
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol., 06 March 2025
Sec. Cultural Psychology
Volume 16 - 2025 | https://doi.org/10.3389/fpsyg.2025.1422900
 Elisabeth Dromer1,2*
Elisabeth Dromer1,2* Grace Jacob1,2
Grace Jacob1,2 Monnica T. Williams1,3
Monnica T. Williams1,3 Seyed Mohammad Mahdi Moshirian Farahi3
Seyed Mohammad Mahdi Moshirian Farahi3 Wina Darius1,2
Wina Darius1,2 Cary Samuel Kogan1,2
Cary Samuel Kogan1,2 Jude Mary Cénat1,2*
Jude Mary Cénat1,2*Background: Data from the United States showed that Black individuals face unique issues related to obsessive-compulsive disorder (OCD). However, Canadian research on OCD among Black individuals remains very limited. The present study aims to document obsessive-compulsive (OC) symptoms and related risk and protective factors in Black individuals aged 15 to 40 years old in Canada.
Methods: A total of 860 Black individuals (75.6% female) aged 15–40 years were recruited as part of the Black Community Mental Health in Canada (BcoMHealth) project. Independent t-tests, ANOVA, and multivariable linear regressions were used to assess OC symptom severity and identify risk and protective factors.
Results: Black individuals presented high levels of OC symptoms. Results showed that Black individuals born in Canada experienced more OC symptoms compared to those born abroad. Results also showed that there were no differences between Black women, Black men, and those who identified their sex as “other.” Everyday discrimination, internalized racism, and microaggressions positively predicted OC symptoms, while social support negatively predicted OC symptoms.
Limitations: Limitations of this study include its cross-sectional nature, which prevents us from establishing causal links, not assessing for the clinical diagnosis of OCD, and using self-report measures. Results support that different forms of racial discrimination contribute to the development and severity of OC symptoms in Black individuals in Canada. Social support may play a protective role for those individuals. These factors must be considered in future research and in the assessment and treatment of Black individuals with OCD.
Obsessive-compulsive disorder (OCD) is a potentially debilitating condition that impacts the individuals who suffer from it as well as those close to them. OCD can vary in its presentation. In fact, people from differing ethnic groups appear to vary in their symptomology. In particular, Black individuals in the United States (US) may be more likely to engage, among others, in double checking (a common OCD symptom), which has been attributed to this group’s unique experience of anti-Black racism both presently and historically (Williams et al., 2017c). However, little is known of this disorder in Canada, especially in Black individuals. There is a need to address this knowledge gap in order to better understand the unique aspects of their experiences, so as to better tailor treatment to this group.
OCD is a disorder characterized by the presence of time-consuming and distressing obsessions (unwanted and recurrent thoughts) and/or compulsions (repetitive behaviors or mental acts used to manage obsessions) (American Psychiatric Association, 2013; World Health Organization, 2019). Worldwide, its prevalence is estimated to be 1.5% in women and 1.0% in men (Fawcett et al., 2020). Research on its prevalence in Canada is scarce. Data from the 2012 Canadian Community Health Survey—Mental Health showed the lifetime prevalence of OCD to be 0.93% (95% CI 0.75–1.11) for Canadians over the age of 15 (Osland et al., 2018). Additionally, Canadian prevalence data on OCD is limited in that it does not disaggregate by race or ethnicity—a color-blind approach very common in Canadian health research (Fante-Coleman and Jackson-Best, 2020; Fryberg and Stephens, 2010).
The majority of research on OCD has been conducted in populations from the US. However, until less than two decades ago, these studies did not investigate OCD within Black populations (Williams et al., 2010). The first comprehensive study of OCD among African Americans and Black Caribbeans found 12-month and lifetime rates of OCD among them of 1.63 and 1.49% respectively, suggesting similar prevalence rates to the general population (Himle et al., 2008). There is also a dearth of data on risk and protective factors for OCD in Black individuals. Sociocultural risk factors for OCD in African American children and youth identified, to date, include low income and perceived racism, while identified protective factors include items such as social support and religious coping (Williams and Jahn, 2016). Other studies by Williams and colleagues also found that everyday racial discrimination (but not non-racial discrimination) was positively associated with OCD obsessions (Williams et al., 2021; Williams et al., 2017c). Hence, while research on OCD in Black populations is limited, the current data show a prevalence in Black communities similar to that found in the general population and suggest important links between OCD and racial discrimination.
The connection between racial discrimination and OC symptoms was revealed by multiple studies conducted in the US by Williams and other researchers during the last decade (Williams and Jahn, 2016; Williams et al., 2017c; Wilson and Thayer, 2020). These studies revealed that Black individuals who experience racial discrimination are more likely to experience OC symptoms. Indeed, it is well known that experiencing racial discrimination is related to an increase in stress, which in turn leads to deleterious effects on the health of individuals (Cénat, 2022). Concretely, higher levels of experienced racial discrimination result in a worsening of many pre-existing mental health conditions, such as OCD (Lewis and Neville, 2015; Williams et al., 2017c). However, beyond a general stress process model, unwanted obsessions and unwanted compulsions can also be a function of the nature of racism. For example, anti-Black racism can take the form of assumptions of intellectual inferiority, which may be operationalized as excessive criticism for minor mistakes towards Black individuals. In turn, to prevent negative judgment, Black individuals may engage in excessive double-checking, a common OCD compulsion (Williams et al., 2017c). Thus, racial discrimination may be indirectly associated with OCD because of its inherent stressful nature, and it may also directly impact OCD and the nature of Black individuals’ obsessions and compulsions.
Very rarely will people who enact racism admit they are acting out of racial animus. Hence, when people experience racism, it is common for targets to believe they are being mistreated due to negative qualities about themselves (Williams et al., 2020). Therefore, lacking an explanation for being treated worse than others, many Black people start to believe they are defective in some way and may adopt negative stereotypes about their racial group. This is called internalized racism and is connected to numerous negative mental health outcomes (Cénat et al., 2022; Haeny et al., 2021; Kogan et al., 2022). Internalized racism has never been studied in connection with OCD, but one might predict that, like other forms of racism, it is a risk factor for OCD.
Although symptoms of OCD in Black Canadians may be comparable the general population, there are distinct factors that affect OCD among Black people. Thus, this study aims to inform our understanding of OCD in Black Canadians by: (1) assessing their self-reported obsessive-compulsive (OC) symptoms and (2) examining possible risk and protective factors associated with OC symptoms in this population.
A total of 860 Black individuals (75.6% female) aged 15–40 years (M = 24.96 years, SD = 6.29) and living in Canada were recruited as part of the Black Community Mental Health in Canada (BcoMHealth) project. Descriptive statistics are reported in Table 1. Details on the recruitment methods used in this study and more in-depth descriptions of the sample can be found in previous publications (Cénat et al., 2021a; Cénat et al., 2021b). Upon giving consent, participants completed the online survey on Qualtrics™ (Provo, USA), where they filled out a number of questionnaires, including the ones presented in this study. Respondents received compensation either through a course credit, or a $15 e-gift card, depending on the situation. Ethical approval was obtained from the University of Ottawa and Université du Québec en Outaouais research ethics boards.
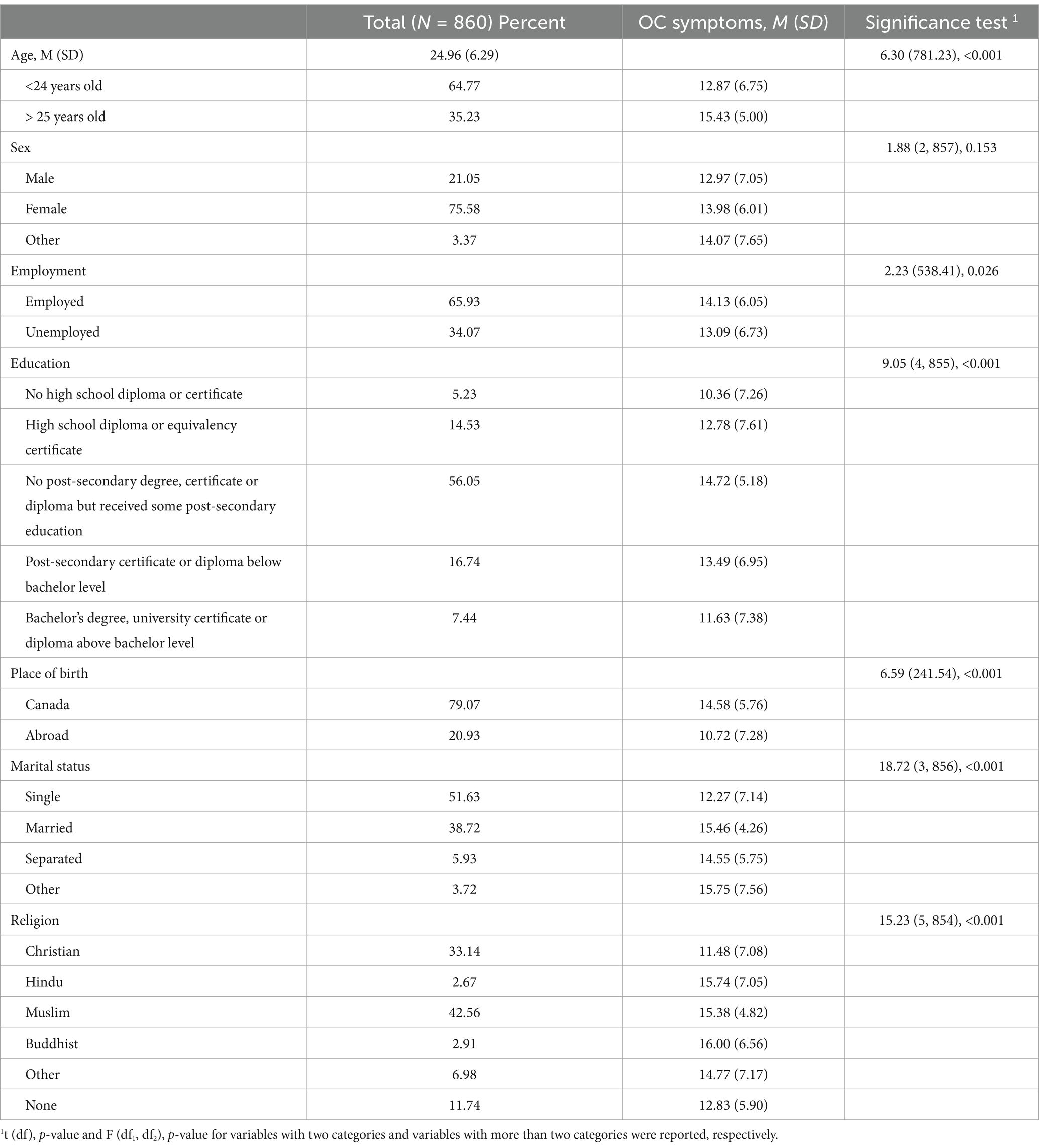
Table 1. Sample characteristics and OC symptoms.
This questionnaire was used to assess sociodemographic information (e.g., gender, education level, marital status, place of birth, religion, etc.).
This questionnaire consists of 5 items assessing the perceived sources of racial discrimination that individuals face and the extent to which they are present in the respondent’s life (Williams et al., 1997). For example, one item is “because of your skin colour: you are treated with less courtesy.” This scale is rated on a 6-point scale ranging from “Almost every day” to “Never.” A high score indicates that there is a high incidence of perceived racial discrimination. Cronbach’s alpha: 0.90.
This questionnaire contains 12 items that assess the extent to which an individual agrees with certain stereotypical statements related to their ethnic group and race (e.g., straight hair is better than my natural hair texture) (Molina and James, 2016). This scale is scored on a 4-point scale ranging from “Very true” to “Not true at all.” It has no formal scoring, but a high score indicates a greater prevalence of internalized racism. The following items must be reverse scored: 1 and 3. The Cronbach’s alpha of our sample was 0.78.
This questionnaire is composed of 14 items assessing the experiences of racial microaggressions (i.e., microinsults, microassaults) among Black individuals (Mercer et al., 2011). For example, one item includes “Someone told me that I am not like other people of my racial/ethnic background.” This scale is rated on a 5-point scale ranging from “This has never happened to me” to “This event happened to me and I was extremely upset.” A high score indicates that the incidence of racial microaggressions is high. Cronbach’s alpha in the present sample was 0.86.
This questionnaire consists of 12 items evaluating the sources of social support of an individual, which are divided into three groups: friends (items 6, 7, 9, and 12), significant other (items 1, 2, 5, and 10) and family (items 3, 4, 8, and 11) (Zimet et al., 1988). An example item is “I can count on my friends when things go wrong.” This scale is scored on a 6-point scale from “Very Strongly Disagree,” to “Very Strongly Agree.” The Cronbach’s alpha coefficients were of 0.85 for friends, 0.91 for significant other, and 0.87 for family (total reliability score of 0.88) (Zimet et al., 1988). The Cronbach’s alpha in our sample was 0.90.
This questionnaire contains 10 self-rated items assessing the severity of obsessions and compulsions (Goodman et al., 1989). For example, one item is “How much of your time is occupied by obsessive thoughts.” This scale is rated on a 5-point scale, and ranges from 0 (no symptoms) to 4 (severe symptoms), and participants can receive a score between 0 and 40. A higher score represents more severe symptoms of obsessions and compulsions (Goodman et al., 1989; Steketee et al., 1996). More precisely a total score between 0 and 7 indicates subclinical levels of symptoms, 8–15 mild symptoms, 16–23 moderate symptoms, 24–31 severe symptoms, 32–40 extreme symptoms (Wootton and Tolin, 2016). The Cronbach’s alpha of our sample was 0.87.
To compare means of OC symptoms between the sociodemographic characteristics of the sample, we used independent t-tests (for the variables with two categories) and one-way ANOVAs (for the variables with more than two categories). A series of pairwise comparisons using Tukey’s test were performed. Bivariate correlations between continuous variables were tested using Pearson’s r correlations (Table 2). Following this, hierarchical multiple linear regressions were conducted with three models to see what variables significantly predicted OC symptoms. Model 1 included sociodemographic variables. In Model 2, variables related to the experience of racial discrimination were added. In Model 3, social support was included. Standardized scores of the continuous variables were used for the regression analysis. Categorical variables included age, sex, education, marital status, employment status, place of birth, and religion. Age was also included in the regression analysis as a continuous variable. The multicollinearity assumption was checked using the variance inflation factor (VIF). We only included sociodemographic variables which were significant in the preliminary multiple regression analysis (see Supplementary Table S1 for other variables). All statistical analyses were performed using SPSS 28 and Stata/SE 16.1.
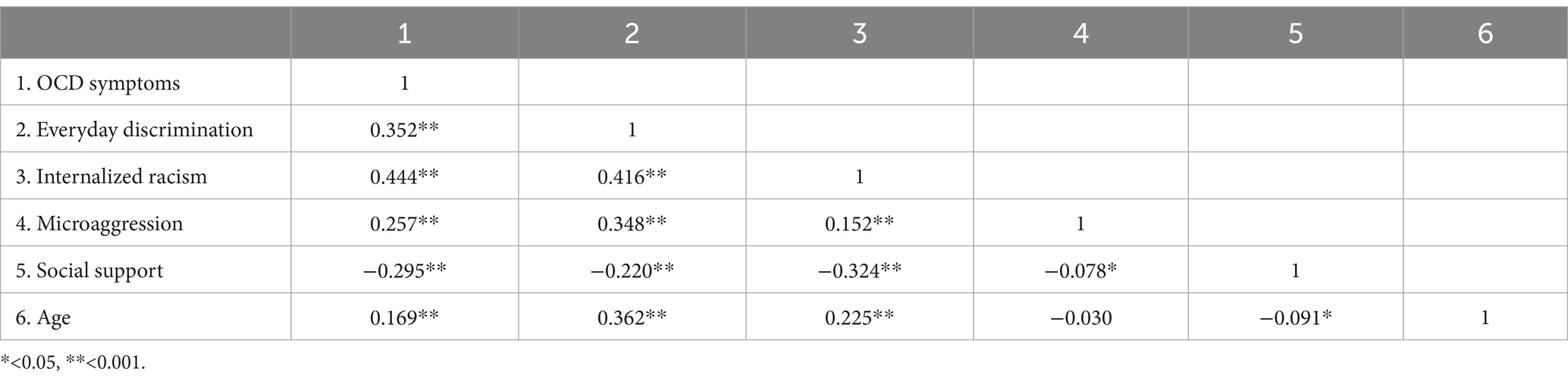
Table 2. Zero-order correlations.
ANOVAs and t-test results are displayed in Table 1. Participants reported, on average, mild levels of OC symptoms (Total Y-BOCS score: M = 13.77, SD = 6.31). Results of the t-tests showed that mean OC score was significantly higher in participants who were born in Canada (M = 14.58, SD = 5.76) comparatively to those who were born abroad (M = 10.72, SD = 7.28), t (241.54) = 6.59, p < 0.001. Similar results were found for those who were employed (M = 14.13, SD = 6.05) compared to those who were unemployed (M = 13.09, SD = 6.73), t (538.41) = 2.23, p = 0.026. In addition, results showed that those aged 25 years old and more (M = 15.43, SD = 5.00) were more likely to experience OC symptoms compared to those aged 24 years old and less (M = 12.87, SD = 6.75), t (781.23) = 6.30, p < 0.001.
ANOVAs demonstrated significant differences among the different marital status (F (3, 856) = 18.72, p < 0.001), religions (F (5, 854) = 15.23, p < 0.001), and education level (F (4. 855) = 9.05, p < 0.001) of participants. Pairwise comparisons showed that married participants (M = 15.46, SD = 4.26) had a higher mean OC symptom score than single participants (M = 12.27, SD = 7.14). Moreover, single participants (M = 12.27, SD = 7.14) had a lower mean OC symptom score than participants who had “other” marital status (M = 15.75, SD = 7.56). Christians (M = 11.48, SD = 7.08) had lower mean OC symptoms compared to Muslims (M = 15.38, SD = 4.82), Buddhist (M = 16.00, SD = 6.56), Hindu (M = 15.74, SD = 7.05), and “other” religions (M = 14.77, SD = 7.17), p Christian-Muslim < 0.001; p Christian-Buddhist = 0.005; p Christian-Hindu = 0.016; p Christian-Other = 0.002. Furthermore, Muslims (M = 15.38, SD = 4.82) had a significantly higher mean OC symptom score than participants with no religion (M = 12.83, SD = 5.90). Results also showed that participants with no high school education (M = 10.36, SD = 7.26) had a lower mean OC symptom score than participants with an incomplete post-secondary degree (M = 14.72, SD = 5.18; p < 0.001) and those with a post-secondary degree (M = 13.49, SD = 5.95; p = 0.026). Participants with a high school degree (M = 12.78, SD = 7.61) had a lower mean OC symptom score than participants with an incomplete post-secondary degree (M = 14.72, SD = 5.18; p = 0.016). Participants with an incomplete post-secondary degree (M = 14.72, SD = 5.18) had a higher mean OC symptom score than participants with a bachelor’s degree/university certificate (M = 11.63, SD = 7.38; p = 0.002). No mean differences between sex groups were found, F (2, 857) = 1.88, p = 0.153.
Predictors of Model 1 (see Table 3) accounted for 8.7% of the variance. After adding everyday racial discrimination, internalized racism, and racial microaggressions to the model, R2 increased by 16.7% to a total of 25.4% of variance explained, suggesting a notable contribution of these three predictors to the model. After adding social support to the model, the R2 increased by 2.0%. In total, the predictors in the final model accounted for 27.4% of the variance. The results of the final model showed that experience of everyday discrimination (B = 0.63, p = 0.006), degree of internalized racism (B = 1.76, p < 0.001), and racial microaggressions (B = 1.05, p < 0.001) were positively associated with OC symptoms. Results also revealed that increased social support scores were negatively associated with OC symptoms (B = −0.96, p < 0.001). Age as a continuous variable was not a significant predictor of OC symptoms, despite the group differences observed when grouping participants in the two age categories (24 and under, and 25 and over).
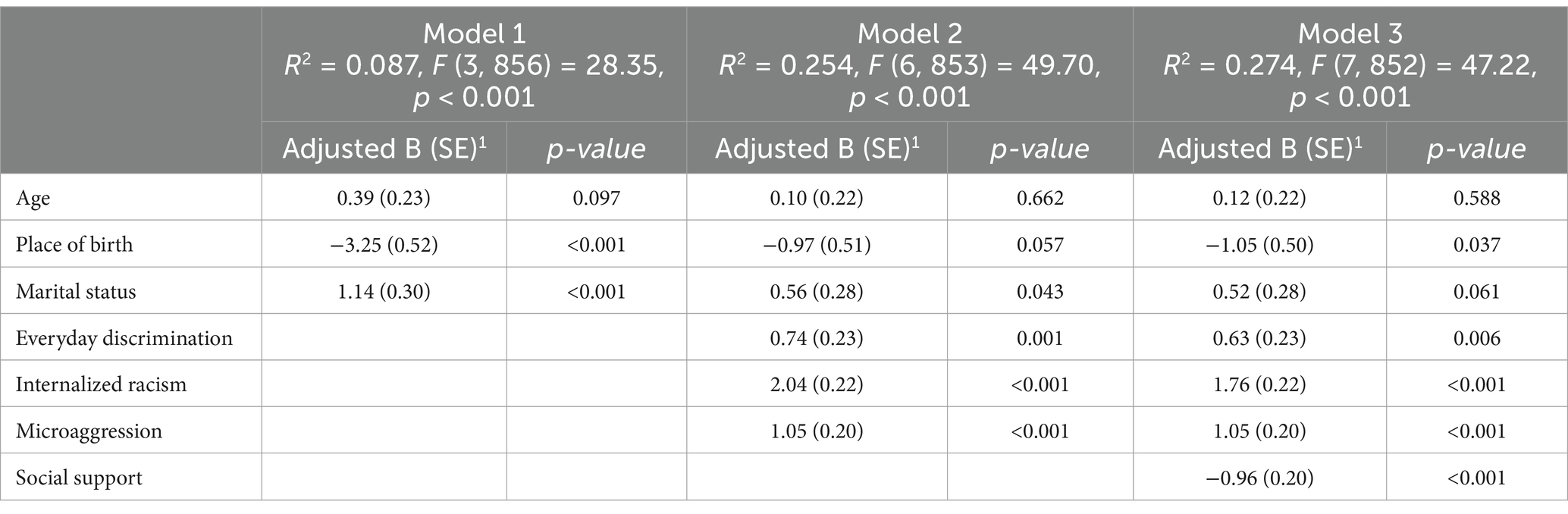
Table 3. Hierarchical Multiple Regressions Results for OC Symptoms and Various Sociodemographic Variables.
As the first Canadian study to explore OCD in Black communities in Canada, the present work provides new insights on risk and protective factors of OC symptoms in Black individuals.
There were some notable differences in symptom severity between various social groups. First, age was positively correlated with OC symptoms. Indeed, when categorized into two groups, individuals 25 years old and older had higher mean OC symptom scores than those 24-year-old and younger. These results make sense since participants in the sample are young. Indeed, in the US, Black individuals have a later identified age of onset for OCD (Himle et al., 2008), which could be due to barriers to diagnosis and treatment (Williams et al., 2012). Another reason discussed by Williams et al. (2017a,b,c) is that there are greater mortality rates among individuals with OCD than for those without the disorder. In addition, a study in Denmark found that individuals with OCD have a significantly higher mortality rate from natural and unnatural causes (Meier et al., 2016). Finally, being a part of a marginalized ethnic group could have an impact and increased the rate of OC symptoms among 25 years old and older Black individuals due to barriers accessing early interventions and effective treatment (Williams et al., 2017b).
OC symptoms were higher among Canadian-born individuals compared to those coming from abroad. In Canada, one in four Black person is born in the country (Domey and Patsiurko, 2024). Research has shown that when immigrants arrive to Canada, they are in better health than Canadian-born individuals (Beiser, 2005). This is known as the healthy immigrant effect. However, their health declines as they spend more time in their new country (Elshahat et al., 2022; Ng, 2011). Selection effects can also have an impact on the selection of immigrants who are healthier into Canada. Indeed, health screenings by host countries ensure that the healthiest citizens are selected for immigration (Kennedy et al., 2015), leaving “unhealthy” migrants in their country unable to immigrate. These phenomena could explain the presence of lower OC symptoms found in this study among Black individuals not born in Canada.
OC symptoms were higher among certain religious groups. Notably, Muslims had higher symptoms than Christians. This may be due to the cultural practices of the religions. As described in Yorulmaz et al. (2009), there are predetermined behavioural requirements in Islam, as this is a ritualistic religion. There rituals place an emphasis on purity, cleanliness, and prayers. These features of the religion could contribute to presence of OC symptoms and, when done to the extreme, can resemble OCD (Yorulmaz et al., 2010).
Finally, individuals with some post-secondary education and those with a post-secondary certificate had more OC symptoms compared to individuals with less or more education. While previous research has highlighted the negative impact of OCD on educational attainment in Black individuals (Himle et al., 2012; Williams et al., 2017b)—wherein individuals with OCD are less likely to receive a high level of education because of the impact of their symptoms—the contrary is not a common finding of the literature on OCD. Indeed, the sample in this study showed that those with an incomplete high school diploma had the lowest OC symptom score. This finding could be explained by the low age of our sample: many individuals may have simply not completed high school yet. In addition, individuals who have not completed high school represent only a small percentage of the sample in this study. Hence, results from such a small sample size should be interpreted with caution.
This study shows that everyday racial discrimination and microaggressions are predictors of obsessive-compulsive symptoms, which is consistent with US work reporting a significant association between OCD symptoms and racism (Williams et al., 2017c). Studies have hypothesized that the psychological resources necessary to deal with experiences of racial discrimination can diminish the resources available to manage other stressors, in this case, obsessions and/or compulsions. This, in turn, may lead to an increase in OC symptoms (Soto et al., 2011; Williams et al., 2017c). In addition, distress caused by racial discrimination was found to be a bigger predictor of OC symptoms than the frequency of this discrimination. Everyday racial discrimination is associated with serious psychological distress among African Americans (Chae et al., 2011). Hence, the distress associated with experiences of racial discrimination could also deplete the psychological resources that are available for Black individuals, which in turn could also lead to increased OC symptoms. Experiences of racial discrimination thus impact OCD in two ways that both lead to depleted resources and ultimately increased OC symptoms: individuals have to deal directly with the experiences of racial discrimination and have to deal with the psychological distress caused by these experiences.
Interestingly, internalized racism was the largest predictor of OC symptoms in Black Canadians in this study. This is the first time this construct has been measured in the context of OC symptoms, making this finding particularly notable. Internalized racism is linked to an array of negative mental health outcomes, such as increased anxiety and shame (Graham et al., 2016; Speight, 2007). Both have also been associated with OCD (Stein et al., 2010; Szentágotai-Tătar et al., 2020; Visvalingam et al., 2022). Hence, individuals with higher levels of internalized racism may experience more shame and/or anxiety. This could lead to more negative self-talk and more anxious thoughts, which in turn could lead to increased OC symptoms, and explain the relationship between internalized racism and OCD. More research on the link between OCD and internalized racism is needed.
Williams and Jahn (2016) theorized that social support was a protective factor for Black people in terms of the development of OCD. Correspondingly, we found that social support was negatively correlated with OC symptoms in our sample. Previous research on OCD and its relation to family relationships in Black Americans has highlighted the negative impact of OCD on family relationships and the impact of negative family interactions on family relationships (Himle et al., 2017). Hence, we theorize that individuals who report high levels of social support are experiencing the opposite phenomenon, wherein experiencing positive social interactions and support helps them deal with obsessions and compulsions in a way that reduces OC symptoms. For example, if instead of being criticized for their compulsions, individuals are met with kindness and understanding, they may experience fewer of them. This theory has been highlighted in previous work on OCD and social support in the general population (Palardy et al., 2018).
Some limitations should be considered. First, due to the cross-sectional nature of the study, causal links between OC symptoms and other variables, such as internalized racism, cannot be established. In addition, not assessing for the clinical diagnosis of OCD directly prevents us from establishing the prevalence of OCD in Black communities in Canada—which has yet to be done and is needed. Similarly, not collecting information concerning the nature of the obsessions and compulsions also limits our ability to paint a full portrait of OCD in Black individuals in Canada. Not assessing the participants’ use of psychopharmacological treatments also limits the generalizability of our findings. It is information that could be asked to be sure that those who declared fewer symptoms of OCD do not receive medication to manage them. Finally, using self-report measures may have limited the accuracy of the information obtained.
The results of this research help to highlight future avenues for research. First, future studies should investigate the prevalence of OCD symptoms and diagnoses in Black individuals in Canada. These studies should also explore the differences between Black Canadians with OCD and their White and other racialized counterparts. Studies should specifically investigate the experiences related to the types of symptoms (obsessions and compulsions) and how they impact the daily life of Black Canadians compared to other racial and ethnic groups. Second, future studies with longitudinal design should continue to examine the role of different forms of racial discrimination as risk factors for OCD and related symptoms. Internalized racism—as one of the most pervasive and damaging consequences of racial microaggressions and individual, institutional, and systemic racism—should especially be included in such work. Longitudinal studies are needed to better understand the mechanisms underlying the links between internalized racism, other forms of racism, and OC symptoms to find ways to mitigate their impact on OCD. Third, further research is needed on protective factors related to OCD in Black individuals to understand the mechanisms through which these factors lead to lower levels of OC symptoms. Such research is crucial for both OCD prevention and intervention, and to build resilience in Black communities and other ethnic and racial groups.
This study highlights a number of risk and protective factors of OC symptoms in Black individuals in Canada. These include place of birth, employment status, marital status, religious affiliation, and education. Additionally, everyday racial discrimination and internalized racism seem to be particularly important predictors of OC symptoms in Black people living in Canada. These findings should inform future research and treatment of OCD among Black people in Canada. They also highlight the importance of exploring the impact of racism, and more specifically everyday racial discrimination, on psychological symptoms, which is consistent with studies published on depression and anxiety (Cénat et al., 2021b; Kogan et al., 2022). Although cross-sectional, these findings should inform future studies on the evaluation and treatment of OCD among Black individuals in Canada. This is necessary so that assessment and treatment of OCD can be provided to Black individuals in a culturally appropriate and anti-racist manner (Cénat, 2020; Cénat et al., 2024).
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by University of Ottawa and Université du Québec en Outaouais. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
ED: Conceptualization, Writing – original draft, Writing – review & editing. GJ: Conceptualization, Writing – original draft, Writing – review & editing. MW: Conceptualization, Writing – review & editing. SM: Formal Analysis, Writing – original draft, Writing – review & editing. WD: Writing – original draft, Writing – review & editing. CK: Writing – review & editing. JMC: Conceptualization, Methodology, Project administration, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was supported by the Public Health Agency of Canada (grant number 1920-HQ-000053), the Social Sciences and Humanities Research Council (SSHRC) and Canadian Institutes of Health Research (CIHR) (grant number 469050).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2025.1422900/full#supplementary-material
American Psychiatric Association (2013). Diagnostic and statistical manual of mental disorders: DSM-5. 5th Edn: American Psychiatric Association.
Beiser, M. (2005). The health of immigrants and refugees in Canada. Can. J. Public Health 96, S30–S44. doi: 10.1007/BF03403701
Cénat, J. M. (2020). How to provide anti-racist mental health care. Lancet Psychiatry 7, 929–931. doi: 10.1016/S2215-0366(20)30309-6
Cénat, J. M. (2022). Complex racial trauma: evidence, theory, assessment, and treatment. Perspect. Psychol. Sci. 18, 675–687. doi: 10.1177/17456916221120428
Cénat, J. M., Dalexis, R. D., Darius, W. P., Kogan, C. S., and Guerrier, M. (2022). Prevalence of current PTSD symptoms among a sample of black individuals aged 15 to 40 in Canada: the major role of everyday racial discrimination, racial microaggresions, and internalized racism. Can. J. Psychiatr. 68, 178–186. doi: 10.1177/07067437221128462
Cénat, J. M., Hajizadeh, S., Dalexis, R. D., Ndengeyingoma, A., Guerrier, M., and Kogan, C. (2021a). Prevalence and effects of daily and major experiences of racial discrimination and microaggressions among black individuals in Canada. J. Interpers. Violence 37, NP16750–NP16778. doi: 10.1177/08862605211023493
Cénat, J. M., Haeny, A. M., and Williams, M. T. (2024). Providing antiracist cognitive-behavioral therapy: Guidelines, tools, and tips. Psychiatry Research 339, 116054. doi: 10.1016/j.psychres.2024.116054
Cénat, J. M., Kogan, C., Noorishad, P. G., Hajizadeh, S., Dalexis, R. D., Ndengeyingoma, A., et al. (2021b). Prevalence and correlates of depression among black individuals in Canada: the major role of everyday racial discrimination. Depress. Anxiety 38, 886–895. doi: 10.1002/DA.23158
Chae, D. H., Lincoln, K. D., and Jackson, J. S. (2011). Discrimination, attribution, and racial group identification: implications for psychological distress among black Americans in the National Survey of American life (2001–2003). Am. J. Orthopsychiatry 81, 498–506. doi: 10.1111/j.1939-0025.2011.01122.x
Domey, N., and Patsiurko, N. (2024). The diversity of the black populations in Canada, 2021: a sociodemographic portrait. Available at: https://www150.statcan.gc.ca/n1/pub/89-657-x/89-657-x2024005-eng.htm
Elshahat, S., Moffat, T., and Newbold, K. B. (2022). Understanding the healthy immigrant effect in the context of mental health challenges: a systematic critical review. J. Immigr. Minor. Health 24, 1564–1579. doi: 10.1007/s10903-021-01313-5
Fante-Coleman, T., and Jackson-Best, F. (2020). Barriers and facilitators to accessing mental healthcare in Canada for black youth: a scoping review. Adolesc. Res. Rev. 5, 115–136. doi: 10.1007/s40894-020-00133-2
Fawcett, E. J., Power, H., and Fawcett, J. M. (2020). Women are at greater risk of OCD than men: a meta-analytic review of OCD prevalence worldwide. J. Clin. Psychiatry 81:13075. doi: 10.4088/JCP.19r13085
Fryberg, S. A., and Stephens, N. M. (2010). When the world is colorblind, American Indians are invisible: a diversity science approach. Psychol. Inq. 21, 115–119. doi: 10.1080/1047840X.2010.483847
Goodman, W. K., Price, L. H., Rasmussen, S. A., Mazure, C., Fleischmann, R. L., Hill, C. L., et al. (1989). The Yale-Brown obsessive compulsive scale: I. Development, use, and reliability. Arch. Gen. Psychiatry 46, 1006–1011. doi: 10.1001/archpsyc.1989.01810110048007
Graham, J. R., West, L. M., Martinez, J., and Roemer, L. (2016). The mediating role of internalized racism in the relationship between racist experiences and anxiety symptoms in a black American sample. Cult. Divers. Ethn. Minor. Psychol. 22, 369–376. doi: 10.1037/cdp0000073
Haeny, A. M., Holmes, S. C., and Williams, M. T. (2021). The need for shared nomenclature on racism and related terminology in psychology. Perspect. Psychol. Sci. 16, 886–892. doi: 10.1177/17456916211000760
Himle, J. A., Muroff, J. R., Taylor, R. J., Baser, R. E., Abelson, J. M., Hanna, G. L., et al. (2008). Obsessive-compulsive disorder among African Americans and blacks of caribbean descent: results from the national survey of American life. Depress. Anxiety 25, 993–1005. doi: 10.1002/da.20434
Himle, J. A., Taylor, R. J., and Chatters, L. M. (2012). Religious involvement and obsessive compulsive disorder among African Americans and black Caribbeans. J. Anxiety Disord. 26, 502–510. doi: 10.1016/j.janxdis.2012.02.003
Himle, J. A., Taylor, R. J., Nguyen, A. W., Williams, M. T., Lincoln, K. D., Taylor, H. O., et al. (2017). Family and friendship networks and obsessive-compulsive disorder among African Americans and black Caribbeans. Behav. Ther. 40, 99–105.
Kennedy, S., Kidd, M. P., McDonald, J. T., and Biddle, N. (2015). The healthy immigrant effect: patterns and evidence from four countries. J. Int. Migr. Integr. 16, 317–332. doi: 10.1007/s12134-014-0340-x
Kogan, C. S., Noorishad, P.-G., Ndengeyingoma, A., Guerrier, M., and Cénat, J. M. (2022). Prevalence and correlates of anxiety symptoms among black people in Canada: a significant role for everyday racial discrimination and racial microaggressions. J. Affect. Disord. 308, 545–553. doi: 10.1016/J.JAD.2022.04.110
Lewis, J. A., and Neville, H. A. (2015). Construction and initial validation of the gendered racial microaggressions scale for black women. J. Couns. Psychol. 62, 289–302. doi: 10.1037/cou0000062
Meier, S. M., Mattheisen, M., Mors, O., Schendel, D. E., Mortensen, P. B., and Plessen, K. J. (2016). Mortality among persons with obsessive-compulsive disorder in Denmark. JAMA Psychiatry 73, 268–274. doi: 10.1001/jamapsychiatry.2015.3105
Mercer, S. H., Zeigler-Hill, V., Wallace, M., and Hayes, D. M. M. (2011). Development and initial validation of the inventory of microaggressions against black individuals. J. Couns. Psychol. 58, 457–469. doi: 10.1037/A0024937
Molina, K. M., and James, D. (2016). Discrimination, internalized racism, and depression: a comparative study of African American and afro-Caribbean adults in the US. GPIR 19, 439–461. doi: 10.1177/1368430216641304
Osland, S., Arnold, P. D., and Pringsheim, T. (2018). The prevalence of diagnosed obsessive compulsive disorder and associated comorbidities: a population-based Canadian study. Psychiatry Res. 268, 137–142. doi: 10.1016/J.PSYCHRES.2018.07.018
Palardy, V., El-Baalbaki, G., Fredette, C., Rizkallah, E., and Guay, S. (2018). Social support and symptom severity among patients with obsessive-compulsive disorder or panic disorder with agoraphobia: a systematic review. Eur. J. Psychol. 14, 254–286. doi: 10.5964/ejop.v14i1.1252
Soto, J. A., Dawson-Andoh, N. A., and BeLue, R. (2011). The relationship between perceived discrimination and generalized anxiety disorder among African Americans, afro Caribbeans, and non-Hispanic whites. J. Anxiety Disord. 25, 258–265. doi: 10.1016/j.janxdis.2010.09.011
Speight, S. L. (2007). Internalized racism: one more piece of the puzzle. Couns. Psychol. 35, 126–134. doi: 10.1177/0011000006295119
Stein, D. J., Fineberg, N. A., Bienvenu, O. J., Denys, D., Lochner, C., Nestadt, G., et al. (2010). Should OCD be classified as an anxiety disorder in DSM-V? Depress. Anxiety 27, 495–506. doi: 10.1002/da.20699
Steketee, G., Frost, R., and Bogart, K. (1996). The Yale-Brown obsessive compulsive scale: interview versus self-report. Behav. Res. Ther. 34, 675–684. doi: 10.1016/0005-7967(96)00036-8
Szentágotai-Tătar, A., Nechita, D.-M., and Miu, A. C. (2020). Shame in anxiety and obsessive-compulsive disorders. Curr. Psychiatry Rep. 22:16. doi: 10.1007/s11920-020-1142-9
Visvalingam, S., Crone, C., Street, S., Oar, E. L., Gilchrist, P., and Norberg, M. M. (2022). The causes and consequences of shame in obsessive-compulsive disorder. Behav. Res. Ther. 151:104064. doi: 10.1016/j.brat.2022.104064
Williams, M. T., Chapman, L. K., Simms, J. V., and Tellawi, G. (2017a). “Cross-cultural phenomenology of obsessive-compulsive disorder” in The Wiley handbook of obsessive compulsive disorders. eds. J. S. Abramowitz, D. McKay, and E. A. Storch (Wiley Blackwell), 56–74.
Williams, M. T., Domanico, J., Marques, L., LeBlanc, N. J., and Turkheimer, E. (2012). Barriers to treatment among African Americans with obsessive-compulsive disorder. J. Anxiety Disord. 26, 555–563. doi: 10.1016/j.janxdis.2012.02.009
Williams, M. T., and Jahn, M. E. (2016). Obsessive-compulsive disorder in African American children and adolescents: risks, resiliency, and barriers to treatment. Am. J. Orthopsychiatry 87, 291–303. doi: 10.1037/ort0000188
Williams, M. T., Powers, M. B., Yun, Y. G., and Foa, E. B. (2010). Minority participation in randomized controlled trials for obsessive–compulsive disorder. J. Anxiety Disord. 24, 171–177. doi: 10.1016/j.janxdis.2009.11.004
Williams, M. T., Rouleau, T. M., Torre, J. T. L., and Sharif, N. (2020). Cultural competency in the treatment of obsessive-compulsive disorder: practitioner guidelines. The Cognitive Behaviour Therapist. doi: 10.1017/s1754470x20000501
Williams, M. T., Taylor, R. J., George, J. R., Schlaudt, V. A., Ifatunji, M. A., and Chatters, L. M. (2021). Correlates of obsessive-compulsive symptoms among black Caribbean Americans. Int. J. Ment. Health 50, 53–77. doi: 10.1080/00207411.2020.1826261
Williams, M. T., Taylor, R. J., Himle, J. A., and Chatters, L. M. (2017b). Demographic and health-related correlates of obsessive-compulsive symptoms among African Americans. J. Obses. Compul. Relat. Disord. 14, 119–126. doi: 10.1016/j.jocrd.2017.07.001
Williams, M. T., Taylor, R. J., Mouzon, D. M., Oshin, L. A., Himle, J. A., and Chatters, L. M. (2017c). Discrimination and symptoms of obsessive–compulsive disorder among African Americans. Am. J. Orthopsychiatry 87, 636–645. doi: 10.1037/ort0000285
Williams, D. R., Yu, Y., Jackson, J. S., and Anderson, N. B. (1997). Racial differences in physical and mental health. Socio-economic status, stress and discrimination. J. Health Psychol. 2, 335–351. doi: 10.1177/135910539700200305
Wilson, A., and Thayer, K. (2020). Cross-cultural differences in the presentation and expression of OCD in black individuals: a systematic review. J. Obses. Compul. Relat. Disord. 27:100592. doi: 10.1016/j.jocrd.2020.100592
Wootton, B. M., and Tolin, D. F. (2016). “Obsessive–compulsive disorder” in Encyclopedia of mental health. ed. H. S. Friedman (Academic Press), 227–231.
World Health Organization, (2019). International statistical classification of diseases and related health problems (11th ed.). https://icd.who.int/en
Yorulmaz, O., Gençöz, T., and Woody, S. (2009). OCD cognitions and symptoms in different religious contexts. J. Anxiety Disord. 23, 401–406. doi: 10.1016/j.janxdis.2008.11.001
Yorulmaz, O., Gençöz, T., and Woody, S. (2010). Vulnerability factors in OCD symptoms: cross-cultural comparisons between Turkish and Canadian samples. Clin. Psychol. Psycho. 17, 110–121. doi: 10.1002/cpp.642
Keywords: obsessive-compulsive disorder, everyday racial discrimination, internalized racism, racial microaggressions, social support, Black individuals in Canada
Citation: Dromer E, Jacob G, Williams MT, Moshirian Farahi SMM, Darius W, Kogan CS and Cénat JM (2025) Obsessive-compulsive symptoms and related risk and protective factors in Black individuals in Canada. Front. Psychol. 16:1422900. doi: 10.3389/fpsyg.2025.1422900
Edited by:
Ana Sánchez-Kuhn, University of Almeria, SpainReviewed by:
Filiz Karadag, Gazi University, TürkiyeCopyright © 2025 Dromer, Jacob, Williams, Moshirian Farahi, Darius, Kogan and Cénat. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Elisabeth Dromer, ZWxpc2FiZXRoLmRyb21lckB1b3R0YXdhLmNh; Jude Mary Cénat, amNlbmF0QHVvdHRhd2EuY2E=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.