
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol. , 08 October 2021
Sec. Quantitative Psychology and Measurement
Volume 12 - 2021 | https://doi.org/10.3389/fpsyg.2021.701208
 Amaia Yurrebaso Macho1*
Amaia Yurrebaso Macho1* Alexander L. Ward Mayens1Eva Ma Picado Valverde1Raquel Guzmán Ordaz1Juan Antonio Juanes Méndez1Jose Luis Pérez Iglesias1José Antonio Mirón Canelo1Maria do Rosário Pinto2Alcinda Maria do Sacramento Costa Reis2Joaquim Augusto Simões2Ana Luísa Torres1Marja Silén-Lipponen3Ulla Korhonen3Leena Koponen3Mikko Myllymäki3Aleksandra Jankowiak-Bernaciak4Amelia Patrzała4Grażyna Bączyk4Anna Basa4Paulo Santos Costa5Beatriz Serambeque5Anabela Salgueiro Oliveira5João Pardal5João Manuel Garcia do Nascimento Graveto5Pedro Parreira5
Alexander L. Ward Mayens1Eva Ma Picado Valverde1Raquel Guzmán Ordaz1Juan Antonio Juanes Méndez1Jose Luis Pérez Iglesias1José Antonio Mirón Canelo1Maria do Rosário Pinto2Alcinda Maria do Sacramento Costa Reis2Joaquim Augusto Simões2Ana Luísa Torres1Marja Silén-Lipponen3Ulla Korhonen3Leena Koponen3Mikko Myllymäki3Aleksandra Jankowiak-Bernaciak4Amelia Patrzała4Grażyna Bączyk4Anna Basa4Paulo Santos Costa5Beatriz Serambeque5Anabela Salgueiro Oliveira5João Pardal5João Manuel Garcia do Nascimento Graveto5Pedro Parreira5Healthcare-associated infections are one of the major concerns worldwide. This study presents the development and the validation process of the InovSafeCare scale and aimed at identifying and measuring the ecosystem variables related to healthcare-associated infection (HCAI) prevention and control practices in European nurse students. Qualitative and quantitative approaches were used to (1) elaborate an item pool related to the educational environment, the healthcare setting environment, and the attitudes, beliefs, and performance of the nursing students regarding HCAI prevention and control and (2) analyze psychometric properties of the scale using factor analysis. The validated InovSafeCare scale was applied to undergraduate nursing students of five European Higher Education Institutions. The partial least square structural equation modeling (PLS-SEM) method with SMART-PLS3 software was used. The study sample consists of 657 nursing students, who responded a self-report inventory. From the analyzed data were identified 14 factors. The InovSafeCare scale reveals good validity and reliability of the dimensions in different European countries.
Healthcare-associated infections (HCAIs) are a major concern worldwide, not only because it prolongs hospital stay, with the consequent increased costs for health systems, but also because of the repercussions on the health of patients (European Center for Disease Prevention Control (ECDPC), 2020; World Health Organization, 2020).
In Europe, about 4 million patients acquire an HCAI every year, of which 37,000 end up in deaths [European Center for Disease Prevention Control (ECDPC), 2020]. The ECDPC estimates that around 30% of HCAIs can be prevented with surveillance systems, and prevention and hygiene control programs (2020), meaning they become an indisputable preventive content in healthcare institutions for their different professionals, as well as academic content necessary for all healthcare students [Díaz and Cadena, 2003; Agencia Nacional de Evaluación de la Calidad y Acreditación (ANECA), 2004].
Brosio et al. (2017) study showed that nursing students demonstrate an insufficient knowledge about HCAIs (Brosio et al., 2017). Additionally, nursing students are active practitioners in healthcare institutions, being exposed to a high risk of acquiring infections due to the type of tasks they perform, the direct contact with potentially infectious patients, and the handling of blood and body fluids (Díaz and Cadena, 2003; Rodríguez et al., 2008; Rubio et al., 2008). Despite the previous preparation obtained in laboratory practice and a simulation environment, the perception of risks of infection, attitudes, and motivations toward safe practices and prevention itself through the use of personal protective equipment (PPE) are at the root of this accident rate (Herrera and Gómez, 2003; Ortiz, 2003; Organización Panamericana para la Salud, 2007; Siesto, 2017).
Nursing students are exposed to highly contaminated environments (by either contact with patients, family members, or health personnel who may carry infections), and it is estimated that they are 40% more likely to be infected than the rest of the general population (Cabezas, 2012). According to Tapias et al. (2010), it is through the knowledge of exposure mechanisms and transmission risks, and their prevention that healthcare students and workers can contribute to creating a safe working environment, hence the need to invest in more and better education in this subject, with theoretical classes, theoretical-practical, and simulated practices.
Educationally wise, the implementation of the Bologna Plan (1999) has meant a change in the educational paradigm from teacher-based learning to a student-centered model. This implies a new dynamic in pedagogical methodologies for the acquisition of theoretical knowledge and the development of theoretical-practical competences within the clinical context (Siles González, 2011).
Specifically, in the scope of HCAIs, education needs to accompany the guidelines on core components of infection prevention and control (IPC), based on the priority topics identified, among others, by World Health Organization (2020), including strategies and tools for evaluation. Being a very specific and wide-ranging scientific area, where theoretical knowledge acquired is a tool that supports clinical decision-making, strategies associated with the learning/teaching process are fundamental in this educational area, permitting students to acquire and develop competences throughout their learning pathway.
These proposals, however, always face the challenge of how education and practice translate to an actual change in HCAI safe practices. Humphreys and Richards (2011), for example, discuss how teaching differs between medical and nurse students, where nurse students show a knowledge and performance advantage (Tavolacci et al., 2008; van de Mortel et al., 2010); yet, they catch up with their performance once they advance to postgraduate education. When looking into the educational factors, these changes happen partly due to a higher focus in teaching about HCAI control and prevention, increase in practice (Hunt et al., 2005), learning from supervisors (Snow et al., 2006), awareness, and a change from traditional lecture methods (Helder et al., 2010; Lobo et al., 2010). On the other hand, finding these differences between healthcare personnel education and practices suggests that reforming or improving the quality curriculums would lead to improved HCAI control and prevention practices.
Professional knowledge in nursing, as stipulated by the degree, is also characterized by being practice-oriented. Approximately 50% of the training must be developed in a clinical context, oriented toward learning in a team and in direct contact with patients and the community to organize, provide, and evaluate the care required from the knowledge, capacity, and skills acquired by the student (Zabalza Beraza, 2011; Rodríguez-García, 2019). The contents to be taught in the practices are theoretical and practical and must be developed by both academic and clinical tutors, adapting the contents and the learning process to each context (Zabalza Beraza, 2011). Clinical tutors or supervisors have a relevant role in the teaching and learning process by generating an adequate learning environment, in which other professionals from the care center also participate without educational responsibilities, influencing, and sharing habits, customs, and working conditions of all kinds (Rodríguez-García, 2019).
The introduction of clinical practices aims to teach students of the practical skills necessary to provide competent care, as the link between theory and practice facilitates the assimilation of knowledge and the development of professional skills. Practices must still follow safety standards, that is, based on interventions aimed at avoiding or minimizing harm from patient care (on Joint Commission on Accreditation of Healthcare Organization, 2015). By clinical practice, we understand the care function of the nursing profession, including all the functions and activities that it carries out to respond to the demands of health and illness. Safe HCAI practices should be based on adequate epidemiological surveillance systems that include multifaceted actions that promote safe professional practice by multidisciplinary teams (Dignath et al., 2008; WHO, 2018).
In addition to the educational organization itself (content, planning, direction, and control of the process), learning strategies can be affected by the unique situation of each student, both at the individual level (cognitive, motivational, and behaviors of the subject) and in the environment or learning context (patients, peers, other professionals, teachers, health center structure, and practices) (Quinn and McGrath, 1985; Stoner and Wankel, 1989; Gargallo, 2006). In fact, a study with nurse students showed that the best predictor of hand hygiene compliance was having their mentors practice it as well (Snow et al., 2006). The student intentionally and consciously analyzes the characteristics of the task that is demanded, the resources available for its execution, and the limitations found both on a personal level and in the learning context (Dignath and Büttner, 2008; Dignath et al., 2008; Sitzmann and Ely, 2011). Preventive practice, in short, is not going to depend exclusively on the knowledge or the availability of prevention resources. The desire of the student to put them into practice also weights in this process (Virú-Loza, 2012), a performance on which other variables can mediate besides the cognitive ones, which will have to do with his/her style of behavior, his/her personality traits, the type of affection and emotions he/she experiences at the time, and the motivations that lead him/her to execute the task.
We sum all these broad factors as a foundation to propose an HCAI prevention and control ecological system, taking into account the ecosystem in which the students develop competencies, and use this term to conceptualize what the environment entails for a nurse student. An ecosystem can be defined in its simplest form as the interactive system between organisms and an environment. The term, although rooted in biology, has also been used for social applications, where a human ecosystem is the interactional environment of a social system (individuals, groups, and cultures), with a resource system (Brush, 2014). The human ecosystem has been used in many different domains, including business, education, cybernetics, media, among others, and also in healthcare with the Workforce Ecosystem Model.
More specifically, it comprises of staffing (competence, education, and the volume of work), workflow design (on the job activities), personal/social factors (stress, job satisfaction, and professionalism), physical environment (lights, aesthetics, and sound), and organizational factors (use of teams, division of roles, and shared beliefs) (Hickam et al., 2003).
This said, using this background, we suggest the student ecosystem for HCAI control and prevention practices should involve three key agents that work as a collaborative link to engage in safe-care learning and performance: the educational and work environment, culture, and beliefs; and the student as practitioner and agent of change. We propose these are the root foundations in an ecosystem focused on student learning and development, which guides to acquire competences and values while facilitates a feasible environment to put in practice prevention and control safe practices. This proposal has a different view than the Workforce Ecosystem in a way that allows to have a central focus in the student. Consequently, it allows us to offer a unique view of the nursing environment and also narrow the scope for a more reasonable and answerable questionnaire length. With these goals in mind, we proceed to the development process of the instrument by trying to answer the question: What factors within this framework comprise the student HCAI control and prevention ecosystem?
To explore the perceptions of nursing students regarding their teaching and learning experience in the field of HCAIs prevention and control, and their attitudes and perceived performance, a European Consortium developed the InovSafeCare Questionnaire. This scale will offer the opportunity to explore and understand the current state of HCAIs prevention and control from the perspective of the educational environment, the healthcare organizations environment, and the attitudes, beliefs, and performance of the nursing students. We believe this scale serves a 2-fold purpose: to provide an empirical measurement of HCAIs-related factors within nursing students in Europe, and the potential to analyze how these factors interact to provide more meaningful and efficient proposals to improve safe practices in nurse students. Not having a previous measuring tool to focus on the HCAI of European student, we believe that the InovSafeCare scale can offer a meaningful contribution to start a theoretical framework that can help future improvement designs for safe practices.
The development process of the InovSafeCare scale follows a mixed approach of qualitative and quantitative methods to determine the set of items, underlying the dimensions behind the object of the study, and to test the validity of the items using statistics. This process was divided into two identified studies, where Study 1 follows a qualitative approach to generate the items, while Study 2 analyzes the psychometric properties of the questionnaire through a quantitative approach. Figure 1 demonstrates an overview of the scale development process.
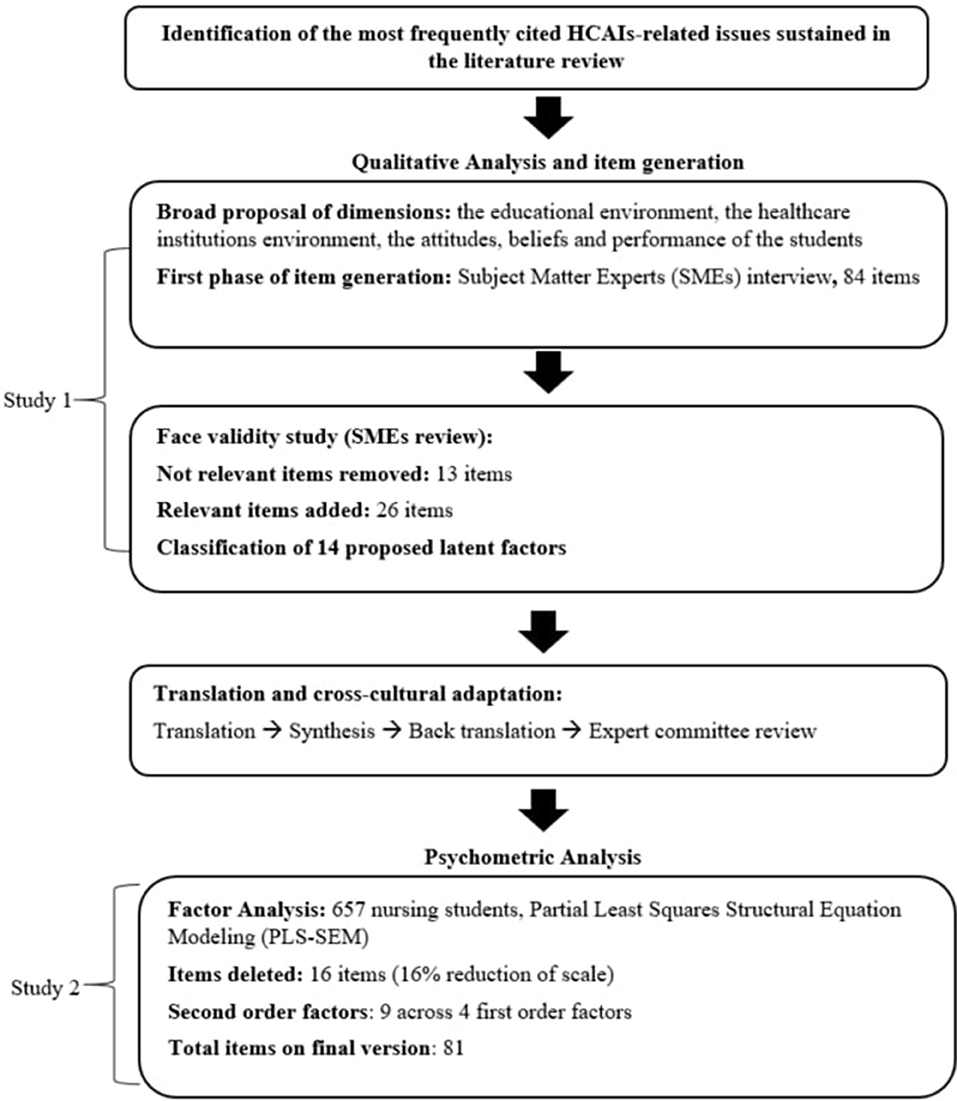
Figure 1. Overview of the InovSafeCare scale development process.
This first study aimed to find the foundation of the HCAI prevention and control content-related ecosystem, develop a preliminary set of items, and adjust them using a content validity study with a panel of experts.
For the development of the items, the theoretical review was previously laid out and a Content Validity Study was used to generate a set of preliminary items to be responded to in Likert-scoring format. Given the inductive approach to the item generation process, it was determined that to reach the objective with this questionnaire, the following topics must be addressed within it: the educational environment, the healthcare institutions environment, the attitudes and beliefs of the students, and the self-reported performance.
To ensure the highest quality and the well-grounded on real-life practicality of the items, the item pool development was subjected to a content validity procedure, where items were generated and submitted to a panel review process by subject matter experts (SMEs) on nursing and HCAI control and prevention practices from each of the participating institutions in the study: The Health School of the Polytechnic Institute of Santarém and the Nursing School of Coimbra from Portugal, the Hipolit Cegielski State University of Applied Sciences in Gniezno from Poland, the Savonia University of Applied Sciences from Finland, and the University of Salamanca from Spain. Each institution had at least two members in its expert review panel.
From a qualitative perspective, items can be derived by discussion according to the Standards of Educational and Psychological Testing by American Psychological Association (1985). In our case, this was facilitated by people who have direct field expertise, related to real-life experiences, and can establish indicators that are critical to our objectives. Our SME panel consisted of nurse supervisors, incumbents, and professors to guide us into what comprises the critical aspect of HCAI prevention and control within the framework of Education, Behavior, and Performance. Critical aspects were transformed into statements or questions that were further refined into an item structure and later discussed and modified until they match what SMEs considered relevant content to measure. Because we want to be as accurate as possible about the direct relevance of items and dimensions to the actual HCAI prevention and control practices, item generation benefits from discussion with SMEs in order to remain practical.
The item generation and revision phase lasted 2 months, which included virtual meetings among the panel members to discuss their feedback on each item on grammar, redundancy, latent factor correspondence, context correction, and relevance to HCAI. This further led to refining the items, ensuring beforehand a coherent topic and context for each of the latent factors, and making sure they were specifically applicable to the nursing students and safe-care topics.
As the scale aims to encompass the European nurse framework, we worked along our consortium to have the study use a diverse sample of the European population. To make sure that the items were equally applicable and understood by the participating countries, we submitted the questionnaire to a cultural adaptation procedure. Following the methodology proposed by Beaton et al. (2020), the items were created in English, and each of the respective countries participating in the study utilized, both, a translator with knowledge about the topic, and one without, to translate it. Both translators proceeded to convert each item, as well as instructions, to the language and wording that best fits their respective culture, and then delivered to the review panel committee of each respective institution to certify faithfulness to the original English version, as well as to the local culture. From these two translated versions, a synthesized third version was created, which was composed of a selection of the better fit of each of the items from the two versions, which was then evaluated by the experts of each institution, and then back-translated into English and sent to evaluate whether translating the questionnaire from the non-English version would still retain the same meaning as the original version.
The scale utilizes, both, formative and reflective factors. A formative factor is defined as when a packet of low-correlated indicators forms the latent factor. As our example, a factor about how dynamical is an institution in teaching about safe practices may have one item about the development of workshops and another about the use of visuals in classrooms for teaching students about HCAI. In this case, the increase in or presence of one does not need to relate to the change in the other. In other words, the sum of the indicators forms the construct. On the other hand, a reflective factor is when the latent construct manifests itself in a packet of correlated indicators. For example, one of our constructs has one item about how interested is the student to continue pursuing a nurse career and another about whether being a nurse will fulfill its professional expectations. The change in these items would be expected to correlate with one another, as the change in both is caused by the latent factor, Career Motivation.
Because the scale includes both types, covariance-based methods (or CBM) are not adequate to analyze the factor structure, as formative factors are not expected to correlate between the items (Hair et al., 2014). For this, we decided to use the partial least square (PLS) method using structural equation modeling (SEM) to test whether our proposed factors retain their structure (PLS-SEM). We used the software SMART-PLS3 to reach this objective, as its algorithm is capable to compute scores for formative (i.e., weights) and reflective (i.e., loadings) factors simultaneously in a single model.
While this method offers the advantage of validating formative constructs, it comes at the consequence of being unable to compute model fit scores traditionally found in CBM, as such, we are not including any of the CBM model fit scores on this report (i.e., chi-square test, comparative fit index, Tucker–Lewis Index, and root mean square error of approximation). Instead, current research in PLS-SEM suggests that model fit scores for these type of statistics are still at early stages (Hair et al., 2018), and thus should be cautious when reporting any. We chose to limit this to exclusively report the standardized root mean square residual (SRMR), which can be used to avoid model misspecification (Henseler et al., 2014). Values <0.1 or 0.08 are considered a good fit.
We explored second-order constructs in the case that the weights or loadings showed a pattern that would allow us to further group them within the factor and, if when revising the items, they made sense as second-order (Becker et al., 2012; Hair et al., 2018). For example, if a factor of seven items had three that showed a specific pattern (i.e., weights and/or conflicting p-values relative to the rest), instead of deleting them, we looked if they had some contextual relationship that may explain the results. If they did, we tried to make the second-order, and if the second-order had significant weight to the second and parent factor, they were retained as second-order. Specifically, we used the repeated indicator approach, which is the well-used method for estimating higher-order constructs in PLS, where the second-order construct is directly measured by reusing the items in the first-order factor (Wilson and Henseler, 2007).
As our example, a factor about prevention culture in health center showed two of its items show weight and p-value pattern different relative to the rest. When looking at the item text, these two items were about giving feedback to the student about safe practices during their placements, while the others were about personnel following and promoting compliance in the health center. By their nature, these two items correspond to the latent factor (Health Institution HCAI prevention culture), thus, we created second-order constructs, dividing this set of themes (Feedback and Compliance). Both had similar, and significant weights to the parent factor, thus, we retained the items by allowing second-order constructs.
Reflective constructs are expected to correlate, and we used loadings, instead of weights, and validity measures for internal consistency generally expected of these types of constructs. Composite reliability (CR) must be above 0.7, and the average variance extracted (AVE) should be above 0.5 (Hair et al., 2010). Below, but close to 0.5, is also permissible, since “AVE is a more conservative measure than CR. Based on CR alone, the researcher may conclude that the convergent validity of the construct is adequate, even though more than 50% of the variance is due to error” (Malhotra and Dash, 2011, p. 702). Formative constructs, on the other hand, are expected to have similar and statistically significant weights to the latent factor and low collinearity. We took a more liberal approach on p-values on formative factors and proceeded to leave the item if the exceeded threshold was not marginal. This is because the tradeoff of statistical confidence with values close to the threshold makes sense when the contribution of an item is unique, such as those found in these types of constructs (Cenfetelli and Bassellier, 2009). We used the variance inflation factor (VIF) to identify any concern in collinearity, with a threshold of anything above 5 a concern, and inadmissible above 10.
After interviewing and discussing with SMEs, it was agreed that the items should cover: (1) knowledge on HCAI prevention and control; (2) the active mission in educational and clinical settings to promote, teach, and reinforce safe practices; (3) how the student views infection control and prevention practices; (4) self-efficacy for safe practices; (5) identification with the nurse role; (6) perceived fatigue; (7) degree of distraction during clinical placements by the environment; and (8) self-reported safe practices. Using these topics as guidance, a total of 84 items were developed for the panel review process.
Panel review feedback brought indications that there were missing essential indicators, less-relevant items present, and vocabulary improvements required, which prompted us to review the item pool. One of the initial constructs aimed to indicate the degree of knowledge of specific bacteria related to HCAI, where the judges pointed out that there is higher relevance in whether prevention protocols and procedures were covered as topics in higher education, arguing that these were more relevant to HCAI control and prevention. In this case, we decided to fully replace the construct (7 items) and develop a set of items related to HCAI content covered in higher education formation (12 items). An example of this new construct is to indicate whether “Safe preparation and administration of intravenous medications” is addressed in the educational institution, as opposed to indicating the degree of knowledge in “Clostridium difficile” by the student, which was the type of item found in the originally proposed construct.
We also modified vocabulary when indicated, and whether there was any relevant content that was missing in the original pool. Specifically, the panel indicated that there was a necessity to measure whether specialized infection-trained link nurse is involved in clinical rotations of students, and an adequate student to teacher ratio in laboratories, which were further generated for the scale as a single item. Additionally, it was indicated that a specific dimension measuring the motives behind following safe practices should be included, as it would allow to gauge how transcendent the well-being of patients is for practitioners. To this, a new construct measuring intrinsic and extrinsic motives for following HCAI control and prevention was developed to fill this requirement with 11 new items, using as guidance Self-Determination Theory (Ryan and Deci, 2000).
Lastly, further discussion with the committee for item-factor correspondence and nomenclature led to propose a fixed set of 14 latent factors through 97 items, which are the following: Higher Education Institution HCAI Theoretical Content (HETheory, 12 items), Higher Education Institution Approach to teach HCAI (HEApproach, 5 items), Higher Education Institution HCAI practice-related approach/resources (HEPractice, 5 items), Health Institution HCAI prevention practices (HIPractice, 7 items), Health Institution HCAI prevention culture (HICulture, 7 items), Personal HCAI Attitudes (PAttitude, 6 items), Personal objection to HCAI prevention and control measures (PObject, 5 items), Self-Efficacy on HCAI prevention and control (SelfEff, 4 items), Career Motivation (CMotivation, 4 items), Fatigue (Fatigue, 6 items), Distraction (Distract, 7 items), Intrinsic motives to comply with HCAI control and prevention measures (IMotive, 7 items), Extrinsic motives to comply with HCAI control and prevention measures (EMotive, 4 items), Self-reported HCAI practices (SRPract, 6 items). Table 1 presents the dimensions in more detail, while Table 2 shows essential modifications done during the item generation phase.
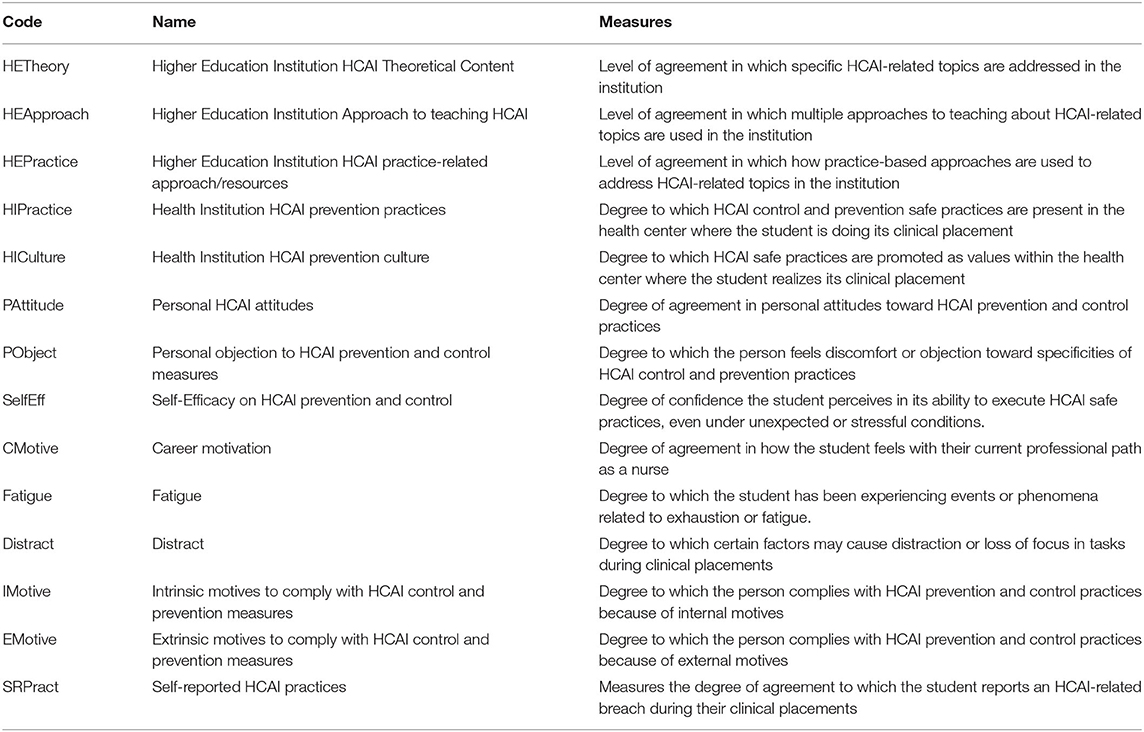
Table 1. InovSafeCare dimensions.
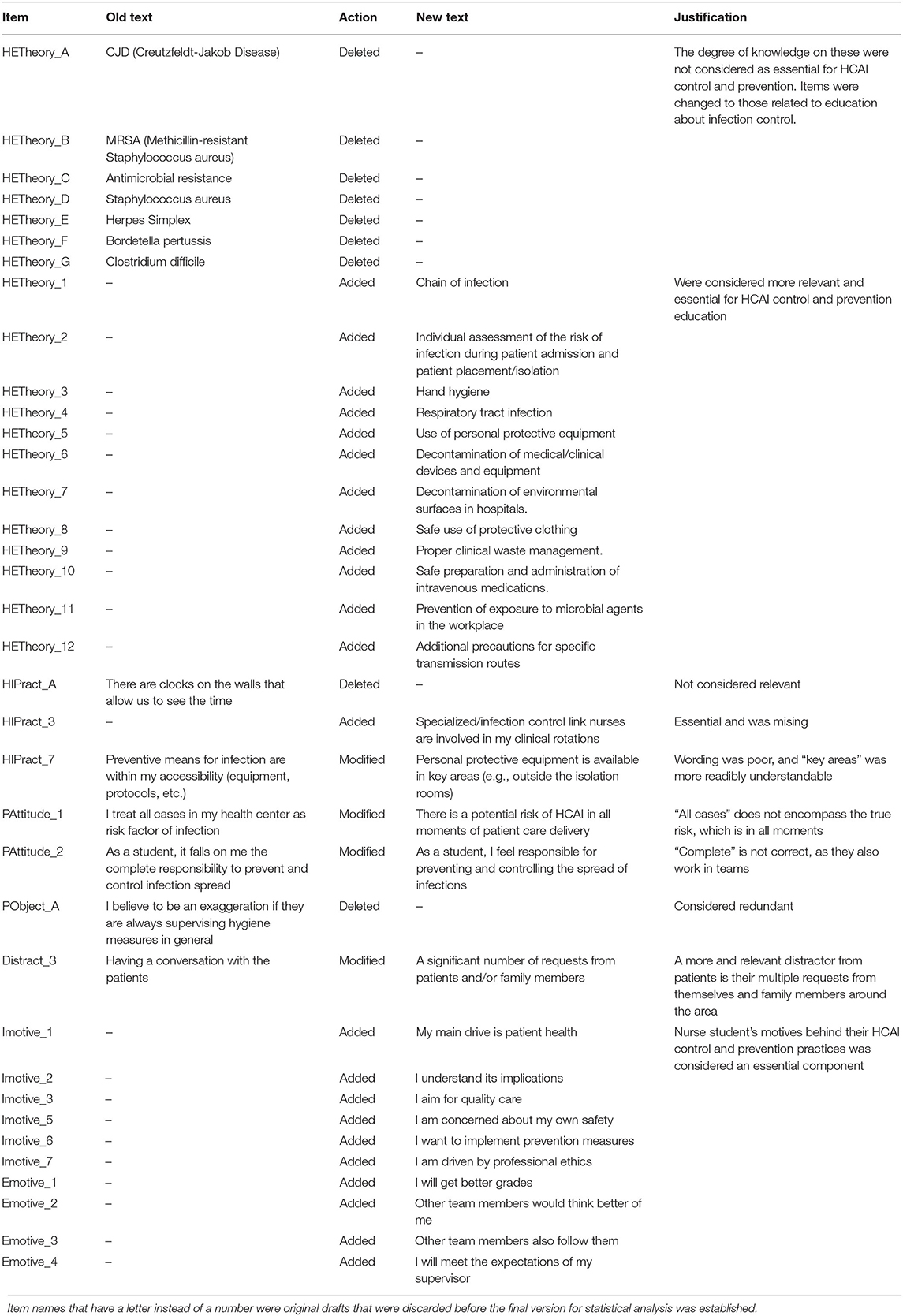
Table 2. Description and justification of original item modifications during their generation phase.
Once the final item pool was approved for testing, the questionnaire was applied in 2019 after approval from the Ethics Committees (Health Sciences Research Unit: Nursing (UICISA: E) of the Nursing School of Coimbra—reference 635/11-2019) to 657 nursing students from the Health School of the Polytechnic Institute of Santarém (ESS-IPS) (107), the Nursing School of Coimbra (ESEnfC) (214), the Hipolit Cegielski State University of Applied Sciences in Gniezno (PWSZ Gniezno) (119), the Savonia University of Applied Sciences (SUAS) (58), and the University of Salamanca (USAL) (158).
Gender-wise, 83 males and 573 females participated, ranging from 18 to 55 years of age, with a mean of 22.5 years.
The factor analysis of a 14-factor conceptualization of 97 items yielded low scores and high p-values in some of the items within the factors HETheory, HEPractice, HIPractice, HICulture, PAttitude, and Distract, with a SRMR above 0.1. More specifically, as outer weights are the measurable indicator of the item-factor relationship, this means they do not properly fit into their assigned latent factor. Regarding reflective factors, there were no cross or outer-loading concerns, however, one item showed a low beta with a high p-value in IMotive. These items (14) were marked for deletion. The reason these items were removed from the item pool is that they also did not adequately adjust to second-order factors either (e.g., regardless of first or second-order, they yielded low betas and high p-values). Table 3 presents the item-factor weights (formative) and loadings (reflective).
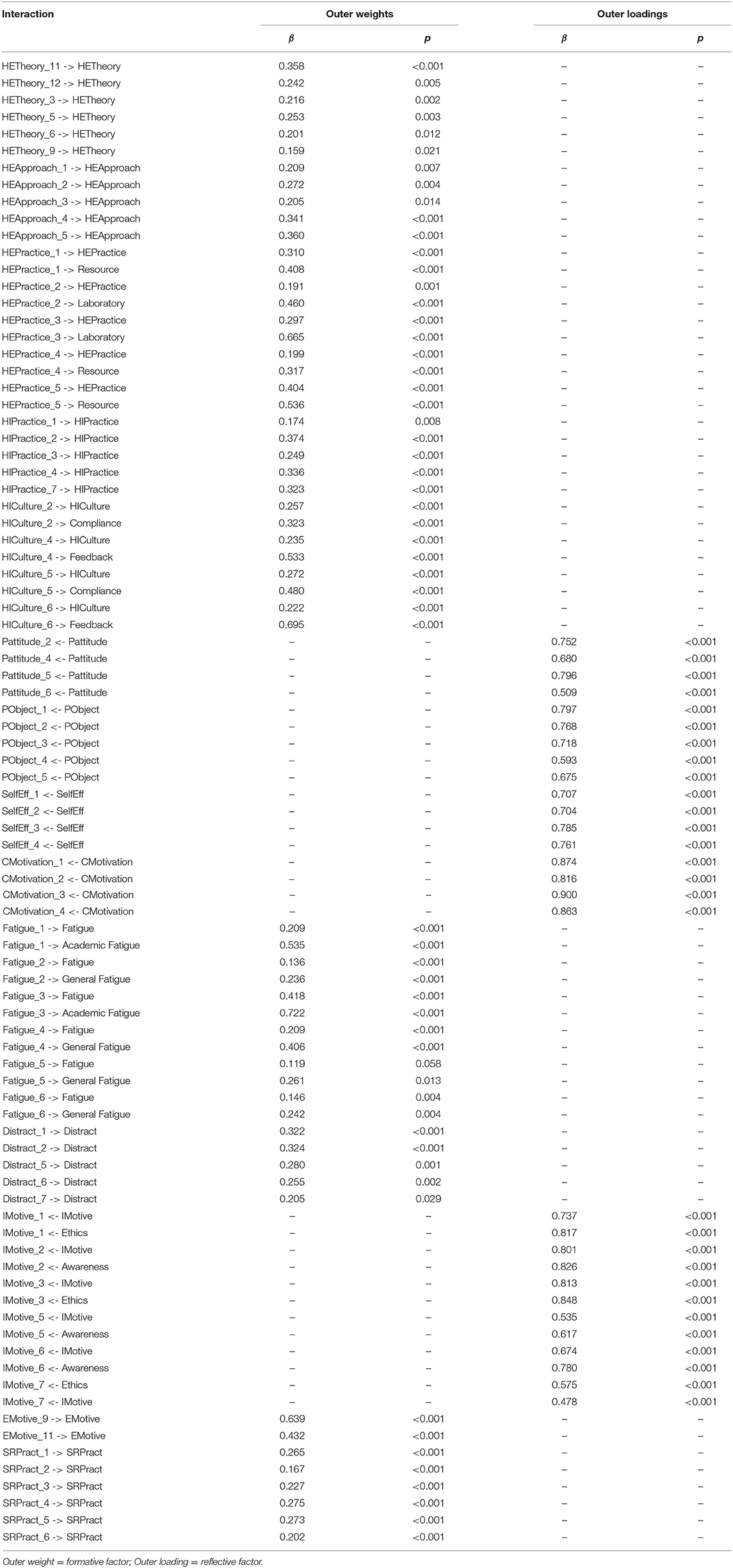
Table 3. Weights and significance.
Additionally, Table 4 presents factor loadings of reflective constructs within a matrix.
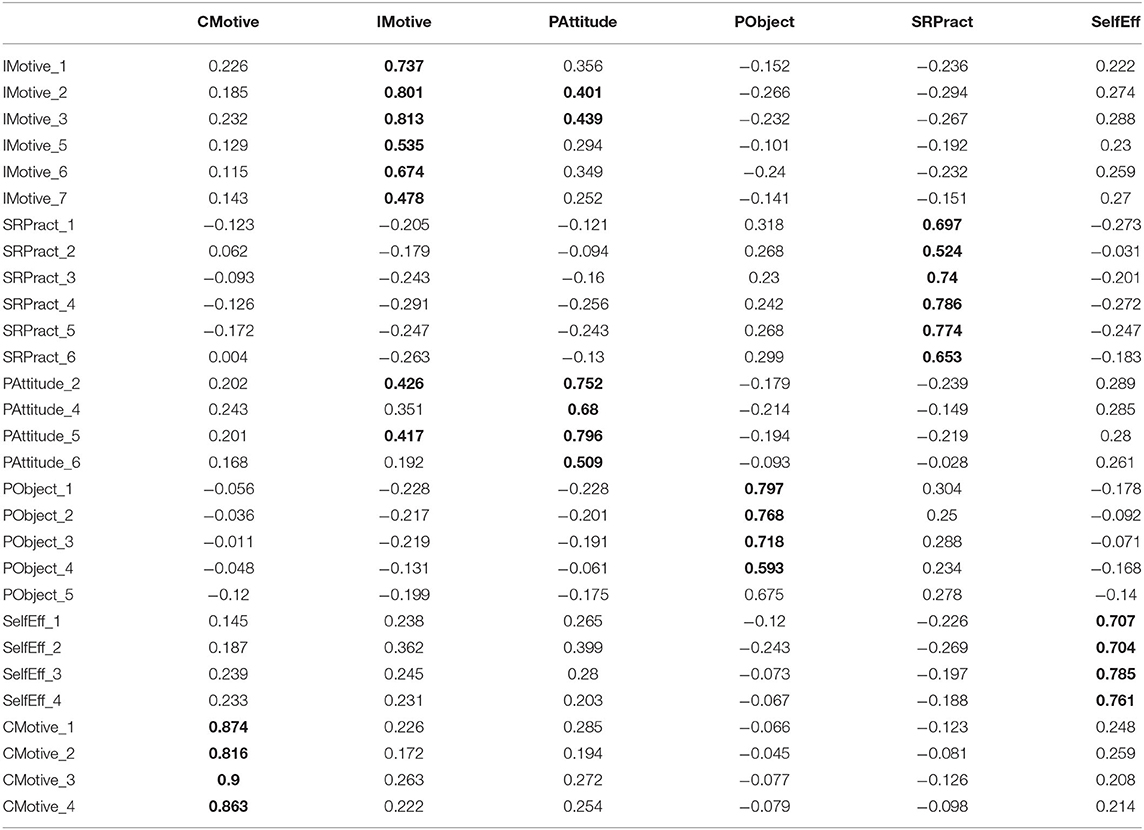
Table 4. Factor loading matrix for reflective factors.
Reflective constructs show that all of their items have adequate loadings, which is generally expected to be above 0.4 on their respective factor. On the other hand, some items also load above this threshold in different factors than the one expected. Specifically, PAttitude and IMotive show some of their items cross-load with each other: IMotive_2 and IMotive_3 with 0.401 and 0.439 in PAttidude; PAttitude_2 and PAttitude_5 with 0.426 and 0.417 in IMotive. This makes contextual sense, given both constructs deal with personal values regarding HCAI control practices, however, both are questioned differently and look for different aspects of these values (i.e., IMotive strictly asks the drive to comply, while PAttitude asks for their attitudes toward the risk of infection). Cross-loading items also present a considerable difference between each factor they load to (i.e., primary loading should be at least 0.2 larger than the secondary), suggesting these not necessarily merit deletion. Following this reasoning, the items were retained for the scale.
Twenty-one items presented coefficients with patterns that suggested a second-order structure. We identified a total of nine second-order factors across four main factors. Specifically, HEPractice shows a distinction between items about laboratory (e.g., student to teacher ratio and sufficient laboratory classes), and resources in practice-based courses (e.g., receiving feedback, technological resources, and simulation sessions). HICulture shows a distinction between items that relate to giving feedback in clinical placements (e.g., receiving guidance and correction) and having role models (e.g., others following example, getting motivated to comply with safe practices, and having supervisors ensure protective equipment is being used). Fatigue shows a distinction between items related to academic-related workload (e.g., clinical placements when tired and academic overload) and general fatigue (e.g., mental, physical, and emotional). IMotive shows a distinction between items about ethical guidelines (e.g., driven by ethics, patient health, and quality care) than from items that relate to awareness of what HCAI entails (e.g., aware of consequences, self-protection, and desire to prevent it). Emotive shows a distinction between items that reflect approval (e.g., meet expectations of supervisor and approval of peers) and the structure of another second-order factor with a packet of two items that did not share a common factor. The text in these two items was “I will get better grades,” and “Other teams also follow them.” These two rogue items make sense as external motives, but not as a single second-order, and were marked for deletion. Table 5 shows second-order text and the relationship to the parent factor.
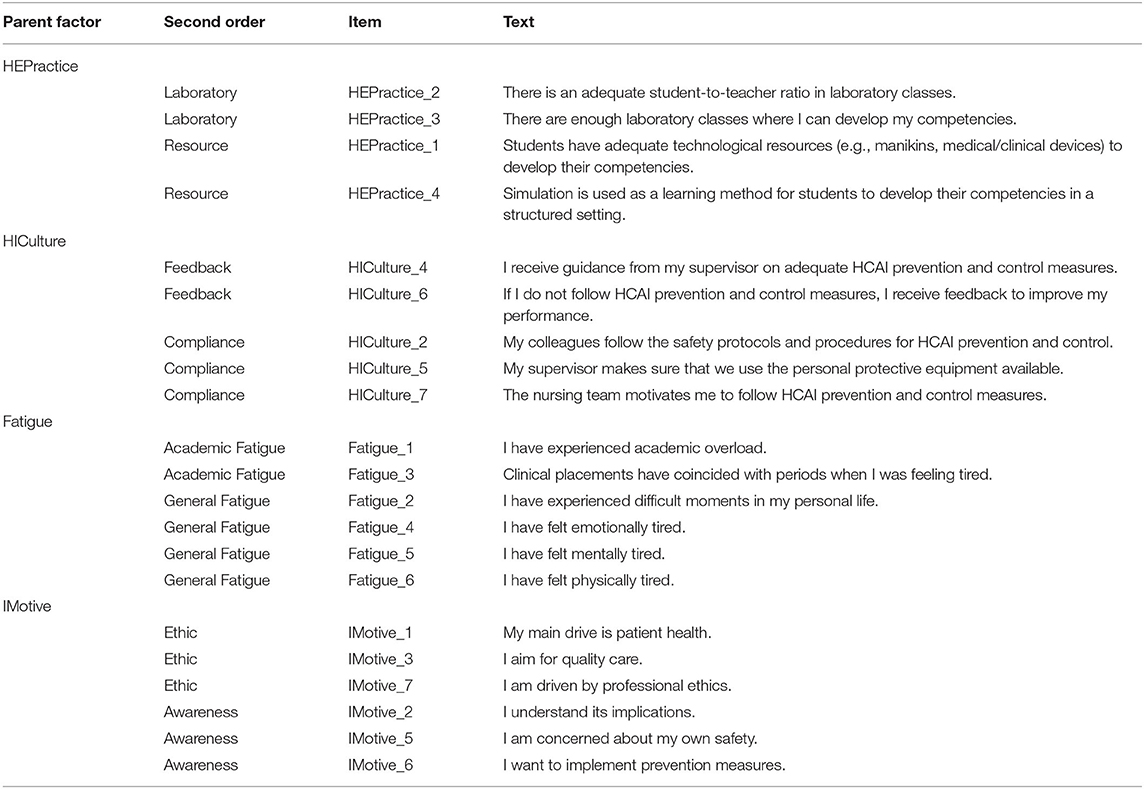
Table 5. Second-order factors.
Reliability and convergent validity results for reflective factors show adequate values: CMotivation (CR = 0.921; AVE = 0.746); SelfEff (CR = 0.828; AVE = 0.547); PObject (CR = 0.837; AVE = 0.510); SRPract (CR = 0.851; AVE = 0.492); PAttitude (CR = 0.783; AVE = 0.480); IMotive (CR = 0.837; AVE = 0.469). While some of the AVE values are below the cutoff value of 0.5, we believe that CR may suffice as it is, per the suggestions by Malhotra and Dash (2011).
According to the analysis, the VIF ranged from 1.3 to 4.3, the highest items being Fatigue_4 (4.042) and Fatigue_5 (4.317), with the rest of the items averaging around 1.7. Looking at the item text in both: “I have felt emotionally tired,” and “I have felt mentally tired,” it makes sense to obtain high VIF values, however, mental and emotional fatigue are logically distinct on their own. As they correspond to the same factor, we decided that their VIF is not a concern. No items were found to have collinearity issues, and none marked for deletion.
Lastly, after all these adjustments, SRMR showed 0.064 and 0.076 values for the saturated and estimated model, respectively, and represent a good model fit.
Table 6 presents descriptive information of each factor (number of items, mean, SD, and kurtosis), and Figure 2 shows the Importance-Performance Map Analysis (IPMA) graph, which determines the relative importance of the constructs within the scale.

Table 6. Total items per factor, mean, and SD.
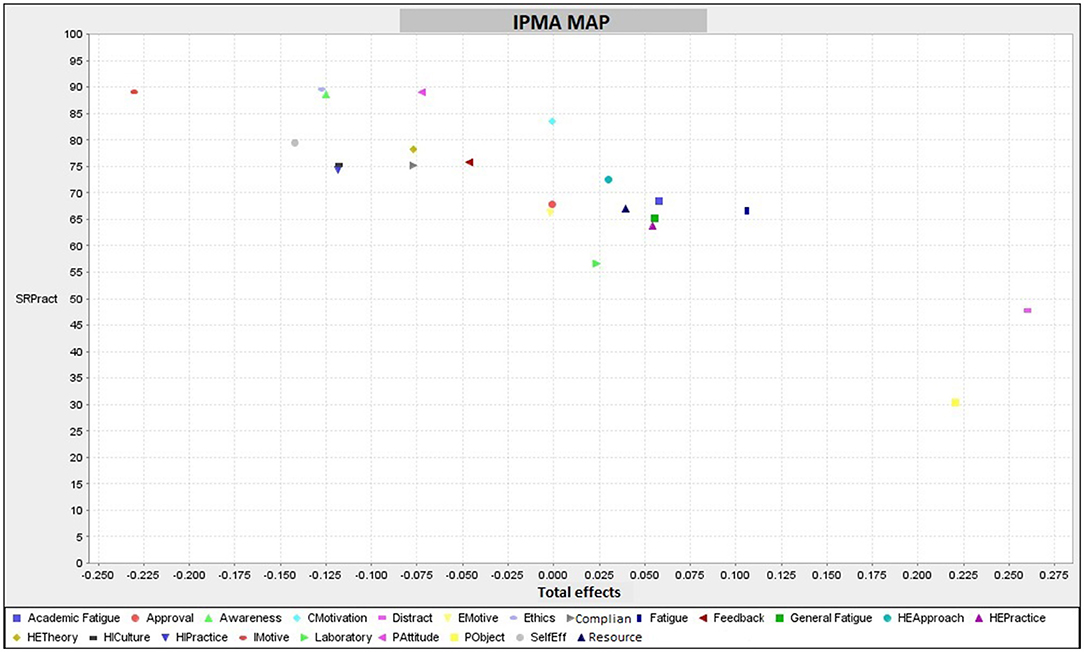
Figure 2. IPMA map.
The development process of the InovSafeCare scale started with the question: “what factors within this framework comprise the student HCAI control and prevention ecosystem?” After a process of qualitative item development, and empirical testing through a quantitative study to answer this question, the resulting scale led to 81 concise items representing the following 14 factors: Higher Education Institution HCAI Theoretical Content, Higher Education Institution Approach to teaching HCAI, Higher Education Institution HCAI practice-related approach/resources, Health Institution HCAI prevention practices, Health Institution HCAI prevention culture, Personal HCAI Attitudes, Personal objection to HCAI prevention and control measures, Self-Efficacy on HCAI prevention and control, Career Motivation, Fatigue, Distract, Intrinsic motives to comply with HCAI control and prevention measures, Extrinsic motives to comply with HCAI control and prevention measures, and Self-reported HCAI practices. These studies evidenced the validity of the construct and adequate psychometric properties of the factors presented.
The constructs, item, and text are presented in Table 7.
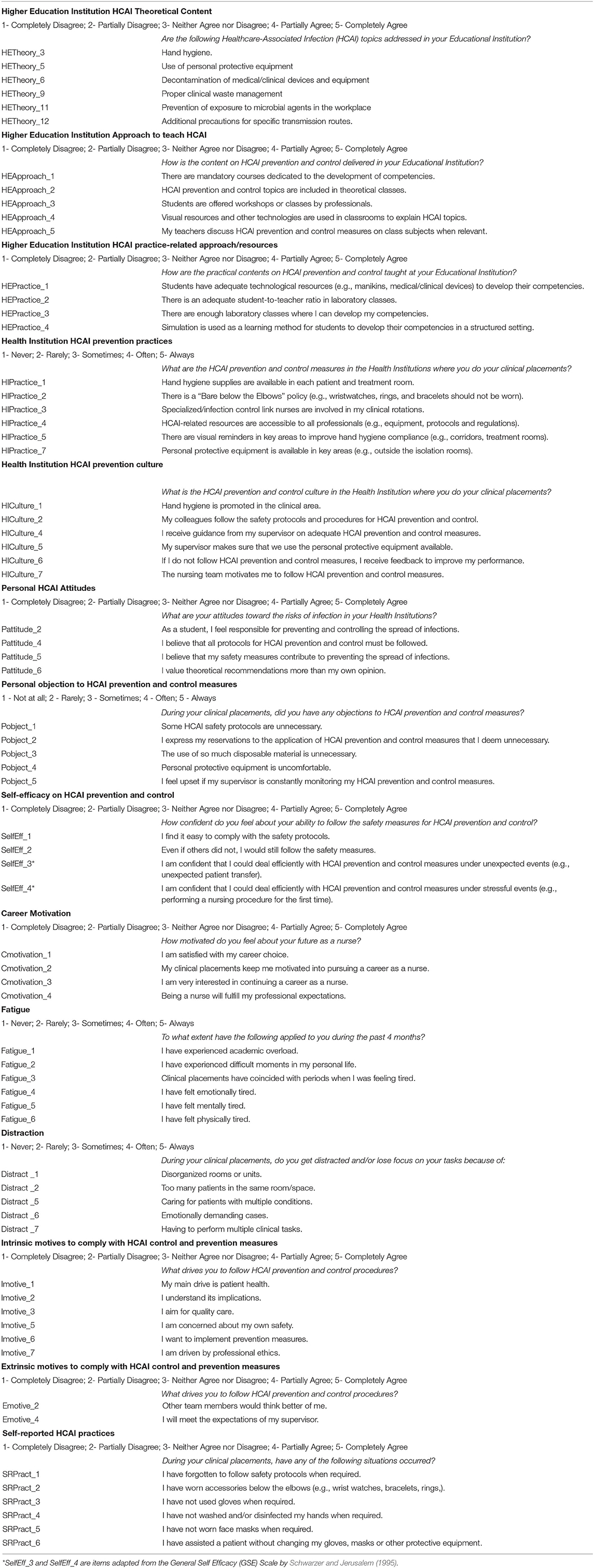
Table 7. InovSafeCare Scale (81 items).
The development of this scale serves both, a research-focused purpose to answer the question “How does the HCAI prevention and control practices ecosystem for students interact within it?”, and a practical purpose, which would be to answer the question “what can we do within this ecosystem to improve safe practices of students?” We use the term ecosystem as an umbrella term in this study to start to thread a theoretical framework, and this scale is a step further to understand, with a more empirical approach, where and how we should focus on improving the quality and practicality of education, work culture, and attitudes in nurse students to lead to a more efficient handling of HCAI breaches during clinical placements, and potential future as a full practitioner.
Future research should start with developing a theoretical model of how these variables interact within themselves and their relevance. A more robust approach would be to use this information to create new training modules that can help improve the ecosystem and use a longitudinal approach to see how it improves real-life performance metrics (e.g., HCAI cases) with its implementation.
The scale utilizes self-reported measures, meaning there is always respondent bias, and its length is also prone to respondent fatigue. Second, method-wise, PLS-SEM is a recent approach to measure and validate formative constructs and structural models, and while this is a current challenge to research into these type of constructs (Hair et al., 2018), we nonetheless used the most current accepted methods to provide the best indicators of validity. On the other hand, although PLS-SEM does not rely on the conventional 1:10 rule of thumb for sample adequacy, the sample may benefit from a bigger pool of participants, as well as a concurrent validity analysis in a future study. Third, the sample represents members of a European consortium of four countries (which itself is a sample of the European Union (EU) population) but would have benefited from more countries within the zone participating. To compensate for this limitation, the foundations behind the questionnaire were guided by the Bologna Declaration 1999's plan in higher education, which provides a uniform guideline for safe practices for all EU members.
The datasets presented in this article are not readily available because the dataset remains for exclusive use by the authors due to participant privacy and informed consent. Requests to access the datasets should be directed to Amaia Yurrebaso Macho, YW1haWF5QHVzYWwuZXM=.
The studies involving human participants were reviewed and approved by Ethics Committees (Health Sciences Research Unit: Nursing (UICISA: E) of the Nursing School of Coimbra—reference 635/11-2019). The patients/participants provided their written informed consent to participate in this study.
All authors listed have made a substantial, direct, and intellectual contribution to the work, and approved it for publication.
This study was part of the InovSafeCare Project, Educating Students for innovative infection prevention and control practices in healthcare settings (2018-1-PT01-KA203-047453), co-funded by the Erasmus+ Programme of the European Union with the support of the c (Portugal).
All authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Agencia Nacional de Evaluación de la Calidad y Acreditación (ANECA) (2004). Libro Blanco de la Titulación de Enfermería de la Agencia Nacional de Evaluación de la Calidad y la Acreditación. Madrid.
American Psychological Association (1985). Standards for Educational and Psychological Testing. Washington, DC: American Psychological Association.
Beaton, D. E., Bombardier, C., Guillemin, F., and Ferraz, M. B. (2020). Directrices para el proceso de adaptación transcultural de medidas de autoinforme, 3186–3191.
Becker, J.-M., Klein, K., and Wetzels, M. (2012). Hierarchical latent variable models in PLS-SEM: guidelines for using reflective-formative type models. Long Range Planning 45, 359–394. doi: 10.1016/j.lrp.2012.10.001
Brosio, F., Kuhdari, P., Stefanati, A., Sulcaj, N., Lupi, S., Guidi, E., et al. (2017). Knowledge and behaviour of nursing students on the prevention of healthcare associated infections. J. Prev. Med. Hygiene 58, E99–E104.
Brush, C. G. (2014). Exploring the Concept of an Entrepreneurship Education Ecosystem. Innovative Pathways for University Entrepreneurship in the 21st Century, 25–39. doi: 10.1108/S1048-473620140000024000
Cabezas, C. (2012). Tuberculosis en personal y estudiantes de salud: un tema pendiente para los servicios de salud y la universidad. Rev. Peru. Med. Exp. Salud Publica. 29, 179–180. doi: 10.1590/S1726-46342012000200002
Cenfetelli, R. T., and Bassellier, G. (2009). Interpretation of formative measurement in Information systems research. MIS Q. 33, 689–707. doi: 10.2307/20650323
Díaz, L. A., and Cadena, L. P. (2003). Riesgo de hepatitis B entre estudiantes de medicina peruanos, luego de exposición a sangre y líquidos corporales. Rev. Gastroenterol. 23, 107–110. Available online at: http://www.scielo.org.pe/pdf/rgp/v23n2/a04v23n2.pdf
Dignath, Ch., and Büttner, G. (2008). Components of fostering self-regulated learning. among students. A meta-analysis on intervention studies at primary and secondary school level. Metacognition Learn. 3, 231–264. doi: 10.1007/s11409-008-9029-x
Dignath, Ch., Büttner, G., and Langfeldt, H. P. (2008). How can primary school students learn self-regulated learning strategies most effectively?: a meta-analysis on self-regulation training programmes. Educ. Res. Revie. 3, 101–129. doi: 10.1016/j.edurev.2008.02.003
European Center for Disease Prevention Control (ECDPC) (2020). Available online at: https://www.ecdc.europa.eu/en
Gargallo, B. (2006). Estrategias de aprendizaje, rendimiento y otras variables relevantes en estudiantes universitarios. Rev. Psicología General Aplicada 59, 109–130. Available online at: https://www.uv.es/gargallo/Estrategias.pdf
Hair, J., Black, W., Babin, B., and Anderson, R. (2010). Multivariate Data Analysis, 7th Edn. Upper Saddle River, NJ: Prentice-Hall, Inc.
Hair, J., Sarstedt, M., Hopkins, L., and Kuppelwieser, V. G. (2014). Partial least squares structural equation modeling (PLS-SEM). An emerging tool in business research. Euro. Business Rev. 26, 106–121. doi: 10.1108/EBR-10-2013-0128
Hair, J. F., Sarstedt, M., Ringle, C. M., and Gudergan, S. P. (2018). Advanced Issues in Partial Least Squares Structural Equation Modeling (PLS-SEM). Thousand Oaks, CA: Sage.
Helder, O. K., Brug, J., Looman, C. W. N., van goudoever, J. B., and Kornelisse, R. F. (2010). The impact of an education program on hand hygiene compliance and nosocomial infection incidence in an urban Neonatal Intensive Care Unit: an intervention study with before and after comparison. Int. J. Nurse Stud. 47, 1245–1252. doi: 10.1016/j.ijnurstu.2010.03.005
Henseler, J., Dijkstra, T. K., Sarstedt, M., Ringle, C. M., Diamantopoulos, A., Straub, D. W., et al. (2014). Common beliefs and reality about partial least squares: comments on Rönkkö & Evermann (2013). Org. Res. Methods 17, 182–209. doi: 10.1177/1094428114526928
Herrera, A., and Gómez, R. (2003). Accidentes por riesgos biológicos en estudiantes de la salud la Universidad Tecnológica de Pereira. Rev. Med. Risaralda. 9.
Hickam, D. H., Severance, S., Feldstein, A., Ray, L., Gorman, P., Schuldheis, S., et al. (2003). The EFFECT of Health Care Working Conditions on Patient Safety. Evidence Report/Technology Assessment Number 74, (Prepared by Oregon Health & Science University Under Contract NO. 290-97-0018.) AHRQ Publication No. 03-E031. Rockville, MD: Agency for Healthcare Research and Quality.
Humphreys, H., and Richards, J. (2011). Undergraduate and postgraduate medical education on the prevention and control of healthcare-associated infection. More progress is needed. Int. J. Infect. Control 7, 1–5. doi: 10.3396/ijic.V7i2.012.11
Hunt, D. C. E., Mohammudally, A., Stone, S. P., and Dacre, J. (2005). Hand-hygiene behaviour, attitudes and beliefs in first year clinical medical students. Int. J. Infect. Control 59, 371–373. doi: 10.1016/j.jhin.2004.09.002
Joint Commission on Accreditation of Healthcare Organization (2015). National Patient Safety Goals. Available online at: http://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals
Lobo, R. D., Levin, A. S., Oliveira, M. S., Gomes, L. M., Gobara, S., Park, M., et al. (2010). Evaluation of interventions to reduce catheter-associated bloodstream infection: Continued tailored education versus one basic lecture. Am. J. Infect. Control 38, 440–448. doi: 10.1016/j.ajic.2009.09.013
Malhotra, N. K., and Dash, S. (2011). Marketing Research an Applied Orientation. London: Pearson Publishing.
Organización Panamericana para la Salud (2007). Guía para la prevención y el control de las infecciones en servicios de salud, dirigida a estudiantes de las carreras de ciencias de la salud. Área de Prevención y Control de Enfermedades. Unidad de Enfermedades Transmisibles. La Paz, Bolivia, HDM/CD/A/456-07.
Ortiz, S. (2003). Riesgos biológicos de los estudiantes de enfermería. Enfermería Clín. 13, 285–289. doi: 10.1016/S1130-8621(03)73822-4
Quinn, R. E., and McGrath, M. R. (1985). “La transformación de las culturas organizacionales: una perspectiva de valores en competencia,” in Cultura Organizacional, eds P. J. Frost, L. F. Moore, M. R. Louis, C. C. Lundberg, and J. Martin (Sage Publications, Inc.), 315–334.
Rodríguez, M., Pérez, M., Pla, J., Miranda, L., Garotte, M., Peña, M., et al. (2008). Riesgos biológicos laborales en el personal de enfermería de una institución hospitalaria. Ciudad La Habana 8:e2722. doi: 10.5867/medwave.2008.02.2722
Rodríguez-García, M. C. (2019). Precepción de los estudiantes del Grado de Enfermería sobre su entorno de prácticas clínicas: un estudio fenomenológico. Enfermería Clín. 29, 265–270. doi: 10.1016/j.enfcli.2018.10.004
Rubio, M., Ávila, G., and Arana, B. (2008). Actitudes de Estudiantes de Enfermería mexicanos al manejar residuos peligrosos biológicos infecciosos. Escola Anna Nery 12, 479–484. doi: 10.1590/S1414-81452008000300013
Ryan, R. M., and Deci, E. L. (2000). Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 55, 68–78. doi: 10.1037/0003-066X.55.1.68
Schwarzer, R., and Jerusalem, M. (1995). “Generalized self-efficacy scale,” in Measures in Health Psychology: A User's Portfolio. Causal and Control Beliefs, eds J. Weinman, S. Wright, and M. Johnston (Windsor: NFER-NELSON), 35–37.
Siesto, A. (2017). Accidente con riesgo biológico en los estudiantes de enfermería de la Universidad de Salamanca durante sus prácticas clínicas. Rev. Enfermería Castilla León 9, 63–77. Available online at: http://www.revistaenfermeriacyl.com/index.php/revistaenfermeriacyl/article/view/192
Siles González, S. (2011). Historia versus cambio: paradigmas científicos y cambio histórico. Perspectivas de futuro de la enfermería en España En: Graván Fernández C coordinadora. Historia de la enfermería. Murcia: DAE. p. 479–512.
Sitzmann, T., and Ely, K. (2011). Un metaanálisis del aprendizaje autorregulado en la formación relacionada con el trabajo y el logro educativo: lo que sabemos y hacia dónde debemos ir. Psychol. Bull. 137, 421–442. doi: 10.1037/a0022777
Snow, M., White, G. L., Alder, S. C., and Stanford, J. B. (2006). Mentor's hand hygiene practices influence student's hand hygiene rates. Am. J. Infection Control 34, 18–24. doi: 10.1016/j.ajic.2005.05.009
Tapias, L. F., Torres, S., Tapias, L., and Santamaria, C. L. (2010). Accidentes biológicos en médicos residentes de Bucaramanga, Colombia. Rev. Col. Cir. 25, 290–299. Available online at: https://www.revistacirugia.org/index.php/cirugia/article/view/139
Tavolacci, M-P., Ladner, J., Bailly, L., Merle, V., Pitrou, I., and Czernichow, P. (2008). Prevention of nosocomial infection and standard precautions: knowledge and source of information among healthcare students. Infect. Control Hosp. Infect. 29, 642–647. doi: 10.1086/588683
van de Mortel, T. F., Apostolopoulou, E., and Petrikkos, G. A. (2010). A comparison of the hand hygiene knowledge, beliefs, and practices of greek nursing and medical students. Am. J. Infect. Control 38, 75–77. doi: 10.1016/j.ajic.2009.05.006
Virú-Loza, M. A. (2012). Prácticas del Personal de Salud relacionadas con las Medidas de Prevención de la Tuberculosis. Rev. Peru. Med. Exp. Salud Publica. doi: 10.1590/S1726-46342012000400030
Wilson, B., and Henseler, J. (2007). “Modeling reflective higher-order constructs using three approaches with PLS path modeling: a Monte Carlo comparison,” in Conference Proceedings ANZMAC-2007, eds M. Thyne and K. R. Deans (Duendin: ANZMAC), 791–800.
World Health Organization (2020). Asesoramiento sobre el uso de mascarillas en la comunidad, durante la atención domiciliaria y en entornos sanitarios en el contexto del brote del nuevo coronavirus (2019-nCoV): orientación provisional, January 29, 2020. World Health Organization. Available online at: https://apps.who.int/iris/handle/10665/330987
Zabalza Beraza, M. A. (2011). El Prácticum en la formación universitaria: estado de la cuestión. Rev. Educ. 354, 21–43. Available online at: http://www.revistaeducacion.educacion.es/re354/re354_02.pdf
Keywords: infections, infection control, learning, nursing, students
Citation: Yurrebaso Macho A, Ward Mayens AL, Picado Valverde EM, Guzmán Ordaz R, Juanes Méndez JA, Pérez Iglesias JL, Mirón Canelo JA, Pinto MdR, Costa Reis AMdS, Simões JA, Torres AL, Silén-Lipponen M, Korhonen U, Koponen L, Myllymäki M, Jankowiak-Bernaciak A, Patrzała A, Bączyk G, Basa A, Costa PS, Serambeque B, Oliveira AS, Pardal J, Graveto JMGdN and Parreira P (2021) Nursing Students' Perceptions on Healthcare-Associated Infection Control and Prevention Teaching and Learning Experience: Development and Validation of a Scale in Four European Countries. Front. Psychol. 12:701208. doi: 10.3389/fpsyg.2021.701208
Received: 28 April 2021; Accepted: 27 August 2021;
Published: 08 October 2021.
Edited by:
Laura Badenes-Ribera, University of Valencia, SpainReviewed by:
Julio C. Penagos-Corzo, University of the Americas Puebla, MexicoCopyright © 2021 Yurrebaso Macho, Ward Mayens, Picado Valverde, Guzmán Ordaz, Juanes Méndez, Pérez Iglesias, Mirón Canelo, Pinto, Costa Reis, Simões, Torres, Silén-Lipponen, Korhonen, Koponen, Myllymäki, Jankowiak-Bernaciak, Patrzała, Bączyk, Basa, Costa, Serambeque, Oliveira, Pardal, Graveto and Parreira. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Amaia Yurrebaso Macho, YW1haWF5QHVzYWwuZXM=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.