
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Rehabil. Sci., 06 July 2022
Sec. Disability, Rehabilitation, and Inclusion
Volume 3 - 2022 | https://doi.org/10.3389/fresc.2022.898804
This article is part of the Research TopicPromoting Participation Following NeurotraumaView all 9 articles
 Christophe Alarie1,2,3Isabelle Gagnon4,5Elaine de Guise2,3,6Michelle McKerral2,3,6Marietta Kersalé1,2,3Béatrice van het Hoog1,2,3Bonnie Swaine1,2,3*
Christophe Alarie1,2,3Isabelle Gagnon4,5Elaine de Guise2,3,6Michelle McKerral2,3,6Marietta Kersalé1,2,3Béatrice van het Hoog1,2,3Bonnie Swaine1,2,3*Introduction: Persistent post-concussion symptoms following a mild traumatic brain injury (mTBI) can impact function and participation of adults. Physical activity is recommended to reduce symptoms and foster return to normal activities. Adults with a mTBI may have personal factors or experience accessibility issues restricting physical activity. Walking is a physical activity accessible to most that could be delivered remotely.
Objectives: Determine the feasibility, safety, and acceptability of a remotely delivered progressive walking intervention designed for adults with persistent mTBI symptoms and explore its effects on health-related outcomes.
Methodology: This feasibility study using a single-group pre-post mixed methods convergent parallel design was conducted remotely. Adults aged 18–65 years with a mTBI reporting persistent symptoms for ≥3 months were recruited. The 8-week remote progressive walking intervention aimed to increase the weekly number of steps walked by 40% based on a 1-week baseline measured by a Fitbit Inspire 2 activity monitor. Feasibility measures were about the intervention, its remote delivery, safety, and acceptability. Health-related outcomes were post-concussion symptoms, kinesiophobia, mood, sleep, fatigue, and quality of life. Semi-structured exit interviews were recorded and transcribed verbatim. Quantitative and qualitative data were analyzed separately, and results merged, compared, and contrasted. Descriptive statistics and paired samples t-tests were used. The qualitative analyses followed an iterative content analysis approach using reflexivity and triangulation of sources.
Results: Twenty adults (16 women) aged 42.5 ± 11.51 years with persisting symptoms for 9.25 ± 6.43 months participated, adhered to 94.38% of sessions, completed the intervention, and found it to be feasible, safe and acceptable. Participants increased weekly total number of steps walked (change = 14,886 ± 18,283; t = 3.55, p = 0.002). Severity of post-concussion symptoms (change = −6.42 ± 10.69; t = −2.62, p = 0.018), kinesiophobia (change = −5 ± 6.86; t = 3.18, p = 0.005), anxiety (change = −1.53 ± 3.01; t = −2.21, p = 0.04), and fatigue (change = −10.21 ± 10.20; t = −4.37, p < 0.001) were reduced, whilst quality of life improved (change = 10.58 ± 13.35; t = 3.46, p = 0.003). Participants' perceptions corroborate most quantitative results; they felt improved self-efficacy about physical activity and provided five key recommendations.
Discussion: This study demonstrates the feasibility, safety, and acceptability of the remote 8-week progressive walking intervention, a promising approach to reduce persisting symptoms, improve physical activity level health-related outcomes and quality of life of adults with persistent post-concussion symptoms following a mTBI.
Adults who sustain a mild traumatic brain injury (mTBI) can experience a range of physical, cognitive, and emotional post-concussion symptoms that persist and negatively impact their function and participation [e.g., work absenteeism, reduced physical activity (PA)] (1–4). Recent reviews and meta-analyses suggest that PA can help reduce persisting symptoms and fosters the return to normal activities (5–9). This evidence supports clinical practice guidelines and expert consensus on sport-related concussion that slow-to-recover adults should engage in PA as part of the management of their mTBI (10–12).
Among PA-based interventions delivered to adults with a mTBI, one of the most promoted approaches is symptom-limited low-to-moderate aerobic exercise performed five–seven times a week at an intensity representing 80% of the heart rate attained when symptoms are exacerbated during a graded exertion test, repeated every 2–3 weeks (13–16). However, there are several limitations associated with this approach. For instance, it requires regular testing of exercise intolerance, in-person supervision and precise monitoring of heart rate during exercise that may not be optimal for all adults with persisting symptoms (e.g., inactive, or aging adults). Indeed, this heterogenous population could experience several barriers to engage and follow this approach as they could be sedentary (17), fear-avoidant (18, 19) and may not have access to specialized equipment (e.g., treadmills, stationary bikes) or rehabilitation if living in a remote area or when it is limited due to sanitary restrictions (e.g., reduced service provision and increased waitlists).
An exercise as simple as walking is an aerobic-based PA accessible to most, that can be delivered remotely and has shown to improve perceived stress and mood of adults with mild, moderate, or severe TBIs living in the community (20). The home-based walking intervention studied by Bellon et al. (20) used a stepwise progressive approach using a pedometer to increase by 40% the total weekly steps walked after a 12-week intervention, an individualized progression that did not require symptom exacerbation to guide exercise progression. Although, this intervention incorporated telephone coaching, it required in-person testing before the intervention, and was not specifically designed for adults with a mTBI. Moreover, Bellon's study did not measure post-concussion symptoms and relevant mTBI health-related outcomes (e.g., anxiety, fatigue, sleep, quality of life) nor did it report on safety and participant acceptability.
In the context of the COVID-19 pandemic, we adapted Bellon's approach and designed a remote progressive walking intervention specifically for adults with persisting post-concussion symptoms of a mTBI. The aim of this study was to determine the feasibility, safety, and acceptability of this 8-week telehealth intervention, and to explore its effects on health-related outcomes.
This study was conducted entirely remotely and followed a single-group pre-post intervention using a mixed method convergent parallel design (21). In other words, we simultaneously collected different qualitative and quantitative data before, during and after the intervention, analyzed both sets of data separately, and combined and compared (e.g., triangulated) the results from these data sources to draw conclusions. The study was approved by the Center for Interdisciplinary Research in Rehabilitation of Greater Montreal (CRIR) Research Ethic Board (#CRIR-1516-1118).
Eligible participants were adults aged 18–65 years old reporting persistent post-concussion symptoms following a mTBI sustained ≥3 months and for ≤3 years before and whose names were on waitlists to receive outpatient rehabilitation at one of five public healthcare TBI specialized programs in Montréal and surrounding area, an urban region in Québec, Canada. To be on the waitlist of a specialized TBI rehabilitation program, participants had a diagnosis of a mTBI and were referred to the program by a physician. Participants had to speak English or French and have access to the internet, a web camera and a microphone on a computer, a smartphone, or a tablet with Bluetooth© able to support Zoom software (Zoom Video Communications Inc., USA provided by the Université de Montréal). Potential participants were excluded from the study if they (1) reported not feeling healthy enough to walk daily [informed by the Physical Activity Readiness Questionnaire (PAR-Q)], (2) reported an injury or a disease such as a sprain, a fracture or testing positive for COVID-19 during the study, or (3) were already following an aerobic exercise program. At all times during their participation in the study, participants could receive services from their doctor, allied health professionals (e.g., physiotherapist, occupational therapist, kinesiologist) and alternative health professionals (e.g., acupuncturists, massage therapists) working inside or outside the specialized program as long as no PA intervention was provided. Non-probabilistic convenience sampling was used until 20 participants were consecutively enrolled and initiated the intervention, a sample consistent with other feasibility studies of PA interventions for youth and children with mTBI (13, 22). Participants were recruited from May to October 2021 by persons independent from the research team from each specialized program who made initial contact calls to individuals on waitlists, briefly introducing the study and inquiring about interest in participating. Once potential participants demonstrated interest, they were contacted by telephone by the first author (CA) to confirm eligibility. An email describing the intervention including the consent form and a secured Zoom URL of the first scheduled session was then sent to each participant (T0). This session consisted of obtaining consent and demographic information through screen sharing, in addition to scheduling the period to obtain baseline walking data and planning the telehealth intervention sessions. Figure 1 reports the flow of participants in the study.

Figure 1. CONSORT diagram of the flow of participants in the study.
The 8-week walking intervention was remotely delivered and consisted of weekly telehealth sessions during which research assistants met with participants to individualize their walking progression and offer motivational support specific to individuals with a mTBI. The intervention aimed to increase the weekly number of steps walked, up to an additional 40% of the steps walked during the 1-week baseline measured with a Fitbit Inspire 2 PA monitor (Fitbit LLC, USA). This progression was inspired by the progression proposed by Bellon et al. (20). Specifically, participants were encouraged to follow a progression rule to increase the number of steps walked per week by 5% of the number of steps walked during baseline, and this was adapted weekly.
During weekly telehealth sessions, research assistants and participants worked collaboratively to establish individualized walking goals for the week informed by the potential obstacles and facilitators to walking perceived by the participants for each upcoming week. Participants could modulate the frequency, duration, distance, and speed of their walks to achieve their goals. To promote attainment of their walking goals, motivational strategies were provided (23). They were also educated about PA and mTBI (e.g., potential health benefits for mTBI symptoms, exercise intolerance principles), and encouraged to attain desired behaviors through feedback, and helped to identify strategies to achieve walking goals (e.g., goal setting, action planning). Participants were asked to record the frequency, the durations of their walks, and their ratings of perceived effort after voluntary walks in an electronic Word software-based (Microsoft Word, Microsoft, USA) walking log to support self-monitoring of their progress. Specific details about the intervention are provided in Supplementary Material I according to the Consensus on Exercise Reporting Template checklist (24).
For each participant, the intervention included 10 individual telehealth sessions supervised by trained research assistants, one session to initiate baseline measurement (T0), two sessions for questionnaire administration, pre and post intervention (T1 and T2), and seven weekly-scheduled sessions for data collection, weekly goal setting and motivational support. Not considered as part of the intervention, participants attended a 20-min instructional session about the use of their Fitbit (between T0 and T1), and an exit interview (T3) within one week after finishing the intervention.
The research assistants were the first author (CA), a doctoral student with over five years of clinical experience, and three students at the master's or undergraduate level in occupational therapy or athletic therapy. Supervised by a senior researcher (BS), the doctoral student provided 20 h of training to the other students to ensure standard delivery of the walking intervention, administration of the measurement tools, data collection and data entry. To ensure intervention and protocol fidelity, pilot testing of the intervention and assessment procedures (e.g., consent, wearing Fitbit, questionnaire completion, exit interview) was conducted with members of the research team. Pilot data were not included in the study.
Participant demographic data (see Table 1) were collected at T0 and included questions about self-reported level of PA (e.g., number of days performing more than 30 min of PA at an intensity that made them breathe harder than usual, the number of minutes of PA per week, and self-rated level of fitness). Questionnaires were administrated at the beginning (T1) and end of the 8-week intervention (T2) followed by an exit interview (T3). Demographic information and questionnaire responses were collected using Zoom screen sharing and annotation tools. The total number of mTBI sustained in one's life was self-reported. Within four days of obtaining consent, participants received in the mail their Fitbit Inspire 2 activity monitor and were invited via email to attend the Fitbit instructional session (between T0 and T1) during which they were instructed how to download, install, and perform initial set-up of the Fitbit application. They were asked to wear the watch on their non-dominant wrist and go about their days as usual for one week to complete the baseline (T0–T1). A piece of masking tape was placed on the watch face to impede participants from viewing their daily number of steps during this initial week and they were instructed to remove the tape only once the intervention began (T1). For the study duration, participants were instructed to always wear the watch but could remove it when bathing or while it charged. A checklist was also provided with the mail package to remind participants about these instructions.
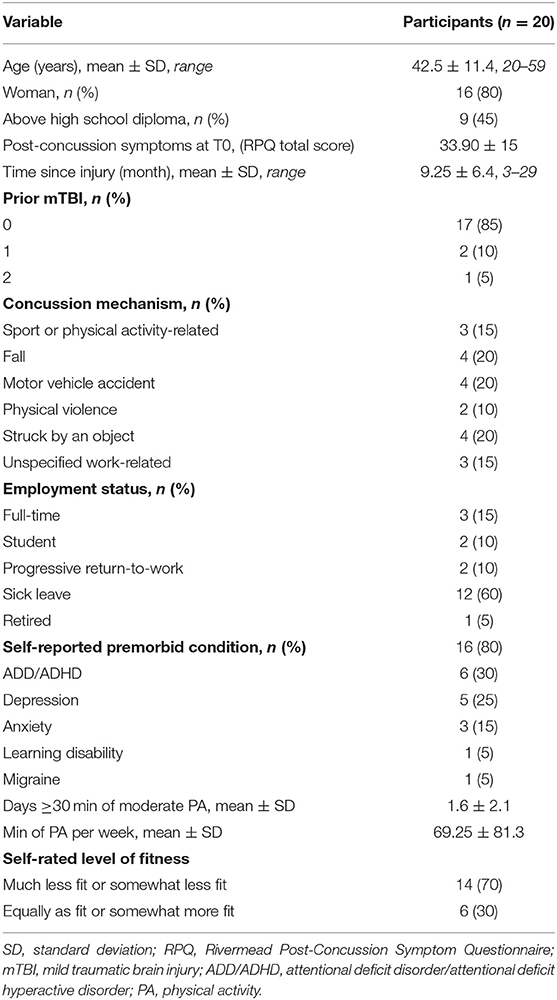
Table 1. Demographic characteristics of participants receiving the telehealth progressive walking intervention (n = 20).
Each week, participants received a personal secured Zoom link by email connecting them to a 30-min one-on-one telehealth virtual meeting with their assigned research assistant. A typical telehealth session unfolded as follows: Participants shared their walking log and synchronized their Fitbit Inspire 2 with the Fitbit application, allowing the research assistant to access steps data. The research assistant and participant then discussed the weekly number of steps, goal attainment, identified actual and potential barriers and facilitators (e.g., fatigue, busy schedule, motivation) and planned new goals for the upcoming week. The time of the next appointment was confirmed and an email containing an updated walking log, new weekly goals and a Zoom link was sent to the participants by email. Weekly reminders were sent by email 24 h before each appointment. At the end of each telehealth session, the research assistant recorded in a journal if participants received health services, if they reported adverse events, if any technological issues occurred during the session and general comments participants shared about the intervention. If an adverse event was reported either during a telehealth session, with a phone call or an email, research assistants were instructed to tell the participant to seek medical attention, as needed. If medical attention was required, the plan was to maintain contact (by telephone or email) with the participant until he or she felt the consequences related to the adverse event were under control. Depending on the severity of the adverse event, a decision to continue or withdraw from the study would be made by the research team.
An exit interview (T3) with each participant was conducted remotely by CA. Using an interview guide based on the acceptability questionnaire developed for this study (see below), participants were asked five open-ended questions about their overall satisfaction with the intervention delivery and the telehealth experience. Interviews were recorded using built-in Zoom recording software and transcribed verbatim.
Feasibility measures and feasibility level criteria, set a priori when possible and aligned with prior research for determining feasibility of PA interventions (13, 25) included: Drop-out rate, measured as three or more missed telehealth sessions or a participant declining to continue the intervention (acceptable drop-out rate set at ≤20%); Adherence to the telehealth sessions (target attendance set at ≥80% of the telehealth sessions for all participants); Number of modifications to scheduled telehealth sessions; Number of adaptations of telehealth sessions; Type of device used to support the telehealth platform; Number of internet connection, video and audio issues; Number of Zoom platform issues; Number of Fitbit monitor issues and; Walking log usage, determined as the number of logs completed and shared with the research team (≥80% of the walking logs). Safety was measured as the number of minor (e.g., fall, minor injury, perceived exacerbation of symptoms due to walking) and major adverse events (e.g., subsequent mTBI, an emergency department visit) resulting from walking. Finally, the acceptability of the intervention with respect to its different characteristics (e.g., duration, frequency of meetings, format, research assistants' expertise and know-how), telehealth setting (e.g., Zoom connection quality), Fitbit activity monitor, perceived impacts of the intervention were assessed using a 17-item 5-point scale questionnaire (1 = strongly disagree, 2 = disagree, 3 = neither agree nor disagree, 4 = agree, 5 = strongly agree) designed for this study (see Supplementary Material II).
The exploratory health-related outcomes included:
• Steps walked over seven days (i.e., number of steps walked per 7 × 24-h periods), measured with a wrist-worn Fitbit Inspire 2 watch, a validated PA monitoring technology in adult population with TBI (26). Additionally, self-reported weekly number of walks, walk duration, and the rating of perceived effort (RPE) using the Borg rating of perceived effort scale, a 0–10-point scale commonly used for individuals with a mTBI (13, 27–29), were recorded by participants in their electronic walking log.
• Post-concussion symptoms, assessed with the Rivermead Post-Concussion Symptom Questionnaire (RPQ), a self-reported validated and reliable 16-item questionnaire using a 5-point scale (total score range = 0–64) (30). Three sub-scores can be calculated, namely cognitive, somatic, and affective symptoms. A higher score indicates a greater number or intensity of symptoms.
• Kinesiophobia, measured by the Tampa Kinesiophobia Scale (TSK-13) a self-reported questionnaire validated for adults with a mTBI including 13 items measured on a 4-point scale (total score range = 13–52) (31). Two sub-scores can be calculated: activity avoidance and somatic focus (i.e., fear of pain and (re)injury). A higher score indicates greater fear.
• Mood, measured with the Hospital Anxiety and Depression Scale (HADS), a self-reported questionnaire validated for adults with a mTBI including 14 items measures using a 4-point scale (total score range = 0–42) (32, 33). Two sub-scores can be calculated representing: depression and anxiety. A higher score represents a higher level of symptoms.
• Sleep quality over the past month, assessed using the Pittsburgh Sleep Quality Index (PSQI), a self-reported questionnaire validated for individuals with a TBI containing 19 items measuring seven domains of sleep on a 4-point scale (total score range = 0–21) (34). A higher score represents poorer perceived sleep quality.
• Fatigue, measured with the Multidimensional Fatigue Inventory (MFI) a self-reported questionnaire validated for adults with a TBI containing 20 items measured using 5-point scale (total score range = 20–100) (35, 36). Five sub-scores are calculated: general, physical, mental, and emotional fatigue and vigor. A higher score indicates a greater level of fatigue.
• Health-related quality of life, measured with the Quality of Life after Brain Injury (QOLIBRI), a self-report questionnaire validated for individuals with a mTBI comprised of 37 items measured using a 5-point scale (total score reported as a percentage) (37). Six sub-scores can be calculated: cognitive, self-perception, life, relational, emotional, and physical satisfaction. A higher score represents a better quality of life.
This mixed-method study used different methodological techniques to gather quantitative and qualitative data. The analyses of each type of data were performed separately and results from these data sources were triangulated.
Descriptive statistics were performed for demographic, feasibility, safety, acceptability, and health-related outcome data. Visual inspection was performed for distribution and completeness of feasibility and health-related outcomes. Satisfaction questionnaire scores were transformed into percentages. Due to the exploratory nature of the study, paired sample Student's t-tests were used to analyze changes in exploratory health-related outcomes (e.g., steps walked, post-concussion symptoms, kinesiophobia, mood, sleep, fatigue, health-related quality of life) before (T1) and after the 8-week intervention (T2). Sensitivity analyses based on the Wilcoxon signed-ranked test were performed and conclusions were coherent with those of the Student's t-tests, except for the mental fatigue sub score of the MFI standardized questionnaire (MFI-Mental). Moreover, using paired sample Student's t-test enables the reporting of Cohen's d effect sizes (38). Quantitative analyses were performed using SAS software (SAS 9.4, SAS Institute, Inc., USA).
Qualitative analyses of exit interviews and journals kept by each research assistant were performed principally by CA, MK and BH and supervised by BS using Nvivo software (Nvivo 1.6, QSR International Inc., USA). The iterative analysis process followed Miles et al. (39) analysis approach. A coding dictionary derived from the interview guide was produced to inform the first cycle of coding. The coding dictionary evolved as transcripts were coded independently and verified by a second analyst. Suggested changes or adjustments were resolved through discussion between analysts and the first author CA. A second cycle of coding determined broader categories. To enhance trustworthiness, triangulation of the broader categories with data recorded in the research assistants' journals provided enriched understanding of participants' experiences but did not modify the overarching categories. Annotations (jottings), reflexive notes and analytical memos were documented thorough the analysis. A search for convergent, divergent, and contradictory information within categories was undertaken and reported (39).
The results of the quantitative and qualitative analysis related to each other were merged, compared, and contrasted to provide an overall interpretation of the feasibility, safety, acceptability, and impacts on health-related outcomes (21). Perspectives of participants including converging, divergent and contrasting results are reported following related quantitative results.
Demographic characteristics of the participants are in Table 1. Twenty French-speaking adults on waitlists of three outpatient rehabilitation programs participated in the 8-week intervention. They each completed the intervention, but one participant only provided the number of steps recorded during week 8 by the Fitbit and did not complete the self-reported questionnaires (T2) or the exit interview (T3). At the beginning of the intervention (T1), all participants reported having symptoms of fatigue, 95% reported feeling slow and being sensitive to noise, and 90% reported having headaches, light sensitivity and difficulty to concentrate and remember. Nineteen participants reported having received health services during the intervention by either a medical doctor (n = 3), an allied health professional (n = 16), or an alternative health professional (n = 5). Following the qualitative content analysis, perspectives of participants were grouped in five broader categories: feasibility, safety, acceptability, impacts on health-related outcomes, and recommendations to improve the walking intervention.
All participants completed the intervention (0 drop-outs). Adherence to the telehealth sessions was 94.38%, 25 sessions were rescheduled, and 10 no-shows were recorded. Thirty-six sessions (18.94 %) diverged from the intervention protocol and needed adaptations (e.g., used telephone, session longer than 45 min, vacation). Twenty-four computer-related technological issues, 33 Zoom issues, and 53 Fitbit activity monitor issues were recorded but these issues were dealt with during the session and did not prevent completion of any session. Visual inspection of the number of steps data revealed that one participant did not wear his watch for three days during week 8 (T2) and was therefore removed from the analysis of the weekly steps. Table 2 provides more details about the feasibility measures.
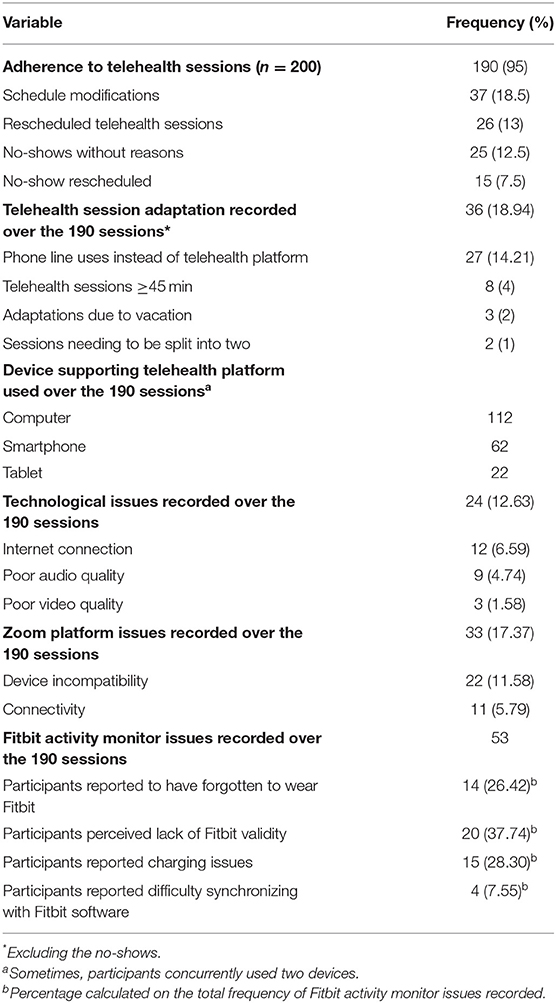
Table 2. Feasibility measures of the telehealth progressive walking intervention (n = 20).
Walking logs were completed by participants following 69.44% of the sessions. Self-reported information on walking logs was however sparse making statistical analysis difficult: 14 participants provided information to compare walk frequencies between week 1 and 8, eight participants for the duration of walks, and seven participants about their rating of perceived effort. Perceptions of participants converged with quantitative feasibility results providing insights about the intervention and issues experienced. Participants found the telehealth progressive walking intervention feasible and felt the quality of the telehealth sessions was good; it was simple and quick to communicate with the research team by email. Technical assistance offered by the research team was good and instructions provided throughout the intervention were clear even when technological issues occurred. Using the Fitbit activity monitor and its online application were considered feasible and helpful for tracking their PA even if issues or dissatisfaction were expressed about the perceived reliability of the Fitbit's step counts measurement, the relatively frequent charging of the watch and its lack of screen brightness outside. The walking log was considered useful to track symptoms and walking progression, but some people experienced difficulties completing the walking log because of their visual symptoms or the electronic format.
We recorded 21 adverse events during the study, 19 of which were exacerbation of post-concussion symptoms after a walk and two musculoskeletal (e.g., knee pain, and calf cramp). No event required medical attention, and all were resolved without complications. Experience of participants converged with the overall safety of the intervention regarding the low frequency of musculoskeletal minor adverse events, contextualized symptom exacerbation, and perceived potential hazards. Indeed, participants considered the walking a safe activity and appreciated that the individualized progression and adapted weekly goals did not put them at risk of overexerting themselves or increasing their symptoms. Some participants felt their safety was at risk (e.g., risk of fall) in the presence of symptoms of dizziness and light sensitivity when walking on uneven terrain and when they walked in an area considered unsafe, or during inclement weather (e.g., storm, heatwave).
Overall acceptability was high. The percentage of participants who responded 4 (agree) or 5 (strongly agree) to all items about the intervention itself was 79%, the remote delivery was 68%, the instrumentation and tools used was 74%, and the perceived health benefits was 79%. All would recommend the intervention to persons with a mTBI. Converging with these results, during the exit interview participants shared their appreciation of the intervention, its telehealth format, its 8-week duration, its weekly frequency, and the relatively short duration of telehealth sessions (about 30 min.). Although some participants found the experience more time consuming than initially expected (e.g., data collection, time to complete walking logs, number of telehealth sessions), participating in the research was a positive experience for everyone; they found the data collected helped them better understand persisting post-concussion symptoms. Research assistants were considered knowledgeable motivators, flexible with scheduling and able to adapt intervention progression according to individual needs. Participants reported wanting the telehealth approach to be embedded in the public healthcare system and would have liked to have received a similar walking program earlier after their injury. They reported the pandemic enhanced their readiness to participate in a telehealth intervention and found themselves familiar/comfortable with the technology used (i.e., Zoom, email exchanges, Fitbit, and its online application). Although participants generally appreciated the intervention in the format given, five areas of improvement emerging from the interviews were found. Table 3 reports main recommendations and significant excerpts from participants.
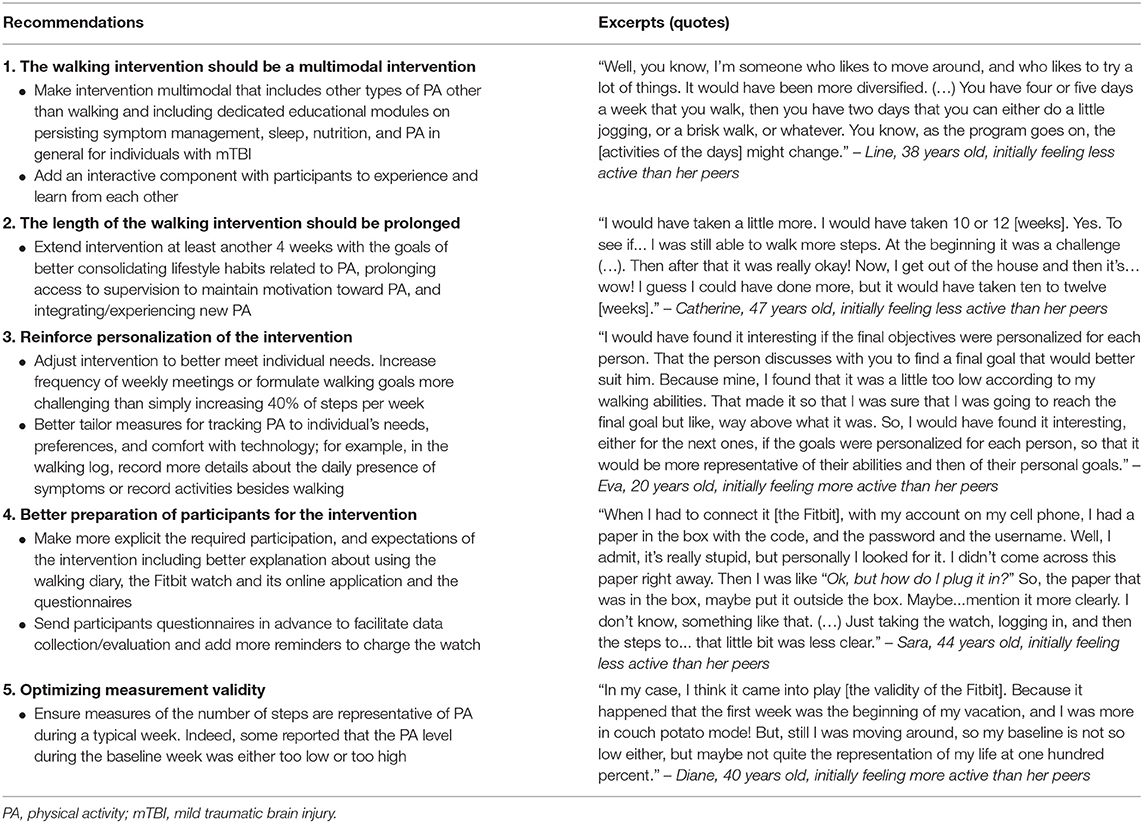
Table 3. Participants' recommendations and excerpts to improve the remotely delivered interventions (n = 19).
Participants significantly (p < 0.01) increased their weekly total number of steps and their average daily number of steps after the intervention, during the weekday and weekends (see Table 4) and reported the intervention impacted positively their participation. In fact, not only did they report an increased number and duration of their walks, they also spent more time in work-related and leisure activities. For example, some participants reported starting to cycle, swim or paddle board and having improved their ability to work on the computer because of screen habituation during the one-on-one telehealth session. Often, participants included their friends and their family during their walks or other PA resulting in strengthened relationships with their friends and family.
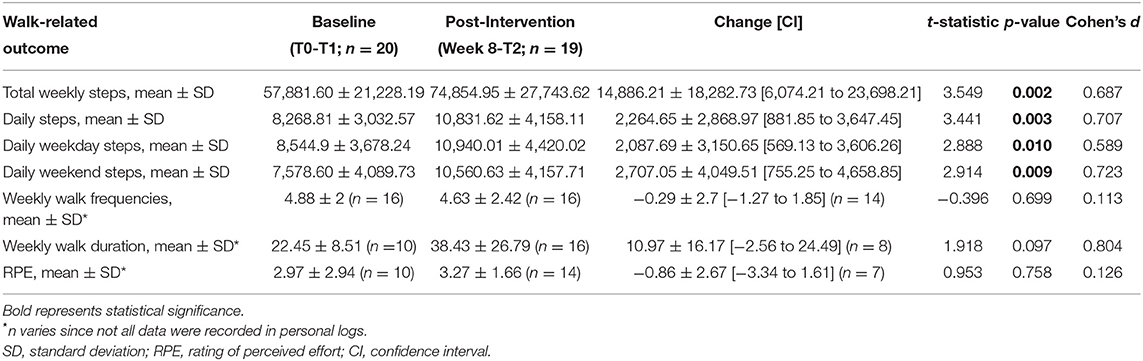
Table 4. Descriptive statistics, paired sample t-test and effect size of steps walked, walk frequencies and duration, and perceived effort of the telehealth progressive walking intervention (n = 20).
Paired sample t-tests indicated that post-concussion symptoms (RPQ-Total), kinesiophobia (TSK-13-Total), anxiety (HADS-Anxiety), and fatigue (MFI-Total) reduced post-intervention (p-values for all four measures = <0.05), while health-related quality of life (QOLIBRI-Total) improved (p = 0.003). Initial and final scores for each questionnaire and their associated subscales, confidence intervals, t-statistics, p-values, and Cohen's d, are provided in Table 5. Similarly, participants qualitatively reported a reduction in their fatigue, their cognitive, emotional, and physical symptoms of mTBI, and that their overall physical condition improved over the course of the intervention (i.e., they had stronger legs and improved cardiorespiratory function). Converging with the quantitative results, they felt the intervention improved some cognitive abilities (e.g., sustained attention), their overall mood, sleep quality (e.g., reduced stress, irritability), and reduced their pain. Some participants reported the intervention helped them lose weight.
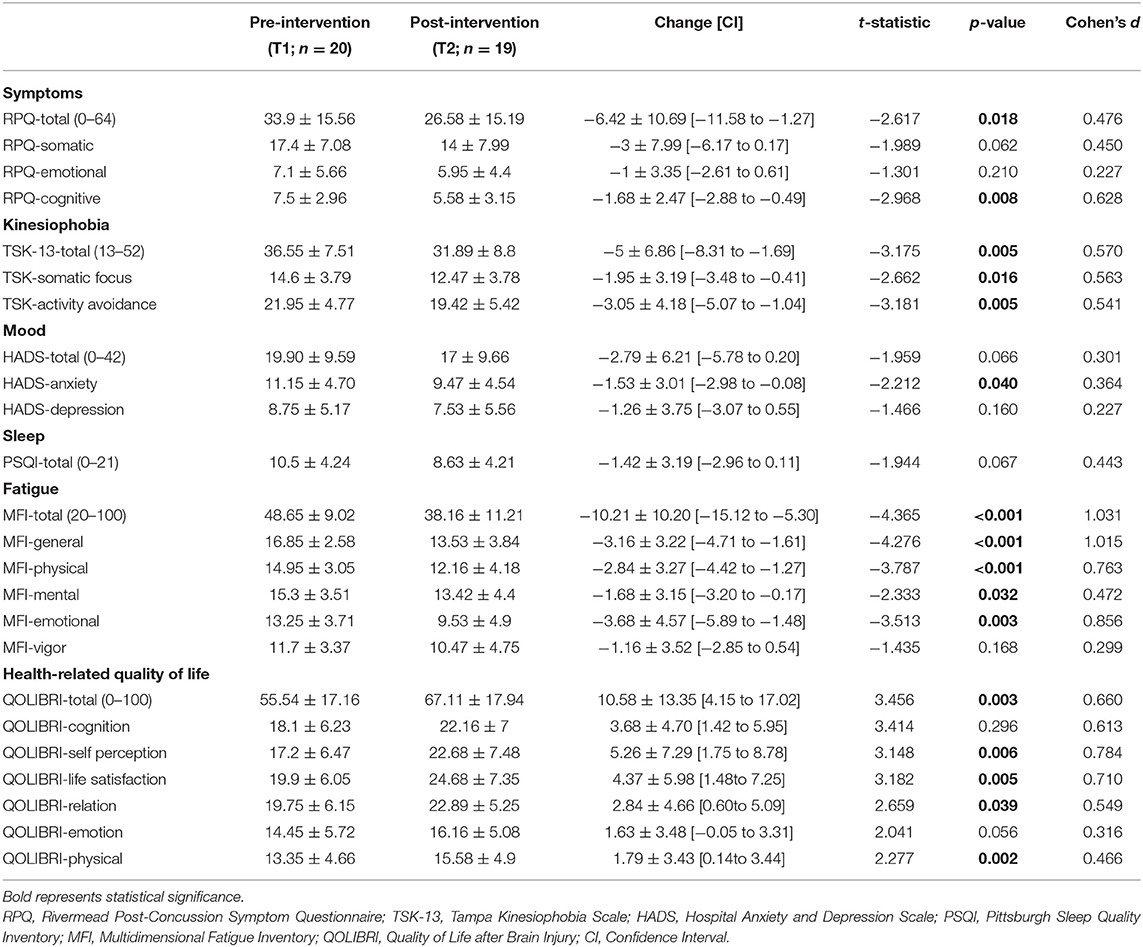
Table 5. Descriptive statistics, paired sample t-test and effect size of post-concussion symptoms, kinesiophobia, mood, sleep, fatigue, and health-related quality of life exploratory health-related outcomes (n = 20).
Additionally, the participants reported improved self-efficacy related to persisting post-concussion symptoms management and PA. They learned more about mTBI, its associated symptoms, the general health benefits of PA and how PA could specifically help improve their mTBI. They reported an increased sense that PA could be beneficial in managing their persisting symptoms and felt that, sometimes, a single walk made them feel better. Helped by the research assistants, participants felt supported to engage in a reflective process about themselves, their physical capacities, symptoms status, PA goals, and self-management skills of symptoms (e.g., energy level, pain). They felt they had a better balance in their lives because the intervention provided structure to their day, contributing to improved personal time management. They felt overall positive impacts on motivation, self-esteem, self-confidence, enjoyment, and well-being due to the walking intervention.
This paper reports on a remotely delivered 8-week progressive walking intervention for adults with persisting symptoms of a mTBI. The results showed the intervention was feasible, safe, and acceptable by adults waiting to receive outpatient rehabilitation. It thus contributes to emerging telehealth approaches for use with individuals with a mTBI (40, 41).
The results suggest the intervention meets the needs of adults with a mTBI because participants were heavily engaged in the intervention. Indeed, they reported being satisfied with all its components and shared they would have liked to have received it earlier in their recovery process. Moreover, there were no drop-outs, and the adherence was similar to that found for other PA interventions (25, 42), and higher than most interventions delivered to individuals with a mTBI (28, 43–46). Most studies about PA intervention for individuals with a mTBI do not even report adherence (7).
Why the participants were so appreciative of the intervention remains somewhat unclear. We hypothesize that the type of PA offered (i.e., low intensity PA in a progressive manner) was probably very appropriate for the participants who were found to have PA levels below those recommended by the Canadian Physical Activity Guidelines (e.g., 150 min of moderate to vigorous aerobic PA per week) (47). Following the intervention, their weekly steps walked, and the daily average steps walked approached numbers similar to those of healthy individuals (48). Walking, or moving around, is essential to participation in real life situations in community, social and civic life, and appears to be non-threatening PA for adults who are slow to recover from a mTBI. However, it remains unclear if walking will remain an activity of choice outside of a pandemic context.
Perhaps the participants appreciated the intervention because the research assistants provided motivational support using behavioral change techniques improving participants' motivation and self-efficacy to be more active (23). Contained in weekly telehealth sessions of <30 min, we provided information about PA and their mTBI, helped with goal setting and action planning, provided feedback on behavior, thus supporting self-monitoring and habit formation to help participants walk more. Little is known about self-efficacy concerning PA among adults with a concussion, however evidence suggests that self-efficacy of self-management behaviors influences participation, life satisfaction and health-related quality of life in persons with newly acquired brain injury, including TBI (49). Moreover, Gagnon et al. (50), found that self-efficacy about PA in children was reduced after a concussion (50). In our recent scoping review of PA interventions for individuals with a mTBI, only about 22% of studies (n = 8/35) on interventions for individuals with a mTBI reported using motivational support in conjunction with a PA intervention (7). Our study suggests the importance of providing motivational strategies when delivering a PA intervention to adults with a mTBI.
It is conceivable that participants appreciated the intervention simply because they felt better. In fact, they reported reduced persisting post-concussion symptoms, several improved health-related outcomes, and their quality of life. Interestingly, using a mixed methods design allowed identification of some divergent results between self-reported questionnaires and participant experiences. For example, participants subjectively reported improved sleep following the intervention, but changes in the PSQI questionnaire total scores did not differ significantly. Also, some reported pain reduction, while others felt they improved their physical fitness and even lost weight. Since walking is an aerobic PA performed at an intensity typically lower than most existing approaches offered to individuals with a mTBI (7), this suggests that the mechanisms underlying improvements in persisting symptoms may not only be related to physiological effects driven by more intense aerobic exercises (e.g., jogging, biking, running), but also about doing exercise itself, an activity often considered pleasurable and associated with leisure-time activity. Given the lack of a control group in this feasibility study, we cannot presume the improvement in symptom status and health-related outcomes are solely related to the PA intervention.
In terms of safety, although participants reported symptom exacerbations after some walking, they reported symptoms resolved by themselves, and no one wanted to drop-out or stop walking because of this. This suggests the walking intervention is no less safe than other PA interventions for individuals with a mTBI, which often report temporary increase in post-concussion symptoms because of exercising (13, 41, 44, 51).
Although the intervention was deemed beneficial, feasible and safe, there were some challenges. First, the rescheduling of telehealth sessions was resource intensive. Because most of these participants were not working or at school at the time, we were often able to reschedule appointments during weekdays, but sometimes scheduling was only possible in the evening and weekends. This could be a challenge when delivering this intervention in either a public or private healthcare setting. Also, the Fitbit watches required troubleshooting by the research assistants throughout the intervention. Before delivering this intervention, research assistants were trained and became familiar with the most common functions on the Fitbit and with its application. This training proved essential as it ensured research assistants could answer most questions and provide technical support. Since participants were not convinced the watches were able to accurately record their PA, extra time was required to teach participants about how the Fitbit detects steps (how it works). Third, although the walking logs were completed almost 70% of the time, their completeness was greatly variable. This made using the walking logs difficult during the intervention to inform walking progression and made it challenging to perform statistical analysis. As some participants reported the walking log to be helpful for self-monitoring progress, and because research assistants needed a measurement of steps to inform future progression, in future research, we recommend dropping the participant Word-based walking log and using only the Fitbit application as the walking log. Indeed, the application has a built-in detailed log that automatically records the daily step count, the frequency, duration, and type of PA, and has the options for recording extra notes by the participants. For example, with the Fitbit, they could note symptom status before and after a walk, or other PA. Additionally, ecological momentary assessments such as sending text messages, or emails containing questions about their symptom status or their perceived effort at planned or random times, could be used to reduce recall bias and improve ecological validity (52). The walking log may be helpful clinically to support self-management of PA and symptoms.
Despite these challenges, this intervention appears to be a promising relatively low-cost approach to promote participation, reduce post-concussion symptoms and improve health-related outcomes among adults with a mTBI. However, we do not know if the changes in health-related outcomes measured with the standardized questionnaires met the minimal clinical important difference because of the lack of consensus about this metric for the instruments when used with adults with a mTBI. Nonetheless, this intervention could be helpful to gradually increase PA level of individuals less active than most, potentially deconditioned and who may want to avoid PA. This telehealth approach can be used to deliver a PA intervention to individuals that cannot access gym equipment, live in remote areas or as a starting point for individuals that experience kinesiophobia (e.g., fear-avoidant). The suggestions gathered during the interviews with our participants about including other modalities, lengthening the intervention, and reinforcing the personalization of the intervention could help further tailor the intervention to needs of adults with a mTBI. Considerations of these recommendations when adapting or implementing this intervention as part of outpatient rehabilitation services is warranted.
The results of this study should be interpreted with caution due to some limitations. First, although the Fitbit technology is valid to measures steps while walking (26), it is somewhat challenging to use step counts when it is worn during a 24-h period. Participants often shared their concerns about the accuracy of the watch to measure steps while they performed other activities reinforcing that the Fitbit technology may have accuracy issues in “free-living settings” (53). Second, the study is at risk for selection bias. Participants were consecutively recruited in a non-probabilistic manner from different waitlists and about 50% of those contacted declined to participate. Study participants may have been more motivated than most and thus not be representative of the heterogeneous adult population of persons with mTBI. Although the sample comprised mostly of woman (80%) differs from those included in a scoping review of studies on PA for individuals with a mTBI (7), these results could contribute to better understanding the perspectives of women with a mTBI participating in a PA intervention. The small sample and the wide range in time since injury (i.e., heterogeneity) limit the generalizability of the findings. The range of time since injury, however, represents the clinical reality of TBI specialized programs involved in our study and highlights that a telehealth PA intervention is a promising approach for individuals with different times since injury. Third, neither participants or research assistants were blinded to the intervention which may have influenced reporting of symptoms, and outcome measurements. To minimize this bias, the research assistants were trained, and they repeatedly informed the participants that the main objective of the study was to determine the feasibility and that criticism and transparency about the intervention was important. Fourth, we cannot draw conclusions about the intervention's effectiveness on health-related outcomes due to the lack of a control group and because of the health services most participants received either from their doctors, their allied or alternative health professionals. No participant received another PA intervention. Furthermore, we cannot conclude whether improvements reported by participants are maintained over time because of the lack of follow-up measures. A future randomized controlled trial including longer term follow-up measures could determine the extent to which this telehealth PA intervention influences post-concussion symptoms, health-related outcomes, and quality of life.
A telehealth progressive walking intervention for adults with persisting symptoms of a concussion is feasible, safe, and acceptable. Participants of the intervention were highly satisfied and provided recommendations to improve the walking intervention. An 8-week walking intervention may be appropriate to integrate into the management of adults with an mTBI. More controlled research with lower risks of bias is warranted in the future to determine the effectiveness of this intervention to increase PA and to evaluate its effects on health-related outcomes.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
This study involving human participants was reviewed and approved by the Center for Interdisciplinary Research in Rehabilitation of Greater Montreal (CRIR) Research Ethics Board. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
CA, BS, IG, EG, and MM conceived, designed the study, and obtained funding. BS oversaw data collection of both quantitative and qualitative analyses. CA coordinated data collection, performed the analysis, drafted the manuscript, and submitted the final version once validated by co-authors. MK and BH supported data collection and helped with quantitative data preparation and qualitative analysis. BS, IG, EG, MM, MK, and BH provided critical revisions of the manuscript and approved the final version. All authors reviewed and approved the final manuscript submitted.
This research and the open access publication fees has been supported by the Fonds de Recherche du Québec en Santé (FRQS). CA received a bursary of Excellence from the École de Réadaptation of the Université de Montréal.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank all participants, the research coordinators (Manon Parisien, Stéphanie Luna, Lynda Cloutier, Jenny Laperriere, Andréanne Guindon) and participating clinicians of all five specialized rehabilitation program with whom we partnered to ensure the delivery of this innovative intervention to their clientele. We also thank to Nicolas Vaillancourt for his involvement in the study preparation and his technological support.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fresc.2022.898804/full#supplementary-material
1. Fineblit S, Selci E, Loewen H, Ellis M, Russell K. Health-related quality of life after pediatric mild traumatic brain injury/concussion: a systematic review. J Neurotrauma. (2016) 33:1561–8. doi: 10.1089/neu.2015.4292
2. Voormolen DC, Polinder S, Von Steinbuechel N, Vos PE, Cnossen MC, Haagsma JA. The association between post-concussion symptoms and health-related quality of life in patients with mild traumatic brain injury. Injury. (2019) 50:1068–74. doi: 10.1016/j.injury.2018.12.002
3. Cooksley R, Maguire E, Lannin NA, Unsworth CA, Farquhar M, Galea C, et al. Persistent symptoms and activity changes three months after mild traumatic brain injury. Aust Occup Ther J. (2018) 65:168–75. doi: 10.1111/1440-1630.12457
4. Perroux M, Lefebvre H, Levert M-J, Malo D. Besoins perçus et participation sociale des personnes ayant un traumatisme crânien léger. Santé Publique. (2013) 25:728. doi: 10.3917/spub.136.0719
5. Lal A, Kolakowsky-Hayner SA, Ghajar J, Balamane M. The effect of physical exercise after a concussion: a systematic review and meta-analysis. Am J Sports Med. (2018) 46:743–52. doi: 10.1177/0363546517706137
6. Haider MN, Bezherano I, Wertheimer A, Siddiqui AH, Horn EC, Willer BS, et al. Exercise for sport-related concussion and persistent postconcussive symptoms. Sports Health. (2020) 13:154–60. doi: 10.1177/1941738120946015
7. Alarie C, Gagnon I, Quilico E, Teel E, Swaine B. Physical activity interventions for individuals with a mild traumatic brain injury: a scoping review. J Head Trauma Rehabil. (2021) 36:205–23. doi: 10.1097/HTR.0000000000000639
8. World Health Organization. International Classification of Functioning, Disability and Health: ICF. Geneva: World Health Organization (1997).
9. Langevin P, Frémont P, Fait P, Dubé M-O, Bertrand-Charette M, Roy J-S. Aerobic exercise for sport-related concussion: a systematic review and meta-analysis. Med Sci Sports Exerc. (2020) 52:2491–99. doi: 10.1249/MSS.0000000000002402
10. Eapen BC, Bowles AO, Sall J, Lang AE, Hoppes CW, Stout KC, et al. The management and rehabilitation of post-acute mild traumatic brain injury. Brain Injury. (2022) 1–10. doi: 10.1080/02699052.2022.2033848
11. Ontario Neurotrauma Foundation. Guideline For Concussion/Mild Traumatic Brain Injury & Persistent Symptoms 3rd Edition, For Adults Over 18 Years Of Age. Toronto, ON: Neurotrauma Fondation (ONF) (2018).
12. McCrory P, Meeuwisse W, Dvorak J, Aubry M, Bailes J, Broglio S, et al. Consensus statement on concussion in sport—the 5th international conference on concussion in sport held in Berlin, October 2016. Br J Sports Med. (2017) 51:838–47.
13. Leddy JJ, Kozlowski K, Donnelly JP, Pendergast DR, Epstein LH, Willer B, et al. preliminary study of subsymptom threshold exercise training for refractory post-concussion syndrome. Clin J Sport Med. (2010) 20:21–7. doi: 10.1097/JSM.0b013e3181c6c22c
14. Bezherano I, Haider MN, Willer BS, Leddy JJ. Practical management: prescribing subsymptom threshold aerobic exercise for sport-related concussion in the outpatient setting. Clin J Sport Med. (2021) 31:465–8. doi: 10.1097/JSM.0000000000000809
15. Moore BM, Adams JT, Barakatt E. Outcomes following a vestibular rehabilitation and aerobic training program to address persistent post-concussion symptoms an exploratory study. J Allied Health. (2016) 45:59E–68E. Available online at: https://www.ingentaconnect.com/contentone/asahp/jah/2016/00000045/00000004/art00012
16. Mercier LJ, Fung TS, Harris AD, Dukelow SP, Debert CT. Improving symptom burden in adults with persistent post-concussive symptoms: a randomized aerobic exercise trial protocol. BMC Neurol. (2020). doi: 10.1186/s12883-020-1622-x
17. Mercier LJ, Kowalski K, Fung TS, Joyce JM, Yeates KO, Debert CT. Characterizing physical activity and sedentary behavior in adults with persistent postconcussive symptoms after mild traumatic brain injury. Arch Phys Med Rehabil. (2021) 102:1918–25.e1. doi: 10.1016/j.apmr.2021.05.002
18. Silverberg N, Cassetta B. Correlates of fear avoidance behavior after mild traumatic brain injury. Arch Phys Med Rehabil. (2019) 100:e172. doi: 10.1016/j.apmr.2019.10.029
19. Silverberg ND, Panenka WJ, Iverson GL. Fear avoidance and clinical outcomes from mild traumatic brain injury. J neurotrauma. (2018) 35:1864–73. doi: 10.1089/neu.2018.5662
20. Bellon K, Kolakowsky-Hayner S, Wright J, Huie H, Toda K, Bushnik T, et al. A home-based walking study to ameliorate perceived stress and depressive symptoms in people with a traumatic brain injury. Brain Inj. (2015) 29:313–9. doi: 10.3109/02699052.2014.974670
21. Edmonds WA, Kennedy TD. An Applied Guide to Research Designs: Quantitative, Qualitative, and Mixed Methods. Thousand Oaks, CA: SAGE Publications (2017). doi: 10.4135/9781071802779
22. Chan C, Iverson GL, Purtzki J, Wong K, Kwan V, Gagnon I, et al. Safety of active rehabilitation for persistent symptoms after pediatric sport-related concussion: a randomized controlled trial. Arch Phys Med Rehabil. (2018) 99:242–9. doi: 10.1016/j.apmr.2017.09.108
23. Michie S, Richardson M, Johnston M, Abraham C, Francis J, Hardeman W, et al. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med. (2013) 46:81–95. doi: 10.1007/s12160-013-9486-6
24. Slade SC, Dionne CE, Underwood M, Buchbinder R. Consensus on Exercise Reporting Template (CERT): explanation and elaboration statement. Br J Sports Med. (2016) 50:1428–37. doi: 10.1136/bjsports-2016-096651
25. Chin LM, Chan L, Woolstenhulme JG, Christensen EJ, Shenouda CN, Keyser RE. Improved cardiorespiratory fitness with aerobic exercise training in individuals with traumatic brain injury. J Head Trauma Rehabil. (2015) 30:382. doi: 10.1097/HTR.0000000000000062
26. Fulk GD, Combs SA, Danks KA, Nirider CD, Raja B, Reisman DS. Accuracy of 2 activity monitors in detecting steps in people with stroke and traumatic brain injury. Phys Ther. (2014) 94:222–9. doi: 10.2522/ptj.20120525
27. Leddy JJ, Baker JG, Kozlowski K, Bisson L, Willer B. Reliability of a graded exercise test for assessing recovery from concussion. Clin J Sport Med. (2011) 21:89–94. doi: 10.1097/JSM.0b013e3181fdc721
28. Leddy JJ, Haider MN, Ellis MJ, Mannix R, Darling SR, Freitas MS, et al. Early subthreshold aerobic exercise for sport-related concussion: a randomized clinical trial. JAMA Pediatr. (2019) 173:319–25. doi: 10.1001/jamapediatrics.2018.4397
29. Borg G. Borg's Rating of Perceived Exertion and Pain Scales. Champaign, IL: Human Kinetics. (1998).
30. King NS, Crawford S, Wenden FJ, Moss NEG, Wade DT. The Rivermead Post Concussion Symptoms Questionnaire: a measure of symptoms commonly experienced after head injury and its reliability. J Neurol. (1995) 242:587–92. doi: 10.1007/BF00868811
31. Wijenberg MLM, Stapert SZ, Verbunt JA, Ponsford JL, Van Heugten CM. Does the fear avoidance model explain persistent symptoms after traumatic brain injury? Brain Inj. (2017) 31:1597–604. doi: 10.1080/02699052.2017.1366551
32. Roberge P, Doré I, Menear M, Chartrand É, Ciampi A, Duhoux A, et al. A psychometric evaluation of the French Canadian version of the Hospital Anxiety and Depression Scale in a large primary care population. J Affect Disord. (2013) 147:171–9. doi: 10.1016/j.jad.2012.10.029
33. Ponsford JL, Ziino C, Parcell DL, Shekleton JA, Roper M, Redman JR, et al. Fatigue and sleep disturbance following traumatic brain injury—their nature, causes, and potential treatments. J Head Trauma Rehabil. (2012) 27:224–33. doi: 10.1097/HTR.0b013e31824ee1a8
34. Fichtenberg NL, Putnam SH, Mann NR, Zafonte RD, Millard AE. Insomnia screening in postacute traumatic brain injury: utility and validity of the Pittsburgh Sleep Quality Index. Am J Phys Med Rehabil. (2001) 80:339–45. doi: 10.1097/00002060-200105000-00003
35. Fillion L, Gélinas C, Simard S, Savard J, Gagnon P. Validation evidence for the French Canadian adaptation of the Multidimensional Fatigue Inventory as a measure of cancer-related fatigue. Cancer Nurs. (2003) 26:143–54. doi: 10.1097/00002820-200304000-00008
36. Kolakowsky-Hayner SA, Bellon K, Toda K, Bushnik T, Wright J, Isaac L, et al. A randomised control trial of walking to ameliorate brain injury fatigue: a NIDRR TBI model system centre-based study. Neuropsychol Rehabil. (2017) 27:1002–18. doi: 10.1080/09602011.2016.1229680
37. von Steinbüchel N, Wilson L, Gibbons H, Hawthorne G, Höfer S, Schmidt S, et al. Quality of Life after Brain Injury (QOLIBRI): Scale Development and Metric Properties. J Neurotrauma. (2010) 27:1167–85. doi: 10.1089/neu.2009.1076
38. Rosenthal R, Cooper H, Hedges L. Parametric measures of effect size. In: The Handbook of Research Synthesis. New York, NY: editRussel Sage Foundation (1994), p. 573.
39. Miles MB, Huberman AM, Saldaña J. Qualitative Data Analysis: A Methods Sourcebook. 3rd ed. Thousand Oaks, CA: SAGE Publications (2014), p. 381.
40. McPherson JI, Saleem GT, Haider MN, Leddy JJ, Torres D, Willer BSJN. Development of a telehealth examination for sport-related concussion in the outpatient setting. Neurology. (2022) 98:S8–9. doi: 10.1212/01.wnl.0000801808.74733.1d
41. Chrisman SPD, Mendoza JA, Zhou C, Palermo TM, Gogue-Garcia T, Janz KF, et al. Pilot study of telehealth delivered rehabilitative exercise for youth with concussion: the Mobile Subthreshold Exercise Program (MSTEP). Frontiers in pediatrics. (2021) 9:237. doi: 10.3389/fped.2021.645814
42. Weinstein AA, Chin LM, Collins J, Goel D, Keyser RE, Chan L. Effect of aerobic exercise training on mood in people with traumatic brain injury: a pilot study. J Head Trauma Rehabil. (2017) 32:E49. doi: 10.1097/HTR.0000000000000253
43. Fait P, Imhoff S, Carrier-Toutant F, Geneviève B. Efficiency of an active rehabilitation intervention in a slow-to-recover paediatric population following a sport-related concussion. Br J Sports Med. (2017) 51:A85–A. doi: 10.1136/bjsports-2016-097270.220
44. Kleffelgaard I, Soberg HL, Bruusgaard KA, Tamber AL, Langhammer B. Vestibular rehabilitation after traumatic brain injury: case series. Phys Ther. (2016) 96:839–49. doi: 10.2522/ptj.20150095
45. Kleffelgaard I, Soberg HL, Tamber A-L, Bruusgaard KA, Pripp AH, Sandhaug M, et al. The effects of vestibular rehabilitation on dizziness and balance problems in patients after traumatic brain injury: a randomized controlled trial. Clin Rehabil. (2019) 33:74–84. doi: 10.1177/0269215518791274
46. Blake H, Batson M. Exercise intervention in brain injury: a pilot randomized study of Tai Chi Qigong. Clin Rehabil. (2009) 23:589–98. doi: 10.1177/0269215508101736
47. Tremblay MS, Warburton DE, Janssen I, Paterson DH, Latimer AE, Rhodes RE, et al. New Canadian physical activity guidelines. Appl Physiol Nurt Metab. (2011) 36:36–46. doi: 10.1139/H11-009
48. Chu AH, Ng SH, Paknezhad M, Gauterin A, Koh D, Brown MS, et al. Comparison of wrist-worn Fitbit Flex and waist-worn ActiGraph for measuring steps in free-living adults. PLoS ONE. (2017) 12:e0172535. doi: 10.1371/journal.pone.0172535
49. Cicerone KD, Azulay J. Perceived self-efficacy and life satisfaction after traumatic brain injury. J Head Trauma Rehabil. (2007) 22:257–66. doi: 10.1097/01.HTR.0000290970.56130.81
50. Gagnon I, Swaine B, Friedman D, Forget R. Exploring children's self-efficacy related to physical activity performance after a mild traumatic brain injury. J Head Trauma Rehabil. (2005) 20:436–49. doi: 10.1097/00001199-200509000-00005
51. Chrisman SPD, Whitlock KB, Mendoza JA, Burton MS, Somers E, Hsu A, et al. Pilot randomized controlled trial of an exercise program requiring minimal in-person visits for youth with persistent sport-related concussion. Front Neurol. (2019) 10:623. doi: 10.3389/fneur.2019.00623
52. Shiffman S, Stone AA, Hufford MR. Ecological momentary assessment. Annu Rev Clin Psychol. (2008) 4:1–32. doi: 10.1146/annurev.clinpsy.3.022806.091415
Keywords: walk, exercise, physical activity, mTBI, concussion, mixed-methods, mild traumatic brain injury, feasibility study
Citation: Alarie C, Gagnon I, Guise Ed, McKerral M, Kersalé M, Hoog Bvh and Swaine B (2022) A Remotely Delivered Progressive Walking Intervention for Adults With Persistent Symptoms of a Mild Traumatic Brain Injury: Feasibility and Exploration of Its Impact. Front. Rehabilit. Sci. 3:898804. doi: 10.3389/fresc.2022.898804
Received: 17 March 2022; Accepted: 06 June 2022;
Published: 06 July 2022.
Edited by:
Linda Barclay, Monash University, AustraliaReviewed by:
Margaret Weightman, Courage Kenny Rehabilitation Institute - Minneapolis, United StatesCopyright © 2022 Alarie, Gagnon, Guise, McKerral, Kersalé, Hoog and Swaine. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bonnie Swaine, bonnie.swaine@umontreal.ca
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.