 Cristina Liviana Caldiroli1*
Cristina Liviana Caldiroli1* Rossella Procaccia2
Rossella Procaccia2 Attà Negri3
Attà Negri3 Andrea Mangiatordi1
Andrea Mangiatordi1 Silvia Sarandacchi1
Silvia Sarandacchi1 Alessandro Antonietti4
Alessandro Antonietti4 Marco Castiglioni1
Marco Castiglioni1- 1Department of Human Sciences “Riccardo Massa”, University of Milano-Bicocca, Milan, Italy
- 2Faculty of Psychology, eCampus University, Novedrate, Italy
- 3Department of Human and Social Sciences, University of Bergamo, Bergamo, Italy
- 4Department of Psychology, Catholic University of the Sacred Heart, Milan, Italy
Numerous research studies show that mindfulness can mitigate the negative impact of trauma on mental health by reducing symptoms of anxiety, mediating the relationship between trauma exposure and mental health, and treating symptoms resulting from traumatic events. During the COVID-19 pandemic, which was considered a traumatic event, the wellbeing of adults and children was severely compromised. Although children seem less vulnerable to the physical effects of the virus, this does not seem to be true for the psychological effects. Indeed, a prolonged period of loss of family activities and routines can have a negative impact on the mental health of children and adolescents. To investigate how mindfulness can help preschool children cope with the effects of COVID-19, a study was conducted on 46 children aged 4–5 years. The programme, based on the work of Jon Kabat-Zinn and adapted to the age of the participants, consisted of eight weekly 45-min sessions. Qualitative and quantitative results showed positive feedback, indicating that mindfulness helps children make sense of their experiences and achieve functional post-traumatic growth. This approach is seen as a challenge to guide children toward the restoration of psychological wellbeing, which is essential for good psychological balance.
1 Introduction
Mindfulness, in its original etymology, refers to a state of mental presence in which one sees internal phenomena as they really are and discriminates between external phenomena and one's own mental projections and distortions (Rinpoche, 1998; Uchiyama, 2004). According to the original tradition, mainly based on Buddhist meditation teachings, mindfulness practice should allow one to move from a state of disequilibrium and suffering to one of greater subjective wellbeing, thanks to a deep knowledge of one's mental states and processes (Shapiro et al., 2006). Since the 1960s, there has also been an interest in meditative practices within clinical psychology, where there has been recognition of the potential for the development of awareness in patients, with important implications for their wellbeing (Keng et al., 2011). The contribution of the Zen Buddhist monk Hanh (1976) and the development of his teachings in the context of clinical and experimental psychology by Kabat-Zinn (1990) were crucial to the cultural integration between Buddhist meditative practice and the new Western forms of mindfulness.
Mindfulness is characterized by two closely related components: the ability to bring attention to the present moment (intentionality, attentional self-regulation) and the attitude of doing so, consisting of curiosity, opennes, and acceptance (Bishop et al., 2004). These components allow the person to relate to his or her experiences in a mindful way, with the attitude of being present to them, but in a non-critical and non-anxious way. This metacognitive awareness corresponds to a decentralized and disarmed way of relating to our thoughts, emotions, and sensations in the present, where the person experiences mental states as mental states rather than as objective reality (“thought is not fact, nor am I”). In this way, mindfulness is seen as a specific way of experiencing the inner and outer world with conscious attention. Without judging them or identifying with their mental content, we accept them moment by moment as they are.
The Mindfulness Based Stress Reduction (MBSR) programme was formulated by Kabat-Zinn in the 1970s. This was the first structured mindfulness-based intervention presented to the scientific community as an effective treatment for pain (Kabat-Zinn, 1982). Since then, there has been a proliferation of research on mindfulness practices and their effects in different populations and settings. This has led to the emergence of many mindfulness-oriented clinical practices, such as Dialectical Behavioral Therapy (Linehan, 1993), Acceptance and Commitment Therapy (Hayes et al., 1999), and Mindfulness-Based Cognitive Therapy (Segal et al., 2002). The efficacy of mindfulness as a therapeutic approach for adults has been demonstrated in numerous clinical conditions, both organic (chronic pain, rheumatoid arthritis, fibromyalgia) and psychological (reducing stress in cancer patients, anxiety, mood disorders, substance abuse) (e.g., Segal et al., 2002; Mace, 2008). More recently, there was the need to implement interventions that help the younger population to restore their psychophysical balance and their individual and social wellbeing (Behan, 2020; Courtney et al., 2020; Xie et al., 2020; Andreu et al., 2023), building on the existing literature on effective interventions with children and adolescents in the case of traumatic and stressful events and replicating them in the current context (Rempel, 2012; Follette et al., 2006; Romeo, 2017; Caldiroli et al., 2020; Kachadourian et al., 2021; Castiglioni et al., 2022; Garcia-Rubio et al., 2023). In particular, there has been a growing interest in the theoretical research and clinical applications of mindfulness in childhood (Greenberg and Harris, 2011; Fabbro and Muratori, 2012; Caldiroli et al., 2020) and, in particularly in school context, working as a preventive method to stress, anxiety, negative emotions, lack of attention or self-regulation (Bockmann and Yu, 2023).
Since mindfulness-based interventions can be useful in coping with stressful situations by promoting self-directed attention, teaching acceptance of negative thoughts and feelings, and promoting non-judgement (Kabat-Zinn, 1994; Goodman and Schorling, 2012; Weis et al., 2021) the present pilot study aims to investigate the protective and preventive value of mindfulness by focusing on one of the most recent events that has had a strong impact on the mental and physical wellbeing of the entire population: the COVID-19 pandemic. The pandemic outbreak in Wuhan in December 2019 had a significant impact on the entire population, drastically altering daily routines and severely affecting individuals' physical and mental health (e.g., Brooks et al., 2020; Fiorillo and Gorwood, 2020; Rudnik et al., 2021; Miyah et al., 2022; Castiglioni et al., 2023; Negri et al., 2023). As with the adult population, children and adolescents also experienced and faced an unprecedented event, with profound alterations in their lifestyles that interfered with their social development in a way that could have long-term ramifications. Faced with this situation and an uncertain future, new worries and anxieties were identified in children. There was a worsening of depressive symptoms, an increase in behavioral problems and social withdrawal, a decrease in self-esteem, and an increase in anxiety and stress (Pfefferbaum and North, 2020; Gonda and Tarazi, 2022).
Mindfulness-based protocols have been found to be effective in the promotion of wellbeing and adjustment in school populations (Beauchemin et al., 2008; Saltzman and Goldin, 2008; Duff, 2024) and in individuals with mental disorders (Biegel et al., 2009; McKeen et al., 2023). In particular, studies have shown that mindfulness-based therapeutic interventions show positive results in the treatment of children and adolescents with oppositional defiant disorder, conduct disorder, attention deficit hyperactivity disorder (ADHD), anxiety, depression, obsessive-compulsive disorder, chronic pain, and substance abuse (Burke, 2010; Zenner et al., 2014; Kallapiran et al., 2015; Swain et al., 2015; Tan, 2016; Zoogman et al., 2015; Black and Slavich, 2016; Cairncross and Miller, 2020; Felver et al., 2016; Evans et al., 2018; Carsley et al., 2018; Caldiroli et al., 2020, 2021). With mindfulness, children and young people increase awareness (react less automatically) and learn to be “consciously present” in the breath, body (tastes, smells, images, sounds), thoughts, emotions, needs, actions, others, and environment (Baer et al., 2006; Chiesa et al., 2013). Mindfulness in developmental age is considered a promising therapeutic practice (Fabbro and Muratori, 2012).
In the current research it was decided to use a mindfulness protocol adapted by Montano and Villani (2018) from the MBSR programme with kindergarten children. The main focus of the present study is to investigate the possible impact of mindfulness on cognitive, emotional, expressive, behavioral and awareness aspects of the individual and, in particular, on attention, memory, creativity, emotional intelligence, interpersonal relationships, awareness, and behavioral control. The aim is to assess the possible benefits and improvements that the training can have on stress management and regulation of thoughts and feelings, especially in a period such as the last few years.
2 Materials and methods
2.1 Participants
A total of 46 children aged between 4 and 5 years participated in the study. The sample consisted of 22 children (10 boys, 12 girls) in the experimental group and 24 children (11 boys, 13 girls) in the control group. The children were divided into the two groups according to the school they attended. It should be noted that at a later stage, at the end of the experimental phase, mindfulness training was also given to the control group. Parents and teachers collaborated in the research to complete the questionnaires and tests.
2.2 Procedure and measures
Several schools in northern Italy were asked to participate in the study by an invitation letter. The first three schools to reply to the invitation were selected for the present pilot study. A quasi-experimental research design with non-equivalent groups and only post-tests was set up. In this research design, the participants are not randomly assigned to the experimental and control groups; consequently, from a methodological point of view, the researcher only compares situations that have already been predetermined in the natural context (Fiorillo and Gorwood, 2020; Cook et al., 1990; Gopalan et al., 2020; Trinchero, 2004).
The pilot study took place from January to December 2022 in three kindergartens on a voluntary basis. During this period, meetings were organized with the school and parents to present the programme and explain its objectives, training sessions with the children took place, and, at the end of the programme, a feedback meeting involved teachers and parents.
Several instruments were used to evaluate the effects of mindfulness training on children, in particular: parents were somministred with two pre-training questionnaires and one post-training questionnaire to assess the effects of COVID-19 on children's lives and the impact of mindfulness training. In addition, a pre-post training questionnaire was administered to assess the children's skills. In the pre-training phase, the questionnaire was completed by the teacher before starting the mindfulness programme. In the post-training phase, the questionnaire was completed by the teacher at the end of the mindfulness programme.
The sessions with the children took place in a noise-free room and with minimal distractions. The 4- and 5-year-old children were divided into two groups on the same day, maintaining the same protocol, room, and experimenter for both groups. Each session began with the placement of mats on the floor, providing the children with a sense of personal space and a secure base. The control group completed the questionnaires at the same time as the experimental group, but without participating in the training. Subsequently, the control group was also administered the mindfulness protocol. To evaluate the effects of the mindfulness training on the children, various instruments were used, including specific questionnaires to investigate any psychological problems and discomforts that had arisen due to the COVID-19 pandemic and to assess benefits and improvements resulting from the mindfulness programme.
2.2.1 Modified and adapted mindfulness programme
Based on the general protocol of Montano and Villani (2018), a simplified protocol was developed, suitable for 4- and 5-year-old children. The features that remained unchanged from the original protocol are: 8 sessions; from 45 to 60 min of duration per session; the weekly schedule; the themes and the order of the sessions. The first session is an introduction to mindfulness and personal “secret garden”; the second is based on the concept of the beginner's mind; the third focuses on thinking and the “wandering mind”; the fourth is based on emotions and emotional intelligence; the fifth concentrates on dealing with stressful events and non-judgment; the sixth is about awareness before action; the seventh session introduces awareness of self and others as a support for difficult communication; and finally the eighth session consolidates attitudes of kindness toward oneself and concludes the programme.
However, to adapt to the needs of younger children, some aspects had to be modified: the number of exercises per session was reduced: one for initial meditation, one in the middle, and one at the end; the time for reviewing the tasks was retained, but an attempt was made to limit the time to a maximum of 15 min (with discussion led by the experimenter); only one psycho-educational moment was established, characterized by one of the proposed activities, which was analyzed in depth with the experimenter; only one reading moment was maintained, with the selection of the passages indicated for the younger children, which were carefully analyzed and contextualized during the group discussion (also guided by the experimenter). It turned out that the children were able to follow and remained attentive and interested throughout the sessions, thanks to the way they were set up. The sessions were structured into three phases as described in Table 1.
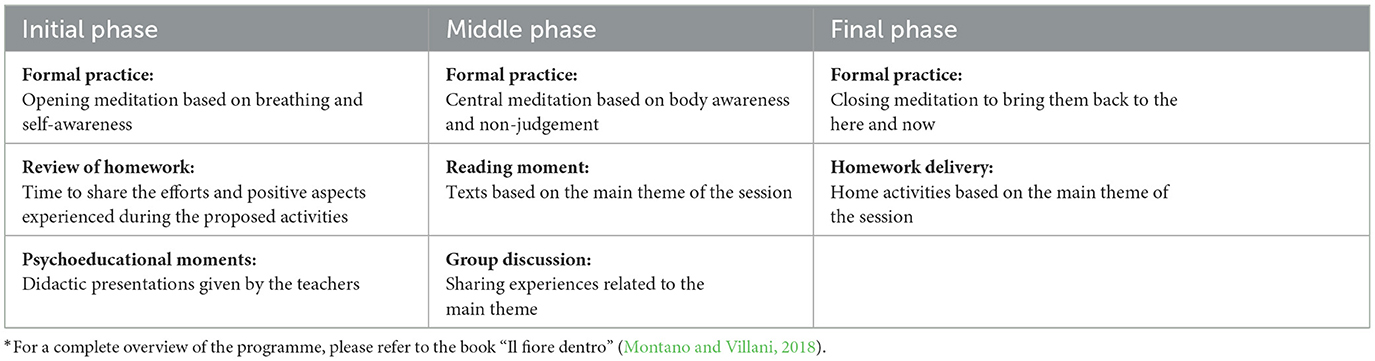
Table 1. General structure of meetings.
2.2.2 Pre-training questionnaire - COVID-19 effects
Parents were asked to respond regarding their child over the past 12 months. The questionnaire consists of a first part of open-ended questions and a second part where they are asked to give their opinion on a scale of 1 (not at all) to 5 (very much). The open questions collected personal data (e.g., age; family composition; who the child lives with; etc.) and data about the period of the pandemic (e.g., whether the child had COVID-19; whether any family members or acquaintances had it; whether the child's school was closed because of COVID-19 and, if so, how often it was closed; whether the child engages in recreational and/or sports activities after school and how they were managed during the pandemic; etc.). The closed questions were more concerned with children's feelings and needs (e.g., did the child feel sorry for the school closure; did the child show more attachment to caregivers since the pandemic; did the child show more irritability/angry since the pandemic; did the child feel more need to do outdoor activities since the pandemic; etc.).
2.2.3 Pre/post parent questionnaire—Mindfulness
Ad hoc questionnaire to assess mindfulness programme impact. In particular, it looks at how the child relates to, manages, recognizes, and expresses emotions, thoughts and feelings about themselves and others before and after the training. The questionnaire was given to the parents. They were asked to rate their child on a scale from 1 (not at all) to 5 (very much). For example, it was asked whether the child shows irritability, whether he is a restless sleeper, whether he is an attentive child, whether he is a creative child, whether he is curious, whether he is able to regulate his emotional reactions (such as fear, joy, sadness), whether he knows how to recognize mistakes, whether he listens to instructions before starting a task, etc.
2.2.4 Questionnaire for the assessment of skills in children—SAI (pre/post training)
This is a tool proposed by A. Antonietti, R. Finazzi and M. Geroldi of the Service of Psychology of Learning and Education in the Age of Development (SPAEE) of the Catholic University of the Sacred Heart. It is designed to assess the abilities (skills) of children around the age of 5. The instrument evaluates a wide range of skills, each with a similar section: attention, memory, spatial cognition, reasoning, creativity, language, feelings, interpersonal relations, motor skills, awareness, planning, and behavioral control. The questionnaire is made up of 24 items, each with 4 possible answers, and the teacher must choose the one that best fits the child. Each skill is presented in relation to a specific situation, so that the respondent can think of a concrete case in which the skill is manifested. In the pre-training phase, the questionnaire was completed by the teacher before starting the mindfulness programme. In the post-training phase, the questionnaire was completed by the teacher at the end of the mindfulness programme. It is noted that for each questionnaire, for each question, the possibility of not answering was given, e.g., by crossing out the space to answer, by choosing “I prefer not to answer” or “I don't know”.
3 Results
The data were analyzed using IBM SPSS Statistics 25 software for parametric tests, selected according to the reference sample and variables. Specifically, chi-squared test, t-test and general linear model were used.
3.1 Descriptive statistics and t-test of the pre-training questionnaire—COVID-19 effects
3.1.1 Descriptive statistics
Some descriptive analyses were carried out to test whether there were significant differences between the experimental and control groups in the initial stage of the research. The results showed that there were no differences between the experimental group and the control group in the initial phase, except for the children's reactions to distance learning. Regarding distance learning, the significant difference (t = 20.255; df = 11; p = 0.042) between the experimental and control groups is due to the fact that the children in the experimental group showed either positive (happiness, calmness, curiosity, etc.) or negative (sadness, anger, fear, tiredness, etc.) emotions toward it, while those in the control group also reported other emotions (e.g., need for attention, boredom, hesitation, etc.). At the time of the data collection, the distance learning was no longer available for the kindergarteners, and the data collected covered a period prior to the mindfulness training. Therefore, considering the other findings, it was not considered worthwhile to investigate beyond this single result. In fact, no significant differences emerged for the other variables: children's gender, family composition during the COVID-19 period, children's direct contact with positive people, any quarantines, school closures, and new fears manifested.
3.1.2 T-test analysis
The results show a better perception of the experimental group, which, despite being penalized by the repeated school closures, showed greater satisfaction with both school attendance and distance learning. They also perceived school as a safe place both before and during the pandemic period. In comparison, the control group showed a more negative reaction in terms of greater irritability, greater attachment to parents, nervousness, fear of relationships, and worry (Table 2). However, there were no significant differences between these two groups in variables related to resentment of school closing, return to school, interest in school activities, perceiving home as safe, adherence to sleep schedules, loss of appetite, questions about epidemic situation, loss of concentration, and activities during lockdown.
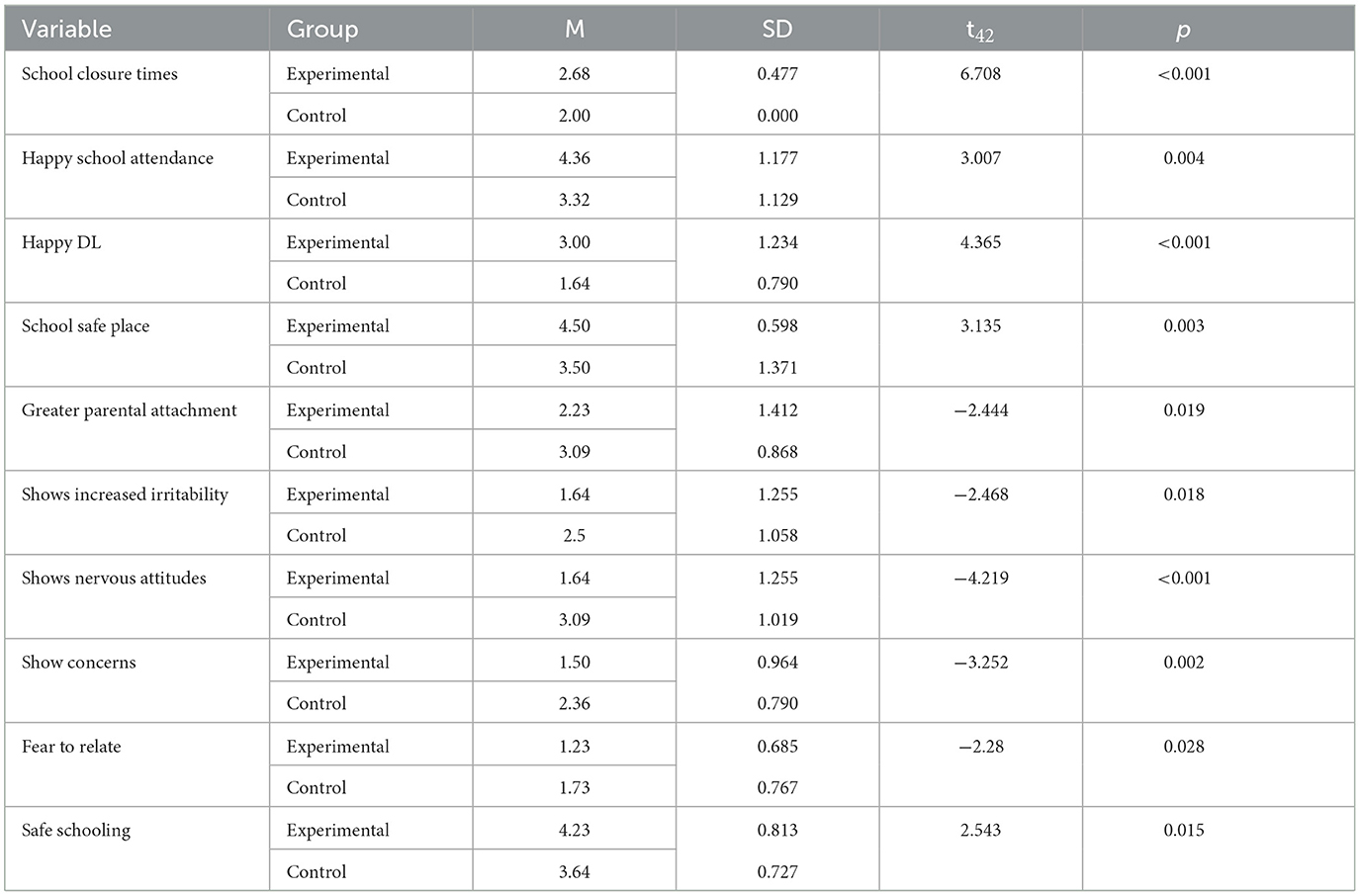
Table 2. Significant COVID effects in the pre-training questionnaire.
3.2 General linear model pre/post parent questionnaire—Mindfulness
To analyze the pre- and post-training questionnaires—mindfulness, a general linear model was used by means of a factor analysis between the experimental and control groups for each variable. The variables that were found to be significant are curiosity, empathy, control of emotional reaction to surprise, emotional reaction control when he/she is the center of attention, positive resolution of conflict, emotion recognition, determination, and listening to instructions (Table 3). All these variables increased significantly in the experimental group and decreased in the control group. The only exceptions were irritability and nervousness. Unlike the other variables, these tended to decrease in the experimental group and increase in the control group.

Table 3. Significant effects between the pre/post questionnaires—mindfulness.
The variables that were not found to be significant were: worry and negative thoughts, irregular appetite, restless sleep, overreaction to anxiety, ability to pay attention, creativity and imagination, emotional response to anger, sadness, happiness, guilt, positive involvement in relationships, and recognition of mistakes.
3.3 General linear model pre/post SAI questionnaire
As will be described, the items were divided into three areas: cognitive, expressive, and behavioral/awareness. The general linear model was used. It was found that there was a significant increase in score in the experimental group in the cognitive area, which includes factors relating to attention, memory, spatial cognition, and reasoning; in the expressive area, which includes factors relating to creativity, language, emotions, and interpersonal relationships; and in the behavior/awareness area, which includes factors related to motor skills, awareness, planning, and control of behavior. In all these areas scores of the control group remained unchanged (Table 4).
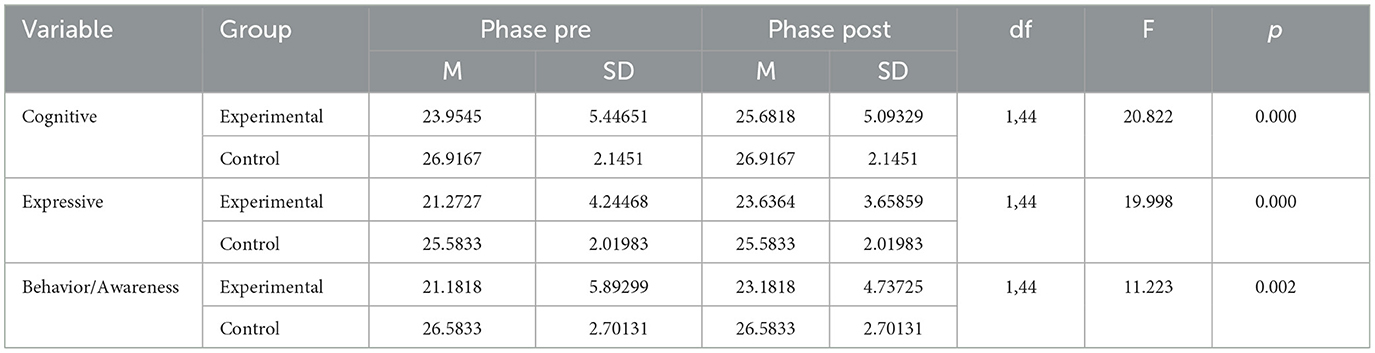
Table 4. Significant variables Pre/Post SAI questionnaire.
4 Discussion
When the emotional impact of COVID-19 on the children was examined, significant differences were found between the experimental group, who took part in the mindfulness programme, and the control group. In fact, the levels of irritability and nervousness decreased significantly in the experimental group, confirming that a mindfulness-based programme can be a protective factor in cases of acute stress, allowing a reduction in stress disorders (Montano and Villani, 2018; Querstret et al., 2020), anxiety (Evans et al., 2008; Lee and Semple, 2019) and depression (Segal et al., 2002), helping them to stay with their fears and uncertainties.
Protective factors and individual resources increased: curiosity and empathy, particularly in the management and recognition of both negative and positive emotions. This again confirms the potential of mindfulness (Guendelman et al., 2017; Weis et al., 2021). Although not statistically significant, the comparison between the pre- and post- training questionnaires showed positive and encouraging results in the experimental group for some variables, confirming the findings of several studies (Kabat-Zinn, 1994; Montano and Villani, 2018; Behan, 2020). In particular, worry decreased in the experimental group while it remained unchanged in the control group, as levels of creativity, imagination, and appetite did. The control of emotional states such as worry, guilt, and fear reactions also tended to improve in the experimental group. This contrasted with the control group, where levels of these variables tended to decrease. Furthermore, a trend toward significance was found for the variable “restless sleep” (F = 3.709; df = 1,37; p = 0.062). From this it can be concluded that sleep quality improved in the experimental group compared to the control group, confirming the claim that mindfulness training adapted to children can improve sleep quality (Huppert and Johnson, 2010). Finally, the analysis of the SAI questionnaires showed a general improvement in cognitive, expressive, and behavioral/awareness areas after the mindfulness training, confirming that participation in the programme is beneficial for factors such as attention and reasoning (Caldiroli et al., 2020; Milaré et al., 2021), creativity (Capurso et al., 2014; Henriksen et al., 2020), awareness (Weis et al., 2021), and behavioral control (Clark, 2020). We can therefore argue that by improving the dimension of awareness the participants in this pilot study were able to develop and enhance their ability to make sense of experiences and to re-read them from a different perspective, in this case in a functional and constructive way (Castiglioni and Faccio, 2010; Castiglioni and Gaj, 2020).
Mindfulness can bring great benefits to people's mental and physical health, even from a preventive perspective. Adapting mindfulness programmes for children and adolescents and promoting them in schools can help prevent the consequences of unexpected stressful events like it was the pandemic. As a matter of fact, ignoring psycho-physical wellbeing can leave people in a precarious state and even worsen their state of health, especially at critical moments that can lead to new worries and uncertainties, and thus psychological consequences such as frustration, lack of meaning, loneliness, stress, anxiety, depression, and psychosis (Shigemura et al., 2020; Castiglioni and Gaj, 2020; Venuleo et al., 2022; Gennaro et al., 2023). In fact, caring for yourself and cultivating positive emotions can help cope with uncomfortable situations and improve health.
Furthermore, from the perspective of positive psychology, mindfulness has worked on the two aspects of hedonic (Kahneman et al., 1999) and eudaimonic (Zambianchi, 2015) wellbeing by improving wellbeing and capacities at both personal and collective levels (Neff and Dahm, 2015).
5 Conclusion
After the programme, it was noted that the mindfulness protocol “Il fiore dentro” (Montano and Villani, 2018), applied to the children in the experimental group, confirmed our hypotheses, favoring an improvement in the cognitive, expressive, and behavioral/awareness areas, reducing the levels of irritability and nervousness that an emergency situation can provoke, and improving the recognition of emotions and empathy. The control group, on the other hand, experienced a decrease in these aspects.
However, it should be borne in mind that this was a pilot study with limitations. Firstly, the size of the sample allowed us to carry out preliminary analyses, which were nevertheless promising. Secondly, the data collection was ad hoc and not by means of standardized questionnaires. This was intentional, as this first phase is part of a larger project and in this first step we wanted to look at the questions in the tests to see if mindfulness training structured in this way could have an effect. The next step will be to expand the sample, use standardized tests, and validate the tests already used at this phase.
In conclusion, teaching mindfulness means improving the quality of life, enhancing psycho-physical wellbeing and increasing resilience. The school is the context par excellence that must prepare individuals for life and promote health: incorporating mindfulness into this and other educational contexts would allow one to look to the future with values such as awareness and confidence.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The study was approved by Ethics Committee of Catholic University of the Sacred Heart, Milan, Italy (CERPS). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
Author contributions
CC: Resources, Writing – review & editing, Writing – original draft, Visualization, Validation, Supervision, Software, Project administration, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. RP: Writing – review & editing, Visualization, Validation, Software, Formal analysis. AN: Writing – review & editing, Visualization, Validation, Software, Formal analysis. AM: Writing – review & editing, Visualization, Validation, Software, Investigation. SS: Writing – review & editing, Visualization, Resources. AA: Writing – review & editing, Visualization, Validation, Supervision, Software, Resources, Methodology, Formal analysis, Data curation. MC: Writing – review & editing, Visualization, Validation, Supervision, Resources, Formal analysis.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer FI declared a shared affiliation, with no collaboration, with the author AA to the handling editor at the time of the review.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Andreu, C. I., García-Rubio, C., Melcón, M., Schonert-Reichl, K. A., and Albert, J. (2023). The effectiveness of a school mindfulness-based intervention on the neural correlates of inhibitory control in children at risk: a randomized control trial. Dev. Sci. 26:e13403. doi: 10.1111/desc.13403
Baer, R. A., Smith, G. T., Hopkins, J., Krietemeyer, J., and Toney, L. (2006). Using self-report assessment methods to explore facets of mindfulness. Assessment 13, 27–45. doi: 10.1177/1073191105283504
Beauchemin, J., Hutchins, T. L., and Patterson, F. (2008). Mindfulness meditation may lessen anxiety, promote social skills, and improve academic performance among adolescents with learning disabilities. Complement. Health Pract. Rev. 13, 34–45. doi: 10.1177/1533210107311624
Behan, C. (2020). The benefits of meditation and mindfulness practices during times of crisis such as COVID-19. Ir. J. Psychol. Med. 37, 256–258. doi: 10.1017/ipm.2020.38
Biegel, G. M., Brown, K. W., Shapiro, S. L., and Schubert, C. M. (2009). Mindfulness-based stress reduction for the treatment of adolescent psychiatric outpatients: a randomized clinical trial. J. Consult. Clin. Psychol. 77, 855–866. doi: 10.1037/a0016241
Bishop, S. R., Lau, M., Shapiro, S., Carlson, L., Anderson, N. D., Carmody, J., et al. (2004). Mindfulness: a proposed operational definition. Clin. Psychol.: Sci. Pract. 11, 230–241. doi: 10.1093/clipsy.bph077
Black, D. S., and Slavich, G. M. (2016). Mindfulness meditation and the immune system: a systematic review of randomized controlled trials. Ann. N. Y. Acad. Sci. 1373, 13–24. doi: 10.1111/nyas.12998
Bockmann, J. O., and Yu, S. Y. (2023). Using mindfulness-based interventions to support self-regulation in young children: A review of the literature. Early Childhood Educ. J. 51, 693–703. doi: 10.1007/s10643-022-01333-2
Brooks, S. K., Webster, R. K., Smith, L. E., Woodland, L., Wessely, S., Greenberg, N., et al. (2020). The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet 395, 912–920. doi: 10.1016/S0140-6736(20)30460-8
Burke, C. A. (2010). Mindfulness-based approaches with children and adolescents: a preliminary review of current research in an emergent field. J. Child Fam. Stud. 19, 133–144. doi: 10.1007/s10826-009-9282-x
Cairncross, M., and Miller, C. J. (2020). The effectiveness of mindfulness-based therapies for ADHD: a meta-analytic review. J. Atten. Disord. 24, 627–643. doi: 10.1177/1087054715625301
Caldiroli, C., Mangiatordi, A., Fornaro, E., Mantovani, F., Castiglioni, M., and Antonietti, A. (2021). Application of a clinical training based on mindfulness in children with attention deficit hyperactivity disorder (ADHD). Medit. J. Clini. Psychol. 9, 38–39. doi: 10.13129/2282-1619/mjcp-3224
Caldiroli, L. C., Malizia, G., Pignarolo, M., Fornaro, E., Mangiatordi, A., Mantovani, F., et al. (2020). Applicazione del training mindfulness in bambini con ADHD. DIS 1, 25–55. doi: 10.14605/DIS0112002
Campbell, D. T. (1957). Factors relevant to the validity of experiments in social settings. Psychol. Bullet. 54, 297–312. doi: 10.1037/h0040950
Capurso, V., Fabbro, F., and Crescentini, C. (2014). Mindful creativity: the influence of mindfulness meditation on creative thinking. Front. Psychol. 4:1020. doi: 10.3389/fpsyg.2013.01020
Carsley, D., Khoury, B., and Heath, N. L. (2018). Effectiveness of mindfulness interventions for mental health in schools: a comprehensive meta-analysis. Mindfulness 9, 693–707. doi: 10.1007/s12671-017-0839-2
Castiglioni, M., Caldiroli, C. L., and Antonietti, A. (2022). Play-based activities with a coderbot robot on a pediatric ward: a case study. Healthcare 10:1209. doi: 10.3390/healthcare10071209
Castiglioni, M., Caldiroli, C. L., Negri, A., Manzoni, G. M., and Procaccia, R. (2023). Linguistic predictors of psychological adjustment in healthcare workers during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 20:4482. doi: 10.3390/ijerph20054482
Castiglioni, M., and Faccio, E. (2010). “Costruttivismi in psicologia clinica,” in Teorie, metodi, ricerche. Torino: Utet Università.
Castiglioni, M., and Gaj, N. (2020). Fostering the reconstruction of meaning among the general population during the COVID-19 pandemic. Front. Psychol. 11:567419. doi: 10.3389/fpsyg.2020.567419
Chiesa, A., Serretti, A., and Jakobsen, J. C. (2013). Mindfulness: top-down or bottom-up emotion regulation strategy? Clin. Psychol. Rev. 33, 82–96. doi: 10.1016/j.cpr.2012.10.006
Clark, L. B. (2020). Utilizing mindfulness based CBT to address anger and aggression in middle schools. J. Child Adolesc. Counsel. 6, 97–109. doi: 10.1080/23727810.2020.1719351
Cook, T. D., Campbell, D. T., and Peracchio, L. (1990). “Quasi-experimentation,” in Handbook of Industrial and Organizational Psychology, eds. M. D. Dunnette and L. M. Hough (Palo Alto, CA: Consulting Psychologists Press) 491–576.
Courtney, D., Watson, P., Battaglia, M., Mulsant, B. H., and Szatmari, P. (2020). COVID-19 impacts on child and youth anxiety and depression: challenges and opportunities. Can. J. Psychiatry 65, 688–691. doi: 10.1177/0706743720935646
Duff, C. (2024). The implementation of mindfulness in early childhood: diversity in the uses and functions of mindfulness and what this may mean for children's well-being. Mind, Brain, Educ. 18, 187–199. doi: 10.1111/mbe.12399
Evans, S., Ferrando, S., Findler, M., Stowell, C., Smart, C., and Haglin, D. (2008). Mindfulness-based cognitive therapy for generalized anxiety disorder. J. Anxiety Disord. 22, 716–721. doi: 10.1016/j.janxdis.2007.07.005
Evans, S., Ling, M., Hill, B., Rinehart, N., Austin, D., and Sciberras, E. (2018). Systematic review of meditation-based interventions for children with ADHD. Eur. Child Adolesc. Psychiatry 27, 9–27. doi: 10.1007/s00787-017-1008-9
Fabbro, F., and Muratori, F. (2012). La mindfulness: un nuovo approccio psicoterapeutico in età evolutiva [Mindfulness: a new psychotherapeutic approach for children]. Giornale Italiano di Neuropsichichiatria dell'Età Evolutiva. Ital. J. Dev. Neuropsichichiatry 32, 248–259.
Felver, J. C., Celis-de Hoyos, C. E., Tezanos, K., and Singh, N. N. (2016). A systematic review of mindfulness-based interventions for youth in school settings. Mindfulness 7, 34–45. doi: 10.1007/s12671-015-0389-4
Fiorillo, A., and Gorwood, P. (2020). The consequences of the COVID-19 pandemic on mental health and implications for clinical practice. Eur. Psychiatr. 63:e32. doi: 10.1192/j.eurpsy.2020.35
Follette, V., Palm, K. M., and Pearson, A. N. (2006). Mindfulness and trauma: Implications for treatment. J. Ration.-Emot. Cognit.-Behav. Thera. 24, 45–61. doi: 10.1007/s10942-006-0025-2
Garcia-Rubio, C., Herrero, M., Luna-Jarillo, T., Albert, J., and Rodríguez-Carvajal, R. (2023). Effectiveness and mechanisms of change of a mindfulness-based intervention on elementary school children: a cluster-randomized control trial. J. Sch. Psychol. 99:101211. doi: 10.1016/j.jsp.2023.04.001
Gennaro, A., Reho, M., Marinaci, T., Cordella, B., Castiglioni, M., Caldiroli, C. L., et al. (2023). Social environment and attitudes toward COVID-19 anti-contagious measures: an explorative study from Italy. Int. J. Environ. Res. Public Health 20:3621. doi: 10.3390/ijerph20043621
Gonda, X., and Tarazi, F. I. (2022). Wellbeing, resilience and post-traumatic growth in the era of COVID-19 pandemic. Eur. Neuropsychopharmacol. 54, 65–66. doi: 10.1016/j.euroneuro.2021.08.266
Goodman, M. J., and Schorling, J. B. (2012). A mindfulness course decreases burnout and improves wellbeing among healthcare providers. Int. J. Psychiat. Med. 43, 119–128. doi: 10.2190/PM.43.2.b
Gopalan, M., Rosinger, K., and Ahn, J. B. (2020). Use of quasi-experimental research designs in education research: Growth, promise, and challenges. Rev. Res. Educ. 44, 218–243. doi: 10.3102/0091732X20903302
Greenberg, M. T., and Harris, A. R. (2011). Nurturing mindfulness in children and youth: Current state of research. Child Dev. Perspect. 6, 161–166. doi: 10.1111/j.1750-8606.2011.00215.x
Guendelman, S., Medeiros, S., and Rampes, H. (2017). Mindfulness and emotion regulation: insights from neurobiological, psychological, and clinical studies. Front. Psychol. 8:220. doi: 10.3389/fpsyg.2017.00220
Hanh, T. N. (1976). The miracle of being awake: A manual on meditation for the use of young activists. The Wheel Publication Nos. 234/235/236. Buddhist Publication Society. Kandy, Sri Lanka.
Hayes, S. C., Strosahl, K. D., and Wilson, K. G. (1999). Acceptance and Commitment Therapy. New York, NY: The Guilford Press.
Henriksen, D., Richardson, C., and Shack, K. (2020). Mindfulness and creativity: Implications for thinking and learning. Think. Skills Creativ. 37:100689. doi: 10.1016/j.tsc.2020.100689
Huppert, F. A., and Johnson, D. M. (2010). A controlled trial of mindfulness training in schools: the importance of practice for an impact on wellbeing. J. Posit. Psychol. 5, 264–274. doi: 10.1080/17439761003794148
Kabat-Zinn, J. (1982). An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: theoretical considerations and preliminary results. Gen. Hosp. Psychiatry 4, 33–47. doi: 10.1016/0163-8343(82)90026-3
Kabat-Zinn, J. (1990). Mindfulness-based stress reduction. Using the wisdom of your body and mind to face stress, pain, and illness. p. 467.
Kabat-Zinn, J. (1994). “Dovunque tu vada ci sei già,” in Cammino Verso la Consapevolezza. Milano: Corbaccio.
Kachadourian, L. K., Harpaz-Rotem, I., Tsai, J., Southwick, S., and Pietrzak, R. H. (2021). Mindfulness as a mediator between trauma exposure and mental health outcomes: results from the National Health and Resilience in Veterans Study. Psychol. Trauma: Theory, Res. Prac. Policy 13, 223–230. doi: 10.1037/tra0000995
Kahneman, D., Diener, E., and Schwarz, N. (1999). Wellbeing: Foundations of Hedonic Psychology. New York: Russell Sage Foundation.
Kallapiran, K., Koo, S., Kirubakaran, R., and Hancock, K. (2015). Review: effectiveness of mindfulness in improving mental health symptoms of children and adolescents: a meta-analysis. Child Adolesc. Ment. Health 20, 182–194. doi: 10.1111/camh.12113
Keng, S. L., Smoski, M. J., and Robins, C. J. (2011). Effects of mindfulness on psychological health: a review of empirical studies. Clin. Psychol. Rev. 31, 1041–1056. doi: 10.1016/j.cpr.2011.04.006
Lee, J., and Semple, R. J. (2019). “Mindfulness-based cognitive therapy for children,” in Handbook of Mindfulness-Based Programmes (Abingdon, Oxfordshire: Routledge).
Linehan, M. M. (1993). Skills Training Manual for Treating Borderline Personality Disorder. New York, NY: The Guilford Press.
McKeen, H., Hook, M., Podduturi, P., Beitzell, E., Jones, A., and Liss, M. (2023). Mindfulness as a mediator and moderator in the relationship between adverse childhood experiences and depression. Curr. Psychol. 42, 6576–6586. doi: 10.1007/s12144-021-02003-z
Milaré, C. A. R., Kozasa, E. H., Lacerda, S., Barrichello, C., Tobo, P. R., and Horta, A. L. D. (2021). Mindfulness-based versus story reading intervention in public elementary schools: effects on executive functions and emotional health. Front. Psychol. 12:576311. doi: 10.3389/fpsyg.2021.576311
Miyah, Y., Benjelloun, M., Lairini, S., and Lahrichi, A. (2022). COVID-19 impact on public health, environment, human psychology, global socioeconomy, and education. Scient.World J. 2022, 5578284. doi: 10.1155/2022/5578284
Montano, A., and Villani, S. (2018). “Programma mindfulness “il fiore dentro,”” in Per insegnare ai bambini a gestire lo stress ed essere più felici. Trento: Erickson.
Neff, K. D., and Dahm, K. A. (2015). “Self-compassion: What it is, what it does, and how it relates to mindfulness,” in Handbook of Mindfulness and Self-Regulation (New York: Springer).
Negri, A., Conte, F., Caldiroli, C. L., Neimeyer, R. A., and Castiglioni, M. (2023). Psychological factors explaining the COVID-19 pandemic impact on mental health: the role of meaning, beliefs, and perceptions of vulnerability and mortality. Behav. Sci. 13:162. doi: 10.3390/bs13020162
Pfefferbaum, B., and North, C. S. (2020). Mental health and the COVID-19 PANDEMIC. N. Engl. J. Med. 383, 510–512. doi: 10.1056/NEJMp2008017
Querstret, D., Morison, L., Dickinson, S., Cropley, M., and John, M. (2020). Mindfulness-based stress reduction and mindfulness-based cognitive therapy for psychological health and wellbeing in nonclinical samples: a systematic review and meta-analysis. Int. J. Stress Manag. 27, 394–411. doi: 10.1037/str0000165
Rempel, K. D. (2012). Mindfulness for children and youth: A review of the literature with an argument for school-based implementation. Can. J. Couns. Psychother. 46, 201–220.
Rinpoche, T. (1998). Carefree Dignity: Discourses on Training in the Nature of Mind. Santa Ana, CA: RYP.
Romeo, R. D. (2017). The impact of stress on the structure of the adolescent brain: implications for adolescent mental health. Brain Res. 1654, 185–191. doi: 10.1016/j.brainres.2016.03.021
Rudnik, A., Anikiej-Wiczenbach, P., Szulman-Wardal, A., Conway, P., and Bidzan, M. (2021). Offering psychological support to university students in Poland during the COVID-19 pandemic: lessons learned from an initial evaluation. Front. Psychol. 12:635378. doi: 10.3389/fpsyg.2021.635378
Saltzman, A., and Goldin, P. (2008). “Mindfulness-based stress reduction for school-age children,” in Acceptance and Mindfulness Treatments for Children and Adolescents: A Practitioner's Guide, eds. L. A. Greco and S. C. Hayes (Oakland, CA: New Harbinger Publications), 139–161.
Segal, Z. V., Teasdale, J. D., Williams, J. M., and Gemar, M. C. (2002). The Mindfulness-Based Cognitive Therapy Adherence Scale: inter-rater reliability, adherence to protocol and treatment distinctiveness. Clin. Psychol. Psychother. 9, 131–138. doi: 10.1002/cpp.320
Shapiro, S. L., Carlson, L. E., Astin, J. A., and Freedman, B. (2006). Mechanisms of mindfulness. J. Clin. Psychol. 62, 373–386. doi: 10.1002/jclp.20237
Shigemura, J., Ursano, R. J., Morganstein, J. C., Kurosawa, M., and Benedek, D. M. (2020). Public responses to the novel 2019 coronavirus (2019-nCoV) in Japan: mental health consequences and target populations. Psychiatry Clin. Neurosci. 74, 281–282. doi: 10.1111/pcn.12988
Swain, J., Hancock, K., Dixon, A., and Bowman, J. (2015). Acceptance and commitment therapy for children: a systematic review of intervention studies. J. Cont.Behav. Sci. 4, 73–85. doi: 10.1016/j.jcbs.2015.02.001
Tan, L. B. (2016). A critical review of adolescent mindfulness-based programmes. Clin. Child Psychol. Psychiat. 21, 193–207. doi: 10.1177/1359104515577486
Venuleo, C., Marinaci, T., Gennaro, A., Castiglioni, M., and Caldiroli, C. L. (2022). The institutional management of the COVID-19 crisis in Italy: a qualitative study on the socio-cultural context underpinning the citizens' evaluation. Mediterranean Journal of Clinical Psychology 10, 1–29.
Weis, R., Ray, S. D., and Cohen, T. A. (2021). Mindfulness as a way to cope with COVID-19-related stress and anxiety. Counsel. Psychother. Res. 21, 8–18. doi: 10.1002/capr.12375
Xie, X., Xue, Q., Zhou, Y., Zhu, K., Liu, Q., Zhang, J., et al. (2020). Mental health status among children in home confinement during the Coronavirus Disease 2019 outbreak in Hubei Province, China. JAMA Pediatr. 174, 898–900. doi: 10.1001/jamapediatrics.2020.1619
Zambianchi, M. (2015). Time perspective and psychological wellbeing in old age. BPA-Appl. Psychol. Bullet. 63:274.
Zenner, C., Herrnleben-Kurz, S., and Walach, H. (2014). Mindfulness-based interventions in schools-a systematic review and meta-analysis. Front. Psychol. 5:603. doi: 10.3389/fpsyg.2014.00603
Keywords: mindfulness, positive psychology, wellbeing, COVID-19, pandemic, trauma, clinical intervention
Citation: Caldiroli CL, Procaccia R, Negri A, Mangiatordi A, Sarandacchi S, Antonietti A and Castiglioni M (2024) Mindfulness and mental health: the importance of a clinical intervention to prevent the effects of a traumatic event. A pilot study. Front. Psychol. 15:1449629. doi: 10.3389/fpsyg.2024.1449629
Received: 15 June 2024; Accepted: 26 September 2024;
Published: 22 October 2024.
Edited by:
Michela Ponticorvo, University of Naples Federico II, ItalyReviewed by:
Floriana Irtelli, Catholic University of the Sacred Heart, ItalyIlaria Terrenghi, University of Milan, Italy
Antonio Ascolese, Università Sigmund Freud Milano, Italy
Copyright © 2024 Caldiroli, Procaccia, Negri, Mangiatordi, Sarandacchi, Antonietti and Castiglioni. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cristina Liviana Caldiroli, Y3Jpc3RpbmEuY2FsZGlyb2xpQHVuaW1pYi5pdA==