
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr., 14 December 2023
Sec. Nutritional Epidemiology
Volume 10 - 2023 | https://doi.org/10.3389/fnut.2023.1248908
 Teresa Partearroyo1*
Teresa Partearroyo1* María de Lourdes Samaniego-Vaesken1
María de Lourdes Samaniego-Vaesken1 Paula Rodríguez-Alonso2María José Soto-Méndez3
Paula Rodríguez-Alonso2María José Soto-Méndez3 Ángela Hernández-Ruiz3
Ángela Hernández-Ruiz3 Ángel Gil3,4,5,6,7
Ángel Gil3,4,5,6,7 Gregorio Varela-Moreiras1
Gregorio Varela-Moreiras1Background: Methionine-methylation cycle and the derived critical functions during infancy are key regulated by folates, vitamins B12, and B6. At present in Spain, there is an absence of studies that assess the intakes and dietary sources of total folates and B12 by children consuming all types of milks and those regularly consuming adapted milk formulas. Thus, our aim was to evaluate folates intakes alongside with vitamins B6 and B12 while describing their major dietary contributors in Spanish children aged one to <10 years.
Methods: A total of 1,448 children aged between 1 and 10 years (49.7% girls and 50.3% boys) from the EsNuPI, a prospective cross-sectional study, were allocated into two cohorts: one Spanish Reference Cohort (SRS) of the general population (n = 707), and another including children consuming adapted milks called Adapted Milk Consumers Cohort (AMS) (n = 741) completed two 24 h dietary recalls used to estimate their nutrient intakes and to compare them to the European Food Safety Authority (EFSA) Population Reference Intakes.
Results: The median intake of vitamin B6 was 1.35 (1.06–1.70) mg/day in the SRS and 1.45 (1.17–1.79) mg/day in the AMS, being significantly higher in the AMS for all age-groups. Prevalence of adequacy for vitamin B6 in the SRS and AMS was 97.7 and 98.7%, respectively. Total folates intakes in the AMS were significantly higher (p ≤ 0.001) in all age groups than in the SRS, independently of age. In addition, the prevalence of adequacy for folates intakes in all groups was more than 60%. Vitamin B12 intake increased with age independently of the type of milk consumed. The prevalence of adequacy for vitamin B12 was highly compliant by all population groups. The major contributors to vitamin B6 were milk and dairy products being significantly higher in AMS than SRS (p ≤ 0.001). The highest contributors to folates intakes were milk and dairy products, cereals, vegetables, and fruits in both groups whereas for vitamin B12 in the SRS sample were milk and dairy products followed by meat and meats products and for adapted milks, were milk and dairy products, followed by eggs, then meat and meats products.
Conclusion: A satisfactory prevalence of adequacy for vitamins B6, and B12 amongst the Spanish children population was observed, which was not the case for folates, regardless of the dietary group evaluated. Nevertheless, a possible strategy to increase folate intake among the youngest children is to increase the consumption of milk and dairy products within a healthier dietary pattern, as these may contribute significantly to the vitamin needs of the infant population.
More than 20 years after the publication of the breakthrough study that revolutionized supplementation policies worldwide, the Medical Research Council Vitamin Study (1), today it is widely recognized that folates deficiency during the periconceptional period can contribute to the development of Neural Tube Defects (NTDs) in the fetus or even affect/impact the newborn with incapacitant conditions such as spina bifida, anencephalia or even heart defects (2, 3). In addition, the availability of the omega-3 long-chain polyunsaturated fatty acid docosahexaenoic, also needed for normal brain development, might be limited by an impaired one-carbon metabolism (4) for which folates, vitamins B12 and B6 are key nutritional regulators. Vitamin B6 and folates are closely working toward maintenance of essential developmental and adult processes (5). In fact, vitamin B6 active form, pyridoxal 5′-phosphate, regulate folates levels and it is a necessary cofactor for enzymes involved in the folates metabolism (Figure 1) (6, 7). Therefore, vitamin B6, folates, and vitamin B12 deficits during child growth might additionally compromise brain development and cognitive function in the future (8). Moreover, the American Academy of Pediatrics has issued a statement advocating a focus on key nutrients for brain development, such as folic acid, vitamin B6 and B12, among others (9).
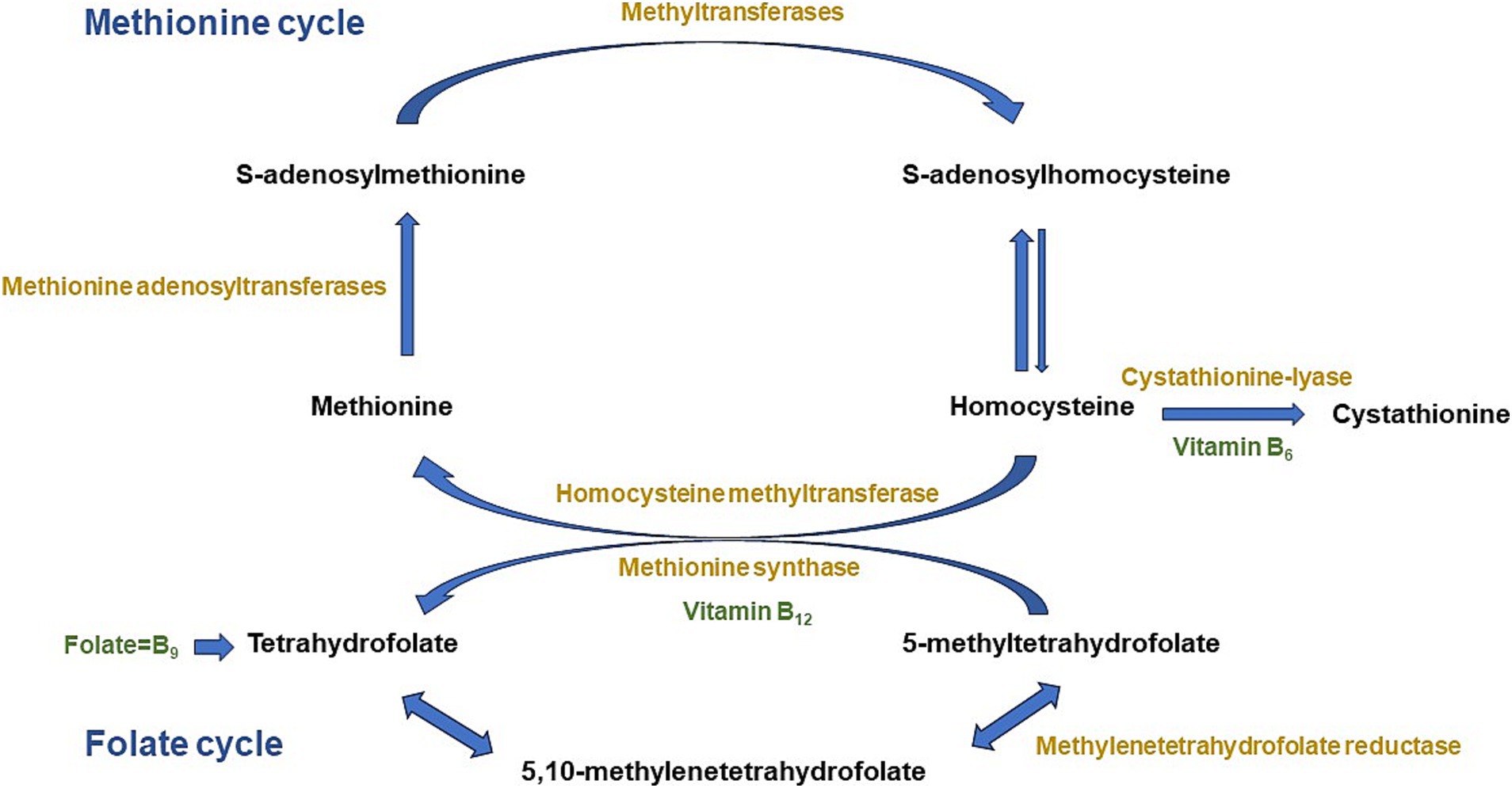
Figure 1. Methionine and folate metabolism and connecting pathways. Adapted from Partearroyo et al. (6).
Folates is the generic term that encompasses several vitamers with the activity of pteroylglutamic acid or vitamin B9 (10), that plays a crucial role in the metabolism of the developing child. Its functions include red blood cell formation and DNA synthesis through the one-carbon cycle (11). Folic acid (FA) is the synthetic form that has a higher bioavailability and which is commonly used in dietetic supplements and fortified food products such as wheat flour (e.g., mandatory fortification) or breakfast cereals (e.g., mainly, voluntary fortification) (12). Like folates, vitamin B6 encompasses a neuroprotective role being a cofactor for glutathione and decreasing the brain’s susceptibility to oxidative stress-based damage (13) and its deficiency contributes to neurodegeneration (14). Vitamin B12 or cyanocobalamin is also involved in red blood cell formation (11) but while folic acid is effective in the treatment of pernicious and other macrocytic anemias (15), vitamin B12 can prevent megaloblastic anemia (16). The interconnection of these vitamins within the one-carbon cycle has been the subject of several studies in the past and still at present, although there is great controversy regarding populations at risk for their deficiency, of which infants are a crucial group to follow up. On the other hand, a strong reason for concern amongst public health authorities about excessive FA intakes has been unmetabolized FA in non-target groups as it was shown that it could accelerate or promote cancer, specifically colorectal (17). Thus, the European Union has not implemented mandatory fortification of any food product and only voluntary fortification takes place. Previous research by Samaniego-Vaesken et al. (18) described the typology and level of fortification available in the Spanish market: most products being ready-to eat breakfast cereals and confectionery products (usually high in added sugars and salt). However, other products such as FA fortified milk and beverages were also frequent. Unfortunately, consumption of these products remains unknown as we lack updated information of fortified food intakes by the Spanish population, including toddlers and children. A study by Egan et al. (19) in Ireland (a voluntary fortification market very similar to the Spanish one in terms of types of products and levels of fortification) showed that voluntary FA fortification levels of food products in Ireland were declining since 2014, and that this might pose implications for FA intakes.
Paradoxically, up to date we did not have a representative sample of the pediatric population like the one provided by the EsNuPi study [Estudio Nutricional en Población Infantil Española (Nutritional Study in Spanish Pediatric Population)] performed in Spanish children aged one to <10 years old (20) in order to update and improve the knowledge on micronutrient intakes related to the methionine cycle.
The novelty of the present work relies on data of micronutrients related to the methionine cycle that has not been previously published elsewhere and does not contain excessive overlap with previously published data from the ESNUPI study. Intakes of these vitamins have not been published in a sample of this age range (one to <10 years old) which is representative of the Spanish population.
Therefore, there is an urgent need for a better and more updated knowledge of the intakes of vitamins related to the methionine cycle in the Spanish pediatric population in order to prevent and/or delay the adverse effects derived from inadequate intakes in this stage of life. In fact, in the present study our objective was to assess folates intakes alongside vitamins B6 and B12 and to describe their major dietary contributors as well as to study the differences between infants who usually consume adapted milks and those consuming all types of milk.
The EsNuPI study is a prospective, cross-sectional, observational study, that took place between October 2018 and January 2019. Full design, protocol and methodology have been published elsewhere (20). The EsNuPI study evaluated the dietary patterns and nutrient intake, in addition to physical activity and sedentary behaviors of Spanish children that lived in urban areas with >50,000 inhabitants, from nine geographical areas as established by Nielsen. These urban areas represent 1.8% of the total number of municipalities of Spain and 52.6% of the total Spanish children population of one to <10 years old (21). We compared two subsamples aged one to <10 years old, one comprising the urban non-vegan individuals who consumed all types of milk in the last 12 months, the “Spanish Reference Sample, SRS,” and another called “Adapted Milk Consumers Sample, AMS” of non-vegan subjects from urban areas who only consumed adapted milks in the last 12 months. The “adapted milks” food group included infant formulas, follow-on milk formulas, toddler’s milk formulas (also known as “young children milk formulas” and in Spain called “growing up” milk formulas) and fortified and enriched milk formulas [i.e., with added docosahexaenoic acid (DHA), calcium, vitamin D, and/or iron]. Originally, the estimated sample consisted of 1,500 individuals, and the sample errors were ± 2.52% and ± 2.59%, respectively, for a 95.5% confidence level and estimation of equally probable categories (p = q = 50%), considering a universe of 2,205,646 children. Final recruitment included a total of 1,514 children (n = 742 SRS; n = 772 AMS) and 1,448 individuals finished the study (95.6% response rate). The EsNuPI study was performed under the declaration of Helsinki, approved by the University of Granada ethical committee (No. 659/CEIH/2018), and registered in ClinicalTrials.gov (Unique Protocol ID: FF01/2019).
A face-to-face interview was completed by participants who provided sociodemographic information and a first 24-h dietary recall (24-h DR). Then, after a week, a second 24-h DR was answered by participants by telephone. The two 24- DR included both, a holiday and school day. MADISON MK (TELECYL. S.A.) collected all personal data of respondents in order to manage and carry out the survey. MADISON MK is responsible and adapted to the new General Data Protection Regulation of the European Union (EU) 2016/679. Each participant provided express consent to participate in the survey. Once the data collection and the survey verification work were finished, the files obtained were anonymized for their processing. Fieldwork was undertaken from October 2018 to January 2019. Further information has been provided by (20).
A general questionnaire was used to collect the following variables in the first interview: place and date of birth, gender, academic level of parents or caregivers (elementary or less/secondary/university/higher education), place of residence, family income level, lifestyle, activity patterns, and sedentary behaviors. Height and weight data were declared by parents or caregivers, based on the child’s pediatric health card.
Two independent 24-h DR to determine children’s dietary intake (proxy report) were provided by parents or caregivers; that included a week and a weekend day (non-consecutive), one being face-to-face and the other by telephone a week later.
Dietary intake was thoroughly described by including the ingredients and methods of preparation that were organized as mealtimes (breakfast, mid-morning, lunch, midafternoon, dinner, and other moments) in order to calculate energy and nutrient distribution during the day.
Assessment of children intakes encompasses many methodological difficulties such as misreporting. Its calculation was performed by the protocol proposed by the European Food Safety Authority (EFSA), based on the work by Goldberg (22) and Black (23) that evaluates the reported energy intake (EIrep) against the energy requirements. In the present manuscript, results included were not adjusted for misreporting, as in the previous study by from Madrigal et al. (24) exclusion of misreporters in the EsNuPI population showed no significant differences in the total energy intake (TEI) and the distributions of relative macronutrient intakes. Thus, it was assumed that it does not significantly modify the results and conclusions of this study.
The adequate completion of the survey was facilitated by resources such as the “Tables of common home measures and habitual portion sizes for the Spanish population” (25) and the “Photo guide of common portions sizes of Spanish foods” (26) that were used by interviewers. In order to calculate the food, beverage, energy and nutrient intakes, the “VD-FEN 2.1” software, a Dietary Evaluation Program developed by the Spanish Nutrition Foundation (FEN) was used. Total folates, B6, and B12 intakes were obtained by calculating the prevalence of adequacy for these micronutrients which was defined as the percentage of the studied population (%) that showed intakes of these vitamins above 80% of the Population Reference Intakes (PRIs) established by the EFSA (27).
The collection of reported dietary intake data resulted in a total of 746 food items that were categorized into 18 food groups as described (20) and then converted into energy and nutrient data for analysis. All estimates were made from an average across the 2 days of diet recording. The normality of the distribution of the variables was obtained with the Kolmogorov-Smirnoff normality test. Median and interquartile range (IQR) were used for continuous variables and frequencies and percentages for categorical variables, to describe folates, vitamins B6, and B12 intake by type of sample (SRS and AMS) gender and age groups. The Mann–Whitney U-test was used for comparisons between SRS and AMS by gender and age group. Kruskal–Wallis Test and the Dunn Test were used to adjust for multiple comparisons and adjustment of the value of p with Bonferroni correction were used to calculate differences among each age group within samples. The level of significance was established at p < 0.05. IBM SPSS 27.0 (IBM Corp., Armonk, NY, USA) was used to perform data analysis.
A total of 1,448 children between the ages of 1 to <10 years (49.7% girls and 50.3% boys) completed the study. Their anthropometric, sociodemographic, and physical activity characteristics have been previously published (24, 28).
Total folates intakes, as well as the prevalence of adequacy are shown in Table 1 for each cohort, by gender and age. When results were analyzed by cohorts, we found that total folates intakes in the AMS were significantly higher (p ≤ 0.001) in all age groups than in the SRS, independently of age. In addition, regarding the prevalence of adequacy for folates intakes (% population above 80% PRI), we found that more than 60% of individuals complied with the recommendations within all groups. However, it is important to note that the prevalence of adequacy to recommended folates intakes for this Spanish young population was significantly higher in the adapted milk cohort than in the reference cohort (p ≤ 0.001), except for the 1 to <3 years group, which did not differ statistically between cohorts.
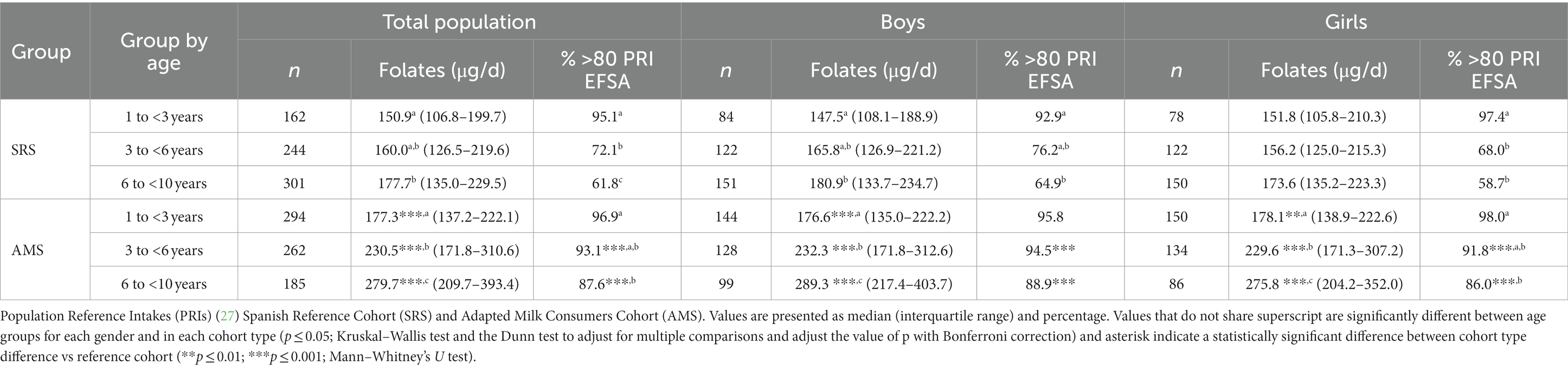
Table 1. Folates intakes and prevalence of adequacy (percentage of population > 80% PRI) by gender and age group in the Spanish Pediatric Population (EsNuPI) study.
Conversely, we observed that when results were analyzed by age groups, as expected, total folates intakes were significantly higher amongst older groups independently of the type of milk consumed, except in the SRS, which had a similar total folates intake regardless of gender and age-group to which they belonged.
When evaluating the proportion of children who reached more than 80% of the PRI for folates by age and gender, we found that, when segmented by gender, in all groups >55% of the individuals met the recommendations. In addition, it is worth emphasizing that the children who consumed adapted milk showed a higher compliance with the recommendations than those from the reference group, except those from early ages (1 to <3 years), who had a high level of compliance with recommendations independently the type of milk they consumed.
Table 2 presents the daily intake of vitamin B6 in the study population and separately by age and gender groups, as well as differentiating between the SRS and the AMS. The median intake of vitamin B6 was 1.35 (1.06–1.70) mg/day in the SRS and 1.45 (1.17–1.79) mg/day in the AMS cohort. Vitamin B6 intakes were significantly higher in the AMS for all age groups with respect to SRS. However, no significant differences were observed regarding vitamin B6 intakes within age groups across the whole sample. Prevalence of adequacy for vitamin B6 in the SRS and AMS was 97.7 and 98.7% respectively, in line with the EFSA criteria (Table 2). Furthermore, the prevalence of adequacy for vitamin B6 estimated by the EFSA criteria was significantly higher in AMS, independently of age (Table 2).
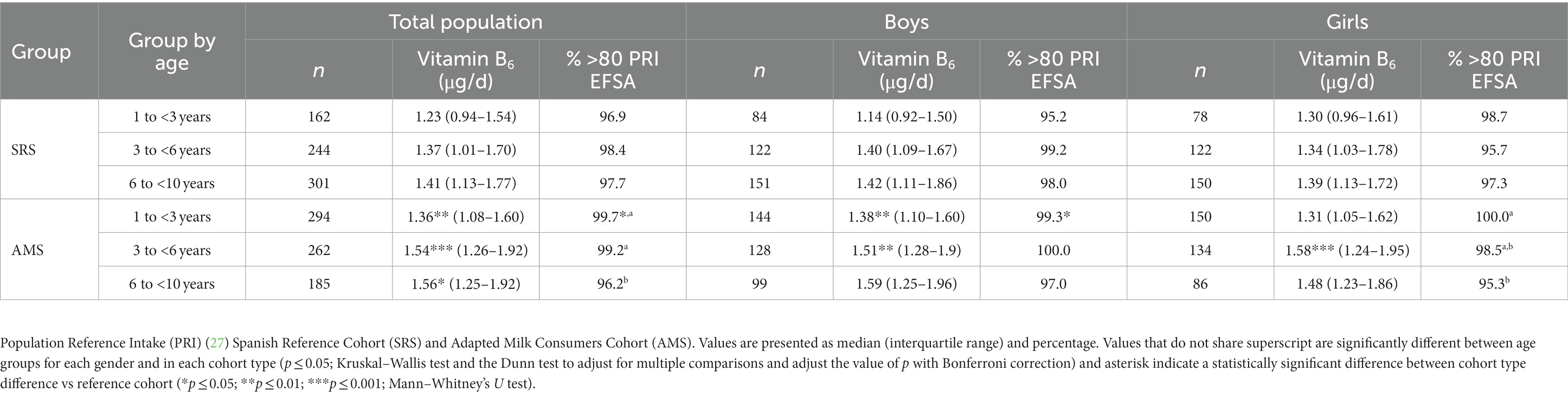
Table 2. Vitamin B6 intakes and prevalence of adequacy (percentage of population > 80% PRI) by gender and age group in the Spanish Pediatric Population (EsNuPI) study.
Table 3 shows the obtained daily intake levels of vitamin B12 by age group, which increased with age independently of the type of milk consumed. When comparing age subgroups, we detected important differences in B12 vitamin intakes amongst boys aged 1 to <3 years, where the AMS had lower vitamin B12 consumption (p ≤ 0.05). Furthermore, the potential prevalence of adequacy for B12 was above 80% PRI in the total study population according to the European PRI (Table 3). Also shown in Table 3 are the results by the total population and age group. When data were analyzed stratified by age group, we found that the prevalence of adequacy for vitamin B12 in accordance with the European PRI was highly compliant by all population groups (>95% compliance) but was significantly higher in the AMS children aged 1 to 3 years vs. the SRS group.
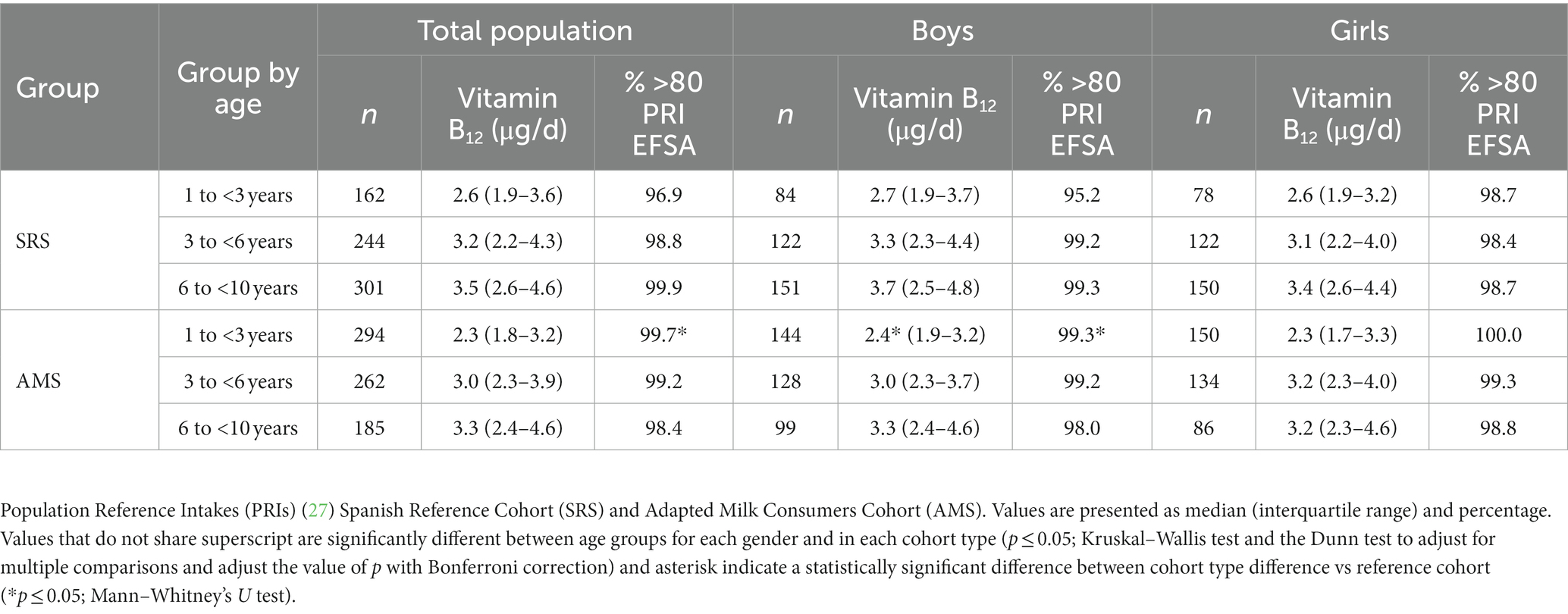
Table 3. Vitamin B12 intakes and prevalence of adequacy (percentage of population above 80% PRI) by gender and age group in the Spanish Pediatric Population (EsNuPI) study.
Figure 2 shows and categorizes the main sources of folates intakes by age group for both samples, amongst children from the EsNuPI study. Data are presented as the median of proportional contribution and only for those foods which contributed at least 1% to folates intakes of the population.
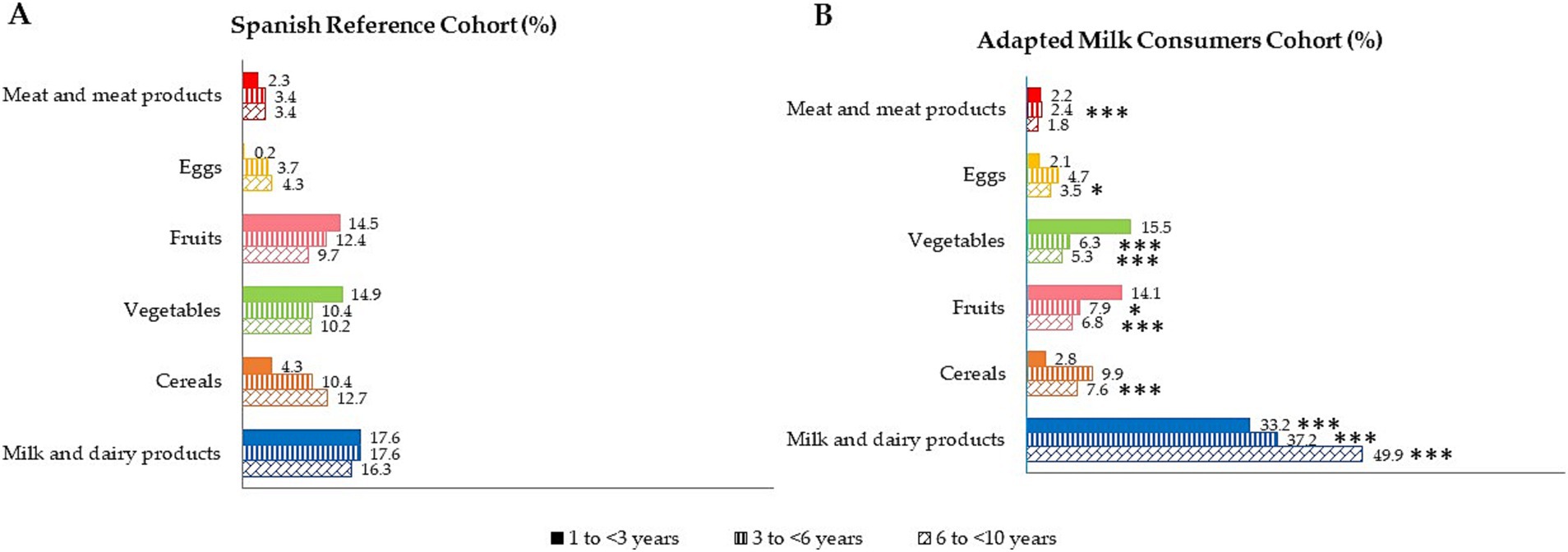
Figure 2. Dietary food and beverage groups contributing to total folates intakes (%) from the EsNuPI study population (“Spanish Pediatric Population”) in both Spanish Reference Cohort (A) and the Adapted Milk Consumers Cohort (B). *p ≤ 0.05 compared to the reference cohort (Mann-Wllitney test). ***p≤0.001 compared to the reference cohort (Mann-Wllitney test). Only foods contributing to folates intakes of the population have been included.
The highest contributors to folates intakes were milk and dairy products, cereals, vegetables, and fruits, in the whole pediatric population. For children in the AMS aged 1 to 3 years, a significantly different contribution was observed, with a higher contribution to folates from the milk and dairy products group AMS compared to the SRS (p ≤ 0.001). Equally, AMS children aged 3 to 6 years had a higher contribution of folates from milk and dairy products (p ≤ 0.001), and a lower folates contribution from vegetables (p ≤ 0.001), meat and meats products (p ≤ 0.001), and fruits (p ≤ 0.05) than SRS children of the same age. The older age group of the AMS presented a higher contribution of folates from milk and dairy products (p ≤ 0.001) and lower contribution from cereals (p ≤ 0.001), meat and meats products (p ≤ 0.001), fruits (p ≤ 0.001), eggs (p ≤ 0.05), and vegetables (p ≤ 0.001) than their counterparts of the SRS.
The contribution (%) of food and beverage categories to the daily vitamin B6 intake is shown, categorized by age group for both samples, in Figure 3. It should be noted that only those foods that contributed at least 1% to the vitamin B6 intake of the population have been included. Milk and dairy products were the main contributors to vitamin B6 for the whole study sample, being significantly higher in AMS than SRS (p ≤ 0.001). The following largest contributors were fruits and meat and meat products, as well as vegetables, with differences between the two cohorts.
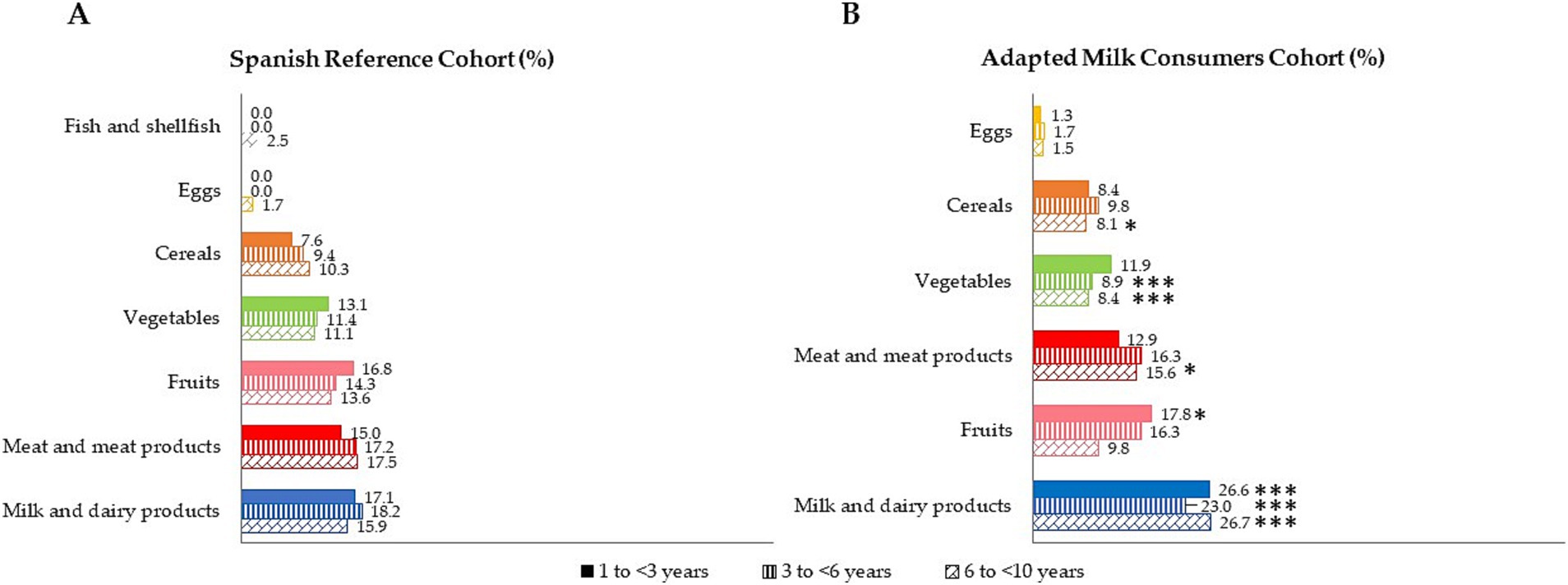
Figure 3. Dietary food and beverage groups contributing to total vitamin B6 intakes (%) from the EsNuPI study population (“Spanish Pediatric Population”) in both Spanish Reference Cohort (A) and the Adapted Milk Consumers Cohort (B). *p≤0.05 compared to the reference cohort (Mann-Wllitney test). ***p≤0.001 compared to the reference cohort (Mann-Wllitney test). Only foods contributing to vitamin B6 intakes of the population have been included.
The median contribution (%) of food groups to vitamin B12 intake, categorized by age group for both samples is shown in Figure 4. Data are presented as the median of proportional contribution and only for those foods which contributed at least 1% to vitamin B12 intakes of the population. In particular, food groups with the highest median proportional contribution to total vitamin B12 intake in the reference sample (SRS) were firstly milk and dairy products (38.3%), followed by meat and meats products (13.1%). Next, eggs accounted for 8.2% of total vitamin B12 intake and, finally, fish and shellfish contributed 4.7%. Moreover, we observed that amongst the sample of adapted milk consumers (AMS), the largest contributors to vitamin B12 intakes were milk and dairy products (42.4%), eggs (12.9%), and meat and meat products (11.1%).
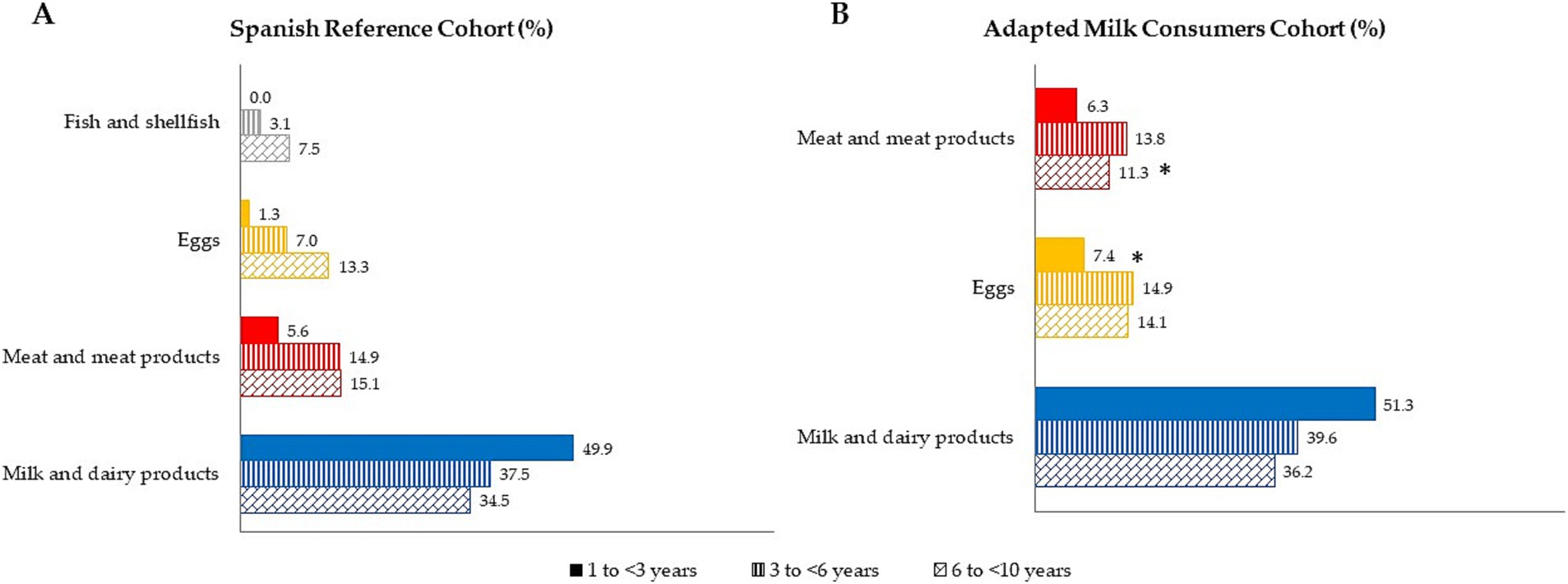
Figure 4. Dietary food and beverage groups contributing to vitamin B12 intakes (%) from the EsNuPI study population (“Spanish Pediatric Population”) in both reference cohort (A) and the Adapted Milk Consumers Cohon (B). *p≤0.05 compared to reference cohort (Mann-Wllitney test). Only foods contributing >l% to vitamin B12 intakes of the population have been included.
When comparing samples by age group (Figure 4), AMS children between 3 and < 6 years obtained higher levels of vitamin B12 intake from eggs (p ≤ 0.05) than SRS children of the same age. In addition, SRS children from 6 to <10 years had a lower contribution to vitamin B12 intake from the meat and meats products group than their counterparts of the AMS (p ≤ 0.05).
It is acknowledged that poor nutritional status, especially suboptimal status of folates, and vitamins B6 and B12 can affect brain function and cognitive performance (29), namely by perturbing one-carbon metabolism, and this can take place in early as well as in later life (30). Children of school age need adequate cognition to obtain higher academic performance (31). As a matter of fact, cognitive processes are substantially related with brain function, physiology and structure (32) and, therefore, its development can be highly dependent on nutrition, physical activity, and social and economic status. For this reason, we studied folates together with vitamins B6 and B12, to find their intakes and major dietary contributors and also to describe the differences between infants at school age who usually consume adapted milks and those consuming all types of milk. In fact, at the light of the results from the present study, we observed a suitable intake of vitamins B6 and B12 but not for folates amongst Spanish children. In turn, we observed that children consuming adapted milk products had higher folates compliance.
Back in 2008, comprehensive reviews published by Black (8) and Molloy (33) examined the mechanisms linking folates and vitamin B12 deficiency to abnormal behaviors and development in infants (disruptions to myelination and inflammatory processes), as well as the effects resulting from these deficiencies. Prevention of folates and vitamin B12 deficiencies is pivotal to this age group and should mostly rely on dietary sources as supplementation is only left to specific situations such as strict vegetarian or vegan children who should supplement B12 (34). Vitamin B12 sources are almost exclusively obtained from the animal kingdom and, therefore, these groups might develop deficiencies if not adequately supplemented. Indeed, a child who is deficient in vitamin B12, will continue to suffer from deficiency symptoms if it is not diagnosed early in infancy. Therefore, school-aged children with B12 deficiency could be affected by altered motor development, cognitive disorders, and speech and language skills impairment (35). Folates which play a key role in the metabolism of the developing child (11) and vitamin B12 deficiency could result in irreversible damage, such as growth stunting (36). In fact, there is also a growing interest in comparing breast and formula feeding in early infancy and their impact later in life, particularly concerning developing diseases such as obesity, hypertension, hyperlipidemia, and diabetes mellitus (37). It is important to highlight that breast milk and/or infant formula are the only sources of nutrition during early infancy and should provide suitable quantities of energy, water, and all essential nutrients (38).
The magnitude of the folate inadequacy in this study in the SRS group was 27%. It was higher than in the study conducted by Serra-Majem et al. (39), in which when assessing the percentage of population predicted to have inadequate intakes of folates using a probability approach, boys 2–5 years had 2.5% and those 6–9 years had 1.7%; however, girls 2–5 years showed 10.1% and those 6–9 years just 2.1%, and the National Dietary Survey on the Child and Adolescent Population in Spain (ENALIA) (40) their estimates showed that in general, water-soluble vitamin intakes were adequate but in the case of folate >50% of the participants older than 9 years had intakes below the specific sex-age estimated average requirement (EAR). Conversely, the degree of folate inadequacy in the children consuming adapted milk had a higher level of compliance with folates recommendations (93.3%) than those in the reference group, except from early ages (1 to <3 years), who had a high level of compliance with recommendations regardless of the type of milk consumed. Nevertheless, it is important to note that dietary folates intakes amongst infants have been previously assessed in Spain, but not specifically targeting the groups studied within the EsNuPI Study (1 to <10 years), and therefore comparison remains limited (39, 41). In addition, the difference could be related to the difference in the use of different methodologies. Nevertheless, data on dietary folate intake in school-age children at a European level show that there are large proportions of this population that do not meet folate recommendations. Indeed, it is striking that a recent review of nutrient intakes from national dietary surveys of 21 surveys in 18 countries in three regions: two of five Northern European countries (Denmark and Norway); 10 out of 17 Western European countries (Germany, Austria, Belgium, Spain, France, Ireland, Italy, the Netherlands, Portugal and the United Kingdom) and six out of 31 Central and Eastern European countries (Bulgaria, Cyprus, Slovenia, Estonia, Latvia and Turkey), the only age group over 3 years with an adequate total folate intake were Irish children aged 13–14 (42). It has earlier been found that an increase of 10% in folate intake from food could result in a 6% increase in serum folate (43). Therefore, nutritional policy-making bodies should consider the need for fortification of foods with folic acid (FA) targeted to this age segment, review the RDIs and formulate specific recommendations to ensure that school-aged children have adequate intake of this micronutrient. However, these strategies will require careful monitoring to ensure effectiveness. Since, Lewis et al. (44) reported that after fortification in the USA, 26% of this population exceeded the tolerable upper limit. Likewise, Pfeiffer et al. (45) estimated that 43% of children up to 5 years of age had an elevated serum folate concentration. Furthermore, in Spain, we have shown that excesses are a common practice in the fortification of FA in breakfast cereals and dairy products, since total folate values were clearly higher than those declared by manufacturers in most cases (18, 46).
This study found that the prevalence of adequacy for vitamin B12, among school-aged children in Spain, based on the European PRI was highly compliant by all population groups (>95% compliance), being only significantly higher in the adapted milk group (AMS) in children aged 1 to 3 years vs. the SRS group, which is consistent with findings from other national or international dietary surveys of children where vitamin B12 intakes have also met the recommended nutrient intakes (RNI) for vitamin B12 at school age (39, 41, 42). The high vitamin B12 adequacy noted in Spanish children may be explained by the dietary patterns followed by the Spanish population, which nowadays includes a high intake of animal products, increasingly distant from the traditional Mediterranean diet (47, 48).
Furthermore, a high proportion of this population group have adequate intakes of vitamin B6. This is consistent with previous Spanish study, which have showed mean intakes of 1.4 and 1.6 mg/day for vitamin B6 in males (2–5 years and 6–9 years, respectively) and female had intake for this vitamin of 1.3 and 1.5 mg/day (2–5 years and 6–9 years, respectively) (39). More recently, in the ANIBES study (41) the youngest age-groups evaluated were those 9–12 years, so only a limited comparison could be undertaken. In addition, 89.7% of children in the ANIBES met the European recommendations for vitamin B6 (49).
Comprehensive information on food sources is key for understanding the strengths/weaknesses as well as the quality of the diet of children from the Spanish population. The major contributors of vitamin B6 for children from our study were milk and dairy products, followed by fruits and meat and meat products. Also, it is noteworthy that the contribution of folates from milk and dairy products in the AMS was significantly higher than in the SRS. Indeed, although milk and dairy products are the main sources of macro-and micronutrients and contribute to the general quality of the diet in both children and adults (50–52), it appears that the infant formulas, follow-on milk formulas, or toddler’s milk formulas consumption may contribute more effectively to achieving the PRIs in the infant population. In addition, in the present study the AMS also showed milk and dairy products as the major B12 contributors but conversely, egg products were the second group as compared to the SRS were meat and meat products. In fact, it is worth remembering that restrictive diets such as vegetarian or vegan encompass a high risk of inadequate intake owing to the exclusion and/or limitation of foods of animal origin. Even more importantly in this stage of exponential growth and development, vitamin B12 deficiency amongst these key population groups has to be taken under consideration by public health authorities (53). It has been estimated that in Europe, the prevalence of vegetarian diets ranges from 1.2 to 1.5% of the population in Portugal and Spain, to about 7% in the United Kingdom and 10% in Germany, although the proportion of vegans is substantially lower (1–3%) all over Europe (54). No specific data are available for infants and children, nonetheless, it is acknowledged that vitamin B12 status can be compromised if supplementation is not provided for these children under a strictly vegans diets.
Our data can be compared with those acquired in other European studies in which the proportion of vitamin B12 and folates obtained from milk and dairy products was significant. For example, milk and dairy products were the major contributors to Greek school children aged 9–13 years (55). In the multi-ethnic population of the Head Start Mothers study (USA), high milk/low sweetened beverage intakes were associated with higher mean intakes of numerous vitamins and minerals, including folates and B6 (56). In Australian preschool children, one-carbon metabolism nutrients (methionine, folates, vitamins B2, B6, and B12) intake was also found highest from dairy products (57).
It is worth underlining and something worrisome that according to our results major folate sources, like vegetables and green-leaf as well as legumes are scarce. Indeed, for all age groups, milk and dairy products was the main folate contributor. Noteworthy the SRS had higher vegetable consumption that the AMS, specially at younger ages. However, in both groups fruit intake was similar.
Amongst the strengths of the EsNuPI study is the novelty of the analysis of a subpopulation representative of the Spanish children aged 1 to <10 years and likewise those who consume adapted milk formulas. The EsNuPI study involves a representative cohort of the Spanish children and an updated source of information on their dietary intakes and patterns and socioeconomic factors. In addition, the 24-h DR information was compiled following the methodology suggested by EFSA (The PAN CAKE-Pilot study) (58).
The study presents, however, several limitations: (1) potential errors in the reported information might have influenced the results of the study questionnaires; (2) children living in urban areas were studied; though, currently, 52.6% of the total Spanish population from 1 to <10 years old live in urban areas; (3) due to the study’s non-invasive design, we did not perform any vitamin analysis on plasma; and (4) this work queried about child’s supplement use [only 2.9% reported the consumption of any type of supplement, compared to the 7–25% reported for Spanish children (40)]. Supplements reported in the 24 h DR were included as part of the food group “cereal-based baby food and supplements.” A specific limitation of studying young children when compared to older ones is that they have limitations in remembering, estimating and cooperating in dietary assessment procedures, this is why caregivers became the main information providers (59). However, one has to consider the bias this might represent for example in school meals or the under or overreporting derived by parents in response to their own dietary beliefs. In fact, there is a tendency amongst parents to overestimate those foods considered healthy and underestimate the least healthy ones. However, as already stated, Madrigal et al. (24) performed an evaluation of misreporting for the EsNuPI study which showed that the exclusion of under or over reporters has no significant influence in children’s TEI, therefore they were included in the present study.
The results showed that higher compliance with folates recommendations was achieved by children consuming adapted milk products. Finally, across all population groups there was a high compliance with B12 and vitamin B6 PRI (>95%) based on the European recommendations, being significantly higher in the adapted milk group (AMS) in children aged 1–3 years vs. the SRS group for vitamin B12. Likewise, the prevalence of adequacy for vitamin B6 estimated by the EFSA criteria was significantly higher in AMS, independently of age. In conclusion, children would largely benefit from healthier dietary patterns increasing the consumption of milk and dairy products, since these may contribute significantly to these vitamin requirements of the infant population. Nevertheless, there is a great need to improve young children’s diet by including high folate sources that contribute to an adequate intake of this vitamin.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by University of Granada Ethical Committee (No. 659/CEIH/2018), and registered in ClinicalTrials.gov (Unique Protocol ID: FF01/2019). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
GV-M and ÁG: funding acquisition, project administration, and supervision. PR-A, MS-M, ÁH-R, GV-M, and ÁG: investigation. MS-V, TP, ÁG, and GV-M: methodology. TP and MS-V: writing—original draft. TP, MS-V, PR-A, MS-M, ÁH-R, ÁG, and GV-M: writing—review and editing. All authors have read and agreed to the published version of the manuscript.
This research was funded by Instituto Puleva de Nutrición (IPN) under an agreement with Spanish Nutrition Foundation (FEN) and Iberoamerican Nutrition Foundation (FINUT). The IPN is a non-profit entity that promotes scientific research mainly in the field of nutrition and health: child nutrition, cardiovascular, bone and digestive health, etc., as well as the dissemination of quality scientific content. While the IPN is funded by the dairy company Lactalis, its actions are based on the decisions of an independent scientific board formed by renowned international scientists. The founder has not taken any decision about the results and the publications obtained from this study.
The authors are grateful to José Manuel Ávila, Aitor Trabanco Llano, and Emma Ruiz for technical support and advice.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor JMH declared a shared affiliation with the author AG at the time of review.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. MRC. Prevention of neural tube defects: results of the Medical Research Council vitamin study. Lancet. (1991) 338:131–7.
2. Czeizel, AE, and Dudas, I. Prevention of the first occurrence of neural-tube defects by periconceptional vitamin supplementation. N Engl J Med. (1992) 327:1832–5.
3. Czeizel, AE, Dudás, I, Vereczkey, A, and Bánhidy, F. Folate deficiency and folic acid supplementation: the prevention of neural-tube defects and congenital heart defects. Nutrients. (2013) 5:4760–75. doi: 10.3390/nu5114760
4. Troen, AM, Chao, WH, Crivello, NA, D’Anci, KE, Shukitt-Hale, B, Smith, DE, et al. Cognitive impairment in folate-deficient rats corresponds to depleted brain phosphatidylcholine and is prevented by dietary methionine without lowering plasma homocysteine. J Nutr. (2008) 138:2502–9. doi: 10.3945/jn.108.093641
5. Freitas-Costa, NC, Andrade, PG, Normando, P, Nunes, KSS, Raymundo, CE, Castro, IRR, et al. Association of development quotient with nutritional status of vitamins B6, B12, and folate in 6–59-month-old children: results from the Brazilian National Survey on child nutrition (ENANI-2019). Am J Clin Nutr. (2023) 118:162–73. doi: 10.1016/j.ajcnut.2023.04.026
6. Partearroyo, T, Vallecillo, N, Pajares, MA, Varela-Moreiras, G, and Varela-Nieto, I. Cochlear homocysteine metabolism at the crossroad of nutrition and sensorineural hearing loss. Front Mol Neurosci. (2017) 10:107. doi: 10.3389/fnmol.2017.00107
7. Rush, J, Moritz, A, Lee, KA, Guo, A, Goss, VL, Spek, EJ, et al. Immunoaffinity profiling of tyrosine phosphorylation in cancer cells. Nat Biotechnol. (2005) 23:94–101. doi: 10.1038/nbt1046
8. Black, MM. Effects of vitamin B12 and folate deficiency on brain development in children. Food Nutr Bull. (2008) 29:S126–31. doi: 10.1177/15648265080292S117
9. Schwarzenberg, SJ, Georgieff, MK, COMMITTEE ON NUTRITION, Daniels, S, Corkins, M, Golden, NH, et al. Advocacy for improving nutrition in the first 1000 days to support childhood development and adult health. Pediatrics. (2018) 141:e20173716. doi: 10.1542/peds.2017-3716
10. Blakley, R. The biochemistry of folic acid and related pteridines. North-Holland Research Monographs Frontiers of Biology Vol. 13. Amsterdam: North-Holland Publishing Company (1969).
11. IOM, Panel on Folate, other B vitamins and Choline. Dietary reference intakes for thiamin, riboflavin, niacin, vitamin B6, folate, vitamin B12, pantothenic acid, biotin, and choline. National Academy of Sciences. Institute of Medicine. Food and Nutrition Board. Washington, D.C.: National Academy Press (1998).
12. Samaniego-Vaesken, ML, Alonso-Aperte, E, and Varela-Moreiras, G. Vitamin food fortification today. Food Nutr Res. (2012) 56:5459. doi: 10.3402/fnr.v56i0.5459
13. Mayengbam, S, Raposo, S, Aliani, M, and House, JD. A vitamin B-6 antagonist from flaxseed perturbs amino acid metabolism in moderately vitamin B-6–deficient male rats. J Nutr. (2016) 146:14–20. doi: 10.3945/jn.115.219378
14. Shibata, K, Yasuhara, Y, and Yasuda, K. Effects of cooking methods on the retention of vitamin B6 in foods, and the approximate cooking loss in daily meals. J Home Econ Jpn. (2001) 52:1187–97.
15. Wills, L. Treatment of «pernicious anaemia of pregnancy» and «tropical anaemia» with special reference to yeast extract as a curative agent. BMJ. (1931) 7:323-7; discussion 328
16. Vilter, RW, Horrigan, D, Mueller, JF, Jarrold, T, Vilter, CF, Hawkins, V, et al. Studies on the relationships of vitamin b12, folic acid, thymine, uracil, and methyl group donors in persons with pernicious anemia and related megaloblastic anemias. Blood. (1950) 5:695–717. doi: 10.1182/blood.V5.8.695.695
17. Kim, YI. Folate: a magic bullet or a double edged sword for colorectal cancer prevention? Gut. (2006) 55:1387–9. doi: 10.1136/gut.2006.095463
18. Samaniego-Vaesken, ML, Alonso-Aperte, E, and Varela-Moreiras, G. Voluntary folic acid fortification levels and nutrient composition of food products from the Spanish market: a 2011-2015 update. Nutrients. (2017) 9:234. doi: 10.3390/nu9030234
19. Egan, E, Kelly, F, and Sweeney, MR. Voluntary folic acid fortification levels of food staples in Ireland continue to decline: further implications for passive folic acid intakes? J Public Health. (2019). 43:281–286. doi: 10.1093/pubmed/fdz125
20. Madrigal, C, Soto-Méndez, MJ, Hernández-Ruiz, Á, Ruiz, E, Valero, T, Ávila, JM, et al. Dietary and lifestyle patterns in the Spanish pediatric population (one to <10 years old): design, protocol, and methodology of the EsNuPI study. Nutrients. (2019) 11:3050. doi: 10.3390/nu11123050
21. Homocysteine Lowering Trialists’ Collaboration. Lowering blood homocysteine with folic acid based supplements: meta-analysis of randomised trials. BMJ. (1998) 316:894–8.
22. Goldberg, GR, Black, AE, Jebb, SA, Cole, TJ, Murgatroyd, PR, Coward, WA, et al. Critical evaluation of energy intake data using fundamental principles of energy physiology: 1. Derivation of cut-off limits to identify under-recording. Eur J Clin Nutr. (1991) 45:569–81.
23. Black, AE. Critical evaluation of energy intake using the Goldberg cut-off for energy intake:basal metabolic rate. A practical guide to its calculation, use and limitations. Int J Obes. (2000) 24:1119–30. doi: 10.1038/sj.ijo.0801376
24. Madrigal, C, Soto-Méndez, MJ, Hernández-Ruiz, Á, Valero, T, Ávila, JM, Ruiz, E, et al. Energy intake, macronutrient profile and food sources of Spanish children aged one to <10 years—results from the EsNuPI study †. Nutrients. (2020) 12:893. doi: 10.3390/nu12040893
25. Fundación Española de la Nutrición (FEN), Tablas de Medidas Caseras y Raciones Habituales de Consumo. (2013). Fundación Española de la Nutrición (FEN): Madrid, Spain.
26. López, R, Martínez de Victoria, E, and Gil, A, Guía Fotográfica de Porciones de Alimentos Consumidos en España. (2019). Fundación Iberoamericana de Nutrición; Universidad de Granada: Granada, Spain
27. European Food Safety Authority. Dietary reference values for nutrients summary report. EFSA Supporting Publications. (2017) 14:e15121E. doi: 10.2903/sp.efsa.2017.e15121
28. Plaza-Díaz, J, Molina-Montes, E, Soto-Méndez, MJ, Madrigal, C, Hernández-Ruiz, Á, Valero, T, et al. Clustering of dietary patterns and lifestyles among Spanish children in the EsNuPI study †. Nutrients. (2020) 12:2536. doi: 10.3390/nu12092536
29. Bellisle, F. Effects of diet on behaviour and cognition in children. Br J Nutr. (2004) 92:S227–32. doi: 10.1079/bjn20041171
30. Caffrey, A, Lamers, Y, Murphy, MM, Letourneau, N, Irwin, RE, Pentieva, K, et al. Epigenetic effects of folate and related B vitamins on brain health throughout life: scientific substantiation and translation of the evidence for health improvement strategies. Nutr Bull. (2023) 48:267–77. doi: 10.1111/nbu.12611
31. Yehuda, S, Rabinovitz, S, and Mostofsky, D. Nutritional deficiencies in learning and cognition. J Pediatr Gastroenterol Nutr. (2006):S22–5. doi: 10.1097/01.mpg.0000255847.77034.a4
32. Gómez-Pinilla, F. Brain foods: the effects of nutrients on brain function. Nat Rev Neurosci. (2008) 9:568–78. doi: 10.1038/nrn2421
33. Molloy, AM, Kirke, PN, Brody, LC, Scott, JM, and Mills, JL. Effects of folate and vitamin B12Deficiencies during pregnancy on fetal, infant, and child development. Food Nutr Bull. (2008) 29:S101–11. doi: 10.1177/15648265080292S114
34. Rasmussen, SA, Fernhoff, PM, and Scanlon, KS. Vitamin B12 deficiency in children and adolescents. J Pediatr. (2001) 138:10–7. doi: 10.1067/mpd.2001.112160
35. Obeid, R, Murphy, M, Solé-Navais, P, and Yajnik, C. Cobalamin status from pregnancy to early childhood: lessons from global experience. Adv Nutr. (2017) 8:971–9. doi: 10.3945/an.117.015628
36. Jensen, CF. Vitamin B12 levels in children and adolescents on plant-based diets: a systematic review and meta-analysis. Nutr Rev. (2022). 81:951–966. doi: 10.1093/nutrit/nuac096
37. Robinson, S, and Fall, C. Infant nutrition and later health: a review of current evidence. Nutrients. (2012) 4:859–74. doi: 10.3390/nu4080859
38. EFSA Panel on Dietetic Products, N. and Allergies. Scientific opinion on nutrient requirements and dietary intakes of infants and young children in the European Union. EFSA J. (2013) 11:3408. doi: 10.2903/j.efsa.2013.3408
39. Serra-Majem, L, Ribas-Barba, L, Pérez-Rodrigo, C, and Bartrina, JA. Nutrient adequacy in Spanish children and adolescents. Br J Nutr. (2006) 96:S49–57. doi: 10.1079/BJN20061701
40. López-Sobaler, AM, Aparicio, A, González-Rodríguez, L, Cuadrado-Soto, E, Rubio, J, Marcos, V, et al. Adequacy of usual vitamin and mineral intake in Spanish children and adolescents: ENALIA study. Nutrients. (2017) 9:131. doi: 10.3390/nu9020131
41. Partearroyo, T, Samaniego-Vaesken, ML, Ruiz, E, Olza, J, Aranceta-Bartrina, J, Gil, Á, et al. Dietary sources and intakes of folates and vitamin B12 in the Spanish population: findings from the ANIBES study. PLoS One. (2017) 12:e0189230. doi: 10.1371/journal.pone.0189230
42. Rippin, HL, Hutchinson, J, Jewell, J, Breda, JJ, and Cade, JE. Child and adolescent nutrient intakes from current national dietary surveys of European populations. Nutr Res Rev. (2019) 32:38–69. doi: 10.1017/S0954422418000161
43. Marchetta, CM, Devine, O, Crider, K, Tsang, B, Cordero, A, Qi, Y, et al. Assessing the association between natural food folate intake and blood folate concentrations: a systematic review and Bayesian meta-analysis of trials and observational studies. Nutrients. (2015) 7:2663–86. doi: 10.3390/nu7042663
44. Lewis, CJ, Crane, NT, Wilson, DB, and Yetley, EA. Estimated folate intakes: data updated to reflect food fortification, increased bioavailability, and dietary supplement use. Am J Clin Nutr. (1999) 70:198–207. doi: 10.1093/ajcn.70.2.198
45. Pfeiffer, CM, Caudill, SP, Gunter, EW, Osterloh, J, and Sampson, EJ. Biochemical indicators of B vitamin status in the US population after folic acid fortification: results from the National Health and nutrition examination survey 1999-2000. Am J Clin Nutr. (2005) 82:442–50. doi: 10.1093/ajcn/82.2.442
46. Samaniego-Vaesken, ML, Alonso-Aperte, E, and Varela-Moreiras, G. Voluntary fortification with folic acid in Spain: an updated food composition database. Food Chem. (2016) 193:148–53. doi: 10.1016/j.foodchem.2014.06.046
47. Partearroyo, T, Laja García, AI, and Varela-Moreiras, G. Strengths and weaknesses of food and diet in the Spanish population of the 21st century. Nutr Hosp. (2019) 36:3–6. doi: 10.20960/nh.02685
48. Partearroyo, T, Samaniego-Vaesken, ML, Ruiz, E, Aranceta-Bartrina, J, Gil, Á, González-Gross, M, et al. Current food consumption amongst the Spanish ANIBES study population. Nutrients. (2019) 11:2663. doi: 10.3390/nu11112663
49. Mielgo-Ayuso, J, Aparicio-Ugarriza, R, Olza, J, Aranceta-Bartrina, J, Gil, Á, Ortega, R, et al. Dietary intake and food sources of niacin, riboflavin, thiamin and vitamin B6 in a representative sample of the Spanish population. The ANIBES study. Nutrients. (2018) 10:846. doi: 10.3390/nu10070846
50. Cifelli, CJ, Auestad, N, and Fulgoni, VL. Replacing the nutrients in dairy foods with non-dairy foods will increase cost, energy intake and require large amounts of food: National Health and nutrition examination survey 2011–2014. Public Health Nutr. (2022) 25:332–43. doi: 10.1017/S1368980020001937
51. O’Neil, CE, Nicklas, TA, and Fulgoni, VL III. Food sources of energy and nutrients of public health concern and nutrients to limit with a focus on milk and other dairy foods in children 2 to 18 years of age: National Health and nutrition examination survey, 2011–2014. Nutrients. (2018) 10:1050. doi: 10.3390/nu10081050
52. Fulgoni, VL III, Keast, DR, Auestad, N, and Quann, EE. Nutrients from dairy foods are difficult to replace in diets of Americans: food pattern modeling and an analyses of the National Health and nutrition examination survey 2003-2006. Nutr Res. (2011) 31:759–65. doi: 10.1016/j.nutres.2011.09.017
53. Kiely, ME. Risks and benefits of vegan and vegetarian diets in children. Proc Nutr Soc. (2021) 80:159–64. doi: 10.1017/S002966512100001X
54. Redecillas-Ferreiro, S, Moráis-López, A, and Manuel Moreno-Villares, J. Position paper on vegetarian diets in infants and children. Committee on nutrition and breastfeeding of the Spanish Paediatric association. Anales de Pediatría. (2020) 92:306.e1–6. doi: 10.1016/j.anpedi.2019.10.013
55. Manios, Y, Moschonis, G, Dekkers, R, Mavrogianni, C, Grammatikaki, E, and van den Heuvel, E. Vitamin B2, vitamin B12 and total homocysteine status in children and their associations with dietary intake of B-vitamins from different food groups: the healthy growth study. Eur J Nutr. (2017) 56:321–31. doi: 10.1007/s00394-015-1082-z
56. O'Neil, CE, Nicklas, TA, Liu, Y, and Franklin, FA. Impact of dairy and sweetened beverage consumption on diet and weight of a multiethnic population of head start mothers. J Am Diet Assoc. (2009) 109:874–82. doi: 10.1016/j.jada.2009.02.012
57. Taylor, RM, Smith, R, Collins, CE, Evans, TJ, and Hure, AJ. Dietary intake and food sources of one-carbon metabolism nutrients in preschool aged children. Eur J Clin Nutr. (2019) 73:1179–93. doi: 10.1038/s41430-018-0376-7
58. Ocké, M, de Boer, E, Brants, H, van der Laan, J, Niekerk, M, van Rossum, C, et al. PANCAKE–pilot study for the assessment of nutrient intake and food consumption among kids in Europe. EFSA Supporting Publications. (2012) 9:339E. doi: 10.2903/sp.efsa.2012.EN-339
Keywords: folates, B12, B6, pediatrics, Spanish children, dietary habits, nutrition assessment, pediatric nutrition
Citation: Partearroyo T, Samaniego-Vaesken MdL, Rodríguez-Alonso P, Soto-Méndez MJ, Hernández-Ruiz Á, Gil Á and Varela-Moreiras G (2023) Dietary intake, nutritional adequacy and food sources of vitamins involved in the methionine-methylation cycle from Spanish children aged one to <10 years: results from the EsNuPI study. Front. Nutr. 10:1248908. doi: 10.3389/fnut.2023.1248908
Edited by:
José María Huerta, Carlos III Health Institute (ISCIII), SpainReviewed by:
Emmanuel Biracyaza, Université de Montréal, CanadaCopyright © 2023 Partearroyo, Samaniego-Vaesken, Rodríguez-Alonso, Soto-Méndez, Hernández-Ruiz, Gil and Varela-Moreiras. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Teresa Partearroyo, dC5wYXJ0ZWFycm95b0BjZXUuZXM=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.