 Wesley Yip
Wesley Yip Andrew B. Chen
Andrew B. Chen Michael F. Basin
Michael F. Basin Giovanni E. Cacciamani
Giovanni E. Cacciamani
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Urol. , 13 September 2022
Sec. Urologic Oncology
Volume 2 - 2022 | https://doi.org/10.3389/fruro.2022.934550
This article is part of the Research Topic Global Disparities in Genitourinary Cancers View all 4 articles
Introduction: Sociodemographic factors have been shown to have significant impacts on bladder cancer (BC) outcomes, but there are conflicting data in the literature regarding certain non-modifiable factors. We sought to determine the effect of sociodemographic factors on survival outcomes after radical cystectomy (RC) for BC.
Materials and methods: A systematic review of population-based cohort studies published before March 2020 from Surveillance, Epidemiology, and End Results (SEER) and National Cancer Database (NCDB) was performed per Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines by searching PubMed®, Scopus®, and Web of Science®. All full-text English-language articles assessing the impact of sociodemographic factors on BC survival after RC were obtained. Two investigators (WY and AC) independently screened all articles. Discrepancies were resolved by consensus. All studies reporting survival outcomes after RC based on any of the sociodemographic factors were included, except for systematic reviews, which were excluded. Primary end points were overall survival (OS) and disease-specific survival (DSS) after RC. Cohort studies reporting Cox proportional hazards or logistic regression analysis were independently screened. Available multivariable hazard ratios (HRs) were included in the quantitative analysis.
Results: Our search returned 147 studies, of which 14 studies (11 SEER and 3 NCDB) were included for cumulative analysis. Only race and gender were evaluable due to heterogeneity of other factors. Compared to White patients, Black patients have worse OS [HR 0.83; 95% confidence intervals (CIs) 0.75, 0.92; p < 0.01; I2 = 79%] and DSS (HR 0.83; 95% CI 0.69, 1.00; p = 0.05; I2 = 69%), Asian patients have worse OS (HR 0.84; 95% CI 0.77, 0.92; p < 0.01; I2 = 15%) but not DSS (HR 0.81; 95% CI 0.31, 2.10; p = 0.66), Hispanic patients have no difference in OS (HR 1.03; 95% CI 0.79, 1.34; p = 0.66; I2 = 72%) or DSS (HR 2.63; 95% CI 0.34, 20.34; p = 0.35), and Native American patients have no difference in OS (HR 2.16; 95% CI 0.80, 5.83; p = 0.13). Compared to men, women have no difference in OS (HR 1.03; 95% CI 0.93, 1.15; p = 0.53; I2 = 92%) nor DSS (HR 0.99; 95% CI 0.90, 1.08; p = 0.78; I2 = 1%).
Conclusions: Disparate BC survival outcomes after RC are present, with Black patients having poorer OS and DSS as compared to White patients. Asian patients have lower OS but not DSS. Survival outcomes do not appear to differentiate by gender. Significant heterogeneity in variable and outcome definitions limited our ability to perform meta-analyses involving other potentially important drivers and sources of disparate outcomes.
Bladder cancer (BC) is the second most common genitourinary cancer in the United States with an estimated 81,400 new cases and 17,980 deaths due to the disease in 2020 (1). Radical cystectomy (RC) for BC remains the gold standard treatment for muscle-invasive and select non–muscle-invasive disease (2). Muscle-invasive BC (MIBC) is a disease with high lethality; even with aggressive multimodal therapy, up to 50% of these patients will develop metastatic disease (3). There are several known surgical and pathological factors associated with improved survival outcomes following RC, including the performance of a lymph node dissection (4), expeditious time to surgery (5), reception of neoadjuvant chemotherapy (6), lower pathologic stage (7), lack of lymphovascular invasion (8), pathologic downstaging (9), and the absence of smoking (10).
Sociodemographic factors have been shown to have significant impacts on BC outcomes, but there are conflicting data in the literature in regard to certain non-modifiable factors. Several large database reviews have reported worse survival outcomes in Black patients compared to White patients with BC, which may be due to delays in diagnosis and treatment (11), although discrepant survival outcomes still exist in those who have undergone RC (12). Female gender has portended inferior oncologic outcomes following RC in some, but not all, major studies (13, 14). Similarly, marital status has been found to have a protective effect after RC in some studies, but no association in another (15–17). Socioeconomic and educational status has been explored in several studies, typically indicating increased risks of advanced disease at presentation (18) but with unclear effects on survival outcomes following RC (11, 19). As such, a systematic review of available studies reporting survival outcomes among BC patients after RC was conducted, followed by a cumulative meta-analysis stratified by sociodemographic factors in order to increase clarity about these potential sources of disparities in BC survival outcomes.
Our research question was designed utilizing the PICOS framework as follows. Population: BC patients. Intervention: RC. Comparison: sociodemographic factors. Outcome: survival. Study designs: population-based cohort studies from administrative databases. We systematically searched the PubMed®, Scopus®, and Web of Science® databases according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines for population-based cohort studies from the Surveillance, Epidemiology, and End Results (SEER) Program and National Cancer Database (NCDB) published before 1 March 2020. All full-text English-language articles assessing the impact of sociodemographic factors on BC survival after RC were obtained by using the search terms bladder cancer, urothelial cancer, radical cystectomy, survival, mortality, gender, sex, women, men, race, marital, marriage, insurance, socioeconomic, sociodemographic, social, SEER, and/or NCDB, in combined strings modified accordingly to each database. The review was not registered, but a protocol can be provided upon request.
Two investigators (WY and AC) independently screened all articles, focusing on cohort studies reporting Cox proportional hazards regression or logistic regression analyses in BC patients after RC. Any disagreements about eligibility were resolved by two senior investigators (GC and SB) until a consensus was reached. All studies reporting survival outcomes after RC based on any of the sociodemographic factors were included, except for systematic reviews, which were excluded.
Primary end points were overall survival (OS) and disease-specific survival (DSS) after RC. Available multivariable hazard ratios (HRs) and corresponding 95% confidence intervals (CIs) were extracted for the quantitative analysis.
A cumulative meta-analysis of the studies was conducted using Review Manager® 5.3 (Cochrane-Collaboration, Oxford, UK) as follows. The HRs and 95% CIs extracted from the multivariable analysis of the eligible studies were pooled for long-term outcomes (survival analysis) as described previously (20). An HR > 1 represented a survival benefit. For studies in which an HR and the standard error (SE) or corresponding 95% CI was not available, we estimated it using the log-rank p-value, number of participants, events, or survival curves available (21). When a study reported the overall mortality (OM) and/or disease-specific mortality (DSM), the outcomes were converted to OS and DSS, respectively (22).
Random and fixed effects (DerSimonian and Laird) were used in case of the presence or absence of heterogeneity, respectively. Heterogeneity was considered not statistically significant when the Cochrane Q-test p-value was >0.1. A transformation of Q-test, the I2 statistic (I2 = 100% × (Q-df)/Q), was used to estimate the consistency of the effect sizes. In case of heterogeneity, the cumulative analysis was performed applying the random effects model. An I2 value of <30% was defined to denote low heterogeneity, a value between 30% and 50% was defined as moderate heterogeneity, and a value of >50% was defined as high heterogeneity (22). An evaluation of publication bias was not performed. A two-sided p-value < 0.05 was considered statistically significant.
Our initial electronic search identified a total of 317 studies, which was decreased to 147 studies after duplicates were removed. After a detailed review by two separate reviewers (WY and AC), 71 studies (54 SEER and 17 NCDB) were selected to report survival outcomes after RC based on sociodemographic factors (Figure 1). Variables for consideration included age, race, gender, marital status, insurance status, socioeconomic status, income level, educational level, hospital type (academic or community), hospital volume, region, and distance from a hospital. However, due to significant heterogeneity in reporting each variable in different studies, only race and gender were evaluable in a cumulative analysis. Ultimately, a total of 14 studies reporting race and gender were selected for quantitative analysis. The details of the included studies are reported in Table 1.
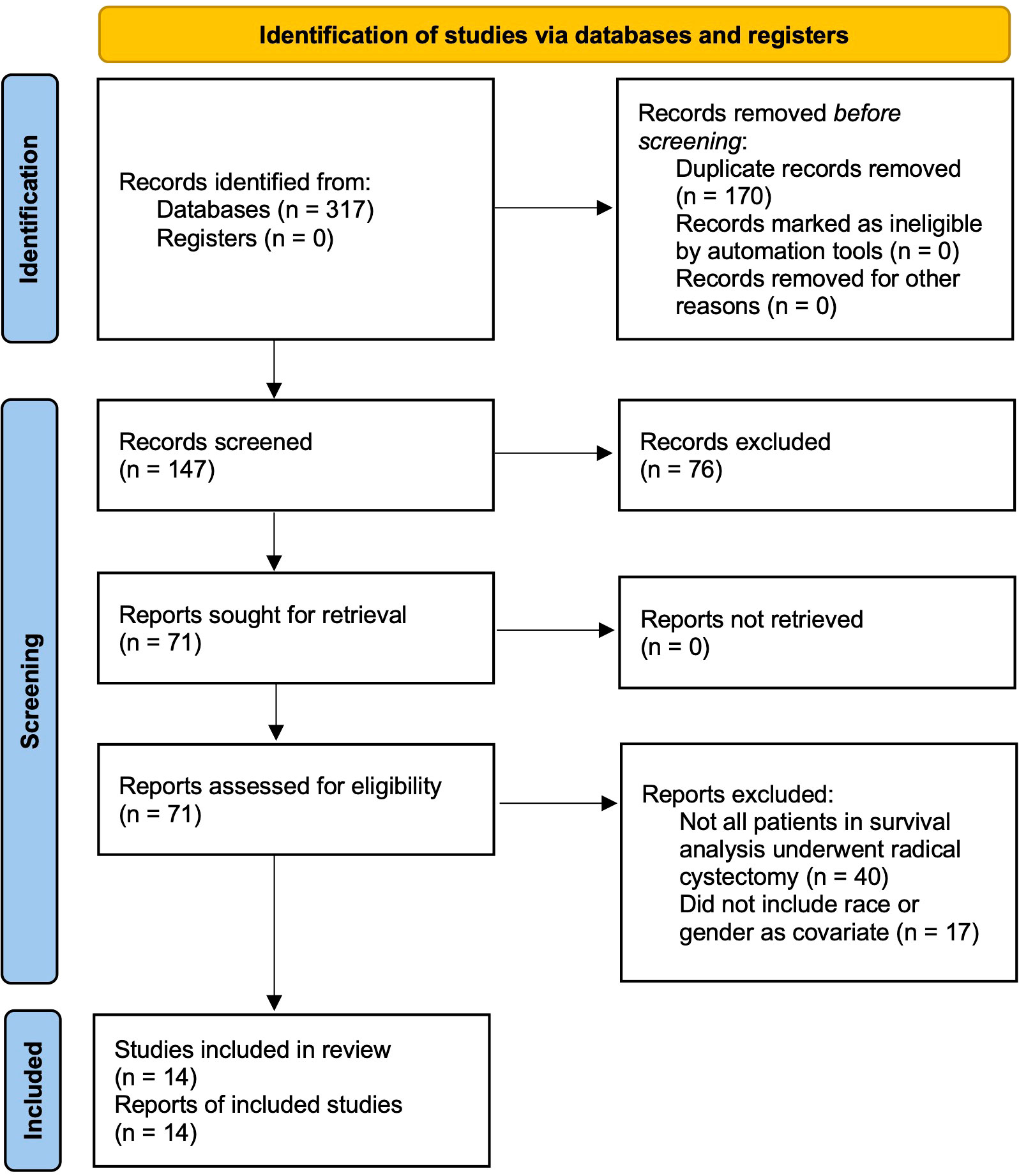
Figure 1 PRISMA flow diagram.
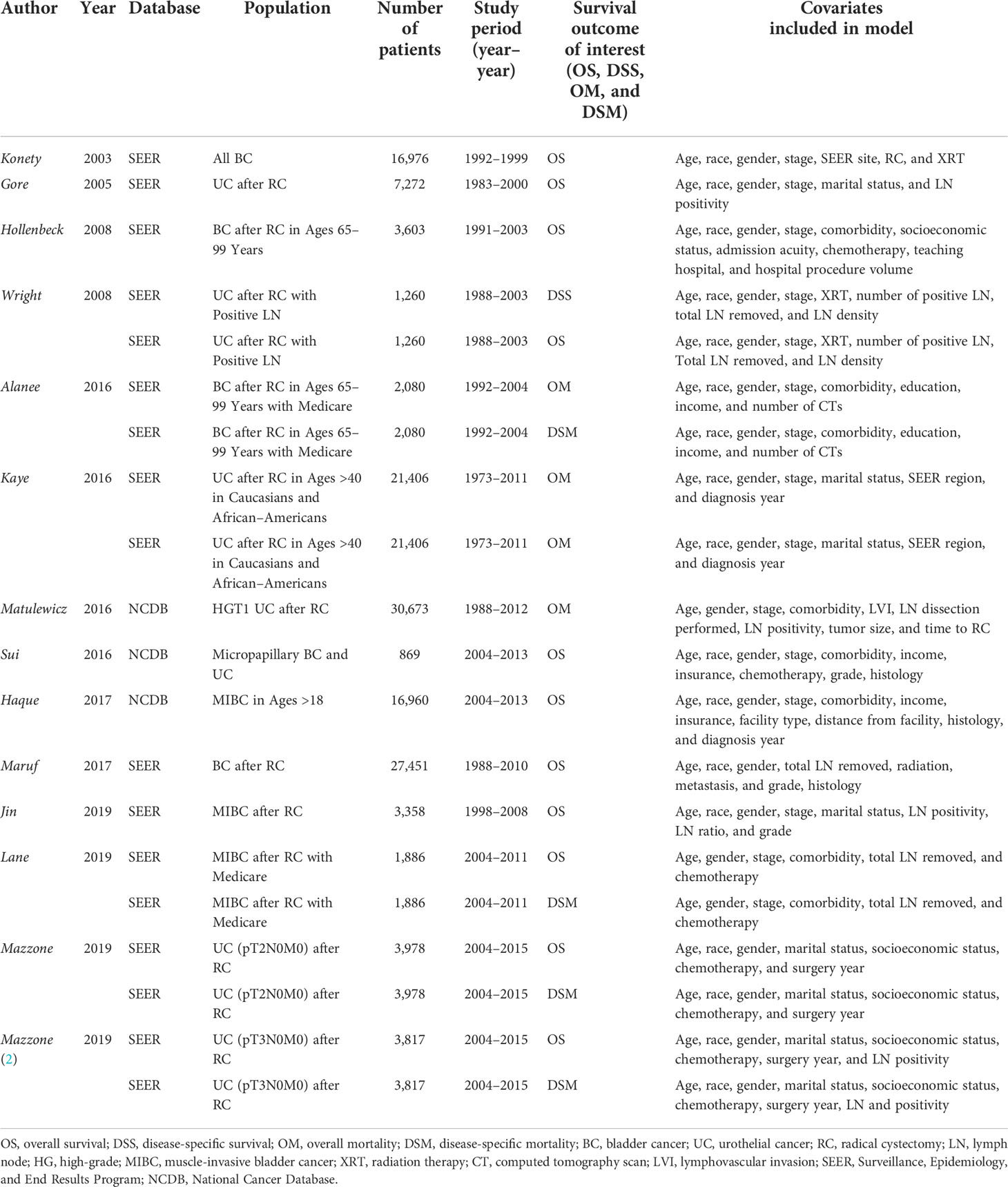
Table 1 Details of studies included in cumulative analyses.
Of the selected studies reporting survival outcomes after RC, not all sociodemographic factors were included in each multivariate model. Thirty-seven studies included age, 12 studies included marital status, 4 studies included insurance status, 2 studies included socioeconomic status, 6 studies included income status, 2 studies included educational status, 7 studies included hospital type, 4 studies included hospital volume, 7 studies included treatment region, and 3 studies included distance from a hospital. Each factor had a variety of reporting classifications and groupings that differed between studies.
A total of 11 studies (10 SEER and 1 NCDB) reported race as a predictor of survival outcomes (11 OS and 5 DSS) (23–33). All 11 studies included Black as a covariate level (23–33), whereas 3 studies included Hispanic (23–25), 3 studies included Asian (23, 25, 27), and 1 study included Native American (27). Our cumulative analysis found that, compared to White patients, Black patients have worse OS (HR 0.83; 95% CI 0.75, 0.92; p < 0.01; I2 = 79%) and DSS (HR 0.83; 95% CI 0.69, 1.00; p = 0.05; I2 = 69%), and Asian patients have worse OS (HR 0.84; 95% CI 0.77, 0.92; p < 0.01; I2 = 15%) but not DSS (HR 0.81; 95% CI 0.31, 2.10; p = 0.66). However, our results did not demonstrate a statistically significant difference between White and Hispanic patients in terms of OS (HR 1.03; 95% CI 0.79, 1.34; p = 0.66; I2 = 72%) or DSS (HR 2.63; 95% CI 0.34, 20.34; p = 0.35). Similarly, our results did not demonstrate a statistically significant difference between White and Native American patients in terms of OS (HR 2.16; 95% CI 0.80, 5.83; p = 0.13). These results are displayed in Figure 2.
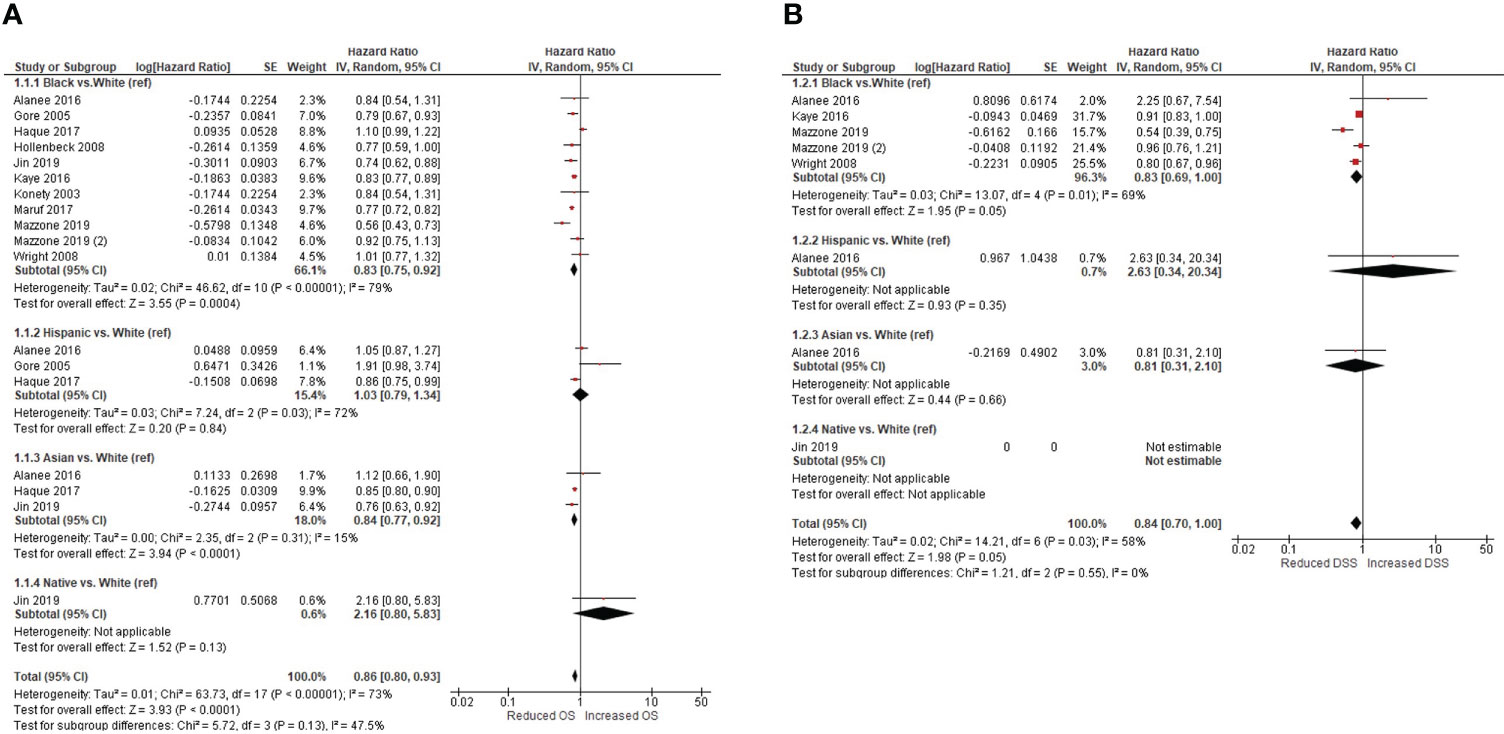
Figure 2 Overall (A) and disease-specific (B) survival based on race.
A total of 10 studies (8 SEER and 2 NCDB) reported gender as a predictor of survival outcomes (10 OS and 4 DSS) (24–27, 31–36). Our cumulative analysis did not demonstrate a statistically significant difference in OS (HR 1.03; 95% CI 0.93, 1.15; p = 0.53; I2 = 92%) nor DSS (HR 0.99; 95% CI 0.90, 1.08; p = 0.78; I2 = 1%) in female patients compared to male patients. These results are displayed in Figure 3.
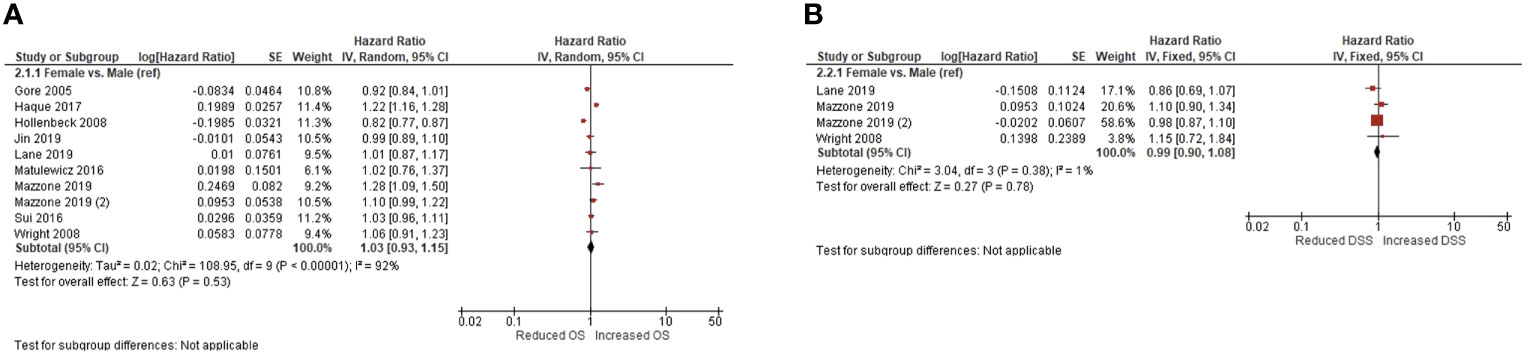
Figure 3 Overall (A) and disease-specific (B) survival based on gender.
The results of this systematic review and cumulative analysis highlight several sociodemographic factors that are associated with worse survival outcomes in patients undergoing RC for BC. Racial disparities are a significant contributor to survival outcomes, especially in Black and Asian patients, whereas gender differences are not. While our initial goal was to investigate the association between a greater number of sociodemographic factors, including marital status, insurance status, socioeconomic status, income level, and educational level, we found that the available data were too heterogeneous in its categorization and collection to be evaluated jointly. As such, cumulative analyses could only be performed to evaluate race and gender in this population. However, this signals the need for consistency in future work to address these critical gaps in knowledge.
Our analysis did find that race was a significant contributor to lower OS in Black and Asian patients compared to White patients, and DSS was worse in Black patients. Several studies of national databases have explored these disparate outcomes in Black patients. In an NCDB review of 12,652 patients undergoing RC for MIBC, Gild et al. found that Black patients were less likely to receive a pelvic lymph node dissection, and, when performed, fewer lymph nodes were removed. Moreover, Black patients were less likely to be treated in a high-volume center, and, when treated in a community program, Black patients had worse OS (12). In another NCDB review, Weiner et al. found that Black patients had worse OS and were less likely to receive timely treatment within 12 weeks of diagnosis. Delayed treatment was also more common in patients living in zip codes with the lowest levels of education and income (11). A lower likelihood of treatment at high-volume centers has been posited as a contributor to these disparate outcomes in several studies (12, 37, 38), which is known to have better perioperative and long-term outcomes (39). Moreover, multiple studies have found that Black patients are less likely to receive guideline-adherent care (40, 41). Therefore, whether the disparate survival outcomes are predominately driven by biological or social factors is unclear, the latter cannot be ignored, given the aforementioned findings of lower quality of and delayed care, as well as treatment in low-volume settings, in Black patients. The difference in OS among Asian patients is less understood and presents a potential avenue for future research. Whereas several studies, as noted above, have sought to determine the predictors of inferior outcomes in Black populations, less have been performed for Asians. Lastly, the collection of ethnic subgroup and nativity status in large population databases would improve the robustness of our understanding of the intersection between race/ethnicity and outcomes. For example, there are differences in known genetic and environmental risk factors, as well as BC incidence and survival rates, among Asian subgroups that will be obscured in the current SEER and NCDB framework (42).
Our finding that there is insufficient evidence to suggest that women have a significant difference in survival outcomes compared to men differs from prior reports, although the available data have been mixed, which was an impetus for this study. One national database review using the NCDB found that women were less likely to receive timely treatment for BC (11), whereas another using the SEER database reported that women were actually more likely to undergo RC than men without any significant difference in delays to treatment (43). In both studies, women had worse OS than men, although women did also present at more advanced stages. However, in the second study (43), women still had worse overall and cancer-specific survival even after propensity score matching, which indicates a potential biological basis for disparate outcomes. Indeed, aggressive molecular subtypes of BC are overrepresented in women (44), and sex-related differences in carcinogen metabolism at the cellular level, with increased urothelial exposure in women, have also been posited (45). Moreover, a prior study has demonstrated that cumulative exposure to estrogen may have a protective effect against BC, but when this production is lost after menopause, there may be a difference in risk (46). On the one hand, variant BC histology is more frequent in women, which are known to have a worse prognosis (47). On the other hand, women are also less frequently referred to urologists and have longer wait times in the evaluation of hematuria, which is potentially due to the higher incidence of cystitis and urinary tract infection treatments but still delays appropriate diagnosis and timely management (48, 49).
In summation, our study provides the results of a cumulative analysis of all evaluable sociodemographic factors (race and gender) of patients undergoing RC for BC in administrative databases. By combining the results of prior studies and adjusting for confounders, our findings provide much stronger conclusions. However, the mechanisms underlying these disparities remain poorly understood. Our findings help to consolidate previous reports to affirmatively address the impact of these factors on survival outcomes and improve risk stratification of these patients while also highlighting our significant gaps in knowledge. The lack of uniformity and consistency across studies reporting sociodemographic factors hampers the ability to draw robust summative conclusions and represents a major arena for future impactful research. Our findings are still clinically relevant, as they highlight weaknesses to be addressed in daily practice. Black patients are a particularly vulnerable population that may benefit from increased outreach for BC awareness and earlier referral to experienced treatment centers. Disparate outcomes are less clear in Asian patients, but the heterogeneity of ethnicity should be considered. Female patients may not necessarily need a more aggressive management plan than men, but the index of suspicion should be higher to avoid continued delays in diagnosis and timely care.
There are several limitations to our study, many of which are inherent to the usage of administrative databases. Firstly, there is the potential for overlapping patient groups across multiple studies using the same database. Whereas this is in part true, our cumulative analysis demonstrates a more robust result, independent of the study period and covariates included in each survival analysis. There was significant heterogeneity in variable and outcome definitions, which, as previously discussed, prevented cumulative analyses beyond race and gender. Patient relocation from one geographic region to another can affect long-term follow-up data. Moreover, there is a possibility that certain studies were not found in our search due to the omission of variations of search terms, such as education or ethnicity. Finally, selection biases can confound the results of survival analyses of adjuvant therapies used in cancer treatments (50).
Disparate BC survival outcomes after RC by race are present, with Black and Asian patients doing worse. Both OS and DSS are poorer in Black than White patients with BC. Asian patients have lower OS, but not DSS, as compared to White patients. Survival outcomes do not appear to differentiate by gender. There is significant heterogeneity by variable and outcome definitions, which is an inherent limitation of administrative databases and the most significant limitation of this study.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
WY: Conception and design, Collection of data, Data analysis, Manuscript writing. GC: Conception and design, Data analysis. AC: Collection of data, Manuscript writing. MB Collection of data, Manuscript writing. SB: Conception and design, Manuscript writing. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin (2020) 70(1):7–30. doi: 10.3322/caac.21590
2. Shariat SF, Karakiewicz PI, Palapattu GS, Lotan Y, Rogers CG, Amiel GE, et al. Outcomes of radical cystectomy for transitional cell carcinoma of the bladder: A contemporary series from the bladder cancer research consortium. J Urol (2006) 176(6 Pt 1):2414–22; discussion 22. doi: 10.1016/j.juro.2006.08.004
3. Witjes JA, Bruins HM, Cathomas R, Compérat EM, Cowan NC, Gakis G, et al. European Association of urology guidelines on muscle-invasive and metastatic bladder cancer: Summary of the 2020 guidelines. Eur Urol (2021) 79(1):82–104. doi: 10.1016/j.eururo.2020.03.055
4. Leissner J, Hohenfellner R, Thüroff JW, Wolf HK. Lymphadenectomy in patients with transitional cell carcinoma of the urinary bladder; significance for staging and prognosis. BJU Int (2000) 85(7):817–23. doi: 10.1046/j.1464-410x.2000.00614.x
5. Russell B, Liedberg F, Khan MS, Nair R, Thurairaja R, Malde S, et al. A systematic review and meta-analysis of delay in radical cystectomy and the effect on survival in bladder cancer patients. Eur Urol Oncol (2020) 3(2):239–49. doi: 10.1016/j.euo.2019.09.008
6. Grossman HB, Natale RB, Tangen CM, Speights VO, Vogelzang NJ, Trump DL, et al. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N Engl J Med (2003) 349(9):859–66. doi: 10.1056/NEJMoa022148
7. Stein JP, Lieskovsky G, Cote R, Groshen S, Feng AC, Boyd S, et al. Radical cystectomy in the treatment of invasive bladder cancer: long-term results in 1,054 patients. J Clin Oncol (2001) 19(3):666–75. doi: 10.1200/JCO.2001.19.3.666
8. Algaba F. Lymphovascular invasion as a prognostic tool for advanced bladder cancer. Curr Opin Urol (2006) 16(5):367–71. doi: 10.1097/01.mou.0000240311.08701.55
9. Zargar H, Zargar-Shoshtari K, Lotan Y, Shah JB, van Rhijn BW, Daneshmand S, et al. Final pathological stage after neoadjuvant chemotherapy and radical cystectomy for bladder cancer-does pT0 predict better survival than pTa/Tis/T1? J Urol (2016) 195(4 Pt 1):886–93. doi: 10.1016/j.juro.2015.10.133
10. Cacciamani GE, Ghodoussipour S, Mari A, Gill KS, Desai M, Artibani W, et al. Association between smoking exposure, neoadjuvant chemotherapy response and survival outcomes following radical cystectomy: Systematic review and meta-analysis. J Urol (2020) 204(4):649–60. doi: 10.1097/JU.0000000000000813
11. Weiner AB, Keeter MK, Manjunath A, Meeks JJ. Discrepancies in staging, treatment, and delays to treatment may explain disparities in bladder cancer outcomes: An update from the national cancer data base (2004-2013). Urol Oncol (2018) 36(5):237.e9–.e17. doi: 10.1016/j.urolonc.2017.12.015
12. Gild P, Wankowicz SA, Sood A, von Landenberg N, Friedlander DF, Alanee S, et al. Racial disparity in quality of care and overall survival among black vs. white patients with muscle-invasive bladder cancer treated with radical cystectomy: A national cancer database analysis. Urol Oncol (2018) 36(10):469.e1–.e11. doi: 10.1016/j.urolonc.2018.07.012
13. Uhlig A, Seif Amir Hosseini A, Simon J, Lotz J, Trojan L, Schmid M, et al. Gender specific differences in disease-free, cancer specific and overall survival after radical cystectomy for bladder cancer: A systematic review and meta-analysis. J Urol (2018) 200(1):48–60. doi: 10.1016/j.juro.2017.11.150
14. Zhang L, Wu B, Zha Z, Qu W, Zhao H, Yuan J. Clinicopathological factors in bladder cancer for cancer-specific survival outcomes following radical cystectomy: A systematic review and meta-analysis. BMC Cancer (2019) 19(1):716. doi: 10.1186/s12885-019-5924-6
15. Sammon JD, Morgan M, Djahangirian O, Trinh QD, Sun M, Ghani KR, et al. Marital status: A gender-independent risk factor for poorer survival after radical cystectomy. BJU Int (2012) 110(9):1301–9. doi: 10.1111/j.1464-410X.2012.10993.x
16. Pruthi RS, Lentz AC, Sand M, Kouba E, Wallen EM. Impact of marital status in patients undergoing radical cystectomy for bladder cancer. World J Urol (2009) 27(4):573–6. doi: 10.1007/s00345-009-0380-6
17. Nelles JL, Joseph SA, Konety BR. The impact of marriage on bladder cancer mortality. Urol Oncol (2009) 27(3):263–7. doi: 10.1016/j.urolonc.2008.04.016
18. Nazemi A, Ghodoussipour S, Pearce S, Bhanvadia S, Daneshmand S. Socioeconomic and insurance status are independent prognostic indicators of higher disease stage and worse prognosis in bladder cancer. Urol Oncol (2019) 37(10):784–90. doi: 10.1016/j.urolonc.2019.04.021
19. Golombos DM, O’Malley P, Lewicki P, Nguyen DP, Stone BV, Al Hussein Al Awamlh B, et al. The impact of socioeconomic status on perioperative complications and oncologic outcomes in patients undergoing radical cystectomy. World J Urol (2017) 35(7):1063–71. doi: 10.1007/s00345-016-1972-6
20. Parmar MK, Torri V, Stewart L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Stat Med (1998) 17(24):2815–34. doi: 10.1002/(SICI)1097-0258(19981230)17:24<2815::AID-SIM110>3.0.CO;2-8
21. Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials (2007) 8:16. doi: 10.1186/1745-6215-8-16
22. Higgins J, Thomas J, Chandler J, Cumpston M, Li T, Page M, et al. Cochrane handbook for systematic reviews of interventions. Cochrane2021. Chichester (UK): John Wiley & Sons (2019).
23. Alanee S, Ganai S, Gupta P, Holland B, Dynda D, Slaton J. Disparities in long-term radiographic follow-up after cystectomy for bladder cancer: Analysis of the SEER-Medicare database. Urol Ann (2016) 8(2):178–83. doi: 10.4103/0974-7796.164852
24. Gore JL, Kwan L, Saigal CS, Litwin MS. Marriage and mortality in bladder carcinoma. Cancer (2005) 104(6):1188–94. doi: 10.1002/cncr.21295
25. Haque W, Verma V, Butler EB, Teh BS. Radical cystectomy versus chemoradiation for muscle-invasive bladder cancer: Impact of treatment facility and sociodemographics. Anticancer Res (2017) 37(10):5603–8. doi: 10.21873/anticanres.11994
26. Hollenbeck BK, Ye Z, Wong SL, Montie JE, Birkmeyer JD. Hospital lymph node counts and survival after radical cystectomy. Cancer (2008) 112(4):806–12. doi: 10.1002/cncr.23234
27. Jin S, Wang B, Zhu Y, Dai W, Xu P, Yang C, et al. Log odds could better predict survival in muscle-invasive bladder cancer patients compared with pN and lymph node ratio. J Cancer (2019) 10(1):249–56. doi: 10.7150/jca.27399
28. Kaye DR, Canner JK, Kates M, Schoenberg MP, Bivalacqua TJ. Do African American patients treated with radical cystectomy for bladder cancer have worse overall survival? Accounting for pathologic staging and patient demographics beyond race makes a difference. Bladder Cancer (2016) 2(2):225–34. doi: 10.3233/BLC-150041
29. Konety BR, Joslyn SA. Factors influencing aggressive therapy for bladder cancer: An analysis of data from the SEER program. J Urol (2003) 170(5):1765–71. doi: 10.1097/01.ju.0000091620.86778.2e
30. Maruf M, Sidana A, Purnell S, Jain AL, Brancato SJ, Agarwal PK. Lymph node dissection during radical cystectomy following prior radiation therapy: Results from the SEER database. Int Urol Nephrol (2018) 50(2):257–62. doi: 10.1007/s11255-017-1751-3
31. Mazzone E, Knipper S, Mistretta FA, Tian Z, Preisser F, Gallina A, et al. Is neoadjuvant chemotherapy for pT2 bladder cancer associated with a survival benefit in a population-based analysis? Cancer Epidemiol (2019) 58:83–8. doi: 10.1016/j.canep.2018.11.007
32. Mazzone E, Nazzani S, Knipper S, Tian Z, Preisser F, Gallina A, et al. Contemporary use and survival after perioperative systemic chemotherapy in patients with locally advanced non-metastatic urothelial carcinoma of the bladder treated with radical cystectomy. Eur J Surg Oncol (2019) 45(7):1253–9. doi: 10.1016/j.ejso.2019.01.218
33. Wright JL, Lin DW, Porter MP. The association between extent of lymphadenectomy and survival among patients with lymph node metastases undergoing radical cystectomy. Cancer (2008) 112(11):2401–8. doi: 10.1002/cncr.23474
34. Lane G, Risk M, Fan Y, Krishna S, Konety B. Persistent muscle-invasive bladder cancer after neoadjuvant chemotherapy: An analysis of surveillance, epidemiology and end results-Medicare data. BJU Int (2019) 123(5):818–25. doi: 10.1111/bju.14529
35. Matulewicz RS, Frainey BT, Oberlin DT, Meeks JJ. High-risk of adverse pathologic features in patients with clinical T1 high-grade bladder cancer undergoing radical cystectomy. J Natl Compr Canc Netw (2016) 14(11):1403–11. doi: 10.6004/jnccn.2016.0150
36. Sui W, Matulay JT, James MB, Onyeji IC, Theofanides MC, RoyChoudhury A, et al. Micropapillary bladder cancer: Insights from the national cancer database. Bladder Cancer (2016) 2(4):415–23. doi: 10.3233/BLC-160066
37. Sukumar S, Ravi P, Sood A, Gervais MK, Hu JC, Kim SP, et al. Racial disparities in operative outcomes after major cancer surgery in the United States. World J Surg (2015) 39(3):634–43. doi: 10.1007/s00268-014-2863-x
38. Konety BR, Allareddy V, Carroll PR. Factors affecting outcomes after radical cystectomy in African americans. Cancer (2007) 109(3):542–8. doi: 10.1002/cncr.22449
39. Hollenbeck BK, Wei Y, Birkmeyer JD. Volume, process of care, and operative mortality for cystectomy for bladder cancer. Urology (2007) 69(5):871–5. doi: 10.1016/j.urology.2007.01.040
40. Barocas DA, Alvarez J, Koyama T, Anderson CB, Gray DT, Fowke JH, et al. Racial variation in the quality of surgical care for bladder cancer. Cancer (2014) 120(7):1018–25. doi: 10.1002/cncr.28520
41. Washington SL, Neuhaus J, Meng MV, Porten SM. Social determinants of appropriate treatment for muscle-invasive bladder cancer. Cancer Epidemiol Biomarkers Prev (2019) 28(8):1339–44. doi: 10.1158/1055-9965.EPI-18-1280
42. Hashibe M, Gao T, Li G, Dalbagni G, Zhang ZF. Comparison of bladder cancer survival among Japanese, Chinese, Filipino, Hawaiian and Caucasian populations in the united states. Asian Pac J Cancer Prev (2003) 4(3):267–73.
43. Williams SB, Huo J, Dafashy TJ, Ghaffary CK, Baillargeon JG, Morales EE, et al. Survival differences among patients with bladder cancer according to sex: Critical evaluation of radical cystectomy use and delay to treatment. Urol Oncol (2017) 35(10):602.e1–.e9. doi: 10.1016/j.urolonc.2017.05.022
44. Kamoun A, de Reyniès A, Allory Y, Sjodahl G, Robertson AG, Seiler R, et al. A consensus molecular classification of muscle-invasive bladder cancer. Eur Urol (2020) 77(4):420–33. doi: 10.1016/j.eururo.2019.09.006
45. Dobruch J, Daneshmand S, Fisch M, Lotan Y, Noon AP, Resnick MJ, et al. Gender and bladder cancer: A collaborative review of etiology, biology, and outcomes. Eur Urol (2016) 69(2):300–10. doi: 10.1016/j.eururo.2015.08.037
46. Daugherty SE, Lacey JV Jr, Pfeiffer RM, Park Y, Hoover RN, Silverman DT. Reproductive factors and menopausal hormone therapy and bladder cancer risk in the NIH-AARP diet and health study. Int J Cancer (2013) 133(2):462–72. doi: 10.1002/ijc.28022
47. Burge F, Kockelbergh R. Closing the gender gap: Can we improve bladder cancer survival in women? - A systematic review of diagnosis, treatment and outcomes. Urol Int (2016) 97(4):373–9. doi: 10.1159/000449256
48. Garg T, Pinheiro LC, Atoria CL, Donat SM, Weissman JS, Herr HW, et al. Gender disparities in hematuria evaluation and bladder cancer diagnosis: A population based analysis. J Urol (2014) 192(4):1072–7. doi: 10.1016/j.juro.2014.04.101
49. Cohn JA, Vekhter B, Lyttle C, Steinberg GD, Large MC. Sex disparities in diagnosis of bladder cancer after initial presentation with hematuria: A nationwide claims-based investigation. Cancer (2014) 120(4):555–61. doi: 10.1002/cncr.28416
Keywords: sociodemographic, bladder cancer, disparities, systematic review, survival
Citation: Yip W, Chen AB, Basin MF, Cacciamani GE and Bhanvadia SK (2022) The impact of non-modifiable sociodemographic factors on bladder cancer survival outcomes after radical cystectomy: A systematic review and cumulative analysis of population cohort studies. Front. Urol. 2:934550. doi: 10.3389/fruro.2022.934550
Received: 02 May 2022; Accepted: 22 August 2022;
Published: 13 September 2022.
Edited by:
Kenrick Ng, University College London, United KingdomReviewed by:
Liang Qu, Austin Health, University of Melbourne, AustraliaCopyright © 2022 Yip, Chen, Basin, Cacciamani and Bhanvadia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wesley Yip, d2VzbGV5eWlwbWRAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.