 Hangqin Lv
Hangqin Lv Xin Yi
Xin Yi Xiangjun Guo
Xiangjun Guo Meichuan Lin
Meichuan Lin Dingxi Bai2
Dingxi Bai2 Xiaoyun Liu
Xiaoyun Liu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol., 26 March 2025
Sec. Psychology of Aging
Volume 16 - 2025 | https://doi.org/10.3389/fpsyg.2025.1550013
This article is part of the Research TopicAging and WorkView all 8 articles
Objective: This study aimed to investigate the correlation between mild cognitive impairment and flourishing among Chinese residents.
Methods: A total of 527 community residents aged ≥18 years were recruited from December 2023 to April 2024. Based on the results of the Ascertain Dementia 8-Item Informant Questionnaire (AD8), participants were classified into a healthy group (n = 356) and a mild cognitive impairment (MCI) group (n = 171). General demographic data, including age, gender, height, weight, place of residence, education level, marital status, household composition, personal income, occupation, and the flourishing scale (FS) were collected for statistical analysis. The analysis was performed using Statistical Product and Service Solutions software. Chi-square test was used to compare differences between the groups, while Kendall’s correlation analysis and multivariate logistic regression were applied to assess the relationship between flourishing and MCI.
Results: Comparisons between the healthy and MCI groups showed that the FS scores in the healthy group were significantly higher than those in the MCI group (p < 0.01). Kendall’s correlation analysis revealed that the score of AD8 was negatively correlated with FS (r = −0.237, p < 0.01). Multivariate analysis indicated that age [odds ratio (OR) = 1.451, 95% confidence interval (CI; 1.107–1.902), p = 0.007], place of residence [OR = 5.523, 95% CI (3.572–8.539), p < 0.001], and FS [OR = 0.421, 95%CI (0.311–0.569), p < 0.001] were correlated with MCI.
Conclusion: Flourishing levels are negatively correlated with MCI, and higher levels of flourishing associated with a lower risk of MCI. This suggests that flourishing may serve as a protective factor against cognitive decline. Additionally, age and place of residence are identified as risk factors for MCI.
Dementia is a major cause of disability in individuals aged >65 years worldwide, including China, and presents significant challenges for policymakers, healthcare providers, and family members (Jia et al., 2020b). The onset and progression of Alzheimer’s disease (AD), the leading cause of dementia, are gradual and span several years to decades before symptoms become evident (Jack et al., 2013; Villemagne et al., 2013). It is characterized by progressively worsening cognitive and functional impairments. Mild cognitive impairment (MCI), considered the first clinical manifestation of AD, occurs when an individual exhibits below-average performance on standardized neuropsychological tests (Studart and Nitrini, 2016). When cognitive impairment becomes significant enough to interfere with daily functioning, the diagnosis of AD is established (Albert et al., 2011). AD is irreversible and can only have its progression delayed. Therefore, paying attention to MCI in the early stages is crucial. Early diagnosis and timely intervention during this phase can help slow down the progression of AD.
MCI imposes a significant burden, affecting the quality of life and psychological well-being (Gates et al., 2014). Those with MCI exhibit lower levels of social support, self-esteem, life satisfaction, positive affect, optimism, and hope but higher levels of negative affect compared with healthy individuals (Dos Santos et al., 2018). Currently, the research on the psychological aspects of MCI is limited. However, some studies indicated that individuals with dementia exhibit a lack of recognition, assessment, and even the ability to feel negative emotions (Balconi et al., 2015; Oliver et al., 2015; Bora et al., 2016) and preserve the ability to recognize positive emotions (Dos Santos et al., 2018; Oliver et al., 2015; Bora et al., 2016; Goodkind et al., 2015; St. Jacques et al., 2015). The incidence of cognitive impairment was also associated with optimism in a study evaluating 4,624 elderly people over 4 years, which showed that high optimism was a protective factor against cognitive impairment and played an important role in maintaining cognitive functioning (Dos Santos et al., 2018; Gawronski et al., 2016). Thus, we should pay more attention to positive psychology. The mission of positive psychology is to understand and foster the factors that allow individuals, communities, and societies to flourish (Fredrickson, 2001).
The flourishing theory, an emerging field of well-being within positive psychology, was originally developed to operationalize mental health in response to the notion that well-being is not merely the absence of mental illness (Jahoda, 1959), but Rather, it encompasses the cultivation of positive emotional experiences, eudaimonic well-being, and meaningful social engagement and contribution (Keyes, 2002; Mock and Smale, 2023). Keyes (2002) conceptualized flourishing within the Mental Health Continuum Model, which defines mental health as a spectrum ranging from languishing (a state of psychological distress and low well-being) to flourishing (optimal mental health with high levels of emotional, psychological, and social well-being). Similarly, Seligman’s (2011) PERMA model identifies five core elements essential for flourishing: Positive Emotion, Engagement, Relationships, Meaning, and Accomplishment, each contributing to overall life satisfaction and psychological resilience.
Most research on flourishing focused on adolescents and the elderly (Parsons et al., 2022; Otgon et al., 2023), its relevance to individuals with MCI remains largely unexplored. Flourishing is the pinnacle of good mental health, and it is constituted by an affective state and psychological and social functioning (Mjøsund, 2021) — elements that have been associated with cognitive health (Rodrigues and Delerue-Matos, 2025; Yang et al., 2024) —understanding its relationship with MCI may provide insights into potential protective mechanisms against cognitive decline. Consequently, this study aims to explore the correlation between MCI and flourishing among Chinese residents.
This cross-sectional study recruited 527 Chinese residents using a convenience sampling between December 2023 and April 2024. Inclusion criteria for residents were (1) the age of ≥18 years and (2) Chinese citizenship. Exclusion criteria for residents comprised (1) individuals with mental illnesses or those unable to communicate and (2) a prior confirmed diagnosis of dementia, stroke, Parkinson’s disease, or other conditions impacting cognitive function. The sample size was determined using Kendall’s sample size estimation method (Stuart and Ord, 2010), which suggests that the sample size should be 5 to 10 times the number of variables. This study analyzed 26 variables, including 10 items from a self-made questionnaire and 16 items from two scales. Considering a 30% inefficiency rate of the questionnaire, the minimal sample size for this study was determined at 507, the final sample size was 527.
Data were collected by nursing undergraduates who underwent standardized training. During their spare time, they collected data in their local communities through face-to-face interviews, during which residents were guided to independently complete the self-administered questionnaires. Before distributing the questionnaires, instructions for this study and informed consent forms were provided to the residents. Data collection commenced only after participants indicated their consent by selecting “yes.”
Regarding demographic data, all residents provided their general data, including age, gender, height, weight, place of residence, education level, marital status, household composition, personal income, and occupation.
The self-reported AD8 has been shown to be effective in differentiating individuals with MCI from those without dementia, with its diagnostic performance also validated in studies primarily involving Chinese populations (Chin et al., 2013; Passler et al., 2021). And it created by the Alzheimer’s Disease Research Center at Washington University in 2005, is an 8-item questionnaire based on informant responses, designed to detect changes within the individual in areas such as memory, orientation, judgment, and functional abilities (Galvin et al., 2005), which may coincide with MCI, in this study, a cut-off score of two or greater suggests that the individual may have MCI (Tanwani et al., 2023; Yin et al., 2020). The informant-rated AD8 demonstrated good internal consistency, with Cronbach’s α = 0.84–0.85 for the English version (Galvin et al., 2006; Shaik et al., 2016) and 0.78 for the Chinese version (Li et al., 2012). It also shows strong interrater reliability, with an intraclass correlation coefficient of 0.85 for the English version (Shaik et al., 2016), and solid test–retest reliability, with weighted κ values between 0.67 and 0.80 for the English version (Galvin et al., 2006; Shaik et al., 2016) and an intraclass correlation coefficient of 0.96 for the Chinese version (Li et al., 2012). The AD8 is less influenced by the individual’s educational background compared to other cognitive assessment tools such as the Mini-Mental State Examination and Montreal Cognitive Assessment (Chin et al., 2013). This feature makes the AD8 particularly useful for detecting cognitive changes across diverse populations without the confounding effect of educational attainment.
Flourishing scale (FS) is a brief 8-item summary measure of the respondent’s self-perceived success in areas such as relationships, self-esteem, purpose, and optimism (Diener et al., 2010). Each item is rated by respondents on a 7-point Likert scale (1 indicates “strongly disagree” and 7 indicates “strongly agree”), with high scores indicating high flourishing, and the total score ranging from 7 to 56 (Cerezo et al., 2024). In this study, we utilized the simplified Chinese version of the FS introduced by Tang et al. (2016), the scale shows excellent reliability and validity, with Cronbach’s α = 0.90–0.93 (Keyes, 2002). And Xiao et al. (2021) further classified this scale into different levels, categorizing FS scores as follows: ≥5 points represented a high flourishing level, 4–4.99 was a medium flourishing level, and < 4 denoted a low flourishing level. The exploratory factor analysis identified a single factor that accounted for 75.03% of the total variance, and the confirmatory factor analysis indicated that all the goodness-of-fit indices were acceptable (Zhang, 2018).
All statistical analyses were conducted using Statistical Product and Service Solutions version 25.0 software (IBM, Armonk, NY, United States). Variables showing statistical differences in the univariate analysis were subsequently included in a multivariable logistic regression model to assess their net effects on cognitive function. Odds ratios (ORs) along with their 95% confidence intervals (CIs) were utilized to evaluate the independent impact of prognostic factors. The Chi-square test was used to assess the differences between groups with categorical variables. Kendall’s correlation analysis was employed to identify associations of the Ascertain Dementia 8-Item Informant Questionnaire score with general information. All p-values were two-tailed, with p < 0.05 indicating statistical significance.
The study was conducted anonymously to ensure the authenticity and validity of the data. Before the survey, the data collectors were trained uniformly and followed by a test after the training to ensure the accuracy and reliability of data collection. The data collectors, who were third-year nursing undergraduates from various locations, conducted the surveys in their communities therefore to reduce language barriers. Data were collected in real-time during the face-to-face interviews.
The sample included 215 males and 312 females aged 18–94 years (average: 53.36 ± 18.06 years). The healthy group comprised 356 subjects aged 18–88 years (average: 49.93 ± 17.75 years), whereas the MCI group included 170 individuals. The Kendall sample estimation algorithm was used, which estimates the sample size 10–15 times the number of variables.
A total of 527 participants were included in the cross-sectional study. The demographic characteristics of the residents are presented in Table 1. Based on the total AD8 scores, participants were grouped into two categories: the healthy group (n = 356) and the MCI group (n = 171), with those scoring ≥2 points on the AD8 classified as the MCI group. Compared with the healthy group, the MCI group had a higher proportion of older and overweight individuals (p < 0.05) but lower numbers of married, single, urban and high-income individuals, and lower FS scores (p < 0.05). However, no statistically significant differences were observed in gender, region, household composition, or occupation (p > 0.05).
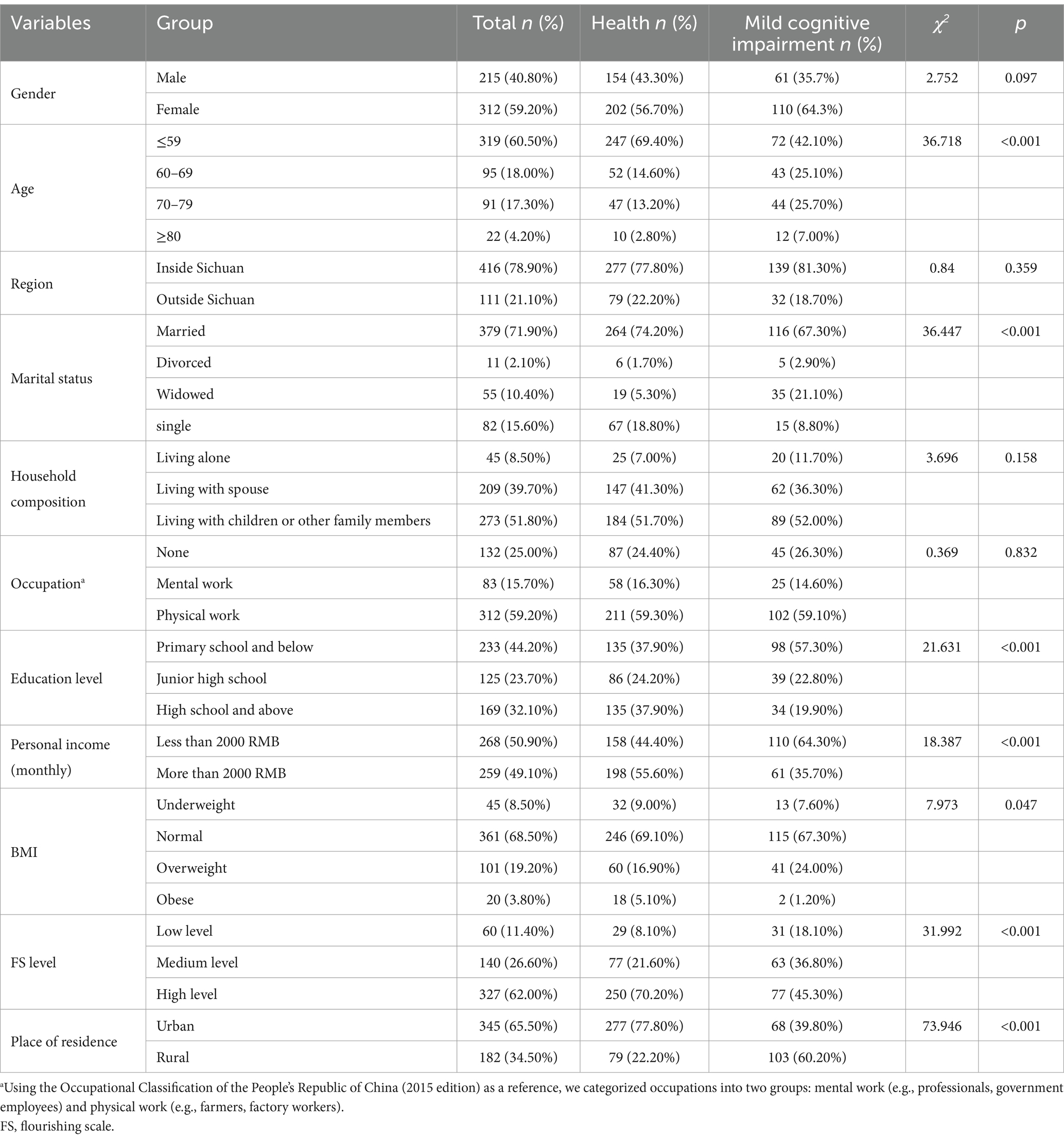
Table 1. Demographic characteristics of the residents.
Kendall’s correlation analysis showed a negative correlation between FS (b = −0.237, p < 0.001), education level (b = −0.187, p < 0.001), personal income (b = −0.191, p < 0.001), and the AD8 score. Additionally, age (b = 0.248, p < 0.001) was positively correlated with the AD8 score (Table 2). The factor values are listed in Table 3.
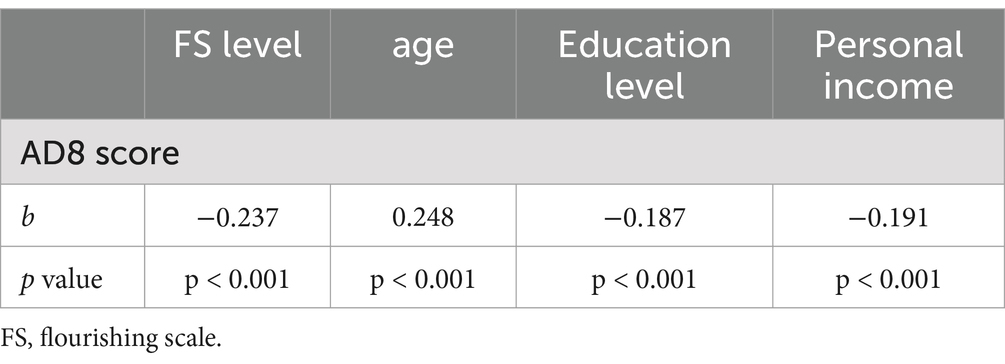
Table 2. Kendall’s correlation analysis of Mild Cognitive Impairment with general information.

Table 3. Factor values of the independent variables.
Univariate logistic regression analysis revealed a statistically significant difference in age, place of residence, and FS level. Age [OR = 1.451, 95% CI (1.107–1.902), p = 0.007], FS [OR = 0.421, 95% CI (0.311–0.569), p < 0.001], and place of residence [OR = 5.523, 95% CI (3.572–8.539), p < 0.001] continued to be independently linked with MCI (Table 4).
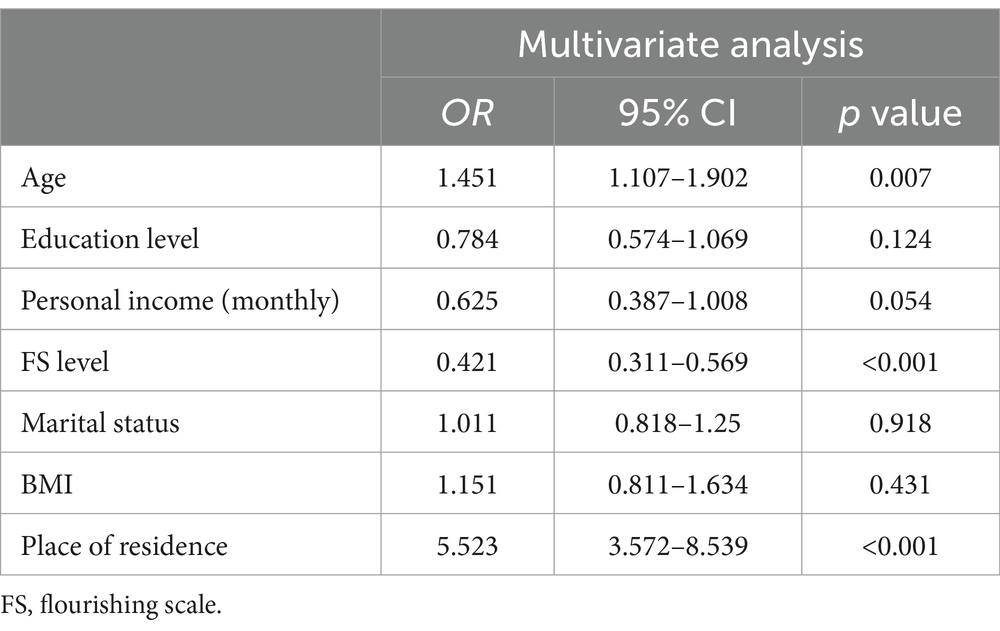
Table 4. Multivariate logistic regression analyses of factors affecting cognitive dysfunction.
Numerous conditions can cause a decline in cognitive function and dementia. This study indicated that MCI is associated with age, personal income, and especially FS scores.
The risk of MCI increases with age and among rural residents, of which age is a nonmodifiable factor (Jia et al., 2020a; Alzheimer's Association, 2015). Age-related MCI is multifactorial, with numerous underlying and frequently co-morbid pathological correlates (Mckenzie et al., 2022). Research indicated that various forms of brain pathology (such as cerebrovascular disease, neuritic plaques, neurofibrillary tangles, Lewy body disease, TDP-43 pathology, and hippocampal sclerosis) can be linked with an increased risk of age-related mild cognitive impairment (Kapasi et al., 2017; Power et al., 2018). Furthermore, living in rural areas is a major risk factor for mild cognitive impairment (Vega and Newhouse, 2014). A study among older Indians demonstrated significant differences in cognitive impairment based on urban or rural residential status, with rural residence identified as a significant risk factor for cognitive impairment (Muhammad, 2023). Similarly, a cross-sectional survey of residents aged ≥65 years from 30 urban and 45 rural communities across China revealed that the prevalence of dementia and AD was notably higher in rural areas than in urban areas (Jia et al., 2014). Urban areas provide better transportation, healthcare access, health information, infrastructure, and educational opportunities, all of which contribute to improved health and quality of life for older residents. In contrast, older adults in rural areas face limited and less adequate services in these areas, increasing the likelihood of developing MCI.
Our study found that flourishing is significantly associated with a lower risk of MCI. Specifically, participants with higher flourishing level had a reduced likelihood of MCI (OR = 0.421, 95%CI: 0.311—0.569, p < 0.001). This finding suggest that flourishing may have a protective effect on cognitive function, potentially by enhancing psychological resilience. Consistent with prior research, our findings indicated that flourishing may protect against cognitive decline by fostering psychological resilience. Psychosocial resilience factors, such as positive emotional states and social support, may contribute more significantly to cognitive well-being than physical health alone (Reichstadt et al., 2007; Jeste et al., 2013; O'brien et al., 2023). Furthermore, psychological resilience and competence play a significant role in slowing down biological aging (Zábó et al., 2023), which aligns with our observation that individuals with higher flourishing scores exhibited better cognitive performance. These may help individuals more effectively cope with neuropathological changes, potentially delaying cognitive decline.
This study identified a correlation between flourishing and MCI. It indicated that individuals with higher flourishing levels have a significantly lower incidence of MCI, with a correlation coefficient of −0.237 (p < 0.001). This suggests that flourishing plays a meaningful role in reducing the risk of MCI and may serve as a protective factor in maintaining cognitive function. However, the research focusing on the relationship between MCI risk and flourishing is scarce. A randomized controlled trial involving 51 participants suggested that positive psychology interventions can enhance the subjective well-being of individuals diagnosed with amnestic MCI, with the benefits persisting for some time after the intervention ends (Tsiflikioti et al., 2023). The study also reflected that MCI may be related to the relatively intact emotional function in early AD (Bozeat et al., 2000). Flourishing may protect cognitive function through multiple pathways, including reducing stress-related neurotoxicity and enhancing emotional regulation. Chronic stress is known to elevate cortisol levels, which can accelerate hippocampal atrophy—a key brain region implicated in early AD (Wells et al., 2019; Hakeem et al., 2025; Sharan and Vellapandian, 2024). However, individuals with higher flourishing levels tend to exhibit greater psychological resilience, which has been linked to lower cortisol reactivity (Heller et al., 2013) and lower stress (Laakso et al., 2025). Additionally, flourishing fosters positive emotional states, which are associated with increased dopamine (Chopra, 2023) and serotonergic activity (Fan et al., 2023), both of which play crucial roles in cognitive processing and emotional regulation (Echouffo-Tcheugui et al., 2018; Ott and Nieder, 2019; Švob Štrac et al., 2016). By mitigating chronic stress and promoting emotional stability, flourishing may serve as a buffer against MCI risk and cognitive decline.
Chronic stress is a well-established risk factor for MCI and AD, primarily due to its impact on the hippocampus, a brain region highly susceptible to stress-induced atrophy (Kennedy et al., 2017; Hyer et al., 2021). Elevated stress levels lead to dysregulation of the hypothalamic–pituitary–adrenal (HPA) axis, resulting in prolonged cortisol exposure, which in turn accelerates neuronal damage and cognitive decline (Magri et al., 2006; Tsigos and Chrousos, 2002). However, increasing evidence suggests that positive psychology techniques, particularly those that foster flourishing, can effectively enhance subjective well-being and mitigate stress levels (Machado et al., 2019; Kinoshita et al., 2024). Flourishing has been linked to improved emotional regulation and lower cortisol reactivity (De Vries et al., 2022), potentially protecting the hippocampus from stress-induced damage. Therefore, flourishing may act as a protective factor against MCI, reducing the impact of stress and emotional disturbances on cognitive health.
Conclusively, in the future, greater attention should be given to the psychological aspects of patients with MCI. Instead of focusing solely on the negative aspects, more positive psychological interventions, such as psychological counseling, positive psychology training, and social support programs, should be implemented. These interventions can improve individuals’ flourishing levels, thereby enhancing their cognitive function.
This study has some limitations, including the use of a non-random sampling method due to constraints in time and workforce, which may have affected generalizability. Future research should improve sampling methods and adopt longitudinal designs to explore causal relationships between flourishing and MCI. Additionally, future studies need to investigate specific impacts of flourishing on various types of MCI.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Ethics Committee of the People’s Hospital of Jinniu District in Chengdu, Sichuan, China. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
HL: Data curation, Formal analysis, Investigation, Writing – original draft, Writing – review & editing. XY: Data curation, Formal analysis, Investigation, Writing – original draft, Writing – review & editing. XG: Investigation, Writing – original draft, Writing – review & editing. ML: Investigation, Writing – original draft, Writing – review & editing. DB: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. XN: Investigation, Writing – original draft. XW: Investigation, Writing – original draft, Writing – review & editing. XL: Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research and/or publication of this article.
We express gratitude to all the Chinese residents who participated in this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Albert, M. S., DeKosky, S. T., Dickson, D., Dubois, B., Feldman, H. H., Fox, N. C., et al. (2011). The diagnosis of mild cognitive impairment due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. 7, 270–279. doi: 10.1016/j.jalz.2011.03.008
Alzheimer's Association (2015). 2015 Alzheimer's disease facts and figures. Alzheimers Dement. 11, 332–384. doi: 10.1016/j.jalz.2015.02.003
Balconi, M., Cotelli, M., Brambilla, M., Manenti, R., Cosseddu, M., Premi, E., et al. (2015). Understanding emotions in frontotemporal dementia: the explicit and implicit emotional Cue mismatch. J. Alzheimers Dis. 46, 211–225. doi: 10.3233/JAD-142826
Bora, E., Velakoulis, D., and Walterfang, M. (2016). Meta-analysis of facial emotion recognition in behavioral variant frontotemporal dementia: comparison with Alzheimer disease and healthy controls. J. Geriatr. Psychiatry Neurol. 29, 205–211. doi: 10.1177/0891988716640375
Bozeat, S., Gregory, C. A., Ralph, M. A., and Hodges, J. R. (2000). Which neuropsychiatric and behavioural features distinguish frontal and temporal variants of frontotemporal dementia from Alzheimer's disease? J. Neurol. Neurosurg. Psychiatry 69, 178–186. doi: 10.1136/jnnp.69.2.178
Cerezo, M. V., Soria-Reyes, L. M., Alarcón, R., and Blanca, M. J. (2024). The flourishing scale: psychometric properties in breast Cancer patients. Integr. Cancer Ther. 23:15347354241249935. doi: 10.1177/15347354241249935
Chin, R., Ng, A., Narasimhalu, K., and Kandiah, N. (2013). Utility of the Ad8 as a self-rating tool for cognitive impairment in an Asian population. Am. J. Alzheimers Dis. Other Dement. 28, 284–288. doi: 10.1177/1533317513481090
Chopra, M. (2023). Exploring the Nexus of gratitude, flourishing, and anxiety in young adults. Int. J. Interdiscip. Appr. Psychol. 1, 218–301.
De Vries, L. P., Van De Weijer, M. P., and Bartels, M. (2022). The human physiology of well-being: a systematic review on the association between neurotransmitters, hormones, inflammatory markers, the microbiome and well-being. Neurosci. Biobehav. Rev. 139:104733. doi: 10.1016/j.neubiorev.2022.104733
Diener, E., Wirtz, D., Tov, W., Kim-Prieto, C., Choi, D. W., Oishi, S., et al. (2010). New well-being measures: Short scales to assess flourishing and positive and negative feelings. Soc. Indic. Res. 97, 143–156. doi: 10.1007/s11205-009-9493-y
Dos Santos, S. B., Rocha, G. P., Fernandez, L. L., De Padua, A. C., and Reppold, C. T. (2018). Association of lower spiritual Well-being, social support, self-esteem, subjective well-being, optimism and hope scores with mild cognitive impairment and mild dementia. Front. Psychol. 9:371. doi: 10.3389/fpsyg.2018.00371
Echouffo-Tcheugui, J. B., Conner, S. C., Himali, J. J., Maillard, P., DeCarli, C. S., Beiser, A. S., et al. (2018). Circulating cortisol and cognitive and structural brain measures: the Framingham heart study. Neurology 91, e1961–e1970. doi: 10.1212/WNL.0000000000006549
Fan, Y., Yang, Y., Shi, L., Zhao, W., Kong, F., and Gong, P. (2023). Genetic architecture of well-being: cumulative effect of serotonergic polymorphisms. Soc. Cogn. Affect. Neurosci. 18:nsad039. doi: 10.1093/scan/nsad039
Fredrickson, B. L. (2001). The role of positive emotions in positive psychology. The broaden-and-build theory of positive emotions. Am. Psychol. 56, 218–226. doi: 10.1037/0003-066X.56.3.218
Galvin, J. E., Roe, C. M., Powlishta, K. K., Coats, M. A., Muich, S. J., Grant, E., et al. (2005). The Ad8: a brief informant interview to detect dementia. Neurology 65, 559–564. doi: 10.1212/01.wnl.0000172958.95282.2a
Galvin, J. E., Roe, C. M., Xiong, C., and Morris, J. C. (2006). Validity and reliability of the Ad8 informant interview in dementia. Neurology 67, 1942–1948. doi: 10.1212/01.wnl.0000247042.15547.eb
Gates, N., Valenzuela, M., Sachdev, P. S., and Singh, M. A. (2014). Psychological well-being in individuals with mild cognitive impairment. Clin. Interv. Aging 9, 779–792. doi: 10.2147/CIA.S58866
Gawronski, K. A., Kim, E. S., Langa, K. M., and Kubzansky, L. D. (2016). Dispositional optimism and incidence of cognitive impairment in older adults. Psychosom. Med. 78, 819–828. doi: 10.1097/PSY.0000000000000345
Goodkind, M. S., Sturm, V. E., Ascher, E. A., Shdo, S. M., Miller, B. L., Rankin, K. P., et al. (2015). Emotion recognition in frontotemporal dementia and Alzheimer's disease: a new film-based assessment. Emotion 15, 416–427. doi: 10.1037/a0039261
Hakeem, M. K., Sallabi, S., Ahmed, R., Hamdan, H., Mameri, A., Alkaabi, M., et al. (2025). A dual biomarker approach to stress: hair and salivary cortisol measurement in students via LC-MS/MS. Anal. Sci. Adv. 6:e70003. doi: 10.1002/ansa.70003
Heller, A. S., van Reekum, C. M., Schaefer, S. M., Lapate, R. C., Radler, B. T., Ryff, C. D., et al. (2013). Sustained striatal activity predicts eudaimonic well-being and cortisol output. Psychol. Sci. 24, 2191–2200. doi: 10.1177/0956797613490744
Hyer, M. M., Shaw, G. A., Goswamee, P., Dyer, S. K., Burns, C. M., Soriano, E., et al. (2021). Chronic adolescent stress causes sustained impairment of cognitive flexibility and hippocampal synaptic strength in female rats. Neurobiol. Stress 14:100303. doi: 10.1016/j.ynstr.2021.100303
Jack, C. R. Jr., Knopman, D. S., Jagust, W. J., Petersen, R. C., Weiner, M. W., Aisen, P. S., et al. (2013). Tracking pathophysiological processes in Alzheimer's disease: an updated hypothetical model of dynamic biomarkers [J]. Lancet Neurol. 12, 207–216. doi: 10.1016/S1474-4422(12)70291-0
Jeste, D. V., Savla, G. N., Thompson, W. K., Vahia, I. V., Glorioso, D. K., Martin, A.’. S., et al. (2013). Association between older age and more successful aging: critical role of resilience and depression. Am. J. Psychiatry 170, 188–196. doi: 10.1176/appi.ajp.2012.12030386
Jia, L., Du, Y., Chu, L., Zhang, Z., Li, F., Lyu, D., et al. (2020a). Prevalence, risk factors, and management of dementia and mild cognitive impairment in adults aged 60 years or older in China: a cross-sectional study. Lancet Public Health 5, e661–e671. doi: 10.1016/S2468-2667(20)30185-7
Jia, L., Quan, M., Fu, Y., Zhao, T., Li, Y., Wei, C., et al. (2020b). Dementia in China: epidemiology, clinical management, and research advances. Lancet Neurol. 19, 81–92. doi: 10.1016/S1474-4422(19)30290-X
Jia, J., Wang, F., Wei, C., Zhou, A., Jia, X., Li, F., et al. (2014). The prevalence of dementia in urban and rural areas of China. Alzheimers Dement. 10, 1–9. doi: 10.1016/j.jalz.2013.01.012
Kapasi, A., Decarli, C., and Schneider, J. A. (2017). Impact of multiple pathologies on the threshold for clinically overt dementia. Acta Neuropathol. 134, 171–186. doi: 10.1007/s00401-017-1717-7
Kennedy, G., Hardman, R. J., Macpherson, H., Scholey, A. B., and Pipingas, A. (2017). How does exercise reduce the rate of age-associated cognitive decline? A review of potential mechanisms. J. Alzheimers Dis. 55, 1–18. doi: 10.3233/JAD-160665
Keyes, C. L. (2002). The mental health continuum: from languishing to flourishing in life. J. Health Soc. Behav. 43, 207–222. doi: 10.2307/3090197
Kinoshita, S., Hanashiro, S., Tsutsumi, S., Shiga, K., Kitazawa, M., Wada, Y., et al. (2024). Assessment of stress and well-being of Japanese employees using wearable devices for sleep monitoring combined with ecological momentary assessment: pilot observational study. JMIR Form. Res. 8:e49396. doi: 10.2196/49396
Laakso, M., Fagerlund, Å., and Lagerström, M. (2025). Increasing student well-being through a positive psychology intervention: changes in salivary cortisol, depression, psychological well-being, and hope. Appl. Psychol. Health Well Being 17:e12616. doi: 10.1111/aphw.12616
Li, T., Wang, H. L., Yang, Y. H., Galvin, J. E., Morris, J. C., and Yu, X. (2012). The reliability and validity of Chinese version of AD8. Zhonghua Nei Ke Za Zhi 51, 777–780.
Machado, L., de Oliveira, I. R., Peregrino, A., and Cantilino, A. (2019). Common mental disorders and subjective well-being: emotional training among medical students based on positive psychology. PLoS One 14:e0211926. doi: 10.1371/journal.pone.0211926
Magri, F., Cravello, L., Barili, L., Sarra, S., Cinchetti, W., Salmoiraghi, F., et al. (2006). Stress and dementia: the role of the hypothalamic-pituitary-adrenal axis. Aging Clin. Exp. Res. 18, 167–170. doi: 10.1007/BF03327435
McKenzie, A. T., Marx, G. A., Koenigsberg, D., Sawyer, M., Iida, M. A., Walker, J. M., et al. (2022). Interpretable deep learning of myelin histopathology in age-related cognitive impairment. Acta Neuropathol. Commun. 10:131. doi: 10.1186/s40478-022-01425-5
Mjøsund, N. H. (2021). “A Salutogenic mental health model: flourishing as a metaphor for good mental health” in Health promotion in health care—Vital theories and research. eds. G. Haugan and M. Eriksson (Cham: Springer), 47–59.
Mock, S. E., and Smale, B. (2023). The relationship of diverse leisure activities with flourishing. Front. Psychol. 14:1130906. doi: 10.3389/fpsyg.2023.1130906
Muhammad, T. (2023). Life course rural/urban place of residence, depressive symptoms and cognitive impairment among older adults: findings from the longitudinal aging study in India. BMC Psychiatry 23:391. doi: 10.1186/s12888-023-04911-9
O'Brien, E., Whitman, K., Buerke, M., Galfalvy, H., and Szanto, K. (2023). Life-satisfaction, engagement, mindfulness, flourishing, and social support: do they predict depression, suicide ideation, and history of suicide attempt in late life? Am. J. Geriatr. Psychiatry 31, 415–424. doi: 10.1016/j.jagp.2022.12.192
Oliver, L. D., Mitchell, D. G., Dziobek, I., MacKinley, J., Coleman, K., Rankin, K. P., et al. (2015). Parsing cognitive and emotional empathy deficits for negative and positive stimuli in frontotemporal dementia. Neuropsychologia 67, 14–26. doi: 10.1016/j.neuropsychologia.2014.11.022
Otgon, S., Myagmarjav, S., Burnette, D., Lkhagvasuren, K., and Casati, F. (2023). Sociodemographic predictors of flourishing among older adults in rural and urban Mongolia. Sci. Rep. 13:1756. doi: 10.1038/s41598-023-28791-x
Ott, T., and Nieder, A. (2019). Dopamine and cognitive control in prefrontal cortex. Trends Cogn. Sci. 23, 213–234. doi: 10.1016/j.tics.2018.12.006
Parsons, R. D., McParland, J. L., Halligan, S. L., Goubert, L., and Jordan, A. (2022). Flourishing among adolescents living with chronic pain and their parents: a scoping review. Paediatr. Neonatal. Pain 4, 158–168. doi: 10.1002/pne2.12088
Passler, J. S., Kennedy, R. E., Crowe, M., Clay, O. J., Howard, V. J., Cushman, M., et al. (2021). The relationship of cognitive change over time to the self-reported ascertain dementia 8-item questionnaire in a general population. Arch. Clin. Neuropsychol. 36, 243–252. doi: 10.1093/arclin/acz045
Power, M. C., Mormino, E., Soldan, A., James, B. D., Yu, L., Armstrong, N. M., et al. (2018). Combined neuropathological pathways account for age-related risk of dementia. Ann. Neurol. 84, 10–22. doi: 10.1002/ana.25246
Reichstadt, J., Depp, C. A., Palinkas, L. A., and Jeste, D. V. (2007). Building blocks of successful aging: a focus group study of older adults' perceived contributors to successful aging. Am. J. Geriatr. Psychiatry 15, 194–201. doi: 10.1097/JGP.0b013e318030255f
Rodrigues, P. M. F., and Delerue-Matos, A. (2025). The effect of social exclusion on the cognitive health of middle-aged and older adults: a systematic review. Arch. Gerontol. Geriatr. 130:105730. doi: 10.1016/j.archger.2024.105730
Seligman, M. E. (2011). Flourish: a visionary new understanding of happiness and well-being. Atria Books: Simon and Schuster.
Shaik, M. A., Xu, X., Chan, Q. L., Hui, R. J. Y., Chong, S. S. T., Chen, C. L. H., et al. (2016). The reliability and validity of the informant Ad8 by comparison with a series of cognitive assessment tools in primary healthcare. Int. Psychogeriatr. 28, 443–452. doi: 10.1017/S1041610215001702
Sharan, P., and Vellapandian, C. (2024). Hypothalamic-pituitary-adrenal (HPA) axis: unveiling the potential mechanisms involved in stress-induced Alzheimer's disease and depression. Cureus 16:e67595. doi: 10.7759/cureus.67595
St. Jacques, P. L., Grady, C., Davidson, P. S., and Chow, T. W. (2015). Emotional evaluation and memory in behavioral variant frontotemporal dementia. Neurocase 21, 429–437. doi: 10.1080/13554794.2014.917681
Stuart, A., and Ord, K. (2010). Kendall's advanced theory of statistics, distribution theory. John Wiley & Sons.
Studart, A. N., and Nitrini, R. (2016). Subjective cognitive decline: the first clinical manifestation of Alzheimer's disease? Dement. Neuropsychol. 10, 170–177. doi: 10.1590/S1980-5764-2016DN1003002
Švob Štrac, D., Pivac, N., and Mück-Šeler, D. (2016). The serotonergic system and cognitive function. Transl. Neurosci. 7, 35–49. doi: 10.1515/tnsci-2016-0007
Tang, X., Duan, W., Wang, Z., and Liu, T. (2016). Psychometric evaluation of the simplified Chinese version of flourishing scale. Res. Soc. Work. Pract. 26, 591–599. doi: 10.1177/1049731514557832
Tanwani, R., Danquah, M. O., Butris, N., Saripella, A., Yan, E., Kapoor, P., et al. (2023). Diagnostic accuracy of ascertain dementia 8-item questionnaire by participant and informant-a systematic review and meta-analysis. PLoS One 18:e0291291. doi: 10.1371/journal.pone.0291291
Tsiflikioti, K., Moraitou, D., Pezirkianidis, C., Papantoniou, G., Sofologi, M., Kougioumtzis, G. A., et al. (2023). Enhancing subjective wellbeing in older individuals with amnestic mild cognitive impairment: a randomized trial of a positive psychology intervention. Behav. Sci. 13:100838. doi: 10.3390/bs13100838
Tsigos, C., and Chrousos, G. P. (2002). Hypothalamic–pituitary–adrenal axis, neuroendocrine factors and stress. J. Psychosom. Res. 53, 865–871. doi: 10.1016/S0022-3999(02)00429-4
Vega, J. N., and Newhouse, P. A. (2014). Mild cognitive impairment: diagnosis, longitudinal course, and emerging treatments. Curr. Psychiatry Rep. 16:490. doi: 10.1007/s11920-014-0490-8
Villemagne, V. L., Burnham, S., Bourgeat, P., Brown, B., Ellis, K. A., Salvado, O., et al. (2013). Amyloid β deposition, neurodegeneration, and cognitive decline in sporadic Alzheimer's disease: a prospective cohort study. Lancet Neurol. 12, 357–367. doi: 10.1016/S1474-4422(13)70044-9
Wells, R. E., Kerr, C., Dossett, M. L., Danhauer, S. C., Sohl, S. J., Sachs, B. C., et al. (2019). Can adults with mild cognitive impairment build cognitive reserve and learn mindfulness meditation? Qualitative theme analyses from a small pilot study. J. Alzheimers Dis. 70, 825–842. doi: 10.3233/JAD-190191
Xiao, R., Zhang, C., Lai, Q., Hou, Y., and Zhang, X. (2021). Applicability of the dual-factor model of mental health in the mental health screening of Chinese college students. Front. Psychol. 11:549036. doi: 10.3389/fpsyg.2020.549036
Yang, Q., Lin, S., Zhang, Z., du, S., and Zhou, D. (2024). Relationship between social activities and cognitive impairment in Chinese older adults: the mediating effect of depressive symptoms. Front. Public Health 12:1506484. doi: 10.3389/fpubh.2024.1506484
Yin, L., Ren, Y., Wang, X., Li, Y., Hou, T., Liu, K., et al. (2020). The power of the functional activities questionnaire for screening dementia in rural-dwelling older adults at high-risk of cognitive impairment. Psychogeriatrics 20, 427–436. doi: 10.1111/psyg.12524
Zábó, V., Csiszar, A., Ungvari, Z., and Purebl, G. (2023). Psychological resilience and competence: key promoters of successful aging and flourishing in late life. Geroscience 45, 3045–3058. doi: 10.1007/s11357-023-00856-9
Keywords: mild cognitive impairment, flourishing, correlation analysis, Chinese residents, AD8
Citation: Lv H, Yi X, Guo X, Lin M, Bai D, Nie X, Wang X and Liu X (2025) Correlation between mild cognitive impairment and flourishing among Chinese residents: a cross-sectional study. Front. Psychol. 16:1550013. doi: 10.3389/fpsyg.2025.1550013
Edited by:
Susana Rubio-Valdehita, Complutense University of Madrid, SpainReviewed by:
Wang Zongqin, Wuhan Mental Health Center, ChinaCopyright © 2025 Lv, Yi, Guo, Lin, Bai, Nie, Wang and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaoyun Liu, NDY2MDY3NzkwQHFxLmNvbQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.