 Sazia Ferdous1†
Sazia Ferdous1† Farah Noshin Chowdhury
Farah Noshin Chowdhury Md. Mostafizur Rahman
Md. Mostafizur Rahman
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Water, 20 October 2022
Sec. Water and Human Health
Volume 4 - 2022 | https://doi.org/10.3389/frwa.2022.950887
This article is part of the Research TopicWorld Water Day 2022: Importance of WASH, Equal Access Opportunities, and WASH Resilience - A Sanitation PerspectiveView all 4 articles
Concerns have been on the rise around the globe regarding better sanitation management, which is one of the basic human rights, owing especially to the present goal of sustainable development, more specifically Sustainable Development Goal (SDG) 6. Proper sanitation management is a challenging issue in Bangladesh. The purpose of this study was to investigate the current state of sanitation and hygiene facilities and management in Chattogram City, Bangladesh. This study was conducted via questionnaire survey, key informant information (KIIs), stakeholder meetings, and field visits. A survey was conducted on slum dwellers and non-slum dwellers (formal settlements) of the city. A total of 400(=n) randomly selected respondents were interviewed (200 from each group) from eight wards of the metropolitan city, six KIIs, and three stakeholder meetings. Field visits were made to observe the conditions along with a pilot survey to validate the questionnaires. A purposive sampling method was employed for this study, while both descriptive and quantitative statistical analyses were conducted. Statistical analysis of the survey results and field observation found inadequate sanitation and hygiene facilities, insufficient community toilets, improper waste disposal, and drainage facilities in the city. Sanitation was worse in slum areas than in the non-slum neighborhoods. 55.4% of slum dwellers had no/little awareness of the sanitary system. While 89% of families in slum areas use shared toilets, unhygienic toilets caused different diseases to 63.7% of respondents. Drainage conditions were almost equally insufficient in both groups. 65% of respondents did not have any community toilets in their locality. The sanitation management system is not well-equipped and it is a pressing need to make better plans and implement sufficient management strategy for the total sanitation of the city.
About 2.3 billion people around the globe lack basic sanitary services. Between 2000 and 2015, the proportion of the worldwide population receiving at least basic sanitation services increased from 59 to 68%. Until 2015, 4.5 billion people in the globe lacked access to a safe sanitation service, in which excreta could be securely disposed of in situ or processed off-site (UN, 2018). The human right to sanitation and water was expressly acknowledged by the United Nations General Assembly, and it is also necessary to accomplish objective six of the Sustainable Development Goals (SDGs) (Hossain et al., 2017). In many regions of the globe, achieving universal access to sufficient as well as equitable sanitation and hygiene by 2030 is a serious concern. Ending open defecation, ensuring that everyone has access to a basic toilet, and putting in place mechanisms for fecal sludge management (FSM) are all part of SDG 6.2. It also emphasizes the significance of personal cleanliness and stresses the need of paying special attention to the requirements of women and girls. The least developed nations had the lowest coverage, with just 27% having basic hand washing facilities. But coverage in urban areas was higher at 39%. Between 2000 and 2015, 892 million individuals were still found to perform open defecation (UN, 2018). In most developing nations, poor sanitation along with hygiene practices are among the main causes of poor health and socioeconomic difficulties, and they constitute a key development stumbling block (Tumwebaze et al., 2013). The manifestation of illness and infections, particularly diarrhea and respiratory tract infections (RTIs), is characterized by poor hygiene and sanitation (WASH) practices (Azupogo et al., 2019). In low-income nations, cholera and typhus remain the leading causes of death among children under the age of five (Escamilla et al., 2013). Improved sanitation is a critical component in preventing sanitary-related gastro-enteric illnesses (Tumwebaze et al., 2013).
In Bangladesh, total sanitation increased by 63%, while open defecation decreased to 3% (World Bank, 2018). Though usually, the sanitation status is much worse in developing countries like Bangladesh where only 57.7% of people in the urban area have access to sanitation facilities (World Bank, 2016). Bangladesh has a population of about 158 million people, making it the world's seventh most populated country. Despite the fact that the country has made significant progress in reducing poverty, a significant part of the population (24.3%) continues to live in poverty, with urban poverty reaching 18.9% (Uddin, 2018). Urbanization in Bangladesh, as in other developing nations, is a rising process that is stable in nature but has a negative impact on urban sustainability. Despite the fact that city governments are worried about the problem, they recurrently fail to solve it owing to uncontrollable and unpredictable rural-to-urban migration, as well as the neglect of the urban poor's sustainable living and access to essential services. Due to a lack of infrastructure services, basic amenities, environmental benefits, etc. the rural poverty problem has virtually been transferred to metropolitan regions (Rana, 2011). In the span of the last three decades, the number of slums in Bangladesh has increased dramatically in tandem with the growth of cities and towns (Sohel Rana, 2009). In Bangladesh, almost 55% of the urban population lives in slums, with intra- and inter-city differences in population size, density, and sanitary conditions (Uddin, 2018). Due to poor sanitation, diarrheal diseases and cholera were found in Bangladesh and untreated drinking water extracted from shallow tube wells could partially contribute to disease propagation (Escamilla et al., 2013). Diarrhea, dysentery, malaria, and dengue fever are examples of water-borne illnesses or diseases linked with contaminated water, inadequate sanitation, and poor food handling procedures (JICA, 2013). Water and sanitation are significant issues in Bangladesh's poverty reduction strategy, and stakeholders and foreign development organizations have paid attention to them (Hossain et al., 2017).
In Chattogram, sanitation is available in 85% of schools and 48% of commercial establishments (World Bank, 2018). Chattogram is Bangladesh's second largest metropolis and the country's major industrial and port city. The city is situated in Bangladesh's south-eastern region, bordering the Bay of Bengal. In the city, there are numerous industrial estates. Chattogram Water Supply and Sewerage Authority is responsible for providing water, sewerage, and drainage services in Chattogram city (CWASA). Due to population expansion and the rise of industrial and commercial activity, the gap between demand and availability of water in the city has widened significantly (JICA, 2013). Chattogram city's population is reportedly around 6.5 million of whom 1.5 million are slum dwellers. The city has a lack of sanitation infrastructures. There are only 36 community toilets accessible to its residents. It is not just the quantity of lavatories that is insufficient; however, the greater part of those is likewise unhygienic and in an incapacitated condition. Additionally, they are not appropriate for everyday use. At present, CWASA has around 75,000 active connections that give direct treated piped water to households. Slum residents in Chattogram, according to new research, are subjected to a wide spectrum of poor, overcrowded, and unsanitary living conditions. Moreover, they have inadequate and insufficient health, sanitation, water, and waste disposal facilities, all of which are stumbling blocks to urban sustainability (Uddin, 2018).
Few studies have looked at the state of WASH practices in Bangladesh, including those in some Chattogram slums (Hanchett et al., 2003; Uddin, 2018). However, these studies were limited in scope. To the best of our knowledge, no extensive study was yet conducted in Bangladesh focusing on the sanitation management of both the slum dwellers and regular residents of any urban area in Bangladesh, not to mention Chattogram city. Therefore, the scope of the present study was to assess the hygiene and sanitation practices among the residents of Chattogram city in Bangladesh by conducting a questionnaire survey while dividing the subject population in regular urban dwellers and slum dwellers, to provide evidence for policy formulation and program planning in addition to creating a strong dataset for future research. First-hand field visits were also made to assess the situation. The study was conducted with the following objectives: (1) to identify the state (strength/weakness) of the sanitation system of Chattogram city and (2) to know the present conditions of community toilets in terms of universal accessibility. The article may contribute to further research on water supply and sanitation study, which will guide those who will work to improve the present situation and may be useful for city managers.
Initially, the idea of a study on the sanitation management of Chattogram city using a questionnaire survey was conceptualized. Then after narrowing down the particular objectives of the study, a combination of a descriptive and analytical cross-sectional study design was made following the selection of the study area. Particular points in the study area were selected for surveying to maintain diversity and also to draw large groups of participants as needed for the study. To achieve the present study objectives, a questionnaire was developed in consultation with the supervisor by considering previous literature, the socio-economic condition, national and international guidelines, and probable survey participants. The survey was conducted from 8 March 2020 to 25 March 2020. A total of 400 research participants completed the survey, which was used for further analysis.
The main study area was Chattogram city in Bangladesh. There are 12 city corporations in Bangladesh. Chattogram City Corporation is one of them. It is divided into 11 thanas: Bakoliya, Bandar, Bayazid, Chandgaon, Double Mooring, Halishahar, Khulshi, Kotwali, Pahartali, Panchlaish, and Patenga. The thanas are subdivided into 41 wards. Eight (08) wards (2, 8, 12 13, 14,15, 16, 23) of the Chattogram City Corporation (CCC) were randomly selected as the study area by the purposive method of random sampling. A list of households (in slum areas) of the selected wards was prepared and equal numbers of households from each slum were selected on the basis of the purposive method of random sampling. Interviews of the non-slum residents (common people) of these wards were also done on the basis of the random sampling principle.
The sample size is the number of completed responses received during the survey that represents part of our target population. To complete this study, random sampling method was utilized where respondents were chosen entirely by chance from the population at large. The sample size was calculated using the following formula:
The sample size formula (Krejcie and Morgan, 1970).
where, N = Population size, Z = Critical value of the normal distribution at the required confidence level, p = Population proportion, e = Margin of error.
n is the sample size which is calculated and determined as 384 based on the following parameters. Z is the Z-value which is 1.96 at a 95% confidence level, e is the confidence interval or margin of error expressed as a decimal (0.05), and p is the population proportion, p = 0.5. In this study, a total of 400 respondents were taken as sample. Sample selection was done using the purposive method of sample selection.
Survey questions and variables were structured by socio-demographic variables, the sanitation situation, and purposive variable. The questionnaire encompassed demographic characteristics (e.g., name, age, gender, profession), sanitation status (e.g., methods of sanitary waste disposal, hand cleaning practice after toilet use, cleaning of toilets, use of cleaning agents, etc.), community toilet status (e.g., availability, usability, hygiene, etc.), and also questions related to personal opinions and awareness (e.g., awareness of sewage disposal, opinion about sanitation status, problems they face, etc.). The data from the sanitation situation questions also captured the sanitation facilities used by the household respondents (shared/private/ community), as well as their perceived cleanliness (very dirty to not dirty at all), the number of households sharing a toilet room, the facilities, and the main problem concerning the cleaning of the shared toilet. Along with the regular question–answer technique, multiple choice options were provided. A random sampling technique was used to select the study subject among the inhabitants of the study area in both study groups. CCC and CWASA were responsible in the questionnaire survey KII (Key Informant Interview).
The data were collected from 400 respondents of mixed ages (aged 10–61 and above) from eight (08) wards (2, 8, 12 13, 14, 15, 16, 23) of Chattogram City Corporation (CCC). Lists of households (in slum areas) of the selected wards were prepared and equal numbers of households from each slum were selected on the basis of purposive random sampling and interviewed. Interviews of the non-slum residents of these same wards (who were also chosen randomly) were done. Individual respondent was taken as the sample unit. The tool for data collection was a pretested semi-structured questionnaire in which research participants were contacted and the questionnaire was conducted physically by face-to-face sessions through the paper-based questionnaire. The questionnaires used differed slightly for two groups of subjects, though there were some comparable traits between the two groups, in which similar questions were used. This was done to optimize data extracted from the two different groups with regard to their individuality and exclusivity of living conditions from each other. In cases where different amenities were available for different groups of people, different questions were asked to optimize findings. They were briefed with an introduction to describe the objectives of the study, as well as ethical issues. An informed and understood verbal consent was taken from the participants of the study. Those individuals who were available after three visits and willing to give verbal consent were included in the study. In cases of interviews of subjects who were minors, this same procedure was followed to obtain consent from them and their parents before commencing. Both field visits and household surveys were conducted. Household heads are interviewed and in the absence of the household head, the second important adult member of the family was interviewed. Data were also collected through non-participatory observation. Though the survey was conducted during the pandemic (COVID) situation, we strictly followed the health and hygienic protocol given by WHO and Bangladesh Govt. to avoid health hazards.
Data collected were reviewed on a daily basis for completeness. Microsoft Excel program was used to analyze and store the data. Statistical analysis was done in the form of; findings from each group were evaluated individually in the form of frequency and percentage. In case of comparable data (between the two groups), p-value was calculated as well. The chi-square test was used to find the p-values, and a significance level of 0.05 was considered while analyzing the data. Finally, all the findings were documented and processed. After processing, all data were analyzed and the final report was prepared.
The demographic information regarding gender, age, and profession of the two groups of people under study were tabulated.
Table 1 shows the socio-demographic information of all respondents regarding gender and age. The analysis revealed that in the total survey a higher participation of female respondents at 52.5% was prevalent, which is about 5% higher than male respondents, as shown in Table 1. From Table 1, we can see a higher response of female respondents from slum people with 60% of the respondents being female respondents and 40% being male respondents. The opposite trend was observed among non-slum dweller respondents with a higher response of males as 55% of the respondents were males, while the number of female participants was 45%.

Table 1. Socio-demographic Information of all respondents regarding gender and age.
In terms of age, 37.85% of respondents were aged 31–40 years, and at least 6.4% were from both age groups 10–20 and above 61. While 30.60% were aged 41–60 years and 22.65% were aged between 21 and 30 years. A similar age trend was found in both study groups.
The profession of the non-slum dwellers was taken into account during the survey as shown in Figure 1. With regards to occupational status, the analysis revealed that 29.5% were service holders, 12.5% were housewives, 9.5% were students, and others were from different professions, including businessmen, bankers, daily laborer, doctors, government service holder, NGO worker, rickshaw puller, shopkeeper, and teachers. However, in case of both groups of respondents, purposive random sampling was used. This may be sometimes considered a limitation of the study as there comes a possibility of bias in choosing respondents.
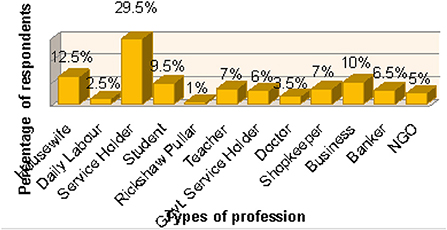
Figure 1. Profession of non-slum dweller questionnaire respondents.
Slum dwellers' living circumstances are typically unhealthy since there is always a high density of inhabitants in slum regions and because they are impoverished. There were just a few latrines available for a huge number of slum inhabitants. The majority of the homes had unsanitary latrines. Slum residents utilize a variety of toilets, whose photographs are shown in Figure 2 and are discussed in the following discussion. Figure 2 compiles photographs of four types of latrines used in these slum areas as A, B, C, and D sub-pictures.
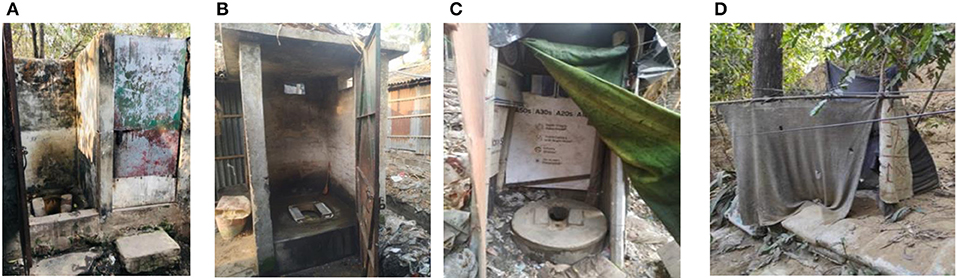
Figure 2. Toilet facilities in slum areas. (A) Pit latrine without slab, (B) pit latrine with slab, (C) hanging toilets, (D) open field toilet.
A typical pit latrine is a hole in the ground with no covering. To keep the pit from collapsing, it may be lined entirely or partly. These types of latrines are considered to be of poor quality generally, with more than 50% structurally unsafe and 50% unhygienic. This sort of toilet typically emits foul odors and is susceptible to insect infestation. Pit latrines are the simplest dry latrine to construct. They are just a hole excavated in the earth with a cover slab or floor over it (Figure 2B) To be deemed upgraded sanitation systems, pit latrines should include a cleanable cover slab. Hanging latrines in slums were traditionally made of corrugated metal and bamboo constructions strung from poles above the ground, allowing excrement to flow straight down into the mud and garbage soup in Figure 2C. During monsoons, residents recall rooms being flooded with stinky mud, followed by epidemics of diarrhea and fever. Open defecation is the act of cleaning one's insides in the open without the use of toilets or other properly designed buildings for the disposal of human waste. Open defecation is primarily associated with rural and impoverished areas of the world, notably in Sub-Saharan Africa and Asia. Defecating in the open is a human habit. People utilize forests, fields, shrubs, open bodies of water, and other open spaces instead of toilets (Figure 2D). When sanitary infrastructure is unavailable, this is a common practice.
Toilets that are solely used by one home or members of the same family are known as private toilets. Toilets that are open to the public are known as community toilets. Shared toilets are toilets that are shared by many households that are often acquainted or share a compound residence.
From field observations, it was seen that almost all the non-slum dwellers used standard low or high commode sanitation systems. While the community toilets were found mostly to be low commode systems and double slab pit latrines alternatively.
Tables 2, 3 show that the majority of slum households (58.9%) use pit toilets with slabs. The pit toilet without a slab is used by 28.8% of the population. 15.3% of people use an open-air hanging toilet. Still, 4% of people use the open field as their toilets in slum areas. Eighty-nine percent of respondents use toilets which are shared by different households. 32.5% (10–20 people) use one shared toilet, which is not hygienic. Nine percent households use private toilet and 2% households use community toilet. The median number of households sharing each toilet room was three (range, minimum 10, and maximum 100). Seventy-seven percent of them responded that they do not have any separate toilets for men and women. Forty-eight percent of respondents use toilets which are enough clean to use but 3% of respondents use very dirty/ not usable toilets. The average percentage of cleanness of slum household toilets 48% of respondents use the toilet, which is clean enough to use. Thirty-six percent of respondents use the toilet which is neither clean nor dirty. Ten percent of respondents use a dirty but usable toilet. Three percent of respondents use the very dirty/ not usable toilet. The rest 3% of respondents use the very clean toilet though their toilets are private. Using those types of toilets, they face different types of problems, such as diseases-associated symptoms like diarrhea, and skin irritations being more frequent (63.7%) in slum areas. 34.8% do not have any permanent toilet structure. 20.4% of people are using toilets that are established in a risky situation and not safe. Safe disposal of excreta is much important for the environment. The study also showed that only 44.6% of people in the slum have some idea about the sanitation system, and the rest 55.4% do not have any idea about the sanitation system. Though about 48.5% population of slums find their toilet clean enough to use, about 49% of the population do not think that their toilets are satisfactorily clean.
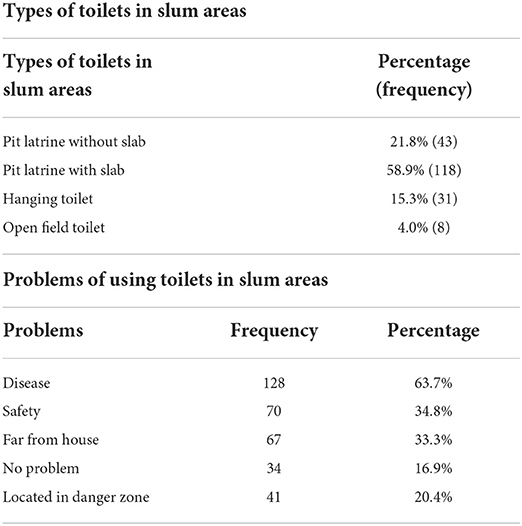
Table 2. Types of toilets and problems of using toilets in slum areas.

Table 3. Slum areas toilet facilities.
For the betterment of analysis, all slum dwellers were divided into seven groups (A, B, C, D, E, F, and G; e.g., A < 10 means less than 10 people share a toilet). This use of slum dwellers' shared toilets is shown in Figure 3. From Figure 3, the percentage of A group is (13.20%). Among them, B group (10–20 people) mostly use one shared toilet which is 32.50%. In group G, 0.5% (near about 100 people) use one shared toilet. In group C, 26.40% (21–30 people) use one shared toilet. In group D, 18.80% (31–40 people) use one shared toilet. In group E, 6.10% (41–50) people) use one shared toilet and in group F, 2.50% (>50) people) use one shared toilet.
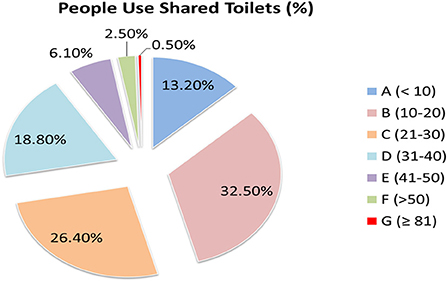
Figure 3. Slum dwellers' use of shared toilets.
These findings match with those of another study that was carried out on slum dwellers in Chattogram city, which found that 41.25% of households are users of pit latrines. Furthermore, a significant proportion of the population, 10%, disposed of excreta in open space/hanging places. It should be noted that the majority of the households shared one bathroom with several families. According to the findings, 76.25% of respondents shared one restroom with 7–9 families. Furthermore, 20% of respondents stated that they share one restroom with four to six households. Furthermore, there are 10–12 households that share a toilet. It is also worth mentioning that, they noticed that during the rainy season, human waste is washed into bodies of water, resulting in the spread of viral and infectious illnesses in slum regions (Uddin, 2018). This finding becomes very concerning as the sanitary conditions, in this case, are very similar to our findings. A study in Lagos, Nigeria has also found deprived condition in slum areas in case of water, sanitation, and hygiene, including waterlogging and waste disposal conditions (Akoteyon et al., 2021). As we can see from our study, the overall condition of these sectors in Chittagong is also unsatisfactory. Thus, an overall poor sanitation condition was identified that may interfere to achieve the SDGs 6 target in the city. Another study on different slums of Dhaka city found living conditions to be unhygienic in terms of their WASH condition (Dana, 2011). Moreover, it can be argued that the hygiene situation in the slums of Dhaka city and Chattogram in our study is somewhat similar.
From Table 4, most of the people, about 49.2%, do not have any idea about sanitary waste disposal methods and 32.2 % are not sure and did not know which one is perfect for sanitary waste disposal methods. 18.6% of respondents have knowledge about sanitary waste disposal methods. Moreover, 71% have no idea about sewerage treatment plant (STP). Yet, the willingness for better sanitation is noticed. As a result, 74% of respondents recommended/motivated their friends/relatives/neighbors to use proper sanitation and hygiene system. Unfortunately, the majority, ~86% believe that their area's total drainage and sanitation system is not perfect.
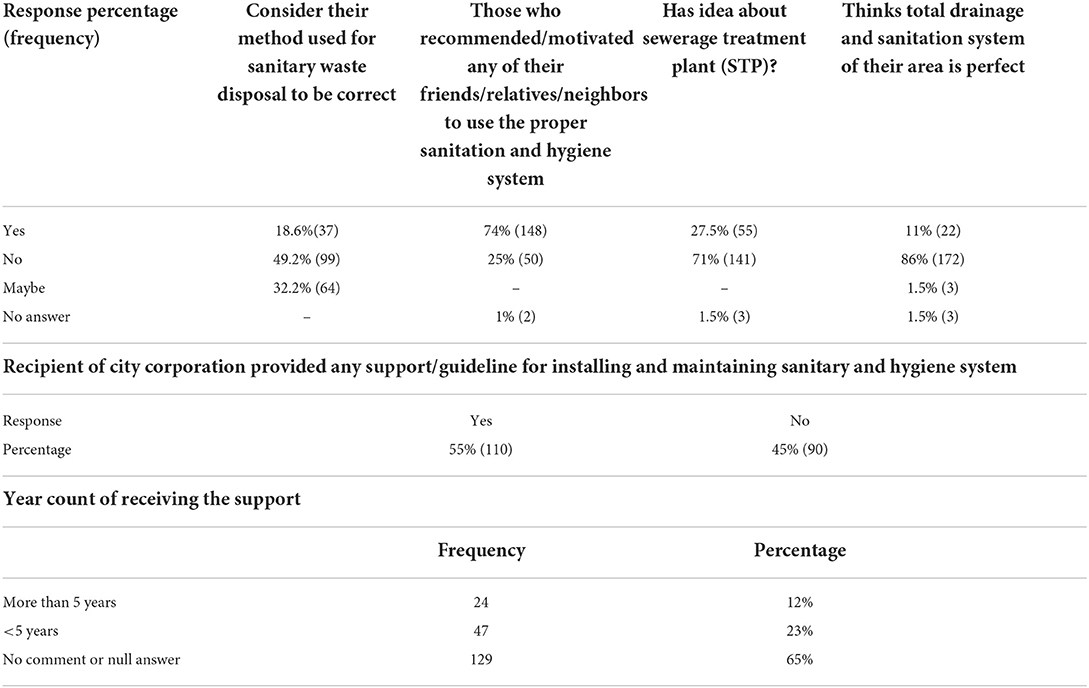
Table 4. Status of sanitation for non-slum dwellers.
Fifty-five percent of participants exerted that they have been the recipients of city corporation provided support/guidelines for installing and maintaining sanitary and hygiene systems. Yet most of them have only been receiving the support for < 5 years, which is 23%. Twelve percent have been receiving the support for more than 5 years. The rest of the receivers were unable to provide a time frame. The conditions of urban WASH are reflected in these data. Another global study has shown that the conditions of urban sanitation and WASH are far from the ideal condition they are in now and at the present rate of development, the situations will take a long time to take place (Hawkins et al., 2013).
A comparative approach was undertaken in our research on slum dwellers' and non-slum dweller participants' sanitation management. Methods of sanitary waste disposal and drainage condition in subject areas for both study groups are shown in Table 5. This comparison is further described in the following discussion.
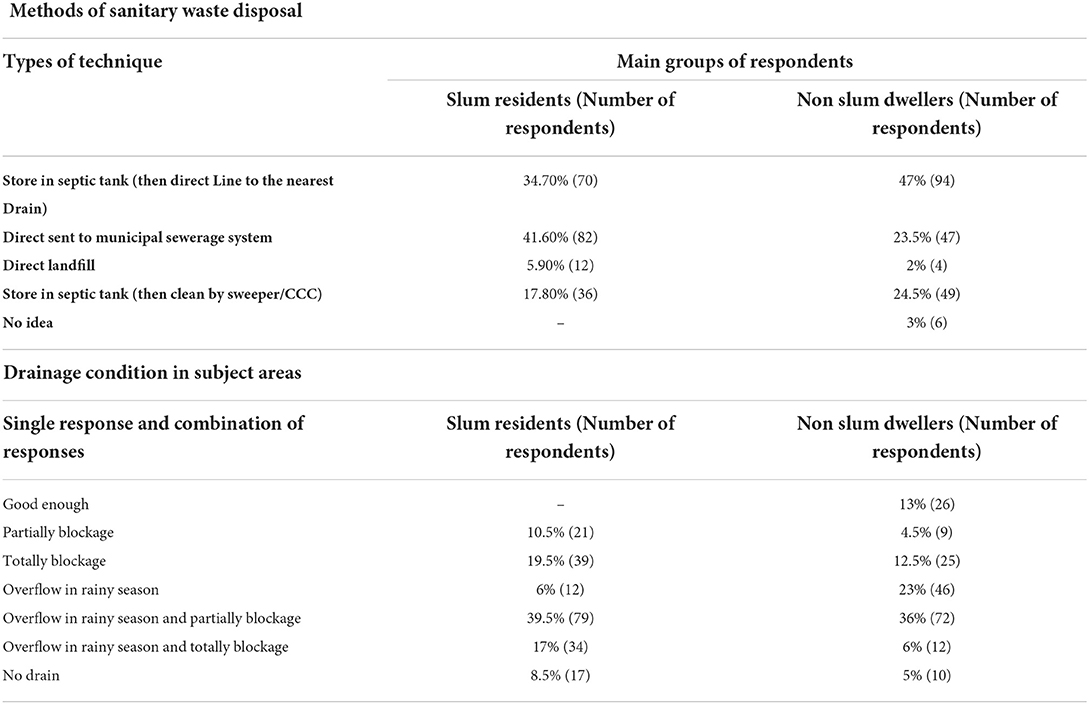
Table 5. Methods of sanitary waste disposal and drainage condition in subject areas for both study groups.
Chattogram City Corporation does not have a proper sanitation disposal method. Among non-slum dweller residents, 47% use septic tanks but their sanitary waste sends to the nearest drain. 23.5% of respondents responded that they do not have any septic tank and their sanitary waste direct send to the municipal sewerage system. This process is quite unhealthy and imposes negative effects on the environment. 24.5% of respondents responded that their sanitary wastes are stored in the septic tank and then cleaned by a sweeper/CCC). Three percent of respondents who rent in different buildings have no idea about sanitary waste disposal methods. Two percent use direct landfill for waste disposal. In slum areas, people are less concerned about sanitary waste disposal methods. Most of the people (41.60%) do not have any septic tank and their sanitary waste is directly sent to the nearest drain. 34.7% of respondents responded that their sanitary waste was stored in the septic tank (than a direct line to the nearest drain). 17.80% use a septic tank and are cleaned by a sweeper. 5.90% use direct landfill for waste disposal.
In both cases, the least number of people used the direct landfill method (2 and 5.90%). Non-slum dweller residents use septic tanks 47% of the time, while slum dwellers use municipal sewage systems 41.60% of the time. The p-value obtained by performing a chi-square test on the methods of sanitary waste disposal by the respondents in Table 5 yielded a value of 0.000005 which shows a value of high statistical significance. Here a value of 0.05 was considered the level of significance.
39.5% of respondents from slum areas and 36% from non-slum dweller residents responded that their nearest drains are not only partially blocked but also overflow during the rainy season. The scenario is very common all over the city. Chattogram city seems to have an insufficient and unplanned drainage system. This sort of advancement is leaving an awful impact on the environment. The residents of various areas of Chattogram including slum areas know about the issue of waterlogging during the rainy season. A moderate to heavy rainfall is sufficient to immerse principal streets, paths, and by-paths of both old and new pieces of the city
The study found that drainage conditions are almost the same in slum areas and non-slum dweller resident areas. 39.5% responds from slum areas and 36% from non-slum dweller residents said that their nearest drains are partially blocked and overflowed during the rainy season. 19.5% of respondents from slum areas and 12.5% from non-slum dweller residents' response that their nearest drains are totally blocked especially during the dry season. Seventeen percent of respondents from slum areas and 6% of respondents from non-slum dweller residents responded that their nearest drains are totally blocked and overflowed during the rainy season. 10.5% of respondents from slum areas and 4.5% from non-slum dweller residents' response that their nearest drains are partially blocked. 6% of respondents from slum areas and 23% from non-slum dweller residents' response that their nearest drains are fine but overflow during the rainy season. 8.5% of respondents from slum areas and 5% from non-slum dweller residents' response that they do not have any drain nearest them. Only 13% responded that their nearest drain is good enough. This is a very small part of even the non-slum dweller resident's population. The p-value obtained by performing a chi-square test on the drainage conditions according to the respondents in Table 5 yielded a value of 3 × 10−11 which is a statistical value of high significance. A level of significance of 0.05 was considered in this test.
Hand and toilet cleaning habits, practices, and facilities in both study groups are shown in Table 6. These findings are elaborated in the following discussion.
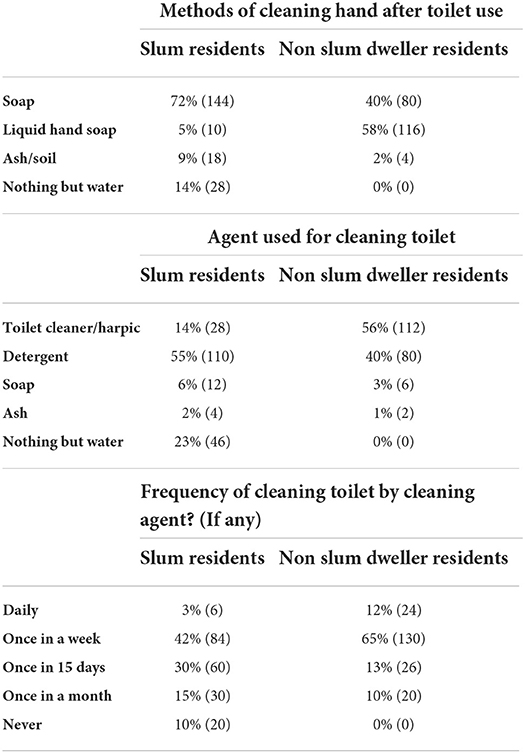
Table 6. Hand and toilet cleaning habits, practices, and facilities in both study groups.
Hygiene practices are not very common in slum areas, sometimes they try to maintain hygiene but most of the time they cannot afford to maintain it due to their poverty. Large number of, 72%, of people use soap to clean their hands. Still 14% of people use nothing but water to clean their hands after using the toilet. They explain that they do not have much money to buy a soap or cleaning agent. Nine percent of them use ash/soil to clean their hands. Only 5% of people use hand wash to clean their hands.
In non-slum dweller residents, though sanitary waste disposal methods of common people are unhealthy but they maintain hygiene. They are concerned to clean their toilet and hands. Non-slum dweller residents are aware of cleaning their hands after using the toilet. Fifty-eight percent of people use liquid hand soap to clean their hands. Forty percent of people use soap to clean their hands. The rest 2% of them use ash/soil to clean their hands. No one uses only water to clean their hands.
These findings seem to show a rather improved practice as globally nearly two-thirds of the population in least developed countries (LDCs) does not have access to soap and water for hand washing at home (UN-Water, 2021).
Non-slum dweller residents are concerned about sanitation and hygiene. In the Table 6 we can see that 65% people clean their toilet by cleaning agent once in a week. Thirteen percent of people clean their toilet with a cleaning agent once in 15 days. Twelve percent of people clean their toilet with a cleaning agent on daily basis. Ten percent of people clean their toilets two times a week. According to the above information, we can say that sanitary waste disposal methods of common people are poor but they maintain hygiene. Fifty-six of people use a cleaning agent/toilet cleaner to clean their toilets. The second most 40% of people use detergent to clean their toilets. Three percent of people use soap to clean their toilet. The rest 2% of the people use ash to clean their toilets.
Hygiene practice is not very common in slum areas. Forty-two percent of people clean their toilet with a cleaning agent once a week, whereas 10% of people never use any cleaning agent. Thirty percent of people clean their toilets with a cleaning agent once in 15 days. Fifteen percent people clean their toilet with a cleaning agent once a month. Only 3% of people clean their toilet two times a week. Moreover, 55% of people use detergent to clean their toilets, and 23% of people use nothing but water to clean their toilets. Fourteen percent of people use a cleaning agent/bleaching powder to clean their toilet. Six percent of people use soap and the rest 2% of people use ash to clean their toilets.
Community toilets are usually separated into male and female facilities, although some are unisex, particularly for little or single-inhabitance community toilets. Progressively, community toilets are open to individuals with handicaps. Some community toilets are for nothing while others charge an expense. In the last case, they are likewise called pay toilets and here and there have a charging turnstile.
Community toilet facilities for both study groups are shown in Table 7. According to Table 7, the numbers of community toilets are not sufficient for the city dwellers. Only 35% of respondents reported they have the facility of community toilets in their locality which is not sufficient for them. Only 15% maintain cleanness and hygiene and most of them are modern toilets. Eighty-eight percent of people reported that they do not have a community toilet that is friendly for women/children/ handicapped people. Most of the other toilets are poorly maintained and there are low facilities for children and women. Community toilets are payable that should be free of charge.

Table 7. Community toilet facilities for both study groups.
Though Chattogram's water supply has improved, the city still lacks sanitary infrastructure, since it is not connected to any type of sewage system or adequate stormwater drainage system. As a result, the majority of the population relies on septic tanks along with pour-flush sanitation systems. Generally, septic tank effluent disposal is anomalous, and septic sludge is not retrieved on a routine basis. It lacks sludge treatment capabilities. As a result, both residential and industrial pollutants are dumped into open bodies of water, posing environmental risks. CWASA has created a comprehensive sanitation development strategy with the World Bank's help and a master plan to put the city under a planned sanitation system. The proposed sewerage investments program aims to gradually bring the entire city population under a modern sewage system (2017–2065) (Bank, 2020).
Strengthening local as well as national authorities' capability to administer and control sanitation systems, including the creation of information management systems, should be a top priority. Participation of a variety of stakeholders, including local people, is also required for effective and sustainable water and sanitation management. To give these groups a “voice,” more precise monitoring is required, in accordance with Target 6.b of SDG that states Support stakeholder participation (UN, 2018). As a result, it is imperative to have the residents' perspective on a city's hygienic conditions in order to get a true image of the city's sanitation management situation.
The strength of the sanitation system
1) Chattogram WASA is developing a master plan which would be the strength of the development of Chattogram City Corporation's sanitation and hygiene conditions.
2) Seven modern community toilets are built for city dwellers.
The weakness of the sanitation system
1) The sanitation and hygiene condition of Chattogram City Corporation is very poor, especially in slum areas.
2) Inadequate personal hygiene practices and facilities.
3) Unhealthy sanitary waste disposal methods are being practiced by city's dwellers which is very harmful to environment and community health.
4) The number of community toilets is not sufficient and most of them are poorly maintained without universal accessibility.
5) Drainage conditions are good in Chattogram, which destroys the urban stormwater discharge with resultant waterlogging of the city.
Stakeholders must take several steps in order to achieve pleasant odor and clean environments owing to adequate sanitation. According to reports from the Chattogram City Corporation, there are 36 community restrooms. Five of them have been closed due to a lack of available leases. People do not utilize them since they are not in a convenient location, and no one is interested in leasing them. In order to address the issues, Chattogram City Corporation allied with Water Aid Bangladesh and Dushtha Shasthya Kendra (DSK). Seven freshly constructed contemporary community restrooms have been opened. As compared to the 36 total community restrooms in CCC, only seven are in good shape and well-maintained. Special need personnel-friendly areas, separate chambers for males and females, locker room, hand washing area, shower, and safe drinking water facility, 24 × 7 power, CCTV camera availability, expert cleaners, and female caretakers were all included in the design of the contemporary community restrooms. However, for 65 lakh individuals, this number is insufficient. The majority of the other restrooms are in poor condition, with limited facilities for children and women. Toilets in public places should be free of charge. A community toilet can give considerably more than access to the toilet for urination and feces as an “away-from-home” toilet room. People also wash their hands, groom themselves in the mirrors, obtain drinking water (e.g., refilling water bottles), attend to menstrual hygiene needs, and dispose of trash. As a result, having a community toilet in the neighborhood is critical; in my survey, 65% of respondents said their neighborhood lacked one. Only 35% of people said they have access to a community toilet (Table 7). It is critical to have enough community restrooms in the area. According to the statistics, 9% of respondents believe that using a community restroom is adequate. Ninety-one percent of respondents said that community restrooms are insufficient for city inhabitants. We discovered that 85% of the general populace is filthy and unsanitary. Only 15% of the toilets are kept clean and sanitary, and the majority of them are contemporary toilets. Going to the bathroom is a basic human requirement. Many individuals, particularly women and girls, are unable to use the restroom when and when they require it. It is important to have a community bathroom in the city that is user-friendly for women, children, and people with disabilities. Eighty-eight of individuals said they do not have access to a community toilet, which is a serious problem.
1. Stakeholders need to educate themselves on the necessity of hygiene and sanitation.
2. They need to learn and propagate the knowledge that, sustainable sanitation practices will only benefit them in the long run, from health to environmental aesthetics.
3. People need to make provisions and awareness about washing hands properly with soap.
4. Cleaning the toilet regularly with cleaners for healthy use of washrooms.
5. Making provisions for better user-friendly community toilet facilities for women, children, and elderly.
6. Taking people with special needs into consideration while constructing toilets.
7. Introduction of healthier sanitary waste disposal method.
8. Providing more administrative support in case of sanitation facilities. Especially for slum dwellers.
9. Constructing drains with a proper plan. Especially in the area that regularly faces waterlogging.
10. Creating awareness about keeping the drain as unclogged and running as possible.
11. Strengthening local authorities' capacity to administer and control sanitation systems, including the creation of information management systems, should be a priority.
12. Participation of a variety of stakeholders including the local people of Chattogram is required for effective and sustainable water and sanitation management.
The result of this study shows that the overall sanitation and hygiene condition of Chattogram City Corporation is largely inadequate. The overall situation maps out to be worse for slum dwellers. Most of them were unaware of sanitation management systems, and shared unclean, unhealthy toilets. Non-slum dwellers had access to moderately clean toilets and hygiene, as well as some kind of waste disposal assistance from the authorities. However, in either group of respondents, an insufficiency of available community toilets and water drainage systems in the area was found. Our thorough field observation also supports this result. A holistic and sustainable approach including all classes of people for the proper sanitation management and drainage in Chattogram city is in urgent need of being devised and deployed.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics review and approval/written informed consent was not required as per local legislation and institutional requirements.
SF: conceptualization, field data collection, data analysis, and manuscript draft. FC: field data collection, data analysis, and manuscript draft. MA: interpretation and manuscript preparation. MB-D: data analysis and manuscript preparation. MR: conceptualization, data analysis, manuscript draft, and overall supervision. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frwa.2022.950887/full#supplementary-material
Akoteyon, I. S., Aliu, I. R., and Soladoye, O. (2021). Household levels of deprivation to wash and residential conditions in slum settlements of Lagos, Nigeria. J. Water Sanit. Hyg. Dev. 11, 60–74. doi: 10.2166/washdev.2020.157
Azupogo, F., Abdul-Rahaman, F., Gyanteh, B., and Atosona, A. (2019). Hygiene and sanitation practices and the risk of morbidity among children 6–23 months of age in Kumbungu District, Ghana. Adv. Public Health 2019, 1–12. doi: 10.1155/2019/4313759
Dana, T. (2011). Unhygienic living conditions and health problems: a study in selected slums of Dhaka City (December 30, 2011.). OIDA Int. J. Sustai. Dev. 2, 27–34
Escamilla, V., Knappett, P. S. K., Yunus, M., Streatfield, P. K., and Emch, M. (2013). Influence of latrine proximity and type on tubewell water quality and diarrheal disease in Bangladesh. Ann. Am. Assoc. Geogr. 103, 299–308. doi: 10.1080/00045608.2013.756257
Hanchett, S., Akhter, S., Khan, M. H., Mezulianik, S., and Blagbrough, V. (2003). Water, sanitation and hygiene in Bangladeshi slums: an evaluation of the wateraid-Bangladesh urban programme. Environ. Urban. 15, 43–56. doi: 10.1177/095624780301500219
Hawkins, P., Blackett, I., and Heymans, C. (2013). Poor-Inclusive Urban Sanitation : An Overview. Poor-Inclusive Urban Sanitation : An Overview. Available online at: http://hdl.handle.net/10986/17385 (accessed January 20, 2022).
Hossain, S. M., Ara, U., Huq, S., Hossain, M. M., Ibne Mahmud, A. I., Isalm, K. R., et al. (2017). Kap study on hygiene and sanitation in a selected rural area of Bangladesh. Proc. Int. Conf. Public Health 13, 01–112. doi: 10.17501/icoph.2017.3111
JICA (2013). Preparatory Survey on Integrated Water Supply Project in the Democratic Socialist Recommunity of March, 13−41. doi: 10.1201/b14894-3
Krejcie, R. V., and Morgan, D. (1970). Small-samlpe techniques. NEA Res. Bull. 30, 607–610. doi: 10.1177/001316447003000308
Rana, M. M. P. (2011). Urbanization and sustainability: challenges and strategies for sustainable urban development in Bangladesh. Environ. Dev. Sustain. 13, 237–256. doi: 10.1007/s10668-010-9258-4
Sohel Rana, M. D. (2009). Status of water use sanitation and hygienic condition of urban slums: a study on Rupsha Ferighat slum, Khulna. Desalination 246, 322–328. doi: 10.1016/j.desal.2008.04.052
Tumwebaze, I. K., Orach, C. G., Niwagaba, C., Luthi, C., and Mosler, H. J. (2013). Sanitation facilities in Kampala slums, Uganda: users' satisfaction and determinant factors. Int. J. Environ. Health Res. 23, 191–204. doi: 10.1080/09603123.2012.713095
Uddin, N. (2018). Assessing urban sustainability of slum settlements in Bangladesh: evidence from Chittagong city. J. Urban Manag. 7, 32–42. doi: 10.1016/j.jum.2018.03.002
UN (2018). SDG6 Synthesis Report 2018. United Nations. Available online at: https://www.unwater.org/communityation_categories/sdg-6-synthesis-report-2018-on-water-and-sanitation/ (accessed January 20, 2022).
UN-Water (2021). Summary progress update 2021 : SDG 6 — water and sanitation for all. UN-Water Integrated Monitoring Initiative, 1–58. Available online at: https://www.unwater.org/new-data-on-global-progress-towards-ensuring-water-and-sanitation-for-all-by-2030/ (accessed January 20, 2022).
World Bank (2016). Word Development Iindicators 2016-SDG-Booklet. World Bank Publications. Available online at: http://databank.worldbank.org/data/download/site-content/wdi-2016-highlights-featuring-sdgs-booklet.pdf (accessed January 20, 2022).
Keywords: sanitation, Chattogram, drainage system, hygiene practice, SDG 6
Citation: Ferdous S, Chowdhury FN, Ali ML, Bodrud-Doza M and Rahman MM (2022) Assessment of urban sanitation status and management gaps in a metropolitan city, Bangladesh: Potential challenges to achieve SDG 6. Front. Water 4:950887. doi: 10.3389/frwa.2022.950887
Received: 23 May 2022; Accepted: 12 September 2022;
Published: 20 October 2022.
Edited by:
Carla Muñoz-Antoli, University of Valencia, SpainReviewed by:
Javier Sotillo, Instituto de Salud Carlos III (ISCIII), SpainCopyright © 2022 Ferdous, Chowdhury, Ali, Bodrud-Doza and Rahman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Md. Mostafizur Rahman, cmFobWFubW1AanVuaXYuZWR1
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.