 Jerson Mekoulou Ndongo1
Jerson Mekoulou Ndongo1 Elysée Claude Bika Lele1Wiliam Richard Guessogo2Laurence Patricia Meche3Clarisse Noel Ayina Ayina1
Elysée Claude Bika Lele1Wiliam Richard Guessogo2Laurence Patricia Meche3Clarisse Noel Ayina Ayina1 Jessica Guyot4Babette Zengue3Marie Yvonne Lobe Tanga3Léon Jules Owana Manga3Abdou Temfemo3
Jessica Guyot4Babette Zengue3Marie Yvonne Lobe Tanga3Léon Jules Owana Manga3Abdou Temfemo3 Nathalie Barth4
Nathalie Barth4 Bienvenu Bongue4Samuel Honoré Mandengue1
Bienvenu Bongue4Samuel Honoré Mandengue1 Peguy Brice Assomo Ndemba5*†
Peguy Brice Assomo Ndemba5*†
- 1Physical Activities and Sport Physiology and Medicine Unit, Faculty of Science, University of Douala, Douala, Cameroon
- 2Department of Human and Social Sciences Applied to Physical Activities and Sports, National Institute of Youth and Sports, Yaoundé, Cameroon
- 3Faculty of Medicine and Pharmaceutical Sciences, University of Douala, Douala, Cameroon
- 4INSERM, U1059, Sainbiose, Dysfonction Vasculaire et Hémostase, Université de Lyon, Université Jean Monnet, Saint-Etienne, France
- 5Faculty of Medicine and Biomedical Sciences, University of Yaounde I, Yaounde, Cameroon
Introduction: Musculoskeletal disorders (MSDs) represent an important threat to public health in both developed and developing countries, and are present in many occupational sectors including education. Regular practice of physical activity (PA) is known elicit preventive effects on the occurrence of MSDs.
Objective: This study aimed at determining the prevalence of MSDs and the preventive impact of PA on their occurrence among secondary school teachers.
Participants and Methods: A cross-sectional study was conducted among 179 teachers in five government secondary schools in Douala, Cameroon. The Nordic and Ricci-Gagnon questionnaires were used to determine MSDs and to assess the level of PA, respectively.
Results: The 12-month and 7-day prevalence of MSD (PMSD-12m and PMSD-7d) were 84.3% and 69.3%, respectively. The most affected body regions by MSDs were neck (PMSD-12m = 54.2%, PMSD-7d = 33.5%), lower back (PMSD-12m = 43%, PMSD-7d = 33%), and shoulders (PMSD-12m = 35%, PMSD-7d = 22.9%). Compared to female, males were protected against MSDs during the last 12 months (OR = 0.37; 95% CI 0.16–0.93; p = 0.04). The risk of MSDs during the last seven days was higher in teachers aged 30-40 years (OR = 2.86; 95% CI 1.14–7.14; p = 0.02) and 40-50 years (OR = 4.28; 95% CI 1.49–16.29; p = 0.008) than those under 30 years. This risk was tripled in inactive teachers (OR = 3.07; 95% CI 1.40–6.78; p = 0.005), compared to their active counterparts.
Conclusion: MSDs are prevalent among secondary school teachers and associated with aging, gender, and lower level of PA
Introduction
Musculoskeletal disorders (MSDs) is a generic term encompassing a set of periarticular disorders that affect the musculoskeletal system, and mainly result in daily pain and functional discomfort (1). These also refer to gradual development of damages in musculoskeletal tissuewhich occurs when the work demand outclasses adaptive capacity of musculoskeletal tissue (2). MSDs can be localized to several body regions affecting body's joints, ligaments, tendons, nerves, muscles, and structures that support limbs, neck and back. MSDs are related to physical effort during work, thereby explaining their high occurrence in workers (3). It is also known that the origin of MSDs is multifactorial, involving a complex interplay between biomechanical stress, individual-related genetic and behavioral factors, environment factors (i.e., organizational work conditions), and psychosocial context (4, 5). These conditions are characterized by pain and limitations in mobility and functional capacity. MSDs disorders are the main contributors to disability worldwide, with low back pain being the primary global cause (6).
MSDs are a cause of public health concern in developed countries such as United States of America (USA), Canada, Finland, France, Sweden, and The United Kingdom. Indeed, MSDs are a major cause of absenteeism and inability to work (4, 6). MSDs are still largely underreported despite their enormous deleterious impact on occupational health and associated morbidity (6). In USA, MSDs accounted for 32% of all pathologies and non-fatal injuries in full-time workers in 2014 (7). Besides, MSDs are ranked first among occupational health diseases in several European countries (2).
Given the challenges related to economic growth, African countries are facing increasingly important prevalence and deleterious effects of MSDs in workers of several occupational sectors, especially in education sector. In Africa, work conditions of teachers are rude and non-ergonomic (e.g., prolonged sitting/standing, usage of inappropriate furniture, inappropriate working space), and expose them to MSDs (8, 9). Previous studies reported a high incidence of MSDs among teachers all around the world (8–12), as well as high prevalence in Africa (13, 14).
Physical activitiy (PA) is defined as any energy-requiring body movement produced by skeletal muscles (15). The World Health Organization (WHO) recommends to practice regularly at least one PA for preventing non-communicable diseases, and thus improving the quality of life (16). The benefits of regular PA on prevention of several health ailments, such as MSDs, have been largely documented (17–19). In this context, PA and sport may be efficient means for preventing, relieving, and treating MSDs (20–25).
The extensive researches on MSDs in developed countries contrasts with the lack of reports in their developing counterparts, especially in African countries, where there is a paucity of data on the prevalence and associated factors of MSDs in teachers. The effect of PA on MSD-related burden is also an important missing link in African context. In this regard, the present study aimed at determining the prevalence of MSDs and associated factors as well as the impact of PA among secondary school teachers of Douala city, Cameroon.
Materials and methods
Study site and population
This cross-sectional and analytical study was carried out at five Government secondary schools in the city of Douala, the economic capital of Cameroon. Teachers willing to participate in the study, with professional experience of at least one year, and having signed an informed consent form were included. Teachers with trauma history and on MSDs related medication were excluded.
Sampling
The minimum sample size required for the study was computed using the Lorentz's formula: N = p (1-p) z2/d2, where N is the minimum sample size; p is the prevalence of MSDs (96%) reported previously by El Gendy and Korish (26); z is the statistic for the desired confidence level (z = 1.96 for confidence at 95%), and d is the accepted margin of error (d = 0.05). Thus, the minimal sample size found was N = 59 participants.
Study design
The study objectives and data collection methods were first explained to administration staff of the government schools, and after issuing administrative authorization, they were explained to teachers. An informed consent form was given to each teacher who accepted to participate in the study. Anthropometric parameters were measured and questionnaire forms were given to each participant. The teachers were asked to returned filled questionnaire within seven days upon reception. Teachers were assisted by research team members if questions were not well understood. Identification codes were assigned to each questionnaire to process and analyze it anonymously. Incomplete and poorly completed questionnaires were excluded from the final analysis. A total of 300 questionnaires were distributed, and 179 (60%) teachers returned correctly filled questionnaires (Figure 1).
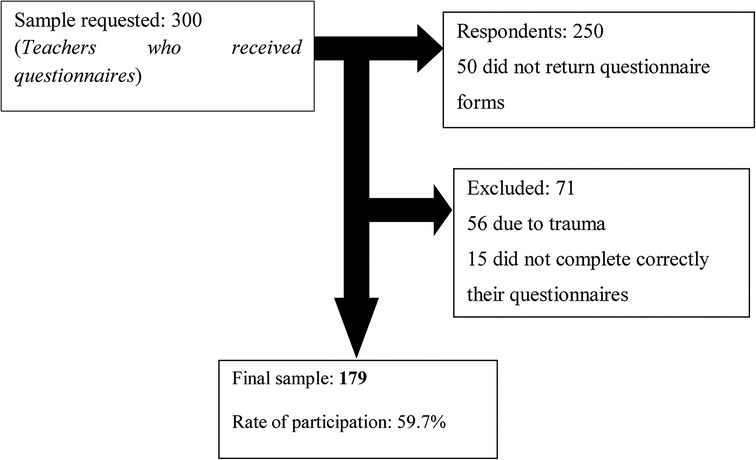
Figure 1. Flow charts of participants.
Data collection
A structured questionnaire was administered to each participant and consisted of three parts. (i) socio-demographic and anthropometric characteristics (age, gender, region of origin and family status weight, height), (ii) socio-professional information (school, job seniority, number of teaching hours a week); (iii) level of PA and prevalence of MSDs during the last six months or last seven days.
Anthropometric parameters
Height was measured using a rod graduated to the nearest centimeter. Weight was measured using an electronic scale Tanita BC-532 (Tokyo, Japan). The body mass index was determined using Quetelet's formula: BMI (kg.m−2) = Weight (kg) / height2 (m2). Based on BMI values, participants were categorized as normal (18.5 < BMI < 25), overweight (25 ≤ BMI < 30), and Obese (BMI ≥ 30).
Musculoskeletal disorders
The Nordic questionnaire (27) was used to determine the prevalence of MSDs. This questionnaire determines the occurrence of MSDs on nine body regions (neck, shoulders, elbows, wrists/hands, upper back, lower back, hips/thighs, knees, ankles/feet) during last 12 months or 7 days. For each body region, the following parameters were evaluated (i) the presence or absence of aches, pains or genes during the last 12 months and/or the last seven days, (ii) absenteeism or not at work during the last 12 months and/or the last seven days due to MSD in the body region concerned, and (iii) the presence or not of a history of trauma in the region concerned. Based on these three items, the prevalence of MSDs during the last 12 months (PMSD-12m) and the last seven days (PMSD−7d) were determined.
Level of physical activity
The Ricci and Gagnon questionnaire was used to determine the level of PA of each participant (28). This questionnaire is a scale divided in two sub-sections, A and B, with four items each. Sub-section A evaluates the duration and intensity of daily common activities such as cleaning, gardening, rural work, and walking. Sub-section B evaluates sport and recreational activities. The total score of points in subsections A and B was used to classify participants as inactive (score < 16), active (16 ≤ score ≤ 32), and very active (score > 32).
Statistical analysis
Qualitative variables were presented as percentages (%). Statistical analyses were conducted using the Statistical Package for Social Science v21.0 (SPSS Inc., Chicago, IL, USA). The normality of quantitative was checked using the Kolmogorov-Smirnov test. Pearson independence Chi2 test was used to compare proportions of unpaired samples. Logistic regression analysis was used to determine factors associated with MSD among teachers. The association between the dependent variable (presence of MSDs) and independent variables (gender, age, PA) was quantified in logistic regression analysis by computing odds ratios (OR), their confidence interval at 95%, and p-value. The level significance was set for a value of p < 0.05.
Results
Most of the participants were females (66.5%) and aged 30–40 years (54.2%). Based on BMI analysis, 30.7% and 28.2% of teachers were overweight and obese, respectively (Table 1).
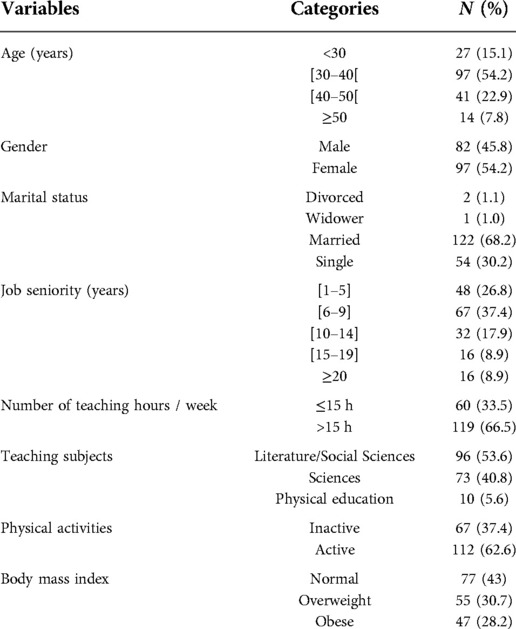
Table 1. Socio-demographic and professional characteristics of the participants.
The prevalence of MSDs by body regions and gender is depicted on Figure 2. The overall prevalence of MSD-12m and MSD-7d was 84.3% and 69.3%, respectively. PMSD-12m value was significantly higher in females compared to males (57.3% vs. 42.7%, p-value = 0.03). MSD-12m and MSD-7d were most frequently reported at neck (54.2% and 33.5%), lower back (43% and 33%), and shoulders (35.2% and 22.9%).
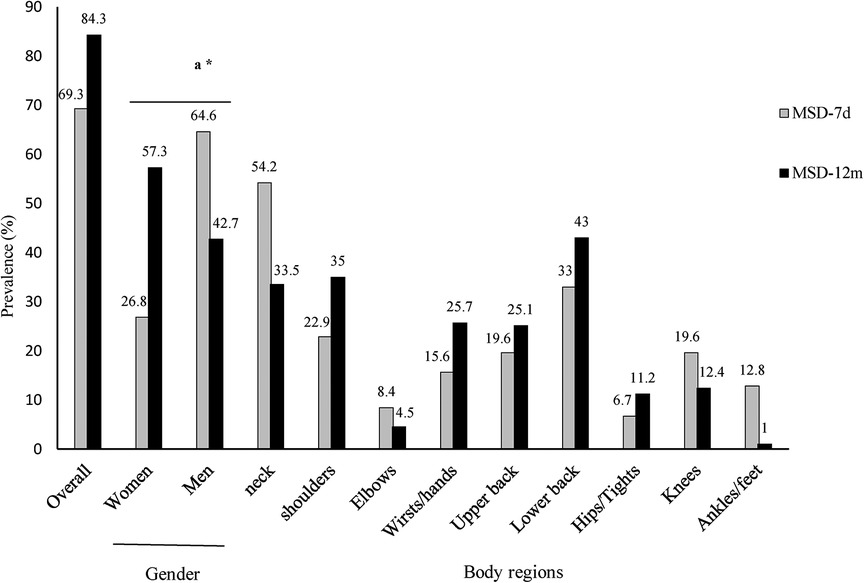
Figure 2. Prevalence of MSDs in body regions and gender.MSD-7d: MSD during the last 7 days; MSD-12m: MSDs during the last 12 months, a: gender comparison of MSD-12 m between males and females; *: p < 0.05.
The teachers reported MSDs at one to nine body regions (Figure 3). The prevalence of MSD-12m and MSD-7d at one body region was 21.8% and 25.1%, respectively. Lower estimates were reported at two body regions (PMSD-12m = 19.0% and PMSD−7d = 19.0%) and three body regions (PMSD-12m = 18.4% and PMSD−7d = 11.7%) (Figure 3).
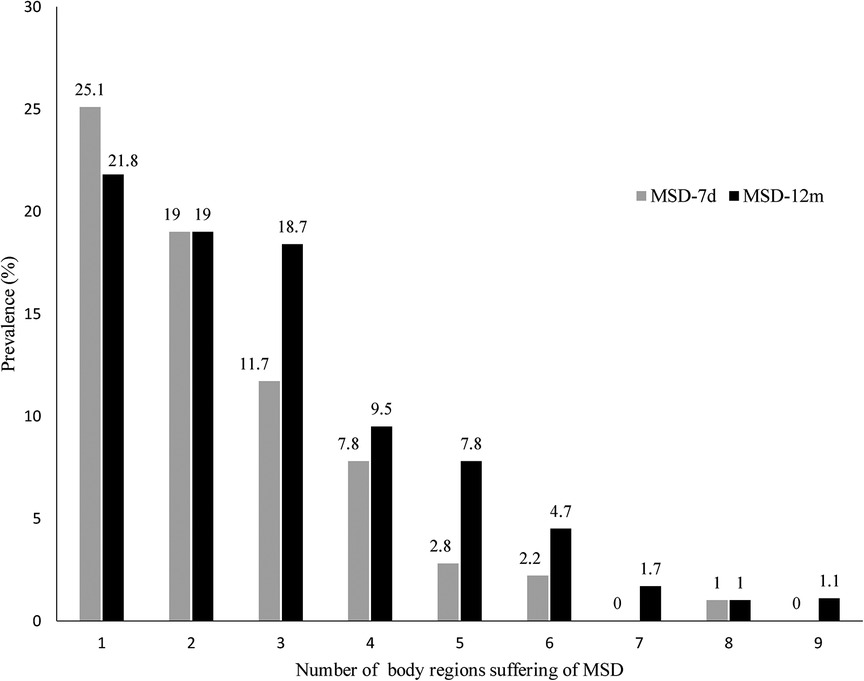
Figure 3. Prevalence of MSD according to the number of body regions affected. MSD-7d: MSD during the last 7 days; MSD-12m: MSDs during the last 12 months.
On multivariate regression analysis, the risk of MSDs was increased by ∼three times in teachers aged 30–40 years (OR = 2.86; 95% CI 1.14–7.14; p = 0.02), and by over four times in those aged 40–50 years (OR = 4.28; 95% CI 1.49–16.29; p = 0.008), compared to those aged below 30 years old. It was also noticed positive effect of PA on the risk of MSD-7d. Teachers classified as “inactive” were three times at risk of MSDs (OR = 3.07; 95% CI 1.40–6.78; p = 0.005), compared with those classified as “active”. In contrast, the risk of MSD-12 m was decreased by 63% in males (OR = 0.37; 95% CI 0.16–0.93; p = 0.04) (Table 2).
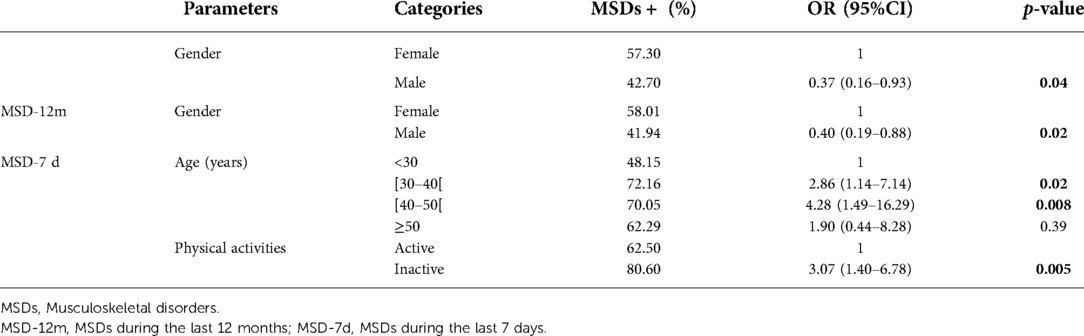
Table 2. Multivariate logistic analysis of associated factors with MSDs.
Discussion
The purpose of this study was to assess the prevalence and determinants of MSDs as well as the impact of PA on MSDs risk, among secondary school teachers of Douala, Cameroon.
A PMSD-12m of 84.3% was in this study, thereby indicating that MSDs were very frequent among secondary teachers. This prevalence is consistent with that reported in different settings including Botswana (83.3%), Nigeria (70.2%), Saudi Arabia (68.50-79.17%), and Philippines (79.17%) (14, 29, 30). Higher PMSD-12m estimates were reported in Chile (90.81%) (31) and Egypt (96%) (26).
More than half (69.3%) of teachers suffered from MSDs during the last seven days, and this is in line with that reported in Bolivia (63.4%) by Solis-Soto et al. (32). Facing execrable working conditions daily e.g., prolonged sitting/standing could explain this high PMSD−7d estimate reported here (8, 9). Several authors opined a multifactorial origin of MSDs including prolonged static muscle load and repetitive work gestures (33–36). A higher teaching load could also explain this high MSDs prevalence. It was reported a teacher-to-student ratio of 1/377 in Cameroon, which is 15 times higher than the UNESCO recommended 1/25 ratio (37, 38).
Consisting with previous studies (26, 39), MSDs were mainly located at neck. In contrast, it was reported a predominance of MSDs at shoulders in Indian and Nigerian teachers, while MSDs were mainly seen at lower back of Kenyan teachers (14, 40, 41). Differences related to working environment and teaching approaches could likely explain these discrepancies observed between the above mentioned studies and the present study. The increased risk of MSDs among older participants found in this study was also reported earlier in other settings (10, 39, 40).
PMSD-12m was significantly higher in women compared to men. Similar observations were done elsewhere on an increased risk of MSD-12m at various body parts (neck, shoulders, upper back, and feet/knees) in female gender in the educational sector (11, 29, 42). According to Ng et al. (43), this predisposition of women to MSDs is due to the fact they are predominant in teaching profession as it was the case in our study. Chong and Chan (9) suggested that females might suffer more frequently from MSDs than males because of lower physical strength, and higher difficulties to manage relatives and professions-elicited stress.
This study confirms the protective role of PA against MSDs, and this finding was also reported in diverse studies on education sector (25, 29, 44, 45), and other occupational sectors (21, 22, 23, 25, 46). Again, other studies found the positive role of PA in improving MSDs symptoms in all body regions (17, 18, 19). Erick and Smith (29) pointed out that PA ≥ 5 h/week was protective against MSDs. On a physiological view, PA increases blood supply to muscles and bones, reduces muscle tension, and preserves joint movement, minimizing pain, injuries, and enhancing their repair (44, 47). Moreover, sufficient PA will result into reduced pain, strengthened weak muscles, and decreased mechanical load on vertebral structures (48). It has been suggested that a regular exercise of ≥30 min/day could stimulate an adequate production of endorphins which are known to reduce MSDs (49, 50).
Limitations
Causes of MSDs being multifactorial, some of them constitute the limits of this study. Therefore, crucial determinants such as psychosocial factors, job/salary satisfaction, quality of life, exposure to workplace violence, and ergonomic factors were not captured, and this represents an important limitation to this study. Also, medical confirmation of MSDs diagnostic was not done. Thus, MSDs prevalence estimates based on the Nordic questionnaire could not reflect the real burden of MSDs among teachers.
Conclusion
This study found a high prevalence of MSDs among Cameroonian secondary school teachers, with a predominance of MSDs at neck, lower back, and shoulders. The study also outlined protective effect of PA in reducing risk of MSDs. It is critical to implement primary MSDs prevention measures to preserve wellbeing of teachers through improvement of work conditions and promotion of PA and sport. All taken together could be very helpful to prevent and control efficiently education sector-related MSDs.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the Institutional Ethics Committee of the University of Douala (N° 2093 CEI-Udo/01/2020/T). The patients/participants provided their written informed consent to participate in this study.
Author contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by LPM, JMN, BLE and PBAN, WRG. The first draft of the manuscript was written by LPM, JMN, BLEC. The study was designed by: CAA, OMLJ, AT, JG, NB, PBAN and SHM. Overall supervision was performed by, BB, SHM. All authors commented on previous versions of the manuscript. All authors contributed to the article and approved the submitted version.
Acknowledgments
The authors would like to express special gratitude to all the secondary's school's administration staff and participants for their cooperation.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Summers K, Jinnett K, Bevan S. Musculoskeletal disorders, workforce health and productivity in the United States. London: The center for work forced health and performance (2015). Lancaster University.
2. World Health Organization. Musculoskeletal Conditions. (2019). Available at: https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions (Accessed May 07, 2022).
3. Da Costa BR, Vieira ER. Risk factors for work-related musculoskeletal disorders: a systematic review of recent longitudinal studies. Am J Ind Med. (2010) 53:285–323. doi: 10.1002/ajim.20750
4. Punnett L, Wegman DH. Work-related musculoskeletal disorders: the epidemiologic evidence and the debate. J Electromyogr Kines. (2014) 14:13–23. doi: 10.1016/j.jelekin.2003.09.015
5. Roquelaure Y. Musculoskeletal Disorders and Psychosocial Factors at Work (December 14, 2018). ETUI Research Paper - Report 142. http://dx.doi.org/10.2139/ssrn.3316143
6. Blyth FM, Briggs AM, Schneider CH, Hoy DG, March LM. The global burden of musculoskeletal pain-where to from here? Am J Public Health. (2019) 109:35–40. doi: 10.2105/AJPH.2018.304747
7. Charles LE, Ma CC, Burchfiel CM, Dong RG. Vibration and ergonomic exposures associated with musculoskeletal disorders of the shoulder and neck. Saf Health Work. (2018) 9:125–32. doi: 10.1016/j.shaw.2017.10.003
8. Cardoso JP, De Queiroz Batista Ribeiro I, Maria de Araújo T, Carvalho FM. Prevalence of musculoskeletal pain among teachers. Rev Bras Epidemiol. (2009) 12:1–10. doi: 10.1590/S1415-790X2009000400010
9. Chong EY, Chan AH. Subjective health complaints of teachers from primary and secondary schools in Hong Kong. Int J Occup Saf Ergon. (2010) 16:23–39. doi: 10.1080/10803548.2010.11076825
10. Korkmaz NC, Cavlak U, Telci EA. Musculoskeletal pain, associated risk factors and coping strategies in school teachers. Sci Res Essays. (2011) 6:649–57. doi: 10.5897/SRE10.1064
11. Mohseni Bandpei MA, Ehsani F, Behtash H, Ghanipour M. Occupational low back pain in primary and high school teachers: prevalence and associated factors. J Manip Physiol Ther. (2014) 37:702–8. doi: 10.1016/j.jmpt.2014.09.006
12. Erick PN, Smith DR. A systematic review of musculoskeletal disorders among school teachers. BMC Musculoskelet Disorder. (2011) 12:260. doi: 10.1186/1471-2474-12-260
13. Eggers LS, Pillay JD, Govender N. Musculoskeletal pain among school teachers: are we underestimating its impact? Occhealth. (2018) 24:46–50. doi: 10.1186/1471-2474-12-260
14. Ojukwu CP, Anyanwu GE, Eze B, Chukwu SC, Onuchukwu CL, Anekwu EM. Prevalence, pattern and correlates of work-related musculoskeletal disorders among school teachers in Enugu, Nigeria. Int J Occup Saf Ergon. (2021) 27:267–77. doi: 10.1080/10803548.2018.1495899
15. World Health Organization. Global recommendations on physical activity for health. Geneva: World Health Organization (2010).
16. Haskell WL, Lee IM, Pate RR, Powell KE, Blair SN, Franklin BA, et al. Physical activity and public health: updated recommendation for adults from the American college of sports medicine and the American heart association. Med Sci Sports Exerc. (2007) 39:1423–34. doi: 10.1249/mss.0b013e3180616b27
17. Sjögren T, Nissinen KJ, Järvenpää SK, Ojanen MT, Vanharanta H, Mälkiä EA. Effects of a workplace physical exercise intervention on the intensity of headache and neck and shoulder symptoms and upper extremity muscular strength of office workers: a cluster randomized controlled cross-over trial. Pain. (2005) 116:119–28. doi: 10.1016/j.pain.2005.03.031
18. Blangsted AK, Søgaard K, Hansen EA, Hannerz H, Sjøgaard G. One-year randomized controlled trial with different physical-activity programs to reduce musculoskeletal symptoms in the neck and shoulders among office workers. Scand J Work Environ Health. (2008) 34:55–65. doi: 10.5271/sjweh.1192
19. Lewis BA, Napolitano MA, Buman MP, Williams DM, Nigg CR. Future directions in physical activity intervention research: expanding our focus to sedentary behaviors, technology, and dissemination. J Behav Med. (2017) 40:112–26. doi: 10.1007/s10865-016-9797-8
20. Verhagen AP, Karels C, Bierma-Zeinstra SM, Burdorf L, Feleus A, Dahaghin S, et al. Ergonomic and physiotherapeutic interventions for treating work-related complaints of the arm, neck or shoulder in adults. Cochrane Database Syst Rev. (2006) 3:1–48. PMID: 17921965
21. Andersen LL, Christensen KB, Holtermann A, Poulsen OM, Sjøgaard G, Pedersen MT, et al. Effect of physical exercise interventions on musculoskeletal pain in all body regions among office workers: a one-year randomized controlled trial. Man Ther. (2010) 15:100–4. doi: 10.1016/j.math.2009.08.004
22. Sihawong R, Janwantanakul P, Sitthipornvorakul E, Pensri P. Exercise therapy for office workers with nonspecific neck pain: a systematic review. J Manipulative Physiol Ther. (2011) 34:62–71. doi: 10.1016/j.jmpt.2010.11.005
23. Kelly D, Shorthouse F, Roffi V, Tack C. Exercise therapy and work-related musculoskeletal disorders in sedentary workers. Occup Med. (2018) 68:262–72. doi: 10.1093/occmed/kqy054
24. Aktürk S, Büyükavcı R, Aktürk Ü. Relationship between musculoskeletal disorders and physical inactivity in adolescents. J Public Health. (2019) 27:49–56. doi: 10.1007/s10389-018-0923-7
25. Diallo SYK, Mweu MM, Mbuya SO, Mwanthi MA. Prevalence and risk factors for low back pain among university teaching staff in Nairobi, Kenya: a cross-sectional study (version 1, peer review: 1 approved, 2 approved with reservations). F1000Res. (2019) 8:808. doi: 10.12688/f1000research.19384.1
26. El Gendy M, Korish MM. Work related musculoskeletal disorders among preparatory school teachers in Egypt. Egypt J Occup Med. (2017) 41:115–26. doi: 10.21608/ejom.2017.965
27. Kuorinka I, Jonsson B, Kilbom A, Vinterberg H, Biering-Sorensen F, Andersson G, et al. Standardised. Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon. (1987) 18:233–7. doi: 10.1016/0003-6870(87)90010-X
28. Bacquaert P, Bacquaert MA. Questionnaire d’Auto-évaluation du niveau de sédentarité Revue de littérature. (2015). Available at: http://www.irbms.com/questionnaire-dauto-evaluation-du niveau-de-sédentarité-revue-de-littérature
29. Erick PN, Smith DR. The prevalence and risk factors for musculoskeletal disorders among school teachers in Botswana. Occup Med Health Aff. (2014) 02:1–12. doi: 10.4172/2329-6879.1000178
30. Amit LM, Malabarbas GT. Prevalence and risk-factors of musculoskeletal disorders among provincial high school teachers in the Philippines. J UOEH. (2020) 42:151–60. doi: 10.7888/juoeh.42.151
31. Vega-Fernández G, Olave E, Lizana PA. Musculoskeletal disorders and quality of life in Chilean teachers: a cross-sectional study. Front Public Health. (2022) 10:810036. doi: 10.3389/fpubh.2022.810036
32. Solis-Soto MT, Schön A, Solis-Soto A, Parra M, Radon K. Prevalence of musculoskeletal disorders among school teachers from urban and rural areas in Chuquisaca, Bolivia: a cross-sectional study. BMC Musculoskelet Disord. (2017) 18:7. doi: 10.1186/s12891-016-1362-7
33. Ariens GA, Van MW, Bongers PM, Bouter LM, Wal G. Physical risk factors for neck pain. Scand J Work Environ Health. (2000) 26:7–19. doi: 10.5271/sjweh.504
34. Huang GD, Feuerstein M, Sauter SL. Occupational stress and work-related upper extremity disorders: concepts and models. Am J Ind Med. (2002) 41:298–314. doi: 10.1002/ajim.10045
35. Andersen JH, Kaergaard A, Mikkelsen S, Jensen UF, Frost P, Bonde JP, et al. Risk factors in the onset of neck/shoulder pain in a prospective study of workers in industrial and service companies. Occup Environ Med. (2003) 60:649–54. doi: 10.1136/oem.60.9.649
36. Palmer KT, Smedley J. Work relatedness of chronic neck pain with physical findings- a systematic review. Scand J Work Environ Health. (2007) 33:165–91. doi: 10.5271/sjweh.1134
37. United Nations Educational, Scientific and Cultural Organization (UNESCO). Teaching contexts and pressures. In: Teachers and teaching in a changing world. 7, place de fontenoy, 75352 Paris 07 SP. Paris, France: UNESCO Publishing (1998). p. 48–76.
38. Owona Manga LJ, Assomo Ndemba P, Lompo Sanon MS, Mekoulou J, Zilli Ebae PV, Bongue B, et al. Burnout and associated factors among secondary teachers in douala, Cameroon. Arch Mal Prof Enviro. (2020) 81:356–64. doi: 10.1016/j.admp.2020.04.013
39. Tami AM, Bika Lele EC, Mekoulou Ndongo J, Ayina Ayina CN, Guessogo WR, Lobe Tanga MY, et al. Epidemiology of musculoskeletal disorders among the teaching staff of the university of douala, Cameroon: association with physical activity practice. Int J Environ Res Public Health. (2021) 18:6004. doi: 10.3390/ijerph18116004
40. Kataria J, Jain S. Prevalence of musculoskeletal disorders among school teachers. Int J Yoga Physiother Phys Educ. (2018) 3:17–9. doi: 10.5897/SRE10.1064
41. Kebede A, Abebe SM, Woldie H, Yenit MK. Low back pain and associated factors among primary school teachers in Mekele city, North Ethiopia: a cross-sectional study. Occup Ther Int. (2019):3862946. doi: 10.1155/2019/3862946
42. Samad NIA, Abdullah H, Moin S, Tamrin SBM, Hashim Z. Prevalence of low back pain and its risk factors among school teachers. Am J Appl Sci. (2010) 7:634–9. doi: 10.3844/ajassp.2010.634.639
43. Ng YM, Ibrahim N, Maakip I. Prevalence and risk factors of musculoskeletal disorders (MSD) among primary and secondary school teachers: a narrative review. Austin J Musculoskelet Disord. (2017) 4:1–6.
44. Khruakhorn S, Sritipsukho P, Siripakarn Y, Vachalathiti R. Prevalence and risk factors of low back pain among the university staff. J Med Assoc Thai. (2010) 93:142–8. PMID: 21294409
45. Beyen TK, Mengestu MY, Zele YT. Low back pain and associated factors among teachers in gondar town, north gondar, amhara region, Ethiopia. Occup Med Health Aff. (2013) 1:127. doi: 10.4172/2329-6879.1000127
46. Weyh C, Pilat C, Krüger K. Musculoskeletal disorders and level of physical activity in welders. Occup Med. (2020) 70:586–92. doi: 10.1093/occmed/kqaa169
47. Nia HS, Haghdoost AA, Beheshti Z, Soleymani MA, Bahrami N, Hojjati H, et al. Relationship between backache and psychological and psychosocial job factors among the nurses. Int J Nurs Midwifery. (2011) 3:86–91. doi: 10.5897/IJNM.9000039
48. Jackson CP, Brown MD. Is there a role for exercise in the treatment of patients with low back pain? Clin Orthop Relat Res. (1983) 179:39–45. PMID: 6225594
49. Kwon MA, Shim WS, Kim MH, Gwak MS, Hahm TS, Kim GS, et al. A correlation between low back pain and associated factors: a study involving 772 patients who had undergone general physical examination. J Korean Med Sci. (2006) 21:1086–91. doi: 10.3346/jkms.2006.21.6.1086
Keywords: musculoskeletal disorders, prevalence, associated factors, secondary school teachers, physical activities, Cameroon
Citation: Mekoulou Ndongo J, Bika Lele EC, Guessogo WR, Meche LP, Ayina Ayina CN, Guyot J, Zengue B, Lobe Tanga MY, Owana Manga LJ, Temfemo A, Barth N, Bongue B, Mandengue SH and Assomo Ndemba PB (2022) Musculoskeletal disorders among secondary school teachers in Douala, Cameroon: The effect of the practice of physical activities. Front. Rehabilit. Sci. 3:1023740. doi: 10.3389/fresc.2022.1023740
Received: 22 August 2022; Accepted: 28 November 2022;
Published: 16 December 2022.
Edited by:
Feng Yang, Georgia State University, United StatesReviewed by:
Lori Portzer, Lebanon Valley College, United StatesDiego Ferreira, Lebanon Valley College, United States
© 2022 Mekoulou Ndongo, Bika Lele, Guessogo, Meche, Ayina Ayina, Guyot, Zengue, Lobe Tanga, Owona Manga, Temfemo, Barth, Bongue, Mandengue, Assomo Ndemba. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Peguy Brice Assomo Ndemba YXNzb21vX25kZW1iYUB5YWhvby5mcg==
†ORCID Peguy Brice Assomo Ndemba orcid.org/0000-0002-9604-0140
Specialty Section: This article was submitted to Rehabilitation for Musculoskeletal Conditions, a section of the journal Frontiers in Rehabilitation Sciences