 Meng Wang
Meng Wang Jing Yu1*
Jing Yu1* Xinyue Yang
Xinyue Yang- 1College of Sports Science, Shenyang Normal University, Shenyang, China
- 2Martial Arts and Dance Academy, Shenyang Sport University, Shenyang, China
- 3Department of Physical Education, Keimyung University, Daegu, Republic of Korea
Objective: Non-integrated primitive reflexes (PRs) in children can lead to issues in motor function and psychological wellbeing, while prior studies have shown correlations between PR integration and neurodevelopmental disorders in children. However, measurement methods for PR integration remain unestablished. Therefore, in the present study, we describe the development of a measurement scale for PR integration, a novel assessment tool to evaluate PR integration in children.
Methods: Combining a literature review, practical experience, and results of specialized group discussions, a preliminary draft of the Children's Primitive Reflex Integration Measurement Scale (CPRIMS) was formulated. Employing a convenience sampling method, participants were selected from first and second-grade students in three primary schools in Liaoning province, Shenyang city, from May to July 2023. Item Discrimination Method (IDM), Critical Ratio Method (CRM), and Internal Consistency Coefficient Method (ICCM) were used for item analysis of pilot testing data. For formal testing data, Cronbach's α assessed the reliability of the scale, while fit indices such as chi-square value/degrees of freedom (χ2/df), Root Mean Square Error of Approximation (RMSEA), and Comparative Fit Index (CFI), along with tests of construct validity, evaluated the scale's validity.
Results: Overall, 555 participants were selected, 234 children with a mean age of 7.59 ± 0.71 years participated in the pilot testing, while 321 children with a mean age of 7.73 ± 0.71 years participated in the formal testing. CPRIMS comprises seven dimensions and seventeen items, including the Moro reflex (MR), Asymmetrical Tonic Neck Reflex (ATNR), Symmetrical Tonic Neck Reflex (STNR), Tonic Labyrinthine Reflex (TLR), Spinal Galant Reflex (SGR), Spinal Perez Reflex (SPR), and Landau Reflex (LR), explaining 88.2% of the total variance. Confirmatory factor analysis revealed a good model fit (χ2/df = 1.631, RMSEA = 0.044, NFI = 0.950, CFI = 0.980, IFI = 0.932, TLI = 0.972). Cronbach's α coefficients for the seven dimensions ranged from 0.730 to 0.945, demonstrating strong reliability.
Conclusion: CPRIMS, which includes dimensions such as MR, ATNR, STNR, TLR, SGR, SPR, and LR, demonstrates strong reliability and validity, indicating that this measure could serve as a reliable and effective tool for assessing the integration levels of PRs in children aged 6 to 9 years old.
1 Introduction
Primitive reflexes (PRs) develop during the fetal or infant stages. During infancy, more than 20 types of PRs are exhibited, including swallowing, breathing, visual and auditory responses, head movements, hand grasping movements, trunk control, and lower limb movements, among others (Bilbilaj et al., 2017). As infants grow and develop, most PRs gradually integrate and evolve into more complex patterns, enabling self-control of body movements and motor skills (Berne, 2006); however, a small portion of these reflexes persist (Wang et al., 2023). PRs initially serve to protect newborns from external stimuli and are gradually integrated into purposeful movements (Berne, 2006). However, if PRs fail to integrate within an appropriate timeframe, they may impact the brain's ability to effectively process sensory information (Blythe, 1996) and lead to motor dysfunction in children (Adams and Craft, 2014), as well as cognitive and psychological issues, and neurodevelopmental disorders (Wang et al., 2023). Specifically, compared to children with non-integrated PRs, those with non-integrated PRs can experience motor dysfunctions (Adams and Craft, 2014), such as difficulties in handling fine and gross motor tasks, poor balance, and challenges with hand-eye coordination (Wang et al., 2023; Blythe, 1996; Adams and Craft, 2014; Blythe, 2002). In terms of cognitive and psychological aspects, children with non-integrated PRs may further struggle with interpersonal interactions, exhibit higher levels of anxiety and oppositional behavior (Melillo et al., 2020; Quevedo et al., 2015; Pecuch et al., 2020; Yang, 2024), and could display hyperactive or impulsive behaviors, particularly during cognitively demanding tasks, or when required to maintain focus for extended periods, which can lead to learning difficulties (Taylor et al., 2004; Konicarova et al., 2013). Additionally, non-integrated PRs have been associated with neurodevelopmental disorders, such as bipolar disorder (Tuysuzoglu et al., 2011), cerebral palsy with movement disorders (Kyllerman et al., 1982; Eek et al., 2018), and dyslexia (Chinello et al., 2018), and are also associated with learning disabilities (Hermann, 2012; Grzywniak, 2017; Feldhacker et al., 2021), scoliosis (Gieysztor et al., 2018), and eating issues (Gieysztor et al., 2022; Hobo et al., 2014).
These challenges can have profound negative impacts on a child's life. As such, the assessment of PR integration holds significant value in the treatment and prevention of motor dysfunctions, mental health issues, and neurodevelopmental disorders in children. However, current research and attention in the field of PRs remain insufficient. Through a review of the literature, it was found that existing measurement tools are not yet well-developed. The INPP Reflex Assessment Test (Blythe, 2017) was adapted from the original Blythe-McGlown Child Questionnaire, initially designed by Blythe and McGlown in 1979, revised in 1998, and further modified by Goddard Blythe in 2006. Nevertheless, the questionnaire heavily relies on comprehensive information, including detailed developmental data from pregnancy to school age. Collecting such data demands respondents to possess strong memory and precise expression skills, which significantly increases the difficulty of data collection. The Bender-Purdue Reflex Test (Bender, 1978) relies on parents or teachers to judge whether a child's PRs are non-integrated based on behavioral and psychological traits associated with different types of children. However, this questionnaire emphasizes superficial behavioral phenomena (e.g., “Not really hyperkinetic or immature” and “Easily distracted by anything and everything”) rather than directly assessing children's primitive reflex integration through specific physical actions, potentially affecting the accuracy of evaluation results. The Schilder Test and Goddard Test (Morrison, 1985; Hickey and Feldhacker, 2022) include well-structured measurement procedures, observation methods, and scoring standards. But they were developed in 2005 and lack clear validity and reliability indicators. Functionally, PRs primarily assist newborns and infants in interacting with their environment through reflexive actions before cortical control is established (Hickey and Feldhacker, 2022). Yet, given the rapid evolution of society, questions arise as to whether the types of non-integrated PRs have changed, whether such phenomena have become more prevalent among children, or whether new characteristics have emerged. Furthermore, inconsistencies in the description of scoring standards for these measurement methods warrant further exploration.
Additionally, our review of studies employing the Schilder Test and Goddard Test revealed variability in the age of participants: Konicarova and Bob (2012) assessed children aged 8–11 years, while Hickey and Feldhacker (2022) focused on children aged 4–6 years. Retained Symmetric Tonic Neck Reflex (STNR), Asymmetric Tonic Neck Reflex (ATNR), and Moro Reflex (MR) can result in behavioral and psychological issues such as anxiety, reading difficulties, and time management problems (Taylor et al., 2004; Gieysztor et al., 2018; Hickey and Feldhacker, 2022). These issues often go undetected before school age but become more apparent as children approach or enter school. To further investigate the behavioral and psychological problems caused by non-integrated PRs, this study aims to explore the integration of PRs in children aged 6–9 years. The study will pioneer the development of the Children's Primitive Reflex Integration Measurement Scale (CPRIMS) to provide a reliable tool for scientifically and objectively assessing the integration levels of PRs in children.
2 Participants and methods
2.1 Participant screening
To construct the sample, a convenience sampling method was applied during May–June 2023 to collect first and second-grade students from three primary schools in Shenyang, China as participants for the pilot study. In June–July 2023, the same method was applied to select students from the same three schools as participants for the formal study. The sample size for the item selection and validity-reliability analysis were determined based on the standard suggested by prior research (Kline, 2011), which recommends a ratio of 5 to 10 participants per item.
The inclusion criteria were as follows: (1) Agreed to voluntarily participate in the measurement; (2) Normal or corrected to normal hearing and vision; and (3) Normal intellectual level. The exclusion criteria were as follows: (1) Lack of basic comprehension and communication abilities; (2) Prior participation in similar types of measurements; (3) Any physical illnesses. Following the application of these criteria, 555 students participated in this study. All participants were recruited through their schools, and written consent was provided by parents or legal guardians. This study was approved by the Ethics Committee of Shenyang Sport University, Liaoning Province, China.
2.2 Initial items for scale development
The item pool and structure of the Primitive Reflex Integration Measurement Scale were developed as follows: First, the methods for evaluating Primitive Reflex Integration in previous studies (Wagner, 2015; Geerlinks, 2018; Feldhacker et al., 2022; Futagi et al., 2012; Bob et al., 2021; Futagi et al., 1992; Zafeiriou et al., 1995, 1999a,b; Zafeiriou, 2000; Konicarova and Bob, 2012, 2013) were organized and combined with practical experience. A panel discussion was then held, involving five special education teachers and five pediatricians, to review, analyze, and refine each item. Adjustments were made to the categorization of dimensions and the simplification of expressions. Initially, the draft scale consisted of 45 items across 13 dimensions, which was then refined to 37 items across 12 dimensions to create the Primitive Reflex Integration Pilot Scale. The final categorization of dimensions would be determined through confirmatory factor analysis. The scale's framework includes the following reflexes: MR, ATNR, STNR, Tonic Labyrinthine Reflex (TLR), Spinal Galant Reflex (SGR), Spinal Perez Reflex (SPR), Landau Reflex (LR), Palmar Grasp Reflex (PAGR), Plantar Grasp Reflex (PLGR), Babkin Reflex (BNR), Hands Pulling Reflex (HPR), and Babinski Reflex (BIR). A 4-point Likert scale was used (0 = Not Present, 1 = Slight, 2 = Noticeable, 3 = Very Noticeable) to form the scoring criteria for the pilot scale (Xue et al., 2023). The measurement was conducted by 10 trained researchers in the relevant field, working in pairs to independently observe and score each participant. If there was a discrepancy in scoring, a third researcher was brought in to resolve the inconsistency.
3 Statistical methods
3.1 Item analysis
Pilot data were analyzed using IBM SPSS Statistics 26.0, employing the following item analysis methods: (1) Item Discrimination Method (IDM): Participants were ranked based on their total scores, with the top 27% categorized as the high-score group, and the bottom 27% as the low-score group. The item discrimination value for each item was calculated by dividing the difference between the mean scores of the high and low groups by the range of scores. Items with a discrimination value of <0.2 were removed (Ebel and Frisbie, 1991); (2) Critical Ratio Method: An independent sample t-test was applied to compare the mean scores between the high and low groups. Items were deleted if the difference did not reach statistical significance (P > 0.05), or if the critical ratio was <3 (Wu, 2010); (3) Internal Consistency Coefficient Method (ICCM): The Cronbach's α coefficient was calculated following the sequential deletion of each item. If the resulting Cronbach's α was greater than the Cronbach's α of the overall scale, the item was considered to reduce the internal consistency of the scale, and was deleted (Lance et al., 2006).
3.2 Reliability and validity analysis
Reliability and validity analysis were conducted using the formal measurement data. The reliability of the scale and its dimensions were assessed based on the calculated Cronbach's α coefficients, with values closer to 1 indicating better reliability. A Cronbach's α > 0.6 indicated acceptable reliability, while a value <0.6 suggested poor reliability (Tsai et al., 2017). In the development of the scale, previous studies (Blythe, 2017; Bender, 1978; Morrison, 1985; Hickey and Feldhacker, 2022; Kline, 2011; Wagner, 2015; Geerlinks, 2018; Feldhacker et al., 2022; Futagi et al., 2012; Bob et al., 2021; Futagi et al., 1992; Zafeiriou et al., 1995, 1999a,b; Zafeiriou, 2000; Konicarova and Bob, 2012, 2013; Blomberg, 2015; Zhao, 2019) have fully validated the theoretical framework of PRs and the dimensions of each type. Therefore, this study directly employed confirmatory factor analysis (CFA) to assess the model fit, without the need for exploratory factor analysis. CFA was conducted using Analysis of Moment Structure 28.0, with reference to the chi-square value/degrees of freedom (χ2/df), Root Mean Square Error of Approximation (RMSEA), Normed Fit Index (NFI), Tucker-Lewis Index (TLI), Incremental Fit Index (IFI), and Comparative Fit Index (CFI) to determine the model fit. Convergent and discriminant validity of the scale were reflected through factor loadings, composite reliability, average variance extracted (AVE), the square root of the AVE, and factor inter-correlations.
4 Results
4.1 Sample characteristics
A total of 555 students participated in this study. Of these, 234 students were involved in the pilot stage of scale development, including 102 boys and 132 girls, with an age range of 6 to 9 years and a mean age of 7.59 ± 0.71 years. In the formal stage of scale development, 321 students participated, comprising 171 boys and 150 girls, with an age range of 6 to 9 years and a mean age of 7.73 ± 0.71 years. The participants in both the pilot and formal stages showed no significant differences in terms of age, family background, education, or income levels.
4.2 Item analysis
After discussion by the expert panel, the initial draft scale, which consisted of 45 items across 13 dimensions, was refined to 37 items across 12 dimensions, resulting in the Primitive Reflex Integration Pilot Scale. The scale's framework includes the following reflexes: MR, ATNR, STNR, Tonic Labyrinthine Reflex (TLR), Spinal Galant Reflex (SGR), Spinal Perez Reflex (SPR), Landau Reflex (LR), Palmar Grasp Reflex (PAGR), Plantar Grasp Reflex (PLGR), Babkin Reflex (BNR), Hands Pulling Reflex (HPR), and Babinski Reflex (BIR). Based on the results of the IDM, CRM, and ICCM tests, a total of 20 items were initially identified for deletion. Specifically, 20 items were deleted according to the IDM test, 17 items based on the CRM test, and 7 items based on the ICCM test. After considering professional knowledge and ensuring content completeness, one item was adjusted and retained. Ultimately, 20 items were deleted, resulting in a preliminary version of the scale with 7 dimensions and 17 items (see Table 1).
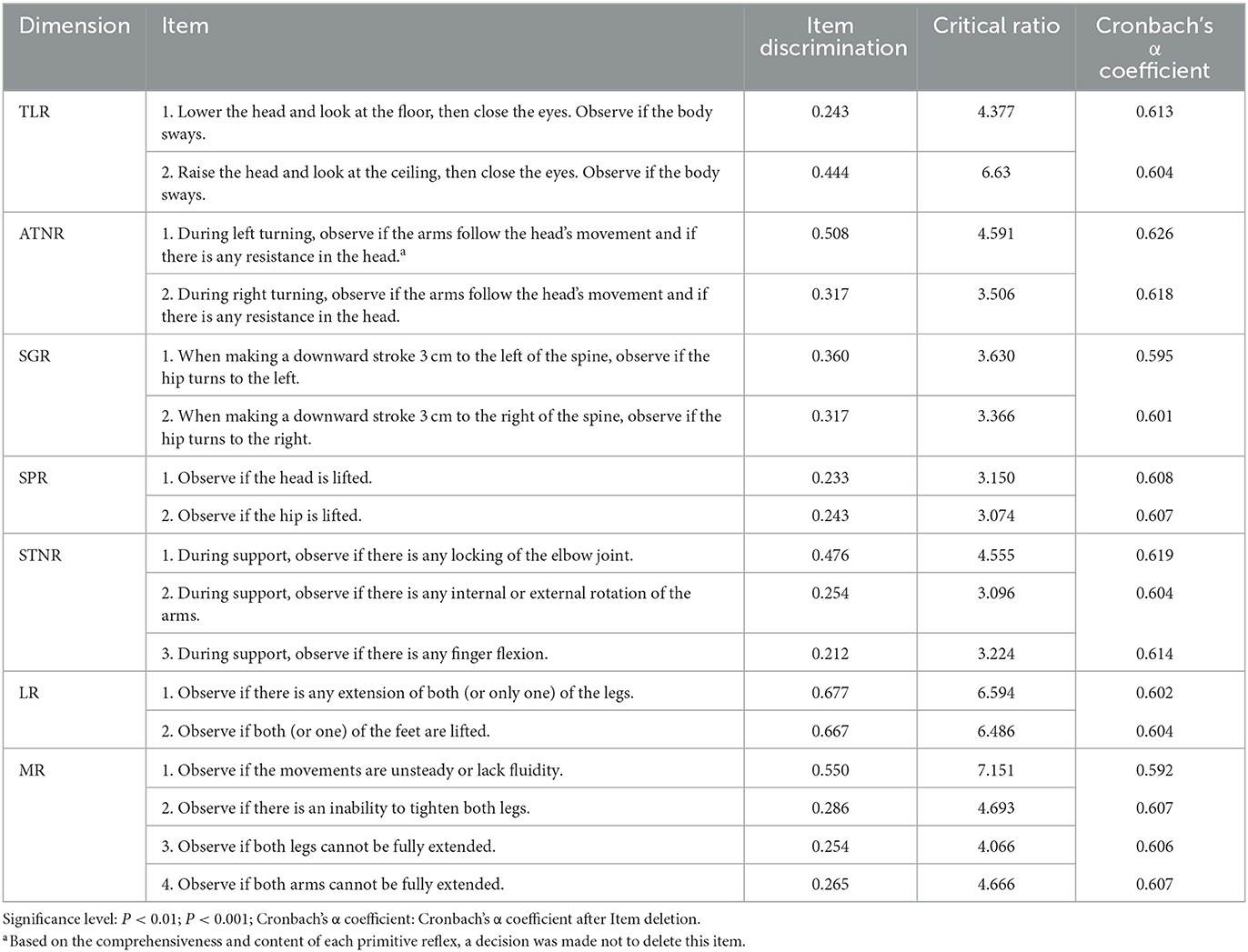
Table 1. Results of the analysis of the preliminary version of the primitive reflex integration scale items.
4.3 Reliability and validity analysis
The Cronbach's α coefficients for the TLR, ATNR, SGR, SPR, STNR, LR, and MR dimensions were 0.730, 0.797, 0.808, 0.945, 0.767, 0.938, and 0.929, respectively, with values ranging from 0.730 to 0.945, all >0.7. Overall, the reliability was within an acceptable range, indicating good internal consistency of the scale. The model fit of the scale was further analyzed using the maximum likelihood method, with results showing [χ2/df = 1.631(<3) (Iacobucci, 2010), RMSEA = 0.044 (< 0.05) (Byrne, 2010), NFI = 0.950 (>0.9) (Lan et al., 2023), IFI = 0.932 (>0.9) (Ganotice et al., 2023), TLI = 0.972 (>0.9) (Heblich et al., 2023), and CFI = 0.980 (>0.9) (Iani et al., 2014)], indicating good model fit. The factor loadings between items and factors ranged from 0.56 to 0.98, all > 0.5 (Wei and Nguyen, 2020) (see Figure 1), indicating that the items corresponding to each latent variable have a certain level of representativeness; Composite reliability (CR) was >0.7 (Tobón and Luna-Nemecio, 2021); and the AVE for each factor was >0.5 (Fornell and Larcker, 1981; Yu et al., 2022), indicating that the convergent validity of each factor is ideal. Additionally, the square root of the AVE for each factor was greater than the correlation coefficients between factors, indicating good discriminant validity of the model (Wang et al., 2022) (see Table 2).
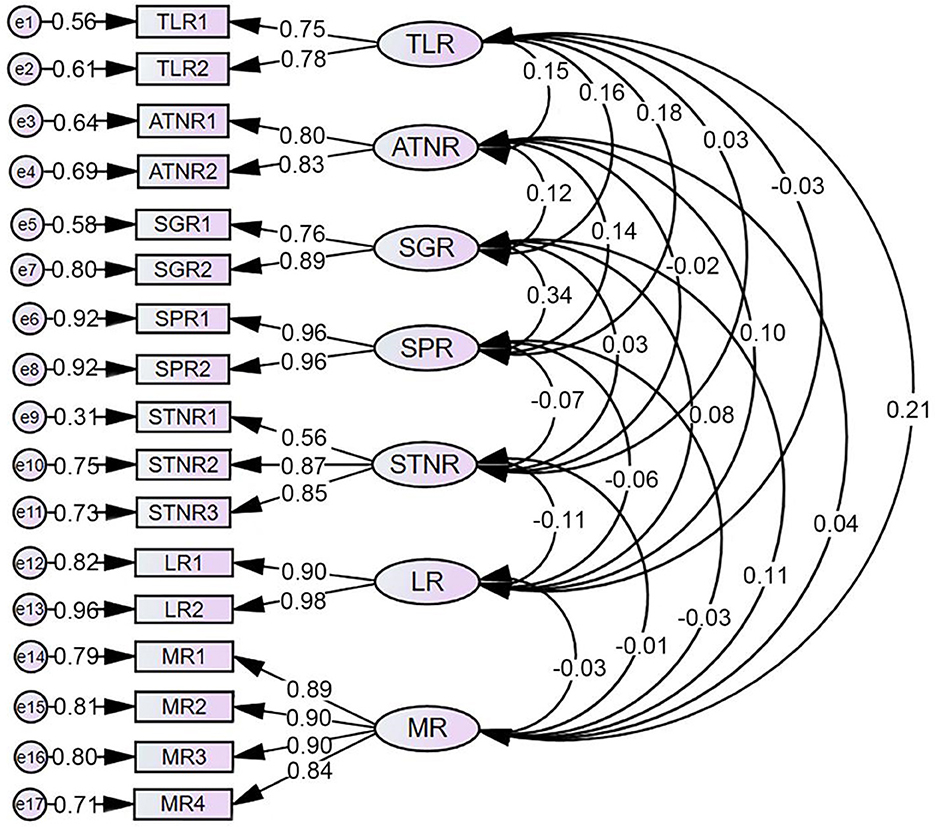
Figure 1. Model of the factor analysis results for the preliminary version of the primitive reflex integration measurement scale.
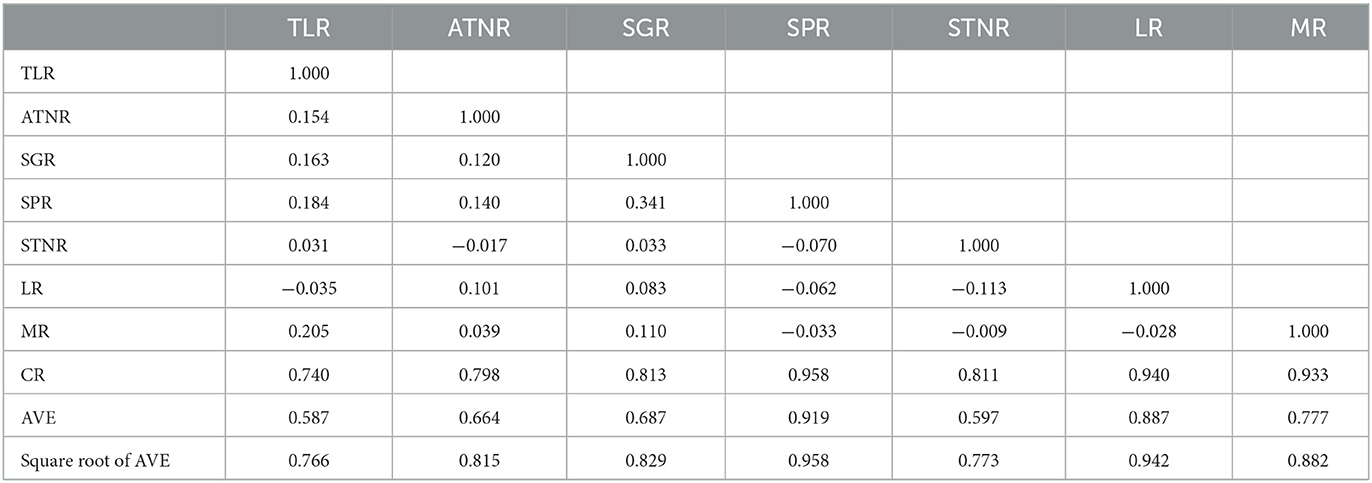
Table 2. Convergent and discriminant validity of the scale.
5 Discussion
This study ultimately developed the CPRIMS, a tool comprising 17 items across 7 dimensions, designed to scientifically assess the integration status of seven primitive reflexes in children. These reflexes include the TLR, ATNR, SGR, SPR, STNR, LR, and MR. By reviewing and analyzing existing research from both domestic and international sources, we summarized the formation, integration timeline, and symptoms of seven types of non-integration reflexes, providing a theoretical foundation for the scale's design.
ATNR typically begins to form in utero, usually appearing around 18 weeks of gestation, and gradually integrating within 3 to 9 months after birth (Berne, 2006; Blythe, 2002). Failure to integrate, in some cases, ATNR may impair children's ability to handle fine and gross motor tasks, leading to motor difficulties (Adams and Craft, 2014; Pecuch et al., 2020). STNR generally appears between 6 to 9 months of age, with integration typically completed within 9 to 11 months postnatally (Berne, 2006; Adams and Craft, 2014). Non-integrated STNR has been associated with poor organizational skills and abnormal hand-eye coordination (Wang et al., 2023). MR generally starts developing in utero around 9 to 12 weeks of gestation and integrates within 4 months after birth (Berne, 2006; Adams and Craft, 2014). Non-integrated MR is associated with emotional dysregulation, anxiety toward new activities, immature social behavior, and symptoms such as inattention or impulsivity (Adams and Craft, 2014; Futagi et al., 2012). TLR consists of two aspects: TLR forward and TLR backward. TLR forward typically forms around 12 weeks after birth, integrating within 3 to 4 months postnatally (Berne, 2006; Blythe, 2002). While TLR backward appears at birth and may take between 6 weeks and 3 years to integrate (Berne, 2006; Adams and Craft, 2014; Blythe, 2002; Pecuch et al., 2020). Non-integrated TLR can impact motor abilities, with TLR forward often associated with low muscle tone and TLR backward with high muscle tone, resulting in postural problems, balance difficulties, and even issues with visual and oculomotor control (Berne, 2006; Adams and Craft, 2014; Blythe, 2002). SGR typically begins developing in utero around 20 weeks of gestation and integrates within 9 months after birth (Adams and Craft, 2014). Non-integrated SGR may result in restlessness, affect short-term memory, disrupt time and spatial orientation development, and impact classroom attention (Adams and Craft, 2014). SPR usually appears at birth and integrates within 3 to 6 months postnatally (Wagner, 2015; Geerlinks, 2018). Non-integrated SPR can lead to hypersensitivity in the auditory and tactile systems, accompanied by sensory processing disorders, overactivity, and poor memory (Wagner, 2015). LR begins developing in utero around 4 weeks of gestation and takes about 3 years to fully integrate (Wagner, 2015; Geerlinks, 2018). Non-integrated LR can result in low muscle tone and potentially affect attention and vision (Wagner, 2015). Failure to integrate PRs can severely affect children's physical, emotional, and cognitive development, underscoring the critical importance of studying and monitoring reflex integration for healthy child development.
The results of this study indicate that CPRIMS achieves acceptable levels of internal consistency, reliability, and validity, demonstrating robust measurement performance. CPRIMS provides researchers with an objective and effective tool for scientifically evaluating primitive reflex integration in children. The development of this scale not only addresses gaps in existing measurement tools but also offers an effective method for identifying potential motor dysfunction, psychological issues, and neurodevelopmental disorders in children.
CPRIMS effectively overcomes the limitations of existing tools. First, the development of this scale enhances the adaptability of primitive reflex assessment tools to the evolving needs of modern society, because as time progresses and society changes, the characteristics and manifestations of unintegrated primitive reflexes may vary throughout the developmental process of children. Second, CPRIMS evaluates specific physical behaviors through direct observation and measurement, rather than assessing primitive reflex integration indirectly through comprehensive developmental information or other observable behaviors. This improves the feasibility and reliability of the assessment while minimizing bias in screening results. Third, CPRIMS follows a rigorous scale development process, incorporating clear validity and reliability indicators. This provides robust support for the credibility of the measurement method, enhancing its scientific rigor and applicability. Fourth, CPRIMS addresses the issue of inconsistent scoring standards by employing clear measurement procedures and standardized scoring systems to evaluate children's primitive reflex integration. This ensures consistency and reproducibility in the measurement and analysis of primitive reflexes, significantly enhancing its utility in both research and clinical contexts. Moreover, it lays a solid foundation for further studies exploring the relationship between developmental disorders and primitive reflexes. Notably, existing assessment tools lack clear age range specifications for their scales. Our scale is specifically developed for children aged 6 to 9 years, a stage that is crucial for both physical and psychological development. Evaluating primitive reflex integration during this period is particularly significant, as it provides valuable insights into children's developmental progress.
The results of this study indicate that CPRIMS achieves acceptable levels of internal consistency, reliability, and validity, demonstrating robust measurement performance. CPRIMS provides researchers with an objective and effective tool for scientifically evaluating primitive reflex integration in children. The development of this scale not only addresses gaps in existing measurement tools but also offers an effective method for identifying potential motor dysfunction, psychological issues, and neurodevelopmental disorders in children.
5.1 Limitations and prospects
This study has certain limitations. Firstly, as a preliminary investigation, the sample is restricted to three elementary schools in a city in China, which presents significant geographical limitations. This may impact the applicability of the scale in other regions and countries. Secondly, although the scale measures seven primitive reflexes closely related to children's physical and psychological development, there are many other important primitive reflexes. For example, the grasp reflex, which is difficult to observe in our sample due to its low elicitation rate, could not be included in the scale.
Future research could expand the survey regions and increase the sample size to facilitate more comprehensive analyses, thereby enriching the content and accuracy of the scale. This would further validate the scale's reliability and validity, and enable the establishment of normative data across diverse populations and age groups. These advancements would significantly enhance the scientific rigor and practical utility of the scale, supporting its broader adoption in both clinical and research applications.
6 Conclusions
CPRIMS is expected to become a powerful tool for assessing the integration status of PRs in children. It can help to identify early signs of developmental issues and provide crucial data support for personalized intervention plans. With further research and refinement, CPRIMS will see widespread use in practice, not only in clinical settings but also in educational and home interventions. Additionally, the widespread application of CPRIMS will promote a deeper understanding and prompt further research into neurodevelopmental disorders in children, further enhancing the efficacy of early diagnosis and intervention.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary material.
Ethics statement
The studies involving humans were approved by the Ethics Committee of Shenyang Sport University, Liaoning Province, China. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
Author contributions
MW: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. JY: Conceptualization, Funding acquisition, Methodology, Resources, Validation, Writing – review & editing. HL: Conceptualization, Methodology, Project administration, Validation, Visualization, Writing – review & editing. CZ: Conceptualization, Investigation, Methodology, Writing – review & editing. YL: Conceptualization, Project administration, Writing – review & editing. XY: Conceptualization, Formal analysis, Methodology, Project administration, Resources, Software, Visualization, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was supported by the National Social Science Fund of China (21BTY096).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2025.1495990/full#supplementary-material
References
Adams, Q., and Craft, J. (2014). Retained primitive reflexes and ADHD: Examining atypical symptomology in the school aged population [masters thesis]. Grand Forks, North Dakota, USA: University of North Dakota UND Scholarly Commons.
Bender, M. L. (1978). The bender-purdue reflex test and training manual. Acad. Ther. 13:322. doi: 10.1177/105345127801300309
Berne, S. A. (2006). The primitive reflexes: considerations in the infant. Optom. Vis. Dev. 37, 139–146.
Bilbilaj, S., Gjipali, A., and Shkurti, F. (2017). Measuring primitive reflexes in children with learning disorders. Eur. J. Multidiscip. Stud. 2, 176–189. doi: 10.26417/ejms.v5i1.p285-298
Blomberg, H. (2015). The rhythmic movement method: A revolutionary approach to improved health and well-being. Lulu.com.
Blythe, S. G. (2002). Reflexes, Learning and Behavior: A Window into the Child's Mind: A Non-invasive Approach to Solving Learning and Behavior Problems. Eugene: Fern Ridge Press. State of Oregon, 10–3.
Blythe, S. G. (2017). Attention, Balance and Coordination: The ABC of Learning Success. Hoboken, NJ: John Wiley and Sons Press, 149–90.
Blythe, S. G. A. (1996). Teacher's Window into the Child's Mind and Papers from the Institute for Neuro-physiological Psychology. A Non-invasive Approach to Solving Learning and Behavior Problems. 1st ed. Fern Ridge Press: State of Oregon. USA, 35–40.
Bob, P., Konicarova, J., and Raboch, J. (2021). Disinhibition of primitive reflexes in attention deficit and hyperactivity disorder: insight into specific mechanisms in girls and boys. Front. Psychiatry 12:430685. doi: 10.3389/fpsyt.2021.430685
Byrne, B. M. (2010). Structural Equation Modeling with AMOS: Basic Concepts, Applications, and Programming (Multivariate Applications Series) 396. New York: Taylor and Francis Group, 7384.
Chinello, A., Di Gangi, V., and Valenza, E. (2018). Persistent primary reflexes affect motor acts: potential implications for autism spectrum disorder. Res. Dev. Disabil. 83, 287–295. doi: 10.1016/j.ridd.2016.07.010
Ebel, R. L., and Frisbie, D. A. (1991). Essentials of Educational Measurement. Englewood, NJ: Prentice Hall Press, 221–33.
Eek, M. N., Olsson, K., Lindh, K., Askljung, B., Påhlman, M., Corneliusson, O., et al. (2018). Intrathecal baclofen in dyskinetic cerebral palsy: effects on function and activity. Dev. Med. Child Neurol. 60, 94–99. doi: 10.1111/dmcn.13625
Feldhacker, D., Cosgrove, R., Feiten, B., Schmidt, K., and Stewart, M. (2021). Relationship between retained primitive reflexes and scholastic performance. Am. J. Occup. Ther. 75:7512505164. doi: 10.5014/ajot.2021.75S2-RP164
Feldhacker, D. R., Cosgrove, R., Feiten, B., Schmidt, K., and Stewart, M. (2022). The correlation between retained primitive reflexes and scholastic performance among early elementary students. J. Occup. Ther. Sch. Early Interv. 15, 288–301. doi: 10.1080/19411243.2021.1959482
Fornell, C., and Larcker, D. F. (1981). Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 18, 39–50. doi: 10.1177/002224378101800104
Futagi, Y., Tagawa, T., and Otani, K. (1992). Primitive reflex profiles in infants: differences based on categories of neurological abnormality. Brain Dev. 14, 294–298. doi: 10.1016/S0387-7604(12)80146-X
Futagi, Y., Toribe, Y., and Suzuki, Y. (2012). The grasp reflex and Moro reflex in infants: hierarchy of primitive reflex responses. Int. J. Pediatr. 2012:191562. doi: 10.1155/2012/191562
Ganotice Jr, F. A., Shen, X., Yuen, J. K. Y., Chow, Y. M. A., Wong, A. M. Y., Chan, K. M. K., et al. (2023). Students' interaction anxiety and social phobia in interprofessional education in Hong Kong: Mapping a new research direction. Ann. Med. 55:2210842. doi: 10.1080/07853890.2023.2210842
Geerlinks, A. (2018). Blomberg Rhythmic Movement Training Canada. (EB/OL). Available at: https://brmtcanada.com (accessed April 5, 2023).
Gieysztor, E., Kowal, M., and Paprocka-Borowicz, M. (2022). Primitive reflex factors influence walking gait in young children: an observational study. Int. J. Environ. Res. Public Health 19:4070. doi: 10.3390/ijerph19074070
Gieysztor, E. Z., Sadowska, L., Choińska, A. M., and Paprocka-Borowicz, M. (2018). Trunk rotation due to persistence of primitive reflexes in early school-age children. Adv. Clin. Exp. Med. 27, 363–366. doi: 10.17219/acem/67458
Grzywniak, C. (2017). Integration exercise programme for children with learning difficulties who have preserved vestigial primitive reflexes. Acta Neuropsychol. 15, 241–256. doi: 10.5604/01.3001.0010.5491
Heblich, B., Terzidis, O., González, M. M., Kuschel, K., Mukadam, M., Birkenbach, M., et al. (2023). Living well: Empirically developed structural equation model for healthy and effective self-regulation. Int. J. Clin. Health Psychol. 23:100375. doi: 10.1016/j.ijchp.2023.100375
Hermann, C. (2012). Primitive reflex retention and its influence on learning behaviour. Int. J. Psychol. 47, 264–265.
Hickey, J., and Feldhacker, D. R. (2022). Primitive reflex retention and attention among preschool children. J. Occup. Ther. Sch. Early Interv. 15, 1–13. doi: 10.1080/19411243.2021.1910606
Hobo, K., Kawase, J., Tamura, F., Groher, M., Kikutani, T., Sunakawa, H., et al. (2014). Effects of the reappearance of primitive reflexes on eating function and prognosis. Geriatr. Gerontol. Int. 14, 190–197. doi: 10.1111/ggi.12078
Iacobucci, D. (2010). Structural equations modeling: Fit indices, sample size, and advanced topics. J. Con. Psychol. 20, 90–98. doi: 10.1016/j.jcps.2009.09.003
Iani, L., Lauriola, M., and Costantini, M. A. (2014). confirmatory bifactor analysis of the hospital anxiety and depression scale in an Italian community sample. Health Qual. Life Outc. 12:84. doi: 10.1186/1477-7525-12-84
Kline, R. B. (2011). Principles and Practice of Structural Equation Modeling. New York: Guilford Press, 40–3.
Konicarova, J., and Bob, P. (2012). Retained primitive reflexes and ADHD in children. Act. Nerv. Super. 54, 135–138. doi: 10.1007/BF03379591
Konicarova, J., and Bob, P. (2013). Asymmetric tonic neck reflex and symptoms of attention deficit and hyperactivity disorder in children. Int. J. Neurosci. 123, 766–769. doi: 10.3109/00207454.2013.801471
Konicarova, J., Bob, P., and Raboch, J. (2013). Persisting primitive reflexes in medication-naïve girls with attention-deficit and hyperactivity disorder. Neuropsychiatr. Dis. Treat. 9, 1457–1461. doi: 10.2147/NDT.S49343
Kyllerman, M., Bager, B., Bensch, J., Bille, B., Olow, I., Voss, H., et al. (1982). Dyskinetic cerebral palsy: I. clinical categories, associated neurological abnormalities and incidences. Acta Paediatr. Scand. 71, 543–550. doi: 10.1111/j.1651-2227.1982.tb09472.x
Lan, J., Zhou, Q., Zhang, X., Xiong, L., Xu, Y., Yu, T., et al. (2023). Construction and reliability and validity testing of the nurse infection control implementation scale. Chongqing Med. 15, 2272–2276.
Lance, C. E., Butts, M. M., and Michels, L. C. (2006). The sources of four commonly reported cutoff criteria: what did they really say? Organ. Res. Methods 9, 202–220. doi: 10.1177/1094428105284919
Melillo, R., Leisman, G., Mualem, R., Ornai, A., and Carmeli, E. (2020). Persistent childhood primitive reflex reduction effects on cognitive, sensorimotor, and academic performance in ADHD. Front. Public Health 8:431835. doi: 10.3389/fpubh.2020.431835
Morrison, D. C. (1985). Neurobehavioral and Perceptual Dysfunction in Learning Disabled Children. Ann Arbor, MI: University of Michigan Press, 159–70.
Pecuch, A., Gieysztor, E., Telenga, M., Wolańska, E., Kowal, M., Paprocka-Borowicz, M., et al. (2020). Primitive reflex activity in relation to the sensory profile in healthy preschool children. Int. J. Environ. Res. Public Health 17:8210. doi: 10.3390/ijerph17218210
Quevedo, K., Johnson, A. E., Loman, M. M., Lafavor, T., Moua, B., Gunnar, M. R., et al. (2015). The impact of early neglect on defensive and appetitive physiology during the pubertal transition: a study of startle and postauricular reflexes. Dev. Psychobiol. 57, 289–304. doi: 10.1002/dev.21283
Taylor, M., Houghton, S., and Chapman, E. (2004). Primitive reflexes and attention-deficit/hyperactivity disorder: developmental origins of classroom dysfunction. Int. J. Spec. Educ. 19, 23–37.
Tobón, S., and Luna-Nemecio, J. (2021). Complex thinking and sustainable social development: validity and reliability of the complex-21 scale. Sustainability 13:6591. doi: 10.3390/su13126591
Tsai, T. H., Chang, H. T., Chang, Y. C., and Chang, Y. S. (2017). Personality disclosure on social network sites: An empirical examination of differences in Facebook usage behavior, profile contents and privacy settings. Comput. Hum. Behav. 76, 469–482. doi: 10.1016/j.chb.2017.08.003
Tuysuzoglu, H., Atesci, F. C., Ozdel, O., and Oguzhanoglu, N. K. (2011). Neurological soft signs in bipolar disorder: the impact of comorbid attention deficit hyperactivity disorder/Iki uclu bozuklukta silik norolojik belirtiler: Dikkat eksikligi hiperaktivite bozuklugu estanisinin etkisi. Arch. Neurol. Psychiatry 48, 107–114. doi: 10.4274/npa.y5655
Wagner, K. (2015). Blomberg Rhythmic Movement Training. (EB/OL). Available at: https://www.brmtusa.com (accessed April 5, 2023).
Wang, M., Yu, J., Kim, H. D., and Cruz, A. B. (2023). Attention deficit hyperactivity disorder is associated with asymmetric tonic neck primitive reflexes: a systematic review and meta-analysis. Front. Psychiatry 14:1175974. doi: 10.3389/fpsyt.2023.1175974
Wang, T., Wang, D., and Liu, Z. (2022). Feedback-seeking from team members increases employee creativity: the roles of thriving at work and mindfulness. Asia Pac. J. Manag. 39, 1321–1340. doi: 10.1007/s10490-021-09768-8
Wei, Z., and Nguyen, Q. T. K. (2020). Local responsiveness strategy of foreign subsidiaries of Chinese multinationals: the impacts of relational-assets, market-seeking FDI, and host country institutional environments. Asia Pac. J. Manag. 37, 661–692. doi: 10.1007/s10490-019-09655-3
Wu, M. (2010). Practical Statistical Analysis of Questionnaires: SPSS Operations and Applications. Chongqing, China: Chongqing University Press, 158–72.
Xue, Y., Xue, B., Zheng, X., Shi, L., Liang, P., Xiao, S., et al. (2023). Associations between internet addiction and psychological problems among adolescents: description and possible explanations. Front. Psychol. 14:1097331. doi: 10.3389/fpsyg.2023.1097331
Yang, X. Y. (2024). An experimental study of the effect of primitive reflex integration therapy on sustained attention in children with ADHD-prone [masters thesis]. Shen Yang. China: Shenyang Normal University.
Yu, M., Lin, H., Wang, G. G., Liu, Y., and Zheng, X. (2022). Is too much as bad as too little? The S-curve relationship between corporate philanthropy and employee performance. Asia Pac. J. Manag. 39, 1511–1534. doi: 10.1007/s10490-021-09775-9
Zafeiriou, D. I. (2000). Plantar grasp reflex in high-risk infants during the first year of life. Pediatr. Neurol. 22, 75–76. doi: 10.1016/S0887-8994(99)00110-1
Zafeiriou, D. I., Tsikoulas, I. G., and Kremenopoulos, G. M. (1995). Prospective follow-up of primitive reflex profiles in high-risk infants: clues to an early diagnosis of cerebral palsy. Pediatr. Neurol. 13, 148–152. doi: 10.1016/0887-8994(95)00143-4
Zafeiriou, D. I., Tsikoulas, I. G., Kremenopoulos, G. M., and Kontopoulos, E. E. (1999a). Plantar response profile of high-risk infants at one year of life. J. Child Neurol. 14, 514–517. doi: 10.1177/088307389901400806
Zafeiriou, D. I., Tsikoulas, I. G., Kremenopoulos, G. M., and Kontopoulos, E. E. (1999b). Moro reflex profile in high-risk infants at the first year of life. Brain Dev. 21, 216–217.
Keywords: primitive reflexes, children, motor function disorder, cognitive psychology, neurodevelopmental disorder
Citation: Wang M, Yu J, Li H, Zhao C, Li Y and Yang X (2025) Development of the children's primitive reflex integration assessment scale. Front. Psychol. 16:1495990. doi: 10.3389/fpsyg.2025.1495990
Received: 16 September 2024; Accepted: 02 January 2025;
Published: 22 January 2025.
Edited by:
Gao-Xia Wei, Chinese Academy of Sciences (CAS), ChinaReviewed by:
Chi Lizhong, Beijing Sport University, ChinaYingying Wang, Shanghai University of Sport, China
Copyright © 2025 Wang, Yu, Li, Zhao, Li and Yang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jing Yu, eXVqaW5nOTg4M0BnbWFpbC5jb20=; Xinyue Yang, Y3ludGhpYXlvbzMzQGdtYWlsLmNvbQ==