 Vrinda V. Naicker
Vrinda V. Naicker Darren Hedley
Darren Hedley Simon M. Bury
Simon M. Bury- Olga Tennison Autism Research Centre, School of Psychology and Public Health, La Trobe University, Melbourne, VIC, Australia
Introduction: Resolution of a child’s diagnosis, the process of accepting and adjusting to the reality of a child’s significant diagnosis, has been often associated with decreased parental stress. Hope, a potential buffer against psychological distress, has been suggested as a potential explanation for this relationship. However, the mediating role of hope in the relationship between resolution of diagnosis and parental stress has not been explored.
Methods: This study aimed to examine whether four types of hope (child, parental, societal, denial of diagnosis) mediated the relationship between resolution to an autism diagnosis and reduced parental stress. Participants included 73 parents (Mage = 43.22, SD = 7.69, female 97.3%) of autistic children (Mage = 11.15, SD = 4.56, male = 67.1%).
Results: Resolution to diagnosis was negatively and significantly correlated with resolution to diagnosis, as well as child, parental and societal hope. These three hopes were also significantly and negatively correlated with parental stress. Importantly, when controlling for level of support and autism awareness, parental hope mediated the relationship between resolution to diagnosis and parental stress. Denial of diagnosis was not correlated with resolution or parental stress but did have significant but weak associate with the other hopes.
Discussion: These findings suggest that hope based on parent’s abilities to support their child and be supported themselves play an important role in parental stress once parents are more resolved to their child’s diagnosis. Supporting parents to manage factors associated with supporting their child’s needs, may benefit parents of autistic children.
1 Introduction
Receiving an autism spectrum disorder (hereafter “autism”; American Psychiatric Association, 2013) diagnosis for a child can be a stressful experience for parents (Poslawsky et al., 2014). Parents’ ability to adjust their expectations of parenthood from pre-diagnosis to post-diagnosis may contribute to this increased stress (Milshtein et al., 2010). This adjustment process, where parents come to terms with the implications of the diagnosis, is known as resolution to diagnosis (Marvin and Pianta, 1996; hereafter “resolution”). Research shows that parents who achieve higher resolution regarding significant diagnoses for their children (e.g., Cerebral Palsy, autism, and psychiatric disorders) often experience positive outcomes, such as reduced parental stress (Sher-Censor and Shahar-Lahav, 2022; Lord et al., 2008). However, less is known about the mechanisms behind why resolution may lead to reduced stress. Increased hope, which acts as a protective factor against psychological distress (Mednick et al., 2007; Ogston et al., 2011), has been suggested as a potential explanation. Despite this, the relationship between resolution and hope has been inconsistent, possibly due to how hope is conceptualized in these studies. We propose that a goal-focused hope, grounded in reality (Bury et al., 2016), may better explain the relationship between resolution and reduced parental stress in parents of autistic children.
1.1 Autism and parental stress
Autism is a neurodevelopmental condition characterized by differences in social communication and interaction skills, as well as restricted, repetitive patterns of behavior (American Psychiatric Association, 2013). These differences can impact autistic children’s inclusion in daily activities, such as school, leading to varying levels of required support in these domains. Diagnosing autism in childhood allows parents the opportunity to provide additional behavioral or academic support during critical developmental years (Okoye et al., 2023). However, the diagnostic and support process can also cause significant distress for parents (Moh and Magiati, 2012).
Parents of children diagnosed with autism experience higher levels of stress compared to parents of typically developing children and those with other disabilities (Bonis, 2016; Dabrowska and Pisula, 2010; Smith et al., 2001). Stress may stem from the additional demands parenting an autistic child may present, such as managing behaviors that challenge, changes in the parent’s life (e.g., routines, relationships with friends and family), as well as difficulties finding and organizing autism services, or overcoming barriers or challenges with the education systems (Bonis, 2016, Hayes and Watson, 2013). Managing this stress is crucial, as it can impact parent–child relationships and the overall wellbeing of both the child and parent (Schieve et al., 2007). Increased stress can alter parenting behaviors, which may influence the child’s symptoms and behaviors (Eshraghi et al., 2022).
Behavioral characteristics, such as the level of challenging behaviors and support needs, are particularly associated with elevated stress levels (Dabrowska and Pisula, 2010; Estes et al., 2009; Pastor-Cerezuela et al., 2016; Yirmiya et al., 2015). Higher support needs place greater demands on parents (Krakovich et al., 2016). Given the impact of stress on the family dynamic, focusing on factors that reduce stress is essential for improving family functioning (Hayes and Watson, 2013).
1.2 Resolution to diagnosis
Resolution to diagnosis is suggested to help parents better manage this stressful time (Sheeran, et al., 1997). Marvin and Pianta (1996) describe resolution as a process of accepting a diagnosis in its entirety, understanding the implications of the diagnosis, and parents adjusting their internal representations and expectations of their child from pre-diagnosis to post-diagnosis. This process involves aligning prior internal representations with the new reality of having a child with different needs (Milshtein et al., 2010).
Derived from attachment theory, particularly secure attachment (Marvin and Pianta, 1996; Oppenheim et al., 2009), resolution involves parents being emotionally available to understand their child’s emotions and meet their caregiving needs (Bowlby, 1969; Allen et al., 1996). Sheeran et al. (1997) found that resolution affects intimate family relationships and broader social circles surrounding the family, making it important to identify factors that impact this process. Da Paz et al. (2018) report that the severity of a child’s symptoms is positively associated with resolution. Additionally, time since diagnosis and prior knowledge of the diagnosis and its impact are linked to increased resolution and reduced stress levels (Al-Oran and Al-Sagart, 2016).
Parents’ knowledge and uncertainty about the diagnosis significantly affect their understanding of autism, contributing to a sense of loss. A lack of knowledge can prevent parents from understanding their child and accessing appropriate support, while greater knowledge serves as a protective factor (Alsayyari, 2018; Heredia-Alvarado, 2017; Rabba et al., 2019). Achieving acceptance and resolution is associated with positive emotional responses and improved interactions with their child (Heredia-Alvarado, 2017; Hotez, 2016; Rabba et al., 2019). In contrast, negative emotions such as denial and blame elongate the resolution process (Ferguson and Vigil, 2019).
Resolved parents experience less guilt, blame, and shame regarding the autism diagnosis (Naicker et al., 2023; Da Paz et al., 2018; Heredia-Alvarado, 2017). Resolution acts as a protective factor, reducing feelings of shame and denial and enhancing parent wellbeing, attunement, and insightfulness in the parent–child relationship (Naicker et al., 2023). Therefore, understanding the factors that influence the resolution process is crucial.
1.2.1 Resolution and stress
One of the common benefits of resolution is its association with lower stress levels among parents (Sheeran et al., 1997; Lord et al., 2008). A scoping review by Sher-Censor and Shahar-Lahav (2022) found unresolved narratives associated with higher parenting stress among 16 studies, including childhood diagnoses of autism, Phenylketonuria, down syndrome, cerebral palsy, Type 1 Diabetes, and psychiatric disorders (e.g., attention deficit hyperactivity disorder and mood disorder). This review found unresolved narratives up to a month after receiving the diagnosis were specifically related to higher stress. A review by Naicker et al. (2023) found that parents with higher resolution reported reduced psychological distress and depression, an overall higher capacity to cope with stress, higher levels of marital satisfaction, and seeking and accessing social support. Importantly, although parents of children diagnosed with autism experience higher levels of stress (Smith et al., 2001), resolution is still associated with lower stress in parents of children with autism (Sheeran et al., 1997). However, while the relationship between resolution and stress is established, explanations for why this relationship exists are less developed. One factor suggested to underpin this relationship is hope.
1.2.2 Resolution and hope
While discussed as a factor of resolution, few studies discuss the direct link between resolution and hope. Some studies found that mentions of hope arise when examining parental experiences with diagnostic processes and raising a child (Rabbitte et al., 2017). Another study found hope to arise regarding the future of their child: the increasing independence of their child and hope surrounding support systems to facilitate their child’s needs (Benderix et al., 2006). However, there is inconsistent evidence regarding the nature of the relationships between hope and resolution (Sher-Censor and Shahar-Lahav, 2022). For example, while Lord et al. (2008) found no significant association between resolution and hope, Popp et al. (2015) found parents to have greater hope when resolved to their child’s Cancer diagnosis. Differences in outcomes may arise when considering theoretical considerations of hope.
1.3 Hope in uncertainty
Hope has traditionally been conceptualized in psychology as a positive expectancy construct (see Hope Theory; Snyder et al., 1991), in which a greater perceived likelihood of success results in higher levels of hopefulness. Theorized this way, hope has similar outcomes to other expectancy-based outcomes (e.g., self-efficacy and optimism), thus the unique nature of hope is unclear. Rather than an expectation of success, alternative approaches to hope show that hope arises in uncertainty (Bury et al., 2016; Miceli and Castelfranchi, 2010; Ogston et al., 2011), when individuals are less assured of success (Bury et al., 2019). Such conceptualizations are more in line with qualitative descriptions of hope, highlighting that hope as emotion is future-focused, and arises for uncertain or uncontrollable outcomes (Bruininks and Malle, 2005), outcomes not well captured in expectancy-based theories of hope. Hope in uncertainty does not suggest that people downplay or ignore the odds, rather for outcomes that are of significant importance to the individual, it is precisely the uncertainty of success that requires one to hope (Bury et al., 2016). Conceptualized thus, research shows hope to be distinct from expectancy measures (Bury et al., 2019) and associated with intention to act, even for outcomes outside one’s sole agency (Bury et al., 2020).
When receiving a significant diagnosis for their child, parent’s uncertainty about their child’s future and their ability to support their child’s needs suggest a good environment for hope. Research suggests that caregivers who receive a significant childhood diagnosis perceive greater uncertainty about the diagnosis and future outcomes for their child and parenting, which is associated with greater initial distress as well as additional hope (Mulligan et al., 2012; Sanders-Dewey et al., 2001). Studies have found hope arises during the diagnostic process with some parents reporting an initial loss of hope when receiving the diagnosis or regarding their initial expectations surrounding therapies, contrastingly gaining a sense of hope within the uncertainty of receiving the diagnosis often from surrounding supports (i.e., professionals, social circles; McPhilemy and Dillenburger, 2013; Reiff et al., 2017; Rabba et al., 2019). Singh (2016) found parents who receive their child’s diagnosis and are presented with initial expectations surrounding the condition, describe minimal hope for the future. However, these parents reported having to create hope, leading to opportunities to challenge boundaries placed on their child’s diagnosis.
In terms of resolution, the resolution includes parent’s expectations and internal representations of their child aligning with their child’s diagnosis, which promotes realistic, but uncertain, expectations for their child’s future (Sher-Censor and Shahar-Lahav, 2022). Dolev et al. (2016) found the process of refocusing attention and realistic expectations leads parents to have a greater understanding of appropriate parenting methods for their child, resulting in parents better responding to child cues. Thus, a hope grounded in possibility, not probability, likely presents a greater resource for parents at such times. Indeed, initial evidence in other domains suggests hope may be a good facilitator of goal-consistent action at such times (Bury et al., 2020).
1.3.1 Stress and hope
Importantly, hope has also been suggested to be a protective factor against psychological distress (Mednick et al., 2007). Ong et al. (2006) found individuals with higher hope displayed reduced stress reactivity, effective emotional recovery, and the ability to keep negative emotions low. Receiving a child’s diagnosis can be strenuous on parent’s wellbeing, with parents reporting the need for hope during the diagnostic process (Nissenbaum et al., 2002). In children diagnosed with Phenylketonuria, Lord et al. (2008) found higher levels of personal hopefulness to be associated with lower levels of parenting stress, while Mednick et al. (2007) identified hope as a protective factor against psychological distress in mothers of children diagnosed with type 1 diabetes. However, little research discusses the relationship between stress and hope in the context of autism, even more so with hope as a mediating factor between stress and resolution. Additionally, the theoretical perspective of hope in this research is not clear, with parents describing hope as including optimism (Nissenbaum et al., 2002), an expectancy-based construct often confused for hope (Bury et al., 2019).
1.3.2 Hope and receiving an autism diagnosis
Hope, then, is a positive future-focused emotion, arising from possible but uncertain goals (Bury et al., 2016; Miceli and Castelfranchi, 2010; Wenzel et al., 2017). To better understand what specific goals parents of children with an autism diagnosis have that may engender hope, we have reviewed the literature to identify specific goals of hope. We found that parents have reported different descriptions of specific hopes, which have been categorized into four different categories: hope for the child, parental hope, societal hope, and denial of diagnosis.
Hope for the child reflects realistic and positive goals for their child’s future and encompasses goals such as parents’ hopes to form meaningful relationships with their child, and future hopes for their child to live a good quality and emotionally fulfilling life (Benderix et al., 2006; McPhilemy and Dillenburger, 2013; Mulligan et al., 2012; Ogston et al., 2011; Reiff et al., 2017; Rabba et al., 2019; Singh, 2016; Blake, 2021). Given a focus on positive strength-based outcomes for the child, resolution seems important for these hopes to arise.
Parental hope reflects parents’ own hopes for themselves, specifically their ability to support their child financially and mentally and to be able to meet their child’s needs (Blake, 2021; Ekas et al., 2016; Mulligan et al., 2012; Ogston et al., 2011). Parental hope also represents parents’ hopes about being supported themselves.
Societal hope reflects parent’s hopes for the greater community coming to better understand and value autism (Ekas et al., 2016; Rabba et al., 2019). This hope is bigger than the individual and represents a broader hope of their child being recognized and supported by society for who they are.
Denial of diagnosis potentially represents more a denial than of a true hope based on reality (McPhilemy and Dillenburger, 2013; Mulligan et al., 2012; Reiff et al., 2017). Rather than a realistic representation of the future, hopes around the denial of diagnosis include wishing that the diagnosis was wrong, could be corrected, or that the child will still be able to meet the parent’s preconceived expectations. Given this hope does not reflect resolution to a diagnosis, we would not expect it to be associated with resolution of diagnosis, or to reduced stress.
1.4 The current study
We investigated the relationship between resolution to diagnosis and parental stress in parents of children with an autism diagnosis. Specifically, we were interested in whether hope mediates the relationship between resolution and parental stress, and what type of hope best explains this relationship. We conducted a single mediation model with multiple hope mediators (Figure 1). We predicted there would be a negative relationship between resolution and parental stress (Hypothesis 1). Next, we predicted there would be an indirect effect of resolution to diagnosis and parental stress via child hope, parental hope, and social hope, whereby resolution will lead to greater hope, and in turn, lower parental stress (Hypotheses 2, 3, and 4). For hope that denies the diagnosis, we tentatively predict that resolution would be negatively associated with negative hope, and positively associated with parental stress.
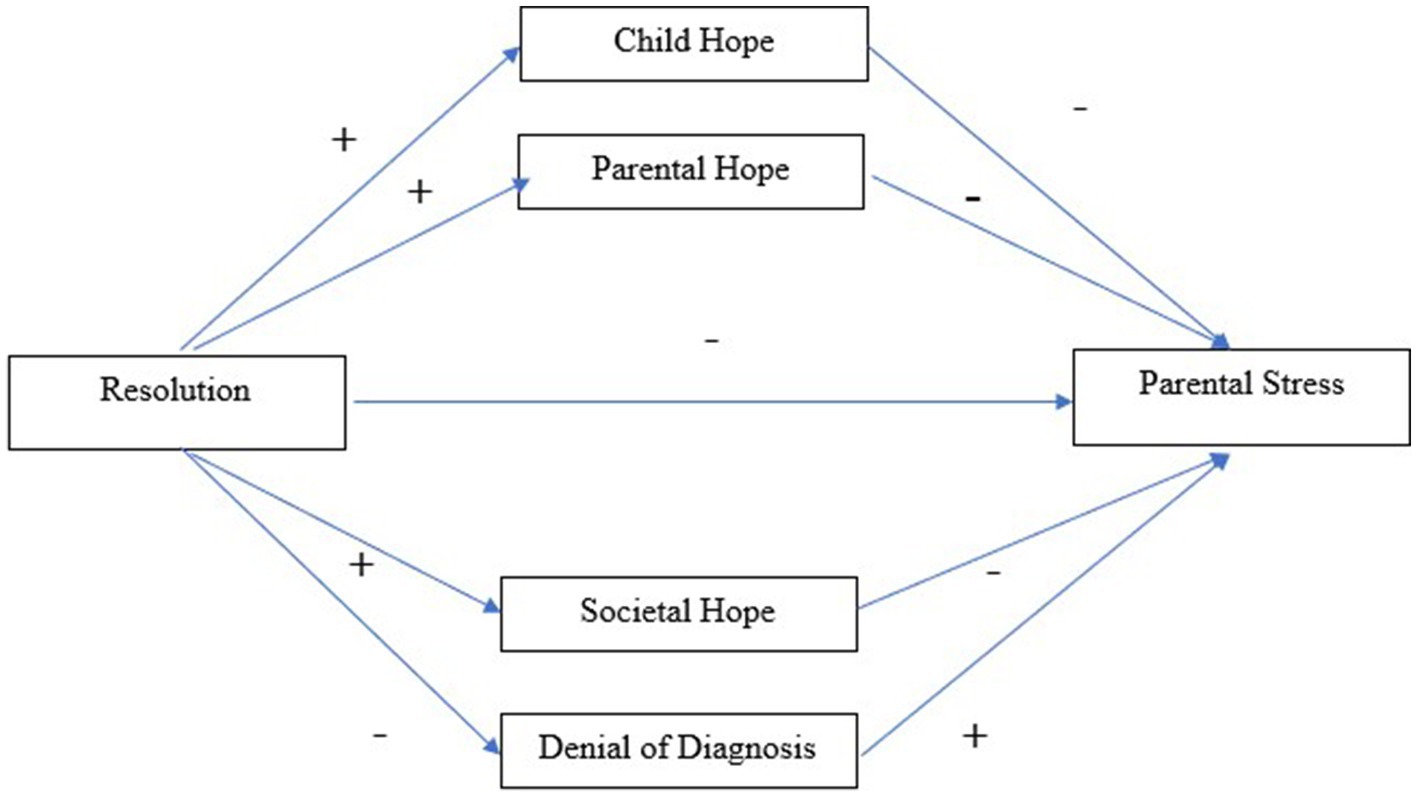
Figure 1. Predicted indirect path of resolution and parental stress via hope (Child, Parental, Societal, Denial of Diagnosis).
2 Method
2.1 Participants
Participants were 73 parents of autistic children (Mage = 43.22, SD = 7.69, female = 97.3%, male = 2.7%) who completed the survey (see Table 1 for sample demographics). Participant’s children (Mage = 11.15, SD = 4.56, Male = 67.1%; Female = 32.9%) were all diagnosed with autism, with a mean diagnosis age of 5.5 (SD = 3.45). Most parents (75%) knew their child’s level of support (Level 1: 13.0%, Level 2: 66.7%, Level 3: 20.4%), with the remaining (25%) parents reporting the perceived level of severity of their child (Level 1: 21.1%, Level 2: 63.2%, Level 3: 15.8%).
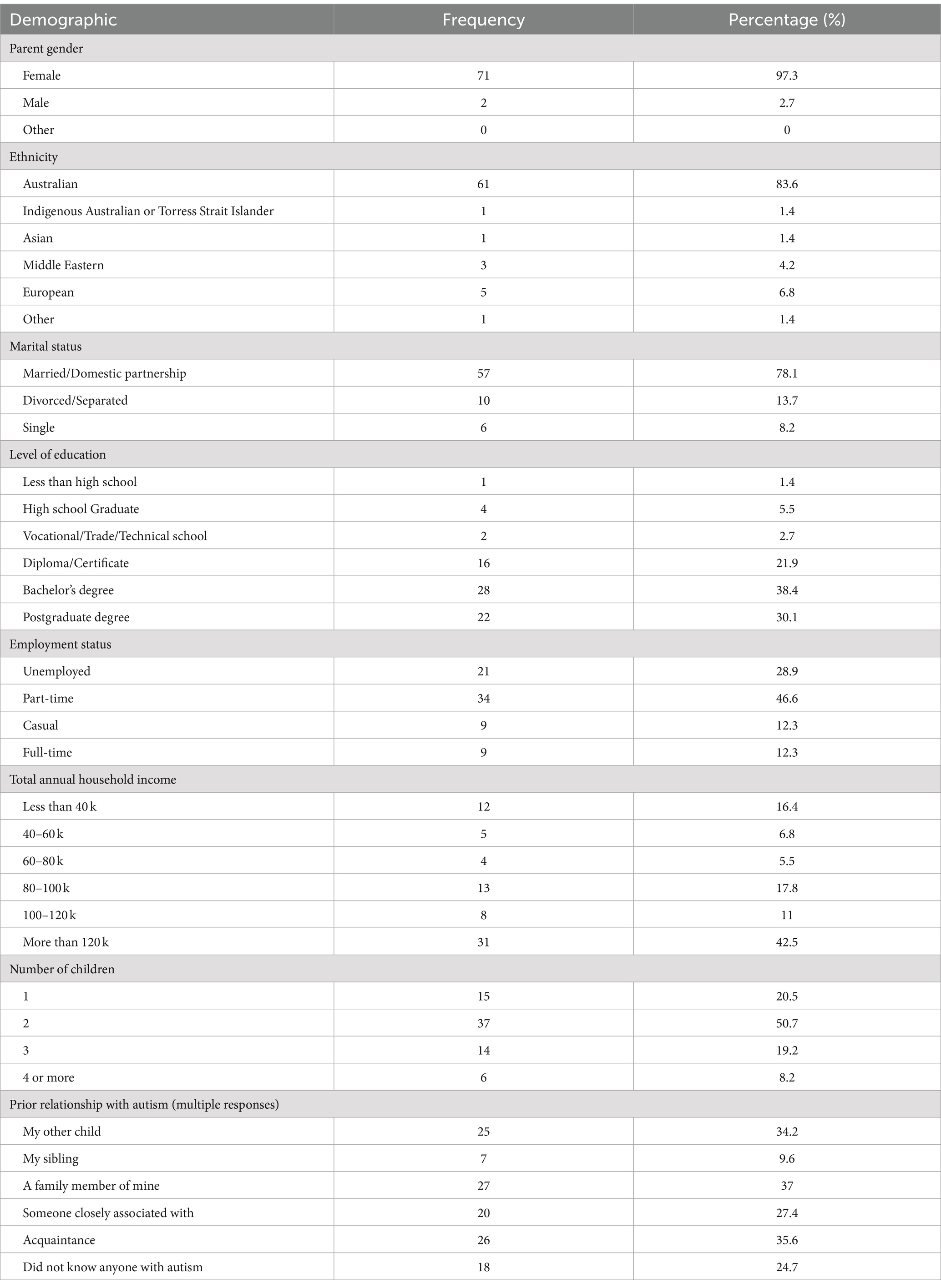
Table 1. Parent demographic information, frequency, and percentages.
2.2 Measures
Participants first completed a demographic questionnaire collecting general information (age, gender, marital and employment status, household information, etc.), the parents’ own characteristics, information regarding the child’s diagnosis, prior knowledge, and prior relationships with individuals with autism. They were then presented with measures for the main variables in the study.
2.2.1 Resolution
The Reaction to Diagnosis Questionnaire (RDQ) (Sher-Censor et al., 2020) is a new self-report measure assessing parental resolution of their child’s diagnosis. The RDQ is a 42-item, 5-point Likert scale (1 = Strongly Disagree, 5 = Strongly Agree), showing good internal consistency across two sample sizes (Sher-Censor et al., 2017). This study purposefully removed an item from the RDQ due to a similar hope formulation to items in the denial of hope (Item 38 “I hope that my child’s condition will improve with time”), while another item was excluded by error (Item 29). Higher scores indicated higher resolved parents (McDonald’s ω = 1.20).
2.2.2 Parental stress
The Parental Stress Scale (PSS) is a widely used standardized scale measuring parental stress (Berry and Jones, 1995). It includes 18 items and a 5-point Likert scale (1 = Strongly Disagree, 5 = Strongly Agree). It encompasses both the demands and fulfilling aspects of parenting, showing adequate reliability and good test–retest reliability and strengths as a cross-cultural measure, presenting possible face validity (Louie et al., 2017). Scores were then averaged with higher scores indicating greater stress levels (McDonald’s ω = 1.06).
2.2.3 Hope
Hope was measured with a new measure targeting four hope-based goals, based on Wenzel et al. (2017). In total, 19 hope statements were created based on prior research (see Introduction section). These studies revealed that parents experienced different sub-sets of hope regarding their children. Thus, the statements examined were categorized into four hope categories. Child hopes (McDonald’s ω = 0.96) included eight statements of hope for their child (“I am hopeful that my child will have a good quality of life”). Parental hope (ω = 0.89) included five statements about the parent’s ability to meet the needs of their child (“I am hopeful that I can be the parent that my child needs me to be”). Societal hope (ω = 0.97) included three items reflecting greater acceptance of autism in society (“I am hopeful that society will see the strengths associated with autistic people”). Denial of diagnosis (ω = 0.75) included three items that reflected a denial or hope that the diagnosis was wrong (“I am hopeful that my child’s diagnosis was a mistake”). All items were measured with a 7-point Likert scale (1 = Strongly Disagree, 7 = Strongly Agree), with a higher mean indicating higher levels of hope in that specific category.
2.2.4 Covariates
We measured four variables to be potential covariates, based on their association with resolution or parental stress in the literature. Autism Knowledge: The Autism Awareness Survey (AAS) (Gillespie-Lynch et al., 2015) was used to assess the accuracy of parent’s knowledge of autism. It includes 13 items measured on a 5-point Likert scale (1 = Strongly Disagree, 5 = Strongly Agree) with higher scores indicating a higher level of knowledge about autism y (α = 0.69). Time since diagnosis was calculated by subtracting the date of diagnosis provided by parents in the demographic survey from the date the survey was taken. Prior relationship with autism: parents were asked if and whom they knew who also had an autism diagnosis, this was then coded into a numerical value (0 = no prior relationship, 1 = prior relationship). The level of support was calculated through demographic questions asking parents about known or perceived level (Level 1 = Requires support, Level 3 = Requires very substantial support) of their child’s support level. Participants only reported perceived level if they did not know their child’s support level, with perceived level used in the absence of the actual level of required support.
2.3 Procedure
This study was granted ethics approval by the La Trobe University Human Research Ethics Committee (Approval number: HEC22124). Participants were recruited via social media of the Olga Tennison Autism Research Centre (OTARC), particularly targeting autism-specific forums, groups, and organizations. Inclusion criteria for participants required the parents of autistic children to be 18 years of age and over. To ensure greater control for broad societal and cultural differences, participants were required to be Australian citizens or permanent residents. Interested individuals were led to the online survey hosted via REDcap (Harris et al., 2019) via the link provided on all advertisement materials. Upon completion of the survey, participants entered a prize draw to win one of ten $50 supermarket gift vouchers.
2.4 Analytic plan
Only 0.29% of the variable data was missing, with Little’s MCAR test Chi-Square (835) = 138.27, p = 1.000, indicating that data were missing at random. Missing data were imputed from the mean of adjacent variables to ensure maximum sample size. One participant only responded to 15% of items for the Autism Awareness Scale, these data could not be imputed so were marked as missing for this measure.
Data were collated and prepared using Statistical Package for Social Scientists, Version 28.0 (SPSS). To test the internal validity of identified factors, McDonald’s Omega was used. Correlation was run using SPSS with 1,000 Bootstrapped confidence intervals indicating significance, including all key variables and the four potential covariates. Mediation analysis was conducted using Model 4 of the PROCESS Macro in SPSS (Hayes, 2018) with 5,000 bootstrapped samples, with covariates that correlated significantly with model variables included as covariates.
3 Results
3.1 Correlation between resolution and parental stress
Pearson correlations were run between all variables, including covariates (Table 2). Resolution had significant positive moderate to strong correlations with child hope, parental hope, and societal hope. Stress was negatively and significantly correlated with child, parental, and societal hope, but there was no significant correlation between stress and hope that denies the diagnosis. Child, parental, and societal hopes were all significantly and positively correlated, with parental and societal hopes strongly and significantly positively correlated. Denial of diagnosis was significantly positively, yet weakly, correlated with the other hope items. Level of support was negatively correlated with denial of diagnosis, as was autism awareness. Prior relationship and times since diagnosis did not correlate with any other variable.
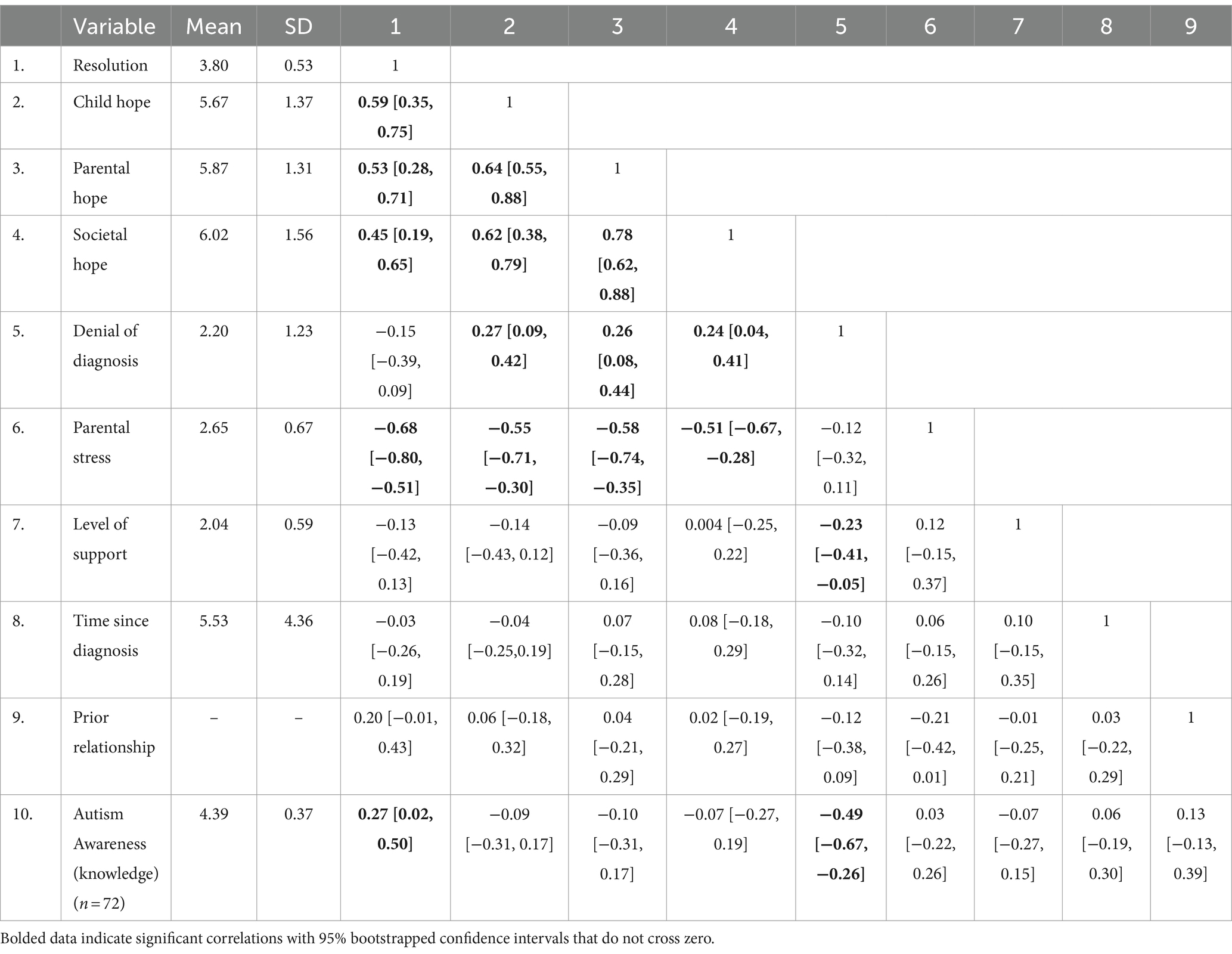
Table 2. Correlations between variables of interest with bias corrected accelerated bootstrapped confidence intervals (95%).
3.2 Mediation analyses
PROCESS was used to test whether different types of hope (child hope, parental hope, societal, and denial) mediated the relationships between resolution and stress, with autism awareness and level of support entered as covariates. Due to the high correlation between parental and societal hope, societal hope was dropped from analyses to avoid problems of collinearity (Hayes, 2018)1.
The total effect model was significant, F = 22.86, (3.68), p < 0.001, and explained 50.22% of the variance. The total, ß = −0.92, SE = 0.11, 95% CI [−0.70–0.73], p < 0.001, and direct effect of resolution on stress were both significant, ß = −0.79 SE = 0.15, 95% CI [−0.49–0.63], p < 0.001, indicating higher resolution was negatively associated with lower parental stress as predicted.
There was a significant indirect effect between resolution and stress via parental hope (Figure 2), ß = −0.15, SE = 0.07, 95% CI [−0.40, −0.002], indicating that after controlling for variables parental hope mediated the link between resolution and stress. Child-focused hope did not mediate the relationship between resolution and stress as the bootstrapped confidence interval crossed zero, ß = 0.04 SE = 0.08, 95% CI [−0.14, 0.19], neither did denial of diagnosis, ß = 0.007, SE = 0.02, 95% CI [−0.03, 0.06]. See Table 3 for the overall results of parallel mediation analysis.
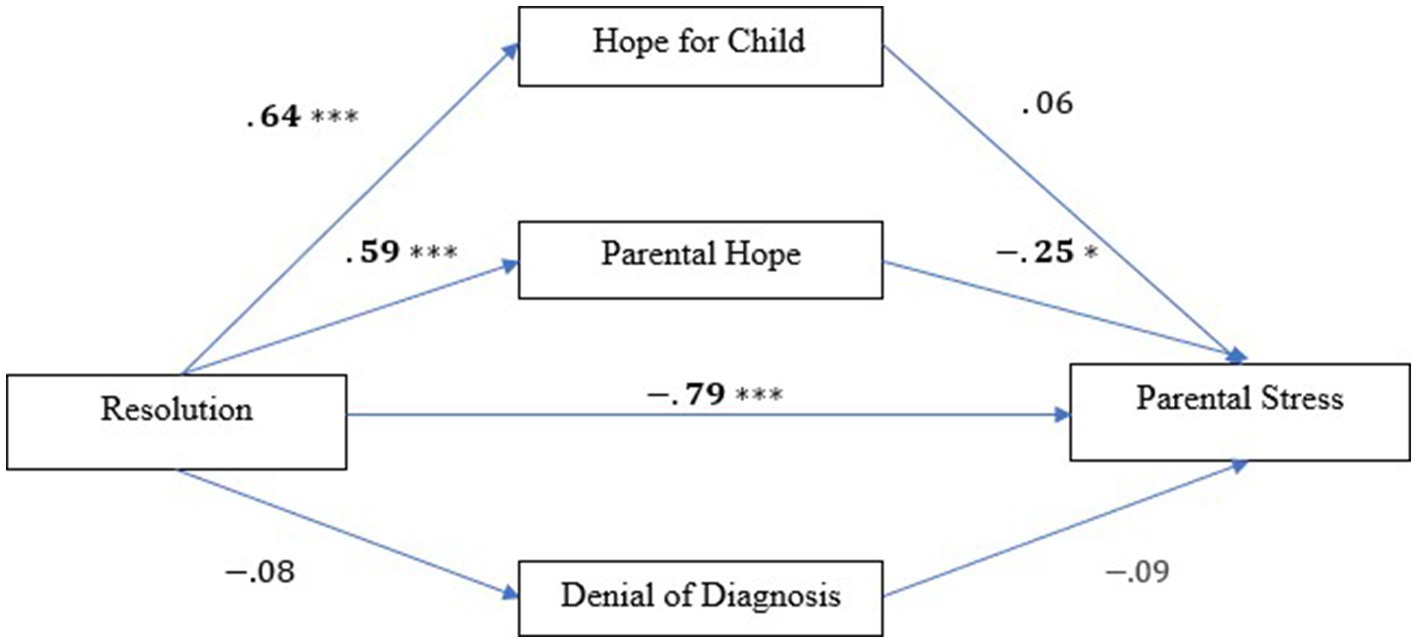
Figure 2. Parallel mediation analyses showing standardized regression coefficients for relationships between resolution, hope (hope for child, parental hope, denial of diagnosis), and parental stress. *p < 0.05, **p < 0.01, ***p <0.001.
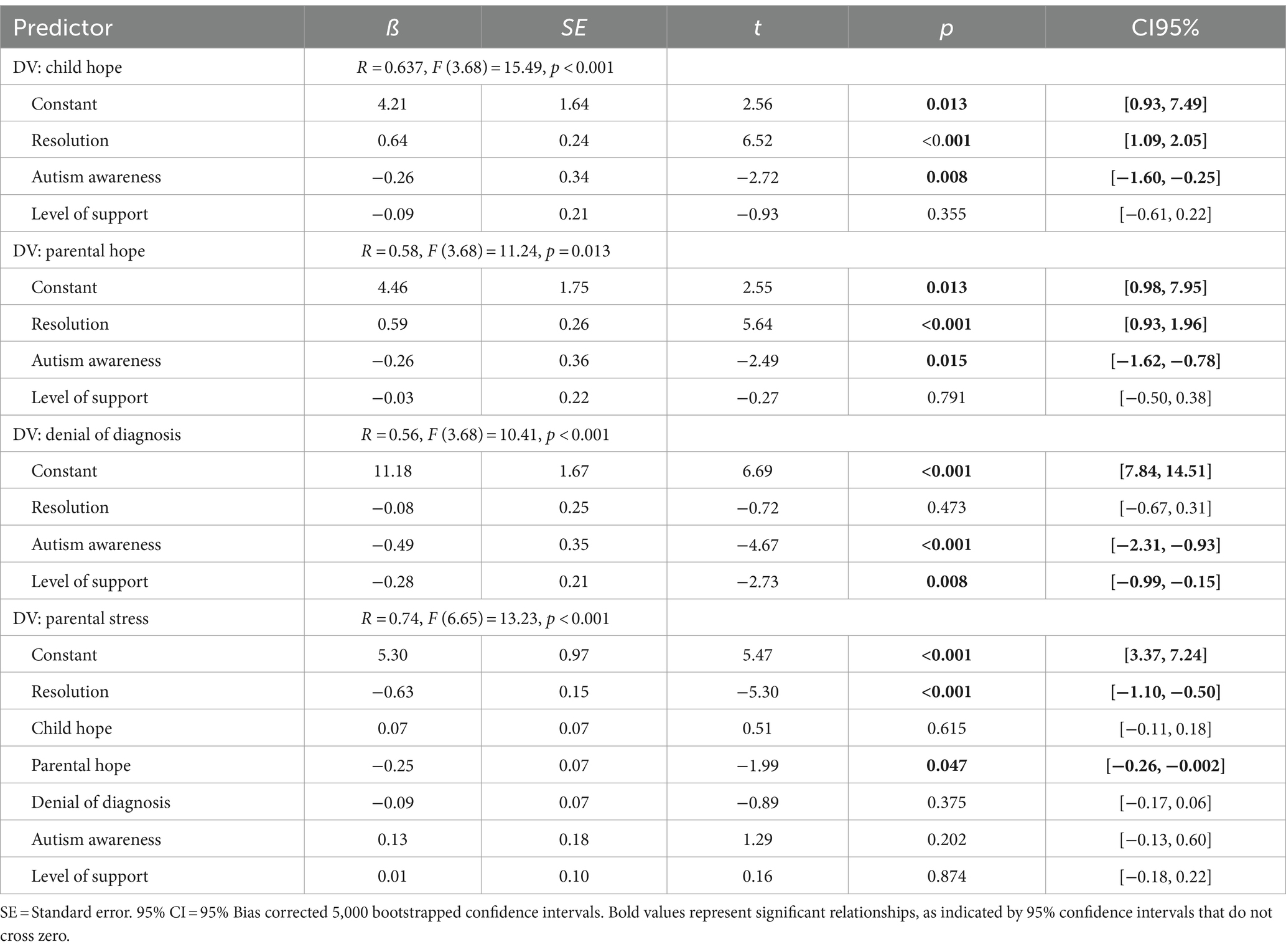
Table 3. Indirect effect of resolution of diagnosis on parental stress, via child hope, parental hope, and denial of diagnosis.
4 Discussion
We investigated the relationship between resolution to diagnosis and parental stress in parents of autistic children, and whether hope mediated this relationship. Consistent with previous literature (Lord et al., 2008), both correlational and regression analysis supported the hypothesis (H1) that parents with greater resolution to diagnosis reported significantly lower levels of stress. This aligns with the broader literature surrounding significant childhood diagnoses (Sheeran et al., 1997; Sher-Censor and Shahar-Lahav, 2022; Lord et al., 2008), highlighting the importance of resolution as a potential avenue for improved wellbeing of parents. While an important finding, especially in terms of autism research, the role that hope plays in explaining this relationship is an important contribution to the literature.
We positioned hope in line with theoretical perspectives that conceptualize hope as a positive emotion arising in times of uncertainty (e.g., Miceli and Castelfranchi, 2010) for outcomes of significant importance to the individual (Bury et al., 2016). Hope in uncertainty is fitting for parents of children of significant diagnosis, who often report uncertainty regarding their child’s future and their ability to meet the needs of their child (Mulligan et al., 2012; Ogston et al., 2011). Indeed, in this study, parental hopes associated with the child and the child’s future wellbeing, the parents’ ability to support the child, and societal expectations were all strongly endorsed by participants. These hopes were also significantly correlated, suggesting that parents hold multiple hopes for their children simultaneously. Interestingly, while endorsed to a much lower degree, with mean scores below the midpoint of the scale, hopes that the diagnosis was wrong, were also weakly associated with the other hope items. This suggests that although parents can hope that their child can have meaningful life outcomes, and be supported by themselves and society, to a much lesser degree, some parents also hope the diagnosis may be a mistake. However, hope was stronger for positive outcomes representing a resolution to and acceptance of the diagnosis of their child, and particularly for hopes regarding the parent’s ability to meet the needs of their child, which were associated with better wellbeing.
Importantly, as predicted (H3), parental hope was shown to mediate the relationship between resolution to diagnosis and parental stress. Parents resolved to their child’s diagnosis had greater hopes that they could support and would be supported to meet the needs of their child, and this was associated with lower levels of stress. This aligns with research suggesting that resolution in parents has been associated with social support and a perceived sense of competence from the parents (Hotez, 2016; Ekas et al., 2016). After receiving the diagnosis, this shift in adjusting to realistic expectations of the potentially different needs of their child post-diagnosis perhaps provides parents with an understanding of themselves as parents (Brown et al., 2021), perhaps resulting in more realistic hope for themselves as a ‘supporting figure’ in their child’s life (Ogston et al., 2011; Rabba et al., 2019). These realistic expectations may contribute to the reduction in stress, as studies show that parents with a well-supported diagnostic experience and family dynamic feel more at ease compared to parents with poor diagnostic experiences (Abbott et al., 2013; Alsayyari, 2018).
Our results suggest that positive hope for the child did not mediate the relationship between resolution and stress. While positively associated with resolution, when considered in the mediation model, hope for the child was not significantly associated with reduced stress. Compared to parental hope, hopes for the child tended to be more distal, and did not have the direct agency that parental hope has. Although the agency is not necessary for hope to emerge and influence behavior (e.g., Bury et al., 2020), it was not associated with reduced parental stress in this study. Thus, our findings suggest that perhaps parents’ hopes in their ability as a parent is more important and indicative of stress, rather than positive hope for their child. Hence, although parents may have great positive hope regarding their child’s wellbeing and abilities (Mulligan et al., 2012; Ogston et al., 2011; Blake, 2021), it does not have a significant effect on the relationship between resolution and stress.
While hope that a diagnosis was mistaken is not necessarily impossible and thus is not technically denying reality, it certainly seems antithetical to the idea of resolution to diagnosis. That being said, hope in the denial of diagnosis was not associated significantly with either resolution or parental stress in this study. It was also not strongly endorsed by participants (mean scores below the mid-point of the scale). Interestingly, this type of hope was negatively associated with parents who reported a greater level of support needs for their children. While it could be reasonable to hope the diagnosis was wrong for those experiencing a greater impact of a diagnosis on their child’s level of need, Yirmiya et al. (2015) suggest parents may find achieving or maintaining a resolved status easier when increased symptom severity is present. Thus, the reality of greater support needs does not allow parents the luxury to foster thoughts of a mistaken diagnosis. Additionally, more accurate knowledge of autism was significantly negatively correlated with denial of diagnosis, suggesting knowledge may act as a protective factor against unrealistic expectations (Alsayyari, 2018; Heredia-Alvarado, 2017; Rabba et al., 2019).
4.1 Theoretical and practical implications
The present study strengthens understanding of the important role resolution to diagnosis has for parent wellbeing, and the importance of hope in this process. These findings suggest that parental hope may be particularly induced in times of uncertainty and likely placed in the possibility of creating more goal-oriented perspectives and formations of hope (Bury et al., 2019). As Rabba et al. (2019) found parents resorted to maintaining hope as a mechanism in managing the uncertainty of receiving a diagnosis, findings support hope, particularly parental hope as a potential protective factor in lessening psychological distress (Lord et al., 2008; Mednick et al., 2007) applied particularly to an autism diagnostic scenario. This aligns with parents expressing the need for support surrounding diagnostic processes and perceived perceptions of social support (Reiff et al., 2017; Rabba et al., 2019, Hotez, 2016). Therefore, parent support and interventions that foster hope in parents’ ability to support their child’s needs may play an important role in parental wellbeing.
4.2 Limitations and future directions
While this research positions the role of hope as a potential mechanism explaining some of the relationships between resolution and parental stress, this study was cross-sectional, thus causal conclusions cannot be made. Future studies may consider longitudinal approaches to resolution research to support the role hope plays in resolution. This study finds preliminary evidence suggesting that parental hope has a greater effect on resolution and stress than hope for the child, however, larger more expansive studies would allow for greater exploration of these variables.
Unlike previous studies (Chamak et al., 2011), this study did not find time since diagnosis to be a factor associated with resolution; however, cohort studies may further explore this inconsistency and determine whether the time since diagnosis is potentially causally linked to resolution (Song and Chung, 2010), as longitudinal studies will be better suited to measuring resolution at different stages of the process. Furthermore, we did not account for participants’ experience of the diagnostic process impacting resolution (Abbott et al., 2013). Given that experiences with professionals who take strength-based approaches are associated with better experiences of the diagnostic process (Anderberg and South, 2021), and can have implications for the recipient of that diagnosis (Bury et al., 2022), the nature of the diagnosis could not only have an impact on resolution, but potentially also parental and child hope that feature strength-based concepts.
4.3 Conclusion
Our findings provide preliminary evidence that parental hope, which is an important factor arising from resolution, may buffer parents against the effect of parental stress. Given this, hope is focused on practical aspects of parents’ beliefs—specifically their ability to meet their child’s needs. Supporting parents in developing a realistic, strength-based understanding of these needs could be important during the diagnostic process.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
This research was approved by La Trobe University Human Research Ethics Committee. The studies were conducted in accordance with the local legislation and institutional requirements. Participants provided informed consent by clicking ‘agree’ after reading study and consent information.
Author contributions
VN: Conceptualization, Formal analysis, Methodology, Writing – original draft, Writing – review & editing, Data curation, Project administration. DH: Conceptualization, Writing – review & editing, Supervision. SB: Supervision, Writing – review & editing, Conceptualization, Formal analysis, Methodology, Project administration, Writing – original draft.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This research was supported by the kind support from La Trobe University, and $1000 student funding from the School of Psychology and Public Health.
Acknowledgments
The authors acknowledge the time and commitment of the parents in our study. The authors also acknowledge Professors Michael Wenzel and Emma Thomas for their support in reviewing and generating hope items.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2024.1443707/full#supplementary-material
Footnotes
1. ^Parental hope was included as it is more frequently cited as a source of hope for parents of autistic children, and it had greater practical outcomes. Running the model separately with societal and parental hope as the sole mediatior (Hayes, 2018) showed both as significant mediators of resolution and parental stress (see Supplementary materials).
References
Abbott, M., Bernard, P., and Forge, J. (2013). Communicating a diagnosis of autism Spectrum disorder-a qualitative study of parents’ experiences. Clin. Child Psychol. Psychiatry 18, 370–382. doi: 10.1177/1359104512455813
Allen, J. P., Hauser, S. T., and Borman-Spurrell, E. (1996). Attachment theory as a framework for understanding sequelae of severe adolescent psychopathology: an 11-year follow-up study. J. Consult. Clin. Psychol. 64, 254–263. doi: 10.1037/0022-006x.64.2.254
Al-Oran, H., and Al-Sagarat, A. (2016). Parenting stress of children with autistic disorder. Open Access Lib. J. 3, 1–10. doi: 10.4236/oalib.1102791
Alsayyari, H.I. (2018), Perceptions of Arab American mothers of children with autism Spectrum disorder an exploratory study. University of South Florida, Available at: http://ez.library.latrobe.edu.au/login?url=https://www.proquest.com/dissertations-theses/perceptions-arab-american-mothers-children-with/docview/2027299308/se-2.
American Psychiatric Association (2013). Diagnostic and statistical manual of mental disorders (DSM-5®). Arlington, VA: American Psychiatric Pub.
Anderberg, E., and South, M. (2021). Predicting parent reactions at diagnostic disclosure sessions for autism. J. Autism Dev. Disord. 51, 3533–3546. doi: 10.1007/s10803-020-04817-5
Benderix, Y., Nordström, B., and Sivberg, B. (2006). Parents’ experience of having a child with autism and learning disabilities living in a group home: a case study. Autism 10, 629–641. doi: 10.1177/1362361307070902
Berry, J. O., and Jones, W. H. (1995). The parental stress scale: initial psychometric evidence. J. Soc. Pers. Relat. 12, 463–472. doi: 10.1177/0265407595123009
Blake, F. E., (2021). Stress and depression levels of fathers parenting a child with autism Spectrum disorder (Doctoral dissertation, Northcentral University). Available at: http://ez.library.latrobe.edu.au/login?url=https://www.proquest.com/dissertations-theses/stress-depression-levels-fathers-parenting-child/docview/2529267766/se-2
Bonis, S. (2016). Stress and parents of children with autism: a review of literature. Issues Ment. Health Nurs. 37, 153–163. doi: 10.3109/01612840.2015.1116030
Brown, M., Marsh, L., and McCann, E. (2021). Experiences of fathers regarding the diagnosis of their child with autism spectrum disorder: a narrative review of the international research. J. Clin. Nurs. 30, 2758–2768. doi: 10.1111/jocn.15781
Bruininks, P., and Malle, B. F. (2005). Distinguishing hope from optimism and related affective states. Motivation and emotion, 29, 324–352. doi: 10.1007/s11031-006-9010-4
Bury, S. M., Haschek, A., Wenzel, M., Spoor, J. R., and Hedley, D. (2022). Brief report: learning about autism: is the source of autism knowledge associated with differences in autism knowledge, autism identity, and experiences of stigma. J. Autism Dev. Disord. 1-8. doi: 10.1007/s10803-022-05823-5
Bury, S. M., Wenzel, M., and Woodyatt, L. (2016). Giving Hope a sporting chance: Hope as distinct from optimism when events are possible but not probable. Motiv. Emot. 40, 588–601. doi: 10.1007/s11031-016-9560-z
Bury, S. M., Wenzel, M., and Woodyatt, L. (2019). Confusing hope and optimism when prospects are good: a matter of language pragmatics or conceptual equivalence? Motiv. Emot. 43, 483–492. doi: 10.1007/s11031-018-9746-7
Bury, S. M., Wenzel, M., and Woodyatt, L. (2020). Against the odds: Hope as an antecedent of support for climate change action. Br. J. Soc. Psychol. 59, 289–310. doi: 10.1111/bjso.12343
Chamak, B., Bonniau, B., Oudaya, L., and Ehrenberg, A. (2011). The autism diagnostic experiences of French parents. Autism 15, 83–97. doi: 10.1177/1362361309354756
Da Paz, N. S., Siegel, B., Coccia, M. A., and Epel, E. S. (2018). Acceptance or despair? Maternal adjustment to having a child diagnosed with autism. J. Autism Dev. Disord. 48, 1971–1981. doi: 10.1007/s10803-017-3450-4
Dabrowska, A., and Pisula, E. (2010). Parenting stress and coping styles in mothers and fathers of pre-school children with autism and down syndrome. J. Intellect. Disabil. Res. 54, 266–280. doi: 10.1111/j.1365-2788.2010.01258.x
Dolev, S., Sher-Censor, E., Baransi, N., Amara, K., and Said, M. (2016). Resolution of the child’s ASD diagnosis among Arab–Israeli mothers: associations with maternal sensitivity and wellbeing. Res. Autism Spectr. Disord. 21, 73–83. doi: 10.1016/j.rasd.2015.09.004
Ekas, N. V., Pruitt, M. M., and McKay, E. (2016). Hope, social relations, and depressive symptoms in mothers of children with autism spectrum disorder. Res. Autism Spectr. Disord. 29-30, 8–18. doi: 10.1016/j.rasd.2016.05.006
Eshraghi, A. A., Cavalcante, L., Furar, E., Alessandri, M., Eshraghi, R. S., Armstrong, F. D., et al. (2022). Implications of parental stress on worsening of behavioral problems in children with autism during COVID-19 pandemic:“the spillover hypothesis”. Mol. Psychiatry 27, 1869–1870. doi: 10.1038/s41380-021-01433-2
Estes, A., Munson, J., Dawson, G., Koehler, E., Zhou, X. H., and Abbott, R. (2009). Parenting stress and psychological functioning among mothers of preschool children with autism and developmental delay. Autism 13, 375–387. doi: 10.1177/1362361309105658
Ferguson, A., and Vigil, D. C. (2019). A comparison of the ASD experience of low-SES Hispanic and non-Hispanic white parents. Autism Res. 12, 1880–1890. doi: 10.1002/aur.2223
Gillespie-Lynch, K., Brooks, P. J., Someki, F., Obeid, R., Shane-Simpson, C., Kapp, S. K., et al. (2015). Changing college students’ conceptions of autism: an online training to increase knowledge and decrease stigma. J. Autism Dev. Disord. 45, 2553–2566. doi: 10.1007/s10803-015-2422-9
Harris, P. A., Taylor, R., Minor, B. L., Elliott, V., Fernandez, M., O'Neal, L., et al. (2019). The REDCap consortium: building an international community of software platform partners. J. Biomed. Inform. 95:103208. doi: 10.1016/j.jbi.2019.103208
Hayes, A. F. (2018). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. New York: Guilford Publications.
Hayes, S. A., and Watson, S. L. (2013). The impact of parenting stress: a meta-analysis of studies comparing the experience of parenting stress in parents of children with and without autism spectrum disorder. J. Autism Dev. Disord. 43, 629–642. doi: 10.1007/s10803-012-1604-y
Heredia-Alvarado, K., (2017). A mother's narrative: experience as a Latino mother with a child diagnosed with autism spectrum disorder. Alliant International University. Available at: http://ez.library.latrobe.edu.au/login?url=https://www.proquest.com/dissertations-theses/mothers-narrative-experience-as-latino-mother/docview/1909311393/se-2.
Hotez, E. (2016). A developmental perspective on parental cognitions and emotions in the context of a parent-mediated intervention for children with ASD : City University of New York.
Krakovich, T. M., McGrew, J. H., Yu, Y., and Ruble, L. A. (2016). Stress in parents of children with autism spectrum disorder: an exploration of demands and resources. J. Autism Dev. Disord. 46, 2042–2053. doi: 10.1007/s10803-016-2728-2
Lord, B., Ungerer, J., and Wastell, C. (2008). Implications of resolving the diagnosis of PKU for parents and children. J. Pediatr. Psychol. 33, 855–866. doi: 10.1093/jpepsy/jsn020
Louie, A. D., Cromer, L. D., and Berry, J. O. (2017). Assessing parenting stress: review of the use and interpretation of the parental stress scale. Fam. J. 25, 359–367. doi: 10.1177/1066480717731347
Marvin, R. S., and Pianta, R. C. (1996). Mothers' reactions to their child's diagnosis: relations with security of attachment. J. Clin. Child Psychol. 25, 436–445. doi: 10.1207/s15374424jccp2504_8
McPhilemy, C., and Dillenburger, K. (2013). Parents' experiences of applied behaviour analysis (ABA)-based interventions for children diagnosed with autistic spectrum disorder. Br. J. Spec. Educ. 40, 154–161. doi: 10.1111/1467-8578.12038
Mednick, L., Cogen, F., Henderson, C., Rohrbeck, C. A., Kitessa, D., and Streisand, R. (2007). Hope more, worry less: Hope as a potential resilience factor in mothers of very young children with type 1 diabetes. Child. Healthcare 36, 385–396. doi: 10.1080/02739610701601403
Miceli, M., and Castelfranchi, C. (2010). Hope: the power of wish and possibility. Theory Psychol. 20, 251–276. doi: 10.1177/0959354309354393
Milshtein, S., Yirmiya, N., Oppenheim, D., Koren-Karie, N., and Levi, S. (2010). Resolution of the diagnosis among parents of children with autism spectrum disorder: associations with child and parent characteristics. J. Autism Dev. Disord. 40, 89–99. doi: 10.1007/s10803-009-0837-x
Moh, T. A., and Magiati, I. (2012). Factors associated with parental stress and satisfaction during the process of diagnosis of children with autism spectrum disorders. Res. Autism Spectr. Disord. 6, 293–303. doi: 10.1016/j.rasd.2011.05.011
Mulligan, J., MacCulloch, R., Good, B., and Nicholas, D. B. (2012). Transparency, hope, and empowerment: a model for partnering with parents of a child with autism spectrum disorder at diagnosis and beyond. Soc. Work. Ment. Health 10, 311–330. doi: 10.1080/15332985.2012.664487
Naicker, V. V., Bury, S. M., and Hedley, D. (2023). Factors associated with parental resolution of a child's autism diagnosis: a systematic review. Front. Psych. 13:1079371. doi: 10.3389/fpsyt.2022.1079371
Nissenbaum, M. S., Tollefson, N., and Reese, R. M. (2002). The interpretative conference: sharing a diagnosis of autism with families. Focus Autism Other Dev. Disabil. 17, 30–43. doi: 10.1177/108835760201700103
Ogston, P. L., Mackintosh, V. H., and Myers, B. J. (2011). Hope and worry in mothers of children with an autism spectrum disorder or down syndrome. Res. Autism Spectr. Disord. 5, 1378–1384. doi: 10.1016/j.rasd.2011.01.020
Okoye, C., Obialo-Ibeawuchi, C. M., Obajeun, O. A., Sarwar, S., Tawfik, C., Waleed, M. S., et al. (2023). Early diagnosis of autism spectrum disorder: a review and analysis of the risks and benefits. Cureus 15:e43226. doi: 10.7759/cureus.43226
Ong, A. D., Edwards, L. M., and Bergeman, C. S. (2006). Hope as a source of resilience in later adulthood. Personal. Individ. Differ. 41, 1263–1273. doi: 10.1016/j.paid.2006.03.028
Oppenheim, D., Koren-Karie, N., Dolev, S., and Yirmiya, N. (2009). Maternal insightfulness and resolution of the diagnosis are associated with secure attachment in preschoolers with autism spectrum disorders. Child Dev. 80, 519–527. doi: 10.1111/j.1467-8624.2009.01276.x
Pastor-Cerezuela, G., Fernández-Andrés, M. I., Tárraga-Mínguez, R., and Navarro-Peña, J. M. (2016). Parental stress and ASD: relationship with autism symptom severity, IQ, and resilience. Focus Autism Other Dev. Disabil. 31, 300–311. doi: 10.1177/1088357615583471
Popp, J. M., Conway, M., and Pantaleao, A. (2015). Parents’ experience with their child’s cancer diagnosis: do hopefulness, family functioning, and perceptions of care matter? J. Pediatr. Oncol. Nurs. 32, 253–260. doi: 10.1177/1043454214563404
Poslawsky, I. E., Naber, F. B., Van Daalen, E., and Van Engeland, H. (2014). Parental reaction to early diagnosis of their children’s autism spectrum disorder: an exploratory study. Child Psychiatry Hum. Dev. 45, 294–305. doi: 10.1007/s10578-013-0400-z
Rabba, A. S., Dissanayake, C., and Barbaro, J. (2019). Parents’ experiences of an early autism diagnosis: insights into their needs. Res. Autism Spectr. Disord. 66:101415. doi: 10.1016/j.rasd.2019.101415
Rabbitte, K., Prendeville, P., and Kinsella, W. (2017). Parents’ experiences of the diagnostic process for girls with autism spectrum disorder in Ireland: an interpretative phenomenological analysis. Educ. Child Psychol. 34, 54–66. doi: 10.53841/bpsecp.2017.34.2.54
Reiff, M., Bugos, E., Giarelli, E., Bernhardt, B. A., Spinner, N. B., Sankar, P. L., et al. (2017). “Set in stone” or “ray of hope”: parents’ beliefs about cause and prognosis after genomic testing of children diagnosed with ASD. J. Autism Dev. Disord. 47, 1453–1463. doi: 10.1007/s10803-017-3067-7
Sanders-Dewey, N. E., Mullins, L. L., and Chaney, J. M. (2001). Coping style, perceived uncertainty in illness, and distress in individuals with Parkinson's disease and their caregivers. Rehabil. Psychol. 46, 363–381. doi: 10.1037/0090-5550.46.4.363
Schieve, L. A., Blumberg, S. J., Rice, C., Visser, S. N., and Boyle, C. (2007). The relationship between autism and parenting stress. Pediatrics 119, S114–S121. doi: 10.1542/peds.2006-2089Q
Sheeran, T., Marvin, R. S., and Pianta, R. (1997). Mothers' resolution of their childs's diagnosis and self-reported measures of parenting stress, marital relations, and social support. J. Pediatr. Psychol. 22, 197–212. doi: 10.1093/jpepsy/22.2.197
Sher-Censor, E., Dan Ram-On, T., Rudstein-Sabbag, L., Watemberg, M., and Oppenheim, D. (2020). The reaction to diagnosis questionnaire: a preliminary validation of a new self-report measure to assess parents’ resolution of their child’s diagnosis. Attach Hum. Dev. 22, 409–424. doi: 10.1080/14616734.2019.1628081
Sher-Censor, E., Dolev, S., Said, M., Baransi, N., and Amara, K. (2017). Coherence of representations regarding the child, resolution of the child’s diagnosis and emotional availability: a study of Arab-Israeli mothers of children with ASD. J. Autism Dev. Disord. 47, 3139–3149. doi: 10.1007/s10803-017-3228-8
Sher-Censor, E., and Shahar-Lahav, R. (2022). Parents’ resolution of their child’s diagnosis: a scoping review. Attach Hum. Dev. 24, 580–604. doi: 10.1080/14616734.2022.2034899
Singh, J. S. (2016). Parenting work and autism trajectories of care. Sociol. Health Illn. 38, 1106–1120. doi: 10.1111/1467-9566.12437
Smith, T. B., Oliver, M. N., and Innocenti, M. S. (2001). Parenting stress in families of children with disabilities. Am. J. Orthopsychiatry 71, 257–261. doi: 10.1037/0002-9432.71.2.257
Snyder, C. R., Harris, C., Anderson, J. R., Holleran, S. A., Irving, L. M., Sigmon, S. T., et al. (1991). The will and the ways: development and validation of an individual-differences measure of hope. J. Pers. Soc. Psychol. 60, 570–585. doi: 10.1037/0022-3514.60.4.570
Song, J. W., and Chung, K. C. (2010). Observational studies: cohort and case-control studies. Plast. Reconstr. Surg. 126, 2234–2242. doi: 10.1097/prs.0b013e3181f44abc
Wenzel, M., Anvari, F., de Vel-Palumbo, M., and Bury, S. M. (2017). Collective apology, hope, and forgiveness. J. Exp. Soc. Psychol. 72, 75–87. doi: 10.1016/j.jesp.2017.05.003
Keywords: resolution, autism spectrum disorder, diagnosis, hope, parent–child relationship, parental wellbeing, acceptance
Citation: Naicker VV, Hedley D and Bury SM (2024) Does hope mediate the relationship between parent’s resolution of their child’s autism diagnosis and parental stress. Front. Psychol. 15:1443707. doi: 10.3389/fpsyg.2024.1443707
Edited by:
Uri Yatzkar, Ziv Medical Center, IsraelCopyright © 2024 Naicker, Hedley and Bury. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Simon M. Bury, cy5idXJ5QGxhdHJvYmUuZWR1LmF1