 Ana L. Vilela-Estrada1,2†‡
Ana L. Vilela-Estrada1,2†‡ David Villarreal-Zegarra3*†‡Anthony Copez-Lonzoy4‡Loida Esenarro-Valencia5,6,7‡José C. Sánchez-Ramírez5,8‡Fernando Lamas-Delgado5,6,9‡Juan Ambrosio-Melgarejo10C. Mahony Reategui-Rivera3‡
David Villarreal-Zegarra3*†‡Anthony Copez-Lonzoy4‡Loida Esenarro-Valencia5,6,7‡José C. Sánchez-Ramírez5,8‡Fernando Lamas-Delgado5,6,9‡Juan Ambrosio-Melgarejo10C. Mahony Reategui-Rivera3‡ Joseph Finkelstein3‡
Joseph Finkelstein3‡- 1CRONICAS Center of Excellence in Chronic Diseases, Universidad Peruana Cayetano Heredia, Lima, Peru
- 2Instituto Peruano de Orientación Psicológica, Lima, Peru
- 3Department of Biomedical Informatics, School of Medicine, University of Utah, Salt Lake City, UT, United States
- 4Unidad de Investigación en Bibliometría, Universidad San Ignacio de Loyola, Lima, Peru
- 5Instituto Nacional de Enfermedades Neoplásicas, Lima, Peru
- 6Escuela de Posgrado, Universidad Peruana Unión, Lima, Peru
- 7Instituto de Neuropsicología y Demencias, Lima, Peru
- 8Universidad de Lima, Lima, Peru
- 9Facultad de Ciencias de la Salud, Universidad SanIgnacio de Loyola, Lima, Peru
- 10National Institute of Health (Peru), Lima, Peru
Background: Although the Hospital Anxiety and Depression Scale (HADS) has been widely studied across various populations, there is still no consensus on its factor structure. This study aims to evaluate the psychometric properties of the HADS in cancer patients.
Methods: Our study was cross-sectional and non-probabilistic. It involved 467 cancer patients aged 18 years and over, who were treated at a public institution specialized in oncology. The Hospital Anxiety and Depression Scale, the Beck Anxiety Inventory, and the Beck Depression Inventory were used. We evaluated their internal structure, measurement invariance, relationship with other variables, and reliability.
Results: It was found that the HADS is best suited to a bifactorial structure where there is one general factor (emotional distress) and two specific factors (anxiety and depression). The HADS demonstrates invariance with respect to sex and years of education. It shows a moderate correlation with the Beck Anxiety Inventory and the Beck Depression Inventory. In addition, it presents acceptable levels of reliability and relationship with instruments used in the diagnosis of anxiety and depression.
Conclusion: The HADS is best suited to a bifactorial structure in cancer populations, with comparisons across both sexes and varying levels of education. Its brevity, versatility, hospital-focused design, and extensive validation make the HADS a very important instrument in the detection of anxiety and depression in cancer patients.
Introduction
According to the Global Burden of Disease Study 2019, anxiety and depression were the leading causes of global disability-adjusted life years (DALYs) and years lived with disability (YLDs) in mental health (GBD 2019 Mental Disorders Collaborators, 2022). Furthermore, it is estimated that anxiety disorders accounted for 28.68 million DALYs (Xiong et al., 2022) and depressive disorders contributed 49.4 million DALYs (GBD 2019 Mental Disorders Collaborators, 2022). In cancer patients, the prevalence of these disorders is higher, with anxiety affecting 9.8–10.3% and depression affecting 16.3–16.5% of patients (Mitchell et al., 2011).
Validated scales are widely used as cost-effective tools for assessing affective disorders (Ehlers et al., 2018; Siu et al., 2016). The literature highlights various instruments used to assess these affective disorders in cancer patients: the Beck Anxiety Inventory (BAI), the Beck Depression Inventory (BDI), and the Hospital Anxiety and Depression Scale (HADS) (Howell et al., 2015). Among these, the HADS is frequently cited in systematic reviews as one of the most widely used instruments for detecting affective disorders in cancer patients (Maters et al., 2013; Vodermaier and Millman, 2011). This instrument, designed for hospital populations, can be used to assess emotional distress from a psychosocial perspective (one-dimensional model) or from a clinical perspective (two-dimensional model of anxiety and depression) (Norton et al., 2013; Zigmond and Snaith, 1983).
Since its inception, the HADS has undergone extensive testing to verify both its validity and reliability in English and other languages (Al Aseri et al., 2015; Christensen et al., 2020; Lin et al., 2017; Reda, 2011; Yang et al., 2019), yielding satisfactory results in various hospital populations such as patients with heart disease, cancer, HIV, and psychiatric disorders. However, studies on the factor structure of the scale have given heterogeneous results (Norton et al., 2013). These studies used methods such as exploratory factor analysis (EFA), confirmatory factor analysis (CFA), and item response theory (IRT). These identified structural models based on one dimension (Waqas et al., 2019), two dimensions (Zigmond and Snaith, 1983), and three dimensions (Caci et al., 2003; Dunbar et al., 2000; Friedman et al., 2001). Therefore, the factorial structure of the HADS is not conclusive, which could affect the validity of the instrument.
Beyond structural analysis, measurement invariance is another essential property to consider, as it enables meaningful comparisons between groups. If measurement invariance holds between two groups, it suggests that both groups interpret and understand the construct being measured in a similar way (Putnick and Bornstein, 2016). Regarding sex, different studies support that invariance is met between men and women (Annunziata et al., 2011; Hunt-Shanks et al., 2010; Iani et al., 2014; Stott et al., 2017a; Stott et al., 2017b; Yang et al., 2019). However, the results of the analysis of invariance between different age groups have shown contradictory findings (Iani et al., 2014; Stott et al., 2017a; Stott et al., 2017b). Preliminary evidence supports invariance among patients with HIV, regardless of infection status (Yang et al., 2019), and among patients with different stages of cancer (Annunziata et al., 2011).
Convergent validity is another important property to analyze, as it refers to the strong and direct relationship expected between instruments that measure the same construct. In that sense, several studies have found a relationship between the HADS and other variables in different settings (palliative care, brain tumor, and specific clinical groups). In terms of the total HADS score, a strong and positive correlation is reported with emotional distress (Emotional Distress Detection Scale—DEDS) (Limonero et al., 2012), post-traumatic stress and demoralization (Belar et al., 2019; Mystakidou et al., 2007a), and with Psychosocial and Spiritual Needs of the Sick at the End of Life (ENP-E, in palliative patients) (Mystakidou et al., 2007b). For the anxiety subscale, a strong and positive correlation was reported with the State–Trait Anxiety Inventory (STAI), the Prostate Cancer Memorial Anxiety Scale (MAX-PC), and the DEDS subscale (Limonero et al., 2012; Mystakidou et al., 2009; Touzani et al., 2019). It showed a moderate correlation with fear of recurrence (FoR) (Hinz et al., 2015; Humphris et al., 2018; Shin et al., 2017) and a strong correlation with non-psychological variables, such as cancer-related fatigue (Fillion et al., 2003). On the depression subscale of the HADS, a strong and moderate positive correlation was reported using the Beck Depression Inventory and the Patient Health Questionnaire (PHQ-9), respectively (Mystakidou et al., 2007a; Rooney et al., 2012), while with non-psychological variables, such as cancer-related fatigue, it also showed a strong correlation (Fillion et al., 2003).
However, there is limited evidence regarding the validity of the Spanish version of the Hospital Anxiety and Depression Scale (HADS) specifically in cancer patients. Previous studies have primarily assessed the validity of the HADS in populations with other clinical conditions, such as pulmonary, rheumatological, infectious, or cardiovascular diseases (Herrero et al., 2003; Luciano et al., 2014; Quintana et al., 2003; Suárez-Mendoza et al., 2019). Importantly, research on other questionnaires has demonstrated that the validity and reliability metrics of psychometric instruments can vary significantly depending on the clinical conditions of the studied populations. Differences have been observed across general populations, individuals with endocrine disorders such as diabetes, and patients with cancer (Hinz et al., 2016; van Dijk et al., 2018). A study conducted in Chile evaluated the validity of the Spanish version of the HADS in a cancer population, but it focused exclusively on a one-factor structure related to emotional distress symptoms (Villoria and Lara, 2018). This approach may have overlooked other potential factor structures, which could provide a more nuanced understanding of the instrument’s performance. Therefore, it is crucial to explore the psychometric properties of the HADS further, considering multiple factor structures to assess its robustness and applicability in cancer patients.
Given the necessity of valid and reliable instruments for detecting affective disorders in Spanish-speaking hospital populations and considering the HADS as one of the most utilized tools for this purpose, this study aimed to evaluate the evidence of validity and reliability of the Spanish version of the HADS in cancer patients.
Materials and methods
Study design
Our study employs a cross-sectional design.
Setting
The evaluation was conducted by psychologists or educational psychologists at a Peruvian public cancer institution in Lima, Peru. The hospital where the study was carried out is a highly specialized facility that receives oncology patient referrals from various regions of Peru. The evaluators were trained in administering the psychometric tests specific to the study. The scales were administered individually to oncology patients with a definitive diagnosis.
Participants
The sample included 500 participants, who fulfilled the following inclusion criteria: being cancer patients of the National Institute of Neoplastic Diseases, are over 18 years old, and can read and write. Furthermore, participants should not present physical discomfort during the administration, nor have cognitive disabilities that limit their understanding or ability to complete the instruments of the current study. The sampling was intentionally non-probabilistic.
Procedures and ethics
The protocol was approved by the INEN Research Ethics Committee and the Research Review Committee (N°239-2018-CIE/INEN). Participants were invited to take part in the research in accordance with conventional ethical standards. After providing written informed consent, they were given a questionnaire that included socio-demographic questions, the Peruvian adaptation of the HADS, the BDI-II, and the BAI.
Instruments
The hospital anxiety and depression scale (HADS)
The HADS is a 14-item questionnaire created by Zigmond and Snaith in 1983 to measure symptoms of anxiety and depression in patients with somatic illnesses (Zigmond and Snaith, 1983). It has questions to detect cognitive symptoms of anxiety and depression. Furthermore, both subscales would provide an overall score for emotional distress (Norton et al., 2013). The scale is Likert-type, where 0 is the lowest score and 3 is the highest score to measure the symptoms experienced during the last week. The score range for the global dimension is 0–42, and the range for each subdimension of anxiety and depression is 0–21.
The HADS translation (Muñiz et al., 2013) from English to Spanish was evaluated by two independent consultants, who based their work on the original Spanish translation of the test by Zigmond and Snaith (1983). Additionally, a reverse translation (Spanish–English) was conducted for further evaluation. Finally, an analysis regarding its clarity, relevance, and appropriateness was carried out by 10 expert judges (eight psychologists and two psychometrists).
The Beck depression inventory—second edition (BDI-II)
The BDI-II is a 21-item multiple-choice self-report inventory created by Beck, Steer, and Brown in 1996 to measure the severity of depressive symptoms in psychiatric patients and in normal adolescents and adults (Beck et al., 1996). It has high internal consistency (α = 0.91) (Brenlla et al., 2013) and test–retest reliability (α = 0.90). The evidence of convergent validity was robust and showed strong correlations with the MMPI (r = 0.58) and Depression Scale of SCL-90 (r = 0.81). The factorial validity obtained two factors: somatic-affective and cognitive-affective, respectively.
The Beck anxiety inventory (BAI)
The BAI is a 21-item self-applied scale created by Beck, Epstein, Brown, and Steer in 1988 to measure the severity of anxiety symptoms in adults and adolescents (Beck et al., 1988) in psychiatric populations. It shows a high internal consistency (α = 0.92) and test–retest reliability over 1 week (r = 75) (Beck et al., 1988). In addition, the BDI has previously been validated in Spanish for a global dimension (Vizioli and Pagano, 2020).
Statistical analysis
Five groups of analyses were conducted. First, the characteristics of the participants were evaluated (socio-demographic characteristics) and item characteristics (standard deviation and mean). Second, a confirmatory factor analysis (CFA) was used with the goal of evaluating 10 models proposed for the Hospital Anxiety and Depression Scale (Norton et al., 2013). Third, the measurement invariance was evaluated to know whether the models were adequate according to groups (sex and education levels). Fourth, the relationship was evaluated with other variables: the Beck Depression Inventory (BDI) and the Beck Anxiety Inventory (BAI). Fifth, internal consistency was evaluated with alpha and omega coefficients.
Confirmatory factor analysis
For the analysis of the factor structure of HADS, the 10 models analyzed in a meta-confirmatory factor analysis were used (Norton et al., 2013; Zigmond and Snaith, 1983). Of these models, one was a one-dimensional model, two were correlated factor models (anxiety-depression), five were 3-factor models (four correlated factor models and one higher-order model), and two were bifactor models (one model with two orthogonal factors and one with three orthogonal factors) (Norton et al., 2013).
CFA is a statistical procedure, which allows checking of the validity of the instrument’s internal structure (Batista-Foguet et al., 2004). In this study, the CFA was used to analyze 10 models that have previously been shown to have adequate goodness-of-fit indices. In addition, for ordinal data, the weighted least squares with mean and variance adjusted (WLSMV) estimator was chosen for the CFA, and a polychoric matrix was used, as these methods are specifically designed for ordinal data (Dominguez-Lara, 2014; Li, 2016). The analysis was conducted in three stages. First, to evaluate the model’s adjustment index, the CFI, TLI, RMSEA, SRMR, and confidence interval (CI) with 90% were considered. Second, to evaluate overlapping factors, the latent correlations between dimensions were to be considered. Third, to evaluate the relevance of a general factor in bifactor models (models 9 and 10), the following indices were used: hierarchical omega (ωH), percentage of uncontaminated correlations (PUC), and explained common variance (ECV). The data would be in favor of the general factor if values of ωH ≥ 0.70, PUC ≥ 0.70, and ECV ≥ 0.60 are found (Dominguez-Lara and Rodriguez, 2017).
Measurement invariance
A measurement invariance analysis was conducted with the aim of evaluating whether the different groups assessed, such as men and women, understand the evaluated construct equivalently (Putnick and Bornstein, 2016). Of the 10 initial models, the most parsimonious and best-fitting models (CFA) were taken. These models underwent measurement invariance analysis. The evaluation of levels of measurement invariance was carried out in two stages. In the first one, it was evaluated at the configuration and metric level; for the configuration level, the factorial structures were evaluated to be equal; for the metric level, the factorial loads were restricted to be equivalent. In the second stage, it was evaluated at the scalar level, where the intercepts were restricted to be equivalent. In both stages, the level of invariance was accepted if the variations in the CFI < 0.01. In addition, the values obtained through the DIF test were reported.
Relationship with other variables
This study examines the relationships between the Hospital Anxiety and Depression Scale (HADS) and other established measures of depression and anxiety, specifically the Beck Depression Inventory (BDI) and the Beck Anxiety Inventory (BAI). It is anticipated that the overall HADS factor will exhibit moderate correlations with both the overall BAI and BDI scores. Furthermore, a high correlation is expected between the first HADS-specific factor, which assesses depressive symptoms, and the general factor of the BDI. Similarly, a strong correlation is anticipated between the second HADS-specific factor, which assesses anxiety, and the general factor of BAI. Specifically, we expect a stronger relationship between instruments measuring the same constructs than between those measuring different constructs. Correlation strengths are categorized as high (r > 0.7), moderate (r > 0.5), and low (r > 0.3) (Mukaka, 2012).
Internal consistency analysis
To identify the consistency measure of the construct, this study performed an internal consistency analysis. Alpha and omega coefficients were used to evaluate internal consistency. In addition, they were acceptable values when the coefficients had values greater than 0.70 (Campo-Arias and Oviedo, 2008).
Software used
R and STATA were used for the analysis. For analysis with R, the following packages were used: ‘lavaan’, ‘semTools’, ‘psych’, and ‘survey’.
Results
Characteristics of the participants
Initially, 500 participants were evaluated. However, 25 (5%) were excluded due to missing data on the HADS, and 8 (1.6%) were excluded for being foreigners (n = 8, 1.6%). The study included 467 participants. The majority of participants were female (75.6%), with ages ranging from 17 to 84 years (mean = 45.9; SD = 14.4). The majority were married or cohabiting (48.4%) and unemployed (78.4%), predominantly homemakers. The detailed characteristics of the participants are presented in Table 1.
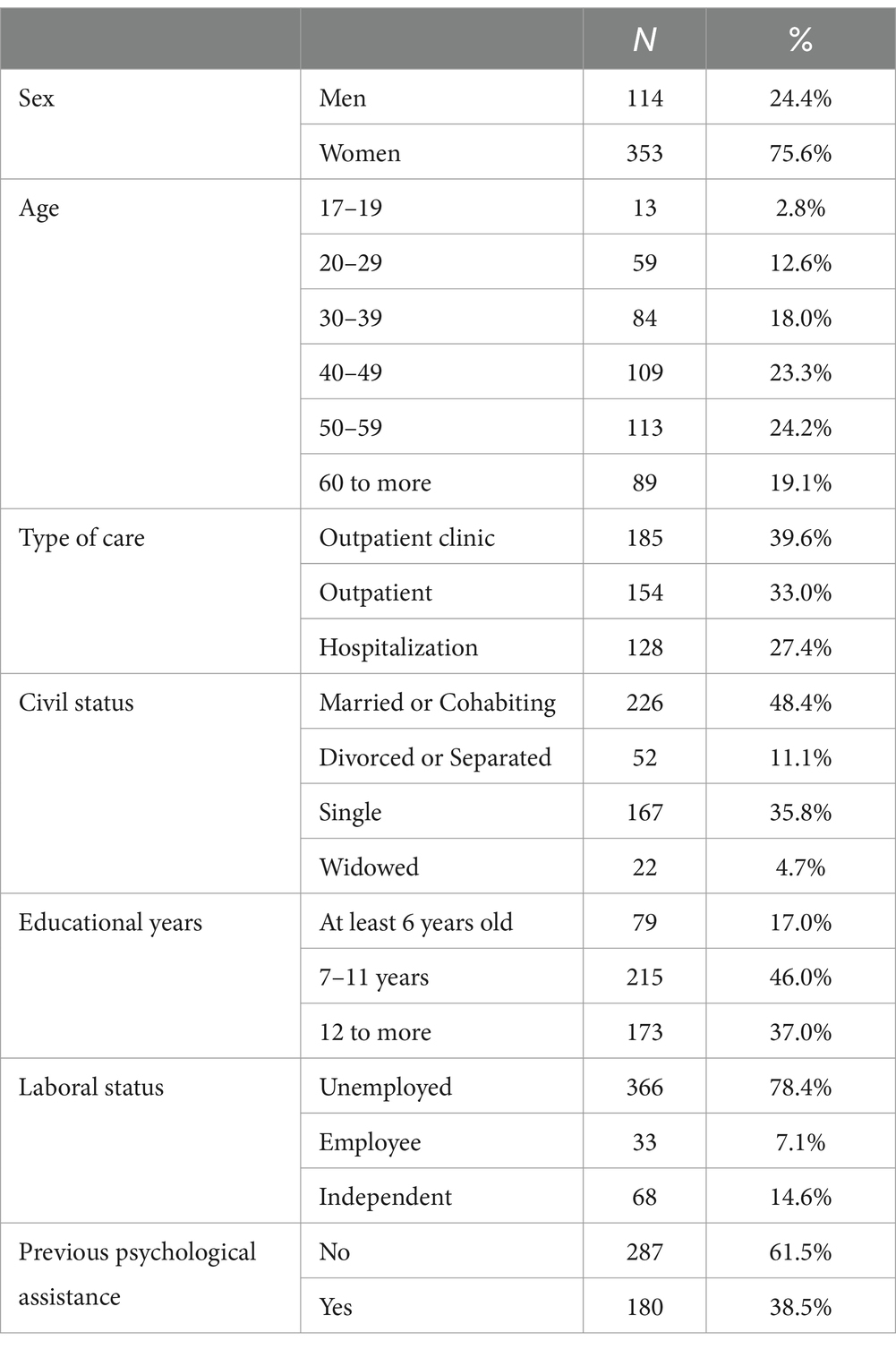
Table 1. Characteristics of the participants (n = 467).
Confirmatory factor analysis
The factor analysis revealed that the one-dimensional model exhibited low goodness-of-fit indices, with CFI and TLI values below the threshold expected for a clinical instrument (< 0.95; Model 1). Consequently, this model was not considered for further analyses. Additionally, the bifactor model of the HADS with three orthogonal factors failed to converge (Model 10), leading to its exclusion. The other models had adequate goodness-of-fit indices (see Table 2).
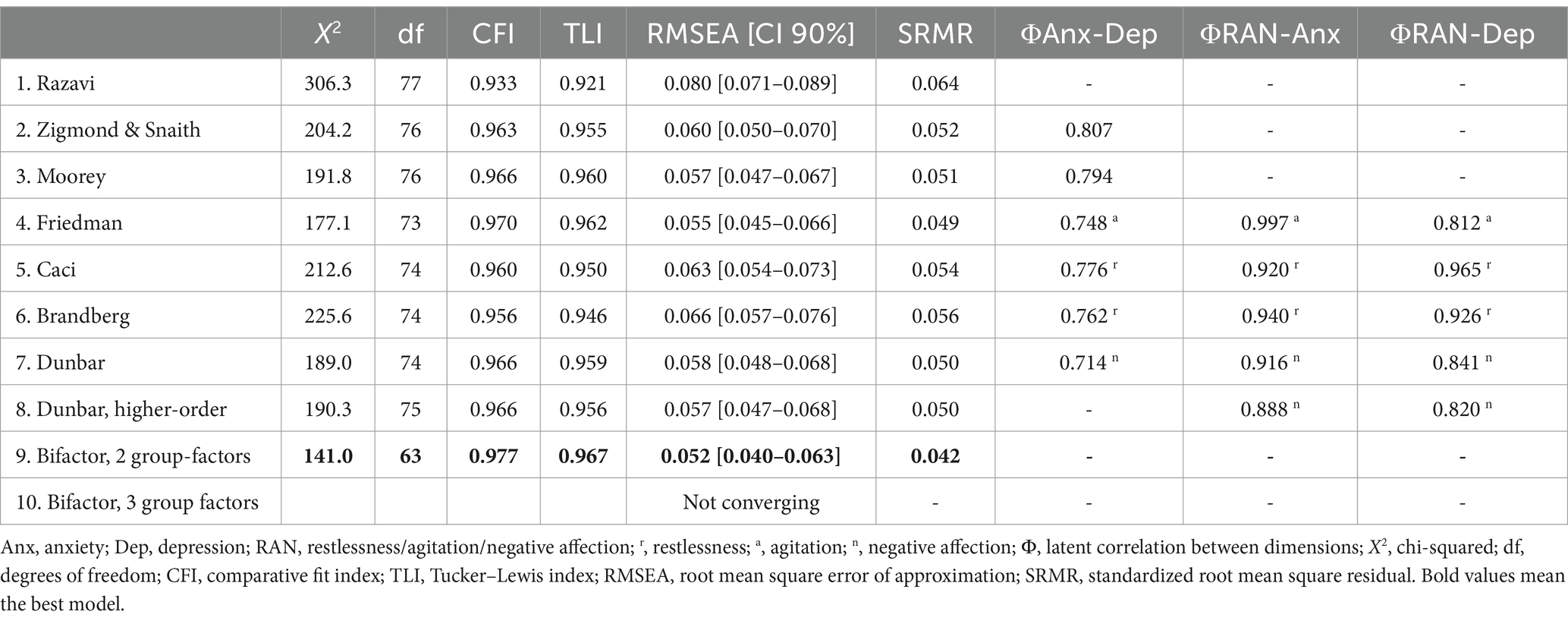
Table 2. Goodness-of-fit indices and latent correlations of each of the models evaluated for HADS.
When analyzing the two-factor model of Zigmond and Snaith, and the three-factor models of Friedman, Caci, Brandberg, and Dunbar, it was found that the latent relationships between their dimensions were extremely high (>0.80). This suggests that the dimensions may be overlapping. Therefore, these models were excluded from the following analyses. In the case of Moorey’s model with the correlated factor model, the latent relationship presented a high value (Φ = 0.794).
In analyzing the remaining bifactor model (with two orthogonal factors), the explained common variance of the general factor was high (>0.70) and the variances of the specific dimensions were adequate (>0.20). Factorial loads were higher in the general factor than in the specific factors (see Table 3). In addition, the bifactor model presents better goodness-of-fit indices than all previous models. According to the values of the indices to evaluate the bifactor models (ωH = 0.80, ECV = 0.72, PUC = 0.54; see Table 3), the existence of one-dimensionality is suggested (Dominguez-Lara and Rodriguez, 2017; Rodriguez et al., 2016). That is why the bifactor model with one general dimension and two specific dimensions of anxiety and depression was selected as the most appropriate. Thus, the rest of the analysis will be carried out with this model.
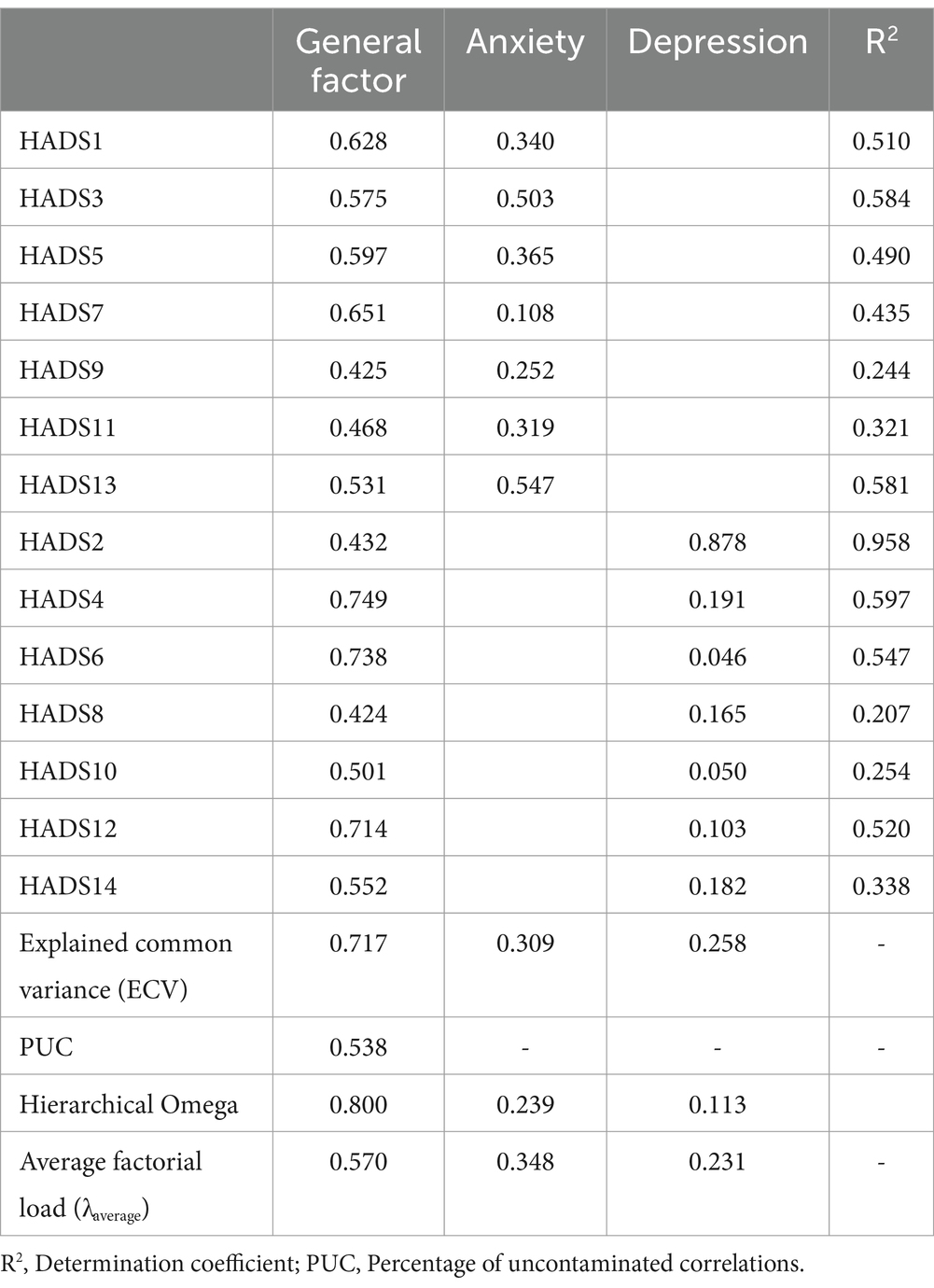
Table 3. Factorial loads and indices of the bifactor model (with two orthogonal factors) of HADS.
Measurement invariance
The invariance analysis identified that the bifactor model with one general factor and two specific factors of anxiety and depression presented invariance according to sex and years of education. It was identified that ΔCFI was less than 0.01 in both cases (see Table 4).
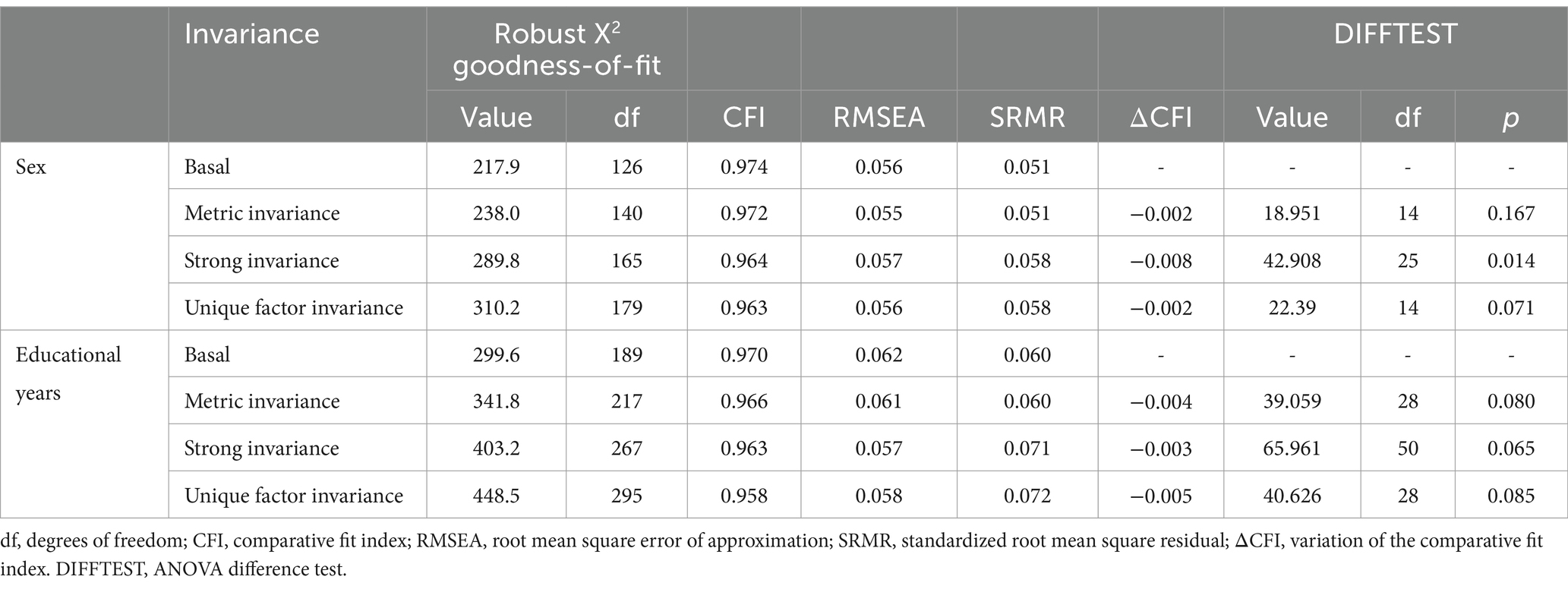
Table 4. Analysis of factor invariance of the HADS bifactor model (with two orthogonal factors) according to sex and educational years.
However, it was found that in the case of sex, the ANOVA test pointed to a significant value (p = 0.01) when comparing metric invariance and strong invariance. It was not considered relevant as the p-value is very sensitive to sample size.
Relationship with other variables
The general factor of the HADS showed a moderate correlation with another depression scale (BDI) (r = 0.65) and an anxiety scale (BAI) (r = 0.67). Additionally, the HADS anxiety-specific factor demonstrated a strong correlation with the Beck Anxiety Inventory (r = 0.70). However, the HADS depression-specific factor showed a moderate correlation with the Beck Depression Inventory (r = 0.58; see Table 5), contrary to expectations, as a strong relationship between the two instruments was anticipated.

Table 5. Spearman correlation between the dimensions of the HADS with the Beck Depression Inventory (BDI) and the Beck Anxiety Inventory (BAI).
Additionally, the correlations between the specific anxiety factor and the BAI (r = 0.70) were higher than with the BDI (r = 0.59), and the correlation between the specific depression factor and the BDI (r = 0.58) was higher than with the BAI (r = 0.50). Therefore, it is considered that discriminant validity between the different measurements was maintained.
Internal consistency analysis
The general factor of the HADS showed high internal consistency, with ω = 0.91 and α = 0.90. Similarly, the specific factors of anxiety (ω = 0.84; α = 0.84) and depression (ω = 0.84; α = 0.84) also presented strong consistency coefficients.
Discussion
Main findings
The Spanish version of the HADS demonstrates adequate psychometric properties, providing evidence of validity and reliability in an oncological population in Peru. Our findings support the presence of a global factor in the HADS, alongside two specific factors: anxiety and depression. These results align with a meta-analysis based on 21 studies involving 21,820 participants, which found that the bifactorial model with two orthogonal-specific factors exhibited the best psychometric properties (Norton et al., 2013). In our study, the specific depression subdimension showed low factor loadings for most items, which may result in this dimension being underrepresented. Nonetheless, at a general level, the model provides evidence of validity based on internal structure.
Moreover, the HADS can be used to compare both sexes, as well as individuals with varying levels of education. This indicates that the instrument is stable (invariant) across these groups. Additionally, the HADS demonstrates validity about other variables. Specifically, the HADS anxiety subdimension strongly correlates with the BAI, while the global HADS score exhibits moderate correlations with both the BDI and BAI, as hypothesized. However, the correlation between the HADS depression subdimension and the BDI score was moderate. Finally, our study found that the HADS global factor and its specific factors of anxiety and depression demonstrated optimal internal consistency coefficients.
Factor analysis
Our study identified that the bifactor model is the most appropriate factorial structure of the Spanish version of HADS in cancer patients in Peru. This is in line with what was found in a systematic review performing a meta-confirmation analysis of the HADS, which also concluded that the bifactor model is the most suitable (Norton et al., 2013). Other studies have identified alternative one-, two-, or three-dimensional models (Annunziata et al., 2011; Emons et al., 2010; Gale et al., 2010; Galindo Vázquez et al., 2015a; Matsudaira et al., 2009; Norton et al., 2013; Terol-Cantero et al., 2015). Our study and the meta-confirmation study mentioned above tested these alternative models and agree that the bifactor model is the most adequate.
This could be due to the fact that some HADS studies have used analytical methods that are not suitable or have proven inefficient for psychometric evaluations (e.g., main components, scree plots, eigenvalues, and varimax) (Christensen et al., 2020; Cosco et al., 2012; Gale et al., 2010; Nezlek et al., 2019). Therefore, this could have introduced bias in their measurements, which could have led them to identify the heterogeneity of models. On the other hand, it is worth mentioning that not all studies evaluated the 10 factorial models assessed in our study, so it is possible that other models could potentially have been more appropriate.
The bifactor model consists of a general factor and specific orthogonal factors (where the correlation between factors is zero). In the bifactor model, it is the general factor that strongly explains the variance of the HADS items, and the specific factors explain the variance of a group of items each (depression explains even items; anxiety explains odd items), although these specific factors explain the items less than the general factor. In the HADS, the specific factors identified would be anxiety and depression. As for the general factor, this would be called emotional distress, which is defined as a state of negative affect, suggesting the presence of affective disorders (Vodermaier et al., 2009). We chose to keep the term emotional distress because it is widely used in the literature when referring to the assessment of both anxiety and depression (Lee et al., 2018; Milligan et al., 2018; Yan et al., 2019).
The existence of a general factor that can explain all the items is in line with the proposal of the transdiagnostic models. These models focus on the underlying common symptoms or processes between diagnostic categories (Mansell et al., 2009; Norton and Paulus, 2017). In this study, emotional distress will be the transdiagnostic factor between anxiety and depression present in the HADS. The evidence is not yet conclusive about the single term or transdiagnostic factors present between anxiety and depression. Therefore, we can find in the literature constructs such as dysregulation of negative affect, repetitive negative thinking, and rumination, which are considered transdiagnostic factors for emotional disorders (Akbari et al., 2015; Hofmann et al., 2012; Hsu et al., 2015). On the other hand, the bifactor structure of the HADS appears to solve the problem of overlapping symptoms between anxiety and depression and the high correlation between the factors (anxiety and depression) (Aarstad et al., 2005; Kirkova et al., 2011; Schellekens et al., 2020), stating that both constructs are present in an orthogonal way and it is the general factor that explains most of the variance of the items.
When the HADS was developed, the physical symptoms of anxiety and depression were omitted to avoid confusion with natural physical symptoms associated with patients’ illnesses in hospitals (Zigmond and Snaith, 1983). As a result, the HADS was originally designed to assess the emotional and cognitive aspects of anxiety and depression. Transdiagnostic models do not contradict the presence of specific factors such as anxiety and depression, as they do not pretend to oppose specific diagnoses. Instead, they suggest using specific models or transdiagnostic depending on whether it is clinically significant or whether the presence of specific diagnoses is necessary, which may well complement the information provided by the transdiagnostic factors (Mansell et al., 2009). Finally, although specific anxiety and depression factors are identified in the structure, it is advisable to exercise caution in considering both dimensions as sufficient for diagnosing anxiety and depression. This would require further evaluation.
In terms of usefulness, three strengths were identified in the HADS bifactor structure. First, the HADS would be a versatile instrument, which would work very well as a filter to identify emotional distress (transdiagnostic factor) and would allow specifying the specific symptomatology (i.e., presence of depression or anxiety symptoms). This would be very useful in terms of further evaluation, giving more information about whether the patient has any emotional disorder and whether it is more specifically anxiety and/or depression. Second, it is important to note the brevity of the HADS, with the 14 items, it has proven to be of great value in detecting emotional distress and symptoms of anxiety and depression. Third, the HADS is a tool that stands out for its configuration, in which physical symptoms are not considered. This is noteworthy because it decreases the likelihood of false positives due to the physical symptoms experienced by hospital patients, which are often confused with the physical symptoms of anxiety and depression.
Measurement invariance
A crucial aspect of clinical assessment is to determine whether the instrument is invariant between different groups, i.e., whether the two or more groups can understand the construct equivalently assessed by the scale and thus make comparisons between those groups (Putnick and Bornstein, 2016). As if an instrument is not invariant among different groups, different sensitivity and specificity analyses will be required, which would limit its clinical use, to name one example.
Our study found that there are no differences in the factor structure of the HADS in the Peruvian oncological population based on sex, as previously evidenced in other studies conducted in a sample of the Italian community and HIV patients in China (Iani et al., 2014; Yang et al., 2019). This suggests that the HADS is useful for detecting symptoms of emotional distress, anxiety, and depression in both sexes, although the clinical manifestations of depression and anxiety may vary according to sex (Zarragoitía Alonso, 2013). It is important to note that other HADS studies, which proposed alternative two-dimensional or three-dimensional factor structures, have also found evidence of invariance between men and women (Annunziata et al., 2011; Czerwiński et al., 2020; Fong and Ho, 2014; Hunt-Shanks et al., 2010; Stott et al., 2017a; Stott et al., 2017b). This is an encouraging finding as the instrument appears to allow for the assessment of anxiety, depression, and emotional distress without distinction by sex in different populations, even when less adequate factorial models are used.
On the other hand, it was shown that the HADS can measure the symptoms of emotional distress, anxiety, and depression in the Peruvian cancer population with different years of study (less than 6 years, between 7 and 11 years, and 12 or more years), one relevant point is that our study has been the first to evaluate the measurement invariance of the HADS based on educational level. It had previously been pointed out that the uneven distribution of the elements of inverse writing could influence vulnerable populations such as individuals with low levels of education due to the difficulty that it would generate in reading activity (Lin et al., 2017). However, these results support that the instrument has an equal factorial structure, the items contribute similarly, and the intersections are equivalent in the groups. Despite the heterogeneous characteristics of the sample, which comes from an institute specialized in cancer and includes populations from different geographical areas of Peru and varying levels of education, this allows us to affirm that the variables are evaluated in the same way across all groups. This is a valuable feature for making informed public health decisions.
Relationship with other variables
Our study found that the specific depression factor of the HADS correlates more strongly with another instrument measuring depression (BDI) than with an instrument measuring anxiety (BAI). Similarly, the specific anxiety factor of the HADS shows a stronger correlation with the BAI than with the BDI. This suggests that the HADS provides evidence of convergent validity, as dimensions measuring the same construct exhibit stronger relationships than those measuring different constructs (Muñiz, 2018). Our findings are supported by previous studies that identified similar relationships in patients with chronic illnesses (Preljevic et al., 2012; Schellekens et al., 2016).
Internal consistency analysis
In the bifactorial model of the HADS were found acceptable levels of reliability (ω > 0.70 and α > 0.70) for both the general factor and the specific factors, which coincide with the results of other studies (Cabrera et al., 2015; Galindo Vázquez et al., 2015b; Li et al., 2016; Martínez López et al., 2012; Terol-Cantero et al., 2015). Having an acceptable level of reliability strengthens and enhances the relevance of using the HADS, as it demonstrates that the instrument provides a good degree of stability in its measurements.
Relevance in public health and psychosocial providers
This study provides different evidence of the validity and reliability of the HADS in the Peruvian oncological population, which supports its use within the context of oncological patient care. The HADS can be used as a tool to evaluate the clinical progress of individuals receiving psychological care in an oncological context. In addition, it can be used as a research tool in clinical trials or longitudinal studies in cancer patients, as it is an instrument with solid evidence of validity and reliability.
The Peruvian health system is overburdened, and mental health professionals are insufficient and have very little time to treat patients (Toyama et al., 2017). Thus, the HADS, because of its brevity (only 14 items) and empirical support, could be a good option for assessing depressive and anxiety symptoms within the hospital setting. Mainly in rural areas of Peru, where the percentage of mental healthcare is much lower (Villarreal-Zegarra et al., 2020) Our findings may be of interest to public health, as implementing the HADS within the primary or hospital care system would help streamline and expedite the processes of identifying and referring patients with any of these symptoms. Therefore, we encourage policymakers to consider incorporating the HADS into clinical practice guidelines.
Strengths and limitations
One of the strengths of our study is the certainty that the participants had cancer as they all had previous medical examinations to confirm the disease. However, our study has five major limitations. First, it does not provide a cohort point for identifying whether participants have symptoms of depression, anxiety, or emotional distress. Therefore, future studies on sensitivity and specificity are needed. Second, our data were selected in a non-probabilistic way, so our results cannot be generalized to the entire cancer population in Peru. Third, because we had a small sample size, we could not perform analyses of variance among other interest groups such as age, income, living in rural and urban areas, or stages of cancer. For example, the necessary assumptions to perform a measurement invariance analysis between age groups were not met, which caused the models to fail to converge. Fourth, the relationship of the HADS with other clinically relevant variables such as quality of life, wellbeing, or other instruments of emotional distress could not be assessed (Mansell et al., 2009; Milligan et al., 2018; Norton and Paulus, 2017). Fifth, our study was non-probabilistic, so the findings could not be generalized to other populations.
Conclusion
Our results support the use of the HADS in the oncological population in Peru, as it demonstrates evidence of both validity and reliability. Our data support a bifactor model of the HADS, with one general factor of emotional distress and two specific factors (anxiety and depression). In addition, it is invariant, presents convergent validity, and has adequate internal consistency coefficients.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found at: the data used in the analysis is attached as https://doi.org/10.6084/m9.figshare.13626773.v2.
Ethics statement
The studies involving humans were approved by Ethical approval was granted by the Ethical Review Committee of the National Institute of Neoplastic Diseases (INEN). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AV-E: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. DV-Z: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Validation, Writing – original draft, Writing – review & editing. LE-V: Conceptualization, Writing – original draft, Writing – review & editing. JS-R: Conceptualization, Writing – original draft, Writing – review & editing. FL-D: Conceptualization, Writing – original draft, Writing – review & editing. JA-M: Conceptualization, Formal analysis, Writing – original draft, Writing – review & editing. AC-L: Conceptualization, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. CR-R: Conceptualization, Formal analysis, Methodology, Writing – original draft, Writing – review & editing,Conceptualization, Formal analysis, Methodology, Writing – original draft, Writing – review & editing,Investigation, Methodology, Validation, Writing – original draft, Writing – review & editing. JF: Investigation, Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The authors thank the support of the members of the Oncological Mental Health Functional Team; evaluating clinical psychologists: Rosa Argüelles Torres, Giovanna Galarza Torres, Flor Arrunátegui Reyes, Hernán Bernedo Del Carpio, Antonio Conso Machuca, Oscar Villanueva Cortés, Sarita Angulo Rubio, Yvo Fernández Montoro; the Psychology Interns team period 2018; and all the patients of the INEN who responded to the evaluation. In addition, thanks to Daniel Rivas for the linguistic revision of the article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Aarstad, H. J., Aarstad, A. K. H., Heimdal, J.-H., and Olofsson, J. (2005). Mood, anxiety and sense of humor in head and neck cancer patients in relation to disease stage, prognosis and quality of life. Acta Otolaryngol. 125, 557–565. doi: 10.1080/00016480510027547
Akbari, M., Roshan, R., Shabani, A., Fata, L., Shairi, M. R., and Zarghami, F. (2015). Transdiagnostic treatment of co-occurrence of anxiety and depressive Disorders based on repetitive negative thinking: a case series. Iran. J. Psychiatry 10, 200–211.
Al Aseri, Z. A., Suriya, M. O., Hassan, H. A., Hasan, M., Sheikh, S. A., Al Tamimi, A., et al. (2015). Reliability and validity of the hospital anxiety and depression scale in an emergency department in Saudi Arabia: a cross-sectional observational study. BMC Emerg. Med. 15:28. doi: 10.1186/s12873-015-0051-4
Annunziata, M. A., Muzzatti, B., and Altoè, G. (2011). Defining hospital anxiety and depression scale (HADS) structure by confirmatory factor analysis: a contribution to validation for oncological settings. Ann. Oncol. 22, 2330–2333. doi: 10.1093/annonc/mdq750
Batista-Foguet, J. M., Coenders, G., and Alonso, J. (2004). Análisis factorial confirmatorio. Su utilidad en la validación de cuestionarios relacionados con la salud. Med. Clin. 122, 21–27. doi: 10.1157/13057542
Beck, A. T., Epstein, N., Brown, G., and Steer, R. A. (1988). An inventory for measuring clinical anxiety: psychometric properties. J. Consult. Clin. Psychol. 56, 893–897. doi: 10.1037/0022-006X.56.6.893
Beck, A. T., Steer, R. A., and Brown, G. K. (1996). Manual for the Beck depression inventory-II. San Antonio, TX: Psychological Corporation.
Belar, A., Arantzamendi, M., Rodríguez-Núñez, A., Santesteban, Y., Martinez, M., López-Saca, M., et al. (2019). Multicenter study of the psychometric properties of the new demoralization scale (DS-II) in Spanish-speaking advanced Cancer patients. J. Pain Symptom Manag. 57, 627–634. doi: 10.1016/j.jpainsymman.2018.11.016
Brenlla, M. E., Messina, V. M., and Aranguren, M. (2013). Adaptación para Buenos Aires de la Escala de Orientaciones Generales de Causalidad (General causality orientations scale - GCOS). Interdisciplinaria 30, 65–84. doi: 10.16888/interd.2013.30.1.4
Cabrera, V., Martín-Aragón, M., Terol, M. D. C., Núñez, R., and Pastor, M. D. L. Á. (2015). La Escala de Ansiedad y Depresión Hospitalaria (HAD) en fibromialgia: análisis de sensibilidad y especificidad. Ter Psicol. 33, 181–193. doi: 10.4067/S0718-48082015000300003
Caci, H., Baylé, F. J., Mattei, V., Dossios, C., Robert, P., and Boyer, P. (2003). How does the hospital and anxiety and depression scale measure anxiety and depression in healthy subjects? Psychiatry Res. 118, 89–99. doi: 10.1016/S0165-1781(03)00044-1
Campo-Arias, A., and Oviedo, H. C. (2008). Revisión/Review Propiedades Psicométricas de una Escala: la Consistencia Interna. Rev. Salud Publica 10, 831–839. doi: 10.1590/S0124-00642008000500015
Christensen, A. V., Dixon, J. K., Juel, K., Ekholm, O., Rasmussen, T. B., Borregaard, B., et al. (2020). Psychometric properties of the Danish hospital anxiety and depression scale in patients with cardiac disease: results from the DenHeart survey. Health Qual. Life Outcomes 18:9. doi: 10.1186/s12955-019-1264-0
Cosco, T. D., Doyle, F., Ward, M., and McGee, H. (2012). Latent structure of the hospital anxiety and depression scale: a 10-year systematic review. J. Psychosom. Res. 72, 180–184. doi: 10.1016/j.jpsychores.2011.06.008
Czerwiński, S. K., Mackiewicz, J. J., Mytlewska, W. M., and Atroszko, P. A. (2020). Factorial validity, measurement invariance and concurrent validity of hospital anxiety and depression scale in a sample of polish undergraduate students. Psychiatr. Psychol. Klin. 20, 13–18. doi: 10.15557/PiPK.2020.0002
Dominguez-Lara, S. A. (2014). ¿Matrices Policóricas/Tetracóricas o Matrices Pearson? Un estudio metodológico. Rev. Argent. Cienc. Comport. 6, 39–48. doi: 10.32348/1852.4206.v6.n1.6357
Dominguez-Lara, S., and Rodriguez, A. (2017). Índices estadísticos de modelos bifactor. Interacciones 3, 59–65. doi: 10.24016/2017.v3n2.51
Dunbar, M., Ford, G., Hunt, K., and Der, G. (2000). A confirmatory factor analysis of the hospital anxiety and depression scale: comparing empirically and theoretically derived structures. Br. J. Clin. Psychol. 39, 79–94. doi: 10.1348/014466500163121
Ehlers, S. L., Davis, K., Bluethmann, S. M., Quintiliani, L. M., Kendall, J., Ratwani, R. M., et al. (2018). Screening for psychosocial distress among patients with cancer: implications for clinical practice, healthcare policy, and dissemination to enhance cancer survivorship. Transl. Behav. Med. 9, 282–291. doi: 10.1093/tbm/iby123
Emons, W. H. M., Sijtsma, K., and Pedersen, S. S. (2010). Dimensionality of the hospital anxiety and depression scale (HADS) in cardiac patients: comparison of Mokken scale analysis and factor analysis. Assessment 19, 337–353. doi: 10.1177/1073191110384951
Fillion, L., Gélinas, C., Simard, S., Savard, J., and Gagnon, P. (2003). Validation evidence for the French Canadian adaptation of the multidimensional fatigue inventory as a measure of Cancer-related fatigue. Cancer Nurs. 26, 143–154. doi: 10.1097/00002820-200304000-00008
Fong, T. C. T., and Ho, R. T. H. (2014). Testing gender invariance of the hospital anxiety and depression scale using the classical approach and Bayesian approach. Qual. Life Res. 23, 1421–1426. doi: 10.1007/s11136-013-0594-3
Friedman, S., Samuelian, J.-C., Lancrenon, S., Even, C., and Chiarelli, P. (2001). Three-dimensional structure of the hospital anxiety and depression scale in a large French primary care population suffering from major depression. Psychiatry Res. 104, 247–257. doi: 10.1016/S0165-1781(01)00309-2
Gale, C. R., Allerhand, M., Sayer, A. A., Cooper, C., Dennison, E. M., Starr, J. M., et al. (2010). The structure of the hospital anxiety and depression scale in four cohorts of community-based, healthy older people: the HALCyon program. Int. Psychogeriatr. 22, 559–571. doi: 10.1017/S1041610210000256
Galindo Vázquez, O., Benjet, C., Juárez García, F., Rojas Castillo, E., Riveros Rosas, A., Aguilar Ponce, J. L., et al. (2015a). Propiedades psicométricas de la Escala Hospitalaria de Ansiedad y Depresión (HADS) en una población de pacientes oncológicos mexicanos. Salud Ment. 38, 253–258. doi: 10.17711/sm.0185-3325.2015.035
Galindo Vázquez, Ó., Meneses García, A., Herrera Gómez, Á., Caballero Tinoco, M., and Aguilar Ponce, J. L. (2015b). Escala Hospitalaria de Ansiedad y Depresión (HADS) en cuidadores primarios informales de pacientes con cáncer: propiedades psicométricas. Psicooncología 12, 383–392. doi: 10.5209/rev_PSIC.2015.v12.n2-3.51016
GBD 2019 Mental Disorders Collaborators, (2022). Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet Psychiatry 9, 137–150. doi: 10.1016/s2215-0366(21)00395-3
Herrero, M. J., Blanch, J., Peri, J. M., De Pablo, J., Pintor, L., and Bulbena, A. (2003). A validation study of the hospital anxiety and depression scale (HADS) in a Spanish population. Gen. Hosp. Psychiatry 25, 277–283. doi: 10.1016/s0163-8343(03)00043-4
Hinz, A., Mehnert, A., Ernst, J., Herschbach, P., and Schulte, T. (2015). Fear of progression in patients 6 months after cancer rehabilitation—a validation study of the fear of progression questionnaire FoP-Q-12. Support. Care Cancer 23, 1579–1587. doi: 10.1007/s00520-014-2516-5
Hinz, A., Mehnert, A., Kocalevent, R. D., Brähler, E., Forkmann, T., Singer, S., et al. (2016). Assessment of depression severity with the PHQ-9 in cancer patients and in the general population. BMC Psychiatry 16:22. doi: 10.1186/s12888-016-0728-6
Hofmann, S. G., Sawyer, A. T., Fang, A., and Asnaani, A. (2012). Emotion dysregulation model of mood and anxiety disorders. Depress. Anxiety 29, 409–416. doi: 10.1002/da.21888
Howell, D., Keshavarz, H., Esplen, M., Hack, T., Hamel, M., Howes, J., et al. (2015). A pan-Canadian practice guideline and algorithm: screening, assessment, and supportive care of adults with cancer-related fatigue. Curr. Oncol. 20, e233–e246. doi: 10.3747/co.20.1302
Hsu, K. J., Beard, C., Rifkin, L., Dillon, D. G., Pizzagalli, D. A., and Björgvinsson, T. (2015). Transdiagnostic mechanisms in depression and anxiety: the role of rumination and attentional control. J. Affect. Disord. 188, 22–27. doi: 10.1016/j.jad.2015.08.008
Humphris, G. M., Watson, E., Sharpe, M., and Ozakinci, G. (2018). Unidimensional scales for fears of cancer recurrence and their psychometric properties: the FCR4 and FCR7. Health Qual. Life Outcomes 16:30. doi: 10.1186/s12955-018-0850-x
Hunt-Shanks, T., Blanchard, C., Reid, R., Fortier, M., and Cappelli, M. (2010). A psychometric evaluation of the hospital anxiety and depression scale in cardiac patients: addressing factor structure and gender invariance. Br. J. Health Psychol. 15, 97–114. doi: 10.1348/135910709X432745
Iani, L., Lauriola, M., and Costantini, M. (2014). A confirmatory bifactor analysis of the hospital anxiety and depression scale in an Italian community sample. Health Qual. Life Outcomes 12:84. doi: 10.1186/1477-7525-12-84
Kirkova, J., Aktas, A., Walsh, D., and Davis, M. P. (2011). Cancer symptom clusters: clinical and research methodology. J. Palliat. Med. 14, 1149–1166. doi: 10.1089/jpm.2010.0507
Lee, M. S., Tyson, D. M., Gonzalez, B. D., Small, B. J., Lechner, S. C., Antoni, M. H., et al. (2018). Anxiety and depression in Spanish-speaking Latina cancer patients prior to starting chemotherapy. Psycho-Oncology 27, 333–338. doi: 10.1002/pon.4462
Li, C.-H. (2016). Confirmatory factor analysis with ordinal data: comparing robust maximum likelihood and diagonally weighted least squares. Behav. Res. Methods 48, 936–949. doi: 10.3758/s13428-015-0619-7
Li, Q., Lin, Y., Hu, C., Xu, Y., Zhou, H., Yang, L., et al. (2016). The Chinese version of hospital anxiety and depression scale: psychometric properties in Chinese cancer patients and their family caregivers. Eur. J. Oncol. Nurs. 25, 16–23. doi: 10.1016/j.ejon.2016.09.004
Limonero, J. T., Mateo, D., Maté-Méndez, J., González-Barboteo, J., Bayés, R., Bernaus, M., et al. (2012). Evaluación de las propiedades psicométricas del cuestionario de Detección de Malestar Emocional (DME) en pacientes oncológicos. Gac. Sanit. 26, 145–152. doi: 10.1016/j.gaceta.2011.07.016
Lin, X., Chen, Z., Jin, L., Gao, W., Qu, B., Zuo, Y., et al. (2017). Rasch analysis of the hospital anxiety and depression scale among Chinese cataract patients. PLoS One 12:e0185287. doi: 10.1371/journal.pone.0185287
Luciano, J. V., Barrada, J. R., Aguado, J., Osma, J., and García-Campayo, J. (2014). Bifactor analysis and construct validity of the HADS: a cross-sectional and longitudinal study in fibromyalgia patients. Psychol. Assess. 26, 395–406. doi: 10.1037/a0035284
Mansell, W., Harvey, A., Watkins, E., and Shafran, R. (2009). Conceptual foundations of the transdiagnostic approach to CBT. J. Cogn. Psychother. 23, 6–19. doi: 10.1891/0889-8391.23.1.6
Martínez López, P., Durá Ferrandis, E., Andreu Vaillo, Y., Galdón Garrido, M. J., Murgui Pérez, S., and Ibáñez Guerra, E. (2012). Structural validity and distress screening potential of the hospital anxiety and depression scale in cancer. Int. J. Clin. Health Psychol. 12, 435–447.
Maters, G. A., Sanderman, R., Kim, A. Y., and Coyne, J. C. (2013). Problems in cross-cultural use of the hospital anxiety and depression scale: “no butterflies in the desert”. PLoS One 8:e70975. doi: 10.1371/journal.pone.0070975
Matsudaira, T., Igarashi, H., Kikuchi, H., Kano, R., Mitoma, H., Ohuchi, K., et al. (2009). Factor structure of the hospital anxiety and depression scale in Japanese psychiatric outpatient and student populations. Health Qual. Life Outcomes 7:42. doi: 10.1186/1477-7525-7-42
Milligan, F., Martinez, F., Aal, S. H. M. A., Ahmed, S. A., Joby, B., Matalam, J. S., et al. (2018). Assessing anxiety and depression in cancer patients. Br. J. Nurs. 27, S18–S23. doi: 10.12968/bjon.2018.27.10.S18
Mitchell, A. J., Chan, M., Bhatti, H., Halton, M., Grassi, L., Johansen, C., et al. (2011). Prevalence of depression, anxiety, and adjustment disorder in oncological, haematological, and palliative-care settings: a meta-analysis of 94 interview-based studies. Lancet Oncol. 12, 160–174. doi: 10.1016/S1470-2045(11)70002-X
Mukaka, M. M. (2012). Statistics corner: a guide to appropriate use of correlation coefficient in medical research. Malawi Med. J. 24, 69–71
Muñiz, J., Elosua, P., and Hambleton, R. K. (2013). Directrices para la traducción y adaptación de los tests: segunda edición. Psicothema 2, 151–157. doi: 10.7334/psicothema2013.24
Mystakidou, K., Tsilika, E., Parpa, E., Galanos, A., and Vlahos, L. (2007a). Psychometric properties of the impact of event scale in Greek Cancer patients. J. Pain Symptom Manag. 33, 454–461. doi: 10.1016/j.jpainsymman.2006.09.023
Mystakidou, K., Tsilika, E., Parpa, E., Sakkas, P., and Vlahos, L. (2009). The psychometric properties of the Greek version of the state-trait anxiety inventory in cancer patients receiving palliative care. Psychol. Health 24, 1215–1228. doi: 10.1080/08870440802340172
Mystakidou, K., Tsilika, E., Parpa, E., Smyrniotis, V., Galanos, A., and Vlahos, L. (2007b). Beck depression inventory: exploring its psychometric properties in a palliative care population of advanced cancer patients. Eur. J. Cancer Care 16, 244–250. doi: 10.1111/j.1365-2354.2006.00728.x
Nezlek, J. B., Rusanowska, M., Holas, P., and Krejtz, I. (2019). The factor structure of a polish language version of the hospital anxiety depression scale (HADS). Curr. Psychol. 40, 2318–2326. doi: 10.1007/s12144-019-0164-0
Norton, S., Cosco, T., Doyle, F., Done, J., and Sacker, A. (2013). The hospital anxiety and depression scale: a meta confirmatory factor analysis. J. Psychosom. Res. 74, 74–81. doi: 10.1016/j.jpsychores.2012.10.010
Norton, P. J., and Paulus, D. J. (2017). Transdiagnostic models of anxiety disorder: theoretical and empirical underpinnings. Clin. Psychol. Rev. 56, 122–137. doi: 10.1016/j.cpr.2017.03.004
Preljevic, V. T., Østhus, T. B., Sandvik, L., Opjordsmoen, S., Nordhus, I. H., Os, I., et al. (2012). Screening for anxiety and depression in dialysis patients: comparison of the hospital anxiety and depression scale and the Beck depression inventory. J. Psychosom. Res. 73, 139–144. doi: 10.1016/j.jpsychores.2012.04.015
Putnick, D. L., and Bornstein, M. H. (2016). Measurement invariance conventions and reporting: the state of the art and future directions for psychological research. Dev. Rev. 41, 71–90. doi: 10.1016/j.dr.2016.06.004
Quintana, J. M., Padierna, A., Esteban, C., Arostegui, I., Bilbao, A., and Ruiz, I. (2003). Evaluation of the psychometric characteristics of the Spanish version of the hospital anxiety and depression scale. Acta Psychiatr. Scand. 107, 216–221. doi: 10.1034/j.1600-0447.2003.00062.x
Reda, A. A. (2011). Reliability and validity of the Ethiopian version of the hospital anxiety and depression scale (HADS) in HIV infected patients. PLoS One 6:e16049. doi: 10.1371/journal.pone.0016049
Rodriguez, A., Reise, S. P., and Haviland, M. G. (2016). Evaluating bifactor models: calculating and interpreting statistical indices. Psychol. Methods 21, 137–150. doi: 10.1037/met0000045
Rooney, A. G., McNamara, S., Mackinnon, M., Fraser, M., Rampling, R., Carson, A., et al. (2012). Screening for major depressive disorder in adults with cerebral glioma: an initial validation of 3 self-report instruments. Neuro-Oncology 15, 122–129. doi: 10.1093/neuonc/nos282
Schellekens, M. P. J., van den Hurk, D. G. M., Prins, J. B., Molema, J., van der Drift, M. A., and Speckens, A. E. M. (2016). The suitability of the hospital anxiety and depression scale, distress thermometer and other instruments to screen for psychiatric disorders in both lung cancer patients and their partners. J. Affect. Disord. 203, 176–183. doi: 10.1016/j.jad.2016.05.044
Schellekens, M. P. J., Wolvers, M. D. J., Schroevers, M. J., Bootsma, T. I., Cramer, A. O. J., and van der Lee, M. L. (2020). Exploring the interconnectedness of fatigue, depression, anxiety and potential risk and protective factors in cancer patients: a network approach. J. Behav. Med. 43, 553–563. doi: 10.1007/s10865-019-00084-7
Shin, J., Goo, A., Ko, H., Kim, J.-H., Lim, S.-U., Lee, H.-K., et al. (2017). Validation study for the Korean version of fear of Cancer recurrence inventory. J. Korean Med. Sci. 32, 1792–1799. doi: 10.3346/jkms.2017.32.11.1792
Siu, A. L., Bibbins-Domingo, K., Grossman, D. C., Baumann, L. C., Davidson, K. W., Ebell, M., et al. (2016). Screening for depression in adults: US preventive services task Force recommendation statement. JAMA 315, 380–387. doi: 10.1001/jama.2015.18392
Stott, J., Orrell, M., and Charlesworth, G. (2017a). Validity and usefulness of the hospital anxiety and depression scale in Carers of people with dementia: evidence from confirmatory factor analysis, concurrent validity, and measurement invariance in a large sample. Am. J. Geriatr. Psychiatry 25, 1270–1280. doi: 10.1016/j.jagp.2017.05.017
Stott, J., Spector, A., Orrell, M., Scior, K., Sweeney, J., and Charlesworth, G. (2017b). Limited validity of the hospital anxiety and depression scale (HADS) in dementia: evidence from a confirmatory factor analysis. Int. J. Geriatr. Psychiatry 32, 805–813. doi: 10.1002/gps.4530
Suárez-Mendoza, A., Petersen-Aranguren, F., Almeida-Velasco, A., Robles-García, R., Camacho, Á., and Fresán-Orellana, A. (2019). Psychometric evaluation of the hospital anxiety and depression scale in Mexican adults with ischemic and hypertensive cardiomyopathy. Arch. Cardiol. Mex. 89, 221–226. doi: 10.24875/acme.M19000060
Terol-Cantero, M. C., Cabrera-Perona, V., and Martín-Aragón, M. (2015). Hospital anxiety and depression scale (HADS) review in Spanish samples. An. Psicol. 31:494. doi: 10.6018/analesps.31.2.172701
Touzani, R., Mancini, J., Troïan, J., Bouhnik, A.-D., Cussenot, O., Gravis, G., et al. (2019). Adaptation and validation of the memorial anxiety scale for prostate cancer (MAX-PC) in a sample of French men. J. Patient Rep. Outcomes 3:60. doi: 10.1186/s41687-019-0150-1
Toyama, M., Castillo, H., Galea, J. T., Brandt, L. R., Mendoza, M., Herrera, V., et al. (2017). Peruvian Mental health reform: a framework for scaling-up Mental health services. Int. J. Health Policy Manag. 6, 501–508. doi: 10.15171/ijhpm.2017.07
van Dijk, S. E. M., Adriaanse, M. C., van der Zwaan, L., Bosmans, J. E., van Marwijk, H. W. J., van Tulder, M. W., et al. (2018). Measurement properties of depression questionnaires in patients with diabetes: a systematic review. Qual. Life Res. 27, 1415–1430. doi: 10.1007/s11136-018-1782-y
Villarreal-Zegarra, D., Cabrera-Alva, M., Carrillo-Larco, R. M., and Bernabe-Ortiz, A. (2020). Trends in the prevalence and treatment of depressive symptoms in Peru: a population-based study. BMJ Open 10:e036777. doi: 10.1136/bmjopen-2020-036777
Villoria, E., and Lara, L. (2018). Assessment of a hospital anxiety and depression scale for cancer patients. Rev. Med. Chile 146, 300–307. doi: 10.4067/s0034-98872018000300300
Vizioli, N., and Pagano, P. (2020). Adaptation of the Beck anxiety inventory in population of Buenos Aires. Interacciones 6:e171. doi: 10.24016/2020.v6n3.171
Vodermaier, A., Linden, W., and Siu, C. (2009). Screening for emotional distress in Cancer patients: a systematic review of assessment instruments. JNCI J. Natl. Cancer Inst. 101, 1464–1488. doi: 10.1093/jnci/djp336
Vodermaier, A., and Millman, R. D. (2011). Accuracy of the hospital anxiety and depression scale as a screening tool in cancer patients: a systematic review and meta-analysis. Support. Care Cancer 19, 1899–1908. doi: 10.1007/s00520-011-1251-4
Waqas, A., Aedma, K. K., Tariq, M., Meraj, H., and Naveed, S. (2019). Validity and reliability of the Urdu version of the hospital anxiety & depression scale for assessing antenatal anxiety and depression in Pakistan. Asian J. Psychiatr. 45, 20–25. doi: 10.1016/j.ajp.2019.08.008
Xiong, P., Liu, M., Liu, B., and Hall, B. J. (2022). Trends in the incidence and DALYs of anxiety disorders at the global, regional, and national levels: estimates from the global burden of disease study 2019. J. Affect. Disord. 297, 83–93. doi: 10.1016/j.jad.2021.10.022
Yan, R., Xia, J., Yang, R., Lv, B., Wu, P., Chen, W., et al. (2019). Association between anxiety, depression, and comorbid chronic diseases among cancer survivors. Psycho-Oncology 28, 1269–1277. doi: 10.1002/pon.5078
Yang, Z., Huang, X., Liu, X., Hou, J., Wu, W., Song, A., et al. (2019). Psychometric properties and factor structure of the Chinese version of the hospital anxiety and depression scale in people living with HIV [original research]. Front. Psychiatry 10:346. doi: 10.3389/fpsyt.2019.00346
Zarragoitía Alonso, I. (2013). Sex and gender differences in depression - proclivity in women. Medwave 13:e5651. doi: 10.5867/medwave.2013.03.5651
Keywords: depression, anxiety, cancer, psychometrics, Peru, hospitals
Citation: Vilela-Estrada AL, Villarreal-Zegarra D, Copez-Lonzoy A, Esenarro-Valencia L, Sánchez-Ramírez JC, Lamas-Delgado F, Ambrosio-Melgarejo J, Reategui-Rivera CM and Finkelstein J (2025) Psychometric properties of the Spanish version of the hospital anxiety and depression scale in cancer patients. Front. Psychol. 15:1497946. doi: 10.3389/fpsyg.2024.1497946
Edited by:
Fadia Shaya, University of Maryland, Baltimore, United StatesReviewed by:
Andreas Hinz, Leipzig University, GermanyMd Fitrat Hossain, University of Maryland, Baltimore, United States
Copyright © 2025 Vilela-Estrada, Villarreal-Zegarra, Copez-Lonzoy, Esenarro-Valencia, Sánchez-Ramírez, Lamas-Delgado, Ambrosio-Melgarejo, Reategui-Rivera and Finkelstein. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: David Villarreal-Zegarra, ZGF2aWQudmlsbGFycmVhbEB1dGFoLmVkdQ==
†These authors share first authorship
‡ORCID: Ana L. Vilela-Estrada, https://orcid.org/0000-0001-5647-465X
David Villarreal-Zegarra, https://orcid.org/0000-0002-2222-4764
Loida Esenarro-Valencia, https://orcid.org/0000-0002-9978-0072
José C. Sánchez-Ramírez, https://orcid.org/0000-0002-5713-4566
Fernando Lamas-Delgado, https://orcid.org/0000-0001-6025-8415
Anthony Copez-Lonzoy, https://orcid.org/0000-0003-4761-4272
C. Mahony Reategui-Rivera, https://orcid.org/0000-0002-4030-8777
Joseph Finkelstein, https://orcid.org/0000-0002-8084-7441