. Front. Psych. 12:745470. doi: 10.3389/fpsyt.2021.745470
Crutzen, R., and Peters, G. Y. (2017). Scale quality: alpha is an inadequate estimate and factor-analytic evidence is needed first of all. Health Psychol. Rev. 11, 242–247. doi: 10.1080/17437199.2015.1124240
Diez-Quevedo, C., Rangil, T., Sanchez-Planell, L., Kroenke, K., and Spitzer, R. L. (2001). Validation and utility of the patient health questionnaire in diagnosing mental disorders in 1003 general hospital Spanish inpatients. Psychosom. Med. 63, 679–686. doi: 10.1097/00006842-200107000-00021
Dovran, A., Winje, D., Overland, S. N., Breivik, K., Arefjord, K., Dalsbø, A. S., et al. (2013). Psychometric properties of the Norwegian version of the childhood trauma questionnaire in high-risk groups. Scand. J. Psychol. 54, 286–291. doi: 10.1111/sjop.12052
Duprey, E. B., Handley, E. D., Wyman, P. A., Ross, A. J., Cerulli, C., and Oshri, A. (2023). Child maltreatment and youth suicide risk: a developmental conceptual model and implications for suicide prevention. Dev. Psychopathol. 35, 1732–1755. doi: 10.1017/S0954579422000414
Georgieva, S., Tomas, J. M., and Navarro-Pérez, J. J. (2021). Systematic review and critical appraisal of childhood trauma questionnaire - short form (CTQ-SF). Child Abuse Negl. 120:105223. doi: 10.1016/j.chiabu.2021.105223
Gerdner, A., and Allgulander, C. (2009). Psychometric properties of the Swedish version of the childhood trauma questionnaire-short form (CTQ-SF). Nord. J. Psychiatry 63, 160–170. doi: 10.1080/08039480802514366
Grassi-Oliveira, R., Cogo-Moreira, H., Salum, G. A., Brietzke, E., Viola, T. W., Manfro, G. G., et al. (2014). Childhood trauma questionnaire (CTQ) in Brazilian samples of different age groups: findings from confirmatory factor analysis. PLoS One 9:e87118. doi: 10.1371/journal.pone.0087118
Grossberg, A., and Rice, T. (2023). Depression and suicidal behavior in adolescents. Med. Clin. North Am. 107, 169–182. doi: 10.1016/j.mcna.2022.04.005
He, J., Zhong, X., Gao, Y., Xiong, G., and Yao, S. (2019). Psychometric properties of the Chinese version of the childhood trauma questionnaire-short form (CTQ-SF) among undergraduates and depressive patients. Child Abuse Neglec 91, 102–108. doi: 10.1016/j.chiabu.2019.03.009
Hernandez, A., Gallardo-Pujol, D., Pereda, N., Arntz, A., Bernstein, D. P., Gaviria, A. M., et al. (2013). Initial validation of the Spanish childhood trauma questionnaire-short form: factor structure, reliability and association with parenting. J. Interpers. Violence 28, 1498–1518. doi: 10.1177/0886260512468240
Hooper, D., Coughlan, J., and Mullen, M. R. (2008). Structural equation modelling: guidelines for determining model fit. Electron. J. Bus. Res. Methods 6, 53–60.
Karos, K., Niederstrasser, N., Abidi, L., Bernstein, D. P., and Bader, K. (2014). Factor structure, reliability, and known groups validity of the German version of the childhood trauma questionnaire (short-form) in Swiss patients and nonpatients. J. Child Sex. Abus. 23, 418–430. doi: 10.1080/10538712.2014.896840
Kenny, D. A., and McCoach, D. B. (2003). Effect of the number of variables on measures of fit in structural equation Modeling. Struct. Equ. Model. 10, 333–351. doi: 10.1207/S15328007SEM1003_1
Kim, D., Park, S. C., Yang, H., and Oh, D. H. (2011). Reliability and validity of the Korean version of the childhood trauma questionnaire-short form for psychiatric outpatients. Psychiatry Investig. 8, 305–311. doi: 10.4306/pi.2011.8.4.305
Kongerslev, M. T., Bach, B., Rossi, G., Trauelsen, A. M., Ladegaard, N., Løkkegaard, S. S., et al. (2019). Psychometric validation of the childhood trauma questionnaire-short form (CTQ-SF) in a Danish clinical sample. Child Abuse Negl. 94:104026. doi: 10.1016/j.chiabu.2019.104026
Kroenke, K., Spitzer, R. L., and Williams, J. B. (2001). The PHQ-9: validity of a brief depression severity measure. J. Gen. Intern. Med. 16, 606–613. doi: 10.1046/j.1525-1497.2001.016009606.x
Liu, R. T., Scopelliti, K. M., Pittman, S. K., and Zamora, A. S. (2018). Childhood maltreatment and non-suicidal self-injury: a systematic review and meta-analysis. Lancet Psychiatry 5, 51–64. doi: 10.1016/S2215-0366(17)30469-8
Malan-Muller, S., Valles-Colomer, M., Foxx, C. L., Vieira-Silva, S., van den Heuvel, L. L., Raes, J., et al. (2022). Exploring the relationship between the gut microbiome and mental health outcomes in a posttraumatic stress disorder cohort relative to trauma-exposed controls. Eur. Neuropsychopharmacol. 56, 24–38. doi: 10.1016/j.euroneuro.2021.11.009
Newcomb, M. D. (1994). Drug use and intimate relationships among women and men: separating specific from general effects in prospective data using structural equation models. J. Consult. Clin. Psychol. 62, 463–476. doi: 10.1037/0022-006X.62.3.463
Pérez, V., Elices, M., Toll, A., Bobes, J., López-Solà, C., Díaz-Marsá, M., et al. (2023). The suicide prevention and intervention study (SURVIVE): study protocol for a multisite cohort study with nested randomized-controlled trials. Spanish J. Psychiatry Ment. Health 16, 16–23. doi: 10.1016/j.rpsm.2020.11.004
Pérez-Balaguer, A., Peñuelas-Calvo, I., Alacreu-Crespo, A., Baca-García, E., and Porras-Segovia, A. (2022). Impulsivity as a mediator between childhood maltreatment and suicidal behavior: a systematic review and meta-analysis. J. Psychiatr. Res. 151, 95–107. doi: 10.1016/j.jpsychires.2022.04.021
Petrikova, M., Kascakova, N., Furstova, J., Hasto, J., and Tavel, P. (2021). Validation and adaptation of the Slovak version of the childhood trauma questionnaire (CTQ). Int. J. Environ. Res. Public Health 18:2440. doi: 10.3390/ijerph18052440
Posner, K., Brown, G. K., Stanley, B., Brent, D. A., Yershova, K. V., Oquendo, M. A., et al. (2011). The Columbia-suicide severity rating scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am. J. Psychiatry 168, 1266–1277. doi: 10.1176/appi.ajp.2011.10111704
Revelle, W. (2023). Psych: Procedures for Psychological, Psychometric, and Personality Research. Evanston, Illinois: Northwestern University.
Rosseel, Y. (2012). Lavaan: an R package for structural equation Modeling. J. Stat. Softw. 48, 1–36. doi: 10.18637/jss.v048.i02
Sacchi, C., Vieno, A., and Simonelli, A. (2018). Italian validation of the childhood trauma questionnaire-short form on a college group. Psychol. Trauma 10, 563–571. doi: 10.1037/tra0000333
Saini, S. M., Hoffmann, C. R., Pantelis, C., Everall, I. P., and Bousman, C. A. (2019). Systematic review and critical appraisal of child abuse measurement instruments. Psychiatry Res. 272, 106–113. doi: 10.1016/j.psychres.2018.12.068
Sheehan, D. V., Sheehan, K. H., Shytle, R. D., Amorim, P., Janavs, J., Weiller, E., et al. (2010). Reliability and validity of the Mini international neuropsychiatric interview for children and adolescents (MINI-KID). J. Clin. Psychiatry 71, 313–326. doi: 10.4088/JCP.09m05305whi
Terwee, C. B., Bot, S. D., de Boer, M. R., van der Windt, D. A., Knol, D. L., Dekker, J., et al. (2007). Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 60, 34–42. doi: 10.1016/j.jclinepi.2006.03.012
World Medical Association . (2013). World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 310, 2191–4. doi: 10.1001/jama.2013.281053
World Health Organization . Child Maltreat. (2022). Available at: https://www.who.int/es/news-room/fact-sheets/detail/child-maltreatment (acessed May 30, 2023).
Keywords: CTQ-SF, reliability, validity, suicide attempt, adolescent
Citation: García-Fernández A, Martínez-Cao C, Sánchez-Fernández-Quejo A, Bobes-Bascarán T, Andreo-Jover J, Ayad-Ahmed W, Cebriá AI, Díaz-Marsá M, Garrido-Torres N, Gómez S, González-Pinto A, Grande I, Iglesias N, March KB, Palao DJ, Pérez-Díez I, Roberto N, Ruiz-Veguilla M, de la Torre-Luque A, Zorrilla I, Pérez V, SURVIVE Group, Sáiz PA and García-Portilla MP (2024) Validation of the Spanish Childhood Trauma Questionnaire-Short Form in adolescents with suicide attempts. Front. Psychol. 15:1378486. doi: 10.3389/fpsyg.2024.1378486
Edited by:
Augustine Osman, University of Texas at San Antonio, United StatesReviewed by:
Ana Fresan, Instituto Nacional de Psiquiatría Ramón de la Fuente Muñíz, MexicoWoojae Myung, Seoul National University Bundang Hospital, Republic of Korea
Copyright © 2024 García-Fernández, Martínez-Cao, Sánchez-Fernández-Quejo, Bobes-Bascarán, Andreo-Jover, Ayad-Ahmed, Cebriá, Díaz-Marsá, Garrido-Torres, Gómez, González-Pinto, Grande, Iglesias, March, Palao, Pérez-Díez, Roberto, Ruiz-Veguilla, de la Torre-Luque, Zorrilla, Pérez, SURVIVE Group, Sáiz and García-Portilla. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alberto Sánchez-Fernández-Quejo, YWxic2FuMjdAdWNtLmVz
†These authors have contributed equally to this work and share last authorship