 Mariagrazia Di Giuseppe1
Mariagrazia Di Giuseppe1 Gabriele Lo Buglio2*
Gabriele Lo Buglio2* Erika Cerasti2
Erika Cerasti2 Tommaso Boldrini3
Tommaso Boldrini3 Ciro Conversano4
Ciro Conversano4 Vittorio Lingiardi2†
Vittorio Lingiardi2† Annalisa Tanzilli2*†
Annalisa Tanzilli2*†- 1Department of History, Humanities and Society, University of Rome Tor Vergata, Rome, Italy
- 2Department of Dynamic and Clinical Psychology, and Health Studies, Faculty of Medicine and Psychology, Sapienza University of Rome, Rome, Italy
- 3Department of Psychology and Educational Science, Pegaso Telematic University, Naples, Italy
- 4Department of Surgical, Medical and Molecular Pathology, Critical and Care Medicine, University of Pisa, Pisa, Italy
Background: Defense mechanisms play a crucial role in depression and anxiety. The current study aimed at estimating the network structure of defense mechanisms in individuals with symptoms of depression and anxiety to understand the most central defenses and relevant connections. Moreover, we aimed at examining the associations between defense mechanisms and symptoms.
Methods: We employed the Symptom Checklist-90 to recruit 655 individuals with depressive and anxiety symptoms during the first wave of the COVID-2019 Pandemic in Italy. Defense mechanisms were assessed with the DMRS-SR-30.
Results: Results showed a main component in the network graph featuring 16 defense mechanisms. Self-assertion was the most central node in the network, displaying positive and negative connections with an array of mature and immature defenses, respectively. Among immature defenses, passive aggression was the most interconnected node. Some mature defenses (i.e., humor, affiliation, and sublimation) were not connected to other nodes. A range of defense mechanisms were associated with anxiety and depressive symptoms.
Conclusions: This is the first research effort supporting the conceptualization of defense mechanisms as a complex system. Results suggest that defense mechanisms of the same cluster (e.g., mature defenses) play different roles in the network. Central defenses (i.e., self-assertion and passive aggression) detected in this study may be promising intervention targets.
Introduction
According to the main theoretical conceptualizations, defense mechanisms (or, simply, defenses) are pivotal concepts to understand psychological functioning and human development (Vaillant, 2000; McWilliams and Weinberger, 2003; Cramer, 2015; Di Giuseppe and Lingiardi, 2023). Defenses operate mostly, but not exclusively, out of consciousness (Perry, 1990), mediating the relationship between emotional conflicts and external stressors (Perry, 2014). Fueled by seminal conceptualizations of Freud (1894), a variety of theoretical contributions and research efforts have been generated on this topic, leading to well-established models assisting therapists and researchers in the identification of defense mechanisms in clinical and research settings. Particularly, the hierarchical model, proposed by Vaillant (1971, 1977) and operationalized by Perry in the Defense Mechanisms Rating Scales (DMRS; Perry, 1990), collocates defenses in a continuum between the maturity and the immaturity pole; in this model, most mature defenses are associated with adaptive responses and high awareness and resilience, while most immature defenses are associated with maladaptive responses, low awareness and psychological distress (Perry et al., 2022; Rice and Hoffman, 2014; Tanzilli et al., 2022; Békés et al., 2023; Carone et al., 2023; Martino et al., 2023; Messina et al., 2023).
The DMRS hierarchy describes 30 defense mechanisms organized into seven defense levels, each of which has a specific defensive function that protects the individual from anxiety, or a sense of threat from internal or external sources, or conflicts (Perry, 2014). From the least to the most adaptive defense levels are: (1) Action defense level, including defenses as acting out, passive aggression, and help-rejecting complaining; (2) Major image-distorting defense level, including defenses as splitting of self-image, splitting of object's image, and projective identification; (3) Disavowal defense level, including defenses as denial, rationalization, projection, and autistic fantasy; (4) Minor image-distorting defense level, including defenses as idealization of self and others' image, devaluation of self and others' image, and omnipotence; (5) Neurotic defense level, including defenses as repression, dissociation, reaction formation, and displacement; (6) Obsessional defense level, including defenses as isolation of affects, intellectualization, and undoing; and (7) High-adaptive defense level, including defenses as affiliation, altruism, anticipation, humor, self-assertion, self-observation, sublimation, and suppression. All DMRS measures, including the one applied to this study, refer to the hierarchical model (Di Giuseppe, 2024). Furthermore, defense levels can be organized into three defensive categories of maturity, namely mature, neurotic, and immature. The immature defensive category is the least adaptive and includes defenses belonging to levels 1 to 4. The neurotic defensive category is in the middle of the hierarchy and includes defenses belonging to levels 5 and 6. Finally, the mature defensive category is on the top of the hierarchy and includes defenses belonging to level 7. Since its deep, comprehensive and empirical-based conceptualization of defenses, the DMRS has inspired the inclusion of specific axis for defense mechanisms assessment in widely used diagnostic manuals (American Psychiatric Association, 1994; Lingiardi and McWilliams, 2017) and it is nowadays known as the closest to a gold-standard method for studying defenses (Silverman and Aafjes-van Doorn, 2023).
Several studies have highlighted the association between specific defense mechanisms and depression (Høglend and Perry, 1998; DeFife and Hilsenroth, 2005; Olson et al., 2009; Martino et al., 2020; Fiorentino et al., 2024) and anxiety (Olson et al., 2009). For example, Fiorentino et al. (2024) underscored the over-reliance on non-mature defenses (i.e., neurotic and immature defenses) in depressive individuals. Moreover, Olson et al. (2009) highlighted that panic disorder is characterized by dissociation.
Notably, depression and anxiety represent the most widespread mental health concerns and often co-occur (Galli et al., 2019; Boldrini et al., 2020; World Health Organization, 2022; Ierardi et al., 2023; König et al., 2023). Such a co-occurrence phenomenon has been referred to as comorbidity (Gelo et al., 2015a,b; Lenzo et al., 2020; Nordgaard et al., 2023; Lo Buglio et al., 2024), a concept that may be considered at least partially artifactual (Borsboom and Cramer, 2013; Vita et al., 2020; Borsboom et al., 2021; Martino et al., 2021). Even though the interconnections between symptoms of comorbid mental disorders have been the focus of several studies (Gelo and Manzo, 2015; Conversano et al., 2023; Boldrini et al., 2024), little knowledge is available on the complex interplay of defense mechanisms in individuals with both depressive and anxiety symptoms.
With the aim of advancing the knowledge on the complex interactions among variables (Gelo et al., 2012, 2015b; Casula et al., 2023; Klocek and Riháček, 2023; Parolin et al., 2023; Sergi et al., 2023), promising findings have been generated within the so-called “network approaches” focusing on associations between pairs of variables in the data, while conditioning on all the other variables (i.e., partial correlations, see “network analysis” section for details) (Borsboom, 2017; Borsboom et al., 2021). Recent advancements in the field provide statistical tools useful for the interpretation of both network properties (e.g., most central variables) and relevant links between them (Borsboom et al., 2021). As an example of a complex system, we can consider a flock of birds, in which the behavior of the former is the result (an “emerging property”) of the interplay of the latter (Borsboom et al., 2022). Similarly, defensive functioning originating from the complex interplay of defense mechanisms may be mirrored and represented by a network structure originated from the complex interconnections of defense mechanisms operating all together. However, even though complexity is (mostly) an implicit assumption of theories and models on defense mechanisms, complex models on defenses are still in their infancy. Research within the network approach may provide promising tools for the transdiagnostic assessment of individuals with depressive and anxiety symptoms, informing the identification of consistent intervention targets. Moreover, it could advance knowledge by explicitly framing defenses as complex systems in individuals with comorbid mental health conditions.
Aim
Given these premises, the current study aimed at investigating the defensive functioning of individuals with high levels of symptoms of depression and anxiety as a network structure, identifying defenses playing a relevant role in the network. Moreover, we also aimed at investigating the associations between defense mechanisms and depressive and anxiety symptoms.
Methods
Participants
Participants were extracted from a larger sample of 6,412 adult responders to an online survey launched to test the psychological impact of COVID-19 during the first wave of the pandemic. Previous studies have investigated participants' responses focusing on several socio-demographic and psychological aspects (Di Giuseppe et al., 2022). For the purpose of this study, we selected about 10% of the participants who self-reported to have high depression and anxiety symptoms at the time they responded to the survey (see Procedures). Selected responders were 655 in total, mostly female adults (N = 392; 59.8 %), while about 19.7% (N = 129) were male and 27.2% (N = 178) were either male or female younger than 30 years of age.
Measures
To evaluate defense mechanisms and symptoms of depression and anxiety we applied the Italian version of two well-validated self-report questionnaires as the DMRS-SR-30 and the SCL-90.
The Defense Mechanisms Rating Scales-Self-Report-30 (DMRS-SR-30; Di Giuseppe et al., 2020) is a 30-item questionnaire developed from the gold-standard DMRS theory (Perry, 1990, 2014) to self-assess the whole hierarchy of defense mechanisms (Di Giuseppe and Perry, 2021). The DMRS-SR-30 provides scores for the overall defensive functioning (ODF), three factors of defensive maturity, seven hierarchically ordered defense levels and 28 constituent defenses. Both the English and Italian version of the measure showed strong psychometric properties (Di Giuseppe et al., 2020; Prout et al., 2022), mostly replicated in the German (Volkert et al., 2022) and Turkish (Yilmaz et al., 2024) version of the scale.
The Symptoms Checklist-90 (SCL-90; Derogatis and Cleary, 1977) is a 90-item questionnaire developed to measure psychological symptoms and distress. It is designed to be appropriate for use with individuals from the community, as well as individuals with either medical or psychiatric conditions (Gomez et al., 2021). The SCL-90 involves nine primary symptom dimensions (i.e., somatization, obsessive-compulsive, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism), but in this study we considered only depression (DEP) and anxiety (ANX) subscales. Because it is one of the most comprehensive and widely used scales addressing psychopathological symptoms, the SCL-90 has been largely validated in several languages and populations, including Italian (Cassano et al., 1999; Prunas et al., 2012).
Procedures
Data were collected from March 13 to April 6, 2020, during the first lockdown imposed by the Italian Government to contrast COVID-19 pandemic spreading. Participants were recruited via social media using snowball sampling and they were asked to give their approval on personal data treatment for research purposes. All procedures followed the ethical standards and were approved by the Ethics Committee of the Local Institution.
Participant selection was made following the criteria published in reference to the Italian version of the Symptom Checklist-90-Revised (SCL-90-R; Sarno et al., 2011). From the best of our acknowledge, this is the only published documents indicating cut-off scores for single SCL subscales (i.e., low, moderate, and high level of symptoms), further differentiated by age (i.e. below vs. above 30 year of age) and gender (i.e., male vs. female). According to Sarno and colleagues' guidelines for determining high levels of depression and anxiety using the SCL-90-R (Sarno et al., 2011), Table 1 shows mean, standard deviation, and cut-off level for depression and anxiety among four subgroups of males and females. We included only individuals scoring above the cut-off levels that indicate the most severe symptoms of both anxiety and depression.
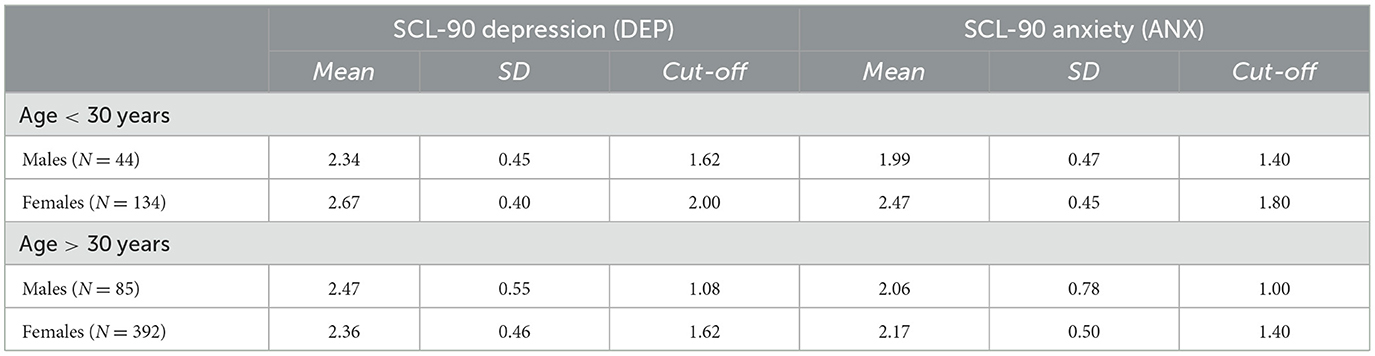
Table 1. Means, standard deviations and cut-offs for depression and anxiety.
Network analysis and correlations
A network approach was applied to investigate the interaction between different defense mechanisms. In network modeling, “node” refers to each variable included in the network structure while “edge” denotes a link between two nodes, representing the presence of a conditional dependence between the corresponding variables (dependence between two variables while controlling for all the other variables; Borsboom et al., 2021). If two nodes in the network are not connected through an edge, the corresponding variables are conditionally independent. Edges are estimated from partial correlations which, in turn, are computed from measured correlations (i.e., the correlation matrix). In this study all the defense mechanisms scores are evaluated with the DMRS-SR-30 as variables for the estimation of an undirected and weighted network. Black and red edges indicate positive and negative connections, respectively—-the ticker the edge, the stronger the connection. We used a Gaussian Graphical Model (GGM) and adopted the EBICglasso estimator, which shrinks to zero weak associations (dropped edges are not relevant to explain the data covariation structure). To examine the centrality of each defense mechanism in the network, we computed the following indices of centrality: (a) strength (i.e., the sum of the absolute edge weights for each node), closeness (i.e., the inverse of the sum of the distances of the target node from all remaining nodes) and betweenness (i.e., the number of shortest paths between any two nodes that pass through a specific node) (Opsahl et al., 2010; Costantini et al., 2015; Borsboom et al., 2021). To assess the robustness of the network structure, we estimated the correlation stability coefficient (CS; the maximum proportion of the sample that can be dropped with recalculated indices that correlate at least 0.7 with the indices of the whole original sample). A value of 0.25 is considered acceptable and a value of 0.50 is recommended by current methodological guidelines. Confidence intervals were computed with bootstrapping (number of boots = 2,500) to examine the variability of edge-weights. The network analysis was conducted in line with relevant instructions in literature (Costantini et al., 2015; Borsboom, 2017; Epskamp and Fried, 2018). We employed the packages qgraph and bootnet of the statistical program R (version 4.2.2; R Core Team, 2016).
Finally, we employed SPSS version 27.0 (IBM Corp, 2020) to compute the Pearson correlations between all DMRS-SR-30 subscales and the two SCL-90 subscales for depression and anxiety.
Results
Network of defense mechanisms
The network structure of defense mechanisms is displayed in Figure 1. Visual inspection revealed a main component including 16 nodes: Passive aggression (D3), Splitting of other's image (D4), Splitting of self-image (D5), Projective identification (D6), Autistic fantasy (D7), Projection (D8), Denial (D10), Devaluation (D13), Repression (D14), Dissociation (D15), Reaction formation (D16), Altruism (D22), Anticipation (D23), Self-assertion (D25), Self-observation (D26), and Suppression (D28). In contrast, the remaining nodes showed only one or no connection with other variables of the network. The correlation matrix and the centrality indices are shown in Supplementary Figure S1 and Figure 2, respectively. The highest node strength was observed for Self-assertion (D25), which was positively connected to Altruism (D22), Self-observation (D26), and Suppression (D28) and negatively connected to Passive aggression (D3), Splitting of self-image (D5), Autistic fantasy (D7), Projection (D8), Devaluation (D13), and Dissociation (D15). Among immature defense mechanisms (clusters 1–4 of the DMRS-SR-30), the defense with the highest node strength was Passive aggression (D3), which was positively connected to Splitting of other's image (D4) and Projective identification (D6) and negatively correlated to Altruism (D22), Anticipation (D23), Self-assertion (D25), Self-observation (D26), and Suppression (D28). The strongest connection was between Intellectualization (D19) and Isolation of affect (D20). Acting out (D1, a defense of the most immature cluster) was isolated from the main component of the network, showing a positive connection only with Help-rejecting complaining (D2; another defense of the most immature cluster). Several defense mechanisms did not exhibit significant connections with other variables of the network, including Affiliation (D21), Humor (D24), Sublimation (D27) (i.e., three mature defenses) Undoing (D18), Displacement (D17), and Rationalization (D9). Among the 16 defenses included in the main component, Autistic fantasy (D7), Projection (D8), Denial (D10), and Reaction formation (D16) displayed only weak connections with other nodes. Overall, defenses belonging to the same clusters of the DMRS-SR-30 played different roles in the network—for example, Self-Assertion (D25; a mature defense) was the most central node of the network, while Sublimation (D27; another mature defense) did not show any significant connection with any other variable; likewise Acting out (D1; an immature defense of the action level) and Help-rejecting complaining (D2; another defense of the action level) were strongly related to each other but remained isolated from Passive aggression (D3; the third defense of the action level), which was instead included in the network. CS was 0.35 for Strength (Supplementary Figure S2). The bootstrapped confidence intervals of the estimated edge weights are displayed in the Supplementary Figure S3.

Figure 1. Defense Network of individual with high level of depression and anxiety. Node colors refer to a priori symptom domains (see legend), and numbers refer to specific individual items (i.e., defense mechanisms). The associations are either positive (colored black) or negative (colored red), with thicker lines representing stronger associations. D1 Acting out, D2 Help-rejecting complaining, D3 Passive aggression, D4 Splitting of other's image, D5 Splitting of self-image, D6 Projective identification, D7 Autistic fantasy, D8 Projection, D9 Rationalization, D10 Denial, D11 Omnipotence, D12 Idealization, D13 Devaluation, D14 Repression, D15 Dissociation, 16 Reaction formation, D17 Displacement, D18 Undoing, D19 Intellectualization, D20 Isolation of affect, D21 Affiliation, D22 Altruism, D23 Anticipation, D24 Humor, D25 Self-assertion, D26 Self-observation, D27 Sublimation, and D28 Suppression.
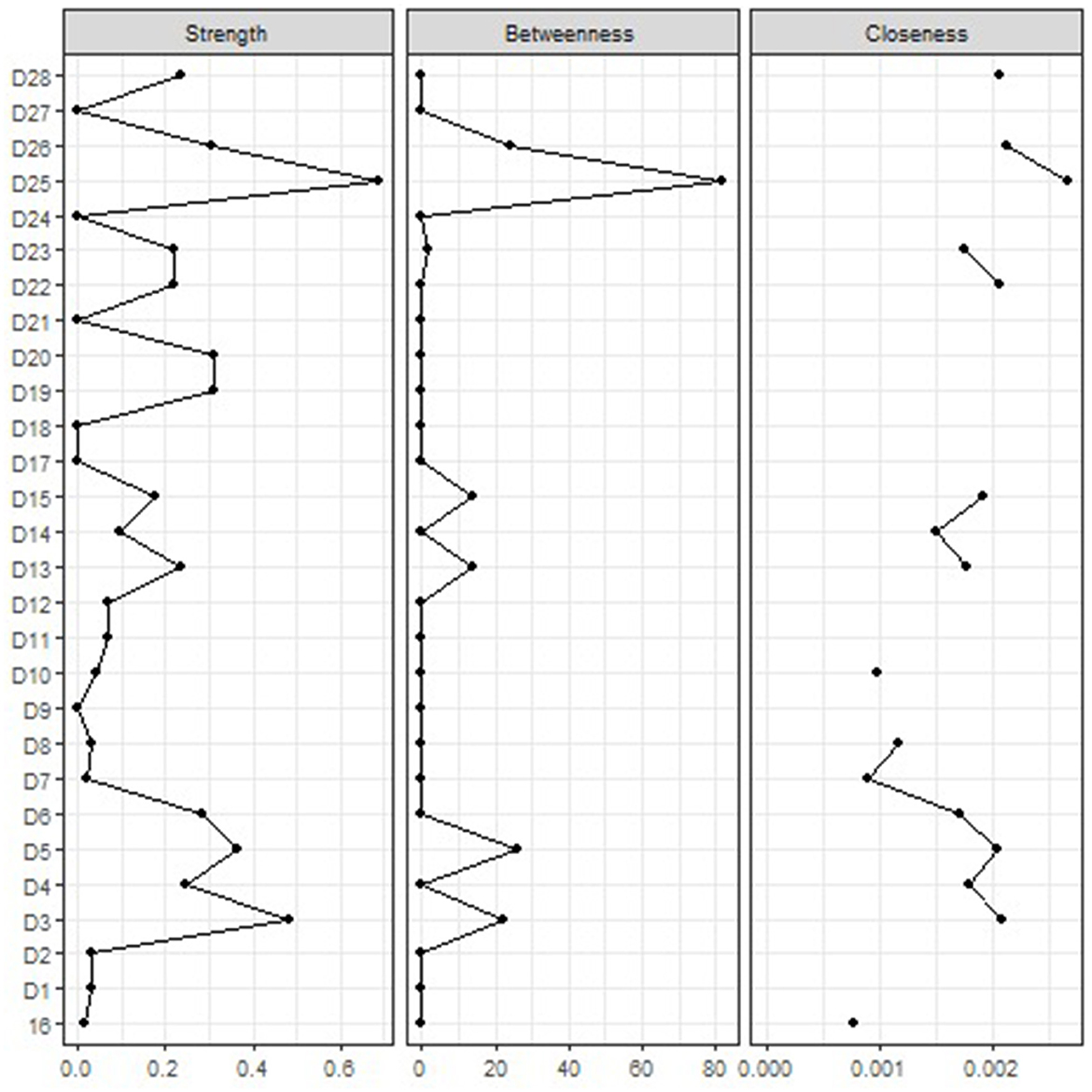
Figure 2. Centrality indices. Centrality indices (i.e., node strength, closeness and betweenness) are shown as standardized z-scores. Legend. D1 Acting out, D2 Help-rejecting complaining, D3 Passive aggression, D4 Splitting of other's image, D5 Splitting of self-image, D6 Projective identification, D7 Autistic fantasy, D8 Projection, D9 Rationalization, D10 Denial, D11 Omnipotence, D12 Idealization, D13 Devaluation, D14 Repression, D15 Dissociation, 16 Reaction formation, D17 Displacement, D18 Undoing, D19 Intellectualization, D20 Isolation of affect, D21 Affiliation, D22 Altruism, D23 Anticipation, D24 Humor, D25 Self-assertion, D26 Self-observation, D27 Sublimation, and D28 Suppression.
Associations between defenses and symptoms
To further understand results of the network analysis, we tested associations between defenses and symptoms of depression and anxiety. Table 2 shows Pearson correlations between all DMRS-SR-30 subscales and the two SCL-90 subscales for depression and anxiety. As expected, ODF and mature defenses (Factor 1) were negatively related to symptoms (r ranging from −0.17 to −0.29; all p < 0.01), while immature defenses (Factor 3) were positively related to both depression (r = 0.34; p < 0.01) and anxiety (r = 0.17; p < 0.01). Mental inhibition and avoidance defenses (Factor 2) was instead related to depression but unrelated to anxiety symptoms.
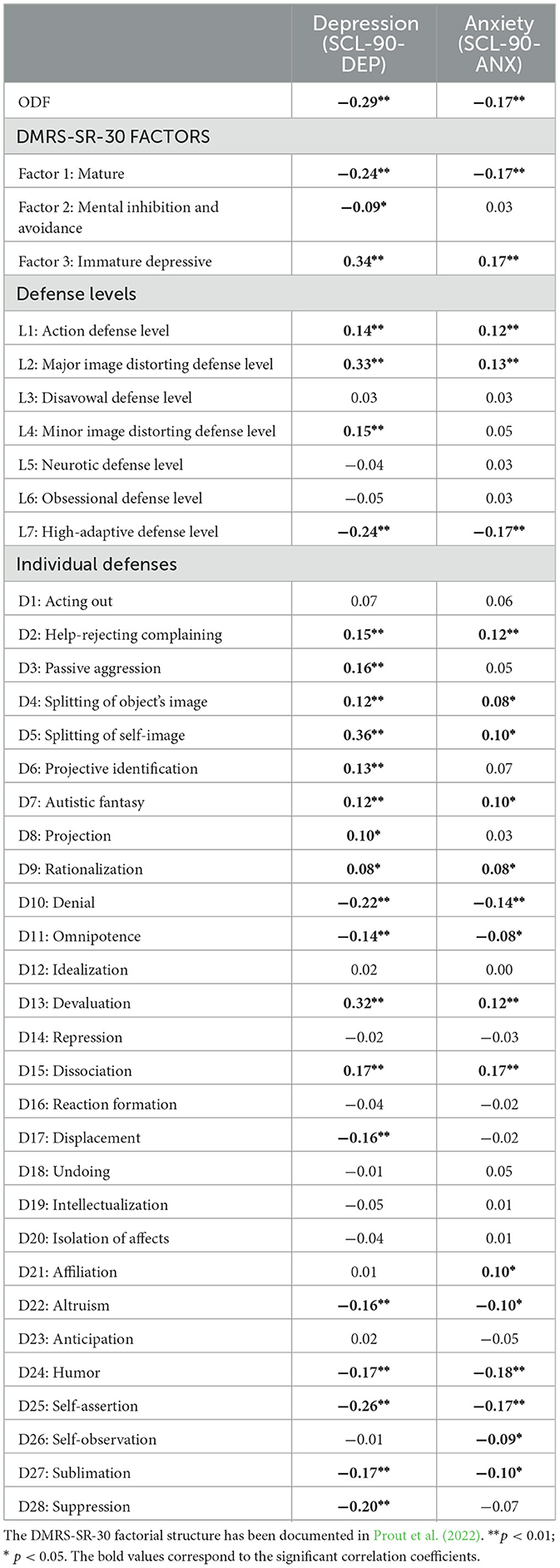
Table 2. Correlations between defenses and symptoms of depression and anxiety.
Among mature defenses, self-assertion (a central node in the network), humor, sublimation, and altruism were negatively associated with both symptoms. Moreover, suppression was also negatively related to depression, while affiliation and self-observation were negatively related to anxiety. Conversely, passive aggression, which resulted as another central node in the network, was positively associated with depression (r = 0.16; p < 0.01), together with most of the depressive defenses (i.e., help-rejecting complaining, splitting of self and object's image, projective identification, projection, and devaluation) and some other immature defenses (rationalization and autistic fantasy). Positive correlations between immature defenses and anxiety resulted in lower intensity and included only help-rejecting complaining, splitting of self and object's image, rationalization, autistic fantasy, and devaluation. Interestingly, the immature defenses denial (r ranging from −0.14 to −0.22; all p < 0.01) and omnipotence (r ranging from −0.08 to −0.14; p ranging from < 0.05 to < 0.01) and the neurotic defense dissociation (r = 0.17; p < 0.01) showed negative and positive association with symptoms, respectively. Finally, displacement was found negatively related to depression, while affiliation was found positively related to anxiety.
Discussion
The network structure
The present study encompasses the innovative representation of defense mechanisms as active components in a complex system (Borsboom et al., 2021) that mutually influence each other (Roefs et al., 2022) giving rise to the “emerging property” of defensive functioning.
Visual inspection of the network structure showed a main interacting component that includes defense mechanisms of different levels: mature, neurotic and immature defenses. This implies that the interaction between different defense mechanisms is not directly dependent on their level of maturity; conversely defenses characterized by the same level of maturity can play a very different role in the network. According to the network approach, defense mechanisms of the same cluster play different roles in the network structure. For example, humor and self-assertion, both mature defenses, play very different roles in the network: while self-assertion can affect several other defenses functioning through its connections, humor has no effect at all, resulting an isolated node. Similarly, passive aggression shows a relevant impact, but does not appear closely connected to the other defenses of the action defense level. In fact, the acting out mechanism was isolated, showing only a positive connection with help-rejecting complaining.
Centrality indices reveal that self-assertion is the most central node in the whole network, whereas passive aggression is the most central node while considering only immature defenses.
In our network structure, self-assertion showed positive connections with suppression, altruism and self-observation, and negative connections with passive aggression, dissociation and splitting of self-image. Individuals employing self-assertion deal “with emotional conflicts, or internal or external stressors, by expressing one's feelings and thoughts directly to achieve goal” (Di Giuseppe and Perry, 2021). Thus, based on our result, we may hypothesize that passive aggression, dissociation and splitting of self-image limit the capacity to be assertive in dealing with internal and external conflicts. Interestingly, while self-assertion is not manipulative or coercive, the individual employing passive aggression is resentful, hostile and expresses his feelings in an un-assertive way (Di Giuseppe and Perry, 2021). Notably, the use of self-assertion might hence be protective in individuals with depressive and anxiety symptoms because it allows the person to function without the anxiety or guilt associated with unexpressed emotions (Perry and Bond, 2017; Martino et al., 2019; de Roten et al., 2021).
As mentioned earlier, self-assertion was positively connected with three high-adaptive defenses. According to the hierarchical model of defense mechanisms and empirical investigations (e.g., Di Giuseppe and Perry, 2021; Perry et al., 2022; Tanzilli et al., 2021), mature defenses are associated with higher awareness, lower psychopathology, and the capability to cope in an optimal way with internal and external stressors.
Regarding immature defenses, passive aggression was positively connected with two defenses featuring in the Major Image-Distorting Defense Level: projective identification and splitting of other's image. According to our network structure, it may be hypothesized that passive aggression, splitting of other's image and projective identification can reinforce each other and generate a feedback loop in which the individual is “stuck” in an immature defensive stance, hindering the possibility to integrate different views, and to express anger in indirect ways and reacts to non-real (or partially real) threats (Prout et al., 2019; Di Giuseppe and Perry, 2021; Taubner et al., 2023).
Overall, our network structure suggests that, beyond symptom presentation, individuals with depressive and anxiety symptoms exhibit a range of interconnections among defenses which modulate responses to intrapersonal and interpersonal conflicts and stressors. Moreover, mature and immature defenses may play a crucial role in anxiety and depression, as both self-assertion and passive aggression were highly central in the network structure. Additional details on the role of defenses in the context of symptom presentation are reported in the Supplementary material S4.
Associations between defenses and symptoms
Two central nodes in the network, namely self-assertion and passive aggression, were negatively associated with depressive and anxiety symptoms and positively associated with depressive symptoms, respectively. These are crucial findings in light of the opposite (“conflicting”) role they play in the defensive functioning of highly depressed and anxious individuals. On one hand, passive aggression is characterized by a facade of overt compliance masking covert resistance toward others. For instance, the subject can fail to express themselves adequately (e.g., being silent for a long while), instead finding indirect and annoying ways to show their opposition to other's influence, which can be associated with depressive symptoms. On the other hand, self-assertion deals with emotional conflict through the direct expression of one's feelings or wishes without feeling guilty or ashamed if unsuccessful. An example could be when the subject can disagree with others and express opinions without being overly hostile, devaluing, or manipulative of others.
Implications
This study provides a network model of defense mechanisms of depression and anxiety. The interconnected nature of our network could resemble the complexity found in cognitive-behavioral models of depression and anxiety, which emphasize the interplay between thoughts, emotions, and behaviors and the impact of cognitive distortions on symptoms (Beck et al., 1979; Powers et al., 2017). Additionally, the Psychodynamic Diagnostic Manual −2nd Edition (Lingiardi and McWilliams, 2017) suggests that there is considerable complexity in the subjective experiences of symptom patterns in anxiety and depression, including affective states, cognitive patterns, somatic states, and relationship patterns.
Recognizing complexity has clinical implications. According to our findings, it could be argued that targeting defenses without relevant connections may not significantly improve defensive functioning. In contrast, psychotherapy targeting highly central defense mechanisms (i.e., self-assertion and passive aggression, as they play a crucial role in our network) might be a more promising strategy since central nodes display more links with other variables in the network. However, longitudinal studies are needed to test this hypothesis. Moreover, passive aggression and self-assertion are closely interconnected, suggesting that therapy could benefit from reducing passive aggression while enhancing self-assertion. This dual approach would help individuals navigate social contexts more effectively, manage stress, and build resilience, ultimately improving their capacity to adapt and positively influence their environment (Perry, 1990).
This study also advances theoretical and clinical understanding of defense mechanisms. A system where mature defenses influence each other could act as a protective factor, fostering emotion regulation and adaptive interpersonal skills. In contrast, a system where immature defenses influence each other could represent a risk factor, limiting resilience and flexibility.
Limitations and future research
Our findings should be read in light of the study limitations. One limitation is that participants were recruited during the first wave of the COVID-19 pandemic, a period marked by increased stress and uncertainty (World Health Organization, 2022). This prompted the use of both mature defenses, which played a protective role, and immature defenses, which were associated with mental health symptoms (Di Giuseppe et al., 2021). To corroborate our findings, replication studies conducted in non-pandemic periods are warranted.
Participants were recruited through an online survey, involving an unequal proportion of women and men in our sample (Di Giuseppe et al., 2021). Although this recruitment procedure is increasingly used in research (Altuncu et al., 2023) and typically contemplates this sample imbalance, this may have led to a slight overrepresentation of defense mechanisms more frequently associated with women. For example, acting out and projection, which are more prevalent among men, may have been underrepresented, while women tend to use more internalizing defenses, such as repression (Cramer, 2000). These documented differences in the use of defenses across genders may have impacted the interconnections in the network; however, further research is warranted.
Furthermore, the use of self-reported measures might have biased the self-assessment of psychological variables due to the effect of social desirability. Further research using clinician- or observer-rated instruments on defenses will be needed to test the generalizability of our results. Moreover, the Italian version of the SCL-90 (the measure we adopted) has no gold-standard cut-offs to identify clinically significant depressive and anxiety symptoms. Given this limitation, we adopted the well-established thresholds of the updated version of this measure, the SCL-90-R (showing crucial similarities with the previous version; Derogatis and Cleary, 1977; Prunas et al., 2012), to identify the study participants. Finally, this study was conducted in the general population, warranting a replication study in clinical samples with both depressive and anxiety mental health conditions.
Conclusion
This is the first study conceptualizing defensive functioning as a complex system. Results of this study might inform future research questions aimed at detecting transdiagnostic intervention targets in individuals with symptoms of depression and anxiety.
Data availability statement
The datasets presented in this article are not readily available because the data that support the findings of this study are available upon reasonable request. Requests to access the datasets should be directed to Z2FicmllbGUubG9idWdsaW9AdW5pcm9tYTEuaXQ=.
Ethics statement
All procedures followed the ethical standards and were approved by the Ethics Committee of the University of Pisa (n. 0036344/2020). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MDG: Conceptualization, Writing – review & editing, Data curation, Formal analysis. GLB: Conceptualization, Writing – review & editing, Methodology, Writing – original draft. EC: Formal analysis, Methodology, Writing – review & editing. TB: Writing – review & editing. CC: Data curation, Writing – review & editing. VL: Supervision, Writing – review & editing. AT: Conceptualization, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2024.1465164/full#supplementary-material
References
Altuncu, K. A., Lomoriello, A. S., Lo Buglio, G., Martino, L., Yenihayat, A., Belfiore, M. T., et al. (2023). Mental health literacy about personality disorders: a multicultural study. Behav. Sci. 13:605. doi: 10.3390/bs13070605
American Psychiatric Association (1994). Diagnostic and Statistical Manual of Mental Disorders (4th ed.). New York: American Psychiatric Publishing, Inc.
Beck, A. T., Rush, A. J., Shaw, B. F., and Emery, G. (1979). Cognitive Therapy of Depression. London: Guilford Press.
Békés, V., Perry, J. C., Starrs, C. J., Prout, T. A., Conversano, C., and Di Giuseppe, M. (2023). Defense mechanisms are associated with mental health symptoms across six countries. Res. Psychother. 26:729. doi: 10.4081/ripppo.2023.729
Boldrini, T., Lo Buglio, G., Cerasti, E., Pontillo, M., Muzi, L., Salcuni, S., et al. (2024). Clinical utility of the at-risk for psychosis state beyond transition: A multidimensional network analysis. Eur. Child. Adolesc. Psychiat. 2024, 1–10. doi: 10.1007/s00787-024-02491-x
Boldrini, T., Tanzilli, A., Di Cicilia, G., Gualco, I., Lingiardi, V., Salcuni, S., et al. (2020). Personality traits and disorders in adolescents at clinical high risk for psychosis: toward a clinically meaningful diagnosis. Front. Psychiatry 11:562835. doi: 10.3389/fpsyt.2020.562835
Borsboom, D. (2017). A network theory of mental disorders. World Psychiat. 16, 5–13. doi: 10.1002/wps.20375
Borsboom, D., and Cramer, A. O. (2013). Network analysis: an integrative approach to the structure of psychopathology. Annu. Rev. Clin. Psychol. 9, 91–121. doi: 10.1146/annurev-clinpsy-050212-185608
Borsboom, D., Cramer, A. O. J., Fried, E. I., Isvoranu, A. M., Robinaugh, D. J., and Dalege, J. (2022). “Chapter 1. Network perspectives,” in Network psychometrics with R: guide for behavioral and social scientists, eds. A. M. Isvoranu, S. Epskamp, L. J. Waldorp, and D. Borsboom (London: Routledge, Taylor and Francis Group). doi: 10.4324/9781003111238-2
Borsboom, D., Deserno, M. K., Rhemtulla, M., Epskamp, S., Fried, E. I., McNally, R. J., et al. (2021). Network analysis of multivariate data in psychological science. Nat. Rev. Methods Primers 1:58. doi: 10.1038/s43586-021-00055-w
Carone, N., Benzi, I. M. A., Muzi, L., Parolin, L. A. L., and Fontana, A. (2023). Problematic internet use in emerging adulthood to escape from maternal helicopter parenting: defensive functioning as a mediating mechanism. Res. Psychother. 26:693. doi: 10.4081/ripppo.2023.693
Cassano, G., Conti, L. J, and Levine, J. (1999). “SCL-90,” in Repertorio delle scale di valutazione in psichiatria, ed. L. Conti (Firenze: SEE), 325–332.
Casula, A., Milazzo, B. M., Martino, G., Sergi, A., Lucifora, C., Tomaiuolo, F., et al. (2023). Non-invasive brain stimulation for the modulation of aggressive behavior: A systematic review of randomized sham-controlled studies. Life 13:1220. doi: 10.3390/life13051220
Conversano, C., Di Giuseppe, M., and Lingiardi, V. (2023). Case report: Changes in defense mechanisms, personality functioning, and body mass index during psychotherapy with patients with anorexia nervosa. Front. Psychol. 14:1081467. doi: 10.3389/fpsyg.2023.1081467
Costantini, G., Epskamp, S., Borsboom, D., Perugini, M., Mõttus, R., Waldorp, L. J., et al. (2015). State of the aRt personality research: a tutorial on network analysis of personality data in R. J. Res. Pers. 54, 13–29. doi: 10.1016/j.jrp.2014.07.003
Cramer, P. (2000). Defense mechanisms in psychology today: Further processes for adaptation. Am. Psychol. 55, 637–646. doi: 10.1037/0003-066X.55.6.637
Cramer, P. (2015). Understanding defense mechanisms. Psychodyn. Psychiatry 43, 523–552. doi: 10.1521/pdps.2015.43.4.523
de Roten, Y., Djillali, S., Crettaz von Roten, F., Despland, J. N., and Ambresin, G. (2021). Defense mechanisms and treatment response in depressed inpatients. Front. Psychol. 12:633939. doi: 10.3389/fpsyg.2021.633939
DeFife, J. A., and Hilsenroth, M. J. (2005). Clinical utility of the Defensive Functioning Scale in the assessment of depression. J. Nerv. Ment. Dis. 193, 176–182. doi: 10.1097/01.nmd.0000154839.43440.35
Derogatis, L. R., and Cleary, P. A. (1977). Confirmation of the dimensional structure of the SCL-90: a study in construct validation. J. Clin. Psychol. 33, 981–989. doi: 10.1002/1097-4679(197710)33:4<981::AID-JCLP2270330412>3.0.CO;2-0
Di Giuseppe, M. (2024). Transtheoretical, transdiagnostic, and empirical-based understanding of defense mechanisms. Mediter. J. Clin. Psychol. 12:4036. doi: 10.13129/2282-1619/mjcp-4036
Di Giuseppe, M., and Lingiardi, V. (2023). From theory to practice: The need of restyling definitions and assessment methodologies of coping and defense mechanisms. Clin. Psychol.: Sci. Pract. 30, 393–395. doi: 10.1037/cps0000145
Di Giuseppe, M., Orr,ù, G., Gemignani, A., Ciacchini, R., Miniati, M., and Conversano, C. (2022). Mindfulness and Defense mechanisms as explicit and implicit emotion regulation strategies against psychological distress during massive catastrophic events. Int. J. Environ. Res. Public Health 19:12690. doi: 10.3390/ijerph191912690
Di Giuseppe, M., and Perry, J. C. (2021). The hierarchy of defense mechanisms: assessing defensive functioning with the defense mechanisms rating scales Q-sort. Front. Psychol. 12:718440. doi: 10.3389/fpsyg.2021.718440
Di Giuseppe, M., Perry, J. C., Lucchesi, M., Michelini, M., Vitiello, S., Piantanida, A., et al. (2020). Preliminary reliability and validity of the DMRS-SR-30, a novel self-report based on the defense mechanisms rating scales. Front. Psychiatry 11:870. doi: 10.3389/fpsyt.2020.00870
Di Giuseppe, M., Perry, J. C., Prout, T. A., and Conversano, C. (2021). Editorial: Recent empirical research and methodologies in defense mechanisms: Defenses as fundamental contributors to adaptation. Front. Psychol. 12:802602. doi: 10.3389/fpsyg.2021.802602
Epskamp, S., and Fried, E. I. (2018). A tutorial on regularized partial correlation networks. Psychol. Methods 23, 617–634. doi: 10.1037/met0000167
Fiorentino, F., Lo Buglio, G., Morelli, M., Chirumbolo, A., Di Giuseppe, M., Lingiardi, V., et al. (2024). Defensive functioning in individuals with depressive disorders: A systematic review and meta-analysis. J. Affect. Disord. 357, 42–50. doi: 10.1016/j.jad.2024.04.091
Freud, S. (1894). “The neuro-psychoses of defence,” in The Standard Edition of the Complete Psychological Works of Sigmund Freud (1893–1899), ed. J. Strachey (London: The Hogarth Press).
Galli, F., Tanzilli, A., Simonelli, A., Tassorelli, C., Sances, G., Parolin, M., et al. (2019). Personality and personality disorders in medication-overuse headache: a controlled study by SWAP-200. Pain Res. Manag. 2019:1874078. doi: 10.1155/2019/1874078
Gelo, O. C. G., and Manzo, S. (2015). “Quantitative approaches to treatment process, change process, and process-outcome research,” in Psychotherapy research: Foundations, process, and outcome, eds. O. C. G. Gelo, A. Pritz, and B. Rieken (Cham: Springer), 247–277. doi: 10.1007/978-3-7091-1382-0_13
Gelo, O. C. G., Pritz, A., and Rieken, B. (2015b). “Preface,” in Psychotherapy research: Foundations, process, and outcome, eds. O. C. G. Gelo, A. Pritz, and B. Rieken (Cham: Springer), 5–6. doi: 10.1007/978-3-7091-1382-0
Gelo, O. C. G., Salcuni, S., and Colli, A. (2012). Text analysis within quantitative and qualitative psychotherapy process research: Introduction to special issue. Res. Psychother. 15, 45–53. doi: 10.4081/ripppo.2012.144
Gelo, O. C. G., Vilei, A., Maddux, J. E., and Gennaro, A. (2015a). Psychopathology as social construction: the case of anorexia nervosa. J. Constr. Psychol. 28, 105–125. doi: 10.1080/10720537.2013.858087
Gomez, R., Stavropoulos, V., Zarate, D., and Palikara, O. (2021). Symptom Checklist-90-Revised: a structural examination in relation to family functioning. PLoS ONE 16:e0247902. doi: 10.1371/journal.pone.0247902
Høglend, P., and Perry, J. C. (1998). Defensive functioning predicts improvement in major depressive episodes. J. Nerv. Ment. Dis. 186, 238–243. doi: 10.1097/00005053-199804000-00006
Ierardi, E., Bottini, M., Preti, E., Di Pierro, R., Madeddu, F., and Riva Crugnola, C. (2023). Attachment styles, mental health, and trauma during the first wave of COVID-19 pandemic in an Italian adult population. Res. Psychother. 26:689. doi: 10.4081/ripppo.2023.689
Klocek, A., and Riháček, T. (2023). The associations between interoceptive awareness, emotion regulation, acceptance, and well-being in patients receiving multicomponent treatment: a dynamic panel network model. Res. Psychother. 26:659. doi: 10.4081/ripppo.2023.659
König, V. L., Fontao, M. I., Casari, L. M., and Taborda, A. R. (2023). Psychotherapists' experiences of telepsychotherapy during the COVID-19 pandemic in Argentina: impact on therapy setting, therapeutic relationship and burden. Res. Psychother. 26:632. doi: 10.4081/ripppo.2023.632
Lenzo, V., Barberis, N., Cannavò, M., Filastro, A., Verrastro, V., and Quattropani, M. C. (2020). The relationship between alexithymia, defense mechanisms, eating disorders, anxiety and depression. Riv. Psichiatr. 55, 24–30. doi: 10.1708/3301.32715
Lingiardi, V., and McWilliams, N. (2017). Psychodynamic diagnostic manual: PDM-2 (2nd ed.). New York: The Guilford Press.
Lo Buglio, G., Boldrini, T., Polari, A., Fiorentino, F., Nelson, B., Solmi, M., et al. (2024). Harmonizing early intervention strategies: scoping review of clinical high risk for psychosis and borderline personality disorder. Front. Psychol. 15:1381864. doi: 10.3389/fpsyg.2024.1381864
Martino, G., Caputo, A., Bellone, F., Quattropani, M. C., and Vicario, C. (2020). Going beyond the visible in type 2 diabetes mellitus: defense mechanisms and their associations with depression and health-related quality of life. Front. Psychol. 11:267. doi: 10.3389/fpsyg.2020.00267
Martino, G., Caputo, A., Vicario, C. M., Feldt-Rasmussen, U., Watt, T., Quattropani, M. C., et al. (2021). Alexithymia, emotional distress and perceived quality of life in patients with hashimoto's thyroiditis. Front. Psychol. 12:667237. doi: 10.3389/fpsyg.2021.667237
Martino, G., Catalano, A., Bellone, F., Russo, G. T., Vicario, C. M., Lasco, A., et al. (2019). As time goes by: anxiety negatively affects the perceived quality of life in patients with type 2 diabetes of long duration. Front. Psychol. 10:1779. doi: 10.3389/fpsyg.2019.01779
Martino, G., Viola, A., Vicario, C. M., Bellone, F., Silvestro, O., Squadrito, G., et al. (2023). Psychological impairment in inflammatory bowel diseases: the key role of coping and defense mechanisms. Res. Psychother. 26:731. doi: 10.4081/ripppo.2023.731
McWilliams, N., and Weinberger, J. (2003). “Psychodynamic psychotherapy,” in Handbook of psychology: Clinical psychology, eds. G. Stricker, T. A. Widiger, and I. B. Weiner (London: John Wiley and Sons, Inc.), 253–277. doi: 10.1002/0471264385.wei0810
Messina, I., Calvo, V., and Grecucci, A. (2023). Attachment orientations and emotion regulation: new insights from the study of interpersonal emotion regulation strategies. Res. Psychother. 26:703. doi: 10.4081/ripppo.2023.703
Nordgaard, J., Nielsen, K. M., Rasmussen, A. R., and Henriksen, M. G. (2023). Psychiatric comorbidity: a concept in need of a theory. Psychol. Med. 2023, 1–7. doi: 10.1017/S0033291723001605
Olson, T. R., Presniak, M. D., and MacGregor, M. W. (2009). Differentiation of depression and anxiety groups using defense mechanisms. J. Nerv. Ment. Dis. 197, 834–840. doi: 10.1097/NMD.0b013e3181beab34
Opsahl, T., Agneessens, F., and Skvoretz, J. (2010). Node centrality in weighted networks: generalizing degree and shortest paths. Soc. Netw. 32, 245–251. doi: 10.1016/j.socnet.2010.03.006
Parolin, L., Milesi, A., Comelli, G., and Locati, F. (2023). The interplay of mentalization and epistemic trust: a protective mechanism against emotional dysregulation in adolescent internalizing symptoms. Res. Psychother. 26:707. doi: 10.4081/ripppo.2023.707
Perry, J. C. (2014). Anomalies and specific functions in the clinical identification of defense mechanisms. J. Clin. Psychol. 70, 406–418. doi: 10.1002/jclp.22085
Perry, J. C., Bekes, V., and Starrs, C. J. (2022). A systematic survey of adults' health-protective behavior use during early COVID-19 pandemic in Canada, Germany, United Kingdom, and the United States, and vaccination hesitancy and status eight months later. Prev Med. Rep. 30:102013. doi: 10.1016/j.pmedr.2022.102013
Perry, J. C., and Bond, M. (2017). Addressing defenses in psychotherapy to improve adaptation. Psychoan. Inquiry 37, 153–166. doi: 10.1080/07351690.2017.1285185
Powers, M. B., de Kleine, R. A., and Smits, J. A. J. (2017). Core mechanisms of cognitive behavioral therapy for anxiety and depression: a review. Psychiatr. Clin. North Am. 40, 611–623. doi: 10.1016/j.psc.2017.08.010
Prout, T. A., Di Giuseppe, M., Zilcha-Mano, S., Perry, J. C., and Conversano, C. (2022). Psychometric properties of the Defense Mechanisms Rating Scales-Self-Report-30 (DMRS-SR-30): internal consistency, validity and factor structure. J. Pers. Assess. 104, 833–843. doi: 10.1080/00223891.2021.2019053
Prout, T. A., Malone, A., Rice, T., and Hoffman, L. (2019). Resilience, defense mechanisms, and implicit emotion regulation in psychodynamic child psychotherapy. J. Contemp. Psychother. 49, 235–244. doi: 10.1007/s10879-019-09423-w
Prunas, A., Sarno, I., Preti, E., Madeddu, F., and Perugini, M. (2012). Psychometric properties of the Italian version of the SCL-90-R: a study on a large community sample. Eur. Psychiat. 27, 591–597. doi: 10.1016/j.eurpsy.2010.12.006
Rice, T. R., and Hoffman, L. (2014). Defense mechanisms and implicit emotion regulation: a comparison of a psychodynamic construct with one from contemporary neuroscience. J. Am. Psychoanal. Assoc. 62, 693–708. doi: 10.1177/0003065114546746
Roefs, A., Fried, E. I., Kindt, M., Martijn, C., Elzinga, B., Evers, A. W. M., et al. (2022). A new science of mental disorders: Using personalised, transdiagnostic, dynamical systems to understand, model, diagnose and treat psychopathology. Behav. Res. Ther. 153:104096. doi: 10.1016/j.brat.2022.104096
Sarno, I., Preti, E., Prunas, A., and Madeddu, F. (2011). SCL-90-R Symptom Checklist-90-R Adattamento italiano. Firenze: Giunti. Organizzazioni Speciali.
Sergi, A., Messina, A., Vicario, C. M., and Martino, G. (2023). A quantum-classical model of brain dynamics. Entropy 25:592. doi: 10.3390/e25040592
Silverman, J., and Aafjes-van Doorn, K. (2023). Coping and defense mechanisms: A scoping review. Clin. Psychol. 30, 381–392. doi: 10.1037/cps0000139
Tanzilli, A., Cibelli, A., Liotti, M., Fiorentino, F., Williams, R., and Lingiardi, V. (2022). Personality, defenses, mentalization, and epistemic trust related to pandemic containment strategies and the COVID-19 vaccine: a sequential mediation model. Int. J. Environ. Res. Public Health 19:14290. doi: 10.3390/ijerph192114290
Tanzilli, A., Di Giuseppe, M., Giovanardi, G., Boldrini, T., Caviglia, G., Conversano, C., et al. (2021). Mentalization, attachment, and defense mechanisms: a Psychodynamic Diagnostic Manual-2-oriented empirical investigation. Res. Psychother. 24:531. doi: 10.4081/ripppo.2021.531
Taubner, S., Ioannou, Y., Saliba, A., Sales, C. M. D., Volkert, J., Protić, S., et al. (2023). Mediators of outcome in adolescent psychotherapy and their implications for theories and mechanisms of change: a systematic review. Eur. Child. Adolesc. Psychiat. doi: 10.1007/s00787-023-02186-9
Vaillant, G. E. (1971). Theoretical hierarchy of adaptive ego mechanisms: a 30-year follow-up of 30 men selected for psychological health. Arch. Gen. Psychiatry 24, 107–118. doi: 10.1001/archpsyc.1971.01750080011003
Vaillant, G. E. (2000). Adaptive mental mechanisms: their role in a positive psychology. Am. Psychol. 55, 89–98. doi: 10.1037/0003-066X.55.1.89
Vita, R., Caputo, A., Quattropani, M. C., Watt, T., Feldt-Rasmussen, U., Puleio, P., et al. (2020). Quality of life in patients with hyperthyroidism: where do we stand? Mediterr. J. Clin. Psychol. 8, 1–28. doi: 10.6092/2282-1619/mjcp-2521
Volkert, J., Zettl, M., and Taubner, S. (2022). Transdiagnostic Assessment of Psychopathology and Resilience: Psychometric Evaluation of the German Version of the Defence Mechanism Rating Scale (DMRS-SR-30) and Relationship with Personality Functioning and Associated Constructs. London: PsychArchives.
World Health Organization (2022). World Mental Health Report: Transforming Mental Health for All. Geneva: WHO.
Keywords: defense mechanisms, DMRS-SR-30, depression, anxiety, network analysis, COVID-19
Citation: Di Giuseppe M, Lo Buglio G, Cerasti E, Boldrini T, Conversano C, Lingiardi V and Tanzilli A (2024) Defense mechanisms in individuals with depressive and anxiety symptoms: a network analysis. Front. Psychol. 15:1465164. doi: 10.3389/fpsyg.2024.1465164
Received: 15 July 2024; Accepted: 25 October 2024;
Published: 08 November 2024.
Edited by:
Gabriella Martino, University of Messina, ItalyReviewed by:
Omar Carlo Gioacchino Gelo, University of Salento, ItalyMaria Rosaria Juli, Magna Græcia University, Italy
Edward Callus, University of Milan, Italy
Copyright © 2024 Di Giuseppe, Lo Buglio, Cerasti, Boldrini, Conversano, Lingiardi and Tanzilli. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gabriele Lo Buglio, Z2FicmllbGUubG9idWdsaW9AdW5pcm9tYTEuaXQ=; Annalisa Tanzilli, YW5uYWxpc2EudGFuemlsbGlAdW5pcm9tYTEuaXQ=
†These authors have contributed equally to this work and share last authorship