 Magnus Vestin1*†
Magnus Vestin1*† Linda Wallin1*†
Linda Wallin1*† Matilda Naesström2
Matilda Naesström2 Ida Blomqvist1
Ida Blomqvist1 Carl Göran Svedin3
Carl Göran Svedin3 Elaine Beaumont4
Elaine Beaumont4 Jussi Jokinen2,5
Jussi Jokinen2,5 Inga Dennhag1
Inga Dennhag1- 1Department of Clinical Science, Child and Adolescent Psychiatry, Umeå University, Umeå, Sweden
- 2Department of Clinical Sciences/Psychiatry, Umeå University, Umeå, Sweden
- 3Department of Social Sciences, Marie Cederschiöld University, Stockholm, Sweden
- 4School of Health and Society, University of Salford, Salford, United Kingdom
- 5Department of Clinical Neuroscience, Karolinska Institutet, Stockholm, Sweden
Introduction: Compassion-focused therapy (CFT) has shown promising outcomes for young people, but research on CFT for this population remains limited. This study aims to evaluate the feasibility and acceptability of a seven-session, therapist-led, internet-based group CFT for young people, and to investigate its preliminary effects.
Methods: A two-arm pilot randomized controlled trial (RCT) was conducted. The study included 42 participants (aged 15–20), experiencing mild to moderate stress, anxiety, or depression, most of whom (90%) were female. In the intervention group, 22 participants were included in the intention-to-treat (ITT) analysis. The trial was registered at ClinicalTrials.gov (NCT05448014).
Results: The intervention group had low attrition and moderate attendance, with 77% completing four or more modules. No adverse events were reported, and participants generally expressed satisfaction with the intervention. Linear regression models showed preliminary between-group differences in two variables. Depressive symptoms increased post-intervention for individuals in the intervention group compared to the waitlist (WL) group (p = 0.002). Self-compassion improved in the intervention group (p = 0.023). These patterns were consistent among participants who completed more than two sessions. Within-group analyses indicated moderate, significant improvements in stress, self-compassion and compassion from others.
Discussion: These preliminary results suggest that CFT is feasible and acceptable and may offer benefits for young people, particularly by enhancing self-compassion and compassion for others. The observed increase in depressive symptoms in the intervention group, despite improvements in self-compassion, warrants further investigation. Larger studies are needed to confirm these preliminary results and to better understand the underlying mechanisms.
1 Introduction
Young people face a variety of daily challenges including physical, cognitive, psychological, and social (Lathren et al., 2019) and have a higher degree of stress, anxiety and depression than at other periods of life (Arnett, 1999; Shorey et al., 2022). These emotional issues among young people have notably increased over the past decades, particularly among females (Shorey et al., 2022; Thapar et al., 2022; Bor et al., 2014), a trend also observed in Sweden (The Swedish National Board of Health and Welfare, 2024; The Public Health Agency of Sweden, 2018) where this study was conducted. Anxiety and depressive disorders are known to be more prevalent in females, with an approximate 2:1 ratio compared with males (Kalin, 2020). Such internalized psychological issues often persist into adulthood if untreated, significantly impacting individuals’ lives (Clayborne et al., 2019; James et al., 2020; Thapar et al., 2012).
Comorbidity among stress, anxiety, and depression is common (Garber and Weersing, 2010; Ehrenreich-May et al., 2017; Kalin, 2020; Vicent et al., 2023), including among young people (Kalin, 2020; Waszczuk et al., 2014). Anxiety and depression are often interwoven rather than distinct constructs across development (McElroy et al., 2018). Evidence-based treatment protocols, particularly those using cognitive behavioral approaches, have been shown to reduce anxiety and depression symptoms in young people (Zemestani et al., 2023; Ehrenreich-May et al., 2017). However, these treatments often focus on symptoms of a single disorder rather than comorbidities or underlying factors (such as self-criticism), leading to suboptimal treatment outcomes (Ehrenreich-May et al., 2017; Wakelin et al., 2022).
Young people’s emotional challenges are frequently linked to concerns about self-evaluation, with negative self-judgment contributing to internal psychological problems (Neff and McGehee, 2010). Shame and self-criticism increase vulnerability and perpetuate issues like stress, anxiety and depression (Gilbert and Procter, 2006). By targeting underlying mechanisms such as emotion dysregulation and negative affect, transdiagnostic treatments can be helpful for those with emotional challenges (Zemestani et al., 2023). Compassion-focused therapy (CFT) is a transdiagnostic approach that targets common psychological processes essential for mental health (Perkins et al., 2023).
The theory of compassion has roots in evolutionary theory, neurobiology, family theory, attachment theory, neuroscience and Buddhist philosophy. CFT contains elements of a variety of therapeutic interventions, including behavior therapy (Gilbert, 2014; Gilbert, 2020). There are several definitions of compassion (Egan et al., 2022; Strauss et al., 2016) and Gilbert’s (2014) definition is “a sensitivity to suffering in self and others, with a commitment to try to alleviate and prevent it” (p. 19). CFT includes psychoeducation on the nature of compassion and Gilbert (2009) suggests that there are three flows of compassion – compassion for self, compassion for others and receiving compassion from others. Low levels of self-compassion and compassion from others have been shown to significantly correlate with both depression and suicidal ideation in adolescents (Jonsson and Dennhag, 2023).
Compassion-focused therapy also involves developing an understanding of the evolved nature of the human mind and body. For example, evolution has left us with “tricky brains” that get caught up in thinking–feeling loops and it has been proposed that human emotions evolved to serve specific functions that are represented by three systems – threat, drive and soothing (Beaumont et al., 2024). The drive system focuses on achieving and activating seeking–engagement strategies; the threat system is threat-focused and its function is to activate strategies that have evolved to keep us safe; and the soothing system is a positive system for well-being that helps to regulate the threat and drive systems (Gilbert, 2014). CFT seeks to increase compassion and activate the soothing system, bringing balance to the threat and drive systems. This approach not only helps young people to cope with current challenges but also prepares them for upcoming stressors and strengthens their willingness to explore (Bluth et al., 2018).
The evidence base for CFT has grown in both clinical and non-clinical populations (Ferrari et al., 2019; Kirby, 2017; Millard et al., 2023; Neff, 2023; Beaumont et al., 2016; Beaumont et al., 2021). Over the past 30 years, studies on CFT have demonstrated benefits for adults, including reductions in depression, self-criticism, distress, and anxiety (Ferrari et al., 2019; Marsh et al., 2018; Williamson, 2020; Craig et al., 2020; Wakelin et al., 2022; Petrocchi et al., 2023).
Despite the importance of intervening during adolescence to prevent the development of psychopathologies (Bluth et al., 2017), relatively few CFT intervention studies have focused on young people (Boggiss et al., 2020; Bluth et al., 2016; Bratt A. et al., 2020; Karr et al., 2020; Seekis et al., 2023). A review by Egan et al. (2022) reported promising outcomes, suggesting that self-compassion interventions can reduce depression and anxiety in young people. However, there remains a need for randomized controlled trials (RCTs) (Bridge et al., 2023), as no RCT has yet evaluated CFT specifically for young people.
Although mental health disorders are highly prevalent in young people (Merikangas et al., 2010; Shorey et al., 2022), most do not receive psychological treatment (Merikangas et al., 2011). In Sweden, access to psychological care varies widely across regions, partly due to availability issues (The Swedish National Board of Health and Welfare, 2019). Internet-based interventions have improved access to effective psychological treatments (Vigerland et al., 2016), with usage growing significantly during the COVID-19 pandemic (Lin et al., 2021). Evidence supports the effectiveness of internet-delivered interventions, including videoconferencing, in improving youth mental health (Porter et al., 2022; von Wirth et al., 2023; Stewart et al., 2017; Karing, 2023; Stewart et al., 2020; Ebert et al., 2015; Välimäki et al., 2017). These interventions may also benefit socioeconomically and digitally marginalized young people (Piers et al., 2023).
Group therapy offers the advantage of reaching multiple young people simultaneously, although some individuals may find it challenging to engage in a group setting (Erekson et al., 2024). Nevertheless, studies suggest that psychotherapy outcomes for young people are comparable in both group and individual formats (Eckshtain et al., 2020). Small group-based CFT with young people has been conducted with positive experiences of the group setting (Bratt A. et al., 2020; Lau-Zhu and Vella, 2023).
This study is part of the project CUST (Compassion-Focused Therapy for Young People with Stress) in northern Sweden, which aims to develop and evaluate internet-based compassion-focused interventions for young people with emotional challenges in rural areas of the country (Dennhag, 2018).
The aim of this study is to determine whether therapist-led internet-based videoconferencing group CFT is feasible and acceptable to use with young people between 15 and 20 years of age in Sweden. Additionally, the study assesses preliminary effects on stress, anxiety and depression symptoms to determine if a larger RCT is justified.
2 Methods
This study was a single-blinded, two-arm (CFT intervention group vs. WL group) randomized controlled trial for young people with mild to moderate symptoms of depression, anxiety or stress. The clinical trial protocol was approved by the Swedish Ethical Review Authority (no. 2021–04357; 2022–01318-02, 2022–02931-02) and registered at ClinicalTrials.gov (NCT05448014). Informed consent was obtained from all participants. The study adhered to the CONSORT statement (Eldridge et al., 2016; Butcher et al., 2022) and participant flow is illustrated in Figure 1.
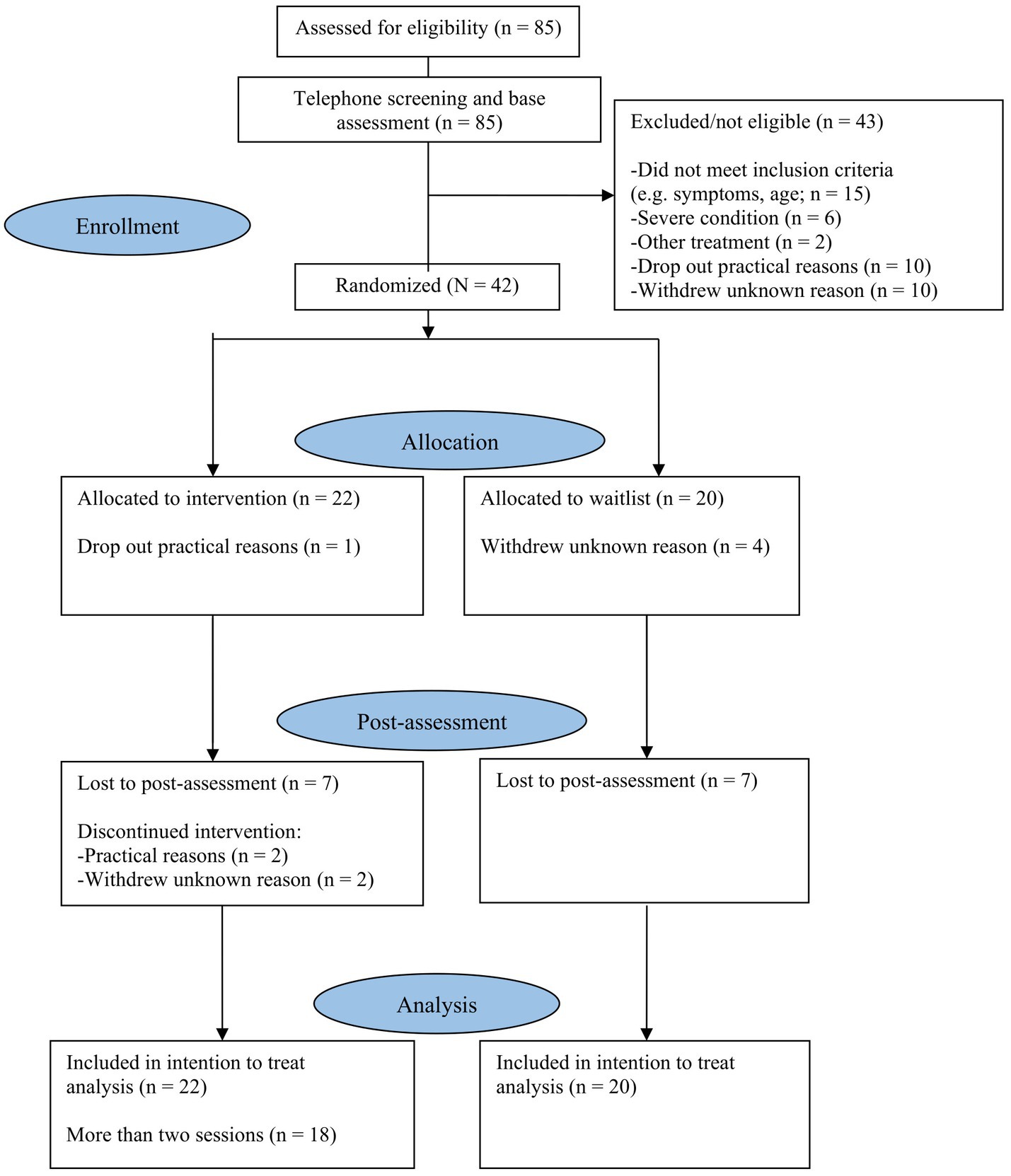
Figure 1. CONSORT flowchart of participants.
2.1 Procedure
A preliminary study was previously conducted with seven participants, six of whom completed the CFT intervention. The results indicated that none of the exercises had a negative impact, and overall, participants reported a positive experience with CFT (Sjölander, 2022).
The current study was promoted to young people via social media, flyers, and direct outreach by project staff or personnel at schools and primary care health centers in northern Sweden. The recruitment efforts were aimed at individuals of all genders. Young people interested in participating contacted a research assistant by text message or email. The research assistants were psychology students with at least 3 years of psychology studies including clinical experience. They administered the assessment procedure, which included web-based questionnaires and a semi-structured phone interview to determine eligibility. The principal investigator (PI; also author Inga Dennhag) regularly supervised the assistants.
Study data were collected and managed using REDCap (Research Electronic Data Capture) hosted at Umeå University (Harris et al., 2009; Harris et al., 2019). REDCap is a secure, web-based platform designed to support data capture for research studies.
A CFT group was initiated once the sufficient number of participants (n = 4–8) were available for randomization. During the same period that a CFT group completed the pre- and post-intervention questionnaires, a WL group did the same. To ensure that the intervention could start with enough participants per group within a reasonable time after sign-up, five non-randomized participants who did not meet the inclusion criteria for symptom level were included in the sessions but excluded from the analyses.
In total, seven CFT groups were conducted between September 2022 and January 2024, covering all seasons of the year. The interventions were led by a psychotherapist, supported by an assistant. Across the seven groups, two psychotherapists served as leaders, with the PI being one of them. Both psychotherapists have experience in providing psychotherapy for young people and the PI has additional training in compassion-based approaches for young people. For the first group, the PI led the sessions, with the other psychotherapist assisting. The therapist and assistants received ongoing supervision from the PI.
2.2 Participants
Participants invited to this study were between 15 and 20 years old. The inclusion criteria were: (a) symptoms of stress (≥22 on PSS) and/or symptoms of anxiety (≥9 in subscale Anxiety in TSCC) and/or symptoms of depression (≥10 in subscale Depression in TSCC), (b) the ability to speak Swedish, (c) the ability to read and complete forms in Swedish, (d) had at least one close and stable relationship with an adult, and (e) ability to participate in an online group setting. The exclusion criteria included: (a) severe psychological issues that could hinder participation in group treatment, (b) suicidal risk (scoring 4 or higher on item 12 in MADRS-Y self-report with clinical assessment of active suicidal intent during the diagnostic screening interview), (c) bipolar disorder, (d) autism, (e) anorexia nervosa, (f) current substance or alcohol dependence, (g) current psychosis, (h) current active participation in psychotherapy, and (i) recent initiation or withdrawal of antidepressant treatment (participants with prescribed medications for anxiety or depressive disorders were eligible if the dosage had remained constant for at least 1 month).
2.3 Randomization
Randomization was performed by a statistician from another department (Registercentrum Norr, Umeå University). Block randomization with a block size of four was used to assign participants to the intervention and WL groups simultaneously. Blinded outcome assessment was applied to minimize bias in estimating treatment effects (Kahan et al., 2014).
2.4 Waitlist control group
Participants in the WL group completed self-report questionnaires at pre-intervention and again after 8 weeks (post-intervention). There was no scheduled contact with study staff during the WL period. However, participants had access to contact details to the research assistant and the PI. After completing the WL, participants were offered the CFT intervention. Those who participated in the intervention after the WL period are not included as intervention participants in the analyses.
2.5 The CFT intervention
A new Swedish CFT workbook (Dennhag, 2021) was developed specifically for young people in Sweden by the last author, Inga Dennhag, inspired by Professor Paul Gilbert’s CFT model and by the CFT ideas and practices developed for young people in The Kindness Workbook (Beaumont and Welford, 2020). The intervention incorporates key elements of CFT, including the three affect regulation systems—threat, drive, and soothing; the development of a compassionate self; addressing self-criticism, shame, and guilt; practicing mindfulness; and fostering emotional regulation through compassion.
The Swedish workbook (Dennhag, 2021) includes seven modules: (1) What is compassion?, (2) Understanding myself, (3) Life compass, (4) Self-compassion and my body, (5) Feelings and compassion, (6) Creating balanced thoughts, and (7) Imagination. There are a total of 20 exercises. Participants received a digital copy of the workbook (Dennhag, 2021) to practice between sessions, and the leaders had PowerPoint slides and a therapist manual containing the same modules as the workbook. Each session followed a consistent structure, designed to strengthen the participants’ capacity for compassion, alternating between theory and exercises, and concluding with an introduction to the homework assignment. An overview of the intervention content is presented in Figure 2.
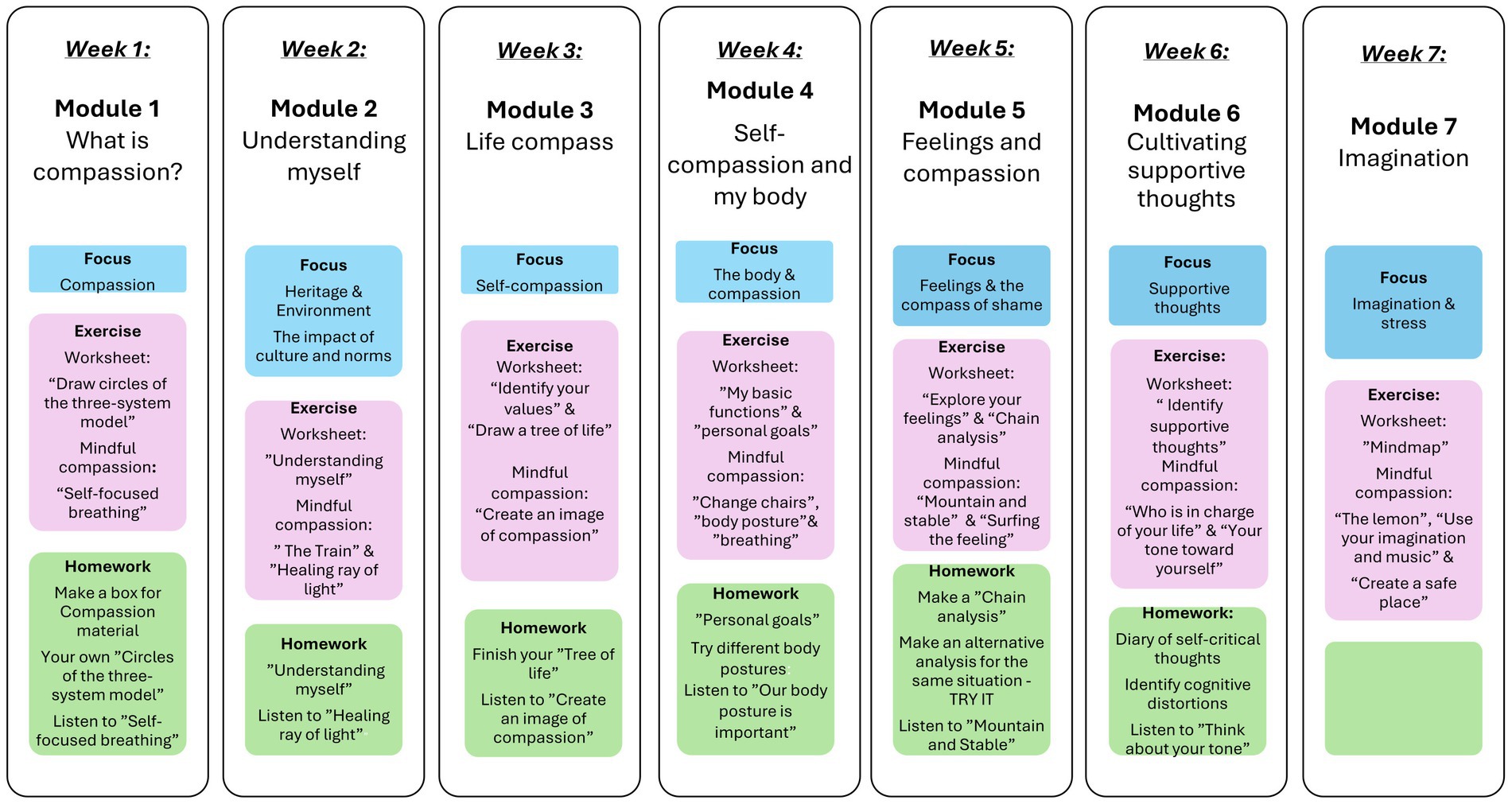
Figure 2. Overview of the CFT intervention structure.
2.6 Acceptability and feasibility
Total dropout rates, as well as the percentage of completed pre-intervention and post-intervention assessments, were analyzed for both groups. The treatment adherence was assessed by classifying participants who completed fewer than half of the modules (<4) as having discontinued treatment (Grudin et al., 2022). The mean number of completed modules was also calculated.
Participants were asked to complete a written evaluation in which they rated the following: (1) whether the content and objectives were clearly explained, (2) whether the training goals were met, (3) the number of sessions they attended (despite attendance records being maintained), (4) the extent to which they completed the homework assignments, and (5) their overall satisfaction with the training. Additionally, the evaluation invited further feedback on the intervention, including perceived advantages and disadvantages.
Participants were instructed to report any adverse events during the intervention period to the research assistants or group leader. Adverse events were also assessed post-intervention with the question: “Did the CFT training help you to feel better?” with one of the response options being: “No, it seems to have made it worse.”
It was also important to assess whether the CFT leaders found the intervention acceptable and if they were able to deliver it as intended, and to identify any difficulties in implementing program elements or other challenges (Teresi et al., 2022). This was investigated through a feedback survey specifically designed for the psychotherapists and their assistants involved in the CFT treatment, administered after all intervention groups were completed.
2.7 Measures
All measures were web-based, self-reported questionnaires administered at pre- and post-intervention.
2.7.1 Primary outcomes
2.7.1.1 TSCC – Trauma Symptom Checklist for Children
The TSCC (Briere, 1996) is a self-report questionnaire for children and adolescents aged 8–17 that measures symptoms related to traumatic experiences. Responses are recorded on a 4-point scale ranging from 0 (“never”) to 3 (“almost all the time”). The internal consistency has shown to be good (Briere, 1996), including for the Swedish translation (Nilsson et al., 2008). TSCC includes six clinical scales with 9–10 items in each. In the current study, the Anxiety and Depression clinical scales were used as primary outcomes, and the Cronbach’s alpha was 0.87.
2.7.1.2 PSS-10 – The 10-item Perceived Stress Scale
The PSS-10 (Cohen S., 1988) is a self-report questionnaire for young people and adults that measures feelings and thoughts related to the stress-associated components of unpredictable, uncontrollable, and overwhelming life events. The self-report is measured on a 5-point scale, ranging from 0 to 4, with higher scores indicating greater levels of stress (Nordin and Nordin, 2013). The PSS-10 has acceptable psychometric properties (Lee, 2012) and its internal consistency has shown to be good, including for the Swedish translation (Nordin and Nordin, 2013). In the current study, the Cronbach’s alpha was 0.85.
2.7.2 Secondary outcomes
2.7.2.1 MADRS-Y – Montgomery–Åsberg Depression Rating Scale – Youth
The MADRS-Y is a self-report questionnaire for young people aged 12 to 20 (Vestin et al., 2022) adapted from the adult version MADRS-S (Svanborg and Åsberg, 1994). This 12-item self-report uses a 7-point scale ranging from 0 (low) to 6 (high), and a higher score indicates more severe depression. MADRS-Y was included in the current study to measure symptoms of depression according to the DSM-5 (American Psychiatric Association, 2013), but as a secondary outcome measure because it has just recently been validated. The internal consistency has been shown to be good in both a Swedish normative sample (Vestin et al., 2022) and a Swedish clinical sample (Vestin et al., 2024). In the current study, the Cronbach’s alpha was 0.82.
2.7.2.2 CEASY-SE – The Compassionate Engagement and Action Scale for Youths – Swedish version
The CEASY-SE is a self-report questionnaire for young people aged 12 to 20, adapted from the adult version CEAS (Gilbert, 2017). It includes the three subscales: compassion for others, compassion from others, and self-compassion (Henje et al., 2020). The 30-item self-report is measured on a 10-point scale ranging from 1 (“never”) to 10 (“always”). The internal consistency has shown to be good in a Swedish sample (Henje et al., 2020). In this study, three control items were removed, resulting in a 27-item version. Each subscale, as well as the total scale, was analyzed separately. In the current study, the Cronbach’s alpha was 0.91 for compassion for others, 0.91 for compassion from others, 0.88 for self-compassion and 0.90 for the total scale.
2.8 Statistical analysis
Statistical analyses were conducted using SPSS version 28.0. Data were screened for faulty values and dependent variables were examined for normality. Boxplots were used to check for outliers and the data were examined for normality. Outliers were treated as missing values. We identified only one outlier in the control group, where extreme values (either very low or very high) were recorded at post-intervention. Continuous variables were checked for normality using histograms and scores for skewness and kurtosis. Normal Q–Q plots and scatterplots indicated that the assumptions of linearity and homoscedasticity were satisfied. Independence of observations was assessed with the Durbin-Watson test and all scales were around 2 (ranging from 1.91 to 2.21). There was no multicollinearity in the regression models measured by variance inflation factor (VIF) and tolerance measures.
Descriptives were calculated using standard measures. Sum scores, means, and standard deviations were calculated for each self-report measure.
Missing data were imputed on pre-test using multiple imputation (n = 354) missing values of 2,586 (13.69%) on PSS, TSCC, CEASY-SE at pre-test, and n = 872 missing values (33.72%) on post-test with 10 iterations and 50 imputations, to enable calculation of sum scores despite the missing items. For the pre-test scores, the imputation model was predicted by the baseline scores of TSCC Anxiety and Depression subscales (complete data), pre-test scores of TSCC, PSS, MADRS-Y, CEASY-SE age, gender, and socioeconomic status, and we used a random seed. For the post-test scores, the imputation model was predicted by the baseline scores of TSCC Anxiety and Depression subscales (complete data) and post-test scores of TSCC, PSS, MADRS-Y, CEASY-SE age, gender, and socioeconomic status were used as predictors, and we used a random seed. WL group and intervention group data were imputed separately. The results from imputed data did not differ from the unimputed data.
We used intention-to-treat analysis (ITT) (Gupta, 2011), meaning that every randomized subject was included in the analyses. We also calculated results for those who participated in more than two intervention sessions. Between-group differences at pre-test between CFT and WL group were calculated with independent t-tests.
Between-group differences on primary and secondary outcome measures were calculated with several linear regressions, where post-test values were the dependent variable, and pre-test values and group (intervention or waitlist group) were the independent variables. Within-group differences were calculated with paired sample t-tests. Both Cohen’s d (using the sample standard deviation of the mean difference) and Hedges’ g corrections (using the sample standard deviation of the mean difference plus a correction factor) were used to illustrate effect sizes. We interpreted the within-group differences according to Cohen’s definition of small (d ≥ 0.20), medium (d ≥ 0.50), and large effects (d ≥ 0.80) (Cohen J., 1988). Hedges’ g is similar to Cohen’s d but includes a correction factor for small samples.
Additionally, within-participant change was calculated using clinically significant change (Jacobson and Truax, 1991; Blampied, 2016). Clinically significant change in stress symptoms (PSS) was computed according to Jacobson and Truax (1991) with two criteria: the change should be reliable and the client should before intervention belong to a dysfunctional domain and after intervention to a functional domain. The cutoff score to separate the dysfunctional domain from the functional domain was computed as c [c = (SD0*M1 + SD1*M0)/(SD0 + SD1) M0 = mean of normative sample, SD0 = standard deviation of normative sample, M1 = mean of patient sample, SD1 = standard deviation of patient sample]. The reliable change was calculated with the Reliable Change Index (RCI), as RCI = (X2-X1)/Sdiff (Sdiff = √2(SE)2) (SE = SD1√1-r, where r is the reliability of PSS; here, r = 0.85). The RCI specifies the amount of change a client must show on a specific psychometric instrument between measurement occasions for that change to be reliable. Participants in the intervention group with a clinically significant change, i.e., both a change from a dysfunctional to a functional domain on PSS and a reliable change, were classified as “recovered.” Participants with only a reliable positive change on PSS were classified as “improved.” Participants with no reliable change were classified as “unchanged” and participants with a reliable negative change were classified as “deteriorated.”
3 Results
The overarching aim was to determine whether therapist-led internet-based group CFT is feasible and acceptable for treating depression, anxiety and stress in young people aged 15 to 20 in Sweden. An overview of the participant flow is presented in Figure 1. Of the total sample (N = 42), 90% of the participants were female and the mean age was 17.2 years (range 15–20 years). For socioeconomic data, the Swedish socioeconomic classification system (SEI) developed by Statistics Sweden (SCB (Statistics Sweden), 1982) was used to estimate a socioeconomic ranking based on six distinct classes. In the current sample, the parents’ socioeconomic status was distributed across only four classes, with no parents classified as unemployed or students. Socio-demographic data did not differ between the intervention and WL groups. The demographic characteristics of the participants are presented in Table 1.
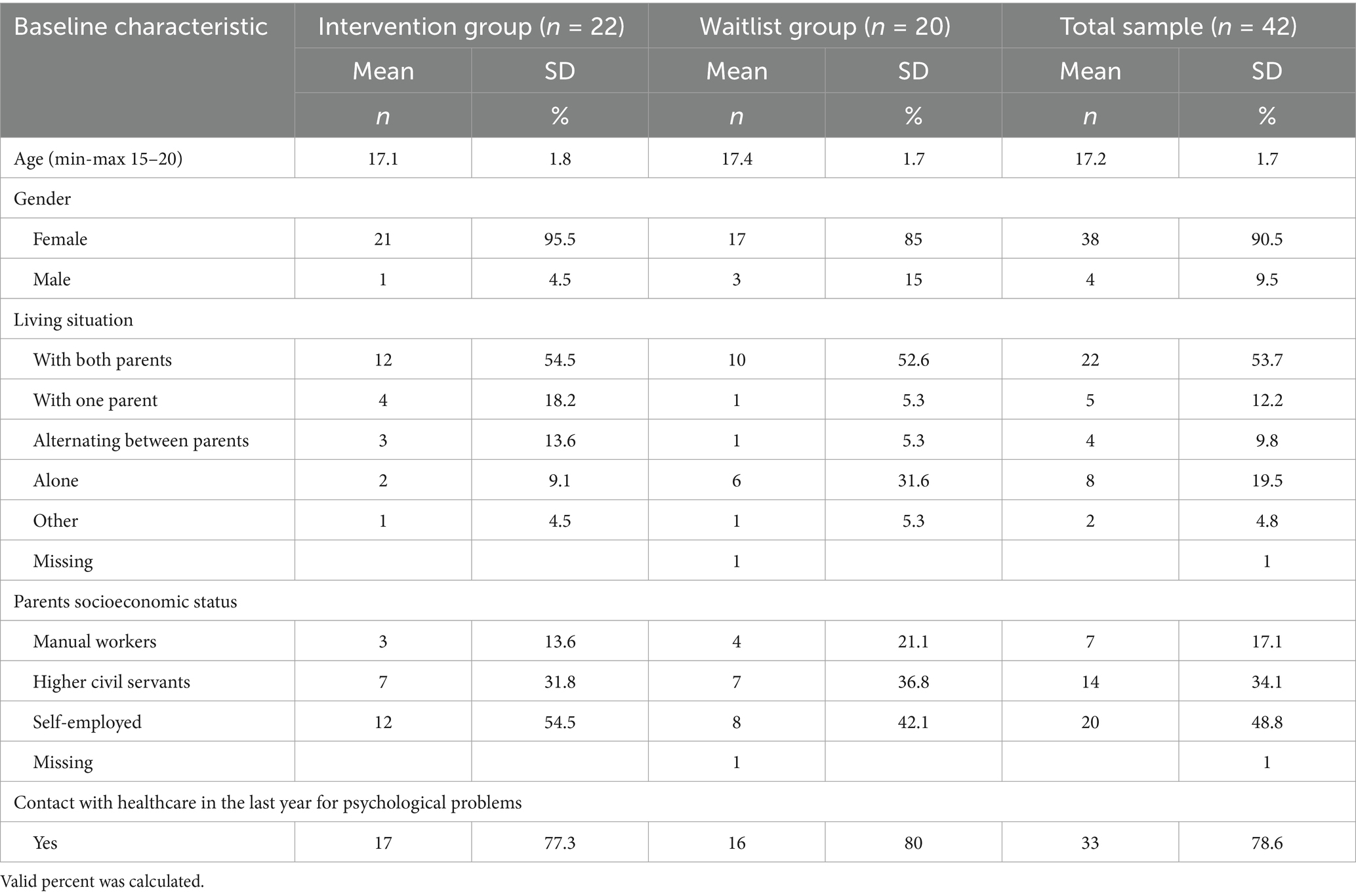
Table 1. Baseline demographic and characteristics for each group and total sample.
3.1 Feasibility and acceptability
Feasibility and acceptability were evaluated based on dropout rates, retention, adherence, participant satisfaction, compliance, and clinician feedback. The dropout rate for the intervention group (n = 22) was 23% (n = 5), while the dropout rate for the WL group was 20% (n = 4). Completion rates for the pre-intervention assessment were 86% overall (n = 36), with 91% for the intervention group (n = 20) and 80% in the WL group (n = 16). Post-intervention assessment rates were 67% overall (n = 28), with 68% for the intervention group (n = 15) and 65% for the WL group (n = 13).
In terms of intervention adherence, participants completed an average of 5.5 modules (M = 4.68, SD = 2.12) out of seven. A total of 18% completed all the modules, while 82% completed more than two modules. Additionally, 77% completed four or more modules, indicating a moderate level of adherence to the intervention. Dropout tended to occur more commonly early in the intervention process. For a detailed overview (see Figure 3).
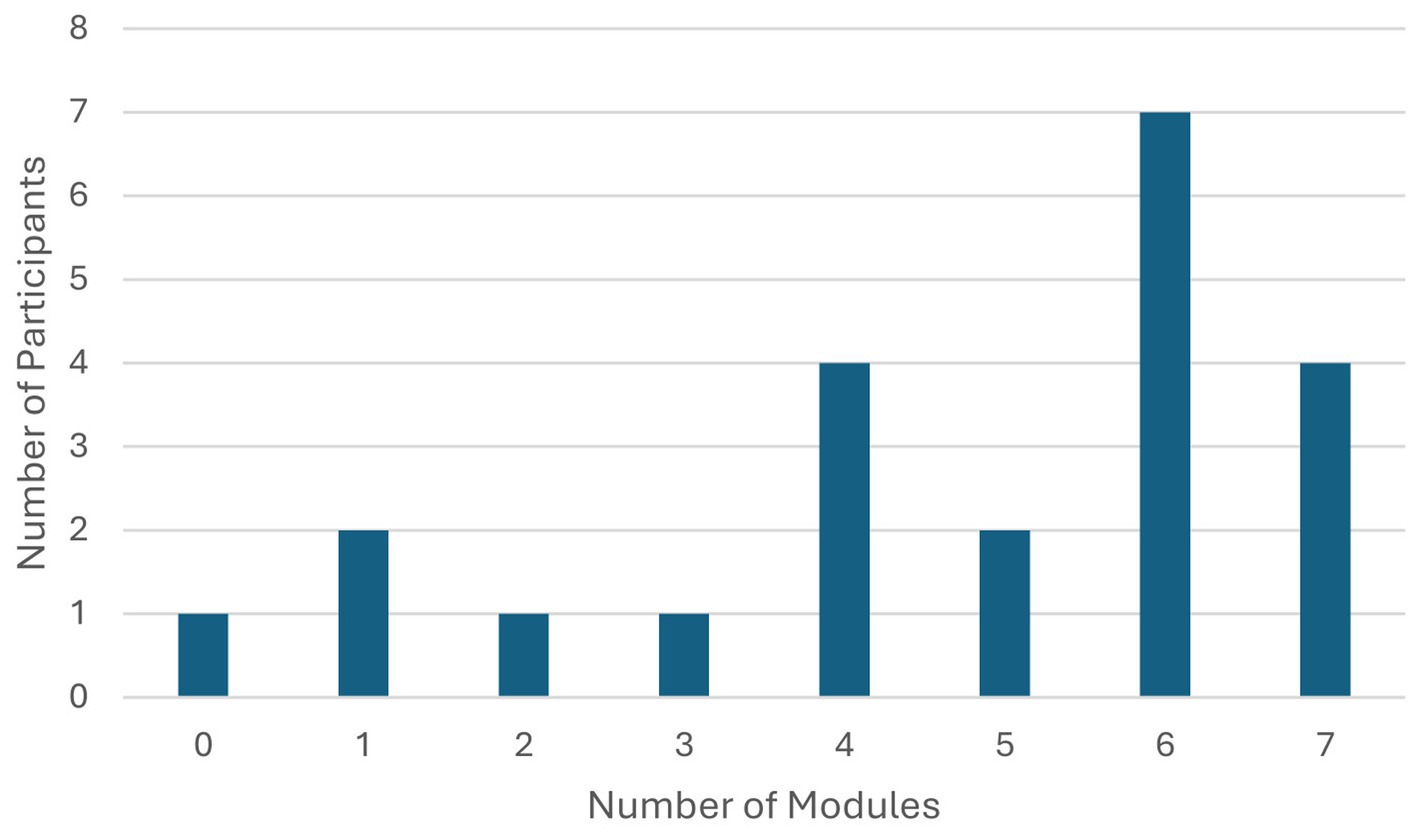
Figure 3. Completed modules during the CFT intervention.
After the intervention, participants in the intervention group completed an evaluation form (n = 15). Most participants (n = 14) felt the intervention’s content and objectives (increasing self-compassion, reducing self-criticism, and improving the regulation of unpleasant emotions) were clearly explained, either completely (n = 10) or to some extent (n = 4) before the start of the intervention. One participant indicated “did not know.” Most participants (n = 13) also felt that the objectives were addressed within the intervention, either completely (n = 7) or to some extent (n = 6). One participant responded “no,” and one selected “did not know.” Approximately one-quarter of the participants (n = 4) reported completing their homework almost always or often, nine completed it sometimes, and two completed it rarely or never. Many participants (n = 10) were either very satisfied (n = 3) or mostly satisfied (n = 7) with the intervention; five participants were neutral, and none were dissatisfied. No adverse events were reported during the intervention, and no participant selected the response “No, it seems to have made it worse” to the question “Did the CFT training help you feel better?”
The psychotherapists and research assistants (hereafter referred to as leaders) who led the groups also completed an evaluation form after the intervention groups were finished (n = 8) to provide additional insights on the intervention’s feasibility. Most leaders found it easy (n = 5) or very easy (n = 2) to implement the CFT intervention according to the protocol, while one leader was neutral. All leaders felt comfortable (n = 5) or very comfortable using the protocol and all of them agreed that the intervention was accepted by the young people [well (n = 5) and very well (n = 3)]. Most leaders found the intervention effective (n = 5), two expressed a neutral response, and one answer was missing.
3.2 Descriptive statistics
Table 2 provides descriptive statistics showing the observed group means and standard deviations for primary and secondary outcomes at both pre-intervention and post-intervention. There was a difference between the intervention and WL groups in the pre-intervention assessment. The intervention group had higher scores for stress, depression, and anxiety.
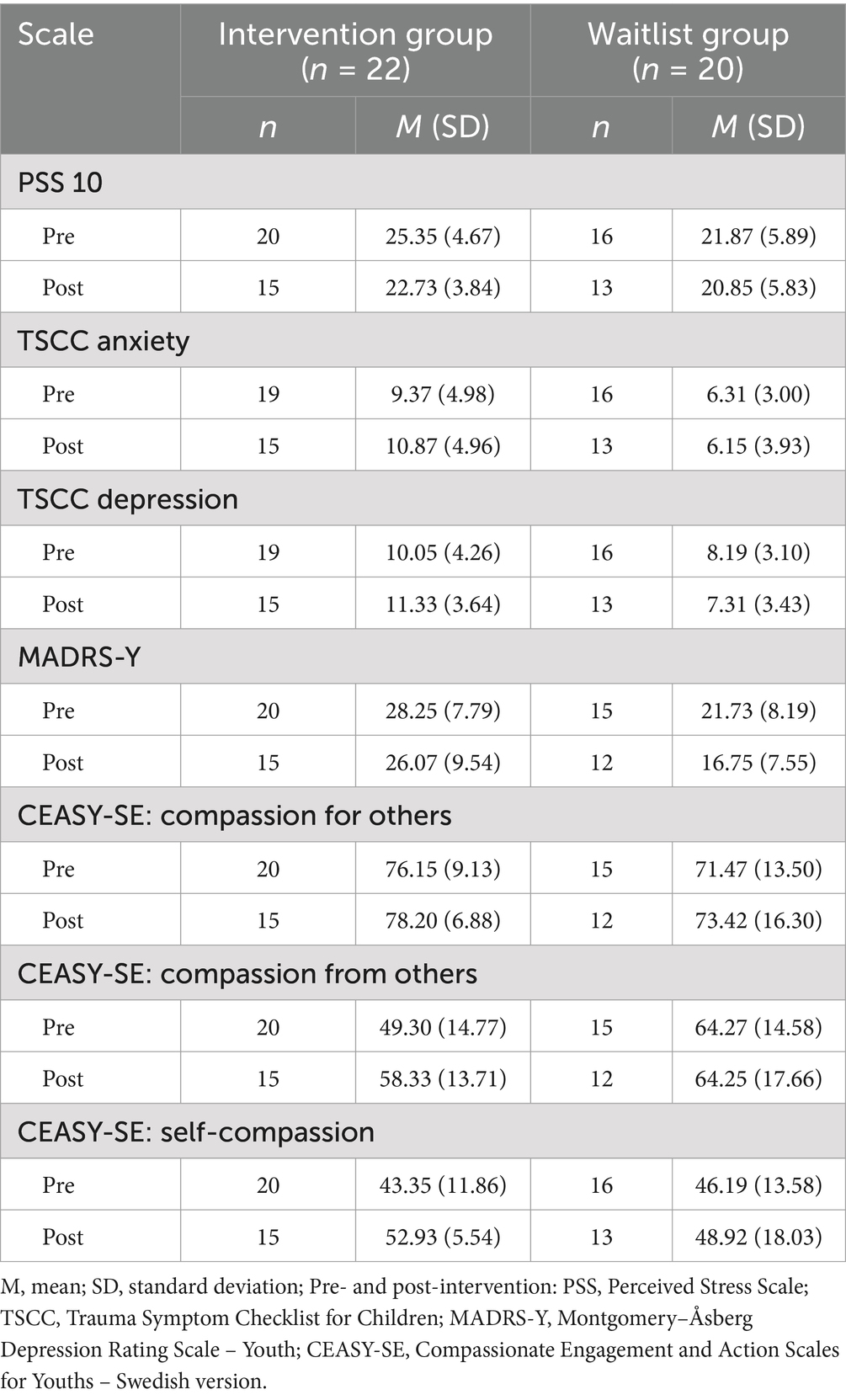
Table 2. Descriptive statistics for observed group means and standard deviations of primary and secondary outcomes.
3.3 Efficacy of the CTF intervention
The preliminary effects on stress, anxiety, and depression symptoms were calculated and presented as both between-group and within-group differences.
3.3.1 Between-group differences
In the linear regression models for intention-to-treat (ITT) analyses, two variables showed significant differences between the intervention and WL groups at the p < 0.05 level. An unexpected finding in the primary outcome was that depression (TSCC Depression subscale) had significantly increased in the intervention group compared to the WL group. This result indicates that depression symptoms deteriorated more in the intervention group than in the WL group. For the secondary outcomes, self-compassion (CEASY-SE) increased significantly in the intervention group and differed significantly from the WL group. Table 3 presents the results of the regression analysis of associations between groups for the ITT.
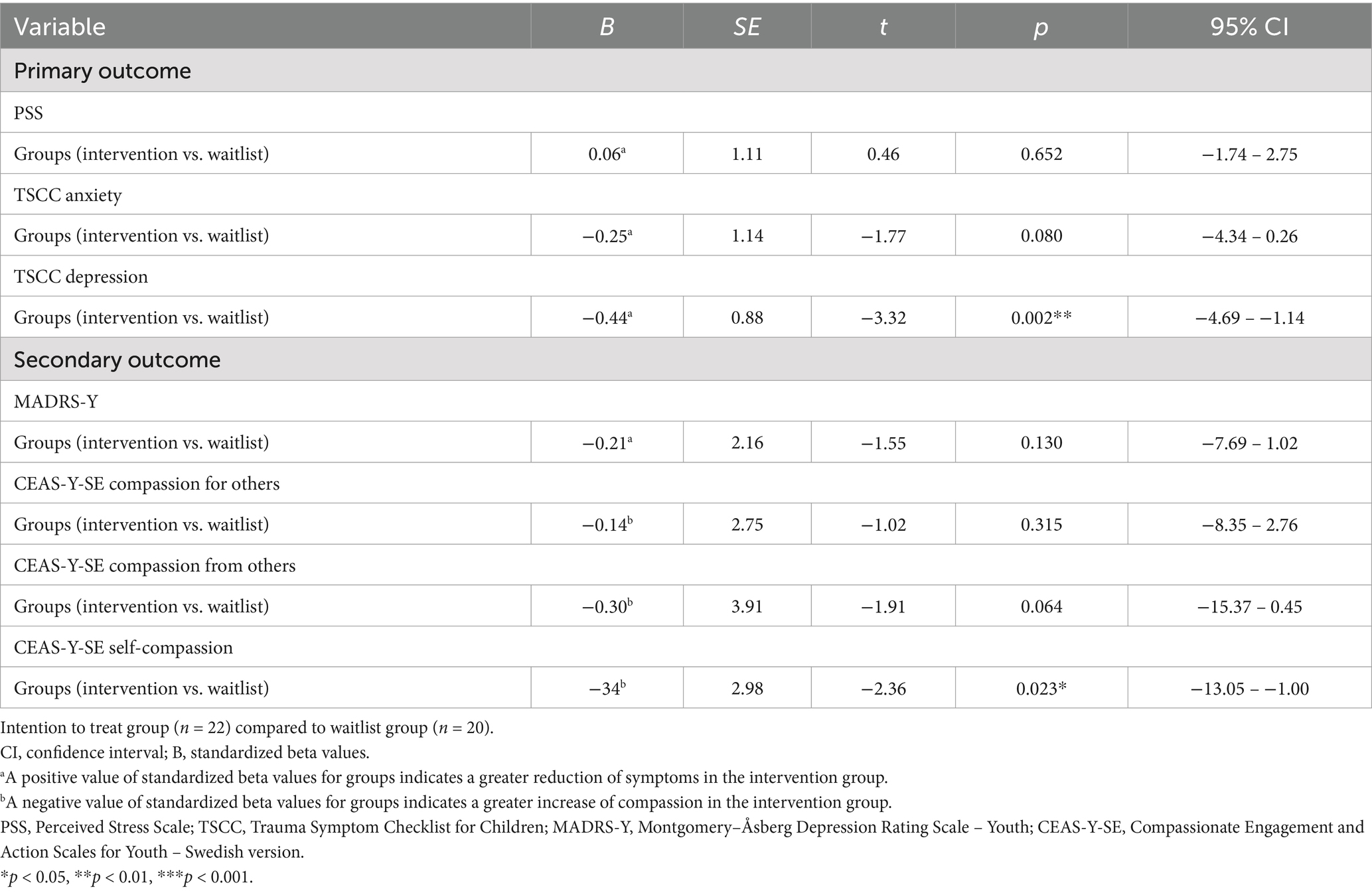
Table 3. Regressions of associations between intervention and waitlist groups.
A pattern similar to the ITT analyses was observed in the analyses based on participation in more than two sessions. Depression (TSCC Depression subscale) significantly increased in the intervention group compared to the WL group. Self-compassion also significantly increased in the intervention group compared to the WL group. See Table 4 for the results.
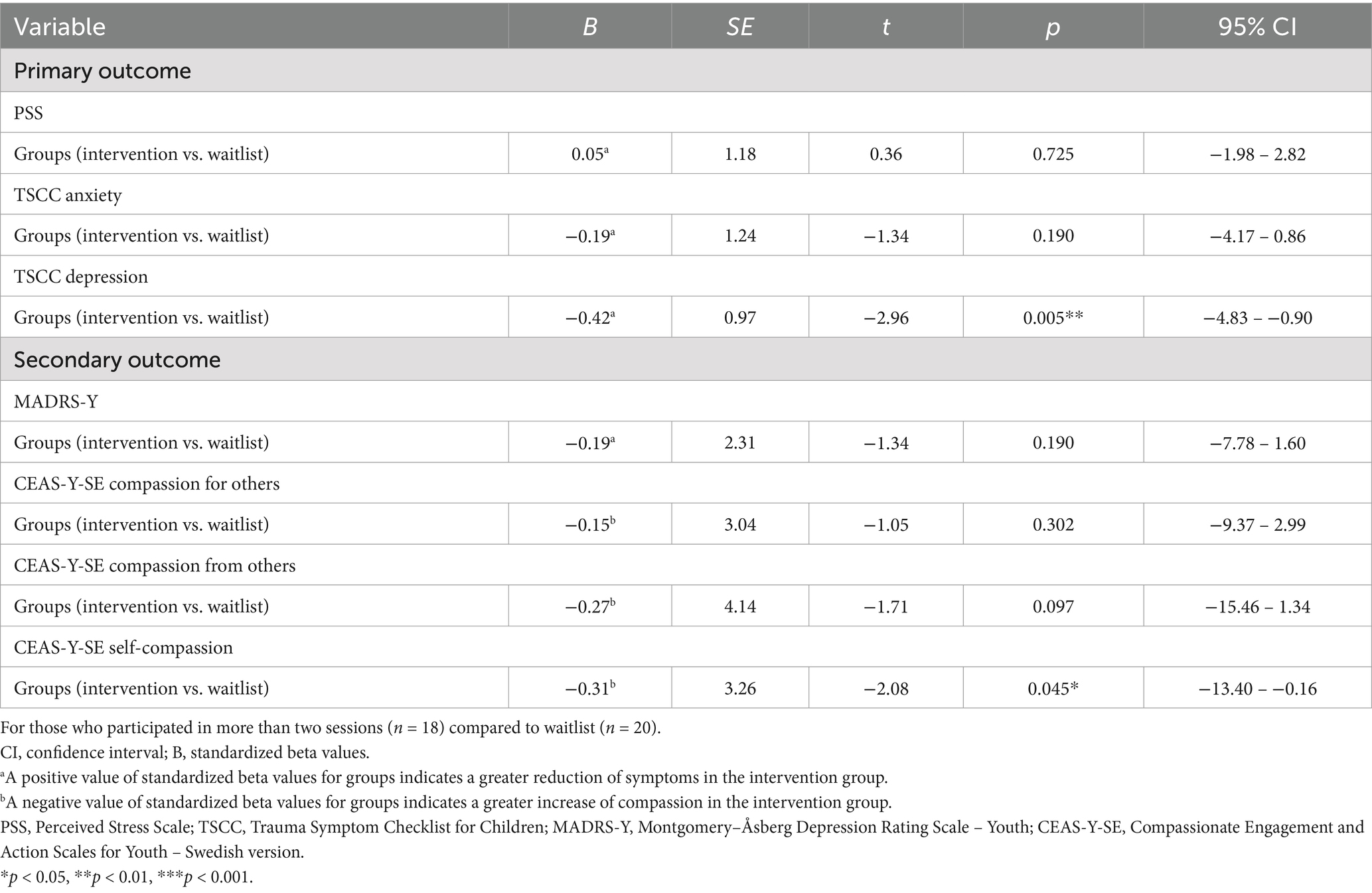
Table 4. Regressions of associations between intervention and waitlist groups values for participants completed more than two sessions.
3.3.2 Within-group differences
Paired sample t-tests were conducted to evaluate within-group differences among the intervention participants who attended more than two sessions. Significant moderate within-group differences were found for perceived stress (p = 0.012), compassion from others (p = 0.013), and self-compassion (p = 0.006). No statistically significant differences were observed for anxiety or depression symptoms or compassion for others. Table 5 presents an overview of the results.
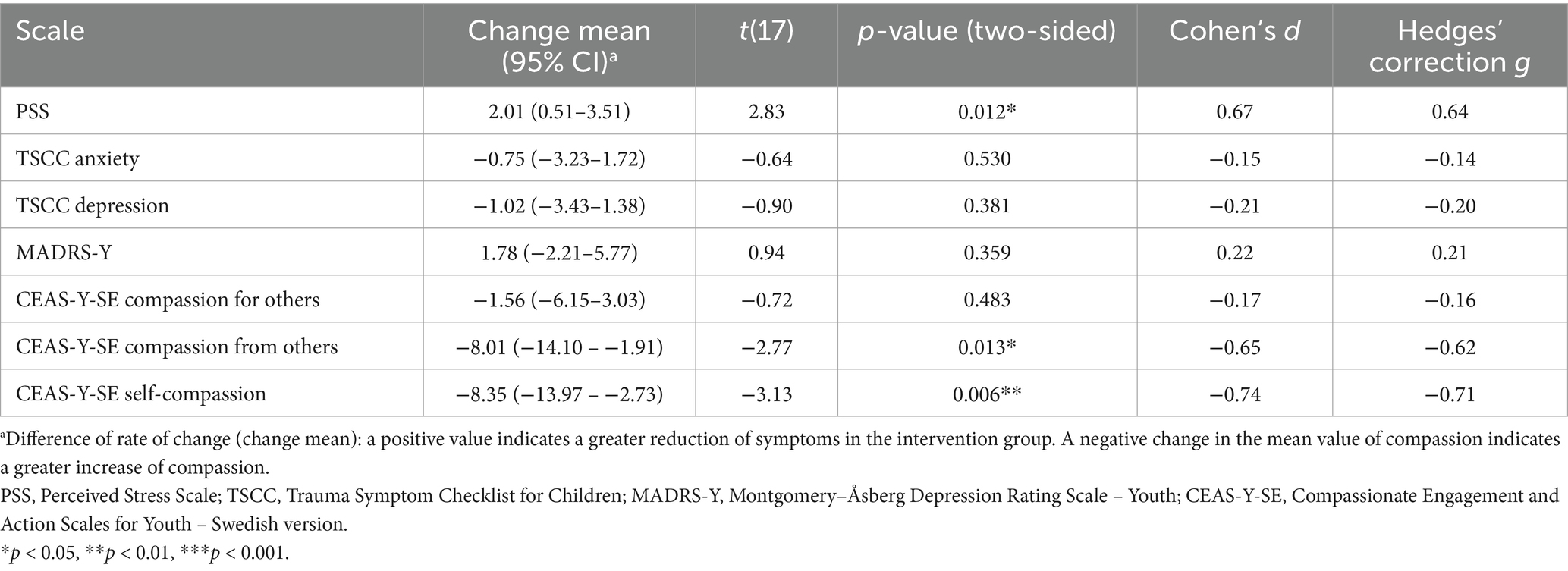
Table 5. Within-group differences between participants in the intervention group who completed more than two sessions (n = 18).
3.3.3 Response and deterioration rates
Clinically significant change analyses were conducted for participants (n = 18) in the intervention group who completed more than two sessions to assess whether they had recovered, improved, deteriorated, or remained unchanged regarding stress symptoms (PSS). The PSS was chosen because most participants identified themselves as stressed, regardless of depression or anxiety symptoms. The comparative normative Swedish sample for the PSS was aged 18–34 [N = 706, 441 women; (Nordin and Nordin, 2013)]. The mean PSS score in the normative sample (M0) was 15.6 (SD0 = 6.67), whereas the mean in the intervention group (M1) was 25.35 (SD1 = 4.67). The cutoff score between a functional and dysfunctional domain was estimated at 21.62 on the PSS, with scores equal to or above the cutoff indicating the dysfunctional domain.
Reliable Change Index (RCI) was calculated to determine whether participants in the intervention group demonstrated a statistically reliable change. An RCI greater than 1.96 (p < 0.05) indicated a real change, and in our sample, participants needed to decrease their PSS scores by at least ≥1.02 (z) scores to achieve a reliable change. On the PSS scale, a score of 21.62 serves as the cutoff between the functional and dysfunctional domains, with the dysfunctional domain encompassing scores above this threshold.
The classification of clinical change indicated that just over three-quarters (78%; n = 14) of all participants were in the dysfunctional domain before therapy. The total outcome, considering a clinical change and a reliable change for PSS, showed that 56% (n = 10) responded positively (either recovered 11%; n = 2 or improved 44%; n = 8), 28% (n = 5) remained unchanged, and 17% (n = 3) in the intervention group deteriorated. See Figure 4 for the individual means of PSS score before and after group intervention and WL. Figure 5 illustrates individual self-compassion scores before and after the intervention for participants who completed more than two sessions and WL group. As seen in the figure, self-compassion displayed a positive trend in the intervention group.
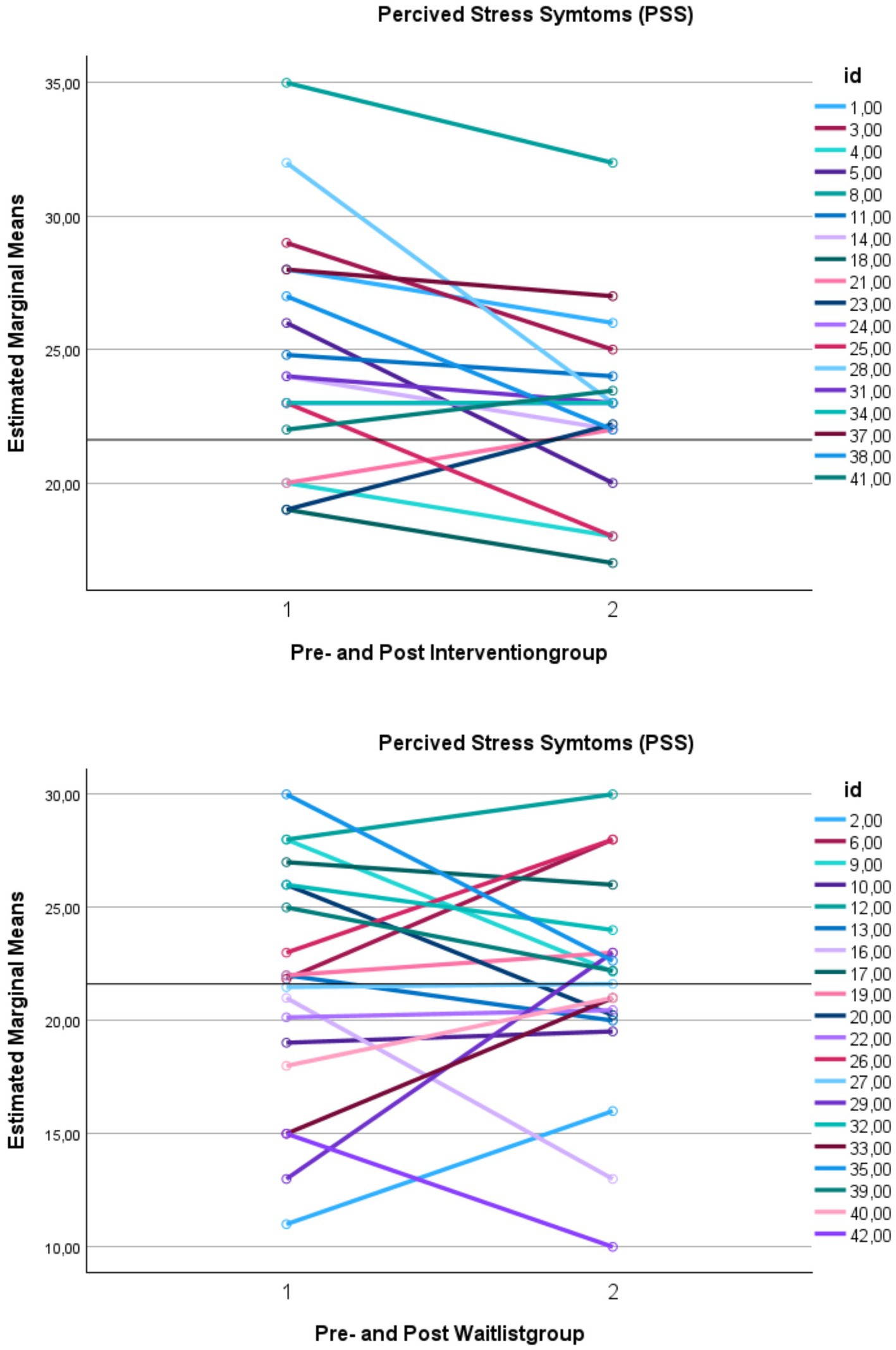
Figure 4. Changes in perceived stress symptoms for participants who attended more than two sessions and waitlist group. This figure demonstrates the means of perceived stress (PSS) over time. PSS, Perceived Stress Scale. Y-axis: Means. X-axis: Time 1 = scores before intervention, and Time 2 = scores after treatment. A cutoff of 21.62 separates functional and dysfunctional domains; scores above represent the dysfunctional domain, while scores below represent the functional domain.
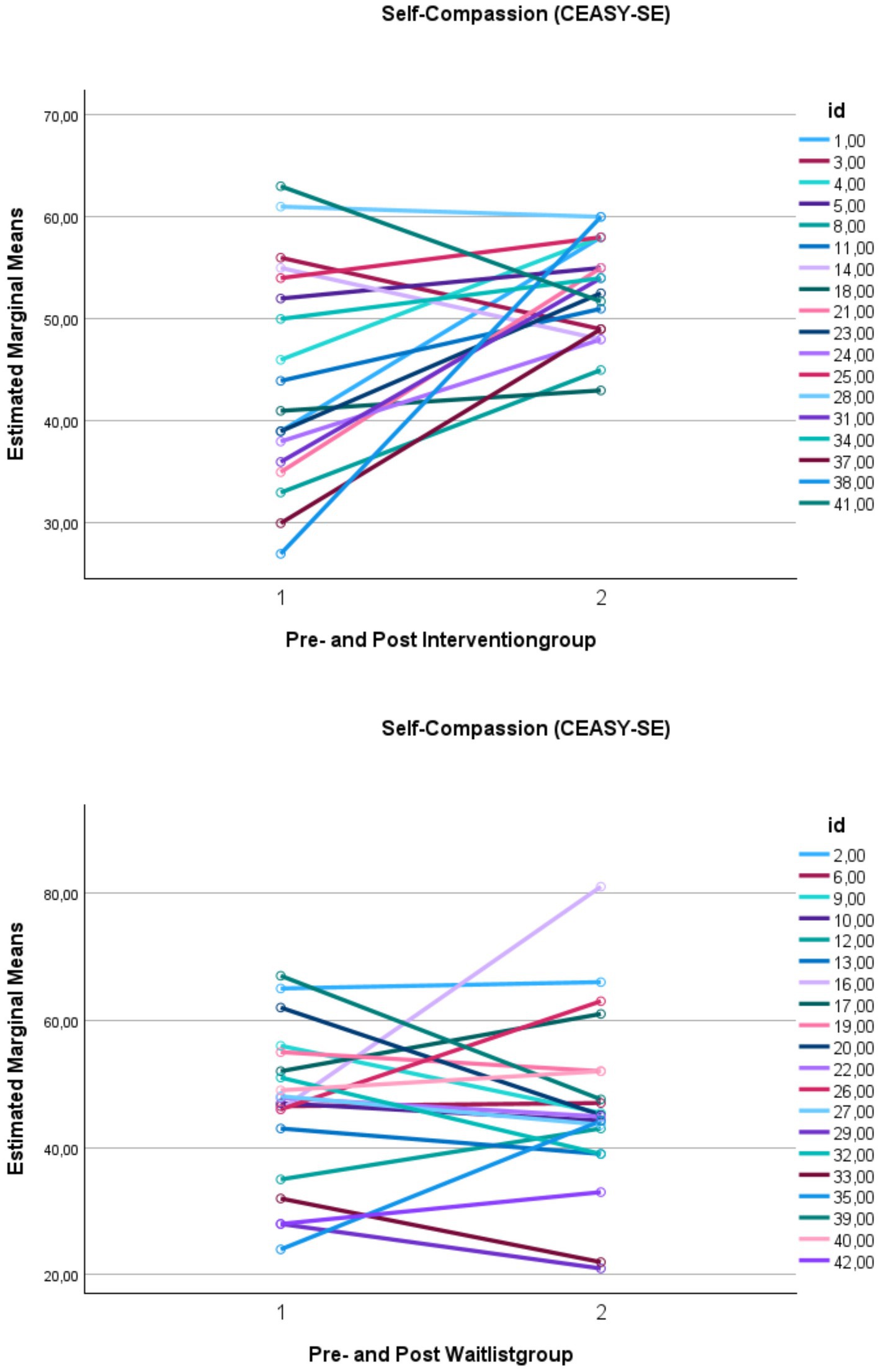
Figure 5. Changes in self-compassion for participants who attended more than two sessions and waitlist group. This figure demonstrates the means of self-compassion (CEAS-Y-SE Self-compassion) over time. CEAS-Y-SE, Compassionate Engagement and Action Scales for Youth – Swedish version. Y-axis: means. X-axis: Time 1 = scores before intervention, and Time 2 = scores after intervention.
4 Discussion
This study aimed to evaluate the feasibility, acceptability, and preliminary efficacy of a new internet-based, videoconferencing group CFT intervention for young people reporting symptoms of stress, depression, and anxiety. The literature in this area remains limited, and to our knowledge, this is the first RCT conducted with a young population. Therefore, this study is an important contribution to research.
4.1 Feasibility and acceptability
Feasibility and acceptability were assessed using a pilot RCT design. The study indicated feasibility and acceptability through low dropout rates, moderate retention and adherence, participant satisfaction, compliance, and positive clinician feedback. Regarding attrition and attendance in the intervention group, 77 % (n = 17) completed four or more modules, and 18 % (n = 4) completed all seven modules. This indicates moderate participant retention and adherence, which is consistent with findings from other studies (Berg et al., 2022; Grudin et al., 2022). In psychological interventions, dropout rates are often high (Biswal et al., 2024), although it is difficult to estimate the dropout rate specifically in young people receiving therapy for depression due to the inconsistency in how dropout has been reported (O'Keeffe et al., 2019). Dropout rates are suggested to be particularly high when defined by the number of attended sessions, as in the current study, compared to definitions based on the therapist’s assessment (de Haan et al., 2013). We believe that attendance might have been higher if some groups had not been scheduled close to vacations and important school-related events (e.g., student parties). Dropout in psychotherapy is generally challenging among young people due to practical barriers, dissatisfaction, and perceived lack of benefits (O'Keeffe et al., 2019; Ogrodniczuk et al., 2005). This study’s relatively low dropout rate (22%) in the intervention group could be attributed to several factors. The therapist-led and internet-based design minimizes accessibility barriers to evidence-based treatment, such as distance and time conflicts with school and work. The young people in the study appeared to find it easy to attend online using only their smartphones or computers. This finding suggests that the internet-based videoconferencing design may help reduce dropout rates, aligning with other studies (Sibinga et al., 2008; Ahola Kohut et al., 2020).
Most participants felt that the intervention’s content and objectives were well explained, a factor known to reduce dropout (Ormhaug and Jensen, 2018; Timulak and Keogh, 2017; Persson et al., 2017; Watsford and Rickwood, 2014). No harm to participants was reported.
In a previous study (Bratt A. et al., 2020), the essential meaning of group-based CFT was described as “gaining the courage to see and accept oneself through meeting with peers who are experiencing similar difficulties” (p. 914). Feeling connected and not being alone is an important part of the journey to approach self-compassion, and a group format might be a helpful contribution. However, the group format for CFT is relatively new and unexplored (Erekson et al., 2024), and more research is needed. Successful therapeutic group treatment requires not only knowledge of CFT but also knowledge of group theory (Bratt A. et al., 2020; Erekson et al., 2024), which was evident in this study.
4.2 Preliminary efficacy
Another aim of this study was to assess the intervention’s preliminary effects on stress, anxiety, and depression both between the intervention and the WL groups, as well as within the intervention group. The goal of our intervention was to increase self-compassion, reduce self-criticism, and improve the regulation of unpleasant emotions to affect symptoms of stress, anxiety, and depression. In previous studies, correlations between self-compassion, self-criticism, stress, anxiety and depression are well-established (Vidal and Soldevilla, 2023; Millard et al., 2023). The primary outcomes showed no significant differences between intervention and WL groups for stress and anxiety, a finding identified in previous research (Bratt A. S. et al., 2020).
Surprisingly, depression significantly increased for the intervention group (p = 0.05) compared to earlier findings in other studies (Han and Kim, 2023; Egan et al., 2022). However, the findings must be interpreted with caution due to the small sample size. A possible explanation might be that in CFT and our intervention, we practice identifying one’s suffering and daring to be touched by it. The transdiagnostic approach and the intervention’s focus on cultivating a compassionate mind reduce shame and self-criticism (Erekson et al., 2024; Gilbert, 2014), which is crucial for well-being (Marsh et al., 2018; Han and Kim, 2023). The young participants might lack awareness of their degree of self-criticism. This process can be painful and increase grief as participants become more able to see, recognize, and admit suffering (Gilbert, 2010, 2017). The participants with increased symptoms of depression might have identified and experienced emotional pain and would potentially have benefited from additional CFT sessions (Asano et al., 2022). Other CFT group treatments for depression have typically included more sessions (usually around 12) (Asano et al., 2022), with a focus on symptoms of shame and self-critical judgment, in addition to cultivating the flow of compassion.
The secondary between-group outcome revealed increased levels of self-compassion, and the study provides preliminary support for significant positive differences between the intervention group and WL group in self-compassion. This result aligns with similar findings for adults (Asano et al., 2022) that self-compassion increased after CFT group treatment compared to WL.
The within-group results showed a moderately difference in stress, compassion from others, and self-compassion, but not for compassion for others, anxiety and depression. Increased self-compassion aligns with previous research in CFT, both individually (Egan et al., 2022; Marsh et al., 2018) and in groups (Erekson et al., 2024; Lucre and Corten, 2013; Millard et al., 2023; Asano et al., 2022).
Classifying each participant’s change as reliable may complement the preliminary effect sizes for researchers and practitioners by providing a more nuanced understanding of the meaningful change at an individual level (Blampied, 2022). The findings from the study suggest a trend in which participants’ stress levels were reduced, and self-compassion increased after completing the intervention, suggesting potential beneficial effects. These are important findings, particularly since this is a group therapy setting. Previous studies with young people show clear links between higher self-compassion and well-being (Bluth and Blanton, 2015; Bluth et al., 2018; Marshall et al., 2015).
Another noteworthy observation is the gender gap among the participants. The study included around 90 % female participants (95.5% in the intervention group and 85% in the WL group), which is higher than in other studies with predominantly female participants (Millard et al., 2023; Marquez, 2024). However, research suggests that boys of all ages are less likely to seek help for mental health issues than girls of the same age. In a recently published review, self-compassion was found to reduce stigma about mental health, which was found to be a barrier for boys (Sheikh et al., 2024). This indicates that CFT group interventions could be considered in the development of future strategies to reduce barriers to help-seeking for boys.
4.3 Limitations
This study has several limitations. It was a pilot RCT feasibility study with a small sample size and preliminary efficacy results. Most participants were female, which reflects the clinical reality but may introduce a gender-based bias. A larger sample size in a longitudinal study with greater statistical power is needed to estimate the intervention’s effects on pre-, post, and follow-up group therapy outcomes.
Feasibility and acceptability were based on self-reporting and retention rates. Acceptability is a multifaceted construct, and a limitation may arise from the operational definitions used in this study. In-depth interviews with the participants could have enhanced the results, providing a stronger basis for understanding prospective and retrospective acceptability.
A limitation of this study is that homework completion was not systematically recorded after each session, even though participants rated the extent to which they completed the homework assignments after the entire treatment. If actual completion had been systematically recorded, it might have provided additional insights into intervention adherence and engagement.
A further limitation was the study design. The design included the primary outcomes of stress, depression, and anxiety symptoms, which was a broad approach with challenges. The study would possibly have benefitted from having self-compassion as the primary outcome, along with stress. Nonetheless, earlier research suggests that CFT improves various clinical symptoms (Millard et al., 2023).
Finally, while participants were randomly allocated to each group, the intervention group presented more severe symptoms of stress, anxiety, and depression and lower levels of self-compassion, which could have created an imbalance. Additionally, fewer participants in the WL group completed post-intervention measures than in the intervention group. However, recommended randomization techniques for small samples (e.g., block randomization, blinded outcome assessment) were used to ensure balance between groups, suggesting that bias should be minimal (Kahan et al., 2014; Netz et al., 2019). Randomization provides each participant an equal chance of assignment, thus helping to make the groups comparable.
4.4 Future research
The research team plans to publish a qualitative study exploring focus group findings, which will examine participants’ feedback about the acceptability and effects of the CFT group intervention. Following necessary adaptions, a larger full-scale, mixed-method, longitudinal RCT study could be explored using a comprehensive CFT program.
4.5 Conclusion
The findings from this study indicate that the internet-based videoconferencing group CFT intervention is feasible and acceptable for reducing stress and increasing levels of compassion in young people aged 15–20 in Sweden. The preliminary between-group results show that the intervention increased self-compassion and depression. Further research using the CFT intervention over a longer period would help us explore if this would reduce symptoms of depression. The current study suggests that a 7-week module was insufficient time to instigate change. The preliminary within-group results indicate a significant moderate decrease in stress, along with a moderate increase in compassion from others and self-compassion. However, the CFT intervention is promising for preventing stress and increasing self-compassion for young people.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The study was approved by the Swedish Ethical Review Authority and conducted in accordance with local legislation and institutional requirements. Written informed consent was required from the participants, but not from their legal guardians, according to the decision of the Swedish Ethical Review Authority.
Author contributions
MV: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. LW: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. MN: Writing – review & editing. IB: Writing – review & editing. CS: Writing – review & editing. EB: Writing – review & editing. JJ: Writing – review & editing. ID: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was supported by clinical research funding (ALF) from the Västerbotten County Council and Medical Faculty Umeå University, Oskarsfund Umeå University, Child and Adolescent Psychiatric Clinic Region Norrbotten, Child and Adolescent Psychiatric Clinic Region Västerbotten and Industrial Doctoral School, Umeå University. Contributions from the National Association for Social and Mental Health and the Kempe-Carlgrenska Foundation have also been received. The founders of the foundations had no role in this study.
Acknowledgments
The authors would like to thank all the young people who participated in this project.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Ahola Kohut, S., Stinson, J., Jelen, A., and Ruskin, D. (2020). Feasibility and acceptability of a mindfulness-based group intervention for adolescents with inflammatory bowel disease. J. Clin. Psychol. Med. Settings 27, 68–78. doi: 10.1007/s10880-019-09622-6
American Psychiatric Association (2013). Diagnostic and statistical manual of mental disorders. 5th Edn. Arlington, VA: American Psychiatric Association.
Arnett, J. J. (1999). Adolescent storm and stress, reconsidered. Am. Psychol. 54, 317–326. doi: 10.1037/0003-066X.54.5.317
Asano, K., Tsuchiya, M., Okamoto, Y., Ohtani, T., Sensui, T., Masuyama, A., et al. (2022). Benefits of group compassion-focused therapy for treatment-resistant depression: A pilot randomized controlled trial. Front. Psychol. 13:903842. doi: 10.3389/fpsyg.2022.903842
Beaumont, E., Bell, T., Mcandrew, S., and Fairhurst, H. (2021). The impact of compassionate mind training on qualified health professionals undertaking a compassion-focused therapy module. Couns. Psychother. Res. 21, 910–922. doi: 10.1002/capr.12396
Beaumont, E., Dagnall, N., Massey, S., and Irons, C. (2024). Evaluating the impact the self-compassion app has on levels of compassion, psychological distress and well-being. Couns. Psychother. Res. 1–11. doi: 10.1002/capr.12841
Beaumont, E., Durkin, M., Mcandrew, S., and Martin, C. R. (2016). Using compassion focused therapy as an adjunct to trauma-focused CBT for fire service personnel suffering with trauma-related symptoms. Cognit. Behav. Therapist. 9:e34. doi: 10.1017/S1754470X16000209
Beaumont, E., and Welford, M. (2020). The kindness workbook: compassionate and creative ways to boost your wellbeing. London, UK: Little, Brown Book Group Limited.
Berg, M., Lindegaard, T., Flygare, A., Sjöbrink, J., Hagvall, L., Palmebäck, S., et al. (2022). Internet-based CBT for adolescents with low self-esteem: a pilot randomized controlled trial. Cogn. Behav. Ther. 51, 388–407. doi: 10.1080/16506073.2022.2060856
Biswal, B., Gandhi, Y., Singla, D. R., Velleman, R., Zhou, B., Fernandes, L., et al. (2024). Interventions for improving adherence to psychological treatments for common mental disorders: A systematic review. Global Mental Health 11:e83. doi: 10.1017/gmh.2024.94
Blampied, N. M. (2022). Reliable change and the reliable change index: still useful after all these years? Cognit. Behav. Therapist 15:e50. doi: 10.1017/S1754470X22000484
Blampied, N. M. (2016). Reliable change and the reliable change index in the context of evidence-based practice: a tutorial review. Wellington, New Zealand: New Zealand Psychological Society Annual Conference.
Bluth, K., and Blanton, P. W. (2015). The influence of self-compassion on emotional well-being among early and older adolescent males and females. J. Posit. Psychol. 10, 219–230. doi: 10.1080/17439760.2014.936967
Bluth, K., Campo, R. A., Futch, W. S., and Gaylord, S. A. (2017). Age and gender differences in the associations of self-compassion and emotional well-being in a large adolescent sample. J. Youth Adolesc. 46, 840–853. doi: 10.1007/s10964-016-0567-2
Bluth, K., Gaylord, S., Campo, R., Mullarkey, M., and Hobbs, L. (2016). Making friends with yourself: A mixed methods pilot study of a mindful self-compassion program for adolescents. Mindfulness 7, 479–492. doi: 10.1007/s12671-015-0476-6
Bluth, K., Mullarkey, M., and Lathren, C. (2018). Self-compassion: A potential path to adolescent resilience and positive exploration. J. Child Fam. Stud. 27, 3037–3047. doi: 10.1007/s10826-018-1125-1
Boggiss, A. L., Consedine, N. S., Schache, K. R., Jefferies, C., Bluth, K., Hofman, P. L., et al. (2020). A brief self-compassion intervention for adolescents with type 1 diabetes and disordered eating: a feasibility study. Diabet. Med. 37, 1854–1860. doi: 10.1111/dme.14352
Bor, W., Dean, A. J., Najman, J., and Hayatbakhsh, R. (2014). Are child and adolescent mental health problems increasing in the 21st century? A systematic review. Aust. N. Z. J. Psychiatry 48, 606–616. doi: 10.1177/0004867414533834
Bratt, A., Gralberg, I.-M., Svensson, I., and Rusner, M. (2020). Gaining the courage to see and accept oneself: group-based compassion-focussed therapy as experienced by adolescent girls. Clin. Child Psychol. Psychiatry 25, 909–921. doi: 10.1177/1359104520931583
Bratt, A. S., Rusner, M., and Svensson, I. (2020). An exploration of group-based compassion-focused therapy for adolescents and their parents. Scand. J. Child and Adolesc. Psychiatr. Psychol. 8, 38–47. doi: 10.21307/sjcapp-2020-005
Bridge, L., Langford, K., Mcmullen, K., Rai, L., Smith, P., and Rimes, K. A. (2023). Acceptability, feasibility and preliminary efficacy of a compassion-based cognitive behavioural intervention for low self-esteem in sexual minority young adults. Clin. Psychol. Psychother. 31:2911. doi: 10.1002/cpp.2911
Briere, J. (1996). Trauma symptom checklist for children. Odessa, FL: Psychological Assessment Resources, 00253–00258.
Butcher, N. J., Monsour, A., Mew, E. J., Chan, A.-W., Moher, D., Mayo-Wilson, E., et al. (2022). Guidelines for reporting outcomes in trial reports: the CONSORT-outcomes 2022 extension. JAMA 328, 2252–2264. doi: 10.1001/jama.2022.21022
Clayborne, Z. M., Varin, M., and Colman, I. (2019). Systematic review and meta-analysis: adolescent depression and long-term psychosocial outcomes. J. Am. Acad. Child Adolesc. Psychiatry 58, 72–79. doi: 10.1016/j.jaac.2018.07.896
Cohen, J. (1988). Statistical power analysis for the behavioral sciences. 2nd Edn. New Jersey: Lawrence Erlbaum.
Cohen, S. (1988). Perceived stress in a probability sample of the United States. The social psychology of health. Thousand Oaks, CA, US: Sage Publications, Inc.
Craig, C., Hiskey, S., and Spector, A. (2020). Compassion focused therapy: a systematic review of its effectiveness and acceptability in clinical populations. Expert. Rev. Neurother. 20, 385–400. doi: 10.1080/14737175.2020.1746184
De Haan, A. M., Boon, A. E., De Jong, J. T. V. M., Hoeve, M., and Vermeiren, R. R. J. M. (2013). A meta-analytic review on treatment dropout in child and adolescent outpatient mental health care. Clin. Psychol. Rev. 33, 698–711. doi: 10.1016/j.cpr.2013.04.005
Dennhag, I. (2018). Compassionfokuserad behandling för ungdomar med stress (CUST). Available at: https://www.umu.se/forskning/projekt/compassionfokuserad-behandling-for-ungdomar-med-stress-cust/ (Accessed September 18, 2024).
Dennhag, I. (2021). Att lära om self-compassion [eng. To learn about self-compassion] [unpublished workbook]. Sweden: Clinical Science: Umeå Universitet.
Ebert, D. D., Zarski, A. C., Christensen, H., Stikkelbroek, Y., Cuijpers, P., Berking, M., et al. (2015). Internet and computer-based cognitive behavioral therapy for anxiety and depression in youth: a meta-analysis of randomized controlled outcome trials. PLoS One 10:e0119895. doi: 10.1371/journal.pone.0119895
Eckshtain, D., Kuppens, S., Ugueto, A., Ng, M. Y., Vaughn-Coaxum, R., Corteselli, K., et al. (2020). Meta-analysis: 13-year follow-up of psychotherapy effects on youth depression. J. Am. Acad. Child Adolesc. Psychiatry 59, 45–63. doi: 10.1016/j.jaac.2019.04.002
Egan, S. J., Rees, C. S., Delalande, J., Greene, D., Fitzallen, G., Brown, S., et al. (2022). A review of self-compassion as an active ingredient in the prevention and treatment of anxiety and depression in Young people. Admin. Pol. Ment. Health 49, 385–403. doi: 10.1007/s10488-021-01170-2
Ehrenreich-May, J., Rosenfield, D., Queen, A. H., Kennedy, S. M., Remmes, C. S., and Barlow, D. H. (2017). An initial waitlist-controlled trial of the unified protocol for the treatment of emotional disorders in adolescents. J. Anxiety Disord. 46, 46–55. doi: 10.1016/j.janxdis.2016.10.006
Eldridge, S. M., Chan, C. L., Campbell, M. J., Bond, C. M., Hopewell, S., Thabane, L., et al. (2016). CONSORT 2010 statement: extension to randomised pilot and feasibility trials. BMJ 355:i5239. doi: 10.1136/bmj.i5239
Erekson, D. M., Griner, D., and Beecher, M. E. (2024). Compassion focused therapy for groups: Transdiagnostic treatment for turbulent times. Int. J. Group Psychother. 74, 149–176. doi: 10.1080/00207284.2024.2314278
Ferrari, M., Hunt, C., Harrysunker, A., Abbott, M. J., Beath, A. P., and Einstein, D. A. (2019). Self-compassion interventions and psychosocial outcomes: a Meta-analysis of RCTs. Mindfulness 10, 1455–1473. doi: 10.1007/s12671-019-01134-6
Garber, J., and Weersing, V. R. (2010). Comorbidity of anxiety and depression in youth: implications for treatment and prevention. Clin Psychol 17, 293–306. doi: 10.1111/j.1468-2850.2010.01221.x
Gilbert, P. (2014). The origins and nature of compassion focused therapy. Br. J. Clin. Psychol. 53, 6–41. doi: 10.1111/bjc.12043
Gilbert, P. (2020). Compassion: from its evolution to a psychotherapy. Front. Psychol. 11:6161. doi: 10.3389/fpsyg.2020.586161
Gilbert, P.. (2017). “Compassion: Definitions and controversies,” in Compassion: Concepts, research and applications. Routledge/Taylor & Francis Group. 3–15.
Gilbert, P., and Procter, S. (2006). Compassionate mind training for people with high shame and self-criticism: overview and pilot study of a group therapy approach. Clin. Psychol. Psychother. 13, 353–379. doi: 10.1002/cpp.507
Grudin, R., Ahlen, J., Mataix-Cols, D., Lenhard, F., Henje, E., Månsson, C., et al. (2022). Therapist-guided and self-guided internet-delivered behavioural activation for adolescents with depression: a randomised feasibility trial. BMJ Open 12:e066357. doi: 10.1136/bmjopen-2022-066357
Gupta, S. K. (2011). Intention-to-treat concept: A review. Perspect. Clin. Res. 2, 109–112. doi: 10.4103/2229-3485.83221
Han, A., and Kim, T. H. (2023). Effects of self-compassion interventions on reducing depressive symptoms, anxiety, and stress: a meta-analysis. Mindfulness 14, 1553–1581. doi: 10.1007/s12671-023-02148-x
Harris, P. A., Taylor, R., Minor, B. L., Elliott, V., Fernandez, M., O'neal, L., et al. (2019). The REDCap consortium: building an international community of software platform partners. J. Biomed. Inform. 95:103208. doi: 10.1016/j.jbi.2019.103208
Harris, P. A., Taylor, R., Thielke, R., Payne, J., Gonzalez, N., and Conde, J. G. (2009). Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 42, 377–381. doi: 10.1016/j.jbi.2008.08.010
Henje, E., Rindestig, F. C., Gilbert, P., and Dennhag, I. (2020). Psychometric validity of the compassionate engagement and action scale for adolescents: a Swedish version. Scand J Child Adolesc Psychiatr Psychol 8, 70–80. doi: 10.21307/sjcapp-2020-007
Jacobson, N. S., and Truax, P. (1991). Clinical significance: a statistical approach to defining meaningful change in psychotherapy research. J. Consult. Clin. Psychol. 59, 12–19. doi: 10.1037/0022-006X.59.1.12
James, A. C., Reardon, T., Soler, A., James, G., and Creswell, C. (2020). Cognitive behavioural therapy for anxiety disorders in children and adolescents. Cochrane Database Syst. Rev. 11:Cd013162. doi: 10.1002/14651858.CD013162.pub2
Jonsson, E., and Dennhag, I. (2023). Compassion in three perspectives: associations with depression and suicidal ideation in a clinical adolescent sample. Scand J Child Adolesc Psychiatr Psychol 11, 120–127. doi: 10.2478/sjcapp-2023-0012
Kahan, B. C., Cro, S., Doré, C. J., Bratton, D. J., Rehal, S., Maskell, N. A., et al. (2014). Reducing bias in open-label trials where blinded outcome assessment is not feasible: strategies from two randomised trials. Trials 15:456. doi: 10.1186/1745-6215-15-456
Kalin, N. H. (2020). The critical relationship between anxiety and depression. Am. J. Psychiatry 177, 365–367. doi: 10.1176/appi.ajp.2020.20030305
Karing, C. (2023). The efficacy of online mindfulness-based interventions in a university student sample: videoconference- or podcast-delivered intervention. Appl. Psychol. Health Well Being 15, 740–756. doi: 10.1111/aphw.12408
Karr, J., Roberson, C., and Tiura, M. (2020). Kind warriors: a qualitative study of a compassion-based intervention for children. Couns. Psychother. Res. 20, 39–45. doi: 10.1002/capr.12266
Kirby, J. N. (2017). Compassion interventions: the programmes, the evidence, and implications for research and practice. Psychol. Psychother. Theory Res. Pract. 90, 432–455. doi: 10.1111/papt.12104
Lathren, C., Bluth, K., and Park, J. (2019). Adolescent self-compassion moderates the relationship between perceived stress and internalizing symptoms. Pers Individ Dif 143, 36–41. doi: 10.1016/j.paid.2019.02.008
Lau-Zhu, A., and Vella, L. (2023). A compassion-focused therapy group for young people who live in foster, adoptive or kinship care: initial development, reflections, and ways forward. Adopt. Foster. 47, 400–414. doi: 10.1177/03085759231207397
Lee, E.-H. (2012). Review of the psychometric evidence of the perceived stress scale. Asian Nurs. Res. 6, 121–127. doi: 10.1016/j.anr.2012.08.004
Lin, T., Stone, S. J., Heckman, T. G., and Anderson, T. (2021). Zoom-in to zone-out: therapists report less therapeutic skill in telepsychology versus face-to-face therapy during the COVID-19 pandemic. Psychotherapy 58, 449–459. doi: 10.1037/pst0000398
Lucre, K. M., and Corten, N. (2013). An exploration of group compassion-focused therapy for personality disorder. Psychol. Psychother. 86, 387–400. doi: 10.1111/j.2044-8341.2012.02068.x
Marquez, J. (2024). Gender differences in school effects on adolescent life satisfaction: exploring cross-national variation. Child Youth Care Forum 53, 389–409. doi: 10.1007/s10566-023-09756-7
Marsh, I. C., Chan, S. W. Y., and Macbeth, A. (2018). Self-compassion and psychological distress in adolescents-a Meta-analysis. Mindfulness 9, 1011–1027. doi: 10.1007/s12671-017-0850-7
Marshall, S. L., Parker, P. D., Ciarrochi, J., Sahdra, B., Jackson, C. J., and Heaven, P. C. L. (2015). Self-compassion protects against the negative effects of low self-esteem: a longitudinal study in a large adolescent sample. Personal. Individ. Differ. 74, 116–121. doi: 10.1016/j.paid.2014.09.013
Mcelroy, E., Fearon, P., Belsky, J., Fonagy, P., and Patalay, P. (2018). Networks of depression and anxiety symptoms across development. J. Am. Acad. Child Adolesc. Psychiatry 57, 964–973. doi: 10.1016/j.jaac.2018.05.027
Merikangas, K. R., He, J. P., Burstein, M., Swanson, S. A., Avenevoli, S., Cui, L., et al. (2010). Lifetime prevalence of mental disorders in U.S. adolescents: results from the National Comorbidity Survey Replication–Adolescent Supplement (NCS-A). J. Am. Acad. Child Adolesc. Psychiatry 49, 980–989. doi: 10.1016/j.jaac.2010.05.017
Merikangas, K. R., He, J. P., Burstein, M., Swendsen, J., Avenevoli, S., Case, B., et al. (2011). Service utilization for lifetime mental disorders in U.S. adolescents: results of the National Comorbidity Survey-Adolescent Supplement (NCS-A). J. Am. Acad. Child Adolesc. Psychiatry 50, 32–45. doi: 10.1016/j.jaac.2010.10.006
Millard, L. A., Wan, M. W., Smith, D. M., and Wittkowski, A. (2023). The effectiveness of compassion focused therapy with clinical populations: A systematic review and meta-analysis. J. Affect. Disord. 326, 168–192. doi: 10.1016/j.jad.2023.01.010
Neff, K. D. (2023). Self-compassion: theory, method, research, and intervention. Annu. Rev. Psychol. 74, 193–218. doi: 10.1146/annurev-psych-032420-031047
Neff, K. D., and Mcgehee, P. (2010). Self-compassion and psychological resilience among adolescents and young adults. Self Identity 9, 225–240. doi: 10.1080/15298860902979307
Netz, Y., Lidor, R., and Ziv, G. (2019). Small samples and increased variability – discussing the need for restricted types of randomization in exercise interventions in old age. Eur. Rev. Aging Phys. Act. 16:17. doi: 10.1186/s11556-019-0224-3
Nilsson, D., Wadsby, M., and Svedin, C. G. (2008). The psychometric properties of the trauma symptom checklist for children (TSCC) in a sample of Swedish children. Child Abuse Negl. 32, 627–636. doi: 10.1016/j.chiabu.2007.09.009
Nordin, M., and Nordin, S. (2013). Psychometric evaluation and normative data of the Swedish version of the 10-item perceived stress scale. Scand. J. Psychol. 54, 502–507. doi: 10.1111/sjop.12071
Ogrodniczuk, J. S., Joyce, A. S., and Piper, W. E. (2005). Strategies for reducing patient-initiated premature termination of psychotherapy. Harv. Rev. Psychiatry 13, 57–70. doi: 10.1080/10673220590956429
O'keeffe, S., Martin, P., Target, M., and Midgley, N. (2019). 'I just stopped Going': A mixed methods investigation into types of therapy dropout in adolescents with depression. Front. Psychol. 10:75. doi: 10.3389/fpsyg.2019.00075
Ormhaug, S. M., and Jensen, T. K. (2018). Investigating treatment characteristics and first-session relationship variables as predictors of dropout in the treatment of traumatized youth. Psychother. Res. 28, 235–249. doi: 10.1080/10503307.2016.1189617
Perkins, A. M., Meiser-Stedman, R., Spaul, S. W., Bowers, G., Perkins, A. G., and Pass, L. (2023). The effectiveness of third wave cognitive behavioural therapies for children and adolescents: A systematic review and meta-analysis. Br. J. Clin. Psychol. 62, 209–227. doi: 10.1111/bjc.12404
Persson, S., Hagquist, C., and Michelson, D. (2017). Young voices in mental health care: exploring children's and adolescents' service experiences and preferences. Clin. Child Psychol. Psychiatry 22, 140–151. doi: 10.1177/1359104516656722
Petrocchi, N., Ottaviani, C., Cheli, S., Matos, M., Baldi, B., Basran, J. K., et al. (2023). The impact of compassion-focused therapy on positive and negative mental health outcomes: results of a series of meta-analyses. Clin. Psychol. 31, 230–247. doi: 10.1037/cps0000193
Piers, R., Williams, J. M., and Sharpe, H. (2023). Review: can digital mental health interventions bridge the 'digital divide' for socioeconomically and digitally marginalised youth? A systematic review. Child Adolesc Ment Health 28, 90–104. doi: 10.1111/camh.12620
Porter, C. M., Galloghly, E., and Burbach, F. R. (2022). The effective delivery of digital CBT: a service evaluation exploring the outcomes of young people who completed video conferencing therapy in 2020. Cognit. Behav. Therapist 15:e27. doi: 10.1017/S1754470X22000216
SCB (Statistics Sweden). (1982). Socio-ekonomisk indelning (SEI). MiS 1982:4. (Swedish Socioeconomic Classification). Stockholm: Statistics Sweden.
Seekis, V., Farrell, L., and Zimmer-Gembeck, M. (2023). A classroom-based pilot of a self-compassion intervention to increase wellbeing in early adolescents. Explore 19, 267–270. doi: 10.1016/j.explore.2022.06.003
Sheikh, A., Payne-Cook, C., Lisk, S., Carter, B., and Brown, J. S. L. (2024). Why do young men not seek help for affective mental health issues? A systematic review of perceived barriers and facilitators among adolescent boys and young men. Eur. Child Adolesc. Psychiatry 34, 565–583. doi: 10.1007/s00787-024-02520-9
Shorey, S., Ng, E. D., and Wong, C. H. J. (2022). Global prevalence of depression and elevated depressive symptoms among adolescents: A systematic review and meta-analysis. Br. J. Clin. Psychol. 61, 287–305. doi: 10.1111/bjc.12333
Sibinga, E. M., Stewart, M., Magyari, T., Welsh, C. K., Hutton, N., and Ellen, J. M. (2008). Mindfulness-based stress reduction for HIV-infected youth: a pilot study. Explore 4, 36–37. doi: 10.1016/j.explore.2007.10.002
Sjölander, J. (2022). Ungdomars erfarenhet av en compassion-baseradgruppintervention online – en kvalitativ studie. Independent thesis Advanced level (professional degree) Student thesis.
Stewart, R. W., Orengo-Aguayo, R. E., Gilmore, A. K., and De Arellano, M. (2017). Addressing barriers to care among Hispanic youth: telehealth delivery of trauma-focused cognitive behavioral therapy. Behav Ther 40, 112–118
Stewart, R., Orengo-Aguayo, R., Young, J., Wallace, M., Cohen, J., Mannarino, A., et al. (2020). Feasibility and effectiveness of a telehealth service delivery model for treating childhood posttraumatic stress: A community-based, open pilot trial of trauma-focused cognitive–behavioral therapy. J. Psychother. Integr. 30, 274–289. doi: 10.1037/int0000225
Strauss, C., Lever Taylor, B., Gu, J., Kuyken, W., Baer, R., Jones, F., et al. (2016). What is compassion and how can we measure it? A review of definitions and measures. Clin. Psychol. Rev. 47, 15–27. doi: 10.1016/j.cpr.2016.05.004
Svanborg, P., and Åsberg, M. (1994). A new self-rating scale for depression and anxiety states based on the comprehensive psychopathological rating scale. Acta Psychiatr. Scand. 89, 21–28. doi: 10.1111/j.1600-0447.1994.tb01480.x
Teresi, J. A., Yu, X., Stewart, A. L., and Hays, R. D. (2022). Guidelines for designing and evaluating feasibility pilot studies. Med. Care 60, 95–103. doi: 10.1097/MLR.0000000000001664
Thapar, A., Collishaw, S., Pine, D. S., and Thapar, A. K. (2012). Depression in adolescence. Lancet 379, 1056–1067. doi: 10.1016/S0140-6736(11)60871-4
Thapar, A., Eyre, O., Patel, V., and Brent, D. (2022). Depression in young people. Lancet 400, 617–631. doi: 10.1016/S0140-6736(22)01012-1
The Public Health Agency of Sweden (2018). Varför har den psykiska ohälsan ökat bland barn och unga i Sverige? Utvecklingen under perioden 1985–2014. Available at: https://www.folkhalsomyndigheten.se/contentassets/628f1bfc932b474f9503cc6f8e29fd45/varfor-psykiska-ohalsan-okat-barn-unga-18023-2-webb-rapport.pdf
The Swedish National Board of Health and Welfare (2019). Nationella riktlinjer – Utvärdering 2019. Vård vid depression och ångestsyndrom. Huvudrapport med förbättringsområden. Available online at: https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/nationella-riktlinjer/2019-5-12.pdf (Accessed September 18, 2024).
The Swedish National Board of Health and Welfare (2024). Förekomst av psykisk ohälsa bland barn och unga vuxna: Aspekter av socioekonomiska utmaningar och förutsättningar. Available at: https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/ovrigt/2024-5-9083.pdf
Timulak, L., and Keogh, D. (2017). The client's perspective on (experiences of) psychotherapy: a practice friendly review. J. Clin. Psychol. 73, 1556–1567. doi: 10.1002/jclp.22532
Välimäki, M., Anttila, K., Anttila, M., and Lahti, M. (2017). Web-based interventions supporting adolescents and Young people with depressive symptoms: systematic review and Meta-analysis. JMIR Mhealth Uhealth 5:e180. doi: 10.2196/mhealth.8624
Vestin, M., Åsberg, M., Wiberg, M., Henje, E., and Dennhag, I. (2022). Psychometric validity of the Montgomery and Åsberg depression rating scale for youths (MADRS-Y). Nord. J. Psychiatry. 77, 421–431. doi: 10.1080/08039488.2022.2135761
Vestin, M., Blomqvist, I., Henje, E., and Dennhag, I. (2024). Psychometric validation of the Montgomery-åsberg depression rating scale – youth (MADRS-Y) in a clinical sample. Nord. J. Psychiatry 78, 525–532. doi: 10.1080/08039488.2024.2374417
Vicent, M., Suriá, R., Gonzálvez, C., Aparicio-Flores, M. D. P., Sanmartín, R., and García-Fernández, J. M. (2023). Emotional profiles of anxiety, depression, and stress: differences in school anxiety. Psychol. Rep. 332941231184384. doi: 10.1177/00332941231184384
Vidal, J., and Soldevilla, J. M. (2023). Effect of compassion-focused therapy on self-criticism and self-soothing: A meta-analysis. Br. J. Clin. Psychol. 62, 70–81. doi: 10.1111/bjc.12394
Vigerland, S., Lenhard, F., Bonnert, M., Lalouni, M., Hedman, E., Ahlen, J., et al. (2016). Internet-delivered cognitive behavior therapy for children and adolescents: A systematic review and meta-analysis. Clin. Psychol. Rev. 50, 1–10. doi: 10.1016/j.cpr.2016.09.005
Von Wirth, E., Meininger, L., Adam, J., Woitecki, K., Treier, A. K., and Döpfner, M. (2023). Satisfaction with videoconference-delivered CBT provided as part of a blended treatment approach for children and adolescents with mental disorders and their families during the COVID-19 pandemic: a follow-up survey among caregivers and therapists. J. Telemed. Telecare 30, 1543–1554. doi: 10.1177/1357633X231157103
Wakelin, K. E., Perman, G., and Simonds, L. M. (2022). Effectiveness of self-compassion-related interventions for reducing self-criticism: A systematic review and meta-analysis. Clin. Psychol. Psychother. 29, 1–25. doi: 10.1002/cpp.2586
Waszczuk, M. A., Zavos, H. M., Gregory, A. M., and Eley, T. C. (2014). The phenotypic and genetic structure of depression and anxiety disorder symptoms in childhood, adolescence, and young adulthood. JAMA Psychiatry 71, 905–916. doi: 10.1001/jamapsychiatry.2014.655
Watsford, C., and Rickwood, D. (2014). Young people's expectations, preferences, and experiences of therapy: effects on clinical outcome, service use, and help-seeking intentions. Clin. Psychol. 18, 43–51. doi: 10.1111/cp.12034
Williamson, J. (2020). Effects of a self-compassion break induction on self-reported stress, self-compassion, and depressed mood. Psychol. Rep. 123, 1537–1556. doi: 10.1177/0033294119877817
Zemestani, M., Ezzati, S., Nasiri, F., Gallagher, M. W., Barlow, D. H., and Kendall, P. C. (2023). A culturally adapted unified protocol for transdiagnostic treatment of anxiety disorders in adolescents (UP-A): a randomized waitlist-controlled trial. Psychol. Med., 54, 385–398. doi: 10.1017/s0033291723001903
Keywords: compassion, young people, stress, randomized controlled trial (RCT), group psychotherapy, internet-based psychotherapy
Citation: Vestin M, Wallin L, Naesström M, Blomqvist I, Svedin CG, Beaumont E, Jokinen J and Dennhag I (2025) Internet-based group compassion-focused therapy for Swedish young people with stress, anxiety and depression: a pilot waitlist randomized controlled trial. Front. Psychol. 16:1547046. doi: 10.3389/fpsyg.2025.1547046
Edited by:
Fabrizio Stasolla, Giustino Fortunato University, ItalyReviewed by:
Nanja Hansen, Aarhus University, DenmarkMolly Patapoff, University of California, San Diego, United States
Copyright © 2025 Vestin, Wallin, Naesström, Blomqvist, Svedin, Beaumont, Jokinen and Dennhag. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Magnus Vestin, bWFnbnVzLnZlc3RpbkB1bXUuc2U=; Linda Wallin, bGluZGEud2FsbGluQHVtdS5zZQ==
†These authors have contributed equally to this work and share first authorship