
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Transplant. , 15 May 2024
Sec. Thoracic Transplantation
Volume 3 - 2024 | https://doi.org/10.3389/frtra.2024.1379695
 Margrethe Flesvig Holt1,2*Stine Holmen1,2,3Katrine Rolid4Kristine V. Brautaset Englund5Charlotte M. Østby1Håvard Ravnestad1,2Arne K. Andreassen1Lars Gullestad1,2,6Einar Gude1Kaspar Broch1,2,6
Margrethe Flesvig Holt1,2*Stine Holmen1,2,3Katrine Rolid4Kristine V. Brautaset Englund5Charlotte M. Østby1Håvard Ravnestad1,2Arne K. Andreassen1Lars Gullestad1,2,6Einar Gude1Kaspar Broch1,2,6
Introduction: Pre-transplant obesity and weight gain after heart transplantation are both associated with increased risk of poor clinical outcomes. We aimed to assess the association between overweight or obesity, exercise capacity, and health-related quality of life in heart transplant recipients.
Methods: This study is based on baseline data from the IronIC trial, in which we randomized 102 heart transplant recipients with iron deficiency to ferric derisomaltose or placebo. We performed cardio pulmonary exercise testing in all participants. To assess quality of life, we used the SF-36v2 questionnaire, using two sum scores: the physical component summary and the mental component summary. A minimal clinically important difference was defined as ≥2 and ≥3 for the physical and the mental component summary, respectively.
Results: 24/102 heart transplant recipients (24%) had a body mass index (BMI) ≥30 kg/m2. Peak oxygen consumption was 17.3 ± 4.6 ml/kg/min in the obese group vs. 24.7 ± 6.4 ml/kg/min in the group with a BMI <30 for a between-group difference of 7.4 (95% confidence interval 4.7–10.2) ml/kg/min: p < 0.001. The physical component summary score was on average 5.2 points lower in the patients with a body mass index ≥30 than in the lower weight group (p = 0.04).
Conclusion: Almost a quarter of our heart transplant recipients in long-term follow-up had a BMI ≥30 kg/m2. These patients had substantially lower exercise capacity and lower quality of life in the physical domain.
Obesity prior to heart transplantation (HTx) and weight gain resulting in overweight or obesity after heart transplantation are associated with adverse cardiovascular events, allograft rejections and death (1–8). The effect of obesity and overweight on physical capacity and quality of life after heart transplantation has not been well studied.
Compared with the general population, heart transplant recipients have reduced physical capacity and reduced health-related quality of life (9–12). Exercise capacity improves substantially after heart transplantation (13). However, it stays lower than that of the general population, with peak oxygen consumption typically reported to range between 50%–70% of predicted values (12).
Quality of life increases substantially after heart transplantation but remains reduced compared with that of the general population (9, 14, 15). Several factors may contribute to reduced quality of life after heart transplantation, including the trauma associated with the pre-existing life-threatening heart failure and the subsequent surgery, as well as comorbidities and adverse effects of life-long treatment with immunosuppressants.
In the general population, the impact of overweight/obesity on health-related quality of life and physical capacity has been extensively studied. Obesity is associated with reduced functional mobility, fatigue, and depression (16–18). It is a well-known cause of reduced quality of life in the normal population (19). However, whether weight gain, overweight, and obesity are associated with health-related quality of life after heart transplantation remains largely unknown.
In this study we aimed to assess the association between obesity, defined as a body mass index (BMI) ≥30 kg/m2, exercise capacity, and health-related quality of life in contemporary heart transplant recipients.
The randomised, controlled, double-blinded Intravenous Iron supplement for Iron deficiency in Cardiac transplant recipients (IronIC) trial was conducted at Oslo University Hospital, Rikshospitalet, the sole solid organ transplantation center in Norway, and has been reported in detail (20). In summary, 102 maintenance heart transplant recipients with iron deficiency and hemoglobin >100 g/L were randomized 1:1 to ferric derisomaltose or placebo (saline). The primary endpoint, peak oxygen consumption at six months after iron infusion, did not differ significantly between the groups (20). The trial was approved by the Regional Committee for Medical Research Ethics South-East Norway and conducted in compliance with the Declaration of Helsinki.
In this sub study of the Ironic trial, we aimed to assess the association between obesity or overweight and exercise capacity and health-related quality of life in heart transplant recipients. Obesity was defined as a body mass index (BMI) ≥30 kg/m2, in line with the cut-off values defined by the World Health Organization (21).
We assessed body composition using the InBody 770 bioelectrical impedance analyser. We registered weight and estimated total body water, total fat, skeletal muscle mass, and waist/hip ratio. Percentage body fat and percentage skeletal muscle mass was estimated by dividing fat mass and skeletal muscle mass, respectively, by total body weight and multiplying by 100.
We measured peak oxygen consumption on a treadmill with a breath-by-breath gas analyser as described previously (20). The test was continued until subjective fatigue was reached. We used a Borg scale value >18 points or a respiratory exchange ratio >1.05 indicative of an adequate maximal exercise test (22). The 2014 American College of Sports Medicine guidelines was used to determine predicted values (23). Patients who were unable to perform a treadmill test, performed the cardiopulmonary exercise test on an electrically braked bicycle ergometer.
We measured hand grip strength using the Kern MAP hand-held dynamometer. The patients performed the test three times with their dominant hand. The highest value was recorded.
Health-related quality of life was examined using the SF-36v2 questionnaire, the EuroQol (EQ) 5D-3L and the EQ visual-analogue scale (VAS). The scores were converted into two norm-based sum scores: the physical component summary score and the mental component summary score. A minimal clinically important difference was defined as ≥2 for the physical component summary score, and ≥3 for the mental component summary score (24). The EQ-5D-3L questionnaire comprises five questions, each with three response alternatives addressing; mobility, self-care, usual activities, pain/discomfort, and anxiety/depression (25). We used a Swedish experience based value set to convert the scores into a summery index (26). The EQ VAS instructs the respondent to rate their overall health from 0 to 100 on a vertical visual analogue scale.
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 28 (IBM Corporation). Data are expressed as means ± standard deviation, medians with interquartile range or numbers with percentages as appropriate. Chi-square test, Fisher's exact test, Mann-Whitney U-test, and t-test for independent samples were used as appropriate. A two-sided p < 0.05 was considered statistically significant.
We enrolled 102 patients in the IronIC trial. Of the 102 participants, 24 patients (24%) were obese. Patient demographics by weight group (≥30 kg/m2 or <30 kg/m2) are presented in Table 1. Age, sex distribution, and time since transplantation were similar in the two groups. Use of beta blockers and loop diuretics was more frequent among patients with a BMI ≥30 kg/m2. There was a tendency towards ischemic reason being more and dilated cardiomyopathy being less frequent reasons for HTx in the patients with BMI ≥30 kg/m2. From approval for heart transplantation to inclusion in the IronIC trial, the patients with BMI ≥30 kg/m2 had gained 9.0 [−1.5 to 18.5] kg vs. 1.0 [−2.0 to 6.5] kg in the group with lower BMI (p = 0.007). For details see Supplementary Material.
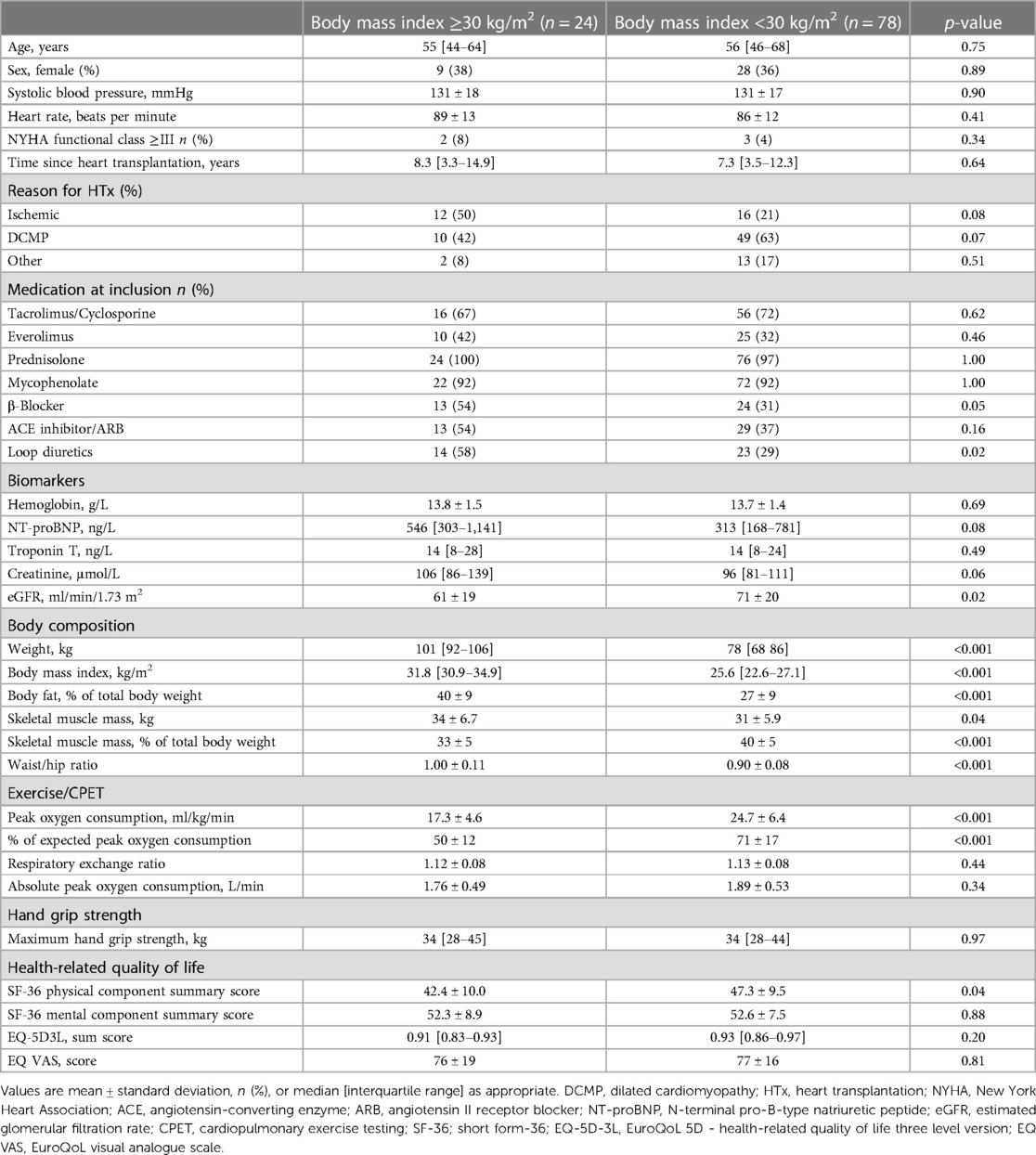
Table 1. Patient characteristics.
The body fat percentage was higher in the patients with a BMI ≥30 kg/m2 than in the group with lower BMI; 40 ± 9% vs. 27 ± 9%, p < 0.001 (Figure 1A and Table 1). The percentage of skeletal muscle mass of total body weight was lower in the obese patients compared with those with a BMI <30 kg/m2. Furthermore, patients with a BMI ≥30 kg/m2 had a significantly higher waist-hip ratio. For details, see Table 1.
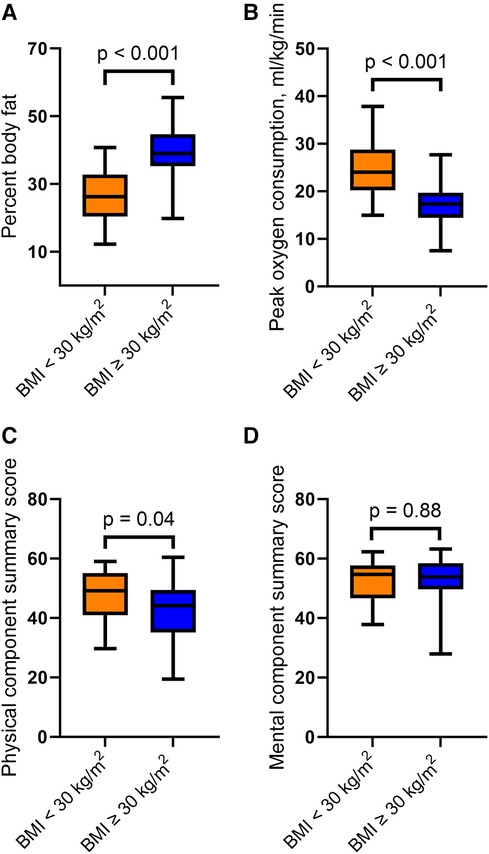
Figure 1. Difference in (A) percentage body fat, (B) peak oxygen consumption, (C) physical component summary and (D) mental component summary, stratified by BMI. P-values for the between group differences. Boxes: 25–75 percentiles; whiskers: 5–95 percentiles.
The peak oxygen consumption was 17.3 ± 4.6 ml/kg/min in the patients with BMI ≥30 kg/m2 vs. 24.7 ± 6.4 ml/kg/min in patients with BMI <30 kg/m2, for a between-group difference of 7.4 (95% confidence interval 4.7–10.2) ml/kg/min; p < 0.001 (Figure 1B). The median respiratory exchange ratio was >1.05 and similar in the two groups, suggesting adequate maximal exercise tests in both groups (Table 1).
There was no difference in hand grip strength between the patients with obesity and the patients with a BMI <30 kg/m2; (Table 1).
There was a statistically and clinically significant difference in the SF-36 physical component summary score between the two groups. The patients with BMI ≥30 kg/m2 had a mean physical component summary score of 42.4 ± 10.0 vs. 47.3 ± 9.5 in the patients with BMI <30 kg/m2; p = 0.04 (Figure 1C). On the other hand, there was no difference in the SF-36 mental component summary score between the two groups (Figure 1D). There were no differences in self-reported quality of life, as assessed by the EQ-5D and EQ VAS. For details, see Table 1.
Our results suggest that many Norwegian heart transplant recipients have overweight or obesity, resulting in part from obesity prior to transplantation and in part from weight gain after transplantation. Patients with a BMI ≥30 kg/m2 have substantially lower exercise capacity and lower health-related quality of life in the physical domain. Despite larger absolute muscle mass in the obese patients, hand grip strength and absolute oxygen uptake were not increased relative to those with a BMI <30 kg/m2.
Obesity prior to heart transplantation is associated with higher post-transplant mortality and with increased incidence of comorbidities, treated rejections, and cardiac allograft vasculopathy (6–8). The International Society for Heart Lung Transplantation (ISHLT) and the 2021 The European Society of Cardiology recommend a BMI <35 kg/m2 prior to listing for heart transplantation (22, 27). Excessive weight gain after heart transplantation is associated with an increased risk of cardiac allograft vasculopathy, non-fatal major adverse cardiovascular events, and allograft rejections (4, 5).
Health-related quality of life and exercise capacity increase after heart transplantation (9, 13–15). There is a positive correlation between health-related quality of life and exercise capacity in heart transplant recipients (10). While the negative effects of obesity on physical capacity and health-related quality of life are well documented in the general population (16–19), our study suggests that this also holds true for heart transplant recipients. There are already recommendations in place to reduce the risks associated with obesity in heart transplant candidates. However, our results suggest that weight control is important also after heart transplantation.
This study has some important limitations. The number of patients was limited, and the participants of the IronIC trial were required to have iron deficiency as defined in heart failure. However, our previous results suggest that this definition of iron deficiency is too liberal in maintenance heart transplant recipients, and that many of the participants were not truly iron deficient (20). We have no reason to believe that obesity is less prevalent in heart transplant recipients without iron deficiency, or that low iron stores would interact with the relationship between BMI and exercise capacity. Furthermore, our patients were included several years after heart transplantation. This make our data vulnerable for survival bias, and our study is not suitable to address survival.
In summary, obese heart transplant recipients had significantly diminished physical capacity and reduced health-related quality of life. However, we do not know whether normalization of BMI would be associated with improvements in these domains. Clinical trials targeting weight-loss in heart transplant recipients are warranted.
The data analyzed in this study is subject to the following licenses/restrictions: Due to the sensitive nature of the data collected for this study, the material will not be made publicly available. Requests to access these datasets should be directed to mafhol@ous-hf.no.
The studies involving humans were approved by the Regional Committee for Medical Research Ethics South-East Norway. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
MH: Data curation, Formal Analysis, Writing – original draft, Writing – review & editing. SH: Writing – original draft, Writing – review & editing. KR: Formal Analysis, Investigation, Methodology, Project administration, Writing – original draft, Writing – review & editing. KE: Data curation, Formal Analysis, Investigation, Methodology, Project administration, Writing – original draft, Writing – review & editing. CØ: Data curation, Investigation, Methodology, Project administration, Writing – original draft, Writing – review & editing. HR: Methodology, Writing – original draft, Writing – review & editing. AA: Methodology, Writing – original draft, Writing – review & editing. LG: Conceptualization, Funding acquisition, Resources, Supervision, Writing – original draft, Writing – review & editing. EG: Methodology, Supervision, Writing – original draft, Writing – review & editing. KB: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This work has been partly funded with a grant from The Bergesen Foundation (grant to MH). The IronIC trial was investigator-initiated. The study was sponsored by the South Eastern Norway Regional Health Authority (grant number 2018027). Pharmacosmos® provided the investigational medicinal products an unrestricted grant. The authors declare that this study received funding from Pharmacosmos®. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frtra.2024.1379695/full#supplementary-material
ACE, angiotensin-converting enzyme; ARB, angiotensin II receptor blocker; BMI, body mass index; DCMP, dilated cardiomyopathy; CPET, cardiopulmonary exercise testing; eGFR, estimated glomerular filtration rate; EQ-5D-3L, EuroQoL 5D - health-related quality of life three level version; EQ VAS, EuroQoL visual analogue scale; HRQoL, health-related quality of life; HTx, heart transplantation; NT-proBNP, N-terminal pro-B-type natriuretic peptide; NYHA, New York Heart Association.
1. Williams JJ, Lund LH, LaManca J, Kunavarapu C, Cohen DJ, Heshka S, et al. Excessive weight gain in cardiac transplant recipients. J Heart Lung Transplant. (2006) 25(1):36–41. doi: 10.1016/j.healun.2005.06.016
2. Baker AM, Levine TB, Goldberg AD, Levine AB. Natural history and predictors of obesity after orthotopic heart transplantation. J Heart Lung Transplant. (1992) 11(6):1156–9.1457440
3. Keteyian SJ, Marks C, Fedel FJ, Ehrman JK, Goslin BR, Connolly A, et al. Assessment of body composition in heart transplant patients. Med Sci Sports Exercise. (1992) 24(2):247–52. doi: 10.1249/00005768-199202000-00015
4. Ram E, Klempfner R, Peled A, Kassif Y, Sternik L, Lavee J, et al. Weight gain post-heart transplantation is associated with an increased risk for allograft vasculopathy and rejection. Clin Transplant. (2021) 35(3):e14187. doi: 10.1111/ctr.14187
5. Grady KL, Naftel D, Pamboukian SV, Frazier OH, Hauptman P, Herre J, et al. Post-operative obesity and cachexia are risk factors for morbidity and mortality after heart transplant: multi-institutional study of post-operative weight change. J Heart Lung Transplant. (2005) 24(9):1424–30. doi: 10.1016/j.healun.2004.08.010
6. Chouairi F, Milner A, Sen S, Guha A, Stewart J, Jastreboff AM, et al. Impact of obesity on heart transplantation outcomes. J Am Heart Assoc. (2021) 10(23):e021346. doi: 10.1161/JAHA.121.021346
7. Foroutan F, Doumouras BS, Ross H, Alba AC. Impact of pretransplant recipient body mass index on post heart transplant mortality: a systematic review and meta-analysis. Clin Transplant. (2018) 32(8):e13348. doi: 10.1111/ctr.13348
8. Doumouras BS, Fan CS, Mueller B, Dipchand AI, Manlhiot C, Stehlik J, et al. The effect of pre-heart transplant body mass index on posttransplant outcomes: an analysis of the ISHLT registry data. Clin Transplant. (2019) 33(7):e13621. doi: 10.1111/ctr.13621
9. Politi P, Piccinelli M, Fusar-Poli P, Klersy C, Campana C, Goggi C, et al. Ten years of “extended” life: quality of life among heart transplantation survivors. Transplantation. (2004) 78(2):257–63. doi: 10.1097/01.TP.0000133537.87951.F2
10. Rolid K, Andreassen AK, Yardley M, Gude E, Bjørkelund E, Authen AR, et al. High-intensity interval training and health-related quality of life in de novo heart transplant recipients—results from a randomized controlled trial. Health Qual Life Outcomes. (2020) 18(1):283. doi: 10.1186/s12955-020-01536-4
11. Yardley M, Gullestad L, Nytrøen K. Importance of physical capacity and the effects of exercise in heart transplant recipients. World J Transplant. (2018) 8(1):1–12. doi: 10.5500/wjt.v8.i1.1
12. Nytrøen K, Rustad LA, Aukrust P, Ueland T, Hallén J, Holm I, et al. High-intensity interval training improves peak oxygen uptake and muscular exercise capacity in heart transplant recipients. Am J Transplant. (2012) 12(11):3134–42. doi: 10.1111/j.1600-6143.2012.04221.x
13. Osada N, Chaitman BR, Donohue TJ, Wolford TL, Stelken AM, Miller LW. Long-term cardiopulmonary exercise performance after heart transplantation. Am J Cardiol. (1997) 79(4):451–6. doi: 10.1016/S0002-9149(96)00785-0
14. Saeed I, Rogers C, Murday A. Health-related quality of life after cardiac transplantation: results of a UK national survey with norm-based comparisons. J Heart Lung Transplant. (2008) 27(6):675–81. doi: 10.1016/j.healun.2008.03.013
15. Karam VH, Gasquet I, Delvart V, Hiesse C, Dorent R, Danet C, et al. Quality of life in adult survivors beyond 10 years after liver, kidney, and heart transplantation. Transplantation. (2003) 76(12):1699–704. doi: 10.1097/01.TP.0000092955.28529.1E
16. Forhan M, Gill SV. Obesity, functional mobility and quality of life. Best Pract Res Clin Endocrinol Metab. (2013) 27(2):129–37. doi: 10.1016/j.beem.2013.01.003
17. Lim W, Hong S, Nelesen R, Dimsdale JE. The association of obesity, cytokine levels, and depressive symptoms with diverse measures of fatigue in healthy subjects. Arch Intern Med. (2005) 165(8):910–5. doi: 10.1001/archinte.165.8.910
18. Luppino FS, de Wit LM, Bouvy PF, Stijnen T, Cuijpers P, Penninx BW, et al. Overweight, obesity, and depression: a systematic review and meta-analysis of longitudinal studies. Arch Gen Psychiatry. (2010) 67(3):220–9. doi: 10.1001/archgenpsychiatry.2010.2
19. Stephenson J, Smith CM, Kearns B, Haywood A, Bissell P. The association between obesity and quality of life: a retrospective analysis of a large-scale population-based cohort study. BMC Public Health. (2021) 21(1):1990. doi: 10.1186/s12889-021-12009-8
20. Brautaset Englund KV, Østby CM, Rolid K, Gude E, Andreassen AK, Gullestad L, et al. Intravenous iron supplement for iron deficiency in cardiac transplant recipients (IronIC): a randomized clinical trial. J Heart Lung Transplant. (2021) 40(5):359–67. doi: 10.1016/j.healun.2021.01.1390
21. WHO. Obesity: preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ Tech Rep Ser. (2000) 894(i-xii):1–253.
22. Mehra MR, Canter CE, Hannan MM, Semigran MJ, Uber PA, Baran DA, et al. The 2016 international society for heart lung transplantation listing criteria for heart transplantation: a 10-year update. J Heart Lung Transplant. (2016) 35(1):1–23. doi: 10.1016/j.healun.2015.10.023
23. Medicine ACoS. ACSM's Guidelines for Exercise Testing and Prescription. Indianapolis: Lippincott Williams & Wilkins (2013).
25. Group E. EQ-5D-3L | About Available online at: https://euroqol.org/1990. Available online at: https://euroqol.org/eq-5d-instruments/eq-5d-3l-about/?_gl=1*1l0dpdb*_up*MQ..*_ga*MTI2MDI3NjU5LjE2OTAzNzA4OTg.*_ga_02T9YV6MT2*MTY5MDM3MDg5Ny4xLjAuMTY5MDM3MDg5Ny4wLjAuMA (updated November 1, 2022).
26. Burström K, Sun S, Gerdtham UG, Henriksson M, Johannesson M, Levin L, et al. Swedish experience-based value sets for EQ-5D health states. Qual Life Res. (2014) 23(2):431–42. doi: 10.1007/s11136-013-0496-4
27. McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: developed by the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. (2022) 24(1):4–131. doi: 10.1002/ejhf.2333
Keywords: heart transplant recipient, HRQoL (health-related quality of life), oxygen consumption (VO2peak), obesity, heart transplantation (HTx)
Citation: Holt MF, Holmen S, Rolid K, Englund KVB, Østby CM, Ravnestad H, Andreassen AK, Gullestad L, Gude E and Broch K (2024) The association between body mass index, exercise capacity, and health-related quality of life in heart transplant recipients. Front. Transplant. 3:1379695. doi: 10.3389/frtra.2024.1379695
Received: 31 January 2024; Accepted: 30 April 2024;
Published: 15 May 2024.
Edited by:
Asishana Avo Osho, Harvard Medical School, United StatesReviewed by:
Suresh Keshavamurthy, University of Texas Southwestern Medical Center, United States© 2024 Holt, Holmen, Rolid, Englund, Østby, Ravnestad, Andreassen, Gullestad, Gude and Broch. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Margrethe Flesvig Holt, mafhol@ous-hf.no
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.