
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Nutr. , 27 September 2022
Sec. Clinical Nutrition
Volume 9 - 2022 | https://doi.org/10.3389/fnut.2022.994607
This article is part of the Research Topic Contribution of the Maternal Microbiome to Offspring Health View all 5 articles
 Shiang Yen Eow1
Shiang Yen Eow1 Wan Ying Gan1*
Wan Ying Gan1* Tiemin Jiang2,3
Tiemin Jiang2,3 Su Peng Loh1
Su Peng Loh1 Ling Jun Lee1
Ling Jun Lee1 Yit Siew Chin1,4
Yit Siew Chin1,4 Leslie Thian Lung Than5
Leslie Thian Lung Than5 Kang Nien How6
Kang Nien How6 Pui Ling Thong7
Pui Ling Thong7 Yanpin Liu2,8
Yanpin Liu2,8 Junying Zhao2,8
Junying Zhao2,8 Lijun Chen2,8*
Lijun Chen2,8*Background: The microbiota plays a key role in early immunity maturation that affects infant health and is associated with the development of non-communicable diseases and allergies in later life.
Objective: The MYBIOTA is a prospective mother-infant cohort study in Malaysia aiming to determine the association between gut microbiota with infant health (temperament, gastrointestinal disorders, eczema, asthma, and developmental delays) in Selangor, Malaysia.
Methods: Pregnant mothers will be enrolled in their first trimester of pregnancy, and follow-ups will be done for infants during their first year of life. Maternal-infant biological samples (blood, feces, saliva, urine, and breast milk), anthropometric, dietary, and clinical information will be collected at different time points from early pregnancy to 12 months postpartum.
Discussion: This study could provide a better understanding of the colonization and development of the gut microbiome during early life and its impact on infant health.
Clinical trial registration: https://clinicaltrials.gov/, identifier NCT04919265.
Gut microbiota plays a critical role in children's developmental pathways, especially in the first 1,000 days of life, due to the interplay between the establishment of the risks for diseases over infants' life course and infant health (1–3). Infant gut microbiota develops after birth, but the initial bacterial colonization occurs as early as when the fetus is still in the lower uterus (1). However, microbial diversity and colonization patterns vary at different time points and among infants (1, 4). More than 95% of the microbiota composition in the infant's intestinal area could be categorized into four major phyla: Firmicutes, Bacteroidetes, Actinobacteria, and Protecteobacteria (1). Two major transitions take place in the gut microbiota during infancy. The first transition characterizes the dominance of Bifidobacterium right after birth and during lactation, followed by the dominance of Bacteroidetes and Firmicutes during the weaning period, the introduction of solids foods, and continued breastfeeding practices, marking the second transition (4, 5).
Recently, increasing evidence have shown the impacts of pre-natal maternal factors on infant gut microbiota through the transmission of metabolic diseases passed from mother to child. The maternal factors are primarily associated with physical health before and during pregnancy as indicated by high pre-pregnancy body mass index (BMI) (6–8), unhealthy weight gain (6, 8), maternal exposure to medications (7–10), and gestational diabetes mellitus (GDM) (7, 8, 11). Furthermore, environmental factors involving maternal diet, including high-fat diet (7, 8, 12), smoking (10, 13), and food insecurity (14) during pregnancy are linked to the changes in infant gut microbiota. The variations in infant gut microbiota due to diet diversity among Malaysian pregnant women of different ethnic groups and the differences between Western and Eastern diets are worth investigating. Additionally, previous studies have shown that breast milk composition (4, 10, 15, 16) and maternal gut microbiota (7, 10) are linked to infant gut microbiota. Nevertheless, the composition of breast milk and gut microbiota of Malaysian women and their effects on infant gut microbiota remains unknown.
Recent discoveries have highlighted how the psychological factors of mothers, including depressive symptoms and stress, would alter gene expressions related to maternal gut homeostasis, subsequently affecting the fetal gut development and oral microbiome (17–19). However, the effects of maternal prenatal psychological factors and infant gut microbiota and immunity remain unclear. Additionally, literature on the association between maternal physical activity level and infant gut microbiota were limited to animal studies (20, 21), hence the requirement to substantiate this association via human studies. An extensive investigation is necessary to determine the influence of maternal pre-natal factors on infants' gut microbiome composition and diversity.
Besides pre-natal factors, accumulating studies have shown that several post-natal factors are associated with the alteration in diversity and abundance of gut microbiota in infants, including gender (22), birth order (4, 10), gestational age (4, 23), delivery mode (4, 22, 24), home settings (25), and pet rearing (24, 26, 27). Meanwhile, inconsistencies were found in associating infant growth (weight, length, and head circumference) with gut microbiota (28). Furthermore, infant feeding patterns (4, 10, 15, 22), dietary intake and diversity (29, 30) were reported as major determinants of the composition and alpha diversity of infant gut microbiota in western countries. However, despite the importance of identifying these factors, no such investigations have been conducted among Malaysian infants. Therefore, studies on infants' diets are essential due to the different dietary intake of Malaysian infants compared to those in western studies. In general, understanding the connection between pre-natal factors, post-natal factors, maternal gut microbiota, and infant gut microbiota is essential for infant health improvement and disease prevention into adulthood.
Recent studies have shown that gut microbiota is associated with temperament (31–33) and risks of gastrointestinal disorders (2, 34), eczema (35), asthma (36), and developmental delays in infants (37, 38). Temperament is a biologically-based individual differences in behavior in the form of activity, affectivity, and self-regulation, which is often used to assess a child's behaviors in early life (39). Gut microbiota influence on temperament traits warrants further inspection due to the rapid neurodevelopment at infancy (31). Thus, the current study aims to holistically understand the connection between behavior and the microbiota-gut-brain axis by studying temperament as a psychosocial variable. Furthermore, alterations in the composition and stability of infant gut microbiota lead to the development of acute and chronic gastrointestinal disorders (34). A local study showed that the prevalence of functional gastrointestinal disorders (FGIDs) among infants, including regurgitation, colic, rumination syndrome, dyschezia, functional constipation, and diarrhea, were 10.5, 1.9, 1,7, 1.3, 1.1, and 0.3%, respectively (40). Children with FGIDs were reported to have a lower quality of life, a high number of doctor visits and hospitalizations, and increased vulnerability of developing a more severe form of FGIDs and pain-related conditions in the future (41). Therefore, more research is needed to understand the association of gut microbiota and gastrointestinal disorders in infants.
Studies have shown a rapid and high diversification of gut microbiota over the first year of life in healthy children, but this is not the case for children with allergy, asthma (42, 43) and malnutrition (44). The prevalence of eczema and wheezing among Malaysian infants was 27.6 and 6.1%, respectively (45), in which the problems could be attributed to the disruption of intestinal microbiota in early life (35, 36). Besides, early life gut microbiota has been shown to be associated with the risk factor of childhood obesity, including infant's appetite traits (46). Infants who have a high abundance of the phylum Firmicutes in their gut microbiota was correlated with lower food responsiveness (46). Additionally, another study elucidated that the phylum Firmicutes was found to be abundant in the gut microbiota of obese children (47). An altered and immature gut microbiota could lead to malnutrition due to impaired energy production, vitamin biosynthesis, and immune protection (48, 49). Thus, early life intervention on immature and unstable gut microbiota is necessary to prevent the worsening of eczema, asthma symptoms, and obesity as infants grow.
Emerging evidence shows that disruption in the development of the gastrointestinal tract during the early post-natal period can affect brain development (37, 50). Impairments of developmental features relative to the child's age often refer as developmental delays (38). Poor performance on developmental domains, such as neurocognitive during childhood may affect health outcomes later in life, including poorer emotional awareness and educational attainment in later adulthood (51). The first year of life in humans is a critical period of rapid gut colonization and brain growth, but little is known about this relationship (38). Therefore, establishing a healthy gut microbiota among infants is essential to ensure optimal growth and development as well as a good quality of life.
Research on gut microbiota and the key determinants of microbial variation among Southeast Asian children remains lacking (52). Specifically, the Malaysian Working Group on Gastrointestinal Health reported a lack of research and awareness on the role of gut microbiota in early life (53). Increased awareness on the importance of gut health will help establish pre-natal and post-natal factors that promote healthy development and functioning of the immune system, gastrointestinal health, and metabolism in infants. In Malaysia, previous studies on gut microbiota mainly focused on pre-adolescent (52, 54) and pre-school children (55). While there are few local mother-infant cohort studies (45, 56, 57), none observed changes in infant gut microbiota over time.
Overall, it is essential to understand the host-microbe interactions in the first year of life since this period is crucial for infant health programming and may influence infant development with short- and long-term health consequences (1–3). The lack of evidence, especially from the Southeast Asia, calls for further studies to understand how gut microbiota in early life affects disease development (allergy, eczema, metabolic disease, and gastrointestinal disease) into adulthood. Since there is a lack of longitudinal research on infant gut microbiota in Malaysia, this cohort study aims to determine the association between gut microbiota with infant health (temperament, gastrointestinal disorders, eczema, asthma, and developmental delays) during the first year of life at different follow-ups. The specific objectives include:
1. To assess infant gut microbiota (composition, taxonomy, diversity, and abundance) during the first year of life.
2. To assess temperament, gastrointestinal disorders, eczema (presence and severity), asthma (likelihood of developing), and developmental delays of infants.
3. To determine the associations between socio-demographic, pre-natal and post-natal factors with gut microbiota in infants at 12 months.
4. To determine the associations between infant gut microbiota and infant health (temperament, gastrointestinal disorders, eczema, asthma, and developmental delays) at 12 months.
The MYBIOTA is a prospective cohort study involving pregnant women in the first trimester (gestational age: 8–12 weeks) and their infants up to 12 months in Selangor, Malaysia. The Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) guideline (58) was used as a reference to develop this study protocol.
The sample size required for this cohort study is 225 mother-infant pairs, considering the effect size of 0.427 (59), confidence level of 95%, power of 80% and attrition rate of 29.0% (45). First, the list of private hospitals in Selangor will be obtained from the Ministry of Health. Next, eight private hospitals will be randomly selected using a computerized random number generator with an estimated participation of 30 eligible pregnant women per hospital in a month. Pregnant women aged between 18 and 45 years old in their first trimester of pregnancy who visit the selected private hospitals and plan to attend post-natal check-ups for at least 1 year in the study area will be recruited. Meanwhile, pregnant women diagnosed with immune deficiency, severe allergic conditions, psychiatric disorders, multiple pregnancies, preterm delivery (<37 weeks), a newborn with congenital abnormalities, and hospitalized in neonatal intensive care unit immediately after birth will be excluded from this study.
Data collection will be conducted from June 2022 to December 2024. Once the recruitment of participants begins, pregnant mothers in their first trimester will be given an information sheet explaining the purpose of the study, and those who agree to join the study are required to provide written informed consent. Data will be collected from the eligible pregnant women during their first trimester (8–12 weeks), second trimester (24 weeks), third trimester (34 weeks) and follow-up infants and mothers post-natally after birth (1–5 days after delivery), at 10–15 days, 1 month, 4 months, 6 months and 12 months of age with a total of nine follow-ups to collect mother-infant biological samples and other relevant information for the research. Types of data and samples to be collected from mothers and infants at each time point are summarized in Figure 1.
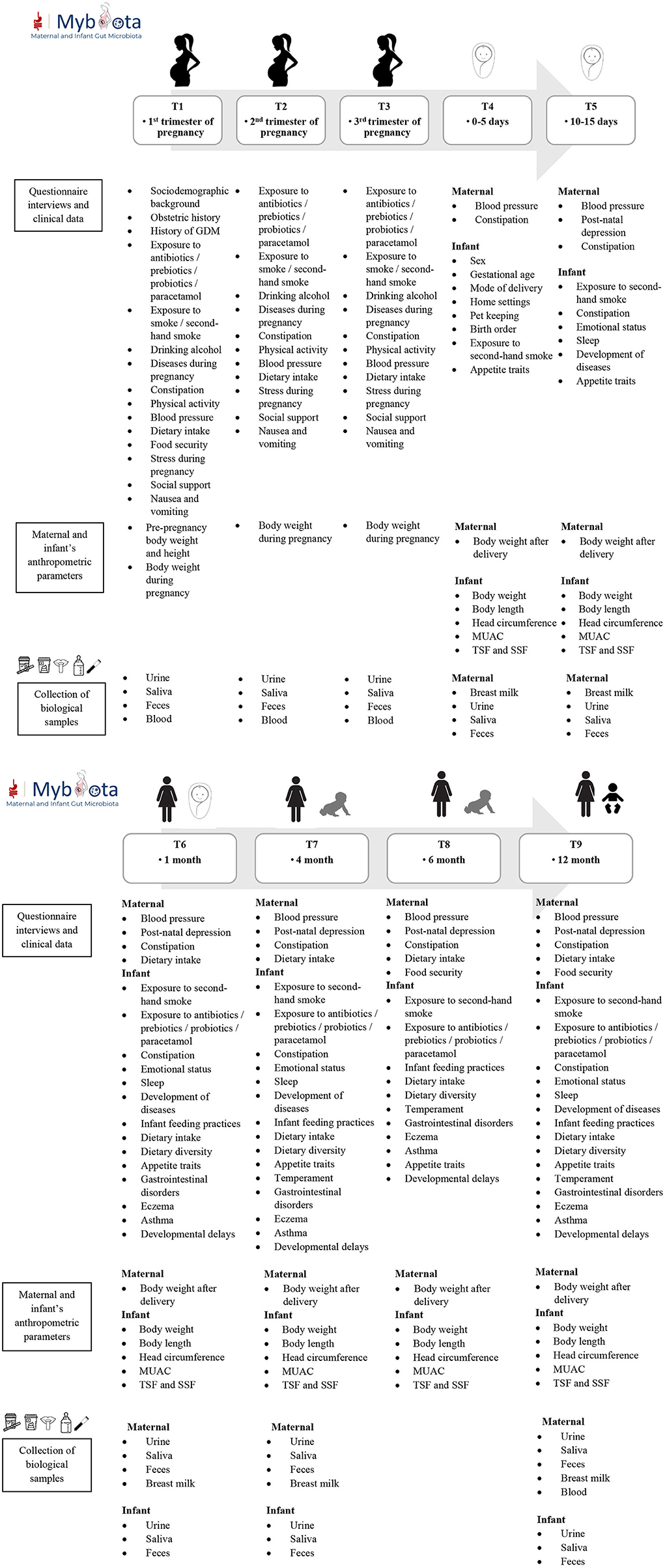
Figure 1. Data collection time points and sample collections of mothers and infants.
Maternal pre-and post-pregnancy body weight, current weight, and height will be extracted from the medical records to determine pre-and post-pregnancy BMI and gestational weight gain. Meanwhile, the infant's birth weight, current weight, length and head circumference at birth will be obtained from the child health record book. In addition, infants will be measured by researchers for their mid-upper arm circumference (MUAC), triceps skinfold (TSF) and subscapular skinfold (SSF) at 1, 4, 6, and 12 months by using a Lufkin Executive Diameter steel tape model W606PM (Cooper Hand Tools, Raleigh, North Carolina, USA) and Harpenden skinfold caliper (British Indicators Limited), respectively.
A venous blood sample (6 ml) will be collected from the pregnant mothers during their routine antenatal check-ups in their first, second, and third trimester and 12 months after delivery by a certified phlebotomist. The blood will be analyzed for serum 25(OH) D level (45), iron, lipid, and metabolome profiles (60, 61) of the mothers. About 100 mg of blood sample will be mixed with 0.6 mL of 2-chlorophenylalanine-methanol solution in a 2 mL EP tube for vortex of 30 s, and then will be grinded, treated with ultrasonic, and centrifuged. Supernatant samples will be filtrated and detected with LC-MS (60). Breast milk samples are self-collected by mothers (62) at 1–5 days, 10–15 days, 1 month, 4 months, and 12 months after delivery. Human milk glycerides, phospholipids, and sphingolipids will be profiled using ultra-performance liquid chromatography/quadrupole-time-of-flight mass spectrometry [UPLC/Q-TOF-MS with electrospray ionization source (ESI)] (63). Meanwhile, the human milk oligosaccharides (HMO) will be quantified using ultra-high-pressure liquid chromatography (UHPLC) with fluorescence detection (64). Next, the membrane protein of milk fat globules will be analyzed with the high-pressure liquid chromatography Q-Exactive mass spectrometry (HPLC-QE MS) (65). Next, the immune parameters and cytokine profiles from human milk will be determined using the Luminex-approach and ELISA kits. Finally, the fatty acids composition analysis will be conducted using transmethylation techniques, capillary gas chromatography, and flame ionization (66).
Pregnant mothers will be interviewed upon recruitment using a pre-tested questionnaire. The information that will be collected includes socio-demographic data (parents' age, ethnicity, educational background, occupation, monthly household income, and marital status), obstetric history (gravida, parity, and smoking during pregnancy), and exposures (antibiotics, prebiotics, probiotics, paracetamol, and family history of diseases, exposure to smoke or second-hand smoke, alcohol consumption, constipation, emotional status, sleep, and disease development). Additionally, their prenatal blood pressure will be retrieved from the medical records.
Mothers will be interviewed about their dietary intake using a 24-h dietary recall at the first, second, and third trimester, and each visit at 1, 4, 6, and 12 months after birth. The dietary data will be analyzed using NutritionistProTM software (Axxya Systems, Redmond, Washington, USA) for energy and nutrients based on the Malaysian Food Composition Database (67) and the ASEAN Food Composition Database (68). Energy and nutrient adequacies are determined based on the Recommended Nutrient Intake (RNI) for Malaysians (69). Furthermore, mothers are interviewed for their infant's dietary intake using a 24-h dietary recall at 1, 4, 6, and 12 months. Infant feeding practices will also be assessed at one, four, six, and 12 months (70). The dietary diversity score will be calculated based on the infant and young child feeding (IYCF) criteria, which includes the intake of seven food groups (grains, roots and tubers, legumes and nuts, dairy products, flesh foods, eggs, vitamin A-rich fruits and vegetables, and other fruits and vegetables) (71).
A set of validated questionnaires will be used to collect information at different time points as the following:
• Physical activity: Pregnancy Physical Activity Questionnaire (PPAQ) (72);
• Food security: Six-item U.S Department of Agriculture (USDA) Food Security Survey Module (FSSM) (73);
• Stress during pregnancy: Perceived Stress Scale (PSS)-10 (74);
• Depression: Edinburgh Postnatal Depression Scale (EPDS) (75);
• Gastrointestinal disorders of infants: Rome IV Diagnostic Questionnaire for Pediatric Functional Gastrointestinal Disorders-Toddler (R4PDQ-Toddler) (76);
• Infant temperament: Revised Infant Behavior Questionnaire (IBQ-R) (77);
• Presence of eczema in infants: five questions of the UK Working Party's Diagnostic Criteria for Atopic Dermatitis (78);
• Severity of eczema symptoms in infants: Patient-Oriented Eczema Measure (POEM) for children (79);
• Asthma symptoms in infants: Asthma Predictive Index (API) (80);
• Appetite traits: Baby Eating Behavior Questionnaire (BEBQ) (0–5 days, 10–15 days and 1 month) (81) and Children Eating Behavior Questionnaire (CEBQ) (4, 6, and 12 months) (82);
• Developmental delays: Ages and Stages Questionnaire, third edition (ASQ-3) (83).
Saliva, urine, and feces self-collection kits will be given to mothers at each visit. Saliva sample will be collected using an oral salivary swab. Mothers are required to remove the swab from Salivette® (Sarstedt, Nümbrecht, Germany) tube and gently roll her and her infant's mouth for 60 s before placing the swab into the salivette tube, per the manufacturer's instructions (65). Urine samples will be collected for metabolomic analysis using a urine collection container with boric acid as the preservative. Fresh feces from mothers and infants will be self-collected into a 5 mL feces collection tube (Sarstedt, Nümbrecht, Germany) with 2 mL of ribonucleic acid (RNA) (65). After collection of the feces sample, the cap of the feces tube will then be closed tightly followed by the shaking of tube for several times. A pad is placed in the diaper and used to collect unsoiled urine and fecal samples from the infant (65).
Mothers will be given a reminder via text and a tutorial video about the timing and methods of self-collection and storage of samples. They are required to notify the researchers once the self-collection and storage are done for transportation arrangements to the laboratory. All biological samples collected will be stored immediately inside a portable insulated container with ice packs at −20 °C and transported within 24-h of collection to the nutrition laboratory at Universiti Putra Malaysia for storage at −80 °C until further analysis. Once all the samples are prepared, aliquots labeled with the specific study ID number without personal information will be air freighted on dry ice and shipped to the National Engineering Center of Dairy for Maternal and Child Health, Beijing, China for further analysis.
The saliva, urine, and fecal samples collected will be analyzed to examine microbiota diversity, richness, and taxonomic composition (65). First, the genomic DNA will be extracted from homogenized fecal samples using the QIAamp Fast DNA Stool Mini Kit (Qiagen, GmbH, Hilden, Germany), following the manufacturer's instruction (65). Then, the polymerase chain reaction (PCR) amplification of the V3-V4 region of 16S rRNA genes with primers Bakt_341F(CCTACGGGNGGCWGCAG) and Bakt_805R (GACTACHVGGGTATCTAATCC) (84) will be performed as the following protocol: 3 min at 95 °C, 25 cycles of 30 s at 95 °C, 30 s at 55 °C, and 30 s at 72 °C (65). Taq DNA polymerase used is the Phusion® High-Fidelity DNA polymerase (M0530S, New England Biolabs, USA). Sequencing libraries will be generated using NEBNext® Ultra DNA Library Prep Kit for Illumina (New England Biolabs, USA). Amplicons will be sequenced using 2 × 250 base pair (bp) paired-end protocol by Illumina HiSeq 2500. USEARCH (version 1.9) (85) will be used to quality filter, cluster, and remove chimeras from demultiplexed 16S rRNA raw sequencing data of the samples. The clustered sequences at 97% similarity level will be utilized to construct operational taxonomic units (OTU) tables and representative sequences will be assigned taxonomy from phylum to species based on the Ribosomal Database Project (RDP) 16S rRNA training set (Version 16) (86).
The composition of short-chain fatty acids (SCFAs) will be identified by using the high pressure liquid chromatographic methods (Jasco Corporation, Japan) (87) and nuclear magnetic resonance (NMR) spectroscopy (88). First, the sample will be homogenized and centrifuged at low speed, and the supernatants will be filtered and mixed with phosphoric acid 0.1% as a mobile phase. Then, the mixture will be injected into the HPLC system, comprising a column Rezex™ ROA-Organic Acid H+ (8%), LC Column 300 × 7.8 mm, (Phenomenex, USA) and a UV detector at 210 nm (87). Next, the immune parameters and cytokine profiles from feces and saliva will be analyzed using the Luminex-approach and ELISA kits (87). Concentrations of the specific cytokines and the chemokines, macrophage migration inhibitory factor, macrophage inflammatory protein-1-α, monocyte chemo-attractant protein-1, immunoglobulins, and eotaxin will be determined (87). Both feces and urine samples will be further analyzed for metabolome using the NMR spectroscopy analysis (65, 88). The samples will be centrifuged, and an aqueous layer will be transferred into a 2 mL centrifuge tube. Finally, the samples will be mixed with 3-(trimethylsilyl)-1-propanesulphonic acid sodium salt (DSS) standard solution before being transferred into a tube for NMR spectroscopy analysis (65).
The IBM SPSS Statistics software version 27 (IBM Corp., Armonk, NY, USA) will be used to analyze the data. Categorical variables will be presented in frequency and percentage, while continuous variables are presented as mean ± standard deviation (SD). The normality of continuous data will be tested using the skewness test (89). Gut microbiota will be analyzed in terms of alpha diversity, beta diversity, and differential abundance of OTUs (87). The incidence rates of asthma, eczema and gastrointestinal disorders among infants will also be calculated. Principal coordinate analysis (PCoA) plots with phylogenetic and non-phylogenetic distances will be plotted (87). One-way ANOVA with corrections (Bonferroni method) and Tukey HSD test will be carried out (89) to test for statistically significant differences in taxonomic richness, diversity measures, bacterial load, and bacterial abundances. Permutational multivariate analysis of variance (PERMANOVA) based on Bray–Curtis distances and 1,000 permutations (89) will be used to evaluate which factors are associated with the composition of the microbiota.
A generalized linear model (GLM) will be used (90) to determine the associations between predictors and gut microbiota and the association between gut microbiota and infant health after controlling for confounders. The strength and precision of each association will be determined using the relative risk (RR) with 95% confidence intervals (CI) after adjusting for potential confounders. The significance level for all statistical analyses will be set at p < 0.05. Meanwhile, the Bonferroni correction will be applied to counteract the effect of multiple testing and avoid multiple spurious positives (91). The alpha value will be adjusted to account for the number of comparisons performed (91).
Knowledge regarding the numerous contributions of the gut microbiota on human health is limited, and a lot remains to be discovered. Recent cohort studies have shown that gut microbiota is associated with temperament during infancy, which refers to biologically-based individual variation in behavior in the form of activity, affectivity, and self-regulation (31, 32). Moreover, alterations and instability of the gut microbiota composition and biodiversity during infancy could lead to the development of gastrointestinal disorders (34), eczema (35), asthma (24, 36, 42, 43), and developmental delays (37, 38).
The rising attention of good gut health development in infants to ensure optimal child development in Malaysia (52–55) necessitates this prospective cohort study. The major contributions of this study would include the prospective cohort study design and providing clarity of temporal sequence between exposures and outcome. This study involves comprehensive and prospective quantitative assessments of mothers and infants. Besides, frequent collections of urine, feces, saliva, and breast milk samples enable a holistic assessment of maternal and infant gut microbiota over time, identifying the microbiota alterations and abundance. However, one of the limitations of this study is the multiple assessments on the pregnant women during their first, second and third trimesters until 12 months postpartum, which could be potentially burdening and lead to high dropout rates. The commitment required in the collection and delivery of bio-samples in the morning may be burdensome for working mothers. These situations will be addressed by providing incentives per visit and a summary of findings and reminders about all the follow-up activities via phone calls and text messages. Another possible limitation is the compliance of mothers and infant sample collections (saliva, feces, urine, and breastmilk). This limitation will be overcome using user-friendly self-collection kits with clear instructions and reminders by the researchers. Furthermore, the researchers will collect samples, thus easing the burden of respondents. Besides, there are concerns on the response and social desirability bias due to the self-report nature of the questionnaire on infant health, including temperament, gastrointestinal disorders, eczema, asthma, and developmental delays. Moreover, differences in sample handling protocols, collection procedures and processing data pipelines could be the limitation of this study.
In general, the launching and implementation of this cohort is challenging, including challenges in logistic and methodological issues such as recruitment, retention, and data collection (92, 93). The common issue in the stage of launching the cohort is that it requires allocation of human resource with training provided to the researchers and enumerators to ensure proper handling of bio-samples (92, 93). During the recruitment stage, a liaison person can be assigned to build up rapport with the respondents and to perform the follow-ups in order to address respondents' concerns about their commitment required for the whole study duration, lack of interest and reluctance to enroll in the study before obtaining the husband's approval (92). Any cases involving lack of interest or husband's reluctance should be dealt with communication and inclusion of husbands in research arrangements to raise their awareness on the importance of their wife participation in the cohort. Importantly, ethical concerns involved in conducting a birth cohort must be carefully considered (93). Besides, the necessary start-up time, staff, and costs must not be underestimated (92). Moreover, additional costs relating to logistic and other expenses must be taken into consideration (92, 93).
The study findings could provide a better understanding of the colonization and development of the gut microbiome during early life. Furthermore, identifying the pre- and post-natal factors contributing to infant gut microbiota helps to fill the current knowledge gap on infant gut health. These findings could help stakeholders such as policymakers and healthcare professionals to develop appropriate educational and intervention programs to address pre- and post-natal factors that cause poor gut health among infants. Such initiatives could reduce the occurrence of preventable NCDs among infants and the financial burden on their families. Moreover, the findings of this study are useful in addressing modifiable risk factors that may impact infant gut microbiota. Suitable lifestyle, environmental, and dietary adjustments could be implemented to strengthen infants' immunity, cognition, and digestion. In summary, the gut-brain axis is a global concern and good gut health maintenance among infants is crucial in ensuring beneficial bacterial composition, diversity, and abundance in early life.
The study will be carried out according to the guidelines in the Declaration of Helsinki. The ethical approval to conduct this study was obtained from the Ethics Committee for Research Involving Human Subject (JKEUPM) (Reference Number: JKEUPM-2021-418). Permission from the Director/General Manager of the selected private hospitals will also be attained prior to the data collection. The study is registered on the ClinicalTrial.gov platform, with the registration number NCT04919265 (https://www.clinicaltrials.gov/ct2/show/NCT04919265). The privacy and confidentially of the participants are protected due to the nature that the data can only be accessed by the research team and the results will be shown in group data. Written informed consent will be obtained from the participants prior to the administration of the study.
The studies involving human participants were reviewed and approved by Ethics Committee for Research Involving Human Subject, Universiti Putra Malaysia. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
SYE, WYG, TJ, SPL, LJL, YL, JZ, and LC conceived and designed the study. SYE, WYG, TJ, LJL, YL, JZ, and LC contributed to the study design and protocol development. SYE, WYG, TJ, SPL, LJL, YSC, LTLT, KNH, PLT, YL, JZ, and LC assisted in preparation of research materials and study launch. SYE, WYG, and LJL drafted the manuscript based on the original protocol. All authors read and approved the final version of the manuscript.
The funding of this research was supported by the Beijing Sanyuan Foods Co. Ltd.
The authors express their gratitude to the management of hospitals for granting permission to the research team to conduct this research.
Authors TJ, YL, JZ, and LC were employed by Beijing Sanyuan Foods Co. Ltd. The funder had the following involvement with the study: involvement in study design, data analysis, decision to publish, or preparation of the manuscript.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Yao Y, Cai X, Ye Y, Wang F, Chen F, Zheng C. The role of microbiota in infant health: from early life to adulthood. Front Immunol. (2021) 12:708472. doi: 10.3389/fimmu.2021.708472
2. Ronan V, Yeasin R, Claud EC. Childhood development and the microbiome-the intestinal microbiota in maintenance of health and development of disease during childhood development. Gastroenterology. (2021) 160:495–506. doi: 10.1053/j.gastro.2020.08.065
3. Sarkar A, Yoo JY, Dutra SVO, Morgan KH, Groer M. The association between early-life gut microbiota and long-term health and diseases. J Clin Med. (2021) 10:459. doi: 10.3390/jcm10030459
4. Rinninella E, Raoul P, Cintoni M, Franceschi F, Miggiano GAD, Gasbarrini A, et al. What is the healthy gut microbiota composition? A changing ecosystem across age, environment, diet, and diseases. Microorganisms. (2019) 7:14. doi: 10.3390/microorganisms7010014
5. Laursen MF. Gut microbiota development: influence of diet from infancy to toddlerhood. Ann Nutr Metab. (2021) 77:21–34. doi: 10.1159/000517912
6. Costa N, Santos P, Ferreira A, Williams B, Figueiredo A, Princisval L, et al. Maternal pre-pregnancy body mass index and gestational weight gain are associated with differences in infant gut microbiota: results from Brazilian prospective birth cohort. Curr Dev Nutr. (2020) 4:1551. doi: 10.1093/cdn/nzaa062_008
7. Miko E, Csaszar A, Bodis J, Kovacs K. The maternal-fetal gut microbiota axis: physiological changes, dietary influence, and modulation possibilities. Life. (2022) 12:424. doi: 10.3390/life12030424
8. Grech A, Collins CE, Holmes A, Lal R, Duncanson K, Taylor R, et al. Maternal exposures and the infant gut microbiome: a systematic review with meta-analysis. Gut Microbes. (2021) 13:1–30. doi: 10.1080/19490976.2021.1897210
9. Coker MO, Hoen AG Dade E, Lundgren S, Li Z, Wong AD, et al. Specific class of intrapartum antibiotics relates to maturation of the infant gut microbiota: a prospective cohort study. BJOG An Int J Obstet Gynaecol. (2020) 127:217–27. doi: 10.1111/1471-0528.15799
10. Vandenplas Y, Carnielli VP, Ksiazyk J, Luna MS, Migacheva N, Mosselmans JM, et al. Factors affecting early-life intestinal microbiota development. Nutrition. (2020) 78:110812. doi: 10.1016/j.nut.2020.110812
11. Soderborg TK, Carpenter CM, Janssen RC, Weir TL, Robertson CE, Ir D, et al. Gestational diabetes is uniquely associated with altered early seeding of the infant gut microbiota. Front Endocrinol. (2020) 11:603021. doi: 10.3389/fendo.2020.603021
12. Mirpuri J. Evidence for maternal diet-mediated effects on the offspring microbiome and immunity: implications for public health initiatives. Pediatr Res. (2021) 89:301–6. doi: 10.1038/s41390-020-01121-x
13. McLean C, Jun S, Kozyrskyj A. Impact of maternal smoking on the infant gut microbiota and its association with child overweight: a scoping review. World J Pediatr. (2019) 15:341–9. doi: 10.1007/s12519-019-00278-8
14. Benjamin-Neelon S, Differding M, Mueller N. Infants from food insecure households have altered gut microbiota (OR01-03-19). Curr Dev Nutr. (2019) 3:1743. doi: 10.1093/cdn/nzz040.OR01-03-19
15. Azad MB. Infant feeding and the developmental origins of chronic disease in the CHILD cohort: role of human milk bioactives and gut microbiota. Breastfeed Med. (2019) 14:S22–4. doi: 10.1089/bfm.2019.0029
16. Notarbartolo V, Giuffrè M, Montante C, Corsello G, Carta M. Composition of human breast milk microbiota and its role in children's health. Pediatr Gastroenterol Hepatol Nutr. (2022) 25:194–210. doi: 10.5223/pghn.2022.25.3.194
17. Jahnke JR, Roach J, Azcarate-Peril MA, Thompson AL. Maternal precarity and HPA axis functioning shape infant gut microbiota and HPA axis development in humans. PLoS ONE. (2021) 16:e0251782. doi: 10.1371/journal.pone.0251782
18. Rodriguez N, Tun HM, Field CJ, Mandhane PJ, Scott JA, Kozyrskyj AL. Prenatal depression, breastfeeding, and infant gut microbiota. Front Microbiol. (2021) 12:664257. doi: 10.3389/fmicb.2021.664257
19. Kang LJ, Koleva PT, Field CJ, Giesbrecht GF, Wine E, Becker AB, et al. Maternal depressive symptoms linked to reduced fecal Immunoglobulin A concentrations in infants. Brain Behav Immun. (2018) 68:123–31. doi: 10.1016/j.bbi.2017.10.007
20. Bhagavata Srinivasan SP, Raipuria M, Bahari H, Kaakoush NO, Morris MJ. Impacts of diet and exercise on maternal gut microbiota are transferred to offspring. Front Endocrinol. (2018) 9:716. doi: 10.3389/fendo.2018.00716
21. Zhou L, Xiao X, Li M, Zhang Q, Yu M, Zheng J, et al. Maternal exercise improves high-fat diet-induced metabolic abnormalities and gut microbiota profiles in mouse dams and offspring. Front Cell Infect Microbiol. (2020) 10:292. doi: 10.3389/fcimb.2020.00292
22. Martin R, Makino H, Yavuz AC, Ben-Amor K, Roelofs M, Ishikawa E, et al. Early-Life events, including mode of delivery and type of feeding, siblings and gender, shape the developing gut microbiota. PLoS ONE. (2016) 11:e0158498. doi: 10.1371/journal.pone.0158498
23. Hill CJ, Lynch DB, Murphy K, Ulaszewska M, Jeffery IB, O'Shea CA, et al. Evolution of gut microbiota composition from birth to 24 weeks in the INFANTMET cohort. Microbiome. (2017) 5:4. doi: 10.1186/s40168-017-0240-3
24. Kim H, Sitarik AR, Woodcroft K, Johnson CC, Zoratti E. Birth mode, breastfeeding, pet exposure, and antibiotic use: associations with the gut microbiome and sensitization in children. Curr Allergy Asthma Rep. (2019) 19:22. doi: 10.1007/s11882-019-0851-9
25. Ayeni FA, Biagi E, Rampelli S, Fiori J, Soverini M, Audu HJ, et al. Infant and adult gut microbiome and metabolome in rural Bassa and urban settlers from Nigeria. Cell Rep. (2018) 23:3056–67. doi: 10.1016/j.celrep.2018.05.018
26. Hernandez J, Rhimi S, Kriaa A, Mariaule V, Boudaya H, Drut A, et al. Domestic environment and gut microbiota: lessons from pet dogs. Microorganisms. (2022) 10:949. doi: 10.3390/microorganisms10050949
27. Levin AM, Sitarik AR, Havstad SL, Fujimura KE, Wegienka G, Cassidy-Bushrow AE, et al. Joint effects of pregnancy, sociocultural, and environmental factors on early life gut microbiome structure and diversity. Sci Rep. (2016) 6:31775. doi: 10.1038/srep31775
28. García-Mantrana I, Selma-Royo M, González S, Parra-Llorca A, Martínez-Costa C, Collado MC. Distinct maternal microbiota clusters are associated with diet during pregnancy: impact on neonatal microbiota and infant growth during the first 18 months of life. Gut Microbes. (2020) 11:962–78. doi: 10.1080/19490976.2020.1730294
29. Matsuyama M, Morrison M, Cao KAL, Pruilh S, Davies PSW, Wall C, et al. Dietary intake influences gut microbiota development of healthy Australian children from the age of one to two years. Sci Rep. (2019) 9:12476. doi: 10.1038/s41598-019-48658-4
30. Homann C-M, Rossel CAJ, Dizzell S, Bervoets L, Simioni J, Li J, et al. Infants' first solid foods: impact on gut microbiota development in two intercontinental cohorts. Nutrients. (2021) 13:2639. doi: 10.3390/nu13082639
31. Aatsinki AK, Lahti L, Uusitupa HM, Munukka E, Keskitalo A, Nolvi S, et al. Gut microbiota composition is associated with temperament traits in infants. Brain Behav Immun. (2019) 80:849–58. doi: 10.1016/j.bbi.2019.05.035
32. Wang Y, Chen X, Yu Y, Liu Y, Zhang Q, Bai J. Association between gut microbiota and infant's temperament in the first year of life in a chinese birth cohort. Microorganisms. (2020) 8:753. doi: 10.3390/microorganisms8050753
33. Xie T, Wang Y, Zou Z, Wu Y, Fan X, Dai J, et al. Relationship between the gut microbiota and temperament in children 1-2 years old in Chinese birth cohort. J Psychiatr Res. (2022) 148:52–60. doi: 10.1016/j.jpsychires.2022.01.041
34. Wei L, Singh R, Ro S, Ghoshal UC. Gut microbiota dysbiosis in functional gastrointestinal disorders: underpinning the symptoms and pathophysiology. JGH Open. (2021) 5:976–87. doi: 10.1002/jgh3.12528
35. Zheng H, Liang H, Wang Y, Miao M, Shi T, Yang F, et al. Altered gut microbiota composition associated with eczema in infants. PLoS ONE. (2016) 11:e0166026. doi: 10.1371/journal.pone.0166026
36. Alsharairi NA. The infant gut microbiota and risk of asthma: the effect of maternal nutrition during pregnancy and lactation. Microorganisms. (2020) 8:1119. doi: 10.3390/microorganisms8081119
37. Laue HE, Coker MO, Madan JC. The developing microbiome from birth to 3 years: the gut-brain axis and neurodevelopmental outcomes. Front Pediatr. (2022) 10:815885. doi: 10.3389/fped.2022.815885
38. Sordillo JE, Korrick S, Laranjo N, Carey V, Weinstock GM, Gold DR, et al. Association of the infant gut microbiome with early childhood neurodevelopmental outcomes. JAMA Netw Open. (2019) 2:e190905. doi: 10.1001/jamanetworkopen.2019.0905
39. Rothbart MK. Temperament, development, and personality. Curr Dir Psychol Sci. (2007) 16:207–12. doi: 10.1111/j.1467-8721.2007.00505.x
40. Chew KS, Em JM, Koay ZL, Jalaludin MY, Ng RT, Lum LCS, et al. Low prevalence of infantile functional gastrointestinal disorders (FGIDs) in a multi-ethnic Asian population. Pediatr Neonatol. (2020) 62:49–54. doi: 10.1016/j.pedneo.2020.08.009
41. Van Tilburg MAL, Hyman PE, Walker L, Rouster A, Palsson OS, Kim SM, et al. Prevalence of functional gastrointestinal disorders in infants and toddlers. J Pediatr. (2015) 166:684–9. doi: 10.1016/j.jpeds.2014.11.039
42. Durack J, Kimes NE, Lin DL, Rauch M, McKean M, McCauley K, et al. Delayed gut microbiota development in high-risk for asthma infants is temporarily modifiable by Lactobacillus supplementation. Nat Commun. (2018) 9:707. doi: 10.1038/s41467-018-03157-4
43. Johnson CC, Ownby DR. The infant gut bacterial microbiota and risk of pediatric asthma and allergic diseases. Transl Res. (2017) 179:60–70. doi: 10.1016/j.trsl.2016.06.010
44. Robertson RC, Manges AR, Finlay BB, Prendergast AJ. The human microbiome and child growth – first 1000 days and beyond. Trends Microbiol. (2019) 27:131–47. doi: 10.1016/j.tim.2018.09.008
45. Woon FC, Chin YS, Ismail IH, Abdul Latiff AH, Batterham M, Chan YM. MICOS Research Group. Maternal Vitamin D levels during late pregnancy and risk of allergic diseases and sensitization during the first year of life—a birth cohort study. Nutrients. (2020) 12:2418. doi: 10.3390/nu12082418
46. Yan C, Zhao H, Nayar N, Rhee KE, Lumeng JC. Diet potentially drives the differentiation of eating behaviours via alterations to the gut microbiome in infants. bioRxiv. (2021) doi: 10.1101/2021.04.24.438478 (Preprint).
47. Orbe-Orihuela YC, Lagunas-Martínez A, Bahena-Román M, Madrid-Marina V, Torres-Poveda K, Flores-Alfaro E, et al. High relative abundance of firmicutes and increased TNF-α levels correlate with obesity in children. Salud Publica Mex. (2018) 60:5–11. doi: 10.21149/8133
48. Iddrisu I, Monteagudo-Mera A, Poveda C, Pyle S, Shahzad M, Andrews S, et al. Malnutrition and gut microbiota in children. Nutrients. (2021) 13:2727. doi: 10.3390/nu13082727
49. Million M, Diallo A, Raoult D. Gut microbiota and malnutrition. Microb Pathog. (2017) 106:127–38. doi: 10.1016/j.micpath.2016.02.003
50. Jena A, Montoya CA, Mullaney JA, Dilger RN, Young W, McNabb WC, et al. Gut-brain axis in the early postnatal years of life: a developmental perspective. Front Integr Neurosci. (2020) 14:44. doi: 10.3389/fnint.2020.00044
51. East P, Doom J, Blanco E, Burrows R, Lozoff B, Gahagan S. Young adult outcomes associated with lower cognitive functioning in childhood related to iron-fortified formula in infancy. Nutr Neurosci. (2022) 25:709–18. doi: 10.1080/1028415X.2020.1804099
52. Chong CW, Ahmad AF, Lim YAL, Teh CSJ, Yap IKS, Lee SC, et al. Effect of ethnicity and socioeconomic variation to the gut microbiota composition among pre-adolescent in Malaysia. Sci Rep. (2015) 5:13338. doi: 10.1038/srep13338
53. Lee YY, Hassan SA, Ismail IH, Chong SY, Raja Ali RA, Amin Nordin S, et al. Gut microbiota in early life and its influence on health and disease: a position paper by the Malaysian working group on gastrointestinal health. J Paediatr Child Health. (2017) 53:1152–8. doi: 10.1111/jpc.13640
54. Khine WWT, Zhang Y, Goie GJY, Wong MS, Liong M, Lee YY, et al. Gut microbiome of pre-adolescent children of two ethnicities residing in three distant cities. Sci Rep. (2019) 9:7831. doi: 10.1038/s41598-019-44369-y
55. Lau ASY, Yanagisawa N, Hor YY, Lew LC, Ong JS, Chuah LO, et al. Bifidobacterium longum BB536 alleviated upper respiratory illnesses and modulated gut microbiota profiles in Malaysian pre-school children. Benef Microbes. (2018) 9:61–70. doi: 10.3920/BM2017.0063
56. Nurliyana AR, Mohd Shariff Z, Mohd Taib MN, Gan WY, Tan KA. Early nutrition, growth and cognitive development of infants from birth to 2 years in Malaysia: a study protocol. BMC Pediatr. (2016) 16:160. doi: 10.1186/s12887-016-0700-0
57. Jan Mohamed HJ, Rowan A, Fong B, Loy SL. Maternal serum and breast milk vitamin D levels: findings from the Universiti Sains Malaysia pregnancy cohort study. PLoS ONE. (2014) 9:e100705. doi: 10.1371/journal.pone.0100705
58. Chan AW, Tetzlaff JM, Altman DG, Laupacis A, Gøtzsche PC, KrleŽa-Jerić K, et al. SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann Intern Med. (2013) 158:200–7. doi: 10.7326/0003-4819-158-3-201302050-00583
59. Azad MB, Konya T, Persaud RR, Guttman DS, Chari RS, Field CJ, et al. Impact of maternal intrapartum antibiotics, method of birth and breastfeeding on gut microbiota during the first year of life: a prospective cohort study. BJOG An Int J Obstet Gynaecol. (2016) 123:983–93. doi: 10.1111/1471-0528.13601
60. Chen Y, Zhou Z, Yang W, Bi N, Xu J, He J, et al. Development of a data-independent targeted metabolomics method for relative quantification using liquid chromatography coupled with tandem mass spectrometry. Anal Chem. (2017) 89:6954–62. doi: 10.1021/acs.analchem.6b04727
61. Want EJ, Masson P, Michopoulos F, Wilson ID, Theodoridis G, Plumb RS, et al. Global metabolic profiling of animal and human tissues via UPLC-MS. Nat Protoc. (2013) 8:17–32. doi: 10.1038/nprot.2012.135
62. Shukri NHM, Wells J, Mukhtar F, Lee MHS, Fewtrell M. Study protocol: an investigation of mother-infant signalling during breastfeeding using a randomised trial to test the effectiveness of breastfeeding relaxation therapy on maternal psychological state, breast milk production and infant behaviour and growth. Int Breastfeed J. (2017) 12:33. doi: 10.1186/s13006-017-0124-y
63. Zhao J, Liu Q, Liu Y, Qiao W, Yang K, Jiang T, et al. Quantitative profiling of glycerides, glycerophosphatides and sphingolipids in Chinese human milk with ultra-performance liquid chromatography/quadrupole-time-of-flight mass spectrometry. Food Chem. (2021) 346:128857. doi: 10.1016/j.foodchem.2020.128857
64. Huang X, Zhu B, Jiang T, Yang C, Qiao W, Hou J, et al. Improved simple sample pretreatment method for quantitation of major human milk oligosaccharides using ultrahigh pressure liquid chromatography with fluorescence detection. J Agric Food Chem. (2019) 67:12237–44. doi: 10.1021/acs.jafc.9b03445
65. Zhao J, Yi W, Liu B, Dai Y, Jiang T, Chen S, et al. MFGM components promote gut Bifidobacterium growth in infant and in vitro. Eur J Nutr. (2022) 61:277–88. doi: 10.1007/s00394-021-02638-5
66. Zhang X, Zhang M, Lin T, Zhao J, Luo Z, Hou J, et al. Relationship between traditional maternal diet pattern and breastmilk composition of rural lactating women during the first month postpartum in Shigatse, Tibet. Food Sci Nutr. (2021) 9:4185–98. doi: 10.1002/fsn3.2384
67. Tee ES, Mohd Ismail N, Mohd Nasir A, Khatijah I. Nutrient Composition of Malaysian Foods. 4th ed. Kuala Lumpur: Institute for Medical Research (1997).
68. Institute Institute of Nutrition Mahidol University. ASEAN Food Composition Database, Electronic version 1. (2014). Available online at: http://www.inmu.mahidol.ac.th/aseanfoods/doc/ASEAN_FCD_V1_2014.pdf (accessed July 7, 2021).
69. National Coordinating Committee on Food and Nutrition. Recommended Nutrient Intakes for Malaysia. A Report of the Technical Working Group on Nutritional Guidelines. Putrajaya: Ministry of Health Malaysia (2017).
70. World Health Organization & United Nations Children's Fund. Indicators for Assessing Infant and Young Child Feeding Practices: Definitions and Measurement Methods. Geneva: World Health Organization & United Nations Children's Fund (2021).
71. Food and Agriculture Organization of the United Nations. Guidelines for Measuring Household and Individual Dietary Diversity. Rome: Food and Agriculture Organization of the United Nations (2013).
72. Chasan-Taber L, Schmidt MD, Roberts DE, Hosmer D, Markenson G, Freedson PS. Development and validation of a pregnancy physical activity questionnaire. Med Sci Sports Exerc. (2004) 36:1750–60. doi: 10.1249/01.MSS.0000142303.49306.0D
73. Blumberg SJ, Bialostosky K, Hamilton WL, Briefel RR. The effectiveness of a short form of the household food security scale. Am J Public Health. (1999) 89:1231–4. doi: 10.2105/AJPH.89.8.1231
74. Cohen S, Kamarck T. Mermelstein R. A global measure of perceived stress. J Health Soc Behav. (1983) 24:385–96. doi: 10.2307/2136404
75. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression: development of the 10-item Edinburgh postnatal depression scale. Br J Psychiatry. (1987) 150:782–6. doi: 10.1192/bjp.150.6.782
76. Hyams JS, Di Lorenzo C, Saps M, Shulman RJ, Staiano A, van Tilburg M. Childhood functional gastrointestinal disorders: child/adolescent. Gastroenterology. (2016) 150:1456–68. doi: 10.1053/j.gastro.2016.02.015
77. Gartstein MA, Rothbart MK. Studying infant temperament via the revised infant behavior questionnaire. Infant Behav Dev. (2003) 26:64–86. doi: 10.1016/S0163-6383(02)00169-8
78. Williams HC, Jburney PG, Hay RJ, Archer CB, Shipley MJ, Ahunter JJ, et al. The UK Working Party's diagnostic criteria for Atopic Dermatitis I Derivation of a minimum set of discriminators for atopic dermatitis. Br J Dermatol. (1994) 131:383–96. doi: 10.1111/j.1365-2133.1994.tb08530.x
79. Charman CR, Venn AJ, Williams HC. The patient-oriented eczema measure. Arch Dermatol. (2004) 140:1513–9. doi: 10.1001/archderm.140.12.1513
80. Castro-Rodríguez JA, Holberg CJ, Wright AL, Martinez FD. A clinical index to define risk of asthma in young children with recurrent wheezing. Am J Respir Crit Care Med. (2000) 162:1403–6. doi: 10.1164/ajrccm.162.4.9912111
81. Llewellyn CH, van Jaarsveld CHM, Johnson L, Carnell S, Wardle J. Development and factor structure of the baby eating behaviour questionnaire in the Gemini birth cohort. Appetite. (2011) 57:388–96. doi: 10.1016/j.appet.2011.05.324
82. Wardle J, Guthrie CA, Sanderson S, Rapoport L. Development of the children's eating behaviour questionnaire. J Child Psychol Psychiatry. (2001) 42:963–70. doi: 10.1111/1469-7610.00792
83. Squires J, Bricker D. Ages & Stages Questionnaires, Third Edition (ASQ-3): A Parent Completed Child Monitoring System. Baltimore, MD: Paul H Brookes Publishing Co, Inc. (2009).
84. Herlemann DPR, Labrenz M, Jürgens K, Bertilsson S, Waniek JJ, Andersson AF. Transitions in bacterial communities along the 2000 km salinity gradient of the Baltic Sea. ISME J. (2011) 5:1571–9. doi: 10.1038/ismej.2011.41
85. Edgar RC. Search and clustering orders of magnitude faster than BLAST. Bioinformatics. (2010) 26:2460–1. doi: 10.1093/bioinformatics/btq461
86. Wang Q, Garrity GM, Tiedje JM, Cole JR. Naive Bayesian classifier for rapid assignment of rRNA sequences into the new bacterial taxonomy. Appl Environ Microbiol. (2007) 73:5261–7. doi: 10.1128/AEM.00062-07
87. García-Mantrana I, Alcántara C, Selma-Royo M, Boix-Amorós A, Dzidic M, Gimeno-Alcañiz J, et al. MAMI: a birth cohort focused on maternal-infant microbiota during early life. BMC Pediatr. (2019) 19:140. doi: 10.1186/s12887-019-1502-y
88. Armstrong CW, McGregor NR, Lewis DP, Butt HL, Gooley PR. The association of fecal microbiota and fecal, blood serum and urine metabolites in myalgic encephalomyelitis/chronic fatigue syndrome. Metabolomics. (2017) 13:8. doi: 10.1007/s11306-016-1145-z
89. George D, Mallery P, IBM SPSS. Statistics 26 Step By Step: A Simple Guide and Reference. New York, NY: Routledge. (2019).
90. McCulloch CE. Generalized linear models. J Am Stat Assoc. (2000) 95:1320–4. doi: 10.1080/01621459.2000.10474340
91. VanderWeele TJ, Mathur MB. Some desirable properties of the Bonferroni correction: is the Bonferroni correction really so bad? Am J Epidemiol. (2019) 188:617–8. doi: 10.1093/aje/kwy250
92. Eskenazi B, Gladstone EA, Berkowitz GS, Drew CH, Faustman EM, Holland NT, et al. Methodologic and logistic issues in conducting longitudinal birth cohort studies: lessons learned from the centers for children's environmental health and disease prevention research. Environ Health Perspect. (2005) 113:1419–29. doi: 10.1289/ehp.7670
Keywords: birth cohort study, microbiota, eczema, asthma, developmental delays, gastrointestinal disorders
Citation: Eow SY, Gan WY, Jiang T, Loh SP, Lee LJ, Chin YS, Than LTL, How KN, Thong PL, Liu Y, Zhao J and Chen L (2022) MYBIOTA: A birth cohort on maternal and infant microbiota and its impact on infant health in Malaysia. Front. Nutr. 9:994607. doi: 10.3389/fnut.2022.994607
Received: 15 July 2022; Accepted: 12 September 2022;
Published: 27 September 2022.
Edited by:
Diego G. Peroni, University of Pisa, ItalyReviewed by:
Phatthanaphong Therdtatha, Chiang Mai University, ThailandCopyright © 2022 Eow, Gan, Jiang, Loh, Lee, Chin, Than, How, Thong, Liu, Zhao and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wan Ying Gan, d2FueWluZ0B1cG0uZWR1Lm15; Lijun Chen, Y2hlbmxpanVuQHNhbnl1YW4uY29tLmNu
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.