
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Nutr., 05 January 2024
Sec. Nutritional Epidemiology
Volume 10 - 2023 | https://doi.org/10.3389/fnut.2023.1279130
This article is part of the Research TopicNutrition and Sustainable Development Goal 10: Reduced InequalitiesView all 15 articles
 Collins John1*Bee Koon Poh2Muhammad Yazid Jalaludin3Godpower Michael4Idris Adedeji5Elizabeth Eberechi Oyenusi6Blessing Akor7,8Nkwoala C. Charles9Vanitha Buthmanaban10Leilani Muhardi11
Collins John1*Bee Koon Poh2Muhammad Yazid Jalaludin3Godpower Michael4Idris Adedeji5Elizabeth Eberechi Oyenusi6Blessing Akor7,8Nkwoala C. Charles9Vanitha Buthmanaban10Leilani Muhardi11Introduction: Triple burden of malnutrition in children remains a significant public health issue. This scoping review aims to assess the information on undernutrition, micronutrient deficiencies and the quality of complementary feeding in various regions in Nigeria.
Methods: A literature search was conducted using PubMed and Google Scholar databases from January 1, 2018 to January 31, 2023 to include studies focusing on 0 to 5 years old children in Nigeria, reporting data on nutritional status, nutrient deficiencies, and published in English.
Results: 73 out of 1,545 articles were included. Stunting remained alarmingly high ranging from 7.2% (Osun, South West) to 61% (Kaduna, North Central), while wasting varied from 1% (Ibadan, South West) to 29% (FCT Abuja, Central) and underweight from 5.9% (Osun, South West) to 42.6% (Kano, North West) respectively. The overall prevalence of anemia and vitamin A deficiency ranged between 55.2 to 75.1 % and 5.3 to 67.6%, respectively. Low rates of achieving minimum dietary diversity and minimum meal frequency were reported across different states depicting the suboptimal quality of complementary feeding. The prevalence of overweight/obesity ranged from 1.5% (Rivers, South South) to 25.9% (Benue, North Central).
Conclusion: Multiple early childhood malnutrition issues exist with a wide disparity across states in Nigeria, particularly in the Northern region. Targeted nutrition interventions must be implemented to improve the situation.
Malnutrition is defined as a “pathological state resulting from inadequate or excess nutrition” (1). According to the World Health Organization (WHO), ‘poor nutrition status’ is the sole important threat to the world’s health, with adequate nutrition being the critical element in helping individuals to live healthy and productive lives. Malnutrition impacts the intergenerational economic growth of a country. Morbidity related to malnutrition leads to a loss in human capital through an education gap and a resultant low-skilled workforce owing to poor cognitive development and reduced school attainment (2). Inadequate food intake and poor dietary quality are directly or indirectly responsible for causing poor health, with the top 6 of the 11 global risk factors associated with dietary imbalances (3).
Malnutrition is expressed through undernutrition (stunting, wasting, and underweight) and/or overnutrition, which is related to a high intake of protein and energy (1). The WHO in 2021 has defined complementary feeding indicators, including minimum dietary diversity (MDD), minimum meal frequency (MMF), and minimum acceptable diet (MAD) (4), as essential in the early years of life to the formation of eating habits that may eventually have short- and long-term implications on the child’s health (5). Severe acute malnutrition (SAM) or protein energy malnutrition (PEM) is a life-threatening condition requiring urgent attention. Over the years, it has been known by different names such as protein-calorie malnutrition, PEM, oedematous malnutrition, nutritional oedema, severe wasting, or based on clinical manifestations including marasmus, kwashiorkor, or marasmic kwashiorkor (6).
Globally there are over 150 million stunted children, 50 million wasted children, and 38 million underweight children (6). In addition, over 40 million children under the age of 5 years are overweight (6). While more countries are dealing with several forms of malnutrition indices, individual children are known to suffer from more than one form of malnutrition indicators across the world (7).
Nigeria is one of the top 10 countries with malnutrition in children aged under 5 years (7). It has the second-highest burden of stunted children in the world and a higher-than-the-world average child-wasting prevalence (8). Within Nigeria, nearly half of all under-5 children were stunted in the North East and North West geopolitical zones, while the rest of Nigeria contributed to 22.0 % of under-5 stunting prevalence (9).
Despite the availability of studies on stunting, there is a paucity of information on other nutritional issues across all the regions of Nigeria. Hence, the objective of this study was to review the current evidence on nutritional status, nutrient intake, and quality of complementary feeding in under-5 children across all the geopolitical zones and states of Nigeria.
Literature searches were carried out using the PubMed and Google Scholar databases. The main search terms used in the literature search were malnutrition, nutritional deficiency, Nigeria, stunting, wasting, or underweight. The details of the search are provided in Table 1. The results are reported according to the PRISMA guidelines for scoping reviews (Figure 1).
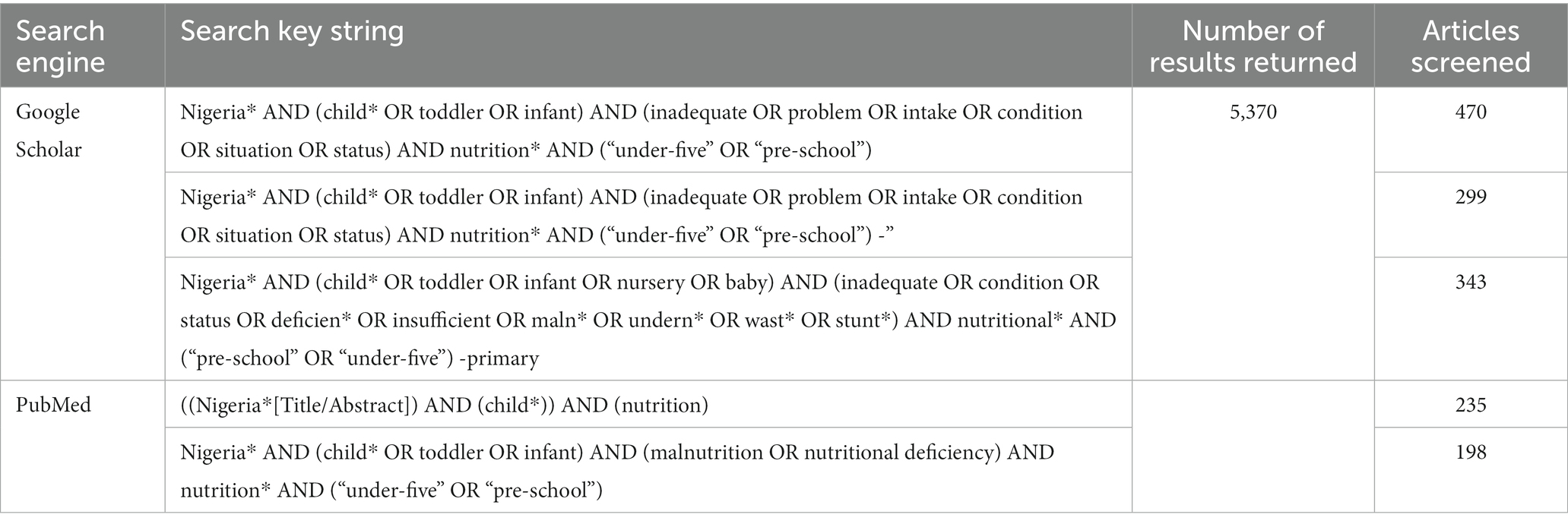
Table 1. Summary of search strategy and results.
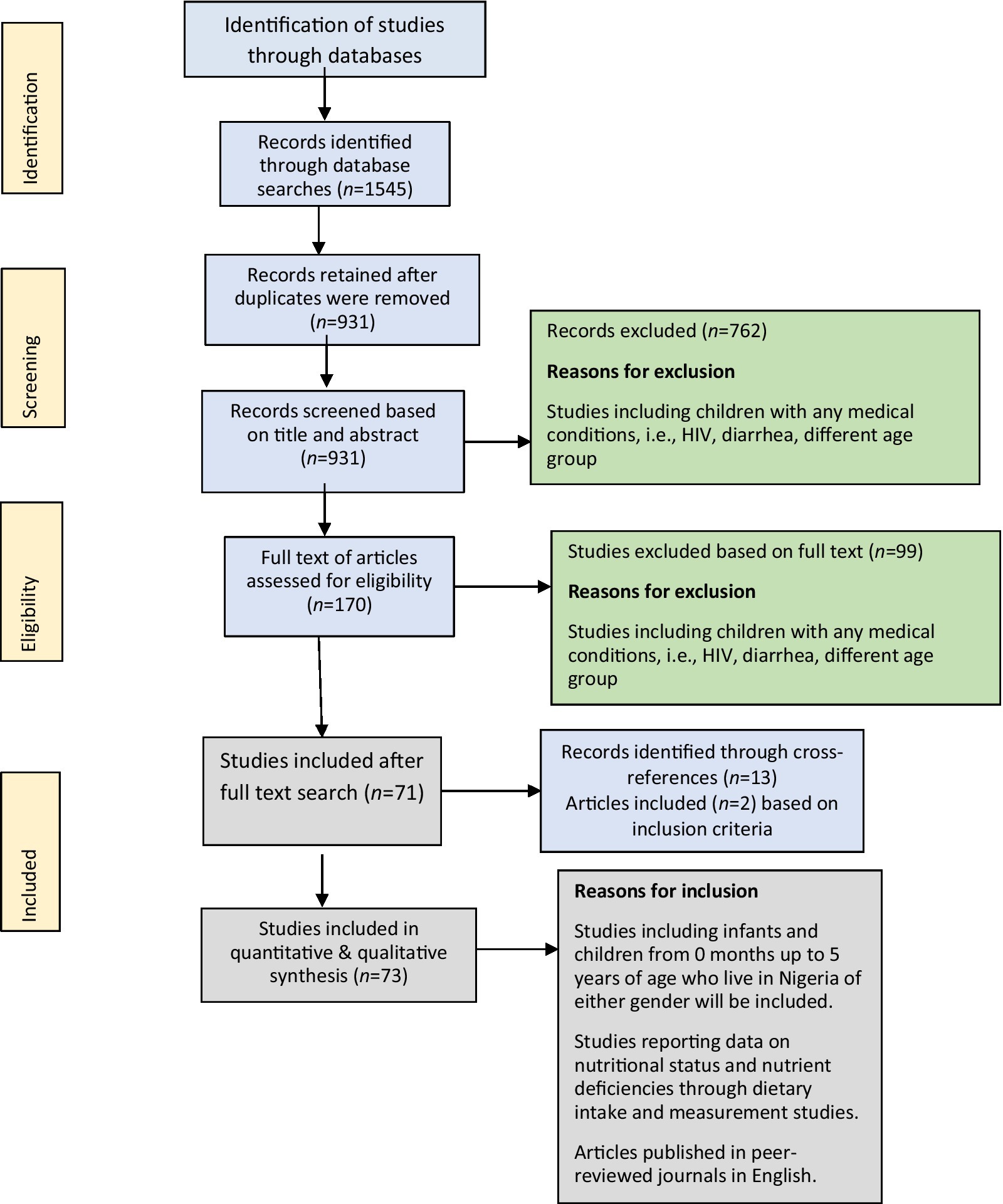
Figure 1. PRISMA flow diagram of study search and selection process.
For all the articles, the search results were extracted and imported into reference management software (Mendeley). All duplicates were removed, and a researcher screened the results based on manuscript’s title and abstract based on the following criteria:
• Studies including infants and children from 0 to 60 months of age of either gender living in Nigeria.
• Studies reporting data on nutritional status and nutrient deficiencies through dietary intake and measurement studies.
• Baseline data from intervention studies.
• Specific case reports if relevant.
• Review articles
• Articles published from 01-01-2018 to 31-01-2023 to focus on recent available data.
• Articles published in peer-reviewed journals in the English language.
• Studies including children with any medical conditions, such as sickle-cell anemia, human immunodeficiency virus (HIV), and diarrhea.
• Grey literature such as reports.
• Single case reports on a specific disease.
Two authors (CJ and LM) reviewed the retrieved full-text articles for final inclusion in the study. If there were any disagreements in the selection of the articles, a third author (PBK or MYJ) acted as a referee to decide whether the article under consideration should be excluded or included. LM extracted date from the eligible retrieved articles to provide extraction of information. No assessment on data quality was implemented.
Data for the following outcomes of interest were extracted from relevant research articles: participant characteristics (age, sex, geographical location, socioeconomic status, weight, and height); nutritional status (stunting, wasting, underweight,) acute malnutrition, overweight, and obesity; nutrient deficiencies biochemical analysis (including iron deficiency anemia, vitamin A, and zinc deficiency); from dietary intake studies including energy; macronutrients (protein, total fat, total calorie); and micronutrients (iron, zinc, vitamin A, calcium, magnesium, phosphorus, vitamin D, B-vitamins, vitamin C, zinc, folate).
Results were pooled by region to facilitate regional comparison. Available data describing the estimation of malnutrition, nutrient status, and dietary quality, including differences by age, gender, and setting (urban vs. rural), are also discussed in the narrative findings for each outcome. The data in the review is incorporated as a range from the lowest to the highest percentage values or as per geopolitical zones in Nigeria, namely North Central, North East, North West, Central, South East, South South, South West or the year of study or publication.
In this study, WHO definitions for various malnutrition status were used. Stunting in a child is defined with a height-for-age Z-score (HAZ) of below minus two standard deviations (−2SD) from the median; wasting as a weight-for-age Z-score of below minus two standard deviations (−2SD) from the median. An underweight is weight-for-height Z-score is less than minus two standard deviations (−2SD) from the median and could be a composite extraction of both stunting and wasting child’s status; a child with severe stunting has HAZ < −3SD and moderately stunting as −3SD ≤ HAZ ≤ −2SD. The same classification also holds for other anthropometric indicators of undernutrition (1). The WHO in 2021 has defined complementary feeding indicators, including MDD (percentage of children 6–23 months of age who consumed foods and beverages from at least 5 out of 8 defined food groups during the previous day), MMF (percentage of children 6–23 months of age who consumed solid, semi-solid or soft foods the minimum number of times or more during the previous day), and MAD (percentage of children 6–23 months of age who consumed at least MDD and MMF during the previous day) (4). Inadequate energy intake used in the study is defined as energy intake less than 80% of recommended daily intake (570–1742 kcal). Similarly, inadequate intake of other micronutrients is also defined as less than 80% of recommended daily nutrient intake (10). Severe and moderate anaemia is defined as <7 g/dl and 7.0–9.9 g/dl, respectively (11).
Seventy-three articles were included in the study based on the inclusion–exclusion criteria. Along with the national prevalence, data was also available from 20 states covering all six geopolitical zones of Nigeria. Amongst the included articles, a majority of studies (84.9%) reported data for the prevalence of undernutrition status (stunting, wasting, and underweight), overweight, and obesity. Articles reporting stunting prevalence (61.6%) were the highest in number, while that reporting wasting (53.4%) and underweight (46.6%) prevalence was relatively less. Only six articles provided information on SAM/PEM (8.2%). Approximately 28.8% of articles reported nutrient intake data, 47.6% reported anemia prevalence, 33.3% reported vitamin A deficiency prevalence, 19.0% reported zinc deficiency, 14.3% reported iron and vitamin D deficiency, while only 1 article each was identified reporting the prevalence of vitamin B12, vitamin C, and potassium deficiency.
On average, only 15% of the articles mentioned the year the study was conducted. Some of the selected articles with year of publication after January 1, 2018, did however cite data from earlier date including those from 2003.
The average national prevalence of SAM/PEM in Nigeria was 8.8% (12, 13); however, the prevalence data reported a wide region-wise variance in prevalence, ranging from 1.9 to 46.0% (14–17) (Supplementary Table 1A). The highest SAM/PEM prevalence was reported from the South West and North West geopolitical zone of Nigeria (15, 16). In the Osun state (South West), the prevalence of Marasmus, Kwashiorkor, and Marasmus-Kwashiorkor were as low as 2.0, 3.0, and 2.0%, respectively (15).
From several retrieved literature, the national prevalence of undernutrition has been reported to decline from 2003 to 2013 and 2018 (45% vs. 37% vs. 36.8 % for stunting, 13% vs. 8% vs. 6.7% for wasting, and 27.2% vs. 28.9 % vs. 21.4% for underweight) (18–20). The regional prevalence of stunting, wasting, and underweight reported a difference from the national prevalence in Nigeria, as seen in the geopolitical zone mapping of Nigeria (Figure 2).

Figure 2. Malnutrition map of Nigeria for (A) stunting, (B) wasting, (C) underweight, (D) overweight and obesity.
As per National Demographic Health Survey (NDHS) 2018, the national stunting prevalence among under-5 children in Nigeria was reported to be 36.1 % (21). The prevalence by zone reported stunting to be the highest in Kaduna in North West (61.3%) (22) and Kwara in the North Central zone (55.8%; Supplementary Table 2) (23). The lowest prevalence of stunting was reported from Osun state in the South West region (7.2%) (24). The severity of stunting varied among states from 3.4% in Rivers (South West) (25) to 54.5% in Kaduna (North West) (26). The prevalence of moderate stunting ranged from 8.2% in Anambra (South East) (27) to 28.8% in Kaduna (North West) (26) (Supplementary Table 2). From 2003 to 2018, the national prevalence of severe stunting reduced from 22.8 to 16.9% (28).
Several states in Nigeria reported a high prevalence of wasting, which was above the national prevalence in Nigeria, including Anambra (South East; 30%) (29), FCT, Abuja (North Central; 29.3%) (30), Bida, Niger (North Central; 27.8%) (31), Ondo (South West; 25.3%) (32), Enugu (South East; 25.0%) (33), Osun (South West; 24.0%) (34), and Kano (North West; 22.8%) (35). The lowest prevalence of wasting (1.0%) was seen in Ifedore, Ondo state (South West) (36). However, none of these studies cited the year of data collection.
The underweight prevalence in Nigerian states ranged from 5.9% in the Osun state (South West) (34) to 42.6% in the North West zone of Nigeria (37). Several states reported underweight prevalence above the national prevalence, with the highest prevalence in North West including Kano State (around 41.9%-42.6%) (35, 37), followed by Enugu state (South East; 39.8%) (24).
There are more than 10 reported risk factors for undernutrition, among others: malaria and anemia (38), having more than four children and religious belief (39), having a respiratory or diarrheal infection (28, 40). However, immunization status, maternal education, parental income, maternal height and body mass index (BMI); as well as having antenatal care less than four times are among commonly reported risk factors (28, 39–43).
It was seen that the overall national prevalence of stunting, wasting, and underweight in urban areas of Nigeria ranged between 26.8–30.6%, 10.5–35.6%, and 23.0–31.2%, respectively, while in the rural regions, it was 44.8–72.8%, 10.5–69.9%, and 35.5–72.9%, respectively (Supplementary Table 3). The highest prevalence of stunting was reported in the urban Ibadan, Oyo state (44) and rural regions of Lagos (39). State-wide prevalence of wasting was almost similar in rural regions compared to urban regions, with the highest prevalence reported from Lagos state (urban: 8.7%; rural: 9.3%) (38). The Ibadan urban region in Oyo state showed a wasting prevalence of 1.8% which was much below the national prevalence (10). The prevalence of underweight was considerably higher in rural compared to urban (19, 37, 45–47) (Figure 3).
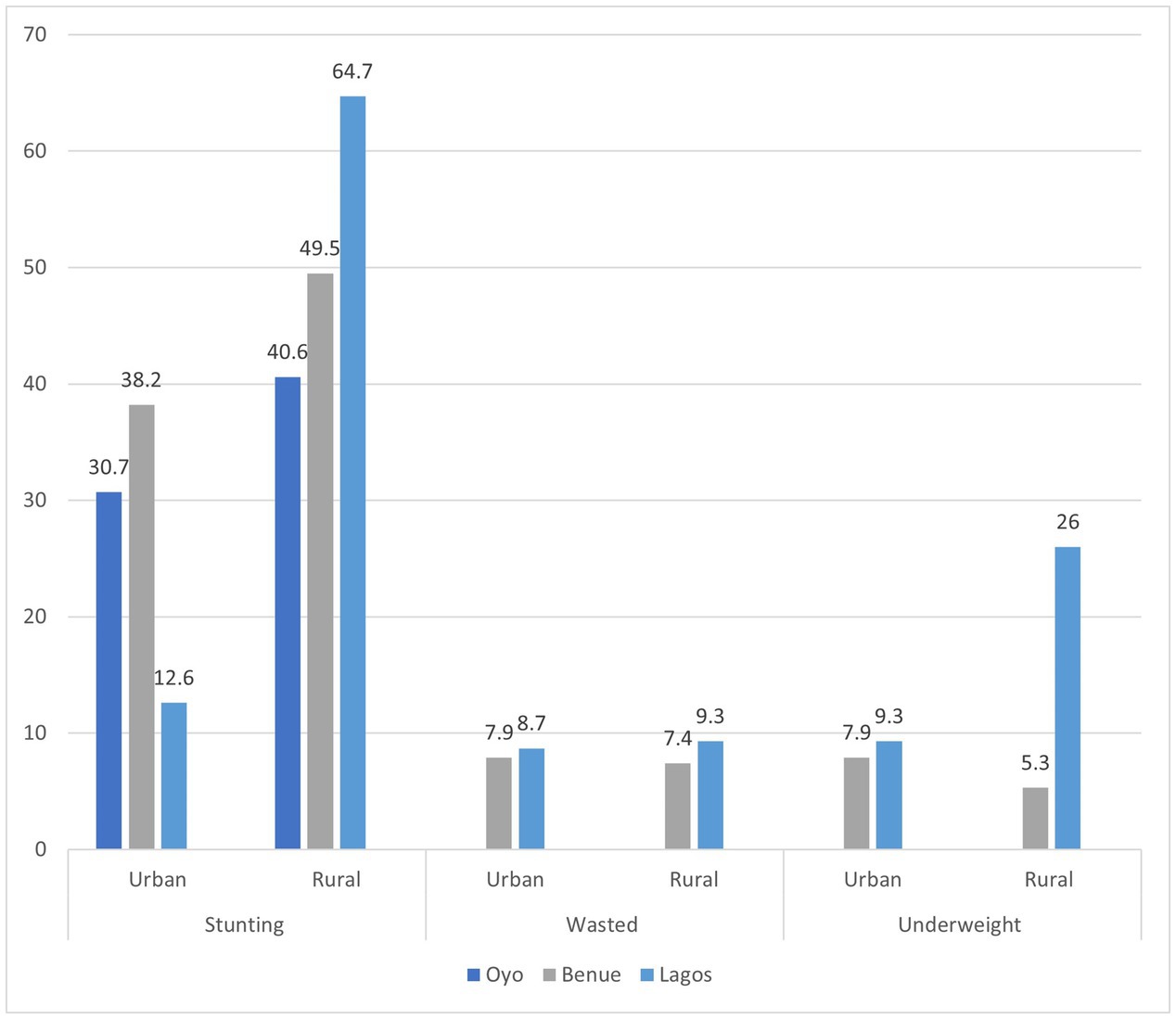
Figure 3. Urban–rural prevalence of undernutrition across a few states in Nigeria.
There was no definitive pattern has been noticed in the prevalence of gender-based undernutrition (Supplementary Table 4). A few studies have reported higher stunting prevalence in males compared to females. The regional prevalence differs from the national prevalence in that the males depict a higher prevalence of stunting and wasting but not underweight (48–51). In contrast, wasting prevalence was slightly higher amongst females than males (22, 50, 52, 53). There were no differences between males and females regarding underweight prevalence (18, 45) (Supplementary Table 4).
In males, wasting prevalence ranged from 2.5 to 50.0%; underweight ranged from 6.0 to 78.0%, while in females, wasting prevalence was reported from 8.0 to 61.0% and underweight from 7.0 to 61.4% (16, 22, 48, 50, 54, 55).
Between 2008 and 2018, the NDHS data reported that the prevalence of stunting among children 6–11 months ranged from 28.9 to 35.4%, while the prevalence of stunting among 0–23 months old was 39.1%, and among 24 to 59 months was 53.3% (55). The prevalence of underweight was stable of around 10% among infants 0–6 months and 6–11 months. However, this number doubled to around 20.0% in older children of 12–60 months.
The prevalence of wasting was the highest among children 12–35 months (Figure 4).
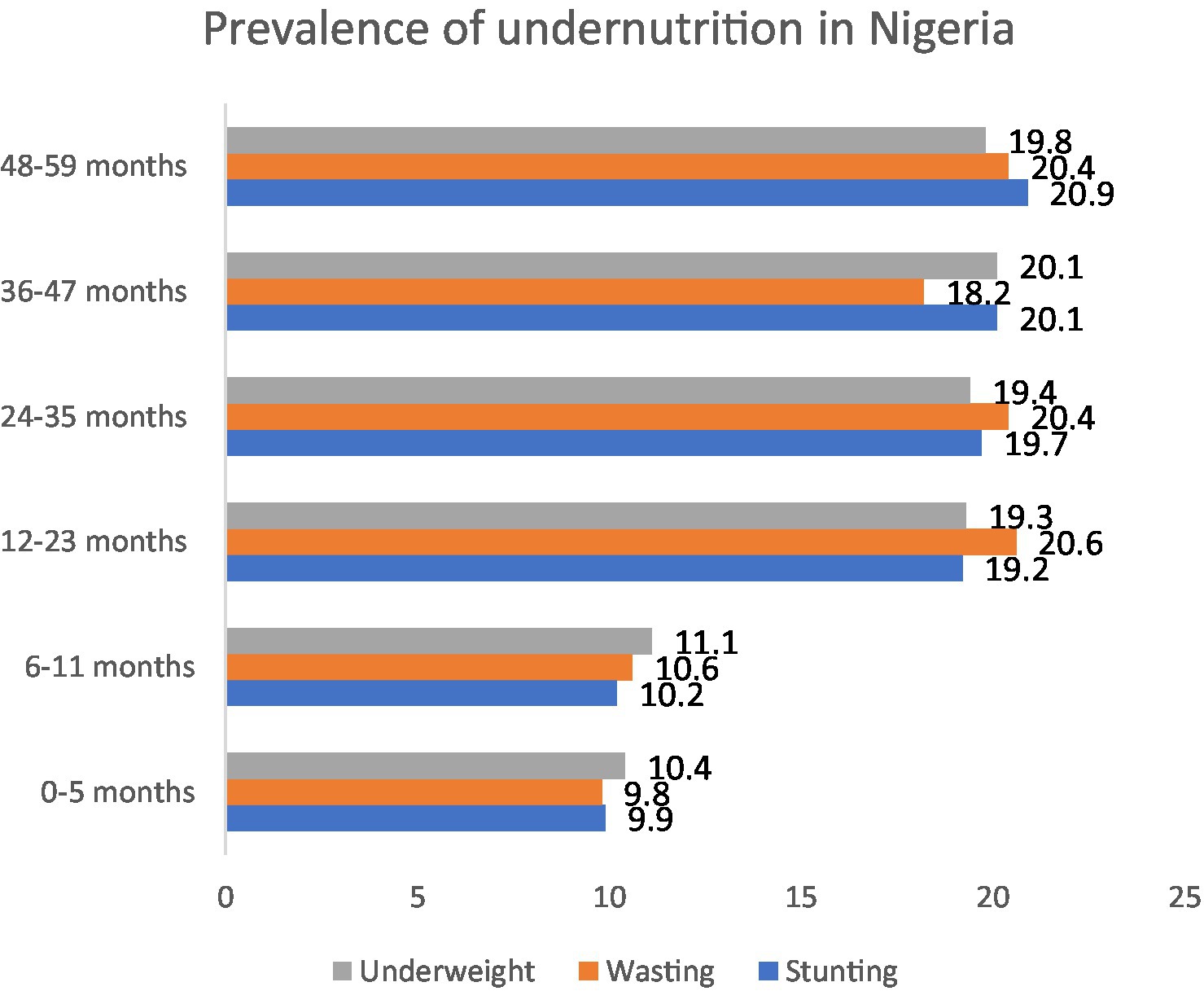
Figure 4. Prevalence of undernutrition among children according to age.
The data collected across 13 states reported the national prevalence of obesity in 2013 to be 4.0% (20, 43), while in 2018, it declined to 2.0%. The overweight prevalence ranged from 1.5 to 25.2%, while obesity ranged from 0.6 to 25.9% among under-5 children in different regions of Nigeria (21, 25, 30, 56, 57). The prevalence of overweight in male children in Ondo and Benue states was 9.8 and 10.5%, while in female children, it was 10.7 and 8.4%, respectively (53, 58) (Supplementary Table 5).
The prevalence of inadequate energy intake ranged from 18.0 to 34.0% (36, 59). A study in Ibadan, Oyo State (South West), reported an inadequate intake of fat (92.0%), protein (46.0%), and carbohydrates (30.0%) (10, 11). Other studies reported that the prevalence of inadequate intake for different micronutrients in under-5 children including zinc 32.0–91.0%, potassium 91.0%, vitamin A 82.0%, vitamin C 80.0%, iron 74.0%, and folate 44.0% (59, 60).
Data from the NDHS shows the national prevalence of anemia among children under-5 years of age in Nigeria has slightly declined from 67.0% reported in 2013 to 58% in 2018 (20). However, the anemia prevalence has shown an upward trend in urban regions from 55.2% in 2010 to 62.0% in 2018, while in rural regions; the prevalence remains similar which was reported around 75.1% in 2010 and 72.5% in 2018 (61).
The prevalence of severe and moderate anemia in males was reported to be 3.6 and 43.3%, respectively, and in females, the prevalence of severe and moderate anemia was 2.9 and 38.4%, respectively (11). The highest prevalence of severe and moderate anemia was reported in children under 1 year (11) (Figure 5A). Moderate iron deficiency ranged from 1.1 to 32.2%, while severe deficiency ranged from 1.1 to 67.8% (16). Having vitamin A deficiency and malaria are some of the risk factors reported to be associated with anemia (62, 63).
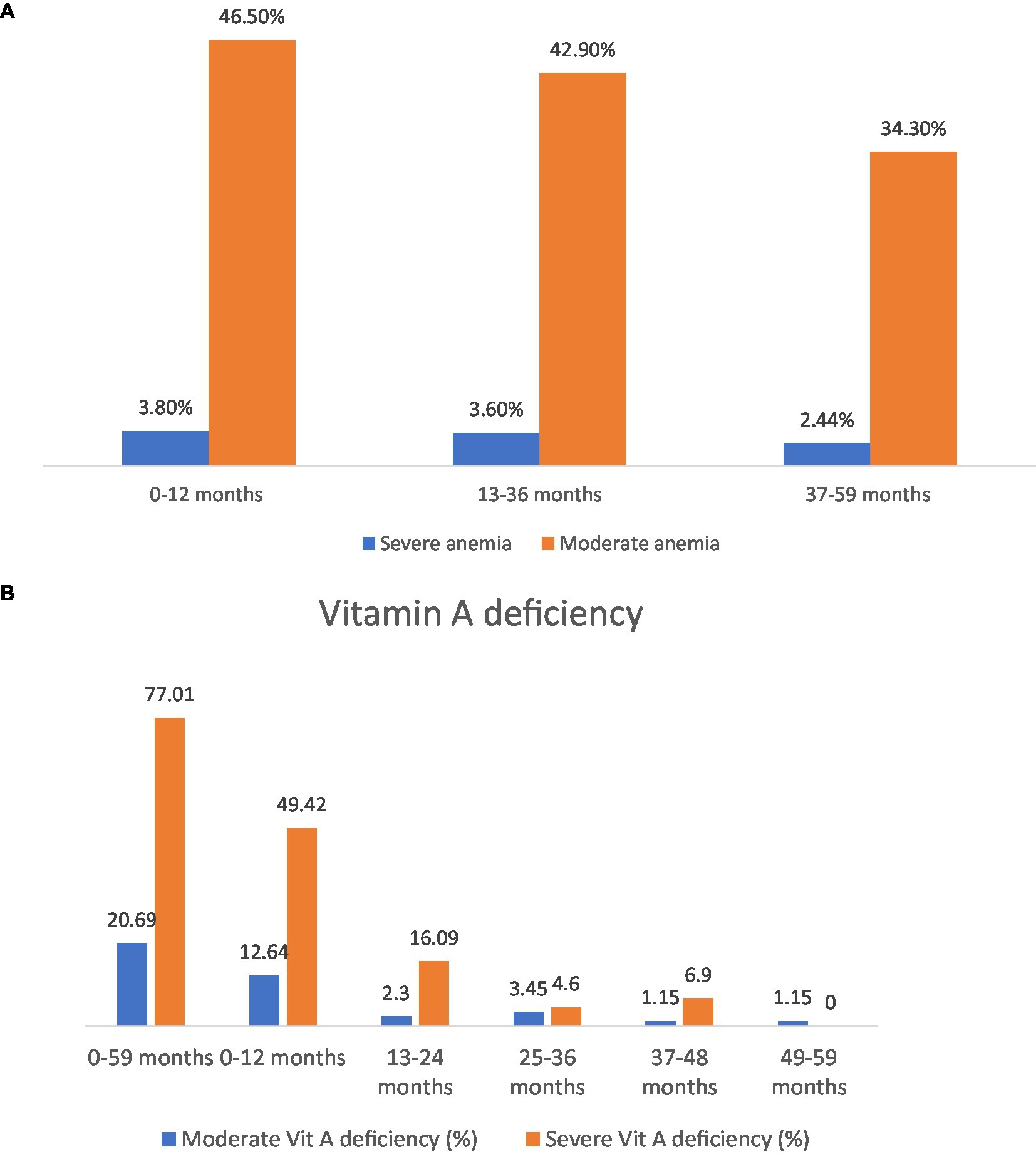
Figure 5. (A) Anemia prevalence in different age groups. (B) Severe vs. moderate vitamin A deficiency in different age groups.
Vitamin A deficiency ranged from 5.3 to 67.6% (24, 64), with a severe deficiency of 77.0 and 20.7% of moderate deficiency (Figure 5B) (16). The prevalence of vitamin A deficiency in a study of children 3 to 5 years of age ranged from 8.0 to 10.0% (65). Factors reported to be associated with vitamin A deficiency are anaemia (16) and low consumption of vitamin A-rich foods (26).
Based on baseline data of an intervention study among toddlers in Lagos (South West), it was reported a deficiency of vitamin D (9.0–37.0%), folate (8.0–21.1%), and vitamin B12 (7.1%) (66). Moderate vitamin D deficiency ranged from 1.15 to 24.14%, while severe deficiency ranging from 2.3 to 50.6% was reported in Kaduna state (16). Low serum zinc was reported in 12.4–26.0%, being higher in males (32.1%) than in females (19.1%) (33, 67).
The proportion of children achieving MDD ranged from 3.0 to 55.2% in Nigeria (37, 54, 68–71) (Table 2). Dietary diversity was classified into low (meals comprising 1–6 food groups) and high (meals comprising 6–12 food groups). The prevalence of low and high dietary diversity reported in one study was 68.5 and 31.5%, respectively (22). While another study reported a total of 85.5% among 6- to 24-month-old children fulfilled the MDD, with the highest prevalence seen in 9- to 11-month-old infants (36.0%) (70).
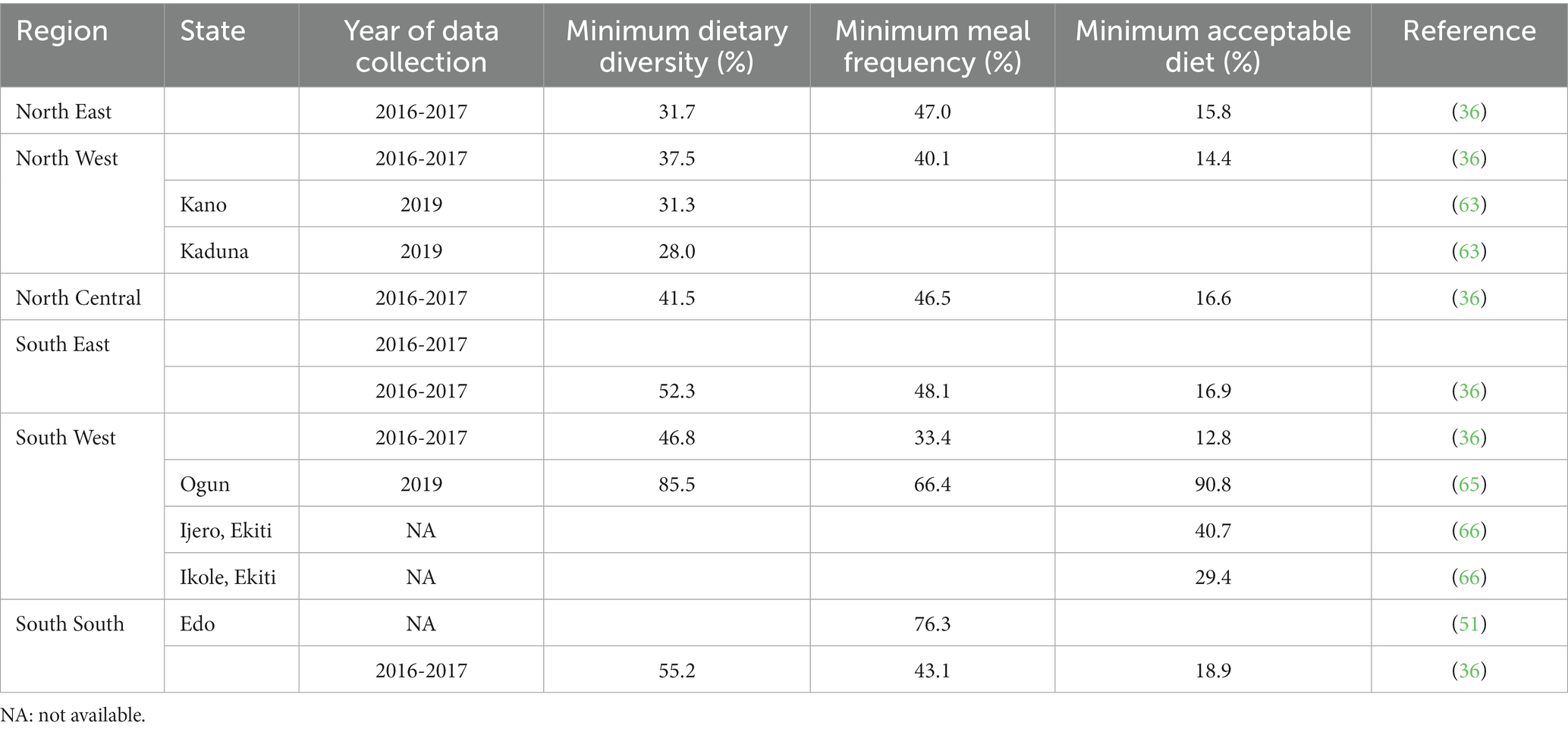
Table 2. Proportion of children who meet the minimum dietary diversity, minimum meal frequency, and minimum acceptable diet across different regions in Nigeria.
The proportion of children achieving MMF ranged from 33.4 to 76.3% (37, 54, 68–70). In a study by Samuel and Ibidapo, the highest prevalence of MMF was 30.0% in infants 9 to 11 months of age. A high prevalence of MAD (90.8%) was reported in children in Osun state (70). Several factors reported in this review to be associated with poor quality of complementary foods are antenatal care visit, child’s welfare clinic visit, mother’s work place and education, as well as household size (70).
This scoping review summarizes available evidence on the burden of malnutrition in under-5 children in various regions of Nigeria as well as the nutrient deficiency and quality of complementary feeding. It highlights the disparities across regions, age groups and gender across several indicators of malnutrition, such as stunting, wasting, underweight, and anemia. While a total of 73 studies were identified, most reported data on nutritional status; only 6 reported the prevalence of SAM/PEM, and a few studies (less than 30%) revealed information on nutrient intake/deficiency or quality of complementary feeding.
The prevalence of stunting, wasting, and underweight in under-5 children was high, exhibiting considerable variations across different zones. The North West and North Central zones have been reported to have the highest prevalence of SAM, stunting, wasting, underweight, iron deficiency anemia, and moderate/severe vitamin D deficiencies and the lowest proportion of children under 6 months who met the MDD and MAD. In contrast, the prevalence of undernutrition was found to be generally lower in South East Nigeria compared to other zones (72).
The high prevalence of poor nutritional status among under-5 children in the Northern zones could be attributed to the militant insurgency, banditry, and cattle rustling hindering a large number of farmers and livestock herders from accessing their farmlands for almost a decade. These disastrous scenarios not only lead to restrictions on agricultural produce but also severe food insecurity, affecting many households residing in these zones, particularly in the rural regions (9, 22, 37, 48, 55). This situation also drives more consumption of staple foods as accessible sources of energy (37). In addition, there were some food taboos for children and pregnant women that restrict their access to certain foods, such as eggs which were more prominent in the Northern region (37). It was also clearly seen that undernutrition prevalence was more pronounced in rural regions than in urban regions.
More than half of the under-5 children have anemia with a higher prevalence reported in rural areas than in urban regions. Studies have shown that anemia in children leads to poor cognition, school achievement, and more behavioral issues as they grow, particularly into middle childhood (73). In several cases, it may lead to irreversible damage to the child’s development (73); hence, efforts to alleviate the anemia burden are necessary in Nigeria. This review also noted that a substantial prevalence of vitamin A deficiency in Nigeria.
Undernutrition particularly in the first 2 years of life, has been reported to lead to an impairment of their ability to resist disease (74, 75), undertake physical activity, and progress in study and school (74, 75). The impact of not achieving growth potential impedes the cognitive development of the child, with enormous and adverse implications on well-being and economic prospects as the child grows into adulthood. Undernutrition in the early years of life leads to reduced educational completion, lower economic productivity, increased morbidity, and reduced life expectancy (9). Studies have shown that children who suffer from undernutrition are not able to complete their education and show deficiencies in vocabulary and mathematics, along with other learning or intellectual disabilities, which leads to reduced economic productivity in adulthood (73, 78). This depletion of human capital not only poses social and economic challenges in disadvantaged communities of Nigeria but also hinders the overall economic and social progress of the country in general.
In addition, this report also shows the high prevalence of overweight and obesity in several states in North Central and South West Nigeria. This confirms the presence of a triple burden of malnutrition among children under 5 years of age in Nigeria which further worsens the dire situation of these children as resources need to be allocated to address these three problems simultaneously (79, 80).
The review reported a high prevalence of underweight and wasting among children between 12-35 months while the highest prevalence of stunting was in children 24-59 months old. In addition, the highest prevalence of severe and moderate anemia was reported in children under 1 year of age. These three conditions could be the root cause of why the prevalence of stunting remained and will continue to be high in Nigeria as has been shown in other countries (81). Studies have shown that underweight/wasting in the early life can persist into failure to thrive and will continue to stunting at a later age (82, 83).
Undernutrition among under-5 children is driven by a mesh of influencing factors, including cultural, behavioral, and environmental factors. The quality of complementary feeding practices is one of the important factors in determining the child’s nutritional status. The 6- to 24-month age group is characterized by increased energy expenditure and need for nutritional requirements through complementary feeding. Inappropriate complementary feeding practices significantly contribute to undernutrition among children contributing as a major cause of disease burden, especially in developing countries (84). Maternal characteristics such as education and BMI were frequently reported in this review as influencing factors for stunting and the quality of complementary foods. This points out the importance to have better education and nutrition status of the mothers to ensure a healthy period during the first 1,000 days. In addition, malaria and anemia seem to counter-influence each other, thus it is important to address both factors together whenever one of these health issues occurred.
Possible interventions that have been shown to reduce the prevalence of malnutrition should be able to address the problem at different levels. These are itemized as follows: (1) at an individual level: increased uptake and attendance of antenatal care visits, lower average number of birth and mandatory vaccination for children and women (81, 85), and improvement of nutrition and health knowledge among girls and pre-pregnant women (81); (2) at the household level: change in behavior to include the use of clean fuel for cooking, encouragement for more hygienic behavior including a reduction in the practice of open defecation (81); (3) at regional level: food subsidies or food-based intervention in the northern region of Nigeria has been shown to simultaneously overcoming multiple nutritional challenges in the area; and (4) at the national level to support at least four times minimal antenatal care, address anemia and malaria (86), to enhance awareness of vaccination in young children (85), create more equitable household economic growth (81, 87), and build infrastructure for greater access to improve toilet facilities (81, 88).
It is crucial to prioritize efforts that enhance, among others, access to nutritious food, improve healthcare services, and implement effective, targeted interventions. Furthermore, there is a need for more monitoring efforts to evaluate the effectiveness of these interventions as a basis for further refinement of the interventions in the future.
This scoping review offers a comprehensive assessment of the nutritional status of children in Nigeria, as well as various related indicators, providing invaluable insights to guide future research endeavours. Furthermore, it highlights the need to invest in public policies and socioeconomic strategies that can foster improved nutrition status and address the underlying issues. This study meticulously collates an array of essential undernutrition parameters, complementary feeding indicators, and dietary intake status pertaining to under-5 children in Nigeria. Drawing from recent data sourced from national health surveys, regional surveys, and other pertinent studies, a spectrum of prevalence rates spanning from low to high has been thoughtfully incorporated based on geopolitical zone. To enhance accessibility, the amassed data has been meticulously organized and presented in a user-friendly mapping format.
Due to the heterogeneity of studies, the absence of precise study years, and limited results for some regions, the undertaking of a comprehensive meta-analysis or applying statistical analysis to individual study results was not feasible.
There is a dearth of data available for micronutrient intake and deficiency. For example, in this review, there were no data retrieved on nutrients related to immunity, such as vitamin C and E (89), or nutrients that are important for bone growth, such as calcium, phosphorus, magnesium (90), and also nutrients that are commonly reported to be deficient in other populations (such as pregnant women in Nigeria) like thiamine and riboflavin (91, 92). For macronutrients, total protein and LCPUFA intake in under-5 children, for example, was notably absent in all of the selected studies.
The culmination of this comprehensive analysis has brought to the forefront a multitude of pressing nutritional problems, prominently underscored by the pervasive triple burden of malnutrition encompassing stunting, overweight, and anemia. The northern zones in Nigeria have emerged as particularly vulnerable, grappling with a more acute undernutrition crisis as evidenced by the array of indicators examined.
Gender differentials further paint a nuanced picture, whereby stunting exhibited a higher prevalence among males, while the prevalence of wasting in several states, was skewed toward females. The widespread occurrence of anemia across diverse geographical regions, reveals noteworthy disparities between urban and rural areas. The high prevalence of vitamin A and D deficiency, along with inadequate nutrient intake, were also notable.
Compounding these challenges, a significant proportion of children were found to lack access to a diverse range of food groups, and fell short of consuming the recommended number of meals per day in their complementary diets.
In light of the far-reaching impact of malnutrition, encompassing the loss of human capital and reduced economic productivity across Nigeria, the imperative for targeted and expeditious nutrition interventions becomes evident. Swift and concerted action are crucial to rectify the prevailing disparities in nutrition status among young children in Nigeria, securing a healthier and more prosperous future for the nation at large.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
CJ: Conceptualization, Data curation, Investigation, Methodology, Writing – review & editing, Formal analysis. BP: Conceptualization, Data curation, Investigation, Writing – review & editing, Formal analysis. MJ: Conceptualization, Formal analysis, Writing – review & editing, Methodology. GM: Formal analysis, Methodology, Writing – review & editing, Data curation. IA: Formal analysis, Methodology, Writing – review & editing, Investigation. OE: Formal analysis, Investigation, Writing – review & editing, Data curation. BA: Formal analysis, Writing – review & editing, Methodology. NC: Formal analysis, Methodology, Writing – review & editing, Data curation. VB: Writing – review & editing. LM: Writing – review & editing, Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Supervision.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors would like to acknowledge and appreciate the medical writer, Pooja S. Banerjee, IJCP Group, New Delhi, India, for her support in the development of the first drafts of the manuscript.
VB and LM are employees of FrieslandCampina.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2023.1279130/full#supplementary-material
1. World Health Organization (2021). Malnutrition [Internet]. Available at: https://www.who.int/news-room/fact-sheets/detail/malnutrition (Accessed August 1, 2023).
2. Chakravarty, N, Tatwadi, K, and Ravi, K. Intergenerational effects of stunting on human capital: where does the compass point? Int J Med Public Health. (2019) 9:105–11. doi: 10.5530/ijmedph.2019.4.24
3. Siddiqui, F, Salam, RA, Lassi, ZS, and Das, JK. The intertwined relationship between malnutrition and poverty. Front Public Health. (2020) 8:453. doi: 10.3389/fpubh.2020.00453
4. WHO, The UNICEF (2021). Indicators for assessing infant and young child feeding practices [internet]. Vol. WHA55 A55/, World Health Organization. 19 p. Available at: http://apps.who.int/iris/bitstream/handle/10665/44306/9789241599290_eng.pdf?sequence=1%0Ahttp://whqlibdoc.who.int/publications/2008/9789241596664_eng.pdf%5Cnhttp://www.unicef.org/programme/breastfeeding/innocenti.htm%5Cnhttp://innocenti15.net/declaration (Accessed August 1, 2023).
5. Leonez, DGVR, de Freitas Melhem, AR, Vieira, DG, de Mello, DF, and Saldan, PC. Complementary feeding indicators for children aged 6 to 23 months according to the breast feeding status. Rev Paulista Pediatria. (2020) 39:e2019408. doi: 10.1590/1984-0462/2021/39/2019408
7. Obasohan, PE, Walters, SJ, Jacques, R, and Khatab, K. Risk factors associated with malnutrition among children under-five years in sub-Saharan African countries: a scoping review. Int J Environ Res Public Health. (2020) 17:8782. doi: 10.3390/ijerph17238782
8. Nwosu, CO, and Ataguba, JEO. Explaining changes in wealth inequalities in child health: the case of stunting and wasting in Nigeria. PLoS One. (2020) 15:e0238191. doi: 10.1371/journal.pone.0238191
9. Amare, M, Benson, T, Fadare, O, and Oyeyemi, M. Study of the determinants of chronic malnutrition in northern Nigeria: quantitative evidence from the Nigeria demographic and health surveys | IFPRI: international food policy research institute. Food Nutr Bull. (2018) 39:296–314. doi: 10.1177/0379572118768568
10. Yahaya, SP, Sanusi, RA, Eyinla, TE, and Samuel, FO. Household food insecurity and nutrient adequacy of under-five children in selected urban areas of Ibadan, southwestern, Nigeria. Afr J Biomed Res. (2021) 24:41–6.
11. Shourove, JH, Meem, FC, Lima, SA, and Islam, GMR. Prevalence of childhood anemia: potential sociodemographic and dietary factors in Nigeria. PLoS One. (2022) 17:e0278952. doi: 10.1371/journal.pone.0278952
12. Fagbamigbe, AF, Kandala, NB, and Uthman, OA. Severe acute malnutrition among under-5 children in low- and middle-income countries: a hierarchical analysis of associated risk factors. Nutrition. (2020) 75–76:110768. doi: 10.1016/j.nut.2020.110768
13. Fagbamigbe, AF, Kandala, NB, and Uthman, OA. Decomposing the educational inequalities in the factors associated with severe acute malnutrition among under-five children in low- and middle-income countries. BMC Public Health. (2020) 20:1–14. doi: 10.1186/s12889-020-08635-3
14. Oyinwola, IO, Ahmed, P, Odusanya, OO, and Oyasakin, AB. Prevalence and risk factors of acute malnutrition among pre-school children in internally displaced person settlements within Abuja municipal area council. Niger J Paediatr. (2022) 49:122–30.
15. Ogunniyi, KAB. A study of protein energy malnutrition (PEM) among under-five children Okuku, Odootin local government area of Osun state, Nigeria. Adeleke Univ J Sci. (2022) 1:258–66.
16. Tanimu, AU, Anigo, KM, Nwajagu, I, and Kahu, J. Assessment of anthropometric indices and micronutrient status of children under five in orphanages of Kaduna Metropolis. Am J Food Nut. (2021) 9:87–95. doi: 10.12691/ajfn-9-2-5
17. Ekechukwu, END, Anyaene, CC, Ikefuna, O, Aguwa, EN, Iroezindu, IC, Okeke, TA, et al. Anthropometric indices and nutritional status of infants in Nigeria – a preliminary study. Lect Notes Networks Syst. (2022) 223:81–95. doi: 10.1007/978-3-030-74614-8_10
18. Akombi Id, BJ, Agho, KE, Renzaho, AM, Hall, JJ, and Merom, DR. Trends in socioeconomic inequalities in child undernutrition: Evidence from Nigeria demographic and health survey (2003 – 2013). PLoS One. (2019) 14:e0211883. doi: 10.1371/journal.pone.0211883
19. Tesfaw, LM, and Fenta, HM. Multivariate logistic regression analysis on the association between anthropometric indicators of under-five children in Nigeria: NDHS 2018. BMC Pediatr. (2021) 21:1–13. doi: 10.1186/s12887-021-02657-5
20. John, C, Al-mansur, M, Leshi, O, Envuladu, E, and Steve-Edemba, C. Nigeria and the global nutrition targets 2025: where are we? J Health Sci Pract. (2022) 21:1–13.
21. Ekholuenetale, M, Okonji, OC, Nzoputam, CI, and Barrow, A. Inequalities in the prevalence of stunting, anemia and exclusive breastfeeding among African children. BMC Pediatr. (2022) 22:1–14. doi: 10.1186/s12887-022-03395-y
22. Kehinde, T, and Favour, E. Food insecurity and nutrition status of farm households in northwestern Nigeria. J Food Sec. (2020) 8:98–104. doi: 10.12691/jfs-8-3-3
23. Fadare, O, Mavrotas, G, Akerele, D, and Oyeyemi, M. Micronutrient-rich food consumption, intra-household food allocation and child stunting in rural Nigeria. Public Health Nutr. (2019) 22:444–54. doi: 10.1017/S1368980018003075
24. Abolurin, OO, Oyelami, OA, and Oseni, SB. A comparative study of the prevalence of zinc deficiency among children with acute diarrhoea in SouthWestern Nigeria. Afr Health Sci. (2020) 20:406. doi: 10.4314/ahs.v20i1.47
25. Okari, TG, Nte, AR, and Frank-Briggs, AI. Prevalence of malnutrition among under-fives in Okrika town, Nigeria. IOSR J Dental Med Sci. (2019) 18:40–5.
26. Abdullahi, SM, Alhassan, YM, Bugaje, MA, and Akuyam, SA. Dietary pattern of undernourished children and their vitamin a status in institute of child health Ahmadu Bello University teaching hospital Zaria. Nigerian J Basic Clin Sci. (2021) 18:18. doi: 10.4103/njbcs.njbcs_11_20
27. Okafor, OC, Okafor, IN, Ezenwa, CB, and Idama, FO. Prevalence of stunting amongst preschool aged children in Awka South. IAA J Biol Sci. (2023) 10:54–60.
28. Adeyemi, O, Toure, M, Covic, N, van den Bold, M, Nisbett, N, and Headey, D. Understanding drivers of stunting reduction in Nigeria from 2003 to 2018: a regression analysis. Food Secur. (2022) 14:995–1011. doi: 10.1007/s12571-022-01279-8
29. Onuekwe, ME. Assessment of nutritional status of pre-school children in Nando, Oyi local government area Anambra state, Nigeria. J Resourcefulness Distin. (2018) 16:119–30.
30. Idowu, SO, Akindolire, AE, Adebayo, BE, Adebayo, AM, and Ariyo, O. Determinants of anthropometric characteristics of under-five children in internally displaced persons´ camps in Abuja municipal area council, Abuja, Nigeria. Pan Afr Med J. (2020) 36:1–12. doi: 10.11604/pamj.2020.36.313.21221
31. Oladele Go OCAGGPDEAEBA. Relationship between the nutritional status of under-five children and family function as seen in the under-five Clinic of Federal Medical Centre Bida, north Central Nigeria. Pediatr Ther. (2022) 12:1000436. doi: 10.35248/2161-0665.22.12.436
32. Olodu, MD, Adeyemi, AG, Olowookere, SA, and Esimai, OA. Nutritional status of under-five children born to teenage mothers in an urban setting, South-Western Nigeria. BMC Res Notes. (2019) 12:116. doi: 10.1186/s13104-019-4147-x
33. Alamu, EO, Eyinla, TE, Sanusi, RA, and Maziya-Dixon, B. Double burden of malnutrition: evidence from a selected Nigerian population. J Nutr Metab. (2020) 2020:5674279. doi: 10.1155/2020/5674279
34. Abolurin, OO, Adegbola, AJ, Oyelami, OA, Adegoke, SA, and Bolaji, OO. Prevalence of vitamin a deficiency among under-five children in South-Western Nigeria. Niger Postgrad Med J. (2018) 25:13–6. doi: 10.4103/npmj.npmj_20_18
35. Maje, MH, Koki, AY, Muhammad, KU, and Kaila, M. Prevalence and socio-economic factors associated with undernutrition among children below five years of age: a case study of Murtala Muhammed specialist hospital. Int J Recent Innov Acad Res. (2019) 3:87–102.
36. Adewole, RO, and Oluwajuyitan, TO. (2022). Effect of Dietary intake on Nutritional Status of under-ve children in Ifedore Local Government Area, Ondo State Nigeria. doi: 10.21203/rs.3.rs-2322337/v1
37. Moeteke, N. Combating childhood multinutrient undernutrition and its inequalities in Nigeria: whitehead’s typology as a policy framework for urgent action. Nigerian J Nut Sci. (2019) 40:120–6.
38. Chukwuocha, UM, Njoku, PU, Ezelote, J, Nwaokoro, JC, and Iwuala, CC. Nutritional status and malaria risk in children under five years in Owerri municipality, south eastern, Nigeria. Hongkong J Pediat Res. (2019) 2:30–5.
39. Senbanjo, IO, Senbanjo, CO, Afolabi, WA, and Olayiwola, IO. Co-existence of maternal overweight and obesity with childhood undernutrition in rural and urban communities of Lagos state, Nigeria. Acta Bio Med Atenei Parmensis. (2019) 90:266. doi: 10.23750/abm.v90i3.7685
40. Grace, OT, and Awoala West, B. The effect of vaccination and childhood morbidity on nutritional status of preschool children in the Niger Delta region of Nigeria. Medico Res Chron. (2019) 6.
41. Ajah, EE, Uleanya, ND, Aniwada, EC, Ndu, A, and Okeke, CC. Determinants of under-nutrition among under-five children in Enugu Metropolis, Southeast Nigeria. Niger J Paediatr. (2021) 48:135–43.
42. Jude, CK, Chukwunedum, AU, and Egbuna, KO. Under-five malnutrition in a south-eastern Nigeria metropolitan city. Afr Health Sci. (2019) 19:3078. doi: 10.4314/ahs.v19i4.29
43. Lawal, SA, Okunlola, DA, Adegboye, OA, and Adedeji, IA. Mother’s education and nutritional status as correlates of child stunting, wasting, underweight, and overweight in Nigeria: evidence from 2018 demographic and health survey. Nutr Health (2023), doi: 10.1177/02601060221146320 [Epub ahead of print].
44. Adepoju, OT, and Bukola, B. Association between stunting and obesity among underfive children in urban and rural areas of Oyo state, Nigeria. Malays J Nutr. (2018) 24:25–34.
45. Ekholuenetale, M, Tudeme, G, Onikan, A, and Ekholuenetale, CE. Socioeconomic inequalities in hidden hunger, undernutrition, and overweight among under-five children in 35 sub-Saharan Africa countries. J Egypt Public Health Assoc. (2020) 95:1–15. doi: 10.1186/s42506-019-0034-5
46. Agu, N, Emechebe, N, Yusuf, K, Falope, O, and Kirby, RS. Predictors of early childhood undernutrition in Nigeria: the role of maternal autonomy. Public Health Nutr. (2019) 22:2279–89. doi: 10.1017/S1368980019000818
47. Nkeiruka, OA, and Ogechi, N. Infant feeding practices of mothers/caregivers and anthropometric indices of infants (0-12 months) in Etche local government area, Rivers state, Nigeria. Int J Innov Res Sci Eng Technol. (2018) 7:1074–80.
48. Danimoh, MA, Idris, SH, Dikko, HG, Olorukooba, AA, Mohammed, A, and Ayodeji, OO. Nutritional status and its determinants among Fulani children aged 6-24 months in a rural Community of Kaduna State, Northwest Nigeria. Eur J Nutr Food Saf. (2020) 12:32–41. doi: 10.9734/ejnfs/2020/v12i630236
49. Amadi, OF, Ezenwosu, O, and Odetunde, OI. A cross-sectional study on nutritional status of preschool aged children in Enugu urban, Nigeria. J Exp Res. (2018) 6:19–26.
50. Osunmakinwa, OO, Oladoyin, VO, Okunlola, O, Ibirongbe, D, Oyeyemi, OT, Awosusi, A, et al. Addressing malnutrition in children: an appraisal of the Ondo state nutrition program. Cureus. (2022) 14:e28595. doi: 10.7759/cureus.28595
51. Ogunnaike, MG, Shittu, AM, Fapojuwo,, Oluwakemi, E, Kehinde,, and Mojisola, O. (2018). Effects of gender gaps in livelihood assets and adoption of climate amrt practices on nutritional outcomes of children in Nigeria. Available at: https://ageconsearch.umn.edu/record/273908
52. Ezeofor, IO, Garcia, AL, and Wright, CM. Criteria for undernutrition screening in hospitalised infants under 6 months: a diagnostic accuracy study in a resource-poor setting. Arch Dis Child. (2020) 105:524–9. doi: 10.1136/archdischild-2019-318313
53. Akande, YO, Abata, GD, Babalola, AO, and Abata, EO. Nutritional status of under five children attending state hospital Okitipupa Ondo state. Int J Res Sci Innov. (2019) VI.
54. Atimati, AO, and Adam, VY. Infant and young child feeding practices and nutritional status of children (0-24 months) in Egor local government area of Edo state, Nigeria. Nigerian J Nut Sci. (2019) 40:1–11.
55. Ezeh, OK, Abir, T, Zainol, NR, Al, MA, Milton, AH, Haque, MR, et al. Trends of stunting prevalence and its associated factors among nigerian children aged 0–59 months residing in the northern Nigeria, 2008–2018. Nutrients. (2021) 13:4312. doi: 10.3390/nu13124312
56. Seer-Uke, EN, Samuel, ES, Agajah, ME, Ikpato, VT, Tyoakaa, AA, Abugu, LI, et al. Nutritional status of children under age five in Benue state, Nigeria. Afr J Food Agric Nutr Dev. (2021) 21:18391–403.
57. Adeniyi, OF, Ekure, E, Olatona, FA, Ajayi, EO, and Nworgu, N. Nutritional assessment and maternal perception of toddler body size using toddler Silhouette scale in Nigeria a developing country. Int J MCH AIDS. (2018) 7:9. doi: 10.21106/ijma.217
58. Manyong, VM, Abdoulaye, T, Ojide, M, Ogundapo, A, Ayoola, GB, Dashiell, K, et al. Household hunger, poverty, and childcare in 5 states of Nigeria and their impacts on nutritional outcomes in preschool children. Food Nutr Bull. (2021) 42:188–209. doi: 10.1177/03795721211009482
59. Afolami, I, Samuel, F, Borgonjen-Van Den Berg, K, Mwangi, MN, Kalejaiye, O, Sanusi, RA, et al. The contribution of provitamin a biofortified cassava to vitamin a intake in Nigerian pre-schoolchildren. Br J Nutr. (2021) 126:1364. doi: 10.1017/S0007114521000039
60. Afolabi OFSaka, AO, Ojuawo, A, and Biliaminu, SA. Serum zinc levels of hospitalized children with acute diarrhea differ by the isolated viruses. Int J Health Sci. (2019) 13:4.
61. Ecker, O, Comstock, A, Babatunde, RO, and Andam, KS. (2020). Poor dietary quality is Nigeria’s key nutrition problem. doi: 10.2499/p15738coll2.133738
62. Isa, H, Bashir, M, and Adedeji, BA. Malaria prevalence and anemia status of children attending a health Facility in Yola. J Adv Microbiol. (2022) 8:25–31.
63. Ajakaye, OG, and Ibukunoluwa, MR. Prevalence and risk of malaria, anemia and malnutrition among children in IDPs camp in Edo state, Nigeria. Parasite Epid Cont. (2020) 8:e00127. doi: 10.1016/j.parepi.2019.e00127
64. Hanson, C, Lyden, E, Anderson-Berry, A, Kocmich, N, Rezac, A, Delair, S, et al. Status of Retinoids and carotenoids and associations with clinical outcomes in maternal-infant pairs in Nigeria. Nutrients. (2018) 10:1286. doi: 10.3390/nu10091286
65. Afolami, I, Mwangi, MN, Samuel, F, Boy, E, Ilona, P, Talsma, EF, et al. Daily consumption of pro-vitamin a biofortified (yellow) cassava improves serum retinol concentrations in preschool children in Nigeria: a randomized controlled trial. Am J Clin Nutr. (2021) 113:221–31. doi: 10.1093/ajcn/nqaa290
66. Owolabi, AJ, Senbanjo, IO, Oshikoya, KA, Boekhorst, J, Eijlander, RT, Kortman, GAM, et al. Multi-nutrient fortified dairy-based drink reduces anaemia without observed adverse effects on gut microbiota in anaemic malnourished nigerian toddlers: a randomised dose–response study. Nutrients. (2021) 13:1566. doi: 10.3390/nu13051566
67. Kennedy, CU, Chukwuebuka, NO, and Uchenna, E. Serum zinc levels in apparently healthy children in Nigeria: are they acceptable. Niger Med J. (2020) 61:291. doi: 10.4103/nmj.NMJ_20_20
68. Resnick, D, Anigo, K, and Anjorin, OM. (2021). Enabling environments for nutrition advocacy: A comparison of infant and young child feeding and food fortification in Nigeria [internet]. Available at: https://papers.ssrn.com/abstract=3955168
69. Iheme, GO, Nzeagwu, OC, Uzokwe, CA, Matthew, S, and Edafioghor, LO. A meta-analysis of compliance with revised WHO-infant and young child feeding indicators in data generation. Clin Nutr ESPEN. (2021) 43:169–73. doi: 10.1016/j.clnesp.2021.03.016
70. Samuel, FO, and Ibidapo, EG. Complementary feeding practices and associated factors among nursing mothers in southwestern Nigeria. Int J Mat Child Health AIDS. (2020) 9:223–31. doi: 10.21106/ijma.363
71. Omotoye, FE, and Adesanmi, RAS. Infant and young child-feeding practices in two local government areas in southwest, Nigeria. J Food Sci Nutr Res. (2019) 2:136–45.
72. United Nation Development Program (2023). Nigeria multidimensional poverty index [internet]. Available at: http://www.undp.org/nigeria-multidimensional-poverty-index [Accessed August 7, 2023].
73. Grantham-McGregor, S, and Ani, C. A review of studies on the effect of Iron deficiency on cognitive development in children. J Nutr. (2001) 131:649S–68S. doi: 10.1093/jn/131.2.649S
74. Degarege, A, Erko, B, Negash, Y, and Animut, A. Intestinal helminth infection, Anemia, undernutrition and academic performance among school children in northwestern Ethiopia. Microorganisms. (2022) 10:1353. doi: 10.3390/microorganisms10071353
75. Ramachandran, P, and Gopalan, HS. Undernutrition & risk of infections in preschool children. Indian J Med Res. (2009) 130:579–83.
76. Muhoozi, GKM, Atukunda, P, Mwadime, R, Iversen, PO, and Westerberg, AC. Nutritional and developmental status among 6- to 8-month-old children in southwestern Uganda: a cross-sectional study. Food Nutr Res. (2016) 60:30270. doi: 10.3402/fnr.v60.30270
77. Matrins, VJB, Toledo Florêncio, TMM, Grillo, LP, Franco M do, CP, Martins, PA, APG, C, et al. Long-lasting effects of undernutrition. Int J Environ Res Public Health. (2011) 8:1817–46. doi: 10.3390/ijerph8061817
78. Lozoff, B, Jimenez, E, Hagen, J, Mollen, E, and Wolf, AW. Poorer behavioral and developmental outcome more than 10 years after treatment for iron deficiency in infancy. Pediatrics. (2000) 105:E51. doi: 10.1542/peds.105.4.e51
79. Ingram, J., IFPRI Blog (2018). To address the triple burden of malnutrition, focus on food systems and demand | IFPRI.
80. Christian, AK, and Dake, FAA. Profiling household double and triple burden of malnutrition in sub-Saharan Africa: prevalence and influencing household factors. Public Health Nutr. (2022) 25:1563–76. doi: 10.1017/S1368980021001750
81. Srivastava, S, and Upadhyay, AK. A success story of reduction in childhood stunting and underweight in India: analysis of pooled data from three rounds of Indian demographic and health surveys (1998-2016). J Biosoc Sci. (2020) 54:106–23. doi: 10.1017/S002193202000070X
82. Angood, C, Khara, T, Dolan, C, Berkley, JA, Roberfroid, D, Seal, A, et al. Research priorities on the relationship between wasting and stunting. PLoS One. (2016) 11:e0153221. doi: 10.1371/journal.pone.0153221
83. Thurstans, S, Sessions, N, Dolan, C, Sadler, K, Cichon, B, Isanaka, S, et al. The relationship between wasting and stunting in young children: a systematic review. Mat Child Nut. (2022) 18:e13246. doi: 10.1111/mcn.13246
84. Dhami, MV, Ogbo, FA, Osuagwu, UL, and Agho, KE. Prevalence and factors associated with complementary feeding practices among children aged 6-23 months in India: a regional analysis. BMC Public Health. (2019) 19:1–16. doi: 10.1186/s12889-019-7360-6
85. Loli, S, and Carcamo, CP. Rotavirus vaccination and stunting: secondary data analysis from the Peruvian demographic and health survey. Vaccine. (2020) 38:8010–5. doi: 10.1016/j.vaccine.2020.10.044
86. Wilson, AL, Bradley, J, Kandeh, B, Salami, K, D’Alessandro, U, Pinder, M, et al. Is chronic malnutrition associated with an increase in malaria incidence? A cohort study in children aged under 5 years in rural Gambia. Parasit Vectors. (2018) 11:451. doi: 10.1186/s13071-018-3026-y
87. Islam, MR, Rahman, MS, Rahman, MM, Nomura, S, De Silva, A, Lanerolle, P, et al. Reducing childhood malnutrition in Bangladesh: the importance of addressing socio-economic inequalities. Public Health Nutr. (2020) 23:72–82. doi: 10.1017/S136898001900140X
88. Husseini, M, Darboe, MK, Moore, SE, Nabwera, HM, and Prentice, AM. Thresholds of socio-economic and environmental conditions necessary to escape from childhood malnutrition: a natural experiment in rural Gambia. BMC Med. (2018) 16:199. doi: 10.1186/s12916-018-1179-3
89. Gombart, AF, Pierre, A, and Maggini, S. A review of micronutrient and immune system. Nutrients, (2020) 12:236. doi: 10.3390/nu12010236
90. Ciosek, Ż, Kot, K, Kosik-Bogacka, D, Łanocha-Arendarczyk, N, and Rotter, I. The effects of calcium, magnesium, phosphorus, fluoride, and lead on bone tissue. Biomolecules. (2021) 11:506. doi: 10.3390/biom11040506
91. Harika, R, Faber, M, Samuel, F, Kimiywe, J, Mulugeta, A, and Eilander, A. Micronutrient status and dietary intake of iron, vitamin a, iodine, folate and zinc in women of reproductive age and pregnant women in Ethiopia, Kenya, Nigeria and South Africa: a systematic review of data from 2005 to 2015. Nutrients. (2017) 9:1096. doi: 10.3390/nu9101096
Keywords: children below 5 years, Nigeria, poor quality of complementary feedings, multiple undernutrition issues, targeted interventions
Citation: John C, Poh BK, Jalaludin MY, Michael G, Adedeji I, Oyenusi EE, Akor B, Charles NC, Buthmanaban V and Muhardi L (2024) Exploring disparities in malnutrition among under-five children in Nigeria and potential solutions: a scoping review. Front. Nutr. 10:1279130. doi: 10.3389/fnut.2023.1279130
Edited by:
Emmanuel Cohen, UMR7206 Eco Anthropologie et Ethnobiologie (EAE), FranceReviewed by:
Olutosin Ademola Otekunrin, Federal University of Agriculture, Abeokuta, NigeriaCopyright © 2024 John, Poh, Jalaludin, Michael, Adedeji, Oyenusi, Akor, Charles, Buthmanaban and Muhardi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Collins John, cchibunkem@yahoo.com
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.