
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychol. , 28 October 2020
Sec. Health Psychology
Volume 11 - 2020 | https://doi.org/10.3389/fpsyg.2020.563876
This article is part of the Research Topic Coronavirus Disease (COVID-19): Psychological, Behavioral, Interpersonal Effects, and Clinical Implications for Health Systems View all 204 articles
 Ronald Fischer1,2*
Ronald Fischer1,2* Tiago Bortolini2
Tiago Bortolini2 Johannes Alfons Karl1
Johannes Alfons Karl1 Marcelo Zilberberg3
Marcelo Zilberberg3 Kealagh Robinson1
Kealagh Robinson1 André Rabelo4
André Rabelo4 Lucas Gemal2
Lucas Gemal2 Daniel Wegerhoff1Thị Bảo Trâm Nguyễn1Briar Irving1
Daniel Wegerhoff1Thị Bảo Trâm Nguyễn1Briar Irving1 Megan Chrystal1
Megan Chrystal1 Paulo Mattos2,5
Paulo Mattos2,5We conducted a rapid review and quantitative summary of meta-analyses that have examined interventions which can be used by individuals during quarantine and social distancing to manage anxiety, depression, stress, and subjective well-being. A literature search yielded 34 meta-analyses (total number of studies k = 1,390, n = 145,744) that were summarized. Overall, self-guided interventions showed small to medium effects in comparison to control groups. In particular, self-guided therapeutic approaches (including cognitive-behavioral, mindfulness, and acceptance-based interventions), selected positive psychology interventions, and multi-component and activity-based interventions (music, physical exercise) showed promising evidence for effectiveness. Overall, self-guided interventions on average did not show the same degree of effectiveness as traditional guided individual or group therapies. There was no consistent evidence of dose effects, baseline differences, and differential effectiveness of eHealth interventions. More research on the effectiveness of interventions in diverse cultural settings is needed.
Social distancing measures are effective in reducing viral spread in the current COVID-19 pandemic but have been shown to increase mental health burdens. These collateral effects are affecting large numbers of individuals globally, requiring urgent attention because of the strains on mental health providers struggling to provide adequate support for people in need. Although there are many self-help guidelines available online and via social media, it is unclear how effective these are. We provide a quantitative review of evidence-based practices that can be used by individuals at home or in confined physical environments during social distancing and quarantine to manage anxiety, depression, and stress. Given the likely continuation of social distancing measures in various parts of the world and shortages in mental health systems globally, our systematic review provides evidence on effective self-guided interventions, either as an initial stand-alone self-help intervention or while waiting for treatment.
What strategies can an individual adopt to maintain good mental health and reduce anxiety and stress during quarantines and physical distancing? Quarantines are psychologically taxing (Brooks et al., 2020), yet quarantines and physical distancing are core behavioral strategies for containing the spread of communicable diseases such as COVID-19. Levels of depression, anxiety, and psychological stress tend to be significantly elevated and can reach clinical levels in both disease survivors as well as the general population during pandemics. For example, Reynolds et al. (2008) reported that over 40% of quarantined Canadians in their sample reported high levels of worry. In the context of the COVID-19 pandemic, Wang et al. (2020) found that 28% of Chinese respondents reported clinically relevant levels of anxiety. Across both studies, over 50% of the sample indicated moderate to high levels of stress. The long-term psychological consequences of quarantine can last for months or possibly years (Brooks et al., 2020; Ho et al., 2020). The current COVID-19 (SARS-CoV-2) pandemic is affecting individuals globally at an unprecedented scale. Although widespread physical distancing measures appears effective in mitigating the spread of COVID-19 (Milne and Xie, 2020), the psychological ramifications of social distancing may result in increased levels of mental health problems in the near-term future.
Public mental health resources are finite, and the mental health services currently available are unlikely to cope with the emerging demands (Dong and Bouey, 2020; Duan and Zhu, 2020; Xiang et al., 2020). Addressing mental health needs within a physical distancing context is critical, given the possibility of continued movement restrictions in the near future to combat repeated outbreaks of SARS-CoV-2 (Kissler et al., 2020). To bolster available mental health services, while also reducing the likelihood of virus transmission, there has been a recent drive to convert usual face-to-face mental health treatments into an online or tele-health format.
However, while such modifications are no doubt vital, they represent only one building block of an organized mental health response, particularly when dealing with a pandemic such as COVID-19. Furthermore, even with increased use of tele-health measures by mental health providers, the shortage of trained professionals coupled with the increased demand on public health services highlights the need for effective and evidence-based self-guided therapeutic interventions (Duan and Zhu, 2020). The “World Health Organization Service Organization Pyramid for an Optimal Mix of Services for Mental Health” highlights self-care approaches (actions taken by individuals to improve their well-being) as an essential component of optimal mental health care (World Health Organization, 2003). In order to promote resilience and to appropriately manage the emerging mental health impacts of the ongoing COVID-19 pandemic, it is necessary to identify effective self-guided approaches to manage the psychological demands experienced during such outbreaks. Self-guided interventions can provide a first point of intervention for concerned individuals to alleviate anxieties, stress and worries, decrease negative mood and depressive symptoms, and increase positive psychological functioning and subjective well-being, either as a stand-alone intervention or while waiting for treatment. Although there are many self-help guidelines available online and via social media, it is unclear how effective these are and how well they are grounded in scientific evidence.
The goal of our rapid review is to provide a broad summary of the current evidence drawn from published meta-analyses in order to evaluate the effectiveness of self-guided therapeutic practices which can be implemented by individuals on their own, including during physical distancing and quarantine measures. We focused on published meta-analyses of randomized controlled trials (RCT) or experimental studies that evaluate the effectiveness of psychological interventions and strategies for a range of psychological outcomes. In particular, we focus on increasing subjective well-being (including life satisfaction, quality of life, happiness), and decreasing anxiety, depression, or stress as key outcomes. Critically, we screened all meta-analyses identified by our search parameters, but only summarize evidence from those meta-analyses which included self-guided conditions which can be performed by individuals alone without the guidance of trained health professionals. Our meta-analysis is more inclusive in scope because previous meta-analyses have: (a) typically focused on either a specific type of intervention or compared a small number of interventions without considering the wider range of possible interventions that might be beneficial; or (b) did not specifically consider the relevance and evidence of self-guided practices that could be performed by individuals alone. Thus, our primary aim is to provide a comparative summary of the available evidence of diverse psychological strategies that can inform recommendations by public health workers and psychologists, as well as be made available to the larger public. The COVID-19 pandemic affects populations of all nations, but interventions are often conducted with Western, industrialized and individualistic samples (Henrich et al., 2010), requiring more attention to cultural differences in effectiveness. We therefore evaluated whether the meta-analyses included in this review reported differences in treatment effectiveness for individuals from different cultural backgrounds. We focus on interventions that might be applicable in the current pandemic (and beyond), but explicitly stress that our data is not based on interventions conducted during the current COVID-19 pandemic. In order to provide actionable advice, we provide an electronic supplement containing selected self-guided exercises based on evidence gathered in this review. These exercises and tasks were selected with attention to possible applications across different cultural and economic contexts.
We performed a PsycInfo and MedLine search on March 22, 2020 to identify meta-analyses that have summarized RCTs or experimental studies that report the effectiveness of interventions on anxiety, depression, stress, or subjective well-being in human populations. The exact search terms and their combination are listed in Appendix A. The inclusion criteria for our review were: (a) quantitative meta-analysis of RCTs or experimental studies; (b) conducted with general populations, clinical or non-clinical samples, or samples selected for anxiety or depression symptoms; (c) the sample was on average 18 years or older; (d) measures of anxiety, depression, stress, or subjective well-being were included; (e) the meta-analysis included interventions that are self-guided or could be used by individuals without supervision or guidance by a trainer, therapist, or mental health professional; and (f) reported sufficient information on effect sizes. Where available, relevant moderator conditions were also extracted for further analysis. We decided to include anxiety and depression clinical samples due to the reported increase of anxiety and depression during quarantines (Brooks et al., 2020). The exclusion criteria for our review were: (a) clinical or patient populations other than individuals or groups with clinical anxiety and depression symptoms; (b) meta-analyses of group-based interventions; (c) meta-analyses of individual therapies or interventions led by or supervised/assisted by another person; (d) meta-analyses that did not clearly report on conditions in criteria a-c; (e) meta-analyses focusing exclusively on children or adolescents; (f) systematic reviews; (g) meta-analyses of cross-sectional or correlational studies; and (h) not published in a peer-reviewed English language journal. Regarding group and clinician-led interventions, we included meta-analyses if the authors tested delivery and application effects and found no significant differences between self-guided and other applications. If a meta-analysis examined those differences and reported differential effects for self-guided interventions, we only included those effect sizes relevant for self-guided interventions.
We identified a substantial number of meta-analyses which examined the effectiveness of specific interventions, particularly for contemporary therapeutic approaches such as mindfulness and acceptance and commitment therapy (e.g., Hayes et al., 2012). Using all eligible meta-analyses may mean that identical primary studies might be included in a series of meta-analyses, leading to potential double-counting and duplication of effect sizes that would bias the overall patterns. To overcome this problem, we adopted the following strategies. First, we screened meta-analyses in a reverse temporal order, starting with the most recent meta-analyses per category. We then identified overlap in included primary studies between subsequent meta-analyses per outcome variable. If there was a 50% overlap or larger between two meta-analyses for a specific outcome variable, we included only the meta-analysis with the larger sample size. We still examined smaller meta-analyses to check if they reported moderator analyses of interest for our purposes, particularly the effectiveness of self-guided vs. other-guided or group interventions and differences in effectiveness between different cultural samples. As not all meta-analyses provided estimates for each of the outcomes of interest in this review, we repeated this process for each outcome variable. See Figure 1 for a PRISMA diagram of the selection process.
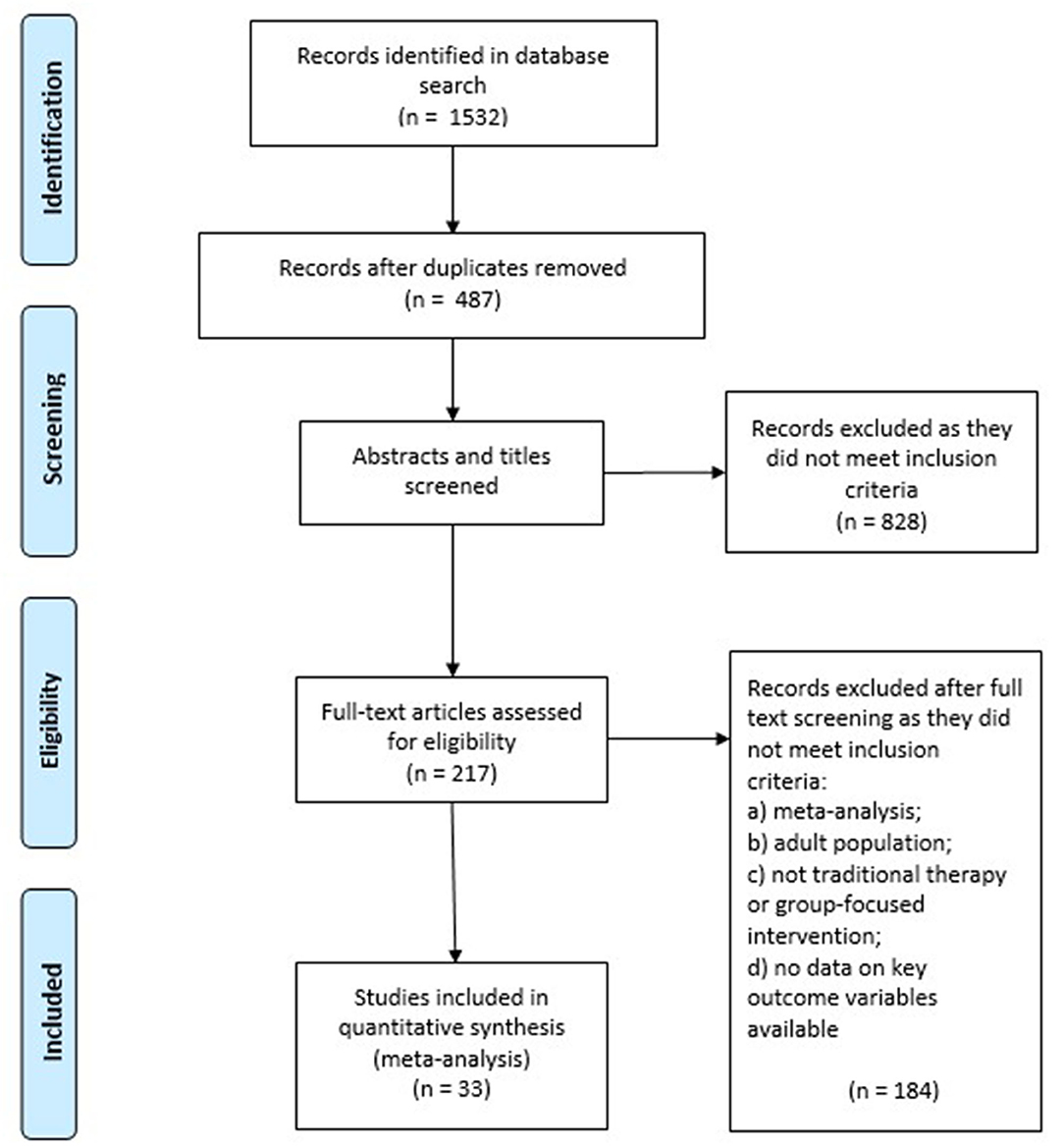
Figure 1. Prisma diagram.
We present the average effect size and 95% confidence interval as reported in the original meta-analyses in the form of a forest plot. The most common effect sizes are variations of the standardized mean difference (typically d or g), therefore, we use these metrics for plotting the effects. If no confidence interval was reported, only the mean effect size is displayed.
However, this visual display does not easily allow a statistical summary of the overall effect sizes. Therefore, we converted standardized mean differences into r and then z-transformed r (Rosenthal, 1991). As expected, the transformed effect size and the original effect size correlated r = 1.0. Inverse variance weights were calculated from sample sizes. If only the overall sample size was available, we used the average sample size per study to estimate sample sizes for subgroups. The average effect sizes per intervention category were computed using rma with REML estimation in the metafor package in R (Viechtbauer, 2010). We report the unstandardized regression weights.
Our sample of meta-analyses included 34 meta-analyses (total number of studies k = 1,390, n = 145,744). The majority of meta-analyses included general population samples, including working adults (meta-analysis k = 16). The second largest sample group were mixed general population and clinical samples (meta-analysis k = 11). Purely clinical samples were included in 4 meta-analyses and students were the primary population in 3 meta-analyses. All but one meta-analysis (Dickens, 2017) exclusively focused on adult populations. Only 5 meta-analyses explicitly reported and tested cross-cultural differences.
We used two approaches to evaluate the relative effectiveness of self-guided interventions. First, we used Cohen (1988) effect size benchmarks to specify small (d = 0.2), medium (d = 0.5), and large (d = 0.8) effect sizes of standardized mean differences. This first allows us to assess the overall effectiveness of self-guided interventions compared to control interventions (typically, waitlist, or active control groups). Second, we compared the overall effect sizes of self-guided interventions against effectiveness benchmarks of traditional clinician-guided psychotherapy for reducing depression symptoms (Cuijpers et al., 2020). The overall effect size of traditional clinician-guided psychotherapy on depression was g = 0.72 (k = 385), with Cognitive-Behavioral Therapy (CBT) showing an effectiveness of g = 0.73 (k = 205); Behavioral Activation Theory g = 1.05 (k = 21), and third-wave therapies (including Acceptance and Commitment Therapy [ACT] and Mindfulness-Based Interventions [MBI]) an effectiveness of g = 0.85 (k = 19).
Table 1 shows an overview of the meta-analyses included in this review. The large majority of psychological intervention meta-analyses that were eligible to be included in our review consisted of meta-analyses of clinical psychology therapy-derived interventions (k = 17), which encompass self-guided CBT, ACT, and MBI, as well as diverse Positive Psychology-based interventions (k = 8).
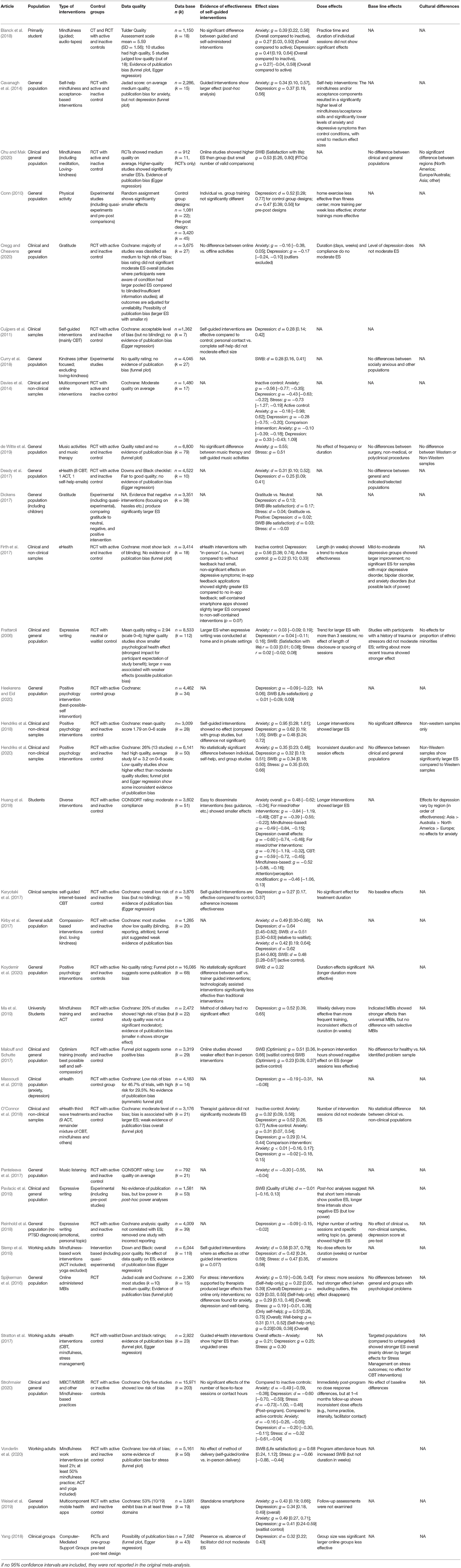
Table 1. Overview of meta-analytical findings.
A large number of studies used therapy-derived interventions including CBT, MBI, and ACT, and showed small to medium effect sizes for reducing anxiety, depression, and stress. Effects for subjective well-being in some analyses showed moderate to large effect sizes (Chu and Mak, 2020; Vonderlin et al., 2020). When compared to active control groups instead of non-active controls or waitlist groups, effect sizes typically diminished but remained statistically significant (e.g., Deady et al., 2017; O'Connor et al., 2018). Overall, the self-guided effect sizes tended to be lower than the effectiveness of traditional clinician-guided therapies, but clearly showed an effectiveness over and above active control groups (e.g., Spijkerman et al., 2016; Stratton et al., 2017). Other meta-analyses found no difference for self-guided compared to clinician-guided interventions (e.g., in general: Spijkerman et al., 2016; O'Connor et al., 2018 found no difference for anxiety and depression). Based on these meta-analyses, self-guided therapy-derived interventions are recommended to improve well-being during isolation.
Positive psychology-based interventions are typically focused on positive functioning, including interventions focusing on optimism, gratitude, or kindness. There is a somewhat older literature on expressive writing (Pennebaker, 1997) which we included here for convenience purposes. Overall, the effect sizes of positive psychology-based interventions were typically small and appear even more strongly affected by the type of control group than therapy-derived interventions (for a particularly striking example, see Dickens, 2017). Some of the positive psychology gratitude interventions differ by the focus of the intervention: either self- or interpersonally-oriented gratitude. These differences appear to be similarly effective (e.g., Cregg and Cheavens, 2020). Cregg and Cheavens (2020) found online compared to off-line applications equally effective, whereas Koydemir et al. (2020) reported greater effectiveness of non-technologically mediated interventions. Hendriks et al. (2020) reported that web-based interventions were as effective as online positive psychology apps. Expressive writing interventions showed the smallest effect sizes overall in this group, whereas compassion and kindness-based interventions showed moderate effect sizes in some meta-analyses (Kirby et al., 2017). Based on these meta-analyses, expressive writing interventions are the least effective, whereas gratitude, especially compassion-based interventions, could be recommended to improve well-being during quarantine and isolation.
Other activity-based interventions comprised a broad category including various physical exercise, arts, and music-based activities. Physical exercise showed weak effects overall in improving subjective well-being, with slightly larger effects for reducing depression (Conn, 2010). Music-based interventions also showed weak to moderate effects in reduced anxiety and stress levels (Panteleeva et al., 2017; de Witte et al., 2019). Therefore, activity-based interventions, including music and physical exercise, show small to moderate effects and could be recommended to improve mental health during isolation.
Multicomponent online and app-based interventions showed small to moderate effects, with diminished effects when compared to standard therapeutic interventions (see for example, O'Connor et al., 2018). Overall, their effectiveness was considerably smaller than similar non-online interventions (e.g., Malouff and Schutte, 2017) or standard in-person therapies. The relative effectiveness of online only compared to smartphone-based apps remains unclear (Firth et al., 2017; Weisel et al., 2019), and thus no clear guidance is available.
Dose effects, or the extent to which people are practicing or using a specific activity, are important to consider when recommending self-guided practice. These might include total practice time, or duration of individual interventions. Several meta-analyses examined the effectiveness of interventions at different dose levels. For therapy- derived interventions, Blanck et al. (2018) and O'Connor et al. (2018) found no dose effects for self-guided CBT-based interventions. In contrast, Firth et al. (2017) reported a reduction (although not statistically significant) in the effectiveness of longer-term smartphone-based interventions, whereas Huang et al. (2018) reported greater effectiveness of longer ACT and CBT-based interventions on depression. Strohmaier (2020), Spijkerman et al. (2016, after removing outliers), and Slemp et al. (2019) found no difference in dose effects for MBI-based interventions. Focusing on life satisfaction, Vonderlin et al. (2020) reported greater life satisfaction was correlated with higher number of mindfulness-based practice hours, whereas Ma et al. (2019) reported inconsistent dose effects for mindfulness-based interventions in students, with a slight increase in effectiveness for weekly practices compared to more frequent sessions.
Positive psychology interventions also showed inconsistent dose effects. Hendriks et al. (2020) reported inconsistent patterns for interventions of more or less than 8 weeks for different outcome variables. Similarly, for expressive writing exercises, the dose effects are inconsistent across the studies that reported them (Frattaroli, 2006; Malouff and Schutte, 2017; Reinhold et al., 2018). For physical exercise, a meta-analysis by Conn (2010) found that home-based unsupervised exercise was less effective than unsupervised exercise in fitness centers. The same meta-analysis also suggested that shorter training overall might be more effective in improving depressive symptoms. de Witte et al. (2019) reported no significant dose effects for music interventions. Examining the overall pattern, dose effects appear inconsistent and no clear guidance is available about optimal levels of practice.
One important concern in recommending self-guided interventions is whether these interventions are applicable for populations experiencing clinically relevant symptoms. In particular, a specific intervention may show no effect or an adverse effect in clinical populations, making the intervention unsafe for such populations. Hence, we investigated whether meta-analyses examined baseline effects of anxiety, depression, or stress on effectiveness, or directly compared the effectiveness between clinical and non-clinical populations.
Among therapy-derived interventions, several meta-analyses found no significant baseline effects or difference between clinical and non-clinical samples (Spijkerman et al., 2016; Deady et al., 2017; O'Connor et al., 2018; Strohmaier, 2020). For positive psychology interventions, several meta-analyses also found no difference between clinical and non-clinical samples (Frattaroli, 2006; Reinhold et al., 2018; Cregg and Cheavens, 2020; Hendriks et al., 2020). Only Pavlacic et al. (2019) reported larger effect sizes for groups with a Post-Traumatic Stress Disorder (PTSD) diagnosis compared to non-PTSD groups. No difference between clinical (labeled socially anxious) and non-clinical populations was found for kindness-based interventions (Curry et al., 2018). Taken together, this suggests that therapy- derived and positive psychology interventions in general could be recommended to populations irrespective of their depression or anxiety levels or clinical diagnosis status. For music interventions, de Witte et al. (2019) reported no differences between different populations in terms of effectiveness. For generic smart-phone applications (including a large number of clinical therapeutic approaches), Firth et al. (2017) reported that effectiveness of these apps was better for individuals diagnosed with mild-to-moderate levels of depression, but groups diagnosed with major depressive disorder, bipolar disorder, and anxiety disorder showed no significant improvement when using these applications. However, these sample sizes were typically small and might have been too small to show the effectiveness of these eHealth apps. Overall, clinical status or level of anxiety or depression do not exert a strong influence on the effectiveness of these self-guided interventions. This is encouraging news to support the wide-spread recommendation of these self-guided interventions in general, in the absence of immediate clinical guidance or supervision.
The current COVID-19 pandemic is affecting all countries. For this reason, we also examined the extent to which the interventions might be applicable and effective in different cultural regions. Unfortunately, only a small number of meta-analyses (k = 5) attended to possible cultural differences in the effectiveness. Chu and Mak (2020) found no significant differences in mindfulness-based interventions between world regions and de Witte et al. (2019) comparing the effectiveness of music interventions reported no differences between Western and non-Western samples. In contrast, Hendriks et al. (2020) compared positive psychology interventions and reported larger effect sizes in non-Western compared to Western samples. However, it is unclear whether these comparisons might be confounded by other study characteristics. An earlier meta-analysis by Hendriks et al. (2018) only focused on non-Western interventions and reported low quality studies. Overall, it is noteworthy that there are relatively few high-quality studies available that have examined the effectiveness of self-guided psychological interventions in samples beyond Western Europe, North America, and Australia.
We were unable to include any studies that exclusively looked at yoga or meditation because meta-analyses of these studies always included group settings or guidance by a trainer or clinician. Based on our inclusion criteria, we were unable to include them in our review. However, the evidence from recent meta-analyses suggests that these interventions are effective for anxiety, depression, and broader mental and physical health (see for example, Sedlmeier et al., 2018; Zoogman et al., 2019) and clinical network meta-analyses attest to their safety and effectiveness (Chen and Shan, 2019). A further advantage of these types of interventions is that they seem to show higher effectiveness in non-Western populations (e.g., Zoogman et al., 2019). Given the wide availability of online yoga and meditation sessions/apps and the overall effectiveness of guided yoga and meditation sessions in situ, we could cautiously recommend the practice of yoga and meditation for improving mental health during quarantine and social distancing conditions.
Figures 2–5 show the effect sizes and confidence intervals (if reported) from the meta-analyses (we converted r coefficients reported in Frattaroli, 2006 into d). We recoded effect sizes for anxiety, depression and stress so that positive numbers indicated a positive change (improvement) for the experimental group compared to the control group. As Figures 2–5 demonstrate, most meta-analyses showed an advantage of the intervention compared to the control group, but the type of control group appeared to impact the observed effect size.
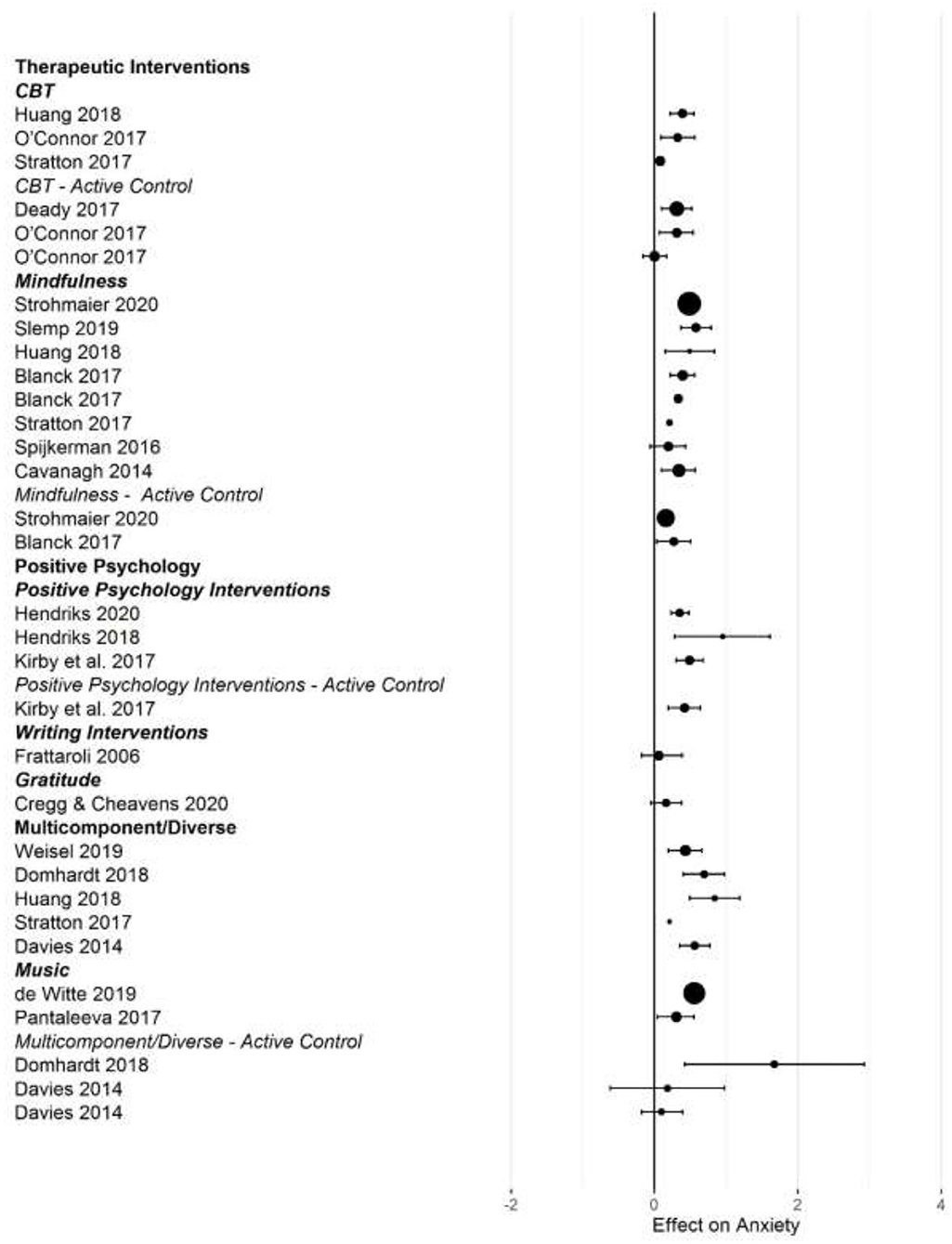
Figure 2. Forest plot of intervention effects on anxiety.
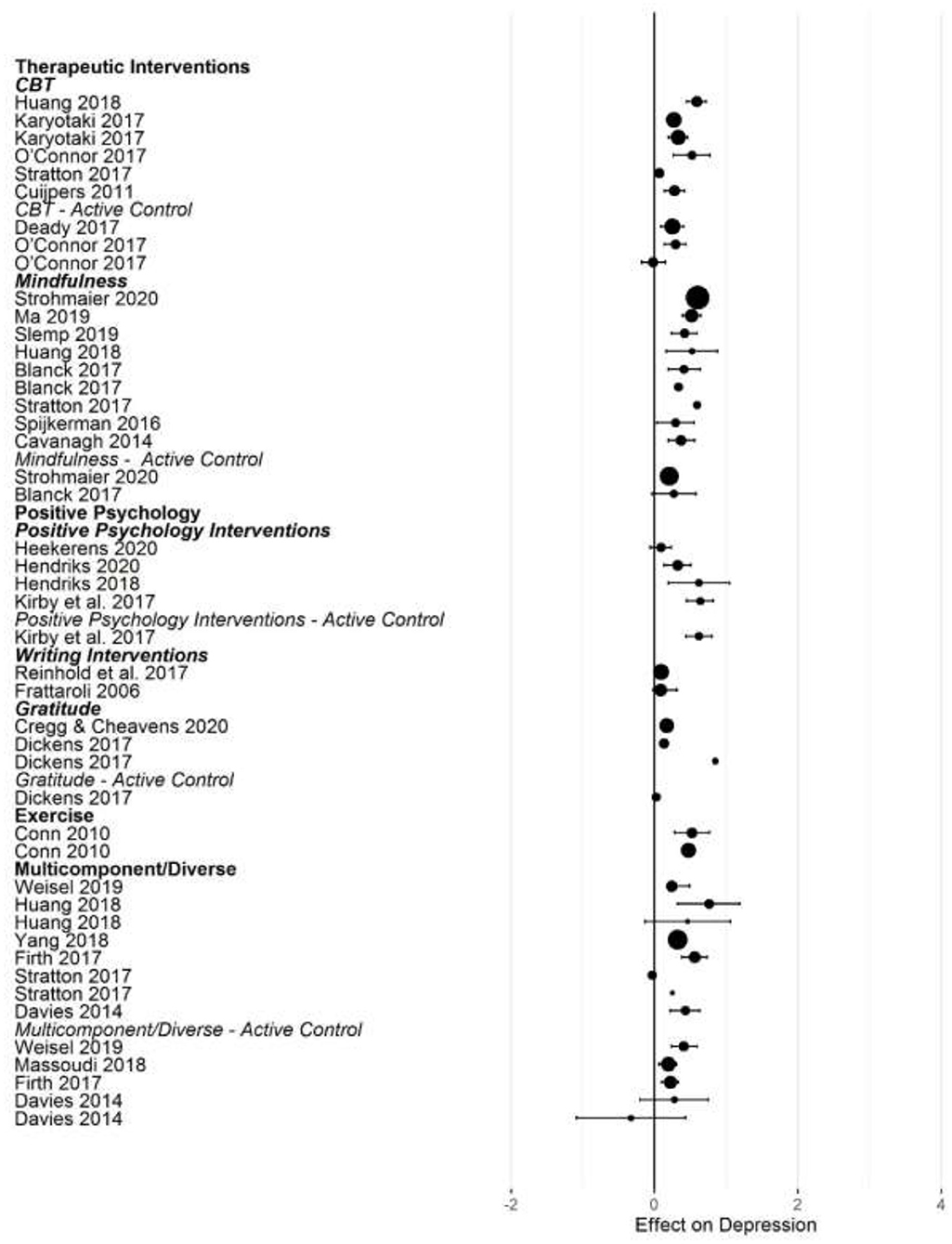
Figure 3. Forest plot of intervention effects on depression.
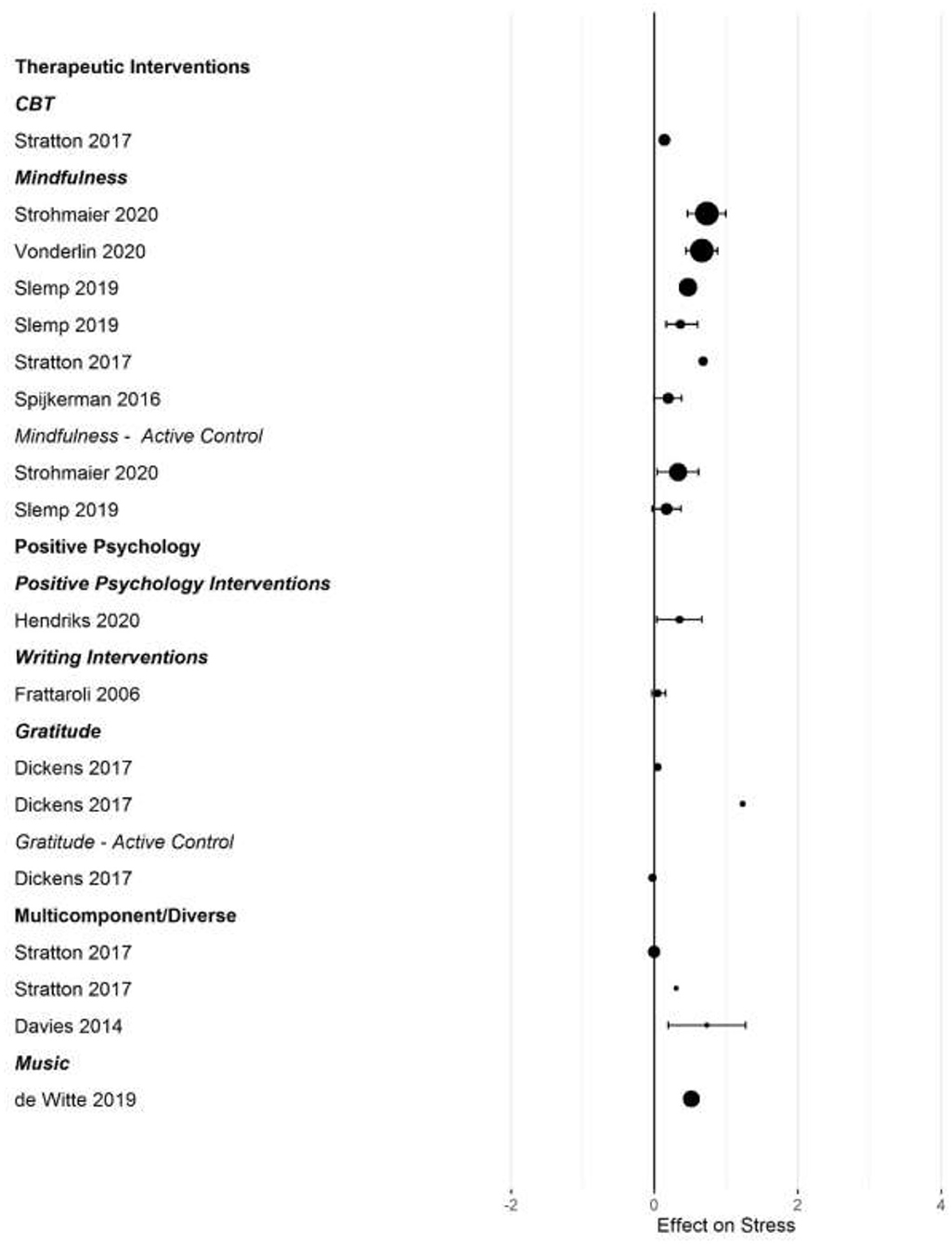
Figure 4. Forest plot of intervention effects on stress.
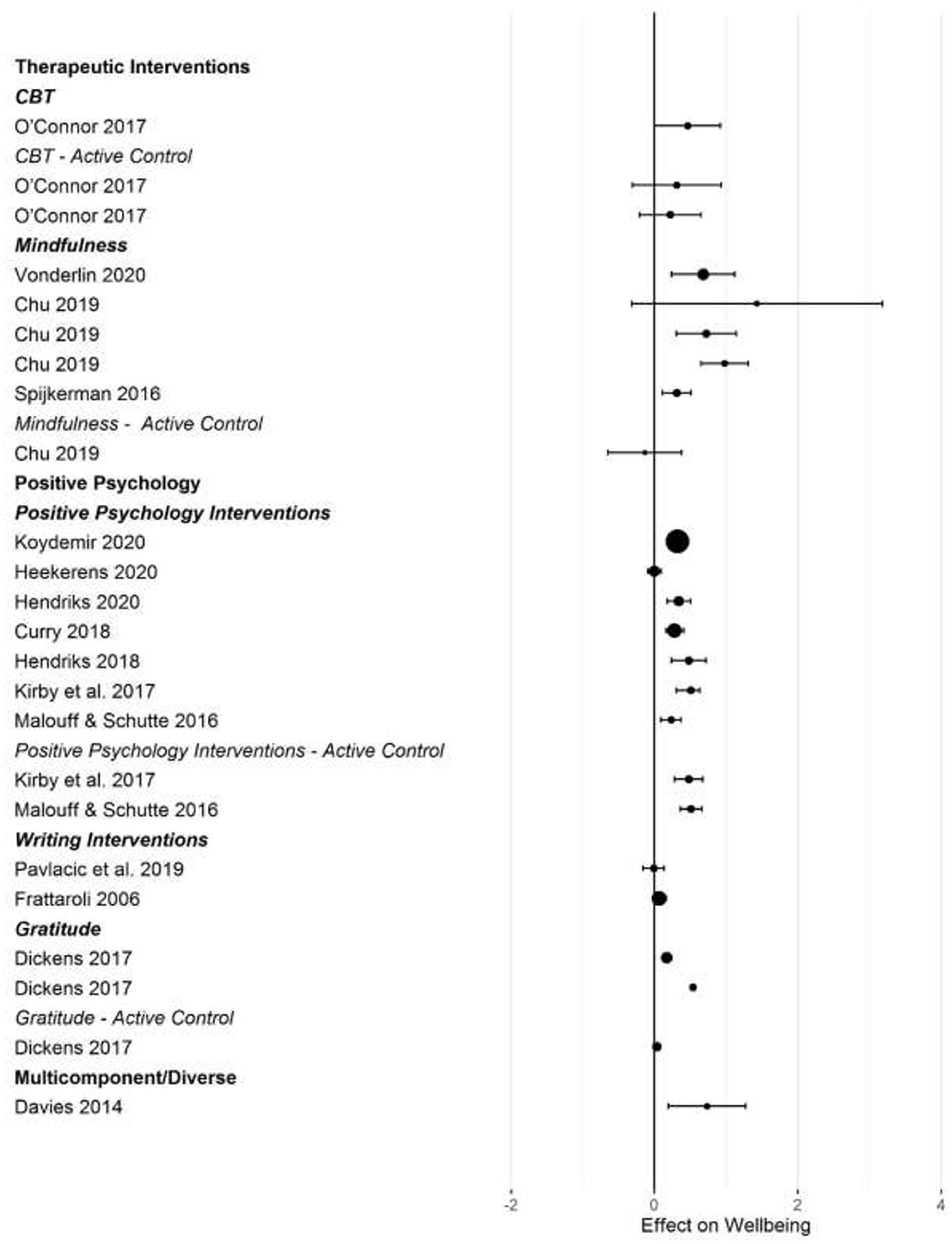
Figure 5. Forest plot of intervention effects on subjective well-being.
After converting standardized mean differences to z-transformed r, the average effect size r was comparable across the four outcome variables, for anxiety r = 0.19 (95% CI: 0.14, 0.24; k = 31); depression r = 0.17 (95% CI: 0.13, 0.20; k = 45); subjective well-being r = 0.19 (95% CI: 0.13, 0.25; k =25), and stress r = 0.19 (95% CI: 0.11,0.26; k =17). Effect sizes computed for comparisons with active control groups yielded smaller effects, but this difference was only significant for depression (Q [1] = 5.70, p = 0.017, R2 = 0.096).
When examining differences between types of interventions, we used therapeutic approaches (CBT, ACT, and MBI) as the reference category. For positive psychology interventions, we separated gratitude and expressive writing interventions from other positive interventions. Due to the small number of effect size summaries available, we included activity-based interventions (exercise, music) with other/multicomponent interventions. For anxiety, we found a significantly larger effect for mixed, multicomponent and other interventions compared to CBT and ACT (b = 0.19 [95% CI: 0.05–0.55]; p = 0.009). For subjective well-being, we found a trend for mindfulness interventions to show larger effect sizes compared to CBT (b = 0.16 [95% CI: = 0.02 −0.34], p = 0.086). For depression, we first controlled for active control group comparisons (see the results reported above). Expressive writing exercises had a significantly smaller effect size on average compared to CBT/ACT based interventions (r = −0.15 [95% CI: −0.29 to −0.00], p = 0.017). We did not find statistically significant differences in the effectiveness of different interventions for stress.
Our rapid review of available meta-analyses demonstrated that there are a number of evidence-based self-guided interventions that can be used by individuals at home to manage depression, anxiety, stress, and well-being during stay-at-home orders, lockdown, and quarantine. Overall, self-guided interventions are better at improving psychological health compared to no intervention (e.g., waitlist controls) and, to some extent, active controls (e.g., comparable treatments). In particular, self-guided therapy-derived interventions (including CBT, ACT, and MBI), mindfulness-based practices, positive psychology interventions, and activity-based interventions (e.g., physical exercise, music listening) appear effective in reducing anxiety, depression, stress, and in increasing subjective well-being compared to both active and inactive control groups. However, dose effects were largely inconsistent. Therefore, we cannot recommend specific intervals or durations for any of the intervention categories. Baseline effects were largely absent, implying that even individuals with elevated stress or psychological problems can use these practices at home without supervision, however we strongly recommend contacting health professionals if an individual is experiencing distress.
The unique context created by social distancing and quarantine necessitates reflection on the way self-guided interventions might be used. Although expressive writing interventions showed effectiveness compared to control groups, effectiveness was consistently lower compared to CBT and ACT-based interventions. Expressive writing about concerns or worries (including detailed reflections of difficult or traumatic events) may not be appropriate without adequate clinical support or guidance (Reinhold et al., 2018), especially when acutely experiencing negative emotional symptoms. Hence, we do not recommend these exercises for individuals to perform unsupervised at this current time of elevated collective worry and distress (see Wang et al., 2020).
Overall, self-guided activities included in these meta-analyses appear effective, but not as effective as in-person or group-based interventions. Therefore, these activities can be useful as a first line of psychological support during stay-at-home and lockdown periods, but they could not and should not replace more guided clinical interventions (either via telehealth or once in-person sessions become available again). Given the current strain on the mental health system and the likelihood of further restrictions in the near future, it is important to provide widely available evidence-based practices to avoid negative collateral effects on mental health at the population level (see Brooks et al., 2020; Duan and Zhu, 2020). This review provides an overview of best-practice self-guided interventions conducted prior to the pandemic that can be recommended and implemented at large scale to help and support populations at risk of mental health problems. However, self-guided interventions need to be complemented by further investment and strengthening of traditional mental health care support.
At the same time, the review clearly highlights blind spots in our understanding of evidence-based practices. More highly controlled research on self-guided and home-based interventions is needed to inform public health decision-making during pandemics that require quarantine and social distancing over potentially long periods of time. What are the ideal levels of compliance for self-guided mental health interventions beyond an initial lockdown period and how can mental health be maintained? When should self-guided interventions first be implemented or recommended to populations at risk and how long should these practices be maintained after the immediate lifting of more restrictive lockdowns? What are the effects of repeated lockdowns: should recommended self-guided interventions be switched or rotated? The meta-analyses summarize studies that were not specifically geared toward evaluating interventions that are focused on home practices during lockdown.
We isolate three main limitations of the current evidence-base to guide future research. A first gap, especially in the current context of global pandemic, is the lack of attention to culturally transferable interventions. Most studies have been conducted with samples from high-income, highly educated, and mainly Western nations. Given the greater population density and living arrangements in non-Western environments, these conditions may make effective mental health interventions even more urgent. We need further national and international multi-center research that includes diverse groups of participants to better understand whether interventions developed for autonomous individuals socialized into societies that emphasize individuality and self-reliance are as applicable and as effective in more community oriented contexts (Smith et al., 2013). A second major concern of current distancing measures which we were unable to address here is the potential for a negative impact on social relationships. The current lockdown measures require greater interpersonal skills, both in terms of living together with others in closed spaces for extended periods of time as well as maintaining contact with others outside the immediate social “bubble.” The current evidence is clearly geared toward the individual as the focus of the intervention, with little emphasis on social relationships (although gratitude interventions might be the single major exception). Thus, we need more evidence of the effectiveness of social interaction interventions. A third limitation is that our evidence is based on interventions that were conducted prior to the current pandemic. It is unclear whether the effectiveness of self-guided interventions is equally effective under the specific conditions of a pandemic. The baseline effects that we report make us cautiously optimistic about the continuing effectiveness of these interventions, even in conditions of increased overall stress and anxiety. A meta-analysis of controlled studies during the current pandemic would be highly beneficial.
Finally, it is worth considering the broader role of psychologists in responding to the COVID-19 pandemic. A major concern for individuals, groups, organizations, and nations is the economic impact of the current pandemic. The mental health impact of quarantine is more dramatic for lower income groups (see Reynolds et al., 2008). The medium and long-term negative economic impact of COVID-19 on the larger population, and especially financially and economically more vulnerable populations also needs greater attention from psychologists. Psychologists need to collaborate with economists and others involved in economic decision-making to consider options to support people to upskill and create new employment opportunities which help to alleviate this financial worry.
In summary, the current evidence suggests that a number of self-guided interventions suitable for at-home practice during lockdown and physical distancing are effective to for improving mental health. Specifically, we recommend interventions based on cognitive behavioral therapy, mindfulness, and acceptance-based activities, selected positive psychology activities, physical exercise, and music as useful first-line mental health interventions. However, these activities are not as effective as in-person and group based therapeutic interventions, and so they should not replace clinician-guided interventions for individuals and groups in need. Many of these interventions are now available via smartphone and web-based applications. In order to provide broad access to such evidence-based interventions to mitigate the negative side-effects of social distancing measures, this article includes an online supplement with selected exercises and further information to help individuals cope with the mental health challenges of physical distancing and quarantine.
Publicly available datasets were analyzed in this study. This data can be found at: https://osf.io/fpx4s/.
RF conceptualized the study and wrote the first draft. RF, TB, JK, MZ, KR, AR, and LG conducted the literature search and data extraction. RF, JK, and TB conducted the analyses and created the visualizations. DW coordinated the activity material collation. DW, TN, BI, and MC collated and summarized the activity material. PM provided feedback and advice. All authors approved the final version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2020.563876/full#supplementary-material
*Blanck, P., Perleth, S., Heidenreich, T., Kröger, P., Ditzen, B., Bents, H., et al. (2018). Effects of mindfulness exercises as stand-alone intervention on symptoms of anxiety and depression: Systematic review and meta-analysis. Behav. Res. Ther. 102, 25–35. doi: 10.1016/j.brat.2017.12.002
Brooks, S. K., Webster, R. K., Smith, L. E., Woodland, L., Wessely, S., Greenberg, N., et al. (2020). The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet 3957, 912–920. doi: 10.1016/S0140-6736(20)30460-8
*Cavanagh, K., Strauss, C., Forder, L., and Jones, F. (2014). Can mindfulness and acceptance be learnt by self-help?: a systematic review and meta-analysis of mindfulness and acceptance-based self-help interventions. Clin. Psych. Rev. 34, 118–129. doi: 10.1016/j.cpr.2014.01.001
Chen, C., and Shan, W. (2019). Pharmacological and non-pharmacological treatments for major depressive disorder in adults: a systematic review and network meta-analysis. Psychiatry Res. 281:112595. doi: 10.1016/j.psychres.2019.112595
*Chu, S. T. W., and Mak, W. W. S. (2020). How mindfulness enhances meaning in life: a meta-analysis of correlational studies and randomized controlled trials. Mindfulness 11, 177–193. doi: 10.1007/s12671-019-01258-9
Cohen, J. (1988). Statistical Power Analysis for the Behavioral Sciences. New Jersey: Lawrence Erlbaum Associates.
*Conn, V. S. (2010). Depressive symptom outcomes of physical activity interventions: meta-analysis findings. Ann. Behav. Med. 39, 128–138. doi: 10.1007/s12160-010-9172-x
*Cregg, D. R., and Cheavens, J. S. (2020). Gratitude interventions: effective self-help? A meta-analysis of the impact on symptoms of depression and anxiety. J. Happ. Studies. doi: 10.1007/s10902-020-00236-6. [Epub ahead of print].
*Cuijpers, P., Donker, T., Johansson, R., Mohr, D. C., van Straten, A., and Andersson, G. (2011). Self-guided psychological treatment for depressive symptoms: a meta-analysis. PLoS ONE 6:e21274. doi: 10.1371/journal.pone.0021274
Cuijpers, P., Noma, H., Karyotaki, E., Vinkers, C. H., Cipriani, A., and Furukawa, T. A. (2020). A network meta-analysis of the effects of psychotherapies, pharmacotherapies and their combination in the treatment of adult depression. World Psychiatry. 19, 92–107. doi: 10.1002/wps.20701
*Curry, O. S., Rowland, L. A., Van Lissa, C. J., Zlotowitz, S., McAlaney, J., and Whitehouse, H. (2018). Happy to help? A systematic review and meta-analysis of the effects of performing acts of kindness on the well-being of the actor. J. Exp. Soc. Psych. 76, 320–329. doi: 10.1016/j.jesp.2018.02.014
Davies, E. B., Morriss, R., and Glazebrook, C. (2014). Computer-delivered and web-based interventions to improve depression, anxiety, and psychological well-being of university students: a systematic review and meta-analysis. J. Med. Intern. Res. 16:e130. doi: 10.2196/jmir.3142
*de Witte, M., Spruit, A., van Hooren, S., Moonen, X., and Stams, G. Y. (2019). Effects of music interventions on stress-related outcomes: a systematic review and two meta-analyses. Health Psych. Rev. 14, 294–324. doi: 10.1080/17437199.2019.1627897
*Deady, M., Choi, I., Calvo, R. A., Glozier, N., Christensen, H., and Harvey, S. B. (2017). eHealth interventions for the prevention of depression and anxiety in the general population: a systematic review and meta-analysis. BMC Psychiatry 17:310. doi: 10.1186/s12888-017-1473-1
*Dickens, L. R. (2017). Using gratitude to promote positive change: A series of meta-analyses investigating the effectiveness of gratitude interventions. Basic Appl. Soc. Psych. 39, 193–208. doi: 10.1080/01973533.2017.1323638
Dong, L., and Bouey, J. (2020). Public mental health crisis during COVID-19 pandemic, China. Emerg. Infect. Dis. 26, 1616–1618. doi: 10.3201/eid2607.200407
Duan, L., and Zhu, G. (2020). Psychological interventions for people affected by the COVID-19 epidemic. Lancet Psychiatry 7, 300–302. doi: 10.1016/S2215-0366(20)30073-0
*Firth, J., Torous, J., Nicholas, J., Carney, R., Pratap, A., Rosenbaum, S., et al. (2017). The efficacy of smartphone-based mental health interventions for depressive symptoms: a meta-analysis of randomized controlled trials. World Psychiatry 16, 287–298. doi: 10.1002/wps.20472
*Frattaroli, J. (2006). Experimental disclosure and its moderators: a meta-analysis. Psychol. Bull. 132, 823–865. doi: 10.1037/0033-2909.132.6.823
Hayes, S. C., Strosahl, K. D., and Wilson, K. G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change. New York, NY: Guilford Press.
*Heekerens, J. B., and Eid, M. (2020). Inducing positive affect and positive future expectations using the best-possible-self intervention: a systematic review and meta-analysis. J. Pos. Psych. doi: 10.1080/17439760.2020.1716052. [Epub ahead of print].
*Hendriks, T., Schotanus-Dijkstra, M., Hassankhan, A., de Jong, J., and Bohlmeijer, E. (2020). The efficacy of multi-component positive psychology interventions: A systematic review and meta-analysis of randomized controlled trials. J.Happ. Stud. 21, 357–390. doi: 10.1007/s10902-019-00082-1
Hendriks, T., Schotanus-Dijkstra, M, Hassankhan, A., Graafsma, T., Bohlmeijer, E., and de Jong, J. (2018). The efficacy of positive psychology interventions from non-Western countries: a systematic review and meta-analysis. Intern. J. Wellbeing 8, 71–98. doi: 10.5502/ijw.v8i1.711
Henrich, J., Heine, S. J., and Norenzayan, A. (2010). The weirdest people in the world? Behav. Brain Sci. 33, 61–83. doi: 10.1017/S0140525X0999152X
Ho, C. S., Chee, C. Y., and Ho, R. C. (2020). Mental health strategies to combat the psychological impact of covid-19 beyond paranoia and panic. Ann. Acad. Med. Singapore, 49, 155–160.
*Huang, J., Nigatu, Y. T., Smail-Crevier, R., Zhang, X., and Wang, J. (2018). Interventions for common mental health problems among university and college students: a systematic review and meta-analysis of randomized controlled trials. J. Psychiatr. Res. 107, 1–10. doi: 10.1016/j.jpsychires.2018.09.018
*Karyotaki, E., Riper, H., Twisk, J., Hoogendoorn, A., Kleiboer, A., Mira, A., et al. (2017). Efficacy of self-guided internet-based cognitive behavioral therapy in the treatment of depressive symptoms: a meta-analysis of individual participant data. JAMA Psychiatry 74, 351–359. doi: 10.1001/jamapsychiatry.2017.0044
*Kirby, J. N., Tellegen, C. L., and Steindl, S. R. (2017). A meta-analysis of compassion-based interventions: current state of knowledge and future directions. Behav. Ther. 48, 778–792. doi: 10.1016/j.beth.2017.06.003
Kissler, S. M., Tedijanto, C., Goldstein, E., Grad, Y. H., and Lipsitch, M. (2020). Projecting the transmission dynamics of SARS-CoV-2 through the postpandemic period. Science 6493, 860–868. doi: 10.1126/science.abb5793
*Koydemir, S., Sökmez, A. B., and Schütz, A. (2020). A meta-analysis of the effectiveness of randomized controlled positive psychological interventions on subjective and psychological well-being. App. Res. Qual. Life. doi: 10.1007/s11482-019-09788-z. [Epub ahead of print].
*Ma, L., Zhang, Y., and Cui, Z. (2019). Mindfulness-based interventions for prevention of depressive symptoms in university students: a meta-analytic review. Mindfulness 10, 2209–2224. doi: 10.1007/s12671-019-01192-w
Malouff, J. M., and Schutte, N. S. (2017). Can psychological interventions increase optimism? A meta-analysis. J. Pos. Psych. 12, 594–604. doi: 10.1080/17439760.2016.1221122
*Massoudi, B., Holvast, F., Bockting, C. L. H., Burger, H., and Blanker, M. H. (2019). The effectiveness and cost-effectiveness of e-health interventions for depression and anxiety in primary care: a systematic review and meta-analysis. J. Aff. Dis. 245, 728–743. doi: 10.1016/j.jad.2018.11.050
Milne, G. J., and Xie, S. (2020). The Effectiveness of Social Distancing in Mitigating COVID-19 Spread: a modelling analysis. medRxiv 1–16. doi: 10.1101/2020.03.20.20040055
*O'Connor, M., Munnelly, A., Whelan, R., and McHugh, L. (2018). The efficacy and acceptability of third-wave behavioral and cognitive eHealth treatments: A systematic review and meta-analysis of randomized controlled trials. Behav. Ther. 49, 459–475. doi: 10.1016/j.beth.2017.07.007
Panteleeva, Y., Ceschi, G., Glowinski, D., Courvoisier, D. S., and Grandjean, D. (2017). Music for anxiety? Meta-analysis of anxiety reduction in non-clinical samples. Psych. Music 46, 473–487. doi: 10.1177/0305735617712424
*Pavlacic, J. M., Buchanan, E. M., Maxwell, N. P., Hopke, T. G., and Schulenberg, S. E. (2019). A meta-analysis of expressive writing on posttraumatic stress, posttraumatic growth, and quality of life. Rev. Gen. Psych. 23, 230–250. doi: 10.1177/1089268019831645
Pennebaker, J. W. (1997). Writing about emotional experiences as a therapeutic process. Psych. Sci. 8, 162–166. doi: 10.1111/j.1467-9280.1997.tb00403.x
*Reinhold, M., Bürkner, P. C., and Holling, H. (2018). Effects of expressive writing on depressive symptoms–a meta-analysis. Clin. Psych Sci. Prac. 25:e12224. doi: 10.1111/cpsp.12224
Reynolds, D. L., Garay, J. R., Deamond, S. L., Moran, M. K., Gold, W., and Styra, R. (2008). Understanding, compliance and psychological impact of the SARS quarantine experience. Epidem. Infect. 136, 997–1007. doi: 10.1017/S0950268807009156
Rosenthal, R. (1991). Meta-Analytical Procedures for Social Research. California, CA: SAGE Publishing. doi: 10.4135/9781412984997
*Sedlmeier, P., Loße, C., and Quasten, L. C. (2018). Psychological effects of meditation for healthy practitioners: an update. Mindfulness 9, 371–387. doi: 10.1007/s12671-017-0780-4
*Slemp, G. R., Jach, H. K., Chia, A., Loton, D. J., and Kern, M. L. (2019). Contemplative interventions and employee distress: a meta-analysis. Stress Health 35, 227–255. doi: 10.1002/smi.2857
Smith, P. B., Fischer, R., Vignoles, V., and Bond, M. H. (2013). Understanding Social Psychology Across Cultures: Engaging With Others in a Changing World. London: SAGE Publishing.
Spijkerman, M. P. J., Pots, W. T. M., and Bohlmeijer, E. T. (2016). Effectiveness of online mindfulness-based interventions in improving mental health: a review and meta-analysis of randomised controlled trials. Clin. Psych. Rev. 45, 102–114. doi: 10.1016/j.cpr.2016.03.009
Stratton, E., Lampit, A., Choi, I., Calvo, R. A., Harvey, S. B., and Glozier, N. (2017). Effectiveness of eHealth interventions for reducing mental health conditions in employees: a systematic review and meta-analysis. PLoS ONE 12:e0189904. doi: 10.1371/journal.pone.0189904
Strohmaier, S. (2020). The relationship between doses of mindfulness-based programs and depression, anxiety, stress, and mindfulness: a dose-response meta-regression of randomized controlled trials. Mindfulness 11, 1315–1335. doi: 10.1007/s12671-020-01319-4
Viechtbauer, W. (2010). Conducting meta-analyses in R with the metafor package. J. Stat. Softw. 36, 1–48. doi: 10.18637/jss.v036.i03
Vonderlin, R., Biermann, M., Bohus, M., and Lyssenko, L. (2020). Mindfulness-based programs in the workplace: a meta-analysis of randomized controlled trials. Mindfulness 11, 1579–1598. doi: 10.1007/s12671-020-01328-3
*Wang, C., Pan, R., Wan, X., Tan, Y., Xu, L., Ho, C. S., et al. (2020). Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Internat. J. Env. Res. Public Health 17:e1729. doi: 10.3390/ijerph17051729
Weisel, K. K., Fuhrmann, L. M., Berking, M., Baumeister, H., Cuijpers, P., and Ebert, D. D. (2019). Standalone smartphone apps for mental health - a systematic review and meta-analysis. NPJ Digital Med. 2:118. doi: 10.1038/s41746-019-0188-8
World Health Organization (2003). Organization of Services for Mental Health WHO Mental Health Policy and Service Guidance Package. WM 30 2003ME V2. Geneva.
Xiang, Y. T., Yang, Y., Li, W., Zhang, L., Zhang, Q., Cheung, T., et al. (2020). Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry 7, 228–229. doi: 10.1016/S2215-0366(20)30046-8
*Yang, Q. (2018). Understanding computer-mediated support groups: a revisit using a meta-analytic approach. Health Commun. 35, 209–221. doi: 10.1080/10410236.2018.1551751
Zoogman, S., Goldberg, S. B., Vousoura, E., Diamond, M. C., and Miller, L. (2019). Effect of yoga-based interventions for anxiety symptoms: A meta-analysis of randomized controlled trials. Spirit. Clin. Prac. 6, 256–278. doi: 10.1037/scp0000202
*^Indicated that study was included in the review.
(“Mental health intervention” OR “self therap*” OR “mindful*” OR “meditation” OR “yoga” OR “positive psychology” OR “gratitude” OR “journaling” OR “expressive writing” OR “low intensity exercise” OR “applied relaxation” OR “self-guided” OR “affective touch” OR “physical exercise” OR “social-media” OR “mindful eating” OR “creative tasks” OR “occupational therap*” OR “social media intervention” OR “mental health app” OR “well-being app” OR “smartphone intervention” OR “art therap*” OR “music therap*”) AND “meta-analy*”
A second search used these more specific search terms:
(“quarantine” OR “isolation” OR “social isolation” OR “confinement”)
AND “meta-analy*”
AND “pandemic.”
Keywords: COVID-19, meta-analysis, self-guided interventions, depression, anxiety, culture, stress, subjective well-being
Citation: Fischer R, Bortolini T, Karl JA, Zilberberg M, Robinson K, Rabelo A, Gemal L, Wegerhoff D, Nguyễn TBT, Irving B, Chrystal M and Mattos P (2020) Rapid Review and Meta-Meta-Analysis of Self-Guided Interventions to Address Anxiety, Depression, and Stress During COVID-19 Social Distancing. Front. Psychol. 11:563876. doi: 10.3389/fpsyg.2020.563876
Received: 19 May 2020; Accepted: 24 September 2020;
Published: 28 October 2020.
Edited by:
Darren C. Treadway, Daemen College, United StatesReviewed by:
Maria A. Zayas, Brenau University, United StatesCopyright © 2020 Fischer, Bortolini, Karl, Zilberberg, Robinson, Rabelo, Gemal, Wegerhoff, Nguyễn, Irving, Chrystal and Mattos. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ronald Fischer, cm9uYWxkLmZpc2NoZXJAdnV3LmFjLm56
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.