 Diego Arenas1,2
Diego Arenas1,2 Miranda Bodi-Torralba1,2
Miranda Bodi-Torralba1,2 Andrea Oliver1,2
Andrea Oliver1,2 Jaume Cantallops1,2Francisco J. Ponseti1,2
Jaume Cantallops1,2Francisco J. Ponseti1,2 Pere Palou-Sampol1,2Juan A. Collado3
Pere Palou-Sampol1,2Juan A. Collado3 Isabel Flórez4Alejandro Galvez-Pol5,6
Isabel Flórez4Alejandro Galvez-Pol5,6 Juan L. Terrasa7,8
Juan L. Terrasa7,8 Carolina Sitges7,8
Carolina Sitges7,8 Víctor Sánchez-Azanza9
Víctor Sánchez-Azanza9 Raúl López-Penadés9
Raúl López-Penadés9 Daniel Adrover-Roig9
Daniel Adrover-Roig9 Adrià Muntaner-Mas1,2,10*
Adrià Muntaner-Mas1,2,10*- 1GICAFE “Physical Activity and Exercise Sciences Research Group”, Faculty of Education, University of the Balearic Islands, Palma, Spain
- 2Department of Pedagogy and Specific Didactics, Institute of Research and Innovation in Education, University of the Balearic Islands, Palma, Spain
- 3Department of Education, Valencian International University, Valencia, Spain
- 4Balearic Institute of Mental Health of Children and Adolescents (IBSMIA), Son Espases University Hospital, Health Research Institute of the Balearic Islands (IdISBa), Palma, Spain
- 5Psychology Department, University of the Balearic Islands, Palma de Mallorca, Palma, Spain
- 6Active Cognition, Embodiment, and Environment Lab, University of the Balearic Islands, Palma de Mallorca, Palma, Spain
- 7Research Institute of Health Sciences (IUNICS), Health Research Institute of the Balearic Islands (IdISBa), Palma, Spain
- 8Department of Psychology, University of the Balearic Islands (UIB), Palma, Spain
- 9Department of Applied Pedagogy and Educational Psychology, Institute of Research and Innovation in Education (IRIE), University of the Balearic Islands, Palma, Spain
- 10PROFITH “PROmoting FITness and Health Through Physical Activity” Research Group, Sport and Health University Research Institute (iMUDS), Faculty of Sport Sciences, University of Granada, Granada, Spain
The Break4Brain project aims to elucidate the effects of both acute and chronic physical activity (PA) on educational achievement in children with and without Attention Deficit Hyperactivity Disorder (ADHD). This study will be conducted in two phases: a cross-over design followed by a hybrid type 1 implementation-effectiveness trial, which includes both a cluster randomized controlled trial (RCT) and a qualitative study. In phase I, 60 children aged 10–12, with 30 each from ADHD and non-ADHD groups, will participate in a laboratory-based study over 4 days within 1 month. They will participate in three counterbalanced experimental conditions: (i) PA with cognitive engagement, (ii) PA without cognitive engagement, and (iii) a cognitively engaging control. This phase will assess acute changes in brain function, academic performance, working memory, inhibitory control, and sustained attention. Phase II will involve 600 children aged 10–12, randomly assigned to either a video-based PA program or a control group (300 children per group) in an 8-week cluster RCT. This phase will also incorporate a qualitative approach to explore the implementation context through pre- and post-intervention semi-structured interviews with teachers and school staff, and questionnaires for students. The outcomes of interest in this phase will include working memory, cognitive flexibility, selective attention, and academic performance. For the cross-over study, we hypothesize that PA conditions will enhance the studied outcomes compared to the control condition. In the RCT, we anticipate that the 8-week active breaks program will result in significant improvements in the selected outcomes compared to the control group. This study is expected to make pioneering contributions by including novel variables and focusing on the ADHD population. Furthermore, if the cluster RCT proves effective, it could offer a practical and cost-effective resource for integrating active breaks into daily school routines.
1 Background
Physical inactivity and sedentary behavior pose a global challenge, impacting not only the physical health of youth but also exerting substantial implications on their brain health (Bull et al., 2020; Guthold et al., 2020). Over the past two decades, a wealth of evidence has accumulated, indicating that physical activity (PA) is among the most promising and cost-effective strategies for improving neurocognitive function (Morales et al., 2024). Thus, promoting PA during youth development can help to enhance the likelihood of academic performance, with childhood representing a particularly crucial stage (Álvarez-Bueno et al., 2017; Lubans et al., 2016; Singh et al., 2019; de Greeff et al., 2018; Muntaner-Mas et al., 2024). Altogether, the available evidence suggests a favorable effect size (small to moderate) of both chronic and acute PA on improving various domains of educational achievement, including brain function, cognition, and academic performance (Li et al., 2017; Sibbick et al., 2022).
Researchers have examined a wide variety of educational outcomes following acute PA in children without a neurodevelopmental disorder. Specifically, some systematic reviews and metanalytic studies shed light on the field and quantified the effect sizes of acute PA. In short, results of the Watson et al. (2017) meta-analyses showed that acute PA had a positive effect on improving on-task and reducing off-task classroom behavior [standardized mean difference = 0.60 (95% CI: 0.20, 1.00)], and this fact led to improvements in academic achievement [standardized mean difference = 1.03 (95% CI: 0.22, 1.84)]. Other reviews conclude that the effects of acute PA on the working memory and cognitive flexibility domains in children are inconclusive and scarce (Pontifex et al., 2019; Paschen et al., 2019). A recent meta-analysis by de Greeff et al. (2018) reviewed studies of children, 6–12 years old, that assessed the effect of single bouts of PA on inhibition. A small to moderate positive effect of acute PA was observed (Hedges’ g = 0.28, 95% CI = 0.01–0.56, p = 0.042). Similarly, investigations of selective and sustained attention have generally observed facilitations in the ability to focus and maintain attention following acute bouts of PA in children (effect sizes ranging from 0.1 to 0.69; Pontifex et al., 2019). In conclusion, the acute effect of PA in children without a neurodevelopmental disorder seems to exert a small but positive effect on educational outcomes.
Acute PA holds also notable benefits for children with cognitive impairments like Attention Deficit Hyperactivity Disorder (ADHD), a prevalent developmental disorder affecting 5.9% of youth globally (Faraone et al., 2021). ADHD symptoms include inattention, impulsivity, and hyperactivity, leading to academic struggles and deficits in multiple cognitive domains such as working memory and inhibitory control (Harrison et al., 2019). While ADHD medication helps manage some symptoms, it does not address learning disorders and executive function deficits effectively (Faraone et al., 2015). Despite several investigations that have examined the effects of acute PA in children with ADHD the exact nature of the response on brain function, cognition, and academic performance is still uncertain. To the best of our knowledge, there is no research examining the effects of acute PA on academic performance in children with ADHD. However, acute PA have been found to elicit transient benefits for overall cognitive performance in children with ADHD (Grassmann et al., 2017; Halperin et al., 2014; Li et al., 2023; Suarez-Manzano et al., 2018; Zhu et al., 2023). Specifically, a meta-analysis suggested that acute PA significantly benefit performance on inhibition, working memory, cognitive flexibility, and attention (Pontifex et al., 2019). This primer review on the topic also concludes that exist potential moderators of effects on cognitive functions related to the specified PA parameters intensity, duration, and volume in children with ADHD. While moderate-intensity aerobic exercise has shown promising results in improving ADHD symptoms and executive functions, research on the potential effects of other PA types, durations, and intensities remains largely unknown (Chan et al., 2022; Yu et al., 2020).
Additionally, recent systematic reviews have underlined the importance of evaluating the impacts of acute PA with low and high cognitive demands on cognitive performance (Paschen et al., 2019; Skulmowski, 2024). Some authors suggest that PA with cognitive engagement incorporates added stimuli, leading to heightened physiological arousal, thereby enhancing executive functions (Tomporowski et al., 2015; Best, 2010). In this regard, PA with cognitive engagement has demonstrated superior and longer-lasting effects on executive functions and ADHD symptoms in children with ADHD (Nejati and Derakhshan, 2021). Nonetheless, findings from other studies contradict this hypothesis, suggesting that PA with cognitive engagement do not necessarily enhance cognitive performance compared to bouts of PA without cognitive engagement or sedentary activities (Bedard et al., 2021). Thus, the current evidence on the effects of PA, as short bursts, and the cognitive demands of such activity in subsequent cognitive function remains elusive.
School environments offer an ideal setting to enhance children’s educational achievement through PA, benefiting both those with and without neurodevelopmental disorders (Howie and Pate, 2012). Specifically, integrating short bursts of PA, known as active breaks, during school time has been suggested as a valuable and feasible strategy in schools settings (World Health Organization, 2024). Active breaks typically last 3–15 min and are led by teachers to enhance learning outcomes, increase daily PA and reduce sedentary time. Examples of programs are TAKE 10! (Stewart et al., 2004), Energizers (Mahar et al., 2006), Transform-US Active Break (TAB) (Lander et al., 2024), and Burn2Learn (Mavillidi et al., 2021). On the one hand, the overall results of these programs have shown promising results of active breaks on brain function, cognition, and academic performance. However, scientific reviews have yielded mixed results, attributing certain differences to the quality and design characteristics of each program (Watson et al., 2017; Daly-Smith et al., 2018; Peiris et al., 2022). Overall, while scientific progress has been made in the field, the ideal dosage of active breaks for improving educational outcomes remains uncertain.
In this context, there is limited research substantiating the adoption, implementation, and sustainability of interventions under real-world conditions (Reis et al., 2016; Wiltsey Stirman et al., 2012), such as school settings. In this scenario, implementation models, such as the Reach, Effectiveness, Adoption, Implementation, and Maintenance (RE-AIM) framework, have been devised to evaluate the public health impact of interventions (Glasgow et al., 1999). School-based PA interventions demand a comprehensive grasp of the educational system, where contextual elements—such as organizational dynamics, intervention stakeholders, and the target population—operate with greater variability compared to the controlled settings typically found in research designs (Wolfenden et al., 2022). Qualitative approaches have been justified as a valid method to develop effective interventions through the examination of facilitators and barriers by the educational agents involved (Chalkley et al., 2018; Lane et al., 2022). Nonetheless, the extant evidence indicates limited consideration of this methodology in school interventions (Gelman et al., 2023; Koorts et al., 2022).
Therefore, exploring the optimal dose of PA, particularly through classroom-based active breaks, is vital for understanding its effectiveness in children with and without ADHD. Identifying this optimal dose is crucial for maximizing the impact on academic performance, cognition, and brain function across both populations. However, a significant gap persists in the literature, especially regarding the effects of large-scale active break programs in school settings. Moreover, implementing such interventions in school settings demands a multifaceted approach, involving collaboration among teachers, school staff, and students (Daly-Smith et al., 2021).
The primary aim of this study is to present the rationale, design, and methods of the Break4Brain Project. This project will investigate: (i) the acute effects of three experimental conditions— PA with cognitive engagement, PA without cognitive engagement, and a cognitively engaging control—on academic performance, cognitive function, and brain function in children aged 10–12, both with and without ADHD, using a cross-over design in a laboratory; and (ii) the chronic effects of two experimental conditions—a video-based PA program and a control condition—on academic performance and cognitive function in school-aged children (10–12 years old) within a school setting, utilizing a cluster RCT. Additionally, it will incorporate a qualitative approach to assess the feasibility of implementing PA initiatives in school settings and will include cost-effectiveness analyses.
2 Methods
2.1 Study design
The Break4Brain project will consist of two distinct phases: phase I will employ a cross-over design (ClinicalTrials.gov identifier: NCT06303674), while phase II will utilize a hybrid type 1 implementation-effectiveness trial (ClinicalTrials.gov identifier: NCT06319833). In phase II, we will implement a type 1 hybrid trial in primary schools across the Balearic Islands (Spain; Curran et al., 2012). The primary goal of this hybrid trial is to evaluate the effectiveness of the cluster RCT. Additionally, the secondary goal aims to better understand the implementation context through a qualitative approach. The qualitative component of phase II will be developed using the most comprehensive theoretical framework available in the literature (Yoshida et al., 2020). The project has been approved by the Ethics Committee of the University of the Balearic Islands (Ref No: 301CER22 for Phase I; and Ref No: 348CER23 for Phase II). Measurement protocols of each phase have been published in Zenodo.1 A SPIRIT schedule and overview of the study design can be found in Tables 1A, 1B. This protocol has been developed following the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) checklist (Supplementary File S1). This research adheres to the guidelines outlined in the Declaration of Helsinki across all its facets. Before participation, explicit written consent will be obtained from both the school staff (phase II) and parents (phase I and II), and the participants’ assent will be also sought. Any modifications to the research protocol will be transparently communicated and duly registered on ClinicalTrials.gov, ensuring accountability and compliance with ethical standards.
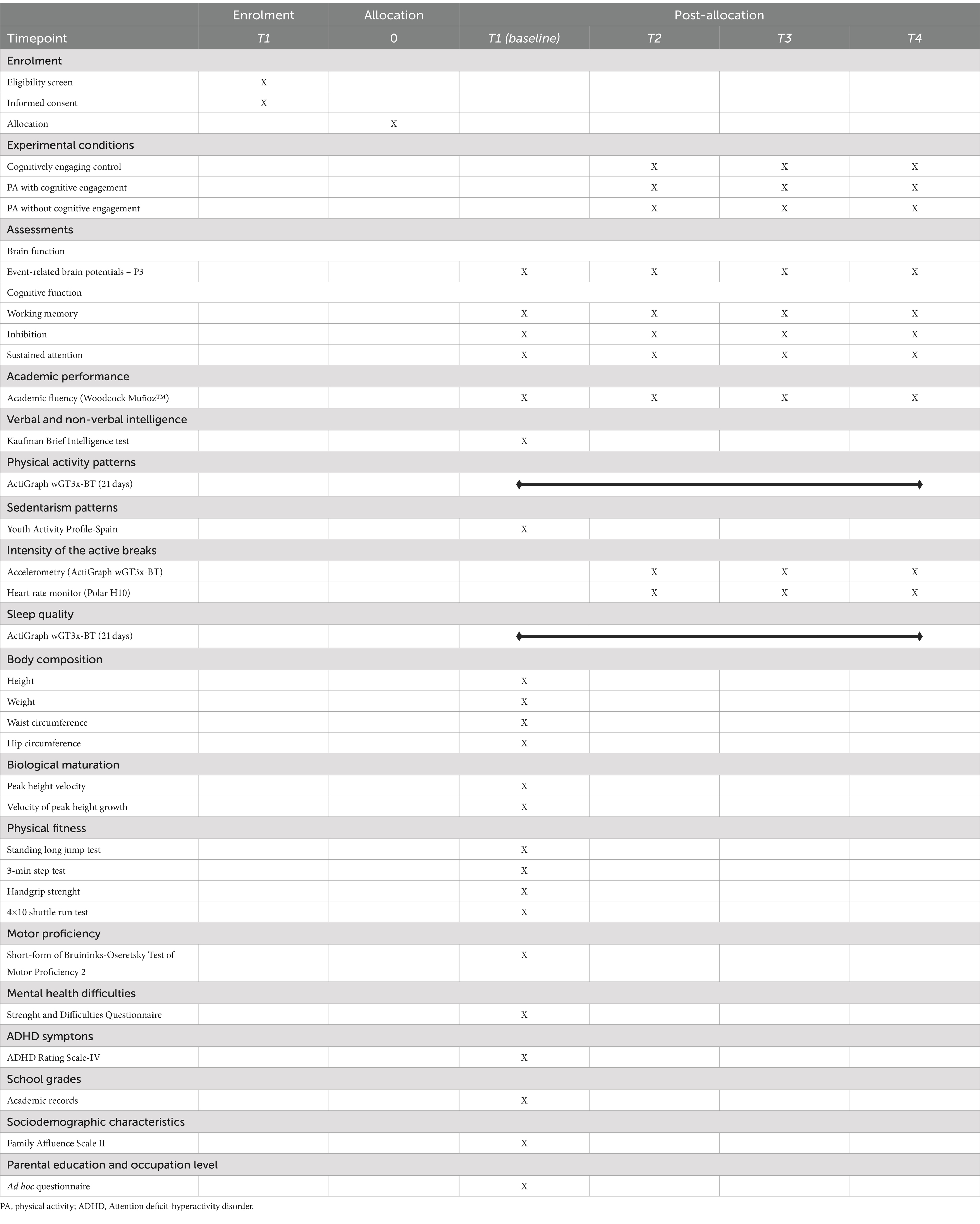
Table 1A. SPIRIT schedule of enrolment, interventions, and assessments of phase I.
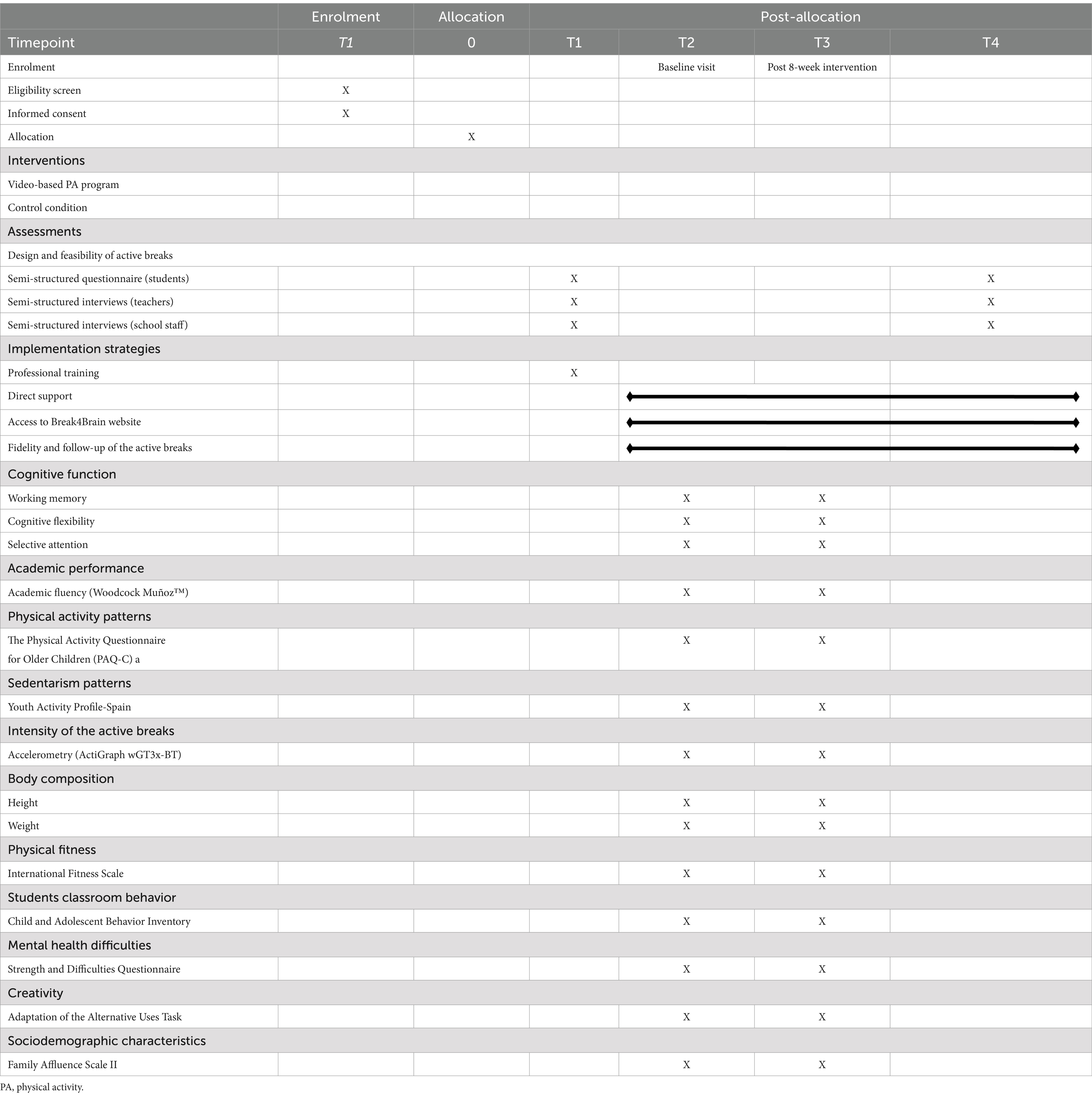
Table 1B. SPIRIT schedule of enrollment, interventions, and assessments of phase II.
In phase I (Figure 1), measurements will be conducted in laboratory settings. Each participant will undergo all experimental conditions, with the order of conditions balanced and outcomes assessed after each. Overall, participants will participate in three experimental conditions (cognitively engaging control, PA with cognitive engagement, and PA without cognitive engagement). Each participant will undergo outcome assessments four times (once at baseline, and three times post each experimental condition), with a seven-day gap between each measurement day (as well-known as washout period, enough to avoid carryover effects; Li et al., 2015). Baseline assessment will take place on the first day without engaging in any experimental conditions.
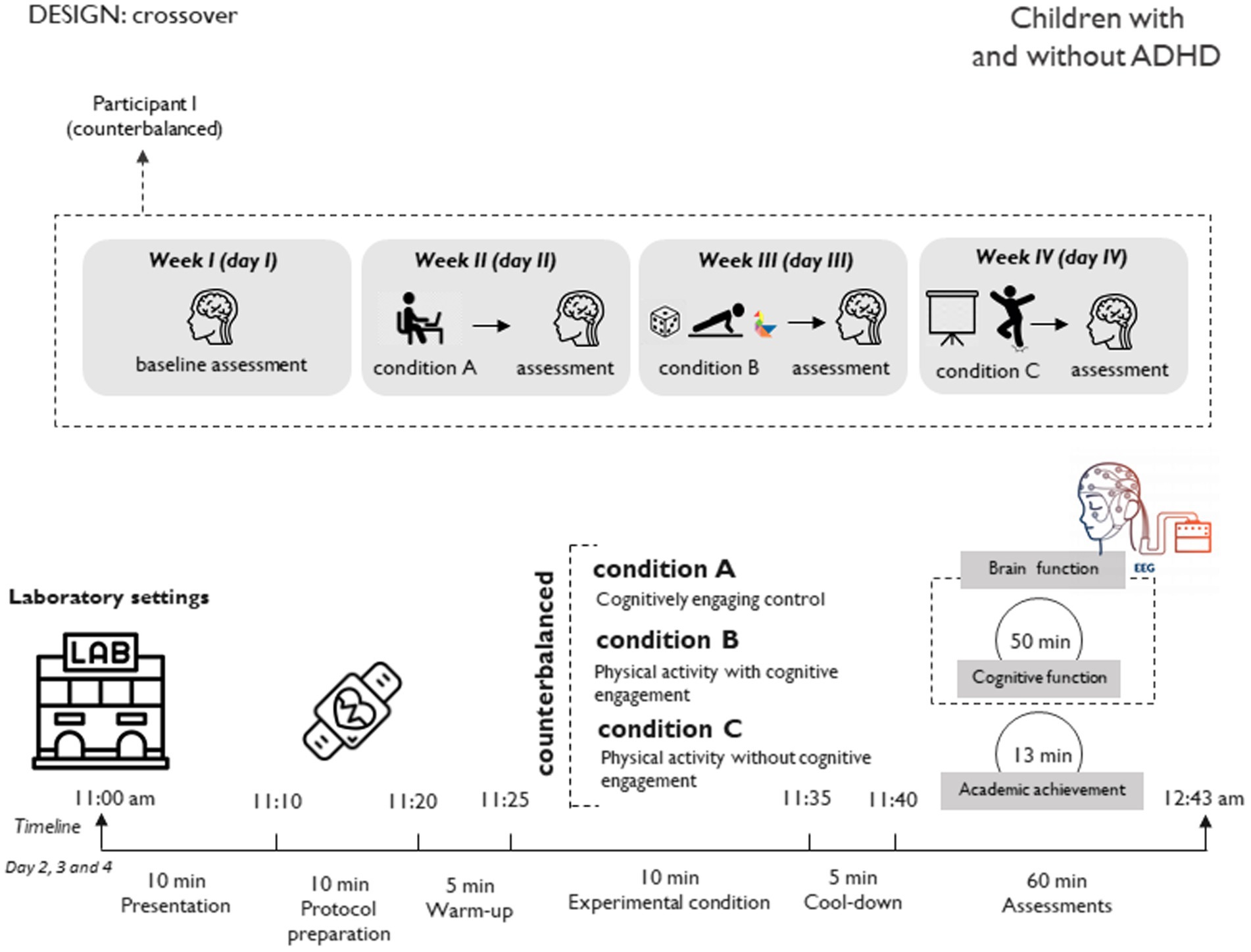
Figure 1. Study design and sample size for phase I (cross-over study).
Concerning phase II (Figure 2A), measurements will be carried out in school settings. Participating schools will be randomly assigned to one of two experimental conditions (control: usual academic lessons; intervention: video-based PA program [physically active without cognitive engagement]). The intervention will take 8 weeks, with the intervention condition implemented daily during this period. To design the experimental condition, a qualitative design will be conducted (Figure 2B).
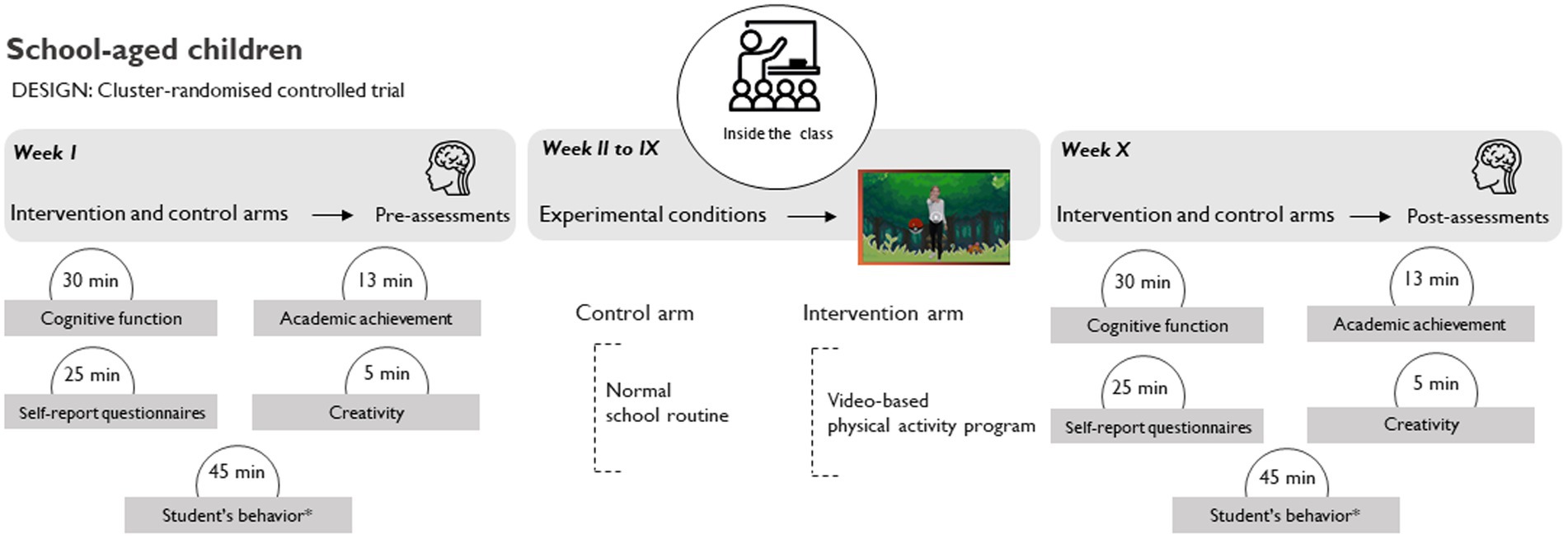
Figure 2. Study design for phase II (hybrid type 1 implementation-effectiveness trial: panel (A) - cluster randomized controlled trial; panel (B) - qualitative study).
2.2 Participants and eligibility criteria
Children aged 10–12 will be recruited for phase I through the dissemination conducted in schools, hospitals, media, and social networks across Majorca (Balearic Islands, Spain). For phase II, recruitment will be focused on children of the same age (10–12 years) from Majorca, Ibiza, and Menorca (Balearic Islands, Spain) using the same dissemination methods.
The age group selection (in both phases) will be based on late childhood’s critical brain development stage, sensitive to maturation (Giedd et al., 1999; Johnson et al., 2009). We will select preadolescents over pubertal participants to avoid the varied changes that occur during puberty, which can interefere the investigation. Our phase I focus on ADHD stems from its childhood onset and lifelong persistence, often accompanied by comorbidities (Sayal et al., 2018). Early ADHD symptom and comorbidity management is crucial, with PA suggested to alleviate adverse effects, including cognitive impairment (Halperin et al., 2014; Hoza et al., 2016). The qualitative section of phase II will involve the participation of students from the class group, teachers, and staff members of the schools. This approach will ensure feedback from the three key stakeholders essential for the successful implementation of a PA intervention in schools based on the RE-AIM framework (Yoshida et al., 2020; Kennedy et al., 2021), and complemented by Daly-Smith et al.’s guidelines (Daly-Smith et al., 2021).
The specific eligibility criteria for each phase are detailed below:
• Phase I
- (i) Children (10–12 years) diagnosed with ADHD by a psychiatrist, a psychologist or a pediatrician using the criteria of the Diagnostic and Statical Manual of Mental Disorders (DSM-5) without physical impairment; and (ii) Children (aged 10–12 years) without any neurodevelopmental or physical impairment.
• Phase II
- Quantitative section: (i) Children (10–12 years) without physical impairments.
- Qualitative section: (i) Children (10–12 years) participating in the study; (ii) Teachers of the class that will participate in the study; and (iii) School staff from a participating school.
2.3 Phase I: laboratory settings
2.3.1 Sample size and power
A within-subjects, 3 conditions (cognitively engaging control, PA with cognitive engagement, and PA without cognitive engagement) × 4 times (baseline, posttest 1, posttest 2, and posttest 3) repeated measures ANOVA design with 15 participants should be sufficiently powered to detect interactions at or above moderate effect sizes f = 0.25 which translates to an approximate Cohen’s d = 0.5 assuming alpha at 0.05, power at 80%, and a correlation among 4 repeated measures of 0.75. Considering the primer of Pontifex et al. (2019), the median sample size utilized within the literature investigating acute effects of acute bouts of PA on cognition has been below 15 participants. Considering this together, and a potential dropout rate of 10% observed in similar studies (Mora-Gonzalez et al., 2019), our investigation will recruit 30 participants with ADHD and 30 without ADHD.
2.3.2 Recruitment and randomization
Recruitment occurs out on a rolling basis, and screening procedures involve verbal screening of potential participants over the phone. Initially, the screener provides an overview of the Break4Brain Project and then obtains verbal consent. The telephone script includes questions regarding participants’ demographic information such as age, gender, and any history of ADHD, along with inquiries about inclusion and exclusion criteria. The total time administered in all screening questions is approximately 10 min. Recruitment began in January 2024 and is still ongoing. Once parents agree to participate via telephone, they sign a written informed consent before their children participate. In addition to obtaining informed consent from parents or legal guardians, this study will also seek verbal assent from the participating children. Prior to their involvement, children will be provided with age-appropriate explanations about the study’s purpose, procedures, and their role within it. They will be encouraged to ask questions and express any concerns they might have. Only those who verbally agree to participate, after understanding the study, will be included.
Randomization of participants into experimental conditions is conducted using R software by an external statistician. This randomization takes place after baseline assessments to minimize the risk of bias during measurements.
2.3.3 Experimental protocol and conditions
Each participant will visit the laboratory for 4 days over 3 weeks (Figure 1). This phase comprises three experimental conditions in a counterbalanced order (Supplementary Figure S1): (i) PA with cognitive engagement, (ii) PA without cognitive engagement, and (iii) cognitively engaging control. Participants will arrive at the laboratory unaware of the experimental condition they will be practicing each day. To minimize the impact of fatigue or excessive physical exertion on performance during the experimental conditions, participants will be advised to avoid intense PA on the day prior to each visit.
2.3.3.1 PA with cognitive engagement condition
This experimental condition will involve participants engaging in PA interspersed with rest periods doing cognitive tasks. Following a structured format, it consists of 10 consecutive 30-s blocks of PA alternated with cognitive tasks, totaling 10 min of PA time with a 1:1 work-to-rest ratio. Additionally, there will be 5 min allocated for warm-up and another 5 min for cool-down activities. The PA will target both aerobic and strength-based metabolism, based on the low integration-low relevance movement strategy (Mavilidi et al., 2022).
To determine the PA to be performed, participants will roll a die. Depending on the outcome, they will carry out the corresponding predetermined exercise, which was already introduced during the warm-up session. In the event of a repeat, the evaluator will replace the card for that specific exercise on the die. Conversely, during rest intervals involving cognitive tasks, participants will engage in solving various “tangram” puzzles. The researcher will manage the timing.
2.3.3.2 Physical activity without cognitive engagement condition
This experimental condition will involve PA interspersed with rest periods (without doing cognitive tasks). This experimental condition will replicate the dose of the preceding one (i.e., maintaining the same work ratio, and duration). Participants will practice PA guided by video observation and imitation,2 based on a protocol that will not require prior experience or knowledge from the participants (Moreau et al., 2017). This video was used by the research staff in a prior study (Gelabert et al., 2023). The PA will also focus on both aerobic and strength-based metabolism, following a strategy with low integration-low relevance movements (Mavilidi et al., 2022).
2.3.3.3 Cognitively engaging control condition
Participants will be instructed to watch a video concerning hygiene habits while remaining seated and at rest for 10 min.3 The researcher will not interact with the participants during this period. It is important to employ control conditions that closely resemble the intervention being studied. This approach helps isolate the hypothesized mechanism of interest (Simons et al., 2016). In our study, it is more clinically relevant to compare the intervention with behaviors commonly employed in classrooms, rather than solely comparing it against students sitting quietly (Pontifex et al., 2019).
2.3.4 Measures
Each participant will individually attend to our laboratory on 4 different days (Figure 1), with a seven-day gap between each measurement day (once at baseline, and three times immediately after each experimental condition). Primary outcomes will be evaluated each day, while the rest will be only assessed at baseline (Table 1A). To mitigate measurement bias, trained researchers will conduct these measurements consistently in the same laboratory setting.
2.3.4.1 Primary outcome measures
2.3.4.1.1 Brain function
Electroencephalogram (EEG) will be recorded during both the n-back and the flanker tasks. Then, EEG datasets will be processed in Brain Vision Analyzer (Version 2.0.4), as well as through custom code implemented in MATLAB using the EEGLAB toolbox (Delorme and Makeig, 2004). From the EEG, we will obtain Event-related brain potentials (ERPs). ERPs will serve as a measure of brain response to discrete events. Electrophysiological activity will be recorded using 32 active electrodes (i.e., BrainVision actiCAP system, Brain Products GmbH, Munich, Germany). The protocol to acquire ERPs is similar to other studies examining executive functions (Galvez-Pol et al., 2018; Galvez-Pol et al., 2018; Luck, 2014). Next, we will aim to epoch the continuous data to obtain an EEG component known as P3 or P300. This component is characterized by a positive deflection in voltage around 300 milliseconds post-stimulus. It is usually elicited in tasks requiring attention and decision-making, reflecting cognitive processes related to stimulus evaluation and categorization. The P300 amplitude varies with the relevance and probability of the stimulus, serving as a key indicator of attentional and working memory processes (Luck, 2014).
2.3.4.2 Secondary outcome measures
2.3.4.2.1 Academic performance
The academic fluency index will be calculated, consisting of the reading, mathematics, and writing fluency subtests of the Bateria III Woodcock Muñoz™ (Muñoz-Sandoval et al., 2005). Reading fluency will assess the participant’s capacity to read simple sentences rapidly, mathematical fluency will gauge the ability to quickly solve simple addition, subtraction, and multiplication problems, and writing fluency will measure the ability to formulate and write sentences promptly. The median reliability coefficient alphas for all age groups for the standard battery ranged from 0.81 to 0.94.
2.3.4.2.2 Cognition
A cognitive test battery covered by working memory, inhibition, and sustained attention will be administered to assess cognitive functions. All the instruments included in the study have undergone prior validation for use with the child population and cover the majority of cognitive domains affected by ADHD disorder (Wade et al., 2020).
The computerized n-back test will be utilized to evaluate the ability to update information in working memory, a component of executive control (Jacola et al., 2014). Participants will be presented with a sequence of stimuli, in this case fruits, and will need to determine if each stimulus matches the one presented ‘n’ items ago (Supplementary Figure S2). Each of the 336 trials will start with the presentation of a central fixation point, followed by an Inter-Trial Interval (ITI) lasting a maximum of 2,500 ms (varies depending on response time). Stimuli will then promptly appear after the ITI and remain on the screen for 500 ms. The n-back test will be built in Opensesame stimuli presentation software (Mathôt et al., 2012). The median reliability coefficient alpha for this task in children population ranges 0.60–0.80.
The computerized flanker test will be used to assess the capacity to inhibit irrelevant stimuli within executive control (Krueger et al., 2009). The test is designed to measure the effect of irrelevant stimuli on cognitive processes. Specifically, participants are tasked with identifying the direction in which a central stimulus (in this case, fishes) is pointing, while simultaneously inhibiting the influence of surrounding distractor stimuli (fishes) (Supplementary Figure S3). Each of the 180 trials will begin with the presentation of a central fixation point, followed by an ITI lasting 1,100 ms, 1,300 ms, or 1,500 ms (variable time). Stimuli will then promptly appear after the ITI and will remain on the screen until the participant responds or up to 3,000 ms. The flanker test will be built in Opensesame stimuli presentation software (Mathôt et al., 2012). The Cronbach’s alpha for the flanker task in children typically falls in the range of 0.70–0.85.
The Conners’ Continuous Performance Test (CPT-3) will be employed to assess sustained attention (McGee et al., 2000). This test will involve presenting a sequence of 360 trials on a screen, displaying letters A through X, with each letter appearing for 250 ms. These trials will be organized into 18 consecutive blocks, each consisting of 20 trials. The intervals between stimuli will vary among the blocks, ranging from 1 to 4 s. The proportion of target stimuli (non-X letters) will remain at 90% of the total trials. The Cronbach’s alpha for the CPT-3 in children falls in the range of 0.70–0.95.
2.3.4.2.3 Physical activity and sedentarism
PA and sedentarism will be measured through an objective measure such as accelerometers (Migueles et al., 2017; ActiGraph wGT3x-BT). Participants will be instructed to wear the accelerometer during their participation in the study (21 days). At baseline, a trained researcher will wear the accelerometer on the non-dominant wrist of the participant. Additionally, participants will be given a sheet where they must record when they do not have the accelerometer with them, as well as data related to sleep. They may remove the accelerometer only during water activities, including showering. Programming and data download will be done through the Actilife software (Version 6.13.4, ActiGraph, LLC). Each day that they will come to the laboratory, a trained researcher will charge the battery (once the experimental condition has been done).
2.3.4.2.4 PA intensity of the experimental conditions
Intensity of the experimental conditions will be assessed using two instruments:
a. Heart rate monitor. Participants will wear a Polar H10 (Speer et al., 2020) heart rate (HR) monitor connected to an iPad via the Polar Team application during the experimental conditions. This will allow us to gauge the PA intensity (classified into five resistance zones: 50–59% – 60–69% – 70–79% – 80–89% – 90–100%, of their HRmax).
b. Accelerometer. The same accelerometer worn by participants since the beginning of the study will continue to be used during the execution of the experimental conditions. This device will help measure the intensity of the PA, classifying it as light, moderate, moderate-to-vigorous.
2.3.4.2.5 Self-report of sedentarism
Sedentary behaviors will also be evaluated using the Youth Activity Profile—Spain (YAP-S). This self-administered questionnaire consists of 15 items and employs a 5-point Likert scale. It utilizes a 7-day recall format and has been validated for use with children (Segura-Díaz et al., 2021). In our study, participants will only need to respond to the final five questions (items 11–15), which specifically refer to sedentary habits. The Cronbach’s alpha for the YAP-S in children falls in the range of 0.70–0.85.
2.3.4.2.6 Sleep quality
Sleep quality will be assessed using the previously introduced accelerometer (ActiGraph wGT3x-BT) with the same data collection procedure as reported before. Moreover, participants will maintain a sleep log, recording details such as wake-up time, daytime sleep episodes, bedtime, sleep onset latency, and any nighttime awakenings.
2.3.4.2.7 Physical fitness components
Physical fitness will be evaluated using the ALPHA fitness test battery which determines speed agility by 4×10 shuttle run test, muscular fitness by handgrip strength (with a dynamometer; TKK 5101 Grip D) and standing long jump test (using a non-elastic tape; SECA 201) (Ruiz et al., 2011). Each measurement will be taken twice, and the maximum score of the two measurements will be recorded. Nonetheless, because of space limitations with our equipment, we will be unable to administer the “20-meter shuttle run test” from the ALPHA battery fitness test to assess cardiorespiratory fitness. Instead, we will adopt the validated “3-min step test” protocol (Jankowski et al., 2015). This test will involve using a step with a height of 30.5 cm with a stepping rate set at 96 beats per minute, which will be measured using a metronome. Moreover, the same pulsometer described earlier (Polar H10) will be used to determine the mean HR of one mine after the test (Speer et al., 2020).
2.3.4.2.8 Motor proficiency
The short form of the Bruininks-Oseretsky Test of Motor Proficiency (BOT-2) will be used (Bruininks and Bruininks, 2005). The short form is composed of 14 subtests based on fine motor precision, fine motor integration, manual dexterity, bilateral coordination, balance, running speed and agility, upper-limb coordination, and strength. The BOT-2 has been administered in children with ADHD (Adhvaryu et al., 2022). The BOT-2 demonstrates high internal consistency, with Cronbach’s alpha values typically ranging from 0.5 to 0.99 across its various subtests and composite scores.
2.3.4.2.9 Body composition
For body mass measurement, participants will be instructed to stand barefoot on an electronic scale (TANITA BC 601, Ltd) with an accuracy of 0.05 kg. Height will be measured using a stadiometer (SECA 213 Ltd) with an accuracy of 0.1 cm. Body mass index (BMI) will then be calculated as weight divided by height squared (kg/m2). Furthermore, waist circumference will be assessed using a non-elastic tape measure (SECA 201) with a range of 0–150 cm and an accuracy of 0.1 cm. Hip circumference will also be measured using the same non-elastic tape measure. Each measurement will be taken twice, and the mean of the two measurements will be recorded.
2.3.4.2.10 Biological maturation
Using data collected, including gender, age, weight, and height, we will determine the peak height velocity (PHV; Mirwald et al., 2002). To accomplish this, the participant’s brainstem height will be measured using the same stadiometer described earlier. This measurement will be repeated twice, and the average of both will be recorded. Additionally, the length of the lower limbs will be recorded, and calculated by subtracting the brainstem height from the overall height. Furthermore, the velocity of peak height growth (VPM) will be calculated using the equations proposed by Moore et al. (2015).
2.3.4.2.11 Verbal and non-verbal intelligence
The Kaufman Brief Intelligence test (K-BIT) will be used to measure verbal and non-verbal intelligence (Cordero and Calonge, 2000). All assessments are grounded in the scores attained from the vocabulary tests, which encompass 45 items of expressive vocabulary and 37 items of definitions, as well as the matrix test consisting of 48 items. This test has been used in children with ADHD (Rodriguez-Martínez et al., 2023). The KBIT- demonstrates high internal consistency, with Cronbach’s alpha values typically ranging from 0.80 to 0.96 across its verbal, non-verbal, and composite scales.
2.3.4.2.12 Mental health difficulties
A parent version of the Spanish-adapted Strengths and Difficulties Questionnaire (SDQ; Barriuso-Lapresa et al., 2014) will be used to evaluate mental health difficulties in children. This questionnaire comprises 25 items and utilizes a 3-point Likert scale. It assesses five dimensions of mental health: emotional problems, behavior problems, hyperactivity-inattention, problems with peers, and prosocial behavior. Parents will provide responses based on their observations of their children’s behavior over the past 6 months. The SDQ has moderate to good internal consistency, with Cronbach’s alpha values generally ranging from 0.50 to 0.83 across its subscales and total difficulties score.
2.3.4.2.13 School grades
An additional academic record will be acquired by gathering the most recent participants’ school grades. Grades in mathematics, Spanish language, Catalan language, and Physical Education will be collected, each scored on a scale from 0 to 10. Subsequently, the Grade Point Average (GPA) will be calculated as the overall average of these grades.
2.3.4.3 Confounding variables
2.3.4.3.1 Sociodemographic characteristics
Socioeconomic status of the children will be assessed using the Family Affluence Scale (FAS-II; Boyce et al., 2006), Version II, a validated instrument consisting of four items specifically designed for measuring socioeconomic status.
2.3.4.3.2 Parental education and occupation level
Parental educational levels will be assessed using a self-report questionnaire completed by both, of the participants’ parents. The questionnaire will include options such as “no elementary school,” “elementary school,” “middle school,” “high school,” and “university completed.” Additionally, the occupations of the participants’ parents will be categorized according to the International Standard Classification of Occupations (ISCO-08) developed by the International Labor Organization. This classification comprises 13 categories: Directors and managers, Scientific and intellectual professionals, Technicians and mid-level professionals, Administrative support personnel, Service workers and salespeople in shops and markets, Farmers and skilled agricultural workers, forestry, and fishing, Officers, operators, and artisans of mechanical arts and other trades, Plant and machine operators and assemblers, Elementary occupations, Military occupations, Housemaker, and Unemployment.
2.3.4.3.3 ADHD symptoms
A Spanish-adapted version of the ADHD Rating Scale-IV (Vallejo-Valdivielso et al., 2019), parent edition, will be used to gauge the frequency of symptoms linked to ADHD. This tool comprises 18 items, divided equally between inattention and hyperactivity, and employs a 3-point Likert scale. Parents will provide their assessments based on observations of their children’s behavior over the previous 6 months. The ADHD Rating Scale-IV parent edition shows excellent internal consistency, with Cronbach’s alpha values typically ranging from 0.86 to 0.96 across its subscales and total score.
2.3.5 Data analysis
Analyses of the outcomes will be conducted using linear mixed models in IBM SPSS Statistics for Windows, Version 20.0 (IBM, Armonk, New York, USA), with alpha levels set at p < 0.05. These models will evaluate the impact of the experimental condition (PA with cognitive engagement, PA without cognitive engagement, or cognitively engaging control), time (baseline, posttest 1, posttest 2, and posttest 3), group (with and without ADHD), and condition-by-group-by-time interaction. Random effects will be incorporated to address the clustered nature of the data. Furthermore, we will assess all assumptions and adjust our analyses for any necessary control variables.
2.4 Phase II: school settings
2.4.1 Sample size and power
A between subjects, 2 conditions (video-based PA program, and control condition) × 2 times (pretest vs. posttest) repeated measures ANOVA design with 138 participants should be sufficiently powered to detect interactions at or above moderate effect sizes f = 0.25 which translates to an approximate Cohen’s d = 0.5 assuming alpha at 0.05, power at 80%, and a correlation among 2 repeated measures of 0.75. Considering these estimations, and a potential dropout rate of 10% observed in similar studies (Mora-Gonzalez et al., 2019), our investigation will recruit 600 participants.
2.4.2 Recruitment and randomization
Recruitment primarily involves contacting to schools in the Balearic Islands via email. The email addresses of each primary school were acquired from the Spanish Ministry of Education website. Once recruited, an initial virtual meeting was made to explain the study’s objectives. Figure 3 illustrates the flow diagram of the participant’s recruitment process. Recruitment began in March 2024 and is still ongoing. Once teachers and parents agree to participate, they sign a written informed consent form before the start of the intervention. In line with phase I, this study will also obtain verbal assent from participating children. Only those who provide verbal agreement, having fully understood the study’s aims and procedures, will be included.
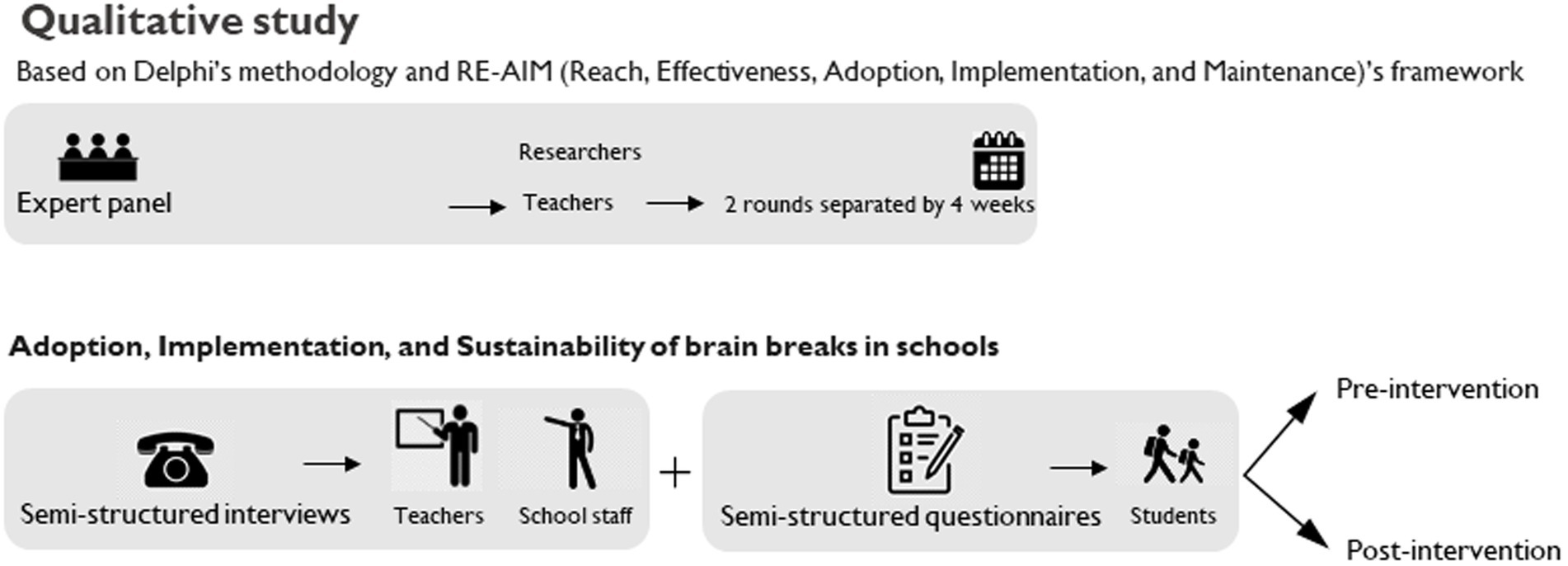
Figure 3. Flow diagram of the participant’s recruitment process.
Randomization of schools into experimental conditions for phase II is carried out using R software by an external statistician.
2.4.3 Experimental protocol
The experimental protocol will be composed of two parts: (a) qualitative: the experimental condition will be developed through a qualitative design involving semi-structured interviews with teachers and school staff, along with semi-structured questionnaires administered to students (Figure 2B). The same process will be replicated after the intervention; (b) quantitative: the intervention will be implemented within school settings during regular curricular hours, taking place inside the classroom (Figure 2A). Specifically, schools randomly selected and assigned to the research arms (video-based PA program, or control condition) will conduct educational achievement assessments twice, separated by 8 weeks. The initial assessment will occur at the pretest stage (week 1), followed by a second assessment immediately after 8 weeks of intervention (week 10).
2.4.3.1 Video-based physical activity program
The experimental condition will occur daily within regular academic lessons. Students in each classroom will engage in the intervention once a day. The classroom teacher, responsible for conducting the intervention, will choose the appropriate time for implementation. The intervention will not be scheduled during PE lessons or immediately after them, nor during lessons following recess.
The administration of this intervention will use a digital platform accessible to each classroom teacher via a password-protected link.4 This platform will facilitate the easy and efficient administration of the video-based PA program. It will feature 10 videos, with five different themes, administered in a randomized manner according to the researcher’s guidelines. However, no theme will repeat throughout the week. To ensure proper use of this tool, classroom teachers will undergo training conducted by the research team before initiating the intervention.
During the intervention, students will follow the instructions in the video and replicate the PA in a gamified format. The structure of the video-based PA program will comprise seven sets of 40-s PA alternated with seven sets of 20-s rest periods, totaling 7 min of intervention with a 2:1 work-to-rest ratio. The PA will target both aerobic and strength-based metabolism, following a strategy with low integration-low relevance movements (Mavilidi et al., 2022).
2.4.3.2 Control group
During the 8-week intervention period, the control group will continue receiving usual academic lessons, without the inclusion of PA that may impact their typical levels during school hours.
2.4.4 Measures
Each educational agent (teachers, school staff, and students) will be involved in the qualitative aspect of this phase and will undergo evaluation 1 month before and 1 month after the intervention. On the other hand, each student from each participating school will undergo evaluation for quantitative variables both before the intervention (1 week before its start) and after the intervention (1 week following its conclusion).
2.4.4.1 Primary outcome measures
2.4.4.1.1 Cognition
A cognitive test battery encompassing working memory, cognitive flexibility, and selective attention will be administered to evaluate cognitive functions. All tests used in this study have undergone previous validation for their appropriateness with the children population.
2.4.4.1.2 Working memory
An adapted version of the digit memory test will be used to measure the working memory (Hill et al., 2010). Students will listen to digit sequences and write them down (i.e., 1, 4, 6). If successful, longer sequences will be given until two consecutive failures occur. One researcher dictates while another oversees. This test includes: “Digits Forward,” where participants write the digits in the given order, and “Backward Digit-Span,” where participants write the digits in reverse order.
2.4.4.1.3 Cognitive flexibility
An adapted version of the Trail-making test (TMT) will be used to assess cognitive flexibility (Howie et al., 2015). The TMT will comprise two parts: (a) TMT-A will evaluate processing speed and visual attention, requiring participants to connect numbers from 1 to 25 in order; (b) TMT-B will assess cognitive flexibility by alternating between numbers and letters in ascending and alphabetical order. Students will record completion times using a digital stopwatch displayed on a screen. The test will be supervised by the two researchers. For the Trail Making Test (TMT) used with children, Cronbach’s alpha generally falls within 0.60–0.80 for its subtests, reflecting moderate reliability.
The d2, test of attention will be used to assess the selective attention (Brickenkamp, 2012). Students must carefully scan each of the 14 lines of the test from left to right, identifying any “d” with two small lines. These are considered relevant elements, while other combinations are irrelevant. Each line allows 20 s for assessment, with one researcher monitoring time and another ensuring the process runs smoothly. For the d2 in children, Cronbach’s alpha values are generally reported to be between 0.75 and 0.90, indicating strong internal consistency.
2.4.4.2 Secondary outcome measures
2.4.4.2.1 Academic performance
The academic fluency index and their subtests will be assessed similarly to phase I of the study (Muñoz-Sandoval et al., 2005). However, the procedure will vary. In this instance, all students within a specific classroom will undertake the tests simultaneously, with two trained researchers overseeing to ensure that each student completes it independently (time will be monitored using a chronometer).
2.4.4.2.2 Design and feasibility of active breaks
The responses collected from semi-structured interviews with teachers and school staff, along with the semi-structured questionnaires administered to students, will be instrumental in shaping the design and assessing the feasibility of implementing active breaks. These tools will be rigorously validated through a Delphi methodology, involving a panel of at least 10 experts (Gillis et al., 2013). The questions will be developed using the RE-AIM framework and further refined according to the guidelines provided by Daly-Smith et al. (2021).
2.4.4.2.3 Physical activity and sedentarism
PA and sedentarism will be calculated by accelerometry (ActiGraph wGT3x-BT), using the same instrument and procedure in phase I (Migueles et al., 2017). Due to the limited availability of accelerometers, one accelerometer will be assigned to each classroom. This accelerometer will rotate among students daily (24-h) until each student has had a turn, being the classroom teacher responsible for its safekeeping. The classroom teacher will keep track of who will wear the accelerometer every day. Moreover, a researcher will handle data retrieval and recharge the battery once a week.
2.4.4.2.4 Intensity of the active breaks
Intensity of the active breaks will be measured by accelerometry (Migueles et al., 2017). Following the procedure of the above section, intensity of the active breaks will be measured. For this reason, the classroom teacher will receive a sheet to note at which time (hours: minutes: seconds) started and finished every active break.
2.4.4.2.5 Self-report of physical activity patterns
An adapted Spanish version of the PA questionnaire for children (PAQ-C) will be administered to evaluate PA patterns (Manchola-González et al., 2017). This self-administered questionnaire employs a seven-day recall period, comprising nine items measured on a 5-point Likert scale. For the PAQ-C, Cronbach’s alpha generally ranges from 0.70 to 0.85, reflecting good internal consistency.
2.4.4.2.6 Self-report of sedentarism
Sedentary patterns will be calculated using the same instrument and procedure (although, in this case, the evaluation will take place within a classroom setting) as in phase I (Segura-Díaz et al., 2021).
2.4.4.2.7 Sleep quality
Following the established procedure for measuring PA and sedentary patterns, sleep quality will be assessed using accelerometry (ActiGraph wGT3x-BT).
2.4.4.2.8 Self-report of physical fitness
Physical fitness will be measured through the adapted Spanish version of the International Fitness Scale (Sánchez-López et al., 2015). This instrument is composed of five items on a 5-point Likert scale. The Cronbach’s alpha of the International Fitness Scale in children, is generally reported to be between 0.70 and 0.85, indicating good internal consistency.
2.4.4.2.9 Self-report of body composition
The height (cm) and weight (kg) of the students will be self-reported by parents, which is a reliable alternative to direct measurements (Rios-Leyvraz et al., 2022). Then, BMI will be also calculated (kg/m2).
2.4.4.2.10 Students’ classroom behavior
Classroom teachers will employ two parts (inattention and hyperactivity-impulsivity) of the Child and Adolescent Behavior Inventory (CABI). Each of these parts is composed of nine items and uses a 6-point Likert scale (Burns et al., 2023).
2.4.4.2.11 Creativity
An adaptation of the Alternative uses task (AUT) will be used to measure creativity (Olson et al., 2021). Students will be required to complete the maximum number of unusual uses for two objects within a 3-min timeframe (with one researcher overseeing the timing and another guaranteeing of the process).
2.4.4.3 Confounding variables
The socioeconomic status of the children will be assessed using the validated Family Affluence Scale (FAS-II), which consists of four items specifically designed to measure socioeconomic status (Boyce et al., 2006). Additionally, self-reported body composition and self-reported PA patterns will also be considered as confounding variables in the analysis.
2.4.5 Implementation strategies and cost-effectiveness analyses
To guarantee the correct development of the intervention, a few implementation strategies will be conducted during the intervention period providing professional training for teachers (i.e., initial meeting before the start of the intervention); offering direct support from researchers (i.e., weekly visit at the school, and direct contact by e-mail or WhatsApp); granting access to the Break4Brain website for administering active breaks; and ensuring fidelity and follow-up of the active breaks (i.e., recording one active break weekly, and documenting daily participation of students).
Concerning the cost-effectiveness analyses, trial costs, and outcomes will be extrapolated to the Spanish population aged 10–12 in government schools, to assess the potential lifetime health and cost outcomes resulting from the intervention (Brown et al., 2024). The cost-effectiveness model will be determined using the validated ACE-Obesity Policy model (Ananthapavan et al., 2020).
2.4.6 Data analysis
2.4.6.1 Quantitative analysis
The outcomes will be analyzed utilizing linear mixed models in IBM SPSS Statistics for Windows, V.20.0 (IBM, Armonk, New York, USA), with significance levels set at p < 0.05. These models will evaluate the effects of the condition (video-based PA program and control group), time (pre and posttest), and the interaction between condition and time. Random effects will be incorporated to address the nested nature of the data, adjusting for clustering effects at the school level. Additionally, baseline PA levels, obesity status, gender, and age will be considered as potential moderators in the analysis. Moreover, all assumptions will be tested, and analyses will be adjusted for control variables if necessary.
2.4.6.2 Qualitative analysis
Qualitative data will be gathered through semi-structured interviews and questionnaires administered by trained researchers. Thematic analysis techniques and a grounded theory approach will organize and manage all essential information obtained from the interviews. Quantitative data of the semi-structured questionnaire will be summarized into means and standard deviations. Semi-structured interviews will be audio-recorded, transcribed verbatim, and anonymized before coding. The analysis will be conducted using “NVivo version 12 Plus” software (QRS International-Melbourne, Australia).
3 Discussion
The main objective of the Break4Brain Project is to examine the acute and chronic effects of PA (either with or without cognitive engagement) on academic performance, cognitive function, and brain function in ADHD-diagnosed and non-diagnosed children, in controlled laboratory settings and schools.
Recently, there has been a surge in studies evaluating the impact of active breaks on various educational outcomes in children (Watson et al., 2017; Daly-Smith et al., 2018). A predominant focus of these studies has been on investigating the effects of PA specifically on children without neurodevelopmental disorders. A strength of this study is that it will compare the findings of children with and without ADHD. Thus, an exploration into this area is warranted to elucidate potential variations in response to acute PA, ultimately facilitating the development of more tailored and effective interventions (in parameters of duration, intensity, or PA type) in both populations.
Based on previous research, our hypothesis for the cross-over design (phase I) is that the experimental conditions involving PA will enhance performance on the studied outcomes. Our recent meta-analysis found that a single bout of PA significantly improves academic outcomes Hedge’s g = 0.35, 95% CI: 0.20–0.50; Muntaner-Mas et al., 2024. However, while our meta-analysis highlighted the overall benefits of PA, it did not reveal that specific characteristics such as intensity or duration significantly moderated the magnitude of these effects. This absence of moderation raises intriguing questions about what other factors might drive the observed improvements. We speculate that the type of PA, rather than just its intensity or duration, may play a crucial role in influencing outcomes. Specifically, we draw on Mavilidis’ theory-driven approach (Mavilidi et al., 2022), which emphasizes the importance of the cognitive and contextual relevance of PA in enhancing learning and academic achievement. According to this framework, physical activities that are less integrated with academic content and have lower cognitive demands may paradoxically yield more significant improvements in certain outcomes. Thus, we speculate that our experimental conditions characterized by low integration and low relevance may lead to the most substantial gains in the studied outcomes. By exploring these nuanced interactions between PA type and academic achievement, our study aims to advance the understanding of how different forms of PA can be strategically employed to enhance educational outcomes, particularly in settings involving children with varying cognitive needs and abilities.
Despite numerous investigations into the effects of PA in children with ADHD, the precise impact on brain function, cognition, and academic performance remains elusive (Chan et al., 2022; Welsch et al., 2021). Current research has primarily focused on specific outcomes or short-term effects, often neglecting a holistic approach that includes a comprehensive battery of tests to assess these variables simultaneously. To the best of our knowledge, there is a significant gap in research that thoroughly examines the effects of acute PA on both brain function and academic performance in children with ADHD, particularly in comparison to their non-ADHD peers. This gap is especially critical given that children with ADHD may exhibit unique responses to PA interventions due to their distinct neurocognitive and behavioral characteristics. These differences suggest that PA might influence ADHD and non-ADHD children in divergent ways, potentially offering specialized benefits or necessitating tailored intervention strategies to maximize effectiveness. For example, a meta-analysis by Li et al. (2023) found that cognitively engaging exercises are particularly effective in improving attention problems in school-aged children with ADHD. This highlights the possibility that specific types of PA, especially those that engage cognitive processes, could be more beneficial for children with ADHD compared to their non-ADHD counterparts.
Regarding school settings, there has often been a disconnect between research evidence and the practical implementation of past interventions (McMullen et al., 2014). For instance, while existing evidence suggests certain strategies might be effective, qualitative feedback from educators reveals differing preferences. Teachers, for example, have consistently expressed a preference for short, video-based PA breaks lasting less than 10 min. This highlights the importance of aligning research with the practical realities and preferences within educational settings to enhance both feasibility and effectiveness. To address this challenge, our cluster RCT will be collaboratively designed with input from educational stakeholders, ensuring that the strategies are not only evidence-based but also practical, sustainable, and aligned with the day-to-day demands of teachers and students. This collaborative approach is crucial for the successful integration of active breaks into the school routine, as it fosters a sense of ownership and relevance among educators, which in turn, increases the likelihood of long-term adoption and sustainability. Moreover, the Break4Brain project’s digital platform significantly alleviates the workload for teachers by providing pre-designed, video-based PA breaks. These videos include clear, step-by-step instructions, allowing teachers to easily implement the activity by simply selecting the appropriate video. This system minimizes the preparation required by teachers and seamlessly integrates PA into the classroom environment without disrupting the flow of the school day. In this sense, and to our knowledge, this is the most comprehensive study in the field of active breaks, as it not only incorporates rigorous research methodologies but also addresses the practical needs of educators through a hybrid type 1 implementation-effectiveness trial. This approach ensures that the interventions are both effective in improving student outcomes and feasible for long-term implementation in real-world educational settings, bridging the gap between research and practice in a meaningful way.
Another strength of this study is that it will measure the fidelity of each student (and class) to the intervention. A recent systematic review and meta-analysis revealed that most published studies have failed to assess fidelity to active breaks (Ruhland and Lange, 2021). This underscores the significance of our approach in ensuring that interventions are implemented as intended, thereby enhancing the reliability and validity of our findings. Additionally, following statements from other systematics reviews (Watson et al., 2017; Infantes-Paniagua et al., 2021), PA patterns and active break intensity will be measured with objective instruments such as accelerometers or HR monitors (in both phases). On the other hand, several limitations warrant mention: (i) the generalizability of the results may be limited to our population context (encompassing factors such as primary school stage, socioeconomic status, etc.); (ii) resource constraints will necessitate the daily rotation of accelerometers among students during phase II.
Ethics statement
The studies involving humans were approved by the Ethics Committee of the University of the Balearic Island. The studies were conducted in accordance with the local legislation and institutional requirements.
Author contributions
DA: Writing – review & editing, Writing – original draft. MB-T: Writing – review & editing. AO: Writing – review & editing. JCa: Writing – review & editing. FP: Writing – review & editing. PP-S: Writing – review & editing. JCo: Writing – review & editing. IF: Writing – review & editing. AG-P: Writing – review & editing, Conceptualization. JT: Writing – review & editing. CS: Writing – review & editing. VS-A: Writing – review & editing, Conceptualization. RL-P: Writing – review & editing, Conceptualization. DA-R: Writing – review & editing, Conceptualization. AM-M: Writing – review & editing, Supervision, Funding acquisition, Conceptualization.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was funded by MCIN/AEI/10.13039/501100011033/ and by FEDER Una manera de hacer Europa under grant number PID2021-123357OA-100. Furthermore, it has received complementary funding from the Institute for Education Research and Innovation (IRIE-UIB).
Acknowledgments
The authors extend their gratitude to all participants who will contribute to the execution of the study (in both phases), especially to the schools for their invaluable assistance in the promotion (phase I) and participation (phase II) in project.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2024.1451731/full#supplementary-material
Footnotes
1. ^https://doi.org/10.5281/zenodo.8374014
2. ^https://www.youtube.com/watch?v=PN7w1X5jPK0
3. ^https://www.youtube.com/watch?v=rZr8geozI_s&list=LL&index=10
References
Adhvaryu, K. P., Karthikbabu, S., and Rao, P. T. (2022). Motor performance of children with attention deficit hyperactivity disorder: focus on the Bruininks-Oseretsky test of motor proficiency. Clin. Exp. Pediatr. 65, 512–520. doi: 10.3345/cep.2021.00962
Álvarez-Bueno, C., Pesce, C., Cavero-Redondo, I., Sánchez-López, M., Martínez-Hortelano, J. A., and Martínez-Vizcaíno, V. (2017). The effect of physical activity interventions on Children’s cognition and metacognition: a systematic review and meta-analysis. J. Am. Acad. Child Adolesc. Psychiatry 56, 729–738. doi: 10.1016/j.jaac.2017.06.012
Ananthapavan, J., Sacks, G., Brown, V., Moodie, M., Nguyen, P., Veerman, L., et al. (2020). Priority-setting for obesity prevention—the assessing cost-effectiveness of obesity prevention policies in Australia (ACE-obesity policy) study. PLoS One 15:e0234804. doi: 10.1371/journal.pone.0234804
Barriuso-Lapresa, L. M., Hernando-Arizaleta, L., and Rajmil, L. (2014). Reference values of the strengths and difficulties questionnaire (SDQ) version for parents in the Spanish population, 2006. Actas Esp. Psiquiatr. 42, 43–48
Bedard, C., Bremer, E., Graham, J. D., Chirico, D., and Cairney, J. (2021). Examining the effects of acute cognitively engaging physical activity on cognition in children. Front. Psychol. 12:653133. doi: 10.3389/fpsyg.2021.653133
Best, J. R. (2010). Effects of physical activity on children’s executive function: contributions of experimental research on aerobic exercise. Dev. Rev. 30, 331–351. doi: 10.1016/j.dr.2010.08.001
Boyce, W., Torsheim, T., Currie, C., and Zambon, A. (2006). The family affluence scale as a measure of national wealth: validation of an adolescent self-report measure. Soc. Indic. Res. 78, 473–487. doi: 10.1007/s11205-005-1607-6
Brickenkamp, R. (2012). D2, Test de Atención (adaptación española de Seisdedos). Madrid: TEA ediciones.
Brown, V., Sheppard, L., Salmon, J., Arundell, L., Cerin, E., Ridgers, N. D., et al. (2024). Cost-effectiveness of reducing children’s sedentary time and increasing physical activity at school: the transform-us! intervention. Int. J. Behav. Nutr. Phys. Act. 21:15. doi: 10.1186/s12966-024-01560-3
Bruininks, R. H., and Bruininks, B. D. (2005). BOT-2 Bruininks-Oseretsky test of motor proficiency. 2nd Edn. Minneapolis, Minnesota: Pearson Assessments.
Bull, F. C., Al-Ansari, S. S., Biddle, S., Borodulin, K., Buman, M. P., Cardon, G., et al. (2020). World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 54, 1451–1462. doi: 10.1136/bjsports-2020-102955
Burns, G. L., Montaño, J. J., Becker, S. P., and Servera, M. (2023). Cognitive disengagement syndrome symptoms from early childhood to adolescence in a nationally representative Spanish sample. J. Clin. Child Adolesc. Psychol. doi: 10.1080/15374416.2023.2272944 [Online ahead of print]
Chalkley, A. E., Routen, A. C., Harris, J. P., Cale, L. A., Gorely, T., and Sherar, L. B. (2018). A retrospective qualitative evaluation of barriers and facilitators to the implementation of a school-based running programme. BMC Public Health 18:1189. doi: 10.1186/s12889-018-6078-1
Chan, Y. S., Jang, J. T., and Ho, C. S. (2022). Effects of physical exercise on children with attention deficit hyperactivity disorder. Biom. J. 45, 265–270. doi: 10.1016/j.bj.2021.11.011
Cordero, A., and Calonge, I. (2000). Adaptación española del K-BIT: test breve de inteligencia de Kaufman [Spanish adaptation of the K-BIT: Kaufman’s brief intelligence test]. K-BIT: Test Breve de Inteligencia de Kaufman, 51–60.
Curran, G. M., Bauer, M., Mittman, B., Pyne, J. M., and Stetler, C. (2012). Effectiveness-implementation hybrid designs: combining elements of clinical effectiveness and implementation research to enhance public health impact. Med. Care 50, 217–226. doi: 10.1097/MLR.0b013e3182408812
Daly-Smith, A., Morris, J. L., Norris, E., Williams, T. L., Archbold, V., Kallio, J., et al. (2021). Behaviours that prompt primary school teachers to adopt and implement physically active learning: a meta synthesis of qualitative evidence. Int. J. Behav. Nutr. Phys. Act. 18:151. doi: 10.1186/s12966-021-01221-9
Daly-Smith, A. J., Zwolinsky, S., McKenna, J., Tomporowski, P. D., Defeyter, M. A., and Manley, A. (2018). Systematic review of acute physically active learning and classroom movement breaks on children’s physical activity, cognition, academic performance and classroom behaviour: understanding critical design features. BMJ Open Sport Exerc. Med. 4:e000341. doi: 10.1136/bmjsem-2018-000341
de Greeff, J. W., Bosker, R. J., Oosterlaan, J., Visscher, C., and Hartman, E. (2018). Effects of physical activity on executive functions, attention and academic performance in preadolescent children: a meta-analysis. J. Sci. Med. Sport 21, 501–507. doi: 10.1016/j.jsams.2017.09.595
Delorme, A., and Makeig, S. (2004). EEGLAB: an open source toolbox for analysis of single-trial EEG dynamics including independent component analysis. J. Neurosci. Methods 134, 9–21. doi: 10.1016/j.jneumeth.2003.10.009
Faraone, S. V., Asherson, P., Banaschewski, T., Biederman, J., Buitelaar, J. K., Ramos-Quiroga, J. A., et al. (2015). Attention-deficit/hyperactivity disorder. Nat. Rev. Dis. Primers 1:15020. doi: 10.1038/nrdp.2015.20
Faraone, S. V., Banaschewski, T., Coghill, D., Zheng, Y., Biederman, J., Bellgrove, M. A., et al. (2021). The world federation of ADHD international consensus statement: 208 evidence-based conclusions about the disorder. Neurosci. Biobehav. Rev. 128, 789–818. doi: 10.1016/j.neubiorev.2021.01.022
Galvez-Pol, A., Calvo-Merino, B., Capilla, A., and Forster, B. (2018). Persistent recruitment of somatosensory cortex during active maintenance of hand images in working memory. Neuroimage 174, 153–163. doi: 10.1016/j.neuroimage.2018.03.024
Galvez-Pol, A., Forster, B., and Calvo-Merino, B. (2018). Modulation of motor cortex activity in a visual working memory task of hand images. Neuropsychologia 117, 75–83. doi: 10.1016/j.neuropsychologia.2018.05.005
Gelabert, J., Sánchez-Azanza, V., Palou, P., and Muntaner-Mas, A. (2023). Efectos agudos de los descansos activos sobre la atención selectiva en escolares acute effects of active breaks on selective attention in schoolchildren. Revista de Psicología del Deporte 32, 277–286.
Gelman, R., Whelan, J., Spiteri, S., Duric, D., Oakhill, W., Cassar, S., et al. (2023). Adoption, implementation, and sustainability of early childhood feeding, nutrition and active play interventions in real-world settings: a systematic review. Int. J. Behav. Nutr. Phys. Act. 20:32. doi: 10.1186/s12966-023-01433-1
Giedd, J. N., Blumenthal, J., Jeffries, N. O., Castellanos, F. X., Liu, H., Zijdenbos, A., et al. (1999). Brain development during childhood and adolescence: a longitudinal MRI study. Nat. Neurosci. 2, 861–863. doi: 10.1038/13158
Gillis, L., Tomkinson, G., Olds, T., Moreira, C., Christie, C., Nigg, C., et al. (2013). Research priorities for child and adolescent physical activity and sedentary behaviours: an international perspective using a twin-panel Delphi procedure. Int. J. Behav. Nutr. Phys. Act. 10:112. doi: 10.1186/1479-5868-10-112
Glasgow, R. E., Vogt, T. M., and Boles, S. M. (1999). Evaluating the public health impact of health promotion interventions: the RE-AIM framework. Am. J. Public Health 89, 1322–1327. doi: 10.2105/AJPH.89.9.1322
Grassmann, V., Alves, M. V., Santos-Galduróz, R. F., and Galduróz, J. C. F. (2017). Possible cognitive benefits of acute physical exercise in children with ADHD: a systematic review. J. Atten. Disord. 21, 367–371. doi: 10.1177/1087054714526041
Guthold, R., Stevens, G. A., Riley, L. M., and Bull, F. C. (2020). Global trends in insufficient physical activity among adolescents: a pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolescent Health 4, 23–35. doi: 10.1016/S2352-4642(19)30323-2
Halperin, J. M., Berwid, O. G., and O’Neill, S. (2014). Healthy body, healthy mind? The effectiveness of physical activity to treat ADHD in children. Child Adolesc. Psychiatr. Clin. N. Am. 23, 899–936. doi: 10.1016/j.chc.2014.05.005
Harrison, J. R., Soares, D. A., Rudzinski, S., and Johnson, R. (2019). Attention deficit hyperactivity disorders and classroom-based interventions: evidence-based status, effectiveness, and moderators of effects in single-case design research. Rev. Educ. Res. 89, 569–611. doi: 10.3102/0034654319857038
Hill, L., Williams, J. H. G., Aucott, L., Milne, J., Thomson, J., Greig, J., et al. (2010). Exercising attention within the classroom. Dev. Med. Child Neurol. 52, 929–934. doi: 10.1111/j.1469-8749.2010.03661.x
Howie, E. K., and Pate, R. R. (2012). Physical activity and academic achievement in children: a historical perspective. J. Sport Health Sci. 1, 160–169. doi: 10.1016/j.jshs.2012.09.003
Howie, E. K., Schatz, J., and Pate, R. R. (2015). Acute effects of classroom exercise breaks on executive function and math performance: a dose-response study. Res. Q. Exerc. Sport 86, 217–224. doi: 10.1080/02701367.2015.1039892
Hoza, B., Martin, C. P., Pirog, A., and Shoulberg, E. K. (2016). Using physical activity to manage ADHD symptoms:the state of the evidence. Curr. Psychiatry Rep. 18:113. doi: 10.1007/s11920-016-0749-3
Infantes-Paniagua, Á., Silva, A. F., Ramirez-Campillo, R., Sarmento, H., González-Fernández, F. T., González-Víllora, S., et al. (2021). Active school breaks and students’ attention: a systematic review with meta-analysis. Brain Sci. 11:675. doi: 10.3390/brainsci11060675
Jacola, L. M., Willard, V. W., Ashford, J. M., Ogg, R. J., Scoggins, M. A., Jones, M. M., et al. (2014). Clinical utility of the N-back task in functional neuroimaging studies of working memory. J. Clin. Exp. Neuropsychol. 36, 875–886. doi: 10.1080/13803395.2014.953039
Jankowski, M., Niedzielska, A., Brzezinski, M., and Drabik, J. (2015). Cardiorespiratory fitness in children: a simple screening test for population studies. Pediatr. Cardiol. 36, 27–32. doi: 10.1007/s00246-014-0960-0
Johnson, S. B., Blum, R. W., and Giedd, J. N. (2009). Adolescent maturity and the brain: the promise and pitfalls of neuroscience research in adolescent health policy. J. Adolesc. Health 45, 216–221. doi: 10.1016/j.jadohealth.2009.05.016
Kennedy, S. G., Sanders, T., Estabrooks, P. A., Smith, J. J., Lonsdale, C., Foster, C., et al. (2021). Implementation at-scale of school-based physical activity interventions: a systematic review utilizing the RE-AIM framework. Obes. Rev. 22:e13184. doi: 10.1111/obr.13184
Koorts, H., Timperio, A., Abbott, G., Arundell, L., Ridgers, N. D., Cerin, E., et al. (2022). Is level of implementation linked with intervention outcomes? Process evaluation of the TransformUs intervention to increase children’s physical activity and reduce sedentary behaviour. Int. J. Behav. Nutr. Phys. Act. 19:122. doi: 10.1186/s12966-022-01354-5
Krueger, C. E., Bird, A. C., Growdon, M. E., Jang, J. Y., Miller, B. L., and Kramer, J. H. (2009). Conflict monitoring in early frontotemporal dementia. Neurology 73, 349–355. doi: 10.1212/WNL.0b013e3181b04b24
Lander, N. J., Contardo Ayala, A. M., Mazzoli, E., Lai, S. K., Orr, J., and Salmon, J. (2024). Beyond “brain breaks”: a new model for integrating classroom-based active breaks. J. Phys. Educ. Recreat. Dance 95, 22–30. doi: 10.1080/07303084.2024.2308253
Lane, C., Naylor, P. J., Shoesmith, A., Wolfenden, L., Hall, A., Sutherland, R., et al. (2022). Identifying essential implementation strategies: a mixed methods process evaluation of a multi-strategy policy implementation intervention for schools. Int. J. Behav. Nutr. Phys. Act. 19:44. doi: 10.1186/s12966-022-01281-5
Li, D., Li, L., Zang, W., Wang, D., Miao, C., Li, C., et al. (2023). Effect of physical activity on attention in school-age children with ADHD: a systematic review and meta-analysis of randomized controlled trials. Front. Physiol. 14:1189443. doi: 10.3389/fphys.2023.1189443
Li, J. W., O’Connor, H., O’Dwyer, N., and Orr, R. (2017). The effect of acute and chronic exercise on cognitive function and academic performance in adolescents: a systematic review. J. Sci. Med. Sport 20, 841–848. doi: 10.1016/j.jsams.2016.11.025
Li, T., Yu, T., Hawkins, B. S., and Dickersin, K. (2015). Design, analysis, and reporting of crossover trials for inclusion in a Meta-analysis. PLoS One 10:e0133023. doi: 10.1371/journal.pone.0133023
Lubans, D., Richards, J., Hillman, C., Faulkner, G., Beauchamp, M., Nilsson, M., et al. (2016). Physical activity for cognitive and mental health in youth: a systematic review of mechanisms. Pediatrics 138, –e20161642.
Lubans, D. R., Sanders, T., Noetel, M., Parker, P., McKay, H., Morgan, P. J., et al. (2022). Scale-up of the internet-based professional learning to help teachers promote activity in youth (iPLAY) intervention: a hybrid type 3 implementation-effectiveness trial. Int. J. Behav. Nutr. Phys. Act. 19:141. doi: 10.1186/s12966-022-01371-4
Luck, S. (2014). An introduction to the event-related potential technique. London, England: Cambridge.
Mahar, M. T., Murphy, S. K., Rowe, D. A., Golden, J., Shields, A. T., and Raedeke, T. D. (2006). Effects of a classroom-based program on physical activity and on-task behavior. Med. Sci. Sports Exerc. 38, 2086–2094. doi: 10.1249/01.mss.0000235359.16685.a3
Manchola-González, J., Bagur-Calafat, C., and Girabent-Farrés, M. (2017). Fiabilidad de la versión española del Cuestionario de actividad física PAQ-C / Reliability of the Spanish Version of Questionnaire of Physical Activity PAQ-C. Revista Internacional de Medicina y Ciencias de la Actividad Física y del Deporte 65, 139–152. doi: 10.15366/rimcafd2017.65.010
Mathôt, S., Schreij, D., and Theeuwes, J. (2012). OpenSesame: an open-source, graphical experiment builder for the social sciences. Behav. Res. 44, 314–324. doi: 10.3758/s13428-011-0168-7
Mavilidi, M. F., Pesce, C., Benzing, V., Schmidt, M., Paas, F., Okely, A. D., et al. (2022). Meta-analysis of movement-based interventions to aid academic and behavioral outcomes: a taxonomy of relevance and integration. Educ. Res. Rev. 37:100478. doi: 10.1016/j.edurev.2022.100478
Mavillidi, M., Mason, C., Leahy, A., Kennedy, S., Eather, N., Hillman, C., et al. (2021). Effect of a time-efficient physical activity intervention on senior school students’ on-task behaviour and subjective vitality: the ‘burn 2 learn’ cluster randomised controlled trial. Educ. Psychol. Rev. 33, 299–323. doi: 10.1007/s10648-020-09537-x
McGee, R. A., Clark, S. E., and Symons, D. K. (2000). Does the conners’ continuous performance test aid in ADHD diagnosis? J. Abnorm. Child Psychol. 28, 415–424. doi: 10.1023/A:1005127504982
McMullen, J., Kulinna, P., and Cothran, D. (2014). Chapter 5 physical activity opportunities during the school day: classroom teachers’ perceptions of using activity breaks in the classroom. J. Teach. Phys. Educ. 33, 511–527. doi: 10.1123/jtpe.2014-0062
Migueles, J. H., Cadenas-Sanchez, C., Ekelund, U., Delisle Nyström, C., Mora-Gonzalez, J., Löf, M., et al. (2017). Accelerometer data collection and processing criteria to assess physical activity and other outcomes: a systematic review and practical considerations. Sports Med. 47, 1821–1845. doi: 10.1007/s40279-017-0716-0
Mirwald, R. L., Baxter-Jones, A. D. G., Bailey, D. A., and Beunen, G. P. (2002). An assessment of maturity from anthropometric measurements. Med. Sci. Sports Exerc. 34, 689–694
Moore, S. A., Mckay, H. A., Macdonald, H., Nettlefold, L., Baxter-Jones, A. D. G., Cameron, N., et al. (2015). Enhancing a somatic maturity prediction model. Med. Sci. Sports Exerc. 47, 1755–1764. doi: 10.1249/MSS.0000000000000588
Mora-Gonzalez, J., Esteban-Cornejo, I., Cadenas-Sanchez, C., Migueles, J. H., Rodriguez-Ayllon, M., Molina-García, P., et al. (2019). Fitness, physical activity, working memory, and neuroelectric activity in children with overweight/obesity. Scand. J. Med. Sci. Sports 29, 1352–1363. doi: 10.1111/sms.13456
Morales, J. S., Alberquilla Del Río, E., Valenzuela, P. L., and Martínez-de-Quel, Ó. (2024). Physical activity and cognitive performance in early childhood: a systematic review and meta-analysis of randomized controlled trials. Sports Med. 54, 1835–1850. doi: 10.1007/s40279-024-02020-5
Moreau, D., Kirk, I. J., and Waldie, K. E. (2017). High-intensity training enhances executive function in children in a randomized, placebo-controlled trial. Elife 6:e25062. doi: 10.7554/eLife.25062
Muñoz-Sandoval, A. F., Woodcock, R. W., McGrew, K. S., and Mather, N. (2005). Batería III Woodcock-Muñoz: Pruebas de aprovechamiento. Itasca, IL: Riverside Publishing.
Muntaner-Mas, A., Morales, J. S., Martínez-de-Quel, Ó., Lubans, D. R., and García-Hermoso, A. (2024). Acute effect of physical activity on academic outcomes in school-aged youth: a systematic review and multivariate meta-analysis. Scand. J. Med. Sci. Sports 34:e14479. doi: 10.1111/sms.14479
Nejati, V., and Derakhshan, Z. (2021). The effect of physical activity with and without cognitive demand on the improvement of executive functions and behavioral symptoms in children with ADHD. Expert. Rev. Neurother. 21, 607–614. doi: 10.1080/14737175.2021.1912600
Olson, J. A., Nahas, J., Chmoulevitch, D., Cropper, S. J., and Webb, M. E. (2021). Naming unrelated words predicts creativity. Proc. Natl. Acad. Sci. U. S. A. 118:e2022340118. doi: 10.1073/pnas.2022340118
Paschen, L., Lehmann, T., Kehne, M., and Baumeister, J. (2019). Effects of acute physical exercise with low and high cognitive demands on executive functions in children: a systematic review. Pediatr. Exerc. Sci. 31, 267–281. doi: 10.1123/pes.2018-0215
Peiris, D. L. I. H. K., Duan, Y., Vandelanotte, C., Liang, W., Yang, M., and Baker, J. S. (2022). Effects of in-classroom physical activity breaks on children’s academic performance, cognition, health behaviours and health outcomes: a systematic review and meta-analysis of randomised controlled trials. Int. J. Environ. Res. Public Health 19:9479. doi: 10.3390/ijerph19159479
Pontifex, M. B., McGowan, A. L., Chandler, M. C., Gwizdala, K. L., Parks, A. C., Fenn, K., et al. (2019). A primer on investigating the after effects of acute bouts of physical activity on cognition. Psychol. Sport Exerc. 40, 1–22. doi: 10.1016/j.psychsport.2018.08.015
Reis, R. S., Salvo, D., Ogilvie, D., Lambert, E. V., Goenka, S., Brownson, R. C., et al. (2016). Scaling up physical activity interventions worldwide: stepping up to larger and smarter approaches to get people moving. Lancet 388, 1337–1348. doi: 10.1016/S0140-6736(16)30728-0
Rios-Leyvraz, M., Ortega, N., and Chiolero, A. (2022). Reliability of self-reported height and weight in children: a school-based cross-sectional study and a review. Nutrients 15:75. doi: 10.3390/nu15010075
Rodriguez-Martínez, E. I., Muñoz-Pradas, R., Arjona, A., Angulo-Ruiz, B. Y., Muñoz, V., and Gómez, C. M. (2023). Neuropsychological assessment of the relationship of working memory with K-BIT matrices and vocabulary in normal development and ADHD children and adolescents. Brain Sci. 13:1538. doi: 10.3390/brainsci13111538
Ruhland, S., and Lange, K. W. (2021). Effect of classroom-based physical activity interventions on attention and on-task behavior in schoolchildren: a systematic review. Sports Med. Health Sci. 3, 125–133. doi: 10.1016/j.smhs.2021.08.003
Ruiz, J. R., Castro-Pinero, J., Espana-Romero, V., Artero, E. G., Ortega, F. B., Cuenca, M. M., et al. (2011). Field-based fitness assessment in young people: the ALPHA health-related fitness test battery for children and adolescents. Br. J. Sports Med. 45, 518–524. doi: 10.1136/bjsm.2010.075341
Sánchez-López, M., Martínez-Vizcaíno, V., García-Hermoso, A., Jiménez-Pavón, D., and Ortega, F. B. (2015). Construct validity and test-retest reliability of the international fitness scale (IFIS) in Spanish children aged 9-12 years. Scand. J. Med. Sci. Sports 25, 543–551. doi: 10.1111/sms.12267
Sayal, K., Prasad, V., Daley, D., Ford, T., and Coghill, D. (2018). ADHD in children and young people: prevalence, care pathways, and service provision. Lancet Psychiatry 5, 175–186. doi: 10.1016/S2215-0366(17)30167-0
Segura-Díaz, J. M., Barranco-Ruiz, Y., Saucedo-Araujo, R. G., Aranda-Balboa, M. J., Cadenas-Sanchez, C., Migueles, J. H., et al. (2021). Feasibility and reliability of the Spanish version of the youth activity profile questionnaire (YAP-Spain) in children and adolescents. J. Sports Sci. 39, 801–807. doi: 10.1080/02640414.2020.1847488
Sibbick, E., Boat, R., Sarkar, M., Groom, M., and Cooper, S. B. (2022). Acute effects of physical activity on cognitive function in children and adolescents with attention-deficit/hyperactivity disorder: a systematic review and meta-analysis. Ment. Health Phys. Act. 23:100469. doi: 10.1016/j.mhpa.2022.100469
Simons, D. J., Boot, W. R., Charness, N., Gathercole, S. E., Chabris, C. F., Hambrick, D. Z., et al. (2016). Do “brain-training” programs work? Psychol. Sci. Public Interest 17, 103–186. doi: 10.1177/1529100616661983
Singh, A. S., Saliasi, E., van den Berg, V., Uijtdewilligen, L., de Groot, R. H. M., Jolles, J., et al. (2019). Effects of physical activity interventions on cognitive and academic performance in children and adolescents: a novel combination of a systematic review and recommendations from an expert panel. Br. J. Sports Med. 53, 640–647. doi: 10.1136/bjsports-2017-098136
Skulmowski, A. (2024). Learning by doing or doing without learning? The potentials and challenges of activity-based learning. Educ. Psychol. Rev. 36:28. doi: 10.1007/s10648-024-09869-y
Speer, K. E., Semple, S., Naumovski, N., and McKune, A. J. (2020). Measuring heart rate variability using commercially available devices in healthy children: a validity and reliability study. Eur. J. Investig. Health Psychol. Educ. 10, 390–404. doi: 10.3390/ejihpe10010029
Stewart, J. A., Dennison, D. A., Kohl, H. W., and Doyle, J. A. (2004). Exercise level and energy expenditure in the TAKE 10! In-class physical activity program. J. Sch. Health 74, 397–400. doi: 10.1111/j.1746-1561.2004.tb06605.x
Suarez-Manzano, S., Ruiz-Ariza, A., De La Torre-Cruz, M., and Martínez-López, E. J. (2018). Acute and chronic effect of physical activity on cognition and behaviour in young people with ADHD: a systematic review of intervention studies. Res. Dev. Disabil. 77, 12–23. doi: 10.1016/j.ridd.2018.03.015
Tomporowski, P. D., McCullick, B., Pendleton, D. M., and Pesce, C. (2015). Exercise and children’s cognition: the role of exercise characteristics and a place for metacognition. J. Sport Health Sci. 4, 47–55. doi: 10.1016/j.jshs.2014.09.003
Vallejo-Valdivielso, M., Soutullo, C. A., de Castro-Manglano, P., Marín-Méndez, J. J., and Díez-Suárez, A. (2019). Validación de la versión en español de la escala de evaluación del trastorno por déficit de atención e hiperactividad (ADHD-RS-IV.es) en una muestra española. Neurologia 34, 563–572. doi: 10.1016/j.nrl.2017.05.010
Wade, L., Leahy, A., Lubans, D. R., Smith, J. J., and Duncan, M. J. (2020). A systematic review of cognitive assessment in physical activity research involving children and adolescents. J. Sci. Med. Sport 23, 740–745. doi: 10.1016/j.jsams.2019.12.020
Watson, A., Timperio, A., Brown, H., Best, K., and Hesketh, K. D. (2017). Effect of classroom-based physical activity interventions on academic and physical activity outcomes: a systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 14:114. doi: 10.1186/s12966-017-0569-9
Welsch, L., Alliott, O., Kelly, P., Fawkner, S., Booth, J., and Niven, A. (2021). The effect of physical activity interventions on executive functions in children with ADHD: a systematic review and meta-analysis. Ment. Health Phys. Act. 20:100379. doi: 10.1016/j.mhpa.2020.100379
Wiltsey Stirman, S., Kimberly, J., Cook, N., Calloway, A., Castro, F., and Charns, M. (2012). The sustainability of new programs and innovations: a review of the empirical literature and recommendations for future research. Implement. Sci. 7:17. doi: 10.1186/1748-5908-7-17
Wolfenden, L., McCrabb, S., Barnes, C., O’Brien, K. M., Ng, K. W., Nathan, N. K., et al. (2022). Strategies for enhancing the implementation of school-based policies or practices targeting diet, physical activity, obesity, tobacco or alcohol use. Cochrane Database Syst. Rev. 2023. doi: 10.1002/14651858.CD011677.pub3
World Health Organization (2024). Promoting physical activity through schools: a toolkit. Available at: https://www.who.int/publications-detail-redirect/9789240035928
Yoshida, Y., Patil, S. J., Brownson, R. C., Boren, S. A., Kim, M., Dobson, R., et al. (2020). Using the RE-AIM framework to evaluate internal and external validity of mobile phone-based interventions in diabetes self-management education and support. J. Am. Med. Inform. Assoc. 27, 946–956. doi: 10.1093/jamia/ocaa041
Yu, C. L., Hsieh, S. S., Chueh, T. Y., Huang, C. J., Hillman, C. H., and Hung, T. M. (2020). The effects of acute aerobic exercise on inhibitory control and resting state heart rate variability in children with ADHD. Sci. Rep. 10:19958. doi: 10.1038/s41598-020-76859-9
Zhu, F., Zhu, X., Bi, X., Kuang, D., Liu, B., Zhou, J., et al. (2023). Comparative effectiveness of various physical exercise interventions on executive functions and related symptoms in children and adolescents with attention deficit hyperactivity disorder: a systematic review and network meta-analysis. Front. Public Health 11:1133727. doi: 10.3389/fpubh.2023.1133727
Keywords: cross-over, cluster randomized controlled trial, physically active lessons, active classroom, EEG, cognition, academic performance, school
Citation: Arenas D, Bodi-Torralba M, Oliver A, Cantallops J, Ponseti FJ, Palou-Sampol P, Collado JA, Flórez I, Galvez-Pol A, Terrasa JL, Sitges C, Sánchez-Azanza V, López-Penadés R, Adrover-Roig D and Muntaner-Mas A (2024) Effects of active breaks on educational achievement in children with and without ADHD: study protocol and rationale of the Break4Brain project. Front. Psychol. 15:1451731. doi: 10.3389/fpsyg.2024.1451731
Edited by:
Sergio Machado, Federal University of Santa Maria, BrazilReviewed by:
Juan Pablo Zavala-Crichton, Universidad Andres Bello, ChileKaisa Kaseva, University of Helsinki, Finland
Copyright © 2024 Arenas, Bodi-Torralba, Oliver, Cantallops, Ponseti, Palou-Sampol, Collado, Flórez, Galvez-Pol, Terrasa, Sitges, Sánchez-Azanza, López-Penadés, Adrover-Roig and Muntaner-Mas. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Adrià Muntaner-Mas, YWRyaWEubXVudGFuZXJAdWliLmVz