 Mei-Jun Zhang
Mei-Jun Zhang Si Liu
Si Liu Xiao-Yun Xiong
Xiao-Yun Xiong Meng-Die Liu2
Meng-Die Liu2
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CONCEPTUAL ANALYSIS article
Front. Psychol., 26 March 2025
Sec. Health Psychology
Volume 16 - 2025 | https://doi.org/10.3389/fpsyg.2025.1499962
Introduction: Research on kinesiophobia in coronary heart disease is increasing, but existing studies primarily adopt concepts from the chronic pain domain, neglecting the specific characteristics of coronary heart disease patients. This gap limits effective identification and management.
Objective: This study aims to clarify the concept of kinesiophobia in coronary heart disease using Rodgers’ evolutionary concept analysis.
Methodology: Rodgers’ evolutionary concept analysis method was applied to review the literature. A comprehensive search was conducted in PubMed, Web of Science, PsycINFO, CINAHL, Cochrane Library, Embase, Scopus, ProQuest, OVID, CNKI, Wanfang Data, CBM, and VIP Database (up to June 30, 2024). Inclusion criteria: Studies on coronary heart disease patients, addressing the concept’s attributes, antecedents, and consequences, published in English or Chinese. Exclusion criteria: Unavailable full text, gray literature, non-peer-reviewed texts, and study protocols.
Results: A total of 31 articles were included. The attributes of kinesiophobia in coronary heart disease patients were identified as self-symptomatic distress, complex emotional responses, subjective avoidance behavior with personality tendencies, and misperceptions with negative reactions. Antecedents included sociodemographic, disease-related, and psychological factors. Consequences encompassed reduced participation in cardiac rehabilitation, decreased functional capacity, increased major adverse cardiac events, and lower quality of life.
Conclusion: In this study, we found that kinesiophobia in patients with coronary heart disease is a subjective avoidance behavior that includes both “fear of pain or weakness” and “fear of cardiac events” based on personality tendencies, driven by complex emotional responses and misperceptions based on their own symptomatic disturbances, and presents an excessive and irrational fear of movement. This analysis highlights the need for early identification and multidisciplinary interventions tailored to this population. It also provides a foundation for developing more specific and objective assessment tools.
Coronary heart disease (CHD), caused by coronary artery atherosclerosis leading to myocardial ischemia, hypoxia, or necrosis, is the leading cause of death globally (Timmis et al., 2020). Patients often face recurrent episodes, frequent hospitalizations, and repeated interventions like coronary angiograms and revascularizations. CHD poses a serious threat to life, health, and imposes a heavy economic burden on individuals and healthcare systems worldwide (Roth et al., 2020; Timmis et al., 2020; Virani et al., 2021). Currently, 423 million people suffer from CHD, accounting for 31% of all deaths annually (Lum et al., 2020). The World Heart Association projects global cardiovascular costs to rise from $863 billion in 2010 to $1,044 billion by 2030 (Virani et al., 2021).
Cardiac rehabilitation (CR) plays a crucial role in secondary prevention for CHD, helping to stabilize, slow, or even reverse atherosclerosis progression. It reduces overall mortality by 13 to 24% and readmission rates by 31% within a year (Resurrección et al., 2019). This comprehensive program spans the acute, stabilized, and lifelong phases of CHD and includes medication, exercise, nutrition, psychosocial support, risk factor management, education, and lifestyle guidance (Knuuti et al., 2020). Exercise rehabilitation, the cornerstone of cardiac rehabilitation, improves myocardial circulation, lowers mortality and readmission rates, reduces functional impairments, and enhances quality of life (Fu et al., 2019; Dibben et al., 2021). However, global participation in exercise rehabilitation remains low at 20–50%, with even lower rates in developing countries (Bäck et al., 2016). A major barrier is kinesiophobia, which affects participation and adherence, negatively impacting patients’ quality of life (Bäck et al., 2016; Knapik et al., 2019; Baykal Sahin et al., 2021; Yang et al., 2023a; Yang et al., 2023d). Studies have shown that 25.4% of patients with CHD have kinesiophobia throughout the course of the disease (Keessen et al., 2020a). Therefore, the identification and intervention of kinesiophobia in patients with CHD is an important topic and challenge.
The term “fear of movement” originated in chronic pain research and refers to avoidance behaviors driven by fear of pain (Lethem et al., 1983). It has since been studied in post-surgery (Masuy et al., 2022), stroke (Wasiuk-Zowada et al., 2021), and heart failure patients (Sentandreu-Mañó et al., 2024). While kinesiophobia is common across patient groups, its triggers and nature vary, making generalization inappropriate. For example, chronic pain patients fear pain-related movements due to catastrophic perceptions of pain (Vlaeyen and Linton, 2012). In contrast, angina in CHD patients is often sudden, brief, and triggered by factors like cold, diet, emotions, or exercise. This pain may signal myocardial ischemia, raising serious concerns about vital organs and death (Bäck et al., 2018). Additionally, Bäck et al. (2012) patients diagnosed with CHD may experience existential fears related to exertion and adverse events due to the specificity of their symptoms. These fears may include a fear of death, concerns about stent dislodgement or displacement during exercise, and anxiety about experiencing another cardiac event. Although kinesiophobia has evolved in coronary heart disease (CHD) patients, its unique characteristics remain underexplored, and despite the focus on exercise interventions, the lack of a conceptual analysis limits the development of targeted interventions and assessment tools, making a clear understanding essential for improving rehabilitation outcomes. Conceptual analysis is essential to address this gap and guide the creation of more precise and effective strategies for managing kinesiophobia in this patient group.
Concept analysis is an effective method for clarifying ambiguous terms widely used across disciplines. Rodgers’ Evolutionary Concept Analysis emphasizes that concepts are dynamic and evolve over time (Rodgers, 1989). To refine their current usage, this approach redefines context, attributes, surrogate and related terms, antecedents, model cases, and consequences, providing a structured foundation for research and practice (Tofthagen and Fagerstrøm, 2010). Unlike traditional methods, evolutionary concept analysis traces a concept’s historical development, examines its key components, explores diverse interpretations, and analyzes its real-world applications (Rodgers et al., 2018). By emphasizing conceptual fluidity and multidimensionality, this method is particularly suitable for studying evolving, cross-disciplinary concepts, offering valuable insights into their theoretical development and practical implications.
This study aims to analyze kinesiophobia in CHD patients using Rodgers’ evolutionary approach, hypothesizing that it is a complex phenomenon influenced by cognitive distortions, emotional responses, and individual personality traits, rather than merely a psychological condition. By examining its core characteristics, this research seeks to provide a clearer theoretical framework to support early identification and the development of effective interventions for kinesiophobia in CHD patients.
Rodgers’ evolutionary conceptual analysis was employed to clarify the concept of kinesiophobia in CHD patients. This method, based on Walker and Avant’s classical approach, focuses on clarifying vague or abstract concepts by analyzing their usage within a discipline, emphasizing changes over time and across contexts (Tofthagen and Fagerstrøm, 2010). Rodgers’ method involves six steps, as outlined in Table 1.
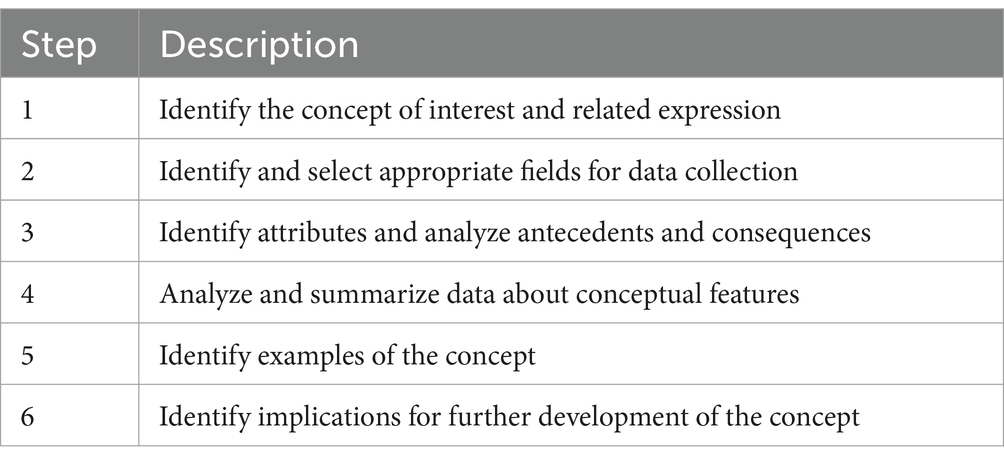
Table 1. Steps for Rodgers’ evolutionary concept analysis.
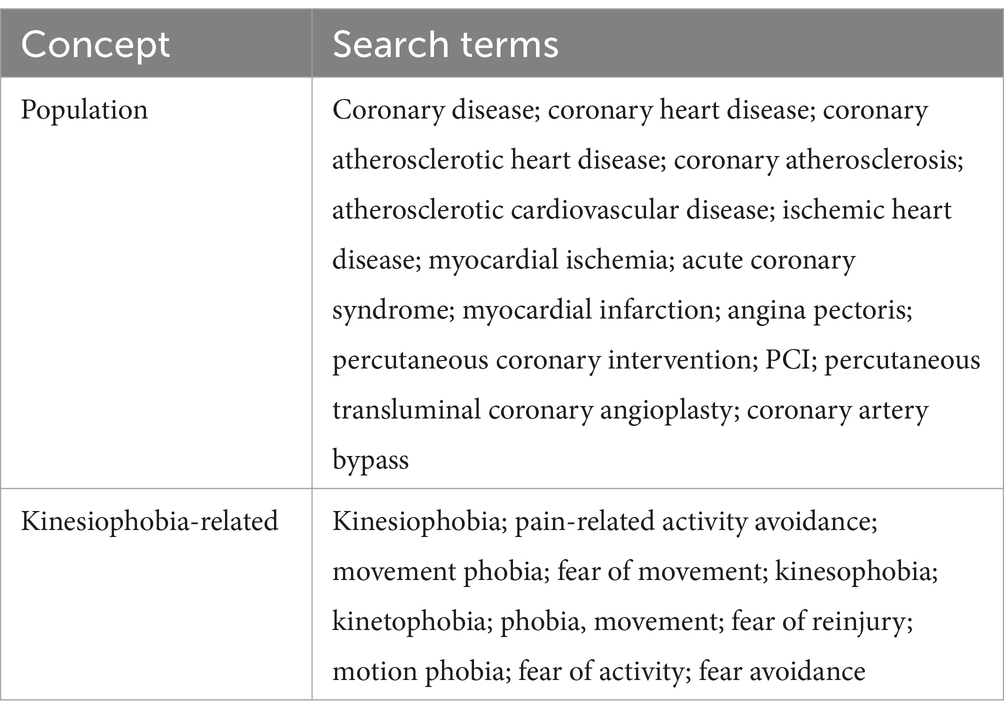
Studies on kinesiophobia in patients with CHD were searched in PubMed, Web of Science, PsycINFO, CINAHL, the Cochrane Library, Embase, Scopus, ProQuest, OVID, CNKI, Wanfang Data, CBM, and VIP Database from library build to June 30, 2024. Additional articles were manually retrieved from reference lists. The search terms used were a combination of MeSH terms and free-text words, categorized as follows:
Inclusion criteria: (1) studies on CHD patients; (2) research addressing the concept’s attributes, evolution, antecedents, and consequences; (3) published in English or Chinese. Exclusion criteria: (1) unavailable full text; (2) gray literature, non-peer-reviewed texts, letters, and study protocols. Detailed search strategies are provided in Supplementary material 1.
In this study, two researchers independently screened the literature, with a third resolving any disagreements. After reviewing the selected studies, the researchers extracted information for conceptual analysis. Initially, 1,197 studies were retrieved, and after removing duplicates, 805 remained. Following title and abstract screening, 722 were excluded, leaving 83 for full eligibility assessment. We excluded 54 studies due to unavailability of full text (n = 8), topic irrelevance (n = 21), non-English/Chinese language (n = 3), registered reports (n = 4), and incorrect focus (n = 18). Two additional articles were sourced from reference lists, resulting in 31 articles for conceptual analysis. A detailed flow chart is shown in Figure 1, with exclusion reasons in Supplementary material 2.
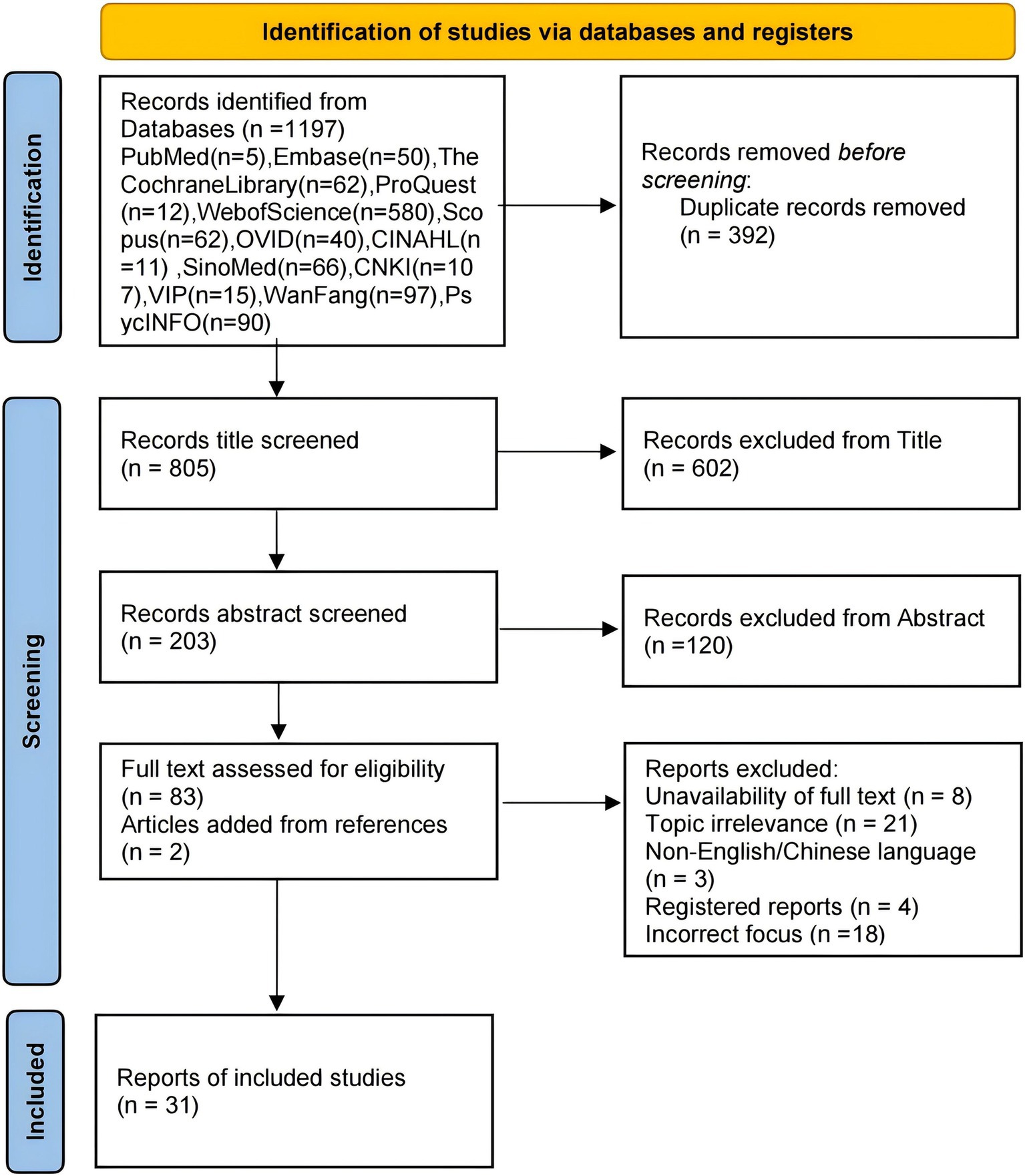
Figure 1. Flowchart of the study selection process of the concept analysis.
In this section, we present the results of the concept analysis, organized into several key components: study characteristics, the evolving definition and use of the concept, surrogate terms and related concepts, attributes, antecedents, consequences, model case, and the final definition of kinesiophobia in patients with CHD. Additionally, we discuss the measurement tool used to assess this concept.
Based on the inclusion and exclusion criteria, 31 papers were finally included for conceptual analysis, 25 in English and 6 in Chinese. Most used cross-sectional and qualitative research designs. Study details are provided in Table 2.
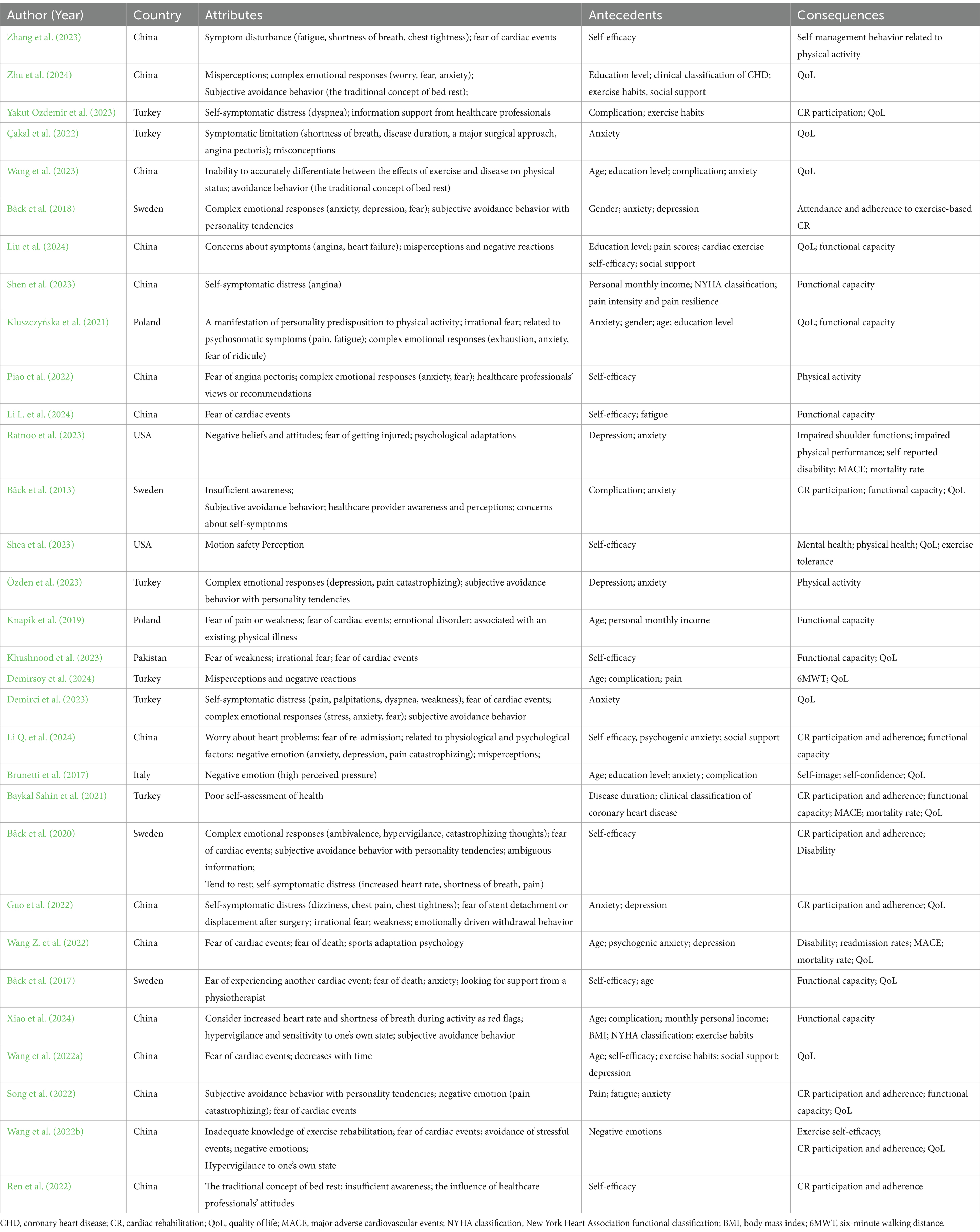
Table 2. Characteristics of the included studies.
Since “kinesiophobia” is not defined in dictionaries, we analyzed its components separately: “kinesis” and “phobia.” In the Oxford Dictionary, “kinesis” means “movement,” referring to “an act of moving the body or part of the body,” while “phobia” is defined as “a strong unreasonable fear of something.” PubMed defines “kinesiophobia” as an anxiety disorder of persistent and irrational fear of movement following an injury. It is related to perceived disability due to injury and catastrophizing in fear of (anticipated) pain and possibility of reinjury.
Lethem et al. (1983) developed the “fear-avoidance” model for pain patients, centering on the fear of pain and distinguishing between “confrontation” and “avoidance” responses. Confrontation involves viewing pain as a temporary nuisance and continuing physical and social activities, while avoidance exaggerates pain, reducing or ceasing movement and leading to severe disability. The model suggests that varying perceptions of negative stimuli can lead to different outcomes. Kori (1990) introduced “kinesiophobia” based on this model to describe fear of movement due to lower back pain, defining it as excessive and irrational fear of movement linked to pain and vulnerability to re-injury. Vlaeyen et al. (1995) expanded the model into a cognitive-behavioral framework, where misinterpretation of exercise or re-injury leads to avoidance behaviors and heightened focus on bodily sensations, worsening the physical and psychological impact of illness. In 2012, Swedish scholar Bäck et al. (2012) first used the Tampa Scale for Kinesiophobia Heart to measure kinesiophobia in CHD patients, and found that 20% of CHD patients suffered from kinesiophobia, which also was the first application of this concept in the field of cardiovascular disease. In this study, the authors followed the concepts proposed in the field of chronic pain. However, it was noted that kinesiophobia in patients with CHD has its own symptomatic peculiarities compared with patients with pain, and that the nature of the perceived threat may vary between different patient groups. Future research is needed to develop a more consistent definition of kinesiophobia in patients with CHD. However, subsequent research has continued using concepts from chronic pain without adapting them for CHD (Bäck et al., 2013; Gołba et al., 2018). Therefore, a consistent definition of kinesiophobia in patients with CHD is necessary.
Surrogate terms are specific words or phrases used to describe a concept (Rodgers, 1989). In medical literature, “fear of movement” and “kinesiophobia” are often used interchangeable (Keessen et al., 2020a; Keessen et al., 2020b; Çakal et al., 2022). Related concepts share similarities with the main concept but differ in characteristics (Rodgers, 1989). For this study, “exercise anxiety” is the relevant term (Çakal et al., 2022; Liu et al., 2024). Researchers suggest that patients who have experienced cardiac events may exhibit anxiety and fear related to physical activity, which is viewed as part of generalized anxiety disorder and associated with preventive behaviors (Vlaeyen et al., 2012; Liu et al., 2024).
Attributes are the defining characteristics of a concept that help identify its presence in a given situation. Identifying these key attributes is essential to distinguish the concept from others (Rodgers and Knafl, 1993). The following attributes of kinesiophobia in CHD patients were summarized from the analysis of the included studies.
Kinesiophobia in different patients is highly heterogeneous due to multiple influences and the complex and diverse characteristics of individuals (Bäck et al., 2013). Patients with CHD who experience a cardiac event can be profoundly disturbed by their own symptoms during exercise (Bäck et al., 2013; Shen et al., 2023; Yakut Ozdemir et al., 2023; Liu et al., 2024). The cardiac-related sensations that occur during physical activity, such as chest tightness and shortness of breath, are similar to the symptoms experienced during a heart attack, leading to a sense of impending doom (Bäck et al., 2020; Çakal et al., 2022; Zhang et al., 2023). This makes it impossible for patients to accurately differentiate between the effects of exercise and illness on their physical condition (Yakut Ozdemir et al., 2023; Zhang et al., 2023). As a result, patients may become increasingly concerned about the potential consequences of physical activity, fearing that exercise could exacerbate their existing cardiac or physical condition, leading to complications, rehospitalization, or other adverse events (Kluszczyńska et al., 2021; Liu et al., 2024). This anxiety manifests as a fear of uncertainty regarding their future physical activity (Guo et al., 2022). This is also confirmed by the study of Çakal et al. (2022). Furthermore, it is worth noting that patients with CHD can exhibit a double fear of movement due to the specificity of their symptoms. The first layer involves a fear of pain or weakness, where patients worry that physical activity might exacerbate the pain in the heart region, prolong its duration, or cause pain and fatigue in other areas (Shen et al., 2023; Wang et al., 2023). The second layer is a fear of cardiac events, where patients are concerned that exercise might cause the dislodgement or displacement of stents, lead to another cardiac event, or even result in death (Bäck et al., 2013; Shea et al., 2023). Among these, the fear of experiencing another cardiac event tends to be more pronounced in patients with CHD (Bäck et al., 2017). This is consistent with the findings of Shen et al. (2023). These intertwined fears intensify the patients’ negative beliefs and attitudes toward physical activity (Xiao et al., 2024).
Kinesiophobia encompasses not only a simple fear of physical activity, but also a complex, multifactorial mindset that stems from a belief in vulnerability (Kluszczyńska et al., 2021). Kluszczyńska et al. (2021) noted that past experiences and current physical conditions may lead patients to worry about the possibility of re-injury. This process involves a complex set of emotional responses including worry, fear, anxiety, depression, frustration, catastrophizing of pain, feelings of inadequacy and embarrassment (Bäck et al., 2017; Knapik et al., 2019; Kluszczyńska et al., 2021; Özden et al., 2023). This complex experience of negative emotions prompts patients to over-amplify unpleasant sensations such as pain, chest tightness, shortness of breath and dyspnea, leading to heightened sensitivity to physical activity (Bäck et al., 2018; Knapik et al., 2019; Kluszczyńska et al., 2021; Piao et al., 2022). Consequently, they perceive physical activity as a potential trigger for cardiac events, ultimately resulting in a harmful cycle of “kinesiophobia – reduced physical activity – decreased exercise capacity – kinesiophobia” (Demirsoy et al., 2024). The study by Liu et al. (2024) also emphasized that negative emotional experiences can have a significant impact on patients’ perception of movement as well as motor behavior. A series of psychological issues can lead to negative outcomes, such as reduced adherence to CR, diminished physical activity capacity, increased readmission rates, and a decline in quality of life (Guo et al., 2022; Demirci et al., 2023; Demirsoy et al., 2024). Moreover, these effects are persistent and may even outweigh the direct physiologic harm caused by the cardiac event itself (Özden et al., 2023). Therefore, improving individual emotional responses is crucial in preventing kinesiophobia in patients with CHD.
In the field of psychology, evidence indicates that temperament and personality traits significantly influence individual behavior (Wang et al., 2022b). Bäck et al. (2018) found that for patients with kinesiophobia, they often tend to be pessimistic about future problems and their personalities are characterized by active avoidance of potential harm. With limited self-awareness, patients tend to judge the intensity and type of exercise their bodies can tolerate based on their previous exercise experience and their own symptoms (Bäck et al., 2013; Bäck et al., 2018; Demirci et al., 2023). The study by Zhu et al. (2024) also showed that personality affects patients’ self-assessment of exercise. In addition, studies have shown that most patients are heavily influenced by the traditional belief that the disease should be controlled by rest and bed confinement (Bäck et al., 2020; Wang et al., 2023). Most of them have a poor level of self-assessment and are therefore hypervigilant about exercise, thus actively avoiding behaviors that may cause injury (Knapik et al., 2019; Ren et al., 2022; Xiao et al., 2024). Thus, kinesiophobia is a manifestation of a personality predisposition toward physical activity (Kluszczyńska et al., 2021).
Exercise after a cardiac event is a long-term process that requires both internal and external support (Piao et al., 2022; Yakut Ozdemir et al., 2023). Advice or perceptions from healthcare professionals can influence patients’ perceptions of the safety of exercise (Ratnoo et al., 2023). When an individual is in a disease state or when his or her health is threatened, it can aggravate the patient’s false perception of the disease, which directly or indirectly affects the patient’s prognosis, quality of life, and even the recovery of social function (Song et al., 2022; Wang et al., 2022b). During the acute phase, healthcare professionals emphasize the importance of absolute bed rest, reinforcing patients’ concerns and fears about their health. However, even when myocardial blood flow has been restored, they are still in a state of panic and tension, fearing that activity will lead to disease recurrence or deterioration (Piao et al., 2022; Yakut Ozdemir et al., 2023). The reason for this may be that the patient lacks proper knowledge about the disease as well as about exercise. The study by Zhu et al. (2024) also emphasized that if information about physical activity and exercise is unclear, it can increase patients’ kinesiophobia. Bäck et al. (2013) noted that patients’ perceptions of illness influence their coping strategies. The higher the level of negative cognition, the greater the fear of physical activity or exercise-induced adverse cardiac events such as angina, myocardial infarction, and readmission (Bäck et al., 2013; Ren et al., 2022; Wang et al., 2023). As irrational fears increase, the severity of kinesiophobia also intensifies, leading to irrational avoidance of physical activities, which ultimately affects the patient’s quality of life and recovery process.
Antecedents are events or phenomena that precede a concept (Rodgers and Knafl, 1993). In this study, antecedents of kinesiophobia in CHD patients were categorized into three areas: sociodemographic factors, disease factors, and psychological factors.
The main sociodemographic factors influencing kinesiophobia in CHD patients include age, gender, social support, education level, exercise habits, and personal monthly income. Studies show that as age increases, patients experience a decline in physical function and activity capacity, often with comorbidities, which increases their fear of falling during exercise and leads to higher levels of kinesiophobia (Bäck et al., 2017; Wang Z. et al., 2022; Wang et al., 2023). Kluszczyńska et al. (2021) emphasized that gender also plays an important role, with women experiencing more pain and fatigue during cardiac rehabilitation exercises and demonstrating greater sensitivity, resulting in higher kinesiophobia level. Social support is a key factor, as patients with strong support systems better understand the process and benefits of exercise rehabilitation, reducing fear and improving adherence to rehabilitation programs (Bourke et al., 2022; Li Q. et al., 2024; Liu et al., 2024). Education level also influences kinesiophobia, with higher literacy associated with lower fear of movement (Brunetti et al., 2017; Kluszczyńska et al., 2021; Liu et al., 2024). In addition, Yakut Ozdemir et al. (2023) also found that patients with a regular exercise routine were more likely to maintain physical activity after a cardiac event because they recognized the benefits of moderate exercise and were actively involved in rehabilitation therapy. Low personal monthly income is an independent risk factor for kinesiophobia, as the financial burden of long-term medical costs leads patients to avoid exercise due to concerns about potential physical risks and additional expenses (Shen et al., 2023).
The main disease factors include symptom severity and complications. Patients in the acute phase or with higher cardiac function grades often experience more severe symptoms, such as chest tightness, shortness of breath, dizziness, fatigue, and a sense of impending doom (Zhu et al., 2024). These symptoms heighten their perception of safety threats, leading to increased sensitivity and resistance to physical activity. Conversely, patients in stable phases or with lower cardiac function grades exhibit milder symptoms and lower levels of kinesiophobia (Shen et al., 2023). Demirsoy et al. (2024) found that pain intensity, frequency, and duration correlate with kinesiophobia levels. Pain can amplify stress responses, increasing both pain perception and kinesiophobia (Shen et al., 2023; Liu et al., 2024). Additionally, CHD patients often have comorbidities such as obesity, anemia, hypertension, stroke, diabetes, and heart failure, which may require multiple medications and worsen their kinesiophobia (Bäck et al., 2013; Yakut Ozdemir et al., 2023).
The primary psychological factors influencing kinesiophobia in CHD patients are anxiety, depression, and self-efficacy. Anxiety, as the main driver, leads to excessive fear of adverse events and avoidance of exercise, while depression, characterized by low mood, fatigue, and negative thoughts, becomes more common after cardiac events due to incomplete recovery and increased risk of future issue (Bäck et al., 2013; Çakal et al., 2022; Wang et al., 2023). Zhang et al. (2023) noted that low exercise self-efficacy, or lack of confidence in performing physical activity, also contributed to avoidance. Positive self-efficacy is linked to good physical and emotional states, while anxiety and fear diminish it (Ren et al., 2022; Song et al., 2022; Wang et al., 2022a).
Kinesiophobia in CHD patients is associated with several negative outcomes, including reduced participation and adherence in CR, decreased functional capacity, increased incidence of major adverse cardiovascular events (MACE) and mortality, and lower quality of life (QoL). Kinesiophobia leads to reduced participation and adherence to rehabilitation, with participation rates decreasing by 1% for each day of delayed inclusion (Thomas, 2024). Patients avoid physical activity due to kinesiophobia, which worsens rehabilitation outcome (Bäck et al., 2020; Ren et al., 2022; Yakut Ozdemir et al., 2023). Studies show that higher levels of kinesiophobia correlate with lower physical activity and declining functional capacity, as patients believe exercise may trigger heart issue (Bäck et al., 2017; Khushnood et al., 2023; Ratnoo et al., 2023). This creates a vicious cycle of physical decline, potentially leading to disability (Xiao et al., 2024). Prolonged inactivity increases the risk of MACE and mortality, with early withdrawal from rehabilitation nearly doubling the risk of death or recurrent events (Pardaens et al., 2017). Kinesiophobia also significantly lowers quality of life, as kinesiophobia leads to maladaptation, physical degeneration, and severe psychological distress, further impacting patients’ survival and well-being (Song et al., 2022; Wang et al., 2022b).
Analysis of typical cases can better help clinical identification, and application of concepts (Tofthagen and Fagerstrøm, 2010). The case described below is a fictionalized account of kinesiophobia in a patient with CHD.
Mr. Wang, a 53-year-old with a history of CHD, hypertension, and heart failure, was admitted for acute myocardial infarction and underwent emergency PCI. Post-surgery, he was advised to remain on bed rest for 24 h. During this time, he frequently worried about his condition, felt ashamed, and viewed himself as weak and unsuccessful, leading to a range of negative emotions such as worry, fear, anxiety, and depression (complex emotional responses). Once stabilized, Mr. Wang was informed he could resume movement, but he resisted, fearing exercise might worsen his symptoms or dislodge his stent, necessitating further surgery (self-symptomatic distress). He also expressed a general reluctance to exercise due to past experiences and a belief that exercise would exacerbate his health issues (subjective avoidance behavior with personality tendencies). Additionally, Mr. Wang admitted to avoiding asking his healthcare provider for guidance on recovery exercises and lacked accurate knowledge about his condition and the benefits of exercise, intensifying his fear of potential negative effects (misperceptions and negative reactions).
Kinesiophobia in patients with CHD is a subjective avoidance behavior that includes both “fear of pain or weakness” and “fear of cardiac events” based on personality tendencies, driven by complex emotional responses and misperceptions based on their own symptomatic disturbances, and presents an excessive and irrational fear of movement. Figure 2 describes the relationship between antecedents, attributes, and consequences.
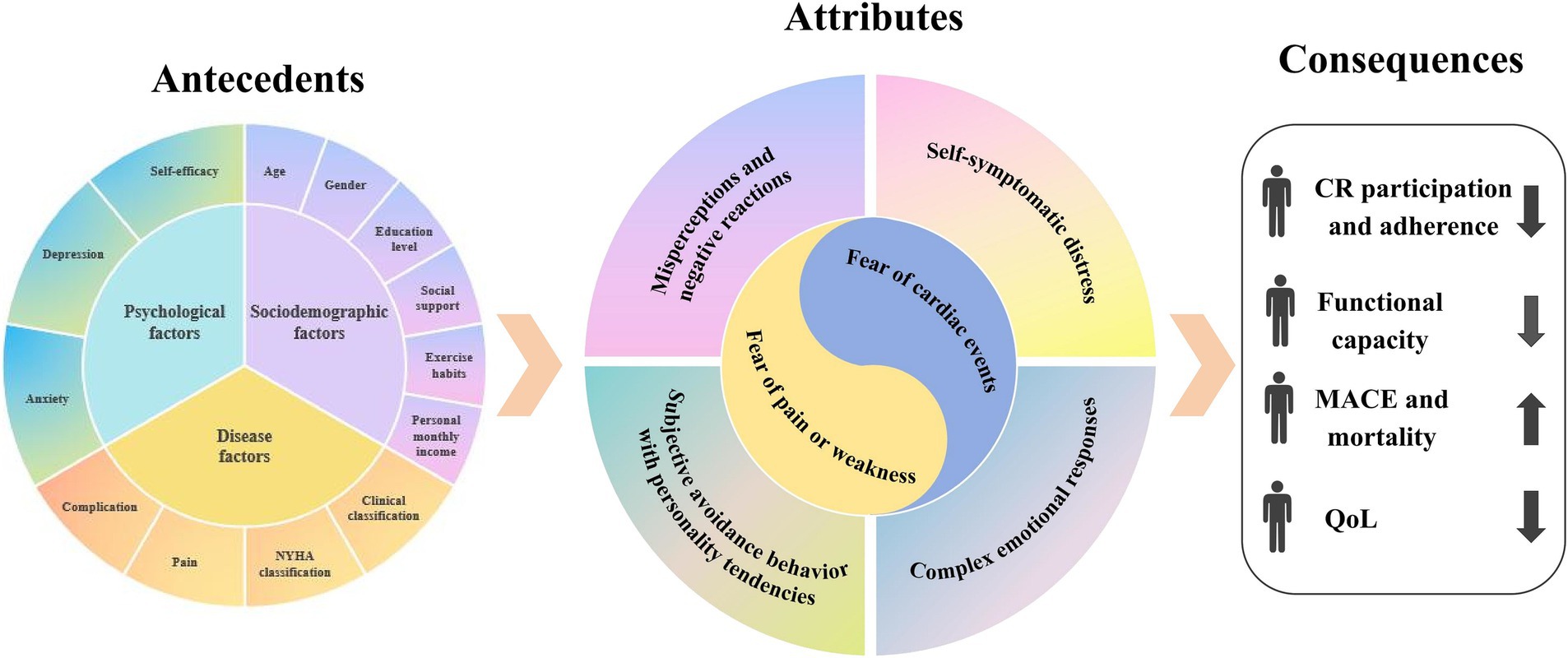
Figure 2. The antecedents, attributes, and consequences of the concept.
Measurement tools define a concept’s characteristics (Tofthagen and Fagerstrøm, 2010). Most assessments of kinesiophobia use general scales rather than specific ones (Jia et al., 2024).
The TSK, developed by Kori (1990), is a widely used questionnaire with four dimensions: repetitive strain injury, re-injury, fear avoidance, and work-related injury, totaling 17 items. A higher score indicates greater kinesiophobia, with a Cronbach’s α of 0.77. Though translated and used in several countries, the TSK, designed for low back pain, has not been tested for reliability and validity in CHD patients (Roelofs et al., 2011).
The TSK-SV Heart, adapted from the TSK by Bäck et al. (2013), includes four dimensions: danger perception, fear of movement, movement avoidance, and dysfunction, with 17 items. Scores range from 17 to 68, with higher scores indicating greater kinesiophobia. It has a Cronbach’s α of 0.78 and has been translated into multiple languages. While the TSK-SV Heart shows strong psychometric properties in Western countries and China, it is intended for a range of heart conditions, not specifically CHD (Ghisi et al., 2017).
Developed by Ozyemisci-Taskiran et al. (2020), Fact-CHD is the first tool specifically for measuring kinesiophobia in CHD patients. It assesses individuals who have had a myocardial infarction, coronary artery bypass surgery, or percutaneous coronary intervention in the past 12 months. The 21-item scale has a Cronbach’s α of 0.92, with higher scores indicating greater exercise fear. However, its adoption outside of its initial setting is limited, and further validation is needed for broader applicability.
Clear conceptual frameworks are crucial for advancing nursing knowledge (Tofthagen and Fagerstrøm, 2010). In previous research, kinesiophobia is generally defined as a psychological state where chronic pain patients fear movement due to pain (Kori, 1990). Currently, research on kinesiophobia in CHD patients has mainly addressed prevalence and influencing factors, with less focus on its underlying attributes and mechanisms (Wang et al., 2023; Yakut Ozdemir et al., 2023; Zhu et al., 2024). This article is the first to specifically describe unique characteristics of kinesiophobia in CHD patients, aiming to differentiate it from similar concepts like “exercise anxiety” and other diseases. We concluded that kinesiophobia in CHD is a subjective avoidance behavior driven by personality traits, complex emotional reactions, and misperceptions related to symptoms, resulting in excessive and irrational fear of movement. Unlike other diseases, kinesiophobia in CHD has two dimensions: “fear of pain or weakness” and “fear of cardiac events,” with the latter being more prevalent (Bäck et al., 2013; Shen et al., 2023). Adverse events, such as chest tightness and pain, exacerbate this fear, causing patients to avoid physical activity due to the fear of triggering similar discomfort (Çakal et al., 2022; Yakut Ozdemir et al., 2023). While “exercise anxiety” is a relevant term, it only represents one emotional component of kinesiophobia (Çakal et al., 2022; Liu et al., 2024). Anxiety involves a tendency to act, driven by the desire for success, whereas fear involves avoidance and a flight response. Understanding these distinctions can help healthcare professionals identify kinesiophobia in CHD patients early and develop targeted interventions.
This article defines kinesiophobia in CHD patients across four dimensions: physiological, psychological, cognitive, and behavioral. Key attributes include self-symptomatic distress, complex emotional responses, subjective avoidance behavior with personality tendencies, misperceptions and negative reactions. CHD patients are highly sensitive to bodily signals, with exercise-related sensations often resembling heart attack symptoms, leading to excessive fear (Bäck et al., 2017; Guo et al., 2022; Demirci et al., 2023). Patients’ uncertainty and fear of cardiac tolerance leads to excessive concern about adverse cardiac events (Knapik et al., 2019; Li L. et al., 2024). Therefore, the most important thing for patients with CHD is to strengthen the control and management of disease symptoms. The most direct and effective way to do this is through pharmacologic intervention and interventional therapy, but it is also critical to enhance patient education and awareness of the disease (Shen et al., 2023). Kinesiophobia in CHD patients reflects both a state and a trait, driven by personality and misconceptions about exercise (Wang et al., 2023; Zhu et al., 2024). Misconceptions and outdated beliefs about exercise lead to avoidance and negative attitudes (Demirci et al., 2023; Zhu et al., 2024). Improving patient education through videos, WeChat groups, and articles can enhance understanding and reduce fear (Piao et al., 2022; Yakut Ozdemir et al., 2023). Encouraging peer support and tailored exercise plans, along with professional guidance, can help patients overcome initial fears and promote a positive view of exercise (Bäck et al., 2020).
kinesiophobia in CHD patients is influenced by socio-demographic, disease-related, and psychological factors, leading to reduced participation in cardiac rehabilitation, lower functional capacity, higher rates of cardiovascular events and mortality, and decreased quality of life (Çakal et al., 2022; Yakut Ozdemir et al., 2023). Early identification of risk factors and targeted prevention are essential. Specific tools can identify high-risk patients, but specific scales for assessing kinesiophobia in CHD are scarce (Ozyemisci-Taskiran et al., 2020). Current scales also underexplore the behavioral aspects of kinesiophobia, which involve complex physiological, psychological, cognitive, and behavioral factors. Future research should incorporate a “behavioral dimension” to improve these scales. Moreover, as existing tools rely on subjective self-reports, objective scales from healthcare professionals’ perspectives are needed for greater accuracy. Recent studies have developed validated tools to assess self-management behavior in home-based cardiac rehabilitation, emphasizing the need for structured and comprehensive evaluation methods in cardiac patients (Yang et al., 2023c; Yang et al., 2024a). While some risk prediction tools identify high-risk patients with subacromial pain syndrome (SAPS) and chronic back pain, no such models exist for CHD patients (Panken et al., 2020; Karartı et al., 2023). This reflects a lack of awareness among healthcare professionals regarding early screening for kinesiophobia in CHD, likely due to the late start of research in this area, an unclear definition, and limited exploration of its mechanisms (Bäck et al., 2012). In the future, healthcare professionals must enhance their risk awareness, and consider developing a precise, targeted risk prediction tool using machine learning algorithms to identify high-risk CHD patients with kinesiophobia early, enabling timely, tailored interventions.
Kinesiophobia in CHD patients primarily stems from symptom distress and misperception. After heart-related events, patients become more sensitive to life-threatening situations and develop a heightened fear of death (Bäck et al., 2020; Shen et al., 2023). Cognitive biases make it difficult for them to distinguish between disease-related symptoms and those triggered by exercise, leading them to avoid physical activity out of fear (Bäck et al., 2013; Piao et al., 2022). Early recognition of symptoms, timely psychological intervention, and safe exercise guidance are essential to reducing kinesiophobia. Cognitive-behavioral therapy (CBT) has shown potential in addressing kinesiophobia (Ploutarchou et al., 2023). Guo et al. (2022) applied CBT in 49 patients post-myocardial infarction and found improvements in daily activity performance, reduced kinesiophobia, and alleviated anxiety and depression. However, some studies suggest that CBT may not have short-term effects on kinesiophobia, indicating a need for further investigation (Vergeld et al., 2021). Moreover, as highlighted by Yang et al. (2023b), it is essential to appropriately monitor both objective indicators and subjective status during patients’ physical activity to ensure exercise safety, while also providing essential technical support and education. Additionally, multidisciplinary team rehabilitation may be a promising approach, though it has not been studied in CHD patients. Its effectiveness has been demonstrated in chronic pain management (Monticone et al., 2014). A proposed team could include doctors, nurses, psychologists, and rehabilitation therapists, providing personalized interventions based on patient needs. In this context, establishing an effective social support network becomes a crucial strategy to enhance exercise participation among patients with chronic heart disease (Yang et al., 2024b). It can play a significant role in alleviating kinesiophobia and promoting long-term rehabilitation.
In conclusion, this study conducts a conceptual analysis of kinesiophobia in CHD patients, exploring its core characteristics and unique attributes to provide a clearer theoretical framework for clinical practice. Our findings emphasize that kinesiophobia is a subjective avoidance behavior influenced by individual traits, emotional responses, and cognitive distortions, beyond being merely a psychological condition. This understanding highlights the need for refined assessment tools and the development of targeted interventions. Integrating psychological support, cognitive-behavioral therapy, and multidisciplinary rehabilitation may improve patient outcomes, while structured patient education can correct misconceptions, promote safe exercise participation, and reduce avoidance behaviors. By addressing kinesiophobia comprehensively, healthcare providers can optimize rehabilitation strategies, enhance adherence to exercise programs, and improve long-term cardiovascular health.
This study has several limitations. As a concept analysis, it primarily relies on existing literature, which may result in incomplete information. Additionally, our systematic literature search was limited to publications in English and Chinese, potentially overlooking relevant studies in other languages. Furthermore, the analysis was influenced by the availability of existing research and our search strategy. Since this study is not a systematic review, we did not assess the quality of the included studies, which may introduce some bias. However, we adhered to standard practices for systematic evaluation to ensure the rigor of our analysis.
As research on kinesiophobia in CHD advances, there remains insufficient evidence on its conceptual content. This study analyzed the attributes, antecedents, and consequences of kinesiophobia in these patients, identifying its unique characteristics. Kinesiophobia in CHD patients is a subjective avoidance behavior that includes both “fear of pain or weakness” and “fear of cardiac events” based on personality tendencies, driven by complex emotional responses and misperceptions based on their own symptomatic disturbances, and presents an excessive and irrational fear of movement. This analysis supports the development of specific assessment tools and helps healthcare professionals design individualized intervention plans for patients.
M-JZ: Writing – original draft, Writing – review & editing, Conceptualization, Data curation, Formal analysis, Methodology, Supervision, Visualization. SL: Conceptualization, Data curation, Formal analysis, Methodology, Supervision, Visualization, Writing – original draft, Writing – review & editing. X-YX: Data curation, Formal analysis, Funding acquisition, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing. M-DL: Data curation, Formal analysis, Writing – original draft, Writing – review & editing. QX: Data curation, Writing – original draft, Writing – review & editing.
The author(s) declare that financial support was received for the research and/or publication of this article. This study was supported by the National Natural Science Foundation of China (No. 72064028) and the Scientific Research Project approved by the Chinese Nursing Association in 2023 (ZHKY202321).
We extend our gratitude to the authors of all the studies included in this review.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2025.1499962/full#supplementary-material
Bäck, M., Caldenius, V., Svensson, L., and Lundberg, M. (2020). Perceptions of Kinesiophobia in relation to physical activity and exercise after myocardial infarction: a qualitative study. Phys. Ther. 100, 2110–2119. doi: 10.1093/ptj/pzaa159
Bäck, M., Cider, Å., Herlitz, J., Lundberg, M., and Jansson, B. (2013). The impact on kinesiophobia (fear of movement) by clinical variables for patients with coronary artery disease. Int. J. Cardiol. 167, 391–397. doi: 10.1016/j.ijcard.2011.12.107
Bäck, M., Cider, Å., Herlitz, J., Lundberg, M., and Jansson, B. (2016). Kinesiophobia mediates the influences on attendance at exercise-based cardiac rehabilitation in patients with coronary artery disease. Physiother. Theory Pract. 32, 571–580. doi: 10.1080/09593985.2016.1229828
Bäck, M., Jansson, B., Cider, A., Herlitz, J., and Lundberg, M. (2012). Validation of a questionnaire to detect kinesiophobia (fear of movement) in patients with coronary artery disease. J. Rehabil. Med. 44, 363–369. doi: 10.2340/16501977-0942
Bäck, M., Lundberg, M., Cider, Å., Herlitz, J., and Jansson, B. (2018). Relevance of Kinesiophobia in relation to changes over time among patients after an acute coronary artery disease event. J. Cardiopulm. Rehabil. Prev. 38, 224–230. doi: 10.1097/HCR.0000000000000265
Bäck, M., Öberg, B., and Krevers, B. (2017). Important aspects in relation to patients' attendance at exercise-based cardiac rehabilitation – facilitators, barriers and physiotherapist's role: a qualitative study. BMC Cardiovasc. Disord. 17:77. doi: 10.1186/s12872-017-0512-7
Baykal Sahin, H., Kalaycioglu, E., and Sahin, M. (2021). The effect of cardiac rehabilitation on kinesiophobia in patients with coronary artery disease. Turk. J. Phys. Med. Rehabil. 67, 203–210. doi: 10.5606/tftrd.2021.5164
Bourke, A., Niranjan, V., O'Connor, R., and Woods, C. (2022). Barriers to and motives for engagement in an exercise-based cardiac rehabilitation programme in Ireland: a qualitative study. BMC Prim Care 23:28. doi: 10.1186/s12875-022-01637-7
Brunetti, N. D., Guerra, A., Ieva, R., Correale, M., Santoro, F., Tarantino, N., et al. (2017). Scared for the scar: fearsome impact of acute cardiovascular disease on perceived kinesiophobia (fear of movement). Clin. Cardiol. 40, 480–484. doi: 10.1002/clc.22682
Çakal, B., Yıldırım, M., and Emren, S. V. (2022). Kinesiophobia, physical performance, and health-related quality of life in patients with coronary artery disease. Postepy Kardiol Interwencyjnej 18, 246–254. doi: 10.5114/aic.2022.122892
Demirci, C., Oksul, M., Ozer, N., and Ozdemir, L. (2023). Effect of mindfulness on fatigue, kinesiophobia and quality of life in patients with acute myocardial infarction. Ann. Clin. Anal. Med. 14, 110–115. doi: 10.4328/ACAM.21365
Demirsoy, N., Taşkıran, Ö. Ö., Atan, T., Durmuş, D., Tur, B. S., Fındıkoğlu, G., et al. (2024). Does fear of activity predict exercise capacity in patients with coronary artery disease in both sexes? A cross-sectional multicenter study. Turk. J. Phys. Med. Rehabil. 70, 73–80. doi: 10.5606/tftrd.2024.12956
Dibben, G., Faulkner, J., Oldridge, N., Rees, K., Thompson, D. R., Zwisler, A. D., et al. (2021). Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst. Rev. 2021:Cd001800. doi: 10.1002/14651858.CD001800.pub4
Fu, C., Wang, H., Wei, Q., He, C., and Zhang, C. (2019). Effects of rehabilitation exercise on coronary artery after percutaneous coronary intervention in patients with coronary heart disease: a systematic review and meta-analysis. Disabil. Rehabil. 41, 2881–2887. doi: 10.1080/09638288.2018.1481148
Ghisi, G. L. D. M., Santos, R. Z. D., Felipe, T. R., Bonin, C. D. B., Pinto, E. F., Guerra, F. E. F., et al. (2017). Validation of the Portuguese version of the Tampa scale for kinesiophobia heart (TSK-SV heart). Rev. Bras. Med. Esporte 23, 227–231. doi: 10.1590/1517-869220172303159416
Gołba, A., Soral, T., Młynarska, A., Dzierzawa, M., Kowalik-Kabat, A., Dębska, B., et al. (2018). Kinesiophobia in patients with cardiovascular disease. Wiad. Lek. 71, 1653–1660.
Guo, W., Zhao, S., and Zhao, L. (2022). Therapeutic effect of cardiac rehabilitation combined cognitive behavioral therapy on kinesiophobia in AMI patients. Cardiac Cardiovasc. Res. 3:2121. doi: 10.54517/ccr.v3i2.2121
Jia, Y., Cui, N., Jia, T., Sattar, J. A., Hamoudi, H., and Song, J. (2024). Measurement properties of assessment tools of Kinesophobia in patients with cardiovascular disease: a systematic review. Int J Nurs Sci 11, 57–65. doi: 10.1016/j.ijnss.2023.12.016
Karartı, C., Basat, H., Özsoy, İ., Özyurt, F., Özsoy, G., Kodak, M., et al. (2023). Biopsychosocial approach in identifying risk factors of Kinesiophobia in persons with subacromial pain syndrome and developing a clinical prediction tool. Indian J. Orthop. 57, 124–136. doi: 10.1007/s43465-022-00781-7
Keessen, P., den Uijl, I., Visser, B., van den Berg-Emons, H. J. G., Latour, C. H. M., Sunamura, M., et al. (2020a). Fear of movement in patients attending cardiac rehabilitation: a validation study. J. Rehabil. Med. 52:jrm00114. doi: 10.2340/16501977-2749
Keessen, P., Latour, C. H. M., van Duijvenbode, I. C. D., Visser, B., Proosdij, A., Reen, D., et al. (2020b). Factors related to fear of movement after acute cardiac hospitalization. BMC Cardiovasc. Disord. 20:495. doi: 10.1186/s12872-020-01783-9
Khushnood, K., Sultan, N., Awan, M. M. A., Altaf, S., Mehmood, R., and Qureshi, S. (2023). Effects of pre-operative physical therapy on functional capacity, Kinesiophobia, and post-operative ICU stay in coronary artery bypass grafting candidates. Iran. Rehabil. J. 21, 81–88. doi: 10.32598/irj.21.1.1673.1
Kluszczyńska, M., Młynarska, A., and Mikulakova, W. (2021). Influence of frailty syndrome on kinesiophobia according to the gender of patients after coronary artery bypass surgery. Healthcare 9:730. doi: 10.3390/healthcare9060730
Knapik, A., Dąbek, J., and Brzęk, A. (2019). Kinesiophobia as a problem in adherence to physical activity recommendations in elderly polish patients with coronary artery disease. Patient Prefer. Adherence 13, 2129–2135. doi: 10.2147/PPA.S216196
Knuuti, J., Wijns, W., Saraste, A., Capodanno, D., Barbato, E., Funck-Brentano, C., et al. (2020). 2019 ESC guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 41, 407–477. doi: 10.1093/eurheartj/ehz425
Lethem, J., Slade, P. D., Troup, J. D., and Bentley, G. (1983). Outline of a fear-avoidance model of exaggerated pain perception--I. Behav. Res. Ther. 21, 401–408. doi: 10.1016/0005-7967(83)90009-8
Li, L., Jing Jing, P., and Shang, Z. (2024). Fatigue and physical activity in post-CABG patients: the parallel mediation model of kinesiophobia and self-efficacy: a prospective multicentre and cross-sectional study in China. BMJ Open 14:e082576. doi: 10.1136/bmjopen-2023-082576
Li, Q., Yan, L., Xing, W., Zhou, C., Li, Y., Wan, B., et al. (2024). The effect of fear-avoidance intervention on kinesiophobia and self-efficacy in patients after percutaneous coronary intervention: study protocol for a clinical randomized controlled trial. Trials 25:517. doi: 10.1186/s13063-024-08349-6
Liu, Y., Ye, F., Liu, J., Yu, J., Fan, L., and Yang, Q. (2024). Study of factors influencing early Kinesiophobia in older patients after coronary artery bypass grafting in China. Heart Surgery Forum 27, E504–E510. doi: 10.59958/hsf.7377
Lum, E., McCreanor, V., Luo, N., and Graves, N. (2020). Quality of life measured by EQ-5D at different treatment time points for coronary artery disease: protocol for a systematic review and meta-analysis. BMJ Open 10:e039311. doi: 10.1136/bmjopen-2020-039311
Masuy, R., Bamelis, L., Bogaerts, K., Depreitere, B., De Smedt, K., Ceuppens, J., et al. (2022). Generalization of fear of movement-related pain and avoidance behavior as predictors of work resumption after back surgery: a study protocol for a prospective study (WABS). BMC Psychol 10:39. doi: 10.1186/s40359-022-00736-5
Monticone, M., Ambrosini, E., Rocca, B., Magni, S., Brivio, F., and Ferrante, S. (2014). A multidisciplinary rehabilitation programme improves disability, kinesiophobia and walking ability in subjects with chronic low back pain: results of a randomised controlled pilot study. Eur. Spine J. 23, 2105–2113. doi: 10.1007/s00586-014-3478-5
Özden, F., Özkeskin, M., Tümtürk, İ., Özlek, E., and Özlek, B. (2023). The investigation of Kinesiophobia, pain catastrophizing, physical activity, anxiety, and depression in patients with myocardial infarction. J. Basic Clin. Health Sci. 7, 684–692. doi: 10.30621/jbachs.1173700
Ozyemisci-Taskiran, O., Demirsoy, N., Atan, T., Yuksel, S., Coskun, O., Aytur, Y. K., et al. (2020). Development and validation of a scale to measure fear of activity in patients with coronary artery disease (fact-CAD). Arch. Phys. Med. Rehabil. 101, 479–486. doi: 10.1016/j.apmr.2019.09.001
Panken, A. M., Staal, J. B., and Heymans, M. W. (2020). Kinesiophobia is not required to predict chronic low back pain in workers: a decision curve analysis. BMC Musculoskelet. Disord. 21:163. doi: 10.1186/s12891-020-3186-8
Pardaens, S., Willems, A. M., Clays, E., Baert, A., Vanderheyden, M., Verstreken, S., et al. (2017). The impact of drop-out in cardiac rehabilitation on outcome among coronary artery disease patients. Eur. J. Prev. Cardiol. 24, 1490–1497. doi: 10.1177/2047487317724574
Piao, J. J., Gu, Y., Ling, Y., Chi, L., Chen, Y., and Wang, R. (2022). Mediating effect of kinesiophobia between self-efficacy and physical activity levels in post-CABG patients: protocol for a prospective, multicentre, cross-sectional study in China. BMJ Open 12:e062013. doi: 10.1136/bmjopen-2022-062013
Ploutarchou, G., Savva, C., Karagiannis, C., Pavlou, K., O'Sullivan, K., and Korakakis, V. (2023). The effectiveness of cognitive behavioural therapy in chronic neck pain: a systematic review with meta-analysis. Cogn. Behav. Ther. 52, 523–563. doi: 10.1080/16506073.2023.2236296
Ratnoo, B., Mulla, A., Oza, F., and Vyas, M. (2023). Prevalence of anxiety, depression, kinesiophobia, and impaired shoulder function in patients following coronary artery bypass grafting: An observational study. J. Indian Coll. Cardiol. 13, 147–153. doi: 10.4103/jicc.jicc_36_23
Ren, P., Zhang, Y., Ding, L., Tang, A., Dong, L., Ge, Y., et al. (2022). The mediating effect of Kinesophobia on self-efficacy and exercise adherence in patients with acute myocardial infarction after PCI. Nurs. J. Chin. People Liberat. Army. 39, 21–24. doi: 10.3969/j.issn.1008-9993.2022.01.006
Resurrección, D. M., Moreno-Peral, P., Gómez-Herranz, M., Rubio-Valera, M., Pastor, L., Caldas de Almeida, J. M., et al. (2019). Factors associated with non-participation in and dropout from cardiac rehabilitation programmes: a systematic review of prospective cohort studies. Eur. J. Cardiovasc. Nurs. 18, 38–47. doi: 10.1177/1474515118783157
Rodgers, B. L. (1989). Concepts, analysis and the development of nursing knowledge: the evolutionary cycle. J. Adv. Nurs. 14, 330–335. doi: 10.1111/j.1365-2648.1989.tb03420.x
Rodgers, B. L., Jacelon, C. S., and Knafl, K. A. (2018). Concept analysis and the advance of nursing knowledge: state of the science. J. Nurs. Scholarsh. 50, 451–459. doi: 10.1111/jnu.12386
Rodgers, B. L., and Knafl, K. A. (1993). Concept development in nursing: Foundations, techniques, and applications. Philadelphia, PA: W. B. Saunders.
Roelofs, J., van Breukelen, G., Sluiter, J., Frings-Dresen, M. H. W., Goossens, M., Thibault, P., et al. (2011). Norming of the Tampa scale for Kinesiophobia across pain diagnoses and various countries. Pain 152, 1090–1095. doi: 10.1016/j.pain.2011.01.028
Roth, G. A., Mensah, G. A., Johnson, C. O., Addolorato, G., Ammirati, E., Baddour, L. M., et al. (2020). Global burden of cardiovascular diseases and risk factors, 1990-2019: update from the GBD 2019 study. J. Am. Coll. Cardiol. 76, 2982–3021. doi: 10.1016/j.jacc.2020.11.010
Sentandreu-Mañó, T., Deka, P., Almenar, L., Tomás, J. M., Ferrer-Sargues, F. J., López-Vilella, R., et al. (2024). Kinesiophobia and associated variables in patients with heart failure. Eur. J. Cardiovasc. Nurs. 23, 221–229. doi: 10.1093/eurjcn/zvad072
Shea, M. G., Farris, S. G., Hutchinson, J., Headley, S., Schilling, P., and Pack, Q. R. (2023). Effects of exercise testing and cardiac rehabilitation in patients with coronary heart disease on fear and self-efficacy of exercise: a pilot study. Int. J. Behav. Med. 31, 659–668. doi: 10.1007/s12529-023-10207-9
Shen, Y., Yan, T., Peng, Q., Zhang, B., Zhao, K., and Yang, Z. (2023). Kinesiophobia in patients with angina pectoris of coronary artery disease: a cross-sectional survey. Heart Lung 57, 7–11. doi: 10.1016/j.hrtlng.2022.07.012
Song, X., Ma, S., Peng, Y., Zhu, Y., An, L., and Li, S. (2022). Influencing factors of kinesiophobia in angina pectoris patients based on structural equation model. J. Nurs. Sci. 37, 64–67. doi: 10.3870/j.issn.1001-4152.2022.12.064
Thomas, R. J. (2024). Cardiac rehabilitation – challenges, advances, and the road ahead. N. Engl. J. Med. 390, 830–841. doi: 10.1056/NEJMra2302291
Timmis, A., Townsend, N., Gale, C. P., Torbica, A., Lettino, M., Petersen, S. E., et al. (2020). European Society of Cardiology: cardiovascular disease statistics 2019. Eur. Heart J. 41, 12–85. doi: 10.1093/eurheartj/ehz859
Tofthagen, R., and Fagerstrøm, L. M. (2010). Rodgers' evolutionary concept analysis--a valid method for developing knowledge in nursing science. Scand. J. Caring Sci. 24, 21–31. doi: 10.1111/j.1471-6712.2010.00845.x
Vergeld, V., Martin Ginis, K. A., and Jenks, A. D. (2021). Psychological interventions for reducing fear avoidance beliefs among people with chronic back pain. Rehabil. Psychol. 66, 386–403. doi: 10.1037/rep0000394
Virani, S. S., Alonso, A., Aparicio, H. J., Benjamin, E. J., Bittencourt, M. S., Callaway, C. W., et al. (2021). Heart disease and stroke statistics—2021 update. Circulation 143, e254–e743. doi: 10.1161/CIR.0000000000000950
Vlaeyen, J. W. S., Kole-Snijders, A. M. J., Boeren, R. G. B., and van Eek, H. (1995). Fear of movement/(re)injury in chronic low back pain and its relation to behavioral performance. Pain 62, 363–372. doi: 10.1016/0304-3959(94)00279-N
Vlaeyen, J. W. S., and Linton, S. J. (2012). Fear-avoidance model of chronic musculoskeletal pain: 12 years on. Pain 153, 1144–1147. doi: 10.1016/j.pain.2011.12.009
Vlaeyen, J. W. S., Morley, S., Linton, S. J., Boersma, K., and de Jong, J. (2012). Pain-related fear: exposure-based treatment of chronic pain. Seattle, WA: IASP Press.
Wang, Y., Fan, J., Shi, X., Wang, M., Lu, J., Lu, M., et al. (2022a). Longitudinal study on kinesiophobia in patients with acute myocardial infarction:the influencing factors. J. Nurs. Sci. 37, 27–31. doi: 10.3870/j.issn.1001-4152.2022.14.027
Wang, Z., Liu, X., Zhang, Q., Yu, M., Zheng, B., Lu, J., et al. (2022). Study on the trajectory of kinesiophobia levels in patients after percutaneous coronary intervention. Chin. J. Nurs. 57, 1035–1041. doi: 10.3761/j.issn.0254-1769.2022.09.002
Wang, Y., Sang, W., Jia, G., Qin, N., Sun, J., Wang, D., et al. (2022b). Causes of high level kinesiophobia in first-episode patients with acute myocardial infarction: a qualitative study. J. Nurs. Sci. 37, 23–25. doi: 10.3870/j.issn.1001-4152.2022.07.023
Wang, Z., Zhang, Y., Wang, Y., Liu, L., and Zhang, J. (2023). Kinesiophobia and its associated factors in patients with coronary heart disease: a cross-sectional study based on latent feature analysis. BMJ Open 13:e072170. doi: 10.1136/bmjopen-2023-072170
Wasiuk-Zowada, D., Knapik, A., Szefler-Derela, J., Brzęk, A., and Krzystanek, E. (2021). Kinesiophobia in stroke patients, multiple sclerosis and Parkinson’s disesase. Diagnostics 11:796. doi: 10.3390/diagnostics11050796
Xiao, J., Wang, R., Xie, M., Xia, R., and Zhang, J. (2024). Latent profiles of kinesiophobia and their relationships with physical activity among patients after percutaneous coronary intervention. J. Nurs. Sci. 39, 42–46. doi: 10.3870/j.issn.1001-4152.2024.01.042
Yakut Ozdemir, H., Ozalevli, S., Felekoglu, E., Baskurt, A. A., and Dursun, H. (2023). Kinesiophobia and associated factors in patients with myocardial infarction. Percept. Mot. Skills 130, 2564–2581. doi: 10.1177/00315125231204059
Yang, Z., Hu, N., Zhang, F., Gao, Y., Zhang, C., and Wang, A. (2024a). A practical tool for measuring home-based cardiac rehabilitation self-management behavior: a multiphase cross-sectional study. J. Am. Heart Assoc. 13:e034486. doi: 10.1161/JAHA.124.034486
Yang, Z., Jia, H., and Wang, A. (2023a). Predictors of home-based cardiac rehabilitation exercise adherence among patients with chronic heart failure: a theory-driven cross-sectional study. BMC Nurs. 22:415. doi: 10.1186/s12912-023-01566-5
Yang, Z., Jia, H., Zhang, F., Huang, H., Hao, X., and Wang, A. (2024b). A behavioural driving model of adherence to home-based cardiac rehabilitation exercise among patients with chronic heart failure: a mixed-methods study. J. Clin. Nurs. 33, 531–542. doi: 10.1111/jocn.16901
Yang, Z., Sun, L., Sun, Y., Dong, Y., and Wang, A. (2023b). A conceptual model of home-based cardiac rehabilitation exercise adherence in patients with chronic heart failure: a constructivist grounded theory study. Patient Prefer. Adherence 17, 851–860. doi: 10.2147/PPA.S404287
Yang, Z., Sun, Y., Wang, H., Zhang, C., and Wang, A. (2023c). A scale for measuring home-based cardiac rehabilitation exercise adherence: a development and validation study. BMC Nurs. 22:259. doi: 10.1186/s12912-023-01426-2
Yang, Z., Zheng, X., Hu, N., Zhang, F., and Wang, A. (2023d). “Challenges to normalcy”-perceived barriers to adherence to home-based cardiac rehabilitation exercise in patients with chronic heart failure. Patient Prefer. Adherence 17, 3515–3524. doi: 10.2147/PPA.S440984
Zhang, S., Wang, Z., Lin, X., Li, Y., Xue, Y., Ban, J., et al. (2023). Kinesiophobia and self-management behaviour related to physical activity in Chinese patients with coronary heart disease: the mediating role of self-efficacy. Nurs. Open 10, 105–114. doi: 10.1002/nop2.1283
Keywords: fear of movement, ischemic heart disease, chronic diseases, physical exercise, physical activity, cardiac rehabilitation
Citation: Zhang M-J, Liu S, Xiong X-Y, Liu M-D and Xiang Q (2025) Kinesiophobia in patients with coronary heart disease: a Rodgers’ evolutionary concept analysis. Front. Psychol. 16:1499962. doi: 10.3389/fpsyg.2025.1499962
Edited by:
Bart Visser, Amsterdam University of Applied Sciences, NetherlandsReviewed by:
Fatih Özden, Mugla University, TürkiyeCopyright © 2025 Zhang, Liu, Xiong, Liu and Xiang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiao-Yun Xiong, eHh5NjY5MkAxNjMuY29t
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.