
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Nutr., 15 March 2022
Sec. Clinical Nutrition
Volume 9 - 2022 | https://doi.org/10.3389/fnut.2022.823039
 Cicero Jonas R. Benjamim1*
Cicero Jonas R. Benjamim1* Andrey Alves Porto2
Andrey Alves Porto2 Vitor Engrácia Valenti2Andressa Crystine da Silva Sobrinho1
Vitor Engrácia Valenti2Andressa Crystine da Silva Sobrinho1 David M. Garner2,3
David M. Garner2,3 Bruno Gualano4
Bruno Gualano4 Carlos Roberto Bueno Júnior1,5
Carlos Roberto Bueno Júnior1,5Background: Although there are a considerable number of clinical studies on nitrate (NO3) rich beetroot juice (BRJ) and hypertension, it is difficult to indicate the real effects of NO3 from BRJ on the BP of hypertensive patients because there are still no estimates of the effects of NO3 derived from BRJ on the BP of hypertension patients.
Objective: To clarify these effects, we developed a systematic literature review with a meta-analysis of randomized clinical trials (RCTs).
Design: The searches were accomplished through EMBASE, Cochrane Library, MEDLINE, CINAHL, Web of Science, and LILACS databases. The study included single or double-blinded RCTs and participants older than 18 years with hypertension [systolic BP (SBP) > 130 mmHg and diastolic BP (DBP) > 80 mmHg]. NO3 BRJ was required to be consumed in a format that possibly blinded participants/researchers. These studies should also report the SBP and DBP values (mmHg) measured before and after the treatment. Risk of Bias tools and GRADE were enforced.
Results: Seven studies were included (218 participants). BRJ intervention time ranged from 3 to 60 days with daily dosages of 70–250 mL of BRJ. After the intervention with NO3 from BRJ, SBP underwent significant changes (p < 0.001) of −4.95 (95% CI: −8.88; −1.01) (GRADE: ⊕⊕⊕○ Moderate), but not for DBP (p = 0.06) −0.90 mmHg (95% CI: −3.16; 1.36) (GRADE: ⊕⊕⊕○ Moderate), compared to the control group.
Conclusions: The NO3 derived from BRJ reduces SBP, but not DBP in patients with arterial hypertension.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=269339.
Beetroot juice (BRJ) is rich in nitrate (NO3) and has the potential to reduce blood pressure (BP). NO3 is a precursor for the production of nitric oxide (NO) and increases its concentrations in the bloodstream, optimizing endothelial function (e.g., vasodilation) (1). A recent meta-analysis found that BRJ NO3 (2–56 days of intervention) reduced typically −3.55 mmHg and −1.32 mmHg for systolic (SBP) and diastolic BP (DBP), respectively, in a mixed sample of individuals with and without arterial hypertension (2). This result is of clinical relevance in the control of arterial hypertension, as a 2-mmHg reduction in BP can reduce mortality from ischemic heart disease by 7 and 10% of mortality from stroke (3). The latest systematic review with only hypertensive patients concluded that there is insufficient evidence to support or refute the use of inorganic NO3 as a strategy to decrease BP. However, this review included studies intervening with NO3 salts not from beetroot only and physical exercise programs, lacking an estimate of the effect of the intervention. Therefore, there are significant limitations to the conclusions on the influence of BRJ in hypertensive patients restricted to its findings (4).
Beetroot is rich in bioactive compounds (betalains, flavonoids, and polyphenols), which can influence the endothelial and pressure responses differently from NO3 salts (5). Although there are a considerable number of clinical studies on BRJ rich in NO3 and hypertension, it is difficult to indicate the real effects of NO3 from BRJ on the BP of hypertensive patients because there are still no estimates of the effects of NO3 derived from BRJ on the BP of patients with hypertension. Based on the information presented above, we raise the following question: is the NO3 of the BRJ capable of decreasing the BP in hypertensive patients? To clarify this issue, our study aimed to carry out a systematic review with meta-analysis to verify the effects of the NO3 of the BRJ on the BP of patients with hypertension and to include subanalyses with BP values obtained by clinical measurements and ambulatory 24-h monitoring.
The review was described according to the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyzes (PRISMA) (6) and is registered in the PROSPERO database (CRD42021269339).
The searches were accomplished through EMBASE, Cochrane Library, MEDLINE (via PubMed), CINAHL, Web of Science, and LILACS databases with the application of the keywords “Beetroot juice” OR “Nitrates” OR “Red beet” OR “Beta vulgaris” AND “Blood pressure” OR “Hypertension.” The search relied on the Boolean NOT for the descriptor “Exercise.”
All articles identified were exported to the Rayyan QCRI program (Qatar Computing Research Institute, Qatar) to exclude duplicates. The studies were screened in the Rayyan program by reading the title and abstract. The eligibility stage was achieved by reading the articles entirely by two independent reviewers (CJRB and AAP). Another reviewer was invited to give a judgment (VEV) if there was a difference of opinion concerning a study.
The studies were required to originate from peer-reviewed journals published from the interception of the database until July 14, 2021. For inclusion, the articles needed to accomplish all the criteria are described below as follows: single or double-blinded RCTs design; participants older than >18 years old, previously diagnosed with hypertension or higher BP inclusion criteria for baseline SBP > 130 mmHg and DBP > 80 mmHg in accordance to American College of Cardiology (ACC) and American Heart Association (AHA) (7). NO3 from BRJ should necessarily be consumed in a format that blinded participants and researchers, and control intervention should use BRJ in a NO3 depleted condition. These studies reported the SBP and DBP values (mmHg) were measured before and after the intervention.
Information about the author, study design, features of the study participants, intervention, and the results of the respective studies were reported. Missing data were requested by contacting the corresponding study authors. This stage was completed independently by one reviewer (CJRB). When the author's correspondent did not answer, the Web Plot Digitizer® was applied to extract data presented in the graphs. We adopted the criteria of extracting the data postintervention, and the mean and standard deviations (MSD) were logged. Values presented with “standard error” or “confidence intervals” (CI) in the studies were transformed to MSD.
The bias analysis was completed at Risk of Bias tools originated in the Cochrane organization (8) via the Review Manager program (RevMan 5.4.1). Risk of bias is a tool founded on the domains (9). The evaluation was split into seven fields: “Random sequence generation,” “Allocation concealment,” “Blinding of participants and personnel,” “Blinding of outcome assessment,” “Incomplete outcome data,” “Selective reporting,” and “Other Bias.” The classification was split into three direct responses: low risk, unclear risk, and high risk. Our deductions were based on the table developed by Carvalho et al. (9), “Reviewer's judgment and criteria for judgment.” Two independent authors achieved the analysis of the risk of bias (CJRB & AAP) and a third (VEV) was consulted if there were any discrepancies in the decisions.
The Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) Working Group (GRADE Working Group, 2004) was surveyed to analyze the certainty of the evidence, including the study design of randomized trials (strong evidence). Study quality (detailed study methods and execution) and significant limitations secondarily were considered in the strength of evidence analysis (10). The summary of the findings table was created using GRADEpro GDT version 4® (McMaster University, ON, Canada).
A narrative synthesis was executed to describe detailed data on how each study was completed. The details for each study were introduced in texts and tables. The results of the individual qualitative analysis for each study were made by analyzing the behavior of SBP and DBP (mmHg) pre- and postintervention BRJ rich in NO3 or without NO3.
In the meta-analysis, we inserted the SBP and DBP clinical values (measured with a sphygmomanometer) and ambulatory 24 h (measuring every 15–30 min during 24-h monitoring). The effects of BRJ interventions on SBP and DBP were assessed on the alteration between the intervention and control groups. The data enforced to construct the meta-analysis was the period postintervention.
Heterogeneity was calculated via the I2 statistic, where a number >50% was considered to indicate substantial heterogeneity between the tests (11). For the values of “95% CI” and “Test for overall effect size,” values of p < 0.05 were assumed as significant differences. We enforced a random-effects model, considering that this is a more conservative method which allows that the heterogeneity of the study may fluctuate beyond chance, providing further generalizable results (8). All data was made by the Review Manager Program (RevMan 5.4.1).
A total of 326 studies were identified via searches in the databases. After the removal of duplicates (n = 116), 210 publications were screened for inclusion. Amongst them, 137 records were excluded after reviewing the title/abstract. The remaining 79 papers were selected for full-text reading. Finally, seven studies were included in the qualitative (systematic review) and quantitative (meta-analysis) synthesis. The search process and selection step details are confirmed in the flow diagram of the PRISMA protocol (Figure 1).
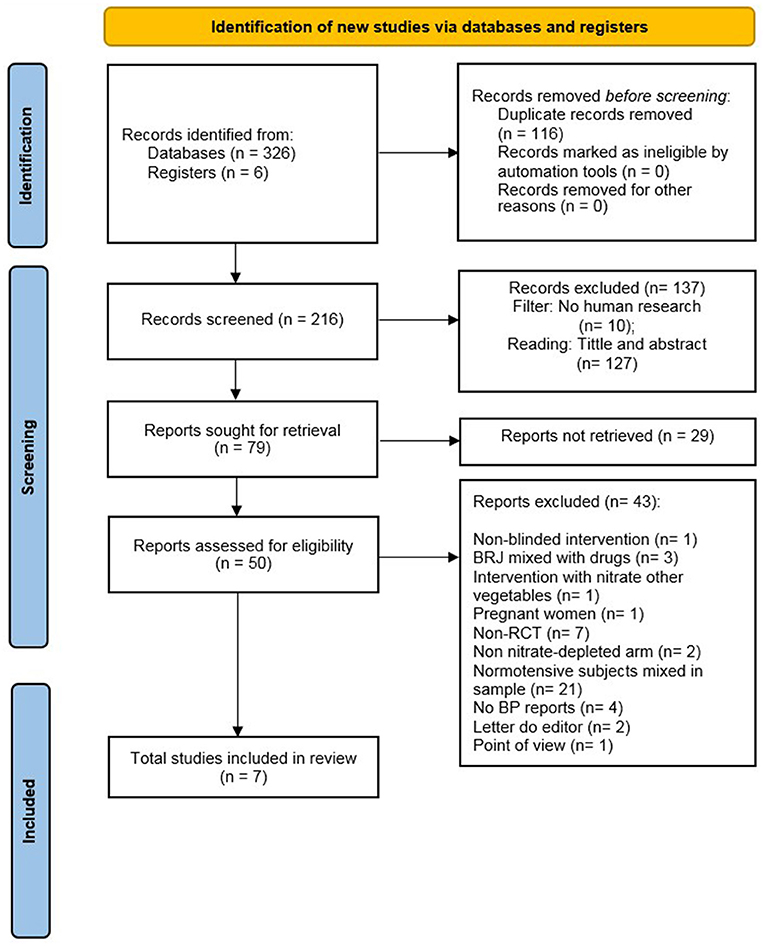
Figure 1. Flowchart prisma.
The studies included in this review were published between 2013 and 2020 (Table 1). Three studies were completed in the United Kingdom (15, 16, 18), and the others were undertaken in Australia (13), Brazil (12), the USA (14), and Ireland (17).
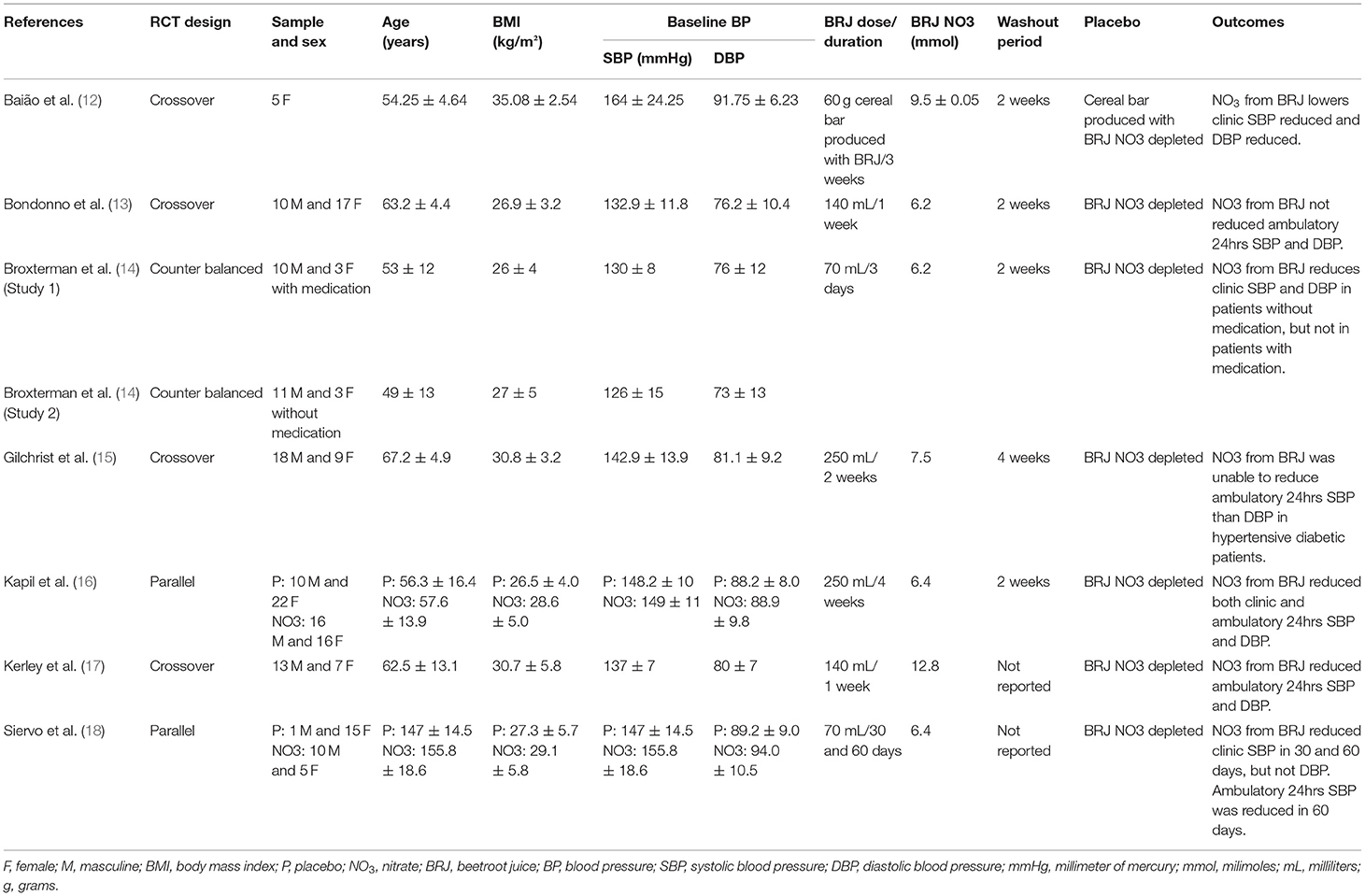
Table 1. Description of the characteristics of the study population, intervention, and outcomes articles by author and year, trial design, sample and sex, age (years), BMI (kg/m2), BP baseline, BRJ dose/duration, BRJ NO3 concentration, washout period, placebo, and outcomes.
All studies included in the systematic review participated in the calculation of the meta-analysis but were allocated into “Clinic” and “Ambulatory” subgroups. Only the studies by Kapil et al. (16) and Siervo et al. (18) performed both clinical and ambulatory 24-h measurements of SBP and DBP and had data entered into both the subgroups. Complementarily, we performed the calculation with the values of all clinical and ambulatory measurements together. The net deviations and 95% CI constant with the BP values for each assay are illustrated in Table 2, Figure 3.
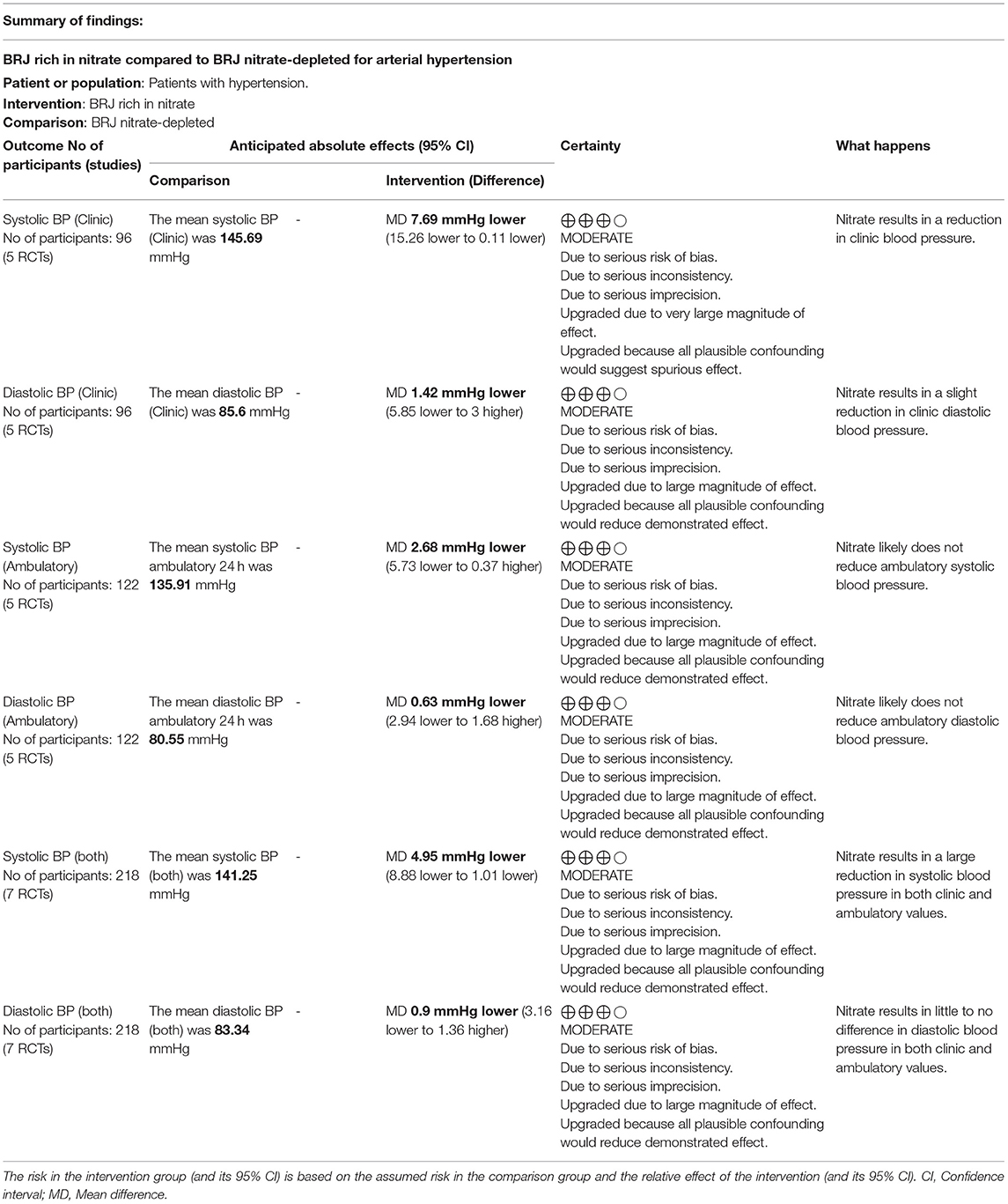
Table 2. Summary of findings: GRADE.
The study by Siervo et al. (18) was included twice in the clinical BP measurement meta-analysis graph, as the measurement of SBP and DBP occurred twice, at 30 (n-1) and 60 (n-2) days after the start of the intervention. The study by Broxterman et al. (14) took results from the two clinical trials: Study 1 was performed with patients using pharmacotherapies for arterial hypertension and Study 2 with patients without pharmacotherapies for arterial hypertension.
Most studies presented “Low risk” or “Uncertain risk” of bias according to the reviewers' judgment (Figure 2). In the domain of “Random sequence generation,” Kapil et al. (16), Baião et al. (12), Broxterman et al. (14), and Gilchrist et al. (15) did not provide information on how the random sequence of treatment was generated and presented an uncertain risk of bias. The studies by Bondonno et al. (13), Kerley et al. (17), and Siervo et al. (18) showed a low risk of bias as they generated the allocation sequence from online software. In the domain of “Allocation concealment,” Kapil et al. (16), Baião et al. (12), Broxterman et al. (14), and Kerley et al. (17) did not provide information on whether the intervention vials were coded with placebo or experimental treatment and who was responsible for this and therefore presented an uncertain risk of bias. Bondonno et al. (13), Gilchrist et al. (15), and Siervo et al. (18) presented a low risk of bias in this domain as they coded interventions, and the codes were placed in sealed letters.
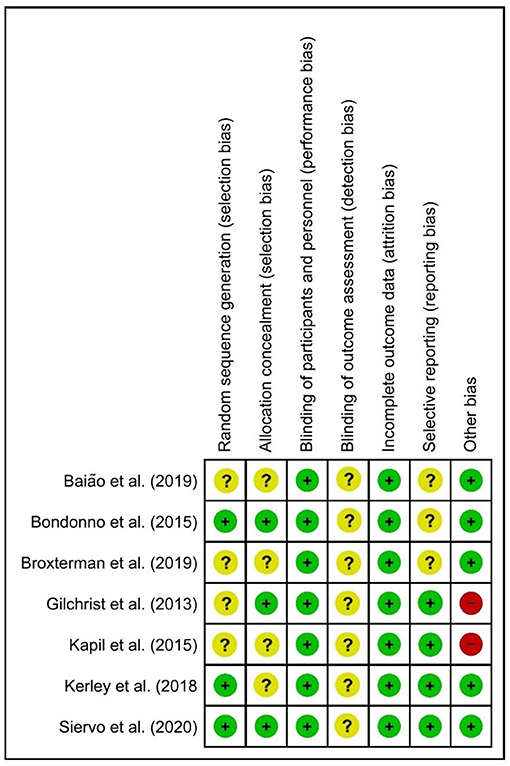
Figure 2. Cochrane risk of bias tool.
In “Blinding of participants and personnel” all studies presented a low risk of bias as they concealed the experimental intervention with the BRJ without NO3. No studies provided information on “Blinding of outcome assessment,” and so all the studies presented an uncertain risk of bias in this domain.
In “Incomplete outcome data,” all studies presented a low risk of bias, as they presented data on all variables that were evaluated in the methodology section of the article. Regarding the “Selective reporting” domain, three of the seven studies presented an uncertain risk of bias, as they did not publish the clinical trial protocol and, it is impossible to know whether the results of all published variables were previously described in the protocols.
For the domain of “Other bias,” the study by Kapil et al. (16) and Gilchrist et al. (15) presented a high risk of bias, as they did not recommend not to use mouthwash or to use antibiotics during the experiments. The other studies (12–14, 17, 18) demonstrated a low risk of bias, as they controlled the pharmacotherapies during the study, provided a list of foods rich in nitrate for participants to avoid during the study, and provided guidelines not to use mouthwash during the study.
The intervention time with BRJ in the studies ranged from 3 to 60 days with daily dosages of 70–250 mL of BRJ. Only two studies reported the time of the day when BRJ was consumed, where Kerley et al. (17) offered BRJ at 09:00 a.m and Gilchrist et al. (15) between 06:00 and 08:00 p.m. Four included studies had crossinterventions (12, 13, 15, 17), two presented a parallel study design (16, 18) and a counterbalanced (14). Five of the seven studies established a washout period between interventions that ranged from 2 to 4 weeks (12–16) (Table 1). Studies performed blood or salivary analyzes to attest to changes in plasma nitrite/nitrate concentrations, and all studies found significant increases in nitrite/nitrate concentrations during and after intervention with NO3 rich BRJ (12–18).
Among five studies that accomplished BP measurements by clinical measurement, four demonstrated a reduction in SBP values (12, 14, 16, 18) and three studies established a reduction in BP DBP (12, 14, 16). Of the five studies that obtained BP values by a 24-h ambulatory measurement, three showed a significant reduction in SBP (16–18) and none of the studies showed a significant reduction in DBP. The benefits of nitrate-rich BRJ in reducing BP were less significant when 24-h ambulatory BP measurement was performed compared to clinical measurement studies. The certainty of evidence from the studies is presented in the GRADE summary of findings (Table 2).
We applied a random effect and mean difference model to quantify the effect size (black diamonds); the diamond dimension represents the 95% CI. A negative effect indicates decreased SBP and DBP values in the nitrate-rich BRJ group compared to placebo.
In clinically measured SBP values, an important decrease was observed in the “Test for overall effect,” where we revealed a p = 0.04 and heterogeneity of 62%. The subtotal (CI) was −7.69 mmHg (95% CI: −15.26; −0.11). In the ambulatory SBP values, no significant changes were observed in “Test for overall effect,” and we found a value of p = 0.16 and heterogeneity of 39%. The subtotal (CI) was −2.68 mmHg (95% CI: −5.73; 0.37). When we calculated SBP values for the two forms of BP measurement (clinical and ambulatory), significant changes were observed, in which for the “Test for overall effect” we found a p < 0.001 and heterogeneity of 67%. The total (CI) was −4.95 (95%CI: −8.88; −1.01) (Figure 3).
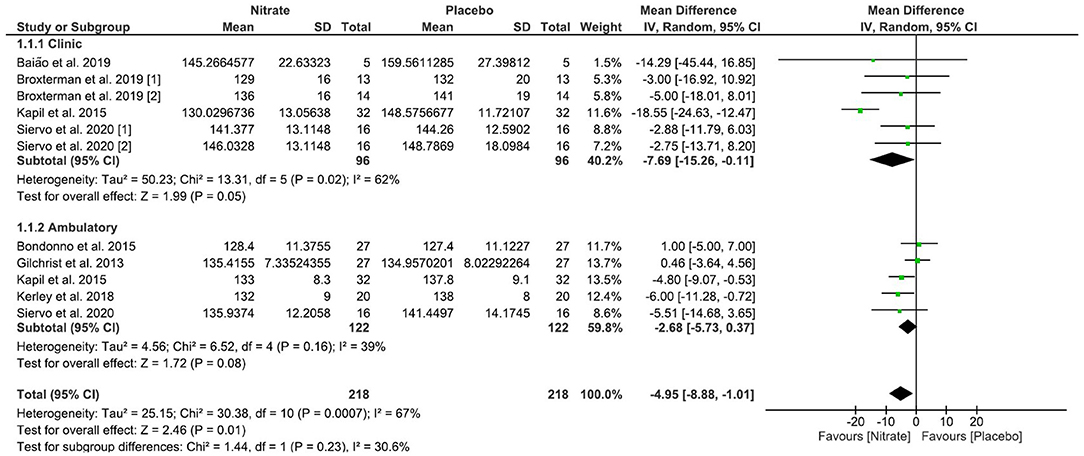
Figure 3. Effects of NO3 derived from BRJ on SBP (mmHg) values.
A significant reduction was observed for the clinical DBP values for “Test for overall effect,” which revealed a value of p = 0.03 and heterogeneity of 59%. The subtotal (CI) was −1.42 mmHg (95% CI: −5.85; 3.00). No significant change was observed for outpatient DBP values. For the “Test for overall effect,” we revealed a value of p = 0.59 and heterogeneity of 22%. The subtotal (CI) was −0.63 mmHg (95%CI: −2.94; 1.68). When outpatient and clinical DBP values were analyzed together in calculating the meta-analysis, no significant change was observed. The “Test for overall effect” revealed a value of p = 0.06 and heterogeneity of 44%. The subtotal CI was −0.90 mmHg (95% CI: −3.16; 1.36) (Figure 4).
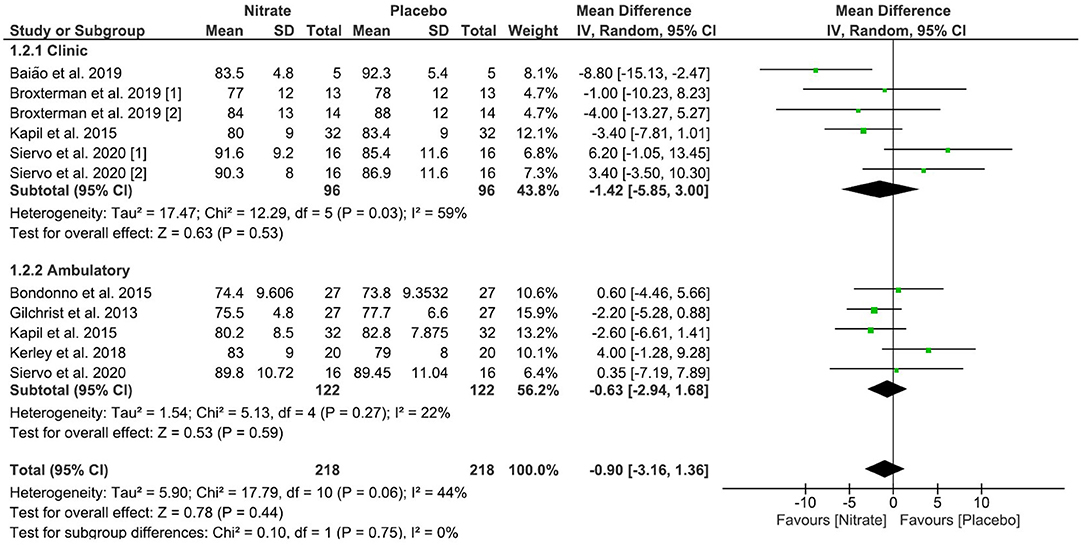
Figure 4. Effects of NO3 derived from BRJ on DBP (mmHg) values.
Sensitivity analyzes were completed to assess the influence of the results of each study on the overall outcome of the meta-analysis (Supplementary Material 1).
This systematic review with meta-analysis was completed with the aim of clarifying the effects of NO3 of the BRJ on the SBP and DBP of patients with arterial hypertension. Our study is innovative due to the stratification of the effects of NO3 between BP values obtained by clinical and 24-h ambulatory measurements, and it is the first meta-analysis to analyze the effects of NO3 of BRJ in an exclusive sample of patients with hypertension.
The increase in NO concentration promotes vascular smooth muscle relaxation by different cellular mechanisms [e.g., activation of K+ channels; cyclic guanosine monophosphate (cGMP)-dependent protein kinase (PKG)] and then promotes blood pressure decrease through muscle relaxation in the endothelium via increased activity of endothelial NO synthase (eNOS) (19). NO also appears to modify neural control of the cardiovascular system by reducing the flow of sympathetic modulation (20). Through nitrate/nitrite salivary and blood tests, the studies included in this review confirmed that the decrease in SBP was due to the increase in nitrate and nitrite mediating the augment in NO production (12–18).
Beetroot juice also has antioxidant substances such as flavonoids, anthocyanins, and betaine mixed to NO3, which can optimize endothelial function and lower blood pressure in different pathways than isolated NO3 salts use (5, 21). Studies with only NO3 salts instead of NO3-rich BRJ demonstrate smaller changes in SBP (2, 22). The synergistic effects of NO3 from BRJ with other beverage components (e.g., betaines, anthocyanins, vitamins, and minerals) on BP are unknown, but we assume they exist. We recognized the difficulty in solving these questions, as studies should control the effects of NO3 from BRJ with an intervention without NO3 and without the bioactive compounds present in BRJ. To date, interventions that offer these characteristics are unknown.
In the subgroup analysis, we divided BP measurements into “clinical” and “ambulatory,” and the calculation of the meta-analysis revealed that the NO3 of the BRJ decreases the SBP of studies in which the values are obtained with clinical measurement. In studies where only ambulatory 24-h data are analyzed, the SBP is not lowered compared to the control group. The values obtained by both clinical and ambulatory measurements were added to the total calculation of the meta-analysis, and the decrease in SBP under the effects of BRJ NO3 remains. For DBP values, a significant reduction was only detected when this parameter was measured clinically but was not diminished when there was a 24-h ambulatory measurement. Furthermore, the analysis of clinical and outpatient values together did not show a significant reduction in DBP, reinforcing that DBP is not significantly influenced by the NO3 of the BRJ.
There is no explanation why the DBP was not reduced. Based on other observations, we understand that this is due to DBP having low or slight variation in studies focused on the treatment of hypertension, especially when the prevalence of hypertensive patients with baseline DBP > 90 mmHg is low, as in the RCTs included in this review (23).
Regarding SBP, the study by Banegas et al. (24), with a sample of 1,04,639 hypertensive patients, demonstrated that its values when obtained by clinical measurement are ~12 mmHg higher than values with 24-h ambulatory measurement, and this study elucidates the importance of analyzing clinical and BP 24-h ambulatory separated in studies that have BP as the main outcome. Our study considers this evidence as the clinical BP was more influenced by the effects of NO3 of the BRJ by the reduction in SBP and DBP, and the values obtained by the clinical measurement were lower compared to the ambulatory 24-h monitoring.
In the sensitivity analysis, we drew attention to observations in two studies included in the clinical measurement subgroup of SBP. The study by Baião et al. (12) had a high standard deviation, probably because of the limited sample of just 5 participants. When that study was omitted from the meta-analysis, a slight difference was noted in the heterogeneity of the “Clinic” subgroup (I2 from 62 to 70%) and the overall analysis (I2 from 67 to 70%), but it did not influence the final result of the meta-analysis on SBP, which decreased to −4.81 mmHg (95% CI: −8.82 to 0.80) in favor of NO3. The study by Kapil et al. (16) revealed a reduction in SBP that differed from other studies, which could be because of the large volume of supplementation (250 mL/day), different from the dose that other studies used (70–14 0mL/day). By withdrawing the study from the meta-analysis, the SBP scores in favor of the intervention decreased to −2.73 mmHg (95% CI: −4.85; −0.61). Statistical heterogeneity (I2) and the test of the difference between subgroups (Chi2) reached 0% and, thus, we reiterate the robustness and data reliability in favor of the intervention. The DBP results did not show alterations in any of the sensitivity analysis scenarios.
The meta-analysis published by Siervo et al. (22) with a mixed sample of healthy and hypertensive patients concluded that NO3 triggered a reduction in SBP of −4.4 mmHg, but DBP did not change significantly. The study's intervention by Siervo et al. (22) differs from our study in that it includes NO3 from BRJ and other sources (e.g., nitrate salts). Despite this, the data corroborated our findings. The meta-analysis by Bahadoran et al. (2), evaluating the effects of BRJ-derived NO3 in a mixed population of patients with and without arterial hypertension, demonstrated a mean reduction of −3.55 mmHg for SBP. Although the study population of Bahadoran et al. (2) differs from ours, the outcome was comparable to our study and similar to that of Siervo et al. (22). In contrast, the study by Bahadoran et al. (2) found a significant decrease in DBP at −1.32 mmHg, while in our metaanalysis and the study by Siervo et al. (22) this result was not achieved.
The studies included in our review had a more extended intervention period when compared to those published in the review by Siervo et al. (22) and hence, the nitrate-rich BRJ may represent an effective strategy for the prevention of cardiovascular complications caused by high blood pressure levels in the short and medium-term. Yet, for BRJ NO3 to be applied as a long-term intervention, RCTs with a duration of >60 days are still needed. The study by Kapil et al. (16), which had the most prolonged duration, with 60 days of intervention and 250 mL of BRJ with NO3, revealed a more significant reduction in SBP and DBP than other studies. The result of this RCT strengthens the data published by Bahadoran et al. (2), in which the intervention of the BRJ with NO3 > 14 days and with a greater volume (>140 mL) tended to reduce SBP and DBP more intensely. Then again, we do not yet know the long-term safety of NO3 use and, consequently, we suggest caution when extrapolating these findings, as we need evidence to prove the long-term safety of NO3 use (25).
The results achieved with this review reinforce the effects of NO3 from BRJ as a vital therapeutic adjuvant for the management and control of arterial hypertension in studies of up to 2 months of intervention. Studies with a prolonged treatment time are still needed to ensure that the NO3 of the BRJ is effective in lowering BP for a long period and, as an alternative, being able to reduce the rates of coronary heart disease, stroke, heart failure, renal failure, and all-cause mortality in hypertensive patients (26).
Bearing in mind that hypertension has a global prevalence, NO3 of the BRJ may have a great contribution to the prevention of complications of arterial hypertension. As a result of its high morbidity, in the USA alone, hypertension is responsible for a cost of US$131 billion per year for its control and complications from the disease (27). It is also imperative to emphasize that adopting nutritional strategies together to control hypertension can enhance the clinical importance of dietary interventions. The diet approach to stop hypertension (DASH), which advocates increased consumption of fruits, vegetables, and low daily fat intake, reduces SBP and DBP by −5.2 mmHg and −2.6 mmHg, respectively (28). Replacing sodium chloride with potassium chloride also has positive contributions in reducing −5 mmHg in SBP and −2 mmHg in DBP (29).
This review is a pioneer in demonstrating the effects of NO3 from the BRJ on BP parameters of an exclusive population of hypertensive patients, along with evaluating clinical and outpatient BP values separately and together. The results are promising and support results already revealed in other meta-analyses commenced on patients with other health features (2, 24).
It should be stated that the included studies had important methodological limitations to be considered. Standardization techniques in clinical and outpatient measurements to obtain BP values were not reported. Clinical trials have a limited number of participants who have different characteristics and conditions (e.g., young and old, taking medication, other chronic diseases). Also, the experimental protocols of the studies have different designs (e.g., crossover, parallel). Despite all these restrictions, we underline that there is no evidence to date to refute the benefits of nitrate-rich BRJ for the cardiovascular health of hypertensive patients.
The aspects identified in this meta-analysis will provide some guidelines for future studies to improve the understanding of nitrate-rich BRJ effects on the cardiovascular health of individuals with hypertension. Since the number of studies with a particular sample of hypertensive patients is still limited, further research is desired to confirm the results achieved in this meta-analysis. A metaregression did not apply due to the small number of studies included in the review. The Cochrane Handbook (8) recommends a minimum number of 10 studies, and we were not able to stratify the effects of specific participants' characteristics (e.g., other morbidities) in the primary studies included in this meta-analysis. Clarifications on the safety of using NO3 chronically are still required to confirm the benefits of NO3 on long-term cardiovascular health. Bearing in mind that the BP values of hypertensive patients are differently influenced by way of measurement in which they are obtained, we suggest that future studies obtain data by the auscultatory (clinical) and ambulatory 24-h monitoring method together. Impending studies may need to analyze the hypotensive effects of other beetroot compounds compared to NO3.
In conclusion, this systematic review with meta-analysis supports that the NO3 of the BRJ is an effective intervention in reducing the SBP of patients with arterial hypertension in interventions of up to 2 months duration.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
CJRB and AP performed conduction of experiments, performed the statistical analysis, wrote introduction, methods, results, and discussion sections. AS and BG improved interpretation analysis and reviewed the manuscript. DG draft the manuscript and improved interpretation analysis and reviewed English Grammar and Spelling. CRBJ and VV supervised the study, draft the manuscript, and gave final approval for the version submitted for publication. All authors contributed to the article and approved the submitted version.
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES) – Finance Code 001.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2022.823039/full#supplementary-material
1. Asgary S, Afshani MR, Sahebkar A, Keshvari M, Taheri M, Jahanian E, et al. Improvement of hypertension, endothelial function and systemic inflammation following short-term supplementation with red beet (Beta vulgaris L.) juice: a randomized crossover pilot study. J Hum Hypertens. (2016) 30:627–32. doi: 10.1038/jhh.2016.34
2. Bahadoran Z, Mirmiran P, Kabir A, Azizi F, Ghasemi A. The nitrate-independent blood pressure-lowering effect of beetroot juice: a systematic review and meta-analysis. Adv Nutr. (2017) 8:830–8. doi: 10.3945/an.117.016717
3. Lewington S, Clarke R, Qizilbash N, Peto R, Collins R, Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. (2002) 360:1903–13. doi: 10.1016/S0140-6736(02)11911-8
4. Remington J, Winters K. Effectiveness of dietary inorganic nitrate for lowering blood pressure in hypertensive adults: a systematic review: a systematic review. JBI Database System Rev Implement Rep. (2019) 17:365–89. doi: 10.11124/JBISRIR-2017-003842
5. Mirmiran P, Houshialsadat Z, Gaeini Z, Bahadoran Z, Azizi F. Functional properties of beetroot (Beta vulgaris) in management of cardio-metabolic diseases. Nutr Metab. (2020) 17:3. doi: 10.1186/s12986-019-0421-0
6. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
7. Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, management of high blood pressure in adults: executive summary: a report of the American college of cardiology/American heart association task force on clinical practice guidelines. J Am Coll Cardiol. (2018) 71:2199–269. doi: 10.1161/HYP.0000000000000075
8. Higgins J, Thomas J. (edsitor). Cochrane Handbook for Systematic Reviews of Interventions. 2nd Edn. Hoboken, NJ: Wiley-Blackwell (2019). doi: 10.1002/9781119536604
9. Carvalho APV, Silva V, Grande AJ. Avaliação do risco de viés de ensaios clínicos randomizados pela ferramenta da colaboração Cochrane. Diagn Tratamento. (2013) 18:38–44.
10. Meader N, King K, Llewellyn A, Norman G, Brown J, Rodgers M, et al. A checklist designed to aid consistency and reproducibility of GRADE assessments: development and pilot validation. Syst Rev. (2014) 3:82. doi: 10.1186/2046-4053-3-82
11. Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. (2002) 21:1539–58. doi: 10.1002/sim.1186
12. Baião D. dos S, d'El-Rei J, Alves G, Fritsch Neves M, Perrone D, et al. Chronic effects of nitrate supplementation with a newly designed beetroot formulation on biochemical and hemodynamic parameters of individuals presenting risk factors for cardiovascular diseases: a pilot study. J Funct Foods. (2019) 58:85–94. doi: 10.1016/j.jff.2019.04.041
13. Bondonno CP, Liu AH, Croft KD, Ward NC, Shinde S, Moodley Y, et al. Absence of an effect of high nitrate intake from beetroot juice on blood pressure in treated hypertensive individuals: a randomized controlled trial. Am J Clin Nutr. (2015) 102:368–75. doi: 10.3945/ajcn.114.101188
14. Broxterman RM, La Salle DT, Zhao J, Reese VR, Richardson RS, Trinity JD. Influence of dietary inorganic nitrate on blood pressure and vascular function in hypertension: prospective implications for adjunctive treatment. J Appl Physiol. (2019) 127:1085–94. doi: 10.1152/japplphysiol.00371.2019
15. Gilchrist M, Winyard PG, Aizawa K, Anning C, Shore A, Benjamin N. Effect of dietary nitrate on blood pressure, endothelial function, and insulin sensitivity in type 2 diabetes. Free Radic Biol Med. (2013) 60:89–97. doi: 10.1016/j.freeradbiomed.2013.01.024
16. Kapil V, Khambata RS, Robertson A, Caulfield MJ, Ahluwalia A. Dietary nitrate provides sustained blood pressure lowering in hypertensive patients: a randomized, phase 2, double-blind, placebo-controlled study. Hypertension. (2015) 65:320–7. doi: 10.1161/HYPERTENSIONAHA.114.04675
17. Kerley CP, Dolan E, James PE, Cormican L. Dietary nitrate lowers ambulatory blood pressure in treated, uncontrolled hypertension: a 7-d, double-blind, randomised, placebo-controlled, cross-over trial. Br J Nutr. (2018) 119:658–63. doi: 10.1017/S0007114518000144
18. Siervo M, Shannon O, Kandhari N, Prabhakar M, Fostier W, Köchl C, et al. Nitrate-rich beetroot juice reduces blood pressure in Tanzanian adults with elevated blood pressure: a double-blind randomized controlled feasibility trial. J Nutr. (2020) 150:2460–8. doi: 10.1093/jn/nxaa170
19. Ashor AW, Chowdhury S, Oggioni C, Qadir O, Brandt K, Ishaq A, et al. Inorganic nitrate supplementation in young and old obese adults does not affect acute glucose and insulin responses but lowers oxidative stress. J Nutr. (2016) 146:2224–32. doi: 10.3945/jn.116.237529
20. Notay K, Incognito AV, Millar PJ. Acute beetroot juice supplementation on sympathetic nerve activity: a randomized, double-blind, placebo-controlled proof-of-concept study. Am J Physiol Heart Circ Physiol. (2017) 313:H59–65. doi: 10.1152/ajpheart.00163.2017
21. Benjamim CJR, S Júnior FW, de Figueirêdo MÍLS, Benjamim CJR, Cavalcante TCF, et al. Beetroot (beta vulgaris L.) extract acutely improves heart rate variability recovery following strength exercise: a randomized, double-blind, placebo-controlled crossover trial-pilot study. J Am Coll Nutr. (2021) 40:307–16. doi: 10.1080/07315724.2020.1774441
22. Siervo M, Lara J, Ogbonmwan I, Mathers JC. Inorganic nitrate and beetroot juice supplementation reduces blood pressure in adults: a systematic review and meta-analysis. J Nutr. (2013) 143:818–26. doi: 10.3945/jn.112.170233
23. Luna RL, Luna LC. Is diastolic pressure losing its clinical usefulness? Arq Bras Cardiol. (2007) 89:e19–21. doi: 10.1590/S0066-782X2007001500010
24. Banegas JR, Ruilope LM, de la Sierra A, Vinyoles E, Gorostidi M, de la Cruz JJ, et al. Clinic versus daytime ambulatory blood pressure difference in hypertensive patients: the impact of age and clinic blood pressure: The impact of age and clinic blood pressure. Hypertension. (2017) 69:211–9. doi: 10.1161/HYPERTENSIONAHA.116.08567
25. Zamani H, de Joode MEJR, Hossein IJ, Henckens NFT, Guggeis MA, Berends JE, et al. The benefits and risks of beetroot juice consumption: a systematic review. Crit Rev Food Sci Nutr. (2021) 61:788–804. doi: 10.1080/10408398.2020.1746629
26. Ettehad D, Emdin CA, Kiran A, Anderson SG, Callender T, Emberson J, et al. Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet. (2016) 387:957–67. doi: 10.1016/S0140-6736(15)01225-8
27. Kirkland EB, Heincelman M, Bishu KG, Schumann SO, Schreiner A, Axon RN, et al. Trends in healthcare expenditures among US adults with hypertension: national estimates, 2003-2014. J Am Heart Assoc. (2018) 7:e008731. doi: 10.1161/JAHA.118.008731
28. Siervo M, Lara J, Chowdhury S, Ashor A, Oggioni C, Mathers JC. Effects of the Dietary Approach to Stop Hypertension (DASH) diet on cardiovascular risk factors: a systematic review and meta-analysis. Br J Nutr. (2015) 113:1–15. doi: 10.1017/S0007114514003341
Keywords: dietary supplementation, Beta vulgaris L., nitrates, nitric oxide, hypertension
Citation: Benjamim CJR, Porto AA, Valenti VE, Sobrinho ACdS, Garner DM, Gualano B and Bueno Júnior CR (2022) Nitrate Derived From Beetroot Juice Lowers Blood Pressure in Patients With Arterial Hypertension: A Systematic Review and Meta-Analysis. Front. Nutr. 9:823039. doi: 10.3389/fnut.2022.823039
Received: 26 November 2021; Accepted: 02 February 2022;
Published: 15 March 2022.
Edited by:
Rakesh C. Kukreja, Virginia Commonwealth University, United StatesReviewed by:
Telmo Pereira, Politécnico de Coimbra, PortugalCopyright © 2022 Benjamim, Porto, Valenti, Sobrinho, Garner, Gualano and Bueno Júnior. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cicero Jonas R. Benjamim, am9uYXNiZW5qYW1pbUB1c3AuYnI=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.