 Chantale Simard1,2,3*
Chantale Simard1,2,3* Véronique Roberge1,2,3Maxime St-Pierre1Jacques Cherblanc2,3,4Christiane Bergeron-Leclerc2,4Mohamed Abdelhafid Kadri1Carl Lacharité5Samuel Bérubé1Laurie Lapointe1Valérie Faucher6
Véronique Roberge1,2,3Maxime St-Pierre1Jacques Cherblanc2,3,4Christiane Bergeron-Leclerc2,4Mohamed Abdelhafid Kadri1Carl Lacharité5Samuel Bérubé1Laurie Lapointe1Valérie Faucher6 Sebastien S. Dufresne1,2,3
Sebastien S. Dufresne1,2,3- 1Département des sciences de la santé, Université du Québec à Chicoutimi (UQAC), Saguenay, QC, Canada
- 2Centre Intersectoriel en Santé Durable (CISD), Université du Québec à Chicoutimi (UQAC), Saguenay, QC, Canada
- 3Réseau Québécois de Recherche en Soins Palliatifs et de Fin de Vie, Québec, QC, Canada
- 4Département des sciences humaines, Université du Québec à Chicoutimi (UQAC), Saguenay, QC, Canada
- 5Département de psychologie, Université du Québec à Trois-Rivières (UQTR), Trois-Rivières, QC, Canada
- 6Département de cancérologie, soins palliatifs et de fin de vie, Centre Intégré Universitaire de Santé et de Services Sociaux du Saguenay-Lac-St-Jean (CIUSSS SLSJ), Chicoutimi, QC, Canada
Background: Advances in pediatric oncology have significantly increased survival rates, yet have introduced challenges in managing long-term treatment side effects. This study process introduces an interdisciplinary clinical intervention program rooted in the family resilience framework, aimed at improving well-being across the cancer trajectory for children and their families, especially those in Canadian communities far from specialized oncology centers with limited access to resources.
Methods: Employing an intervention mapping approach, this program collaboratively involves patients, families, professionals, and researchers. It aims to identify vulnerability factors, establish a logic model of change, and devise comprehensive strategies that include professional interventions alongside self-management tools. These strategies, tailored to address biopsychosocial and spiritual challenges, are adapted to the unique contexts of communities distant from specialized cancer treatment centers. A mixed-methods approach will evaluate program effectiveness.
Expected results: Anticipated outcomes include the empowerment of families with self-management tools and professional support, designed to mitigate biopsychosocial and spiritual complications. By addressing the specific needs and limitations of these communities, the program strives to improve the overall health and well-being of both undergoing treatment and survivorship phases.
Discussion: By focusing on comprehensive care that includes both professional interventions and self-management, this initiative marks a significant shift toward a holistic, family-centered approach in pediatric oncology care for remote communities. It underlines the necessity of accessible interventions that confront immediate and long-term challenges, aiming to elevate the standard of care by emphasizing resilience, professional support, and family empowerment in underserved areas.
1 Introduction
In recent decades, significant progress in diagnostic tools and medical treatments has revolutionized pediatric oncology, resulting in a remarkable increase in survival rates for children facing cancer (Agence de la Santé Publique du Canada, 2024). Currently, the majority of these children will transition to adulthood. However, this progress is accompanied by long-term health challenges that affect both the survivors and their families. These adverse outcomes, influenced by diverse factors such as cancer subtypes, treatment protocols, and family dynamics, can arise during intensive therapy, persist long after treatment, or surface years later (Bhakta et al., 2017; Armstrong et al., 2014; Hudson et al., 2013; Bhakta et al., 2020; Robison and Hudson, 2014).
Estimates suggest that 60–90% of pediatric cancer survivors experience chronic health conditions (National Cancer Institute, 2024), including secondary cancers, cardiac toxicity, growth disorders, endocrinopathies, obesity, and cognitive dysfunctions (Tanner et al., 2020). These issues, coupled with psychosocial, financial, and spiritual challenges, often manifest in adulthood and are frequently overlooked in post-cancer care protocols. This situation is particularly dire in remote communities like Saguenay-Lac-Saint-Jean (Quebec, Canada), where families face the additional burden of limited local healthcare resources and lengthy commutes to specialized oncology centers, amplifying their vulnerability.
The rarity of pediatric cancer results in the necessary care and treatments being primarily concentrated in tertiary care hospitals located in urban areas (Scott-Findlay and Chalmers, 2001). Approximately one in five Canadians lives in a rural area (Statistique Canada, 2013), meaning that 20% of families with a child undergoing cancer treatment must endure prolonged separations from other family members, often lasting several weeks to months. Families living far from pediatric oncology centers face unique hardships, such as disrupted family dynamics, increased financial burden, emotional stress, and limited access to specialized care (Scott-Findlay and Chalmers, 2001; Walling et al., 2019). These families often have to manage secondary family arrangements, which can lead to significant strain (McCubbin et al., 2002). The physical impact of having to stay close to the sick child in unfamiliar environments, such as temporary accommodations, can disrupt normal sleep and eating patterns and exacerbate the side effects of cancer treatments due to long travel distances (Daniel et al., 2013). Psychologically, concerns about travel conditions, access to specialized care, and the roles of caregiving increase anxiety and stress (Walling et al., 2019; Aitken and Hathaway, 1993). The relational aspect is also strained, with families often finding it difficult to maintain social contacts and marital relationships due to long separations and the pressure of medical appointments (Scott-Findlay and Chalmers, 2001). Financially, the costs associated with travel, accommodation, and lost wages add to the burden, making it imperative for interventions to consider these multifaceted challenges (Walling et al., 2019; Daniel et al., 2013; Fluchel et al., 2014).
Addressing these health challenges is a major concern for healthcare professionals. The World Health Organization (WHO) has emphasized the importance of these outcomes, advocating for interventions that bridge gaps in childhood cancer research and care (Organisation Mondiale de la Santé, 2021). This has led to the adoption of holistic strategies focused on identifying, preventing, and mitigating the long-term impacts of cancer (Paul et al., 2024). Multidisciplinary and family-centric approaches during cancer care experience are crucial, as environmental factors play a significant role in preventing developmental issues and disabilities (Corrigan and Feig, 2004; Khan et al., 2022; Wiener et al., 2015). The diagnosis of cancer significantly impacts family dynamics, necessitating resilience to adapt and cope with adversity (Rosenberg et al., 2014; Van Shoors et al., 2015; Rosenberg et al., 2018; Rosenberg et al., 2019).
In this context, resilience emerges as a critical construct; it’s the process that refers to the “capacities in family functioning to withstand and rebound from adversity. More than surviving loss and coping with disruptions, resilience involves positive adaptation: regaining the ability to thrive, with the potential for transformation and positive growth forged through the searing experience” (Walsh, 2016a, p. 904). Walsh’s theoretical framework of family resilience provides valuable insights into how families navigate and recover from crises, highlighting belief systems, organizational patterns, and communication processes as key domains of family functioning. This framework offers a therapeutic approach for professionals aiming to strengthen family resilience. Despite the proven benefits of family resilience, there is a notable lack of research on its application in developing interdisciplinary intervention programs for pediatric cancer patients. This paper outlines the protocol for creating an interdisciplinary clinical intervention program (The Program), rooted in the family resilience framework, specifically tailored to address the risk factors contributing to the vulnerability of families in the Saguenay-Lac-Saint-Jean region.
2 Methods
2.1 Working groups
The development and refinement of The Program will heavily rely on collaboration with Working Groups (WGs) (Bartholomew et al., 2016). These groups will be composed of family members, health professionals, managers, and researchers. The WGs will play a crucial role in each of the six steps of the IM approach, ensuring that the intervention is grounded in practical insights and real-world experiences (Bartholomew et al., 2016).
WGs will be established, drawing members from the three primary participant pools. Each WG is set to comprise no more than nine individuals, ensuring focused, productive dialog. This composition will include seven healthcare professionals (spanning roles such as nurses, psychologists, social workers, physical therapists, pediatricians, spiritual care providers, and managers), one adult who was diagnosed with cancer during childhood, and one family member currently or previously involved in the pediatric cancer journey. This deliberate limitation on group size adheres to the insights of Johnson et al. (1993) and Hackman and Vidmar (1970), who underscored that smaller groups counteract the tendency toward passive involvement—a common pitfall in larger settings. By keeping groups more intimate, we aim to foster an environment conducive to active participation, meaningful exchange, and a deeper, more nuanced exploration of experiences and perspectives.
The initial step of this research endeavor necessitates at least four WG sessions. Each of these crucial meetings will be facilitated by one or more of the project’s dedicated team members. At the commencement of every session, assurances will be provided regarding the strict confidentiality of the data shared and the handling of any other potential ethical considerations. Participants will be informed that all perspectives are valuable, reinforcing that there are no “right” or “wrong” contributions.
Each meeting will conclude with reminders about confidentiality and expressions of gratitude for the participants’ invaluable contributions. Following the acquisition of written consent from the participants, all WG sessions will be audio-recorded. This ensures that detailed information shared during discussions is accessible for precise reference and analysis by the research team.
To comprehensively characterize the participant sample, socio-demographic data will be compiled through self-administered forms at the beginning of the inaugural WG session.
2.2 Intervention mapping approach
The intervention development process is structured according to the Intervention Mapping (IM) approach, which is divided into six key steps. Each step is meticulously designed to ensure a comprehensive and systematic progression from problem identification to program evaluation. The IM approach is inherently collaborative, involving patients, families, professionals, and researchers. It encourages the use of theoretical frameworks to address the multiple dimensions linked to the complex nature of health experiences. The process incorporates data from research, theory, and the experiences and opinions of those directly affected, ensuring a holistic and inclusive approach.
Table 1 provides an overview of each step, including the description, key activities, and expected outcomes. The first column, Step, enumerates the sequential steps in the IM process, from the identification of the problem to the evaluation of the program. The second column, Description, provides a brief explanation of each step, outlining its primary focus and objectives. The third column, Key Activities, details the specific actions and methods employed during each step, highlighting the practical and theoretical approaches used to achieve the objectives. Finally, the fourth column, Outcomes, lists the expected results of each step, illustrating how each phase contributes to the overall goal of developing a robust and effective intervention program. This structured approach ensures a clear, logical progression through the stages of intervention development, providing a solid foundation for creating a tailored, evidence-based program that addresses the unique needs of children with cancer and their families in the Saguenay-Lac-Saint-Jean region.
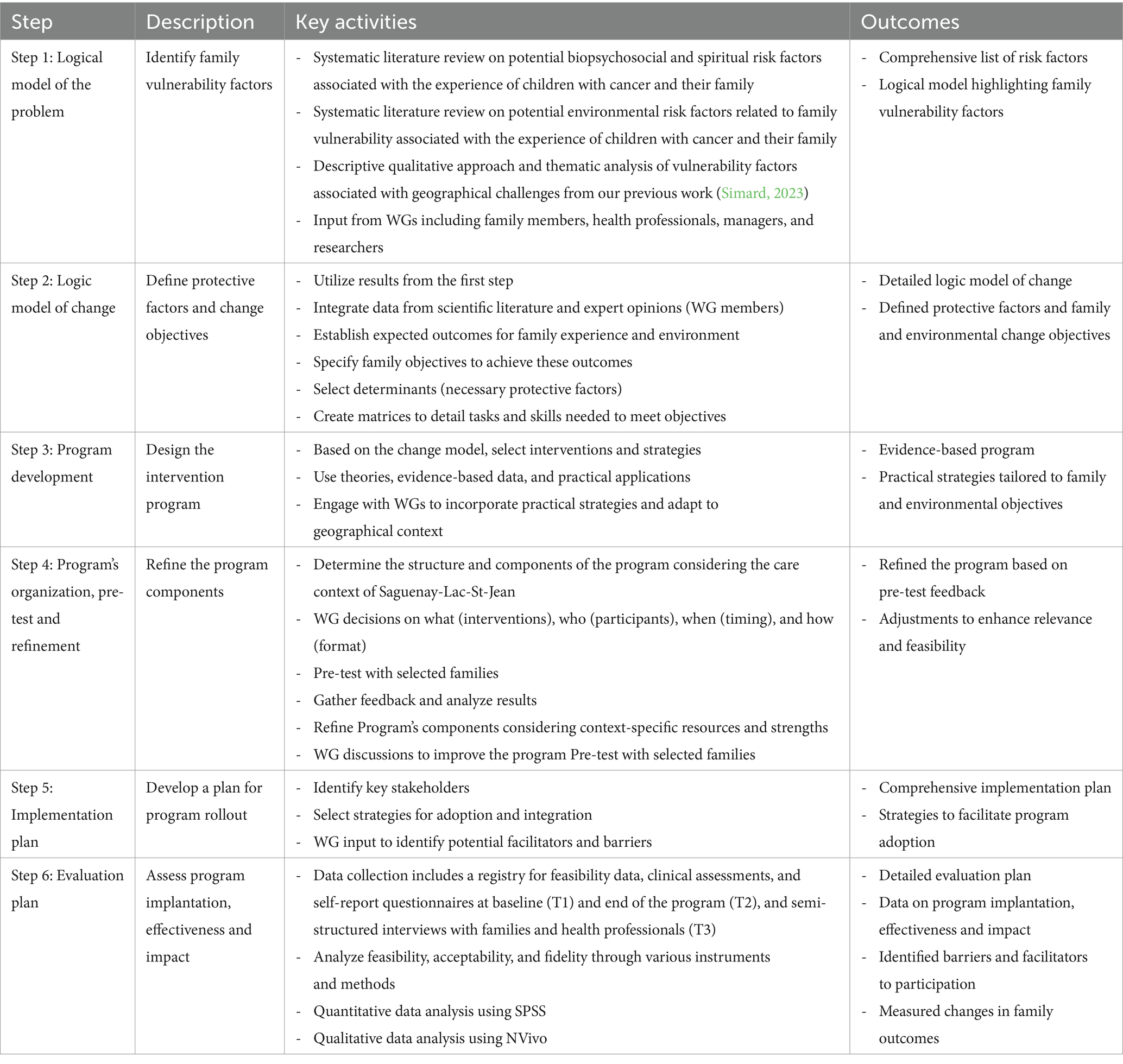
Table 1. Overview of the intervention mapping process steps, descriptions, key activities, and expected outcomes.
2.2.1 Step 1: logical model of the problem: vulnerability in pediatric cancer during treatment and survivorship
The first step in the IM approach involves comprehensively identifying vulnerability factors that contribute to poor outcomes for children with cancer and their families. This step is foundational for tailoring the intervention effectively. Initially, a systematic literature review will identify potential biopsychosocial, spiritual, and environmental risk factors associated with the experiences of these children and their families. Databases such as PubMed, CINAHL, PEDro, and Embase will be used, with the search strategy being carried out by the researchers in the working group.
Our previous study, which employed a descriptive qualitative approach and thematic analysis, identified vulnerability factors linked to geographical challenges (Simard, 2023). This previous work provides essential insights, particularly for understanding the specific impacts of geographic isolation on families in remote areas like Saguenay-Lac-Saint-Jean. We will gather input from WGs that include family members, health professionals, managers, and researchers. These consultations are crucial for capturing diverse perspectives and addressing the multifaceted challenges these families face.
The logical modeling of the problem is informed by the PRECEDE model (Bartholomew et al., 2016), requiring an ecological analysis of the causes, including both risk behaviors and environmental conditions. This approach helps us relate scientific literature findings to those identified in our previous study on the specific impacts of geographic isolation on families dealing with pediatric cancer. Using theoretical frameworks centered on family resilience (Walsh, 2016b) and strengths (Gottlieb, 2013), we analyze the problem further. We establish that insufficient mobilization of family resources and competencies (protective factors) can render families vulnerable, compromising their well-being. Vulnerability occurs when a traumatic family experience (TFE) presents more risk factors than protective factors available to counter them (Walsh, 2016a; Delage, 2008).
The logical model details risk factors from both the child and the family’s experience and their immediate environment, including healthcare, services, and social networks. These risk factors are sub-categorized according to Walsh’s domains of family functioning: communication processes, organizational patterns, and belief systems. This comprehensive model highlights the biopsychosocial, spiritual, and environmental risk factors affecting children with cancer and their families, forming the foundation for subsequent IM steps. Integrating these elements ensures the intervention is both evidence-based and contextually relevant, enhancing its effectiveness (Bartholomew et al., 2016; Bartholomew and Mullen, 2011).
2.2.2 Step 2: logic model of change: prevention and management of health complications during cancer treatment and survivorship
The second step in the IM approach will involve creating a logic model of change to strengthen the resilience of families accompanying children with cancer. This step, as described by Bartholomew et al. (2016), will determine “what the health promotion program is intended to accomplish” (p. 286). After identifying the risk factors causing family problems in the first step, this second step will map out the desired change process for the intervention program.
This phase will be conducted inductively through the second meeting with the WGs. The process will be divided into several key activities. Initially, we will define the expected outcomes concerning the family experience and environment, aiming to enhance the overall well-being of children with cancer and their families by addressing specific biopsychosocial and spiritual challenges. Following this, we will set specific family objectives to achieve these desired outcomes, focusing on improving family resilience, coping strategies, and support systems.
Next, we will identify the necessary protective factors or strengths that will enable families to achieve their objectives, such as emotional support, effective communication, and robust social networks. To operationalize these objectives, detailed matrices will be created to outline the specific actions, strategies, and competencies required to achieve the family and environmental goals (Bartholomew et al., 2016). These matrices will provide a clear roadmap for implementing the intervention, specifying the tasks and skills needed to strengthen family resilience.
The protective factors identified in our previous study on the impact of geographical isolation (Simard, 2023) will be crucial. These factors, integrated with empirical and theoretical data and insights from the WGs, will inform the development of two primary matrices (Bartholomew and Mullen, 2011). The first matrix will focus on the expected family protective factors, while the second will address the family environment, including healthcare, services, and social networks. Both matrices will aim to enhance the resilience of families accompanying children with cancer by detailing specific objectives, actions, strategies, and skills necessary for achieving the desired outcomes.
By following these sub-steps, we will create a comprehensive logic model of change, which will provide a structured and evidence-based framework for the intervention (Bartholomew et al., 2016). This model will ensure that the program is designed to effectively support families, leveraging their strengths and addressing their vulnerabilities to improve their overall well-being and resilience. This methodical approach will not only define the intervention’s objectives but also outline the practical steps needed to achieve them, ensuring that the program is both theoretically sound and practically applicable (Bartholomew et al., 2016; Bartholomew and Mullen, 2011).
2.2.3 Step 3: development of an interdisciplinary intervention program for children with cancer in a real-care setting
The third step will involve developing the logic model of the intervention program (The Program) (Bartholomew et al., 2016). This phase will be conducted during the third session with the WGs. This step requires analyzing and targeting the most effective empirical data, theoretical insights, and exemplary interdisciplinary practices available. It will also involve considering interdisciplinary and family interventions already implemented or suggested by all health professionals and participating family members. Additionally, a systematic literature review will be conducted to identify the best evidence-based interventions, with the search strategy being carried out by the researchers in the working group.
The goal of this step is to identify interventions that best achieve the family and environmental objectives set in the previous step. The Program will aim to prevent child and family vulnerability and optimize their well-being and quality of life. The change supported by The Program is primarily driven by strengthening family resilience, as proposed in the Family Resilience Framework (Walsh, 2016b) and by adopting a strength-based care approach centered on the child and family (Gottlieb, 2013; Gottlieb and Gottlieb, 2017).
During this phase, a summary table will be created. For each family and environmental objective identified in the second step, the table will present more specific goals to facilitate their achievement and associate each with potential interdisciplinary interventions. Given that a single intervention can address multiple objectives simultaneously, some interdisciplinary interventions will be linked to several objectives.
To ensure the interventions are comprehensive and effective, we will incorporate insights from exemplary practices, empirical research, and theoretical frameworks (Bartholomew et al., 2016). This approach will ensure that The Program is not only theoretically sound but also practically applicable, addressing the specific needs and vulnerabilities of families accompanying children with cancer.
By following these sub-steps, we will develop a detailed and actionable intervention program designed to strengthen family resilience and improve the overall well-being and quality of life for these families. This methodical approach will ensure that the program is both evidence-based and contextually relevant, providing a robust foundation for the subsequent steps in the IM process.
2.2.4 Step 4: creation of the interdisciplinary intervention program for children with cancer in real-care contexts, anchored in the family resilience framework
The fourth step will involve pre-testing and refining the structure and components of The Program (Bartholomew et al., 2016). This phase will be conducted during the final session with the WGs. The goal is to determine the what (e.g., relevant and realistic interdisciplinary interventions to achieve the set objectives), who (e.g., children and families undergoing the accompaniment experience, health professionals, managers, and researchers), when (e.g., timing, frequency, duration of each intervention), and how (e.g., format, components, steps, activities) of The Program.
During this step, we will utilize a summary table to guide the discussions. The WGs will identify and define the interventions required to meet the family and environmental objectives established in the previous steps. This will include determining specific actions, strategies, and competencies needed for each objective.
To ensure that the intervention is appropriately tailored to the varying levels of family vulnerability, we will introduce a stratification of intervention intensity. This stratification will range from self-management support to a comprehensive interdisciplinary intervention plan. The method and tool for stratification will be determined by the team, selecting from existing tools such as the Psychosocial Assessment Tool (PAT) (Pai et al., 2008; Kazak et al., 2015). This approach allows the intensity of the intervention to be adapted to the level of vulnerability and specific needs of each family.
The Program will include a variety of strategies or tools designed to achieve the family and environmental objectives identified. These strategies will be categorized according to three major areas of interdisciplinary activity. The first category will focus on the training and clinical support of health professionals regarding pediatric oncology, including initiatives such as training programs, mentorship, and ongoing education. The second category will be oriented toward care management, incorporating strategies like grouping families with similar experiences, ensuring continuity of care by dedicated staff, and providing materials similar to those used in specialized oncology centers. The third category will relate to practice, involving tools and resources such as family guides, follow-up sheets, tools for assessing psychosocial needs, and summaries of child and family records.
By refining The Program through this structured approach, we will ensure that the intervention is comprehensive, evidence-based, and contextually relevant. This refinement process will involve careful consideration of the care context in the Saguenay-Lac-St-Jean (SLSJ) region, ensuring that the interventions are feasible and effective in real-world settings.
Ultimately, this methodical refinement will produce a detailed and actionable intervention program that is both theoretically sound and practically applicable (Bartholomew et al., 2016; Bartholomew and Mullen, 2011), tailored to the unique needs and vulnerabilities of families accompanying children with cancer.
2.2.5 Step 5: development of the program’s implementation plan
The fifth step will involve developing a comprehensive implementation plan for The Program. This phase will be conducted to ensure that the intervention is effectively integrated into the existing healthcare framework and is sustainable over time. The goal is to identify key stakeholders, select appropriate strategies for adoption and integration, and consider factors that could facilitate or hinder the implementation process (Bartholomew et al., 2016).
The WGs will select strategies for the adoption and integration of The Program. These strategies will be informed by insights gathered from the previous steps and will be tailored to fit the specific context of the Saguenay-Lac-Saint-Jean region. We will use the (CFIR) (Carrandi et al., 2024; Damschroder et al., 2009) to guide this process. The CFIR provides a comprehensive approach to assess multiple dimensions that affect implementation, including intervention characteristics, outer and inner setting, characteristics of the individuals involved, and the implementation process itself.
We will also consider potential facilitators and barriers to implementation (Bartholomew et al., 2016; Carrandi et al., 2024). Facilitators might include existing support systems, community engagement, and available resources, while barriers could involve resistance to change, limited resources, or logistical challenges (Bartholomew et al., 2016). By identifying these factors early, we can develop strategies to address them, such as training programs to build capacity, modifying workflows to accommodate new practices, or securing additional funding to support the intervention.
A detailed timeline and action plan will be created, outlining each step of the implementation process. This plan will include specific tasks, responsible parties, deadlines, and necessary resources. Regular progress reviews and adjustments will be made to ensure the implementation stays on track and can adapt to any unforeseen challenges.
To ensure the intervention is comprehensive and effective, we will evaluate key implementation outcomes, including:
• Intervention Characteristics: Assessing the quality, adaptability, and complexity of the intervention to ensure it meets the needs of the target population and can be effectively integrated into existing systems.
• Outer Setting: Evaluating external influences such as patient needs and resources, community support, and external policies or incentives that may impact the implementation process.
• Inner Setting: Examining internal organizational factors, including the culture, readiness for implementation, communication networks, and resources available within the healthcare settings where the intervention will be implemented.
• Characteristics of Individuals: Understanding the knowledge, beliefs, and attitudes of the individuals involved in the implementation process, including health professionals and families.
• Implementation Process: Monitoring the stages of implementation, including planning, engaging stakeholders, executing the intervention, and evaluating its progress and outcomes.
By developing a comprehensive implementation plan using the CFIR framework and evaluating these key implementation outcomes, we will ensure that The Program is effectively integrated into the healthcare system and is sustainable and scalable. This structured approach will enable us to systematically address any challenges and leverage facilitators to enhance the overall impact of the intervention, ultimately improving the well-being and resilience of families accompanying children with cancer.
2.2.6 Step 6: development of the program’s evaluation plan
The sixth step in the Intervention Mapping (IM) approach involves developing a comprehensive evaluation plan to assess the effectiveness and impact of The Program. This phase will ensure that the intervention achieves its intended outcomes and provides valuable insights for future improvements. The evaluation will focus on both process and outcome measures, employing a mixed-methods approach to capture quantitative and qualitative data.
Data collection in this specific step will include a variety of methods to ensure a comprehensive evaluation of The Program. These methods will encompass registries, clinical assessments, self-report questionnaires, and semi-structured interviews with participants and health professionals.
• Registry: An online registry will be used to record feasibility data, such as referral rates, eligibility rates, recruitment rates, time windows, and baseline assessment periods. Acceptability will be assessed by the Credibility Scale and the Treatment Perceptions Questionnaire (TPQ) (Sancassiani et al., 2021). TPQ will provide satisfaction information by collecting the level of agreement (5-point Likert scale, fully disagree to fully agree) regarding items measuring acceptability, suitability, tolerability, expectation of positive benefit, credibility, efficacy, appropriateness, reasonableness, justification, and discomfort.
• Clinical Assessments and Self-Report Questionnaires: Baseline (T1) and post-intervention (T2) clinical assessments and self-report questionnaires (Varni et al., 2007) will document family outcomes (based on step 4), including health-related quality of life, family functioning, anxiety, depression, and distress. These assessments will also evaluate the perceived security, confidence, and satisfaction with program components. Additionally, the number of objectives achieved relative to those set in the previous steps will be assessed. Medical records concerning administration of cancer treatment (baseline dose, dose reduction, delays or cancelation) data will be collected at T3 by using information tallied on the patient electronic medical record.
• Semi-Structured Interviews: At the end of the program (T3), semi-structured interviews will be conducted with participants and health professionals to gather in-depth qualitative data on the feasibility, fidelity, barriers, and facilitators of the intervention. Interviews will be transcribed and analyzed to identify common themes and insights.
By developing a thorough evaluation plan, we will ensure that The Program is systematically assessed for its effectiveness, feasibility, and sustainability (Bartholomew et al., 2016). This approach will provide robust evidence to support the intervention’s impact on the well-being and resilience of families accompanying children with cancer and inform future scaling and adaptation efforts.
Quantitative data will be analyzed using statistical software such as SPSS (IBM Corporation, 2017). Descriptive statistics (Tabachnick and Fidell, 2019) will summarize sociodemographic and clinical characteristics, feasibility indicators, and outcome measures. Comparative analyses (Field, 2017), such as paired t-tests or Wilcoxon signed-rank tests, will evaluate pre- and post-intervention changes. Effect sizes will be calculated to determine the magnitude of changes (Cohen, 1988). Qualitative data from interviews will be analyzed using inductive content analysis procedures (Miles et al., 2014). Themes and patterns will be identified independently by two researchers, and discrepancies will be resolved through discussion to create a common codebook. Data will be coded using software like NVivo to ensure systematic and rigorous analysis.
We will evaluate key implementation outcomes based on the CFIR, including intervention characteristics, outer setting, inner setting, characteristics of individuals, and the implementation process. These outcomes will help us understand the factors influencing the successful integration and sustainability of The Program.
The integration of quantitative and qualitative data will provide a comprehensive understanding of The Program’s effectiveness and impact. This mixed-methods approach will allow us to triangulate findings, identify discrepancies, and gain deeper insights into the intervention’s outcomes and implementation processes. Findings from the evaluation will be used to refine and improve The Program. Feedback loops will be established to ensure that insights from participants and stakeholders are incorporated into ongoing program development and enhancement.
2.3 Research participants
This research necessitates three distinct samples: the first comprising family members of children currently battling cancer or those who have previously faced the disease; the second consisting of adults who were diagnosed with cancer during their childhood; and the third incorporating professionals within the healthcare system who actively contribute to the care of these families. Participants from all categories will be selected using a purposive sampling strategy (Grove et al., 2013), striving for maximum variation (Creswell, 2013). This approach is underpinned by several foundational criteria: participants must (i) be at least 18 years of age, (ii) be French-speaking, (iii) reside in the Saguenay−Lac-Saint-Jean region, and (iv) possess the mental and physical capacity to engage fully in the research process. To promote equity, diversity, and inclusion, as desired in Canadian research, the selection criteria were chosen to avoid marginalizing or discriminating against individuals due to physical or mental health issues. Therefore, the decision to participate is left to the individual’s judgment based on their reality.
The constitution of each sample will be also based on specific inclusion criteria. For the family members sample—the criteria are: (i) being part of a family where a child is undergoing cancer treatment or has done so in the past, and (ii) being actively involved in supporting a child who is either currently receiving treatment or has concluded their treatment within the past 5 years.
For the adult survivors of pediatric cancer sample—the individuals must: (i) have received a cancer diagnosis during childhood, and (ii) be currently undergoing treatment or have completed it within the last 5 years.
Lastly, the healthcare professionals sample requires participants to: (i) be an integral part of a pediatric oncology care team, (ii) work directly with children affected by cancer and their families, and (iii) hold a professional role pertinent to the program under study.
This meticulous selection process ensures a comprehensive and empathetic understanding of the varied experiences and challenges faced by each distinct group, ultimately enriching the research outcomes and their potential applications.
2.4 Ethical considerations
Ethics approval for this study was obtained from the Centre intégré universitaire de santé et de services sociaux du Saguenay-Lac-Saint-Jean. This clinical study will be conducted in accordance with applicable Health Canada regulations, International Conference on Harmonization (ICH) guidelines on current Good Clinical Practice (GCP), and the Declaration of Helsinki. All participants will be given detailed oral and written information about the study. Consent forms describing the study procedures and risks in detail will be given to each participant and written documentation of informed consent will be required prior to starting study protocol.
In adherence to the best ethical practices for the preservation and archiving of research data, all research materials, including signed consent forms, completed questionnaires, and any other essential documents, will be meticulously stored in a secure, fire-resistant filing cabinet, located within a restricted-access office at UQAC. This office will be assigned to one of the lead researchers, thereby ensuring that only authorized personnel can access it, in order to maintain the confidentiality and integrity of the data.
Moreover, to prevent any form of data loss, and then compromise confidentiality, a digital copy of the documents will be created. These files will be encrypted and saved on a secure server at UQAC, with scheduled regular backups to ensure data preservation. These digital security measures are crucial in preventing data losses due to hardware failures, human errors, or natural disasters. The data retention period will be in compliance with ethical and regulatory standards, with a planned retention period of 5 years following the conclusion of the study. Beyond this period, all data will be securely destroyed to ensure that no sensitive or personal information can be retrieved subsequently. This destruction will be conducted under the supervision of an official, and a report confirming the secure destruction of data will be compiled and kept in the project’s archives. It’s also essential to specify that all procedures for data preservation, security, and destruction will be performed in strict compliance with privacy protection regulations and industry ethical guidelines, thereby ensuring the rights and confidentiality of research participants are respected at every stage of the process.
3 Discussion
This protocol is grounded in extensive scientific literature highlighting the multifaceted and challenging nature of the family experience in pediatric oncology. Families dealing with pediatric cancer face significant vulnerabilities and transformations, with these challenges exacerbated by geographic distance from tertiary care centers (Walling et al., 2019; Van Shoors et al., 2015; Wilson et al., 2016). Despite these unique challenges, the experience of families in remote areas remains underexplored, and the care and services provided to them are often inconsistent (Walling et al., 2019).
Parents of children with cancer are particularly vulnerable psychosocially, and those with fewer resources to support their resilience are even more at risk (Rosenberg et al., 2014). Many authors have emphasized the importance of supporting the resilience of these families (McCubbin et al., 2002; Van Shoors et al., 2015; Masera et al., 2013), yet there is a notable gap in the literature regarding interventions specifically designed for families living far from tertiary care centers. This protocol aims to address this gap by supporting the resilience process of these children and their families to prevent and mitigate the potential biopsychosocial and spiritual problems they may face.
As Koumarianou et al. highlight, “Psychosocial interventions in families of children with cancer are considered an effective way of empowering family members to tackle the complex hurdles they face. The ability of parents to develop adaptive coping strategies during the child’s treatment is not only important to their own mental and physical health, but also to their child’s well-being and long-term adjustment with the disease” (Koumarianou et al., 2021) (p. 103).
The systematic development of this program, using a collaborative, interdisciplinary, and ecosystemic approach that integrates theoretical frameworks, empirical evidence, and practical insights from stakeholders, is innovative. It aims to meet the multifaceted needs of families accompanying children with cancer in the Saguenay-Lac-Saint-Jean region. As highlighted by Toruner and Altay (2018) and Snaman et al. (2018), family-centered care is imperative in contemporary pediatric oncology care. However, it is not always clearly understood and integrated into different care settings. The collaborative approach with children, families, and healthcare team members in this protocol is designed to facilitate this integration.
Methodologically, the logical models and matrices associated with the program in this study will offer rigorous syntheses of the vulnerability issues faced by these children and their families, the strengthening of their resilience process, and the necessary multidisciplinary strategies to ultimately improve their well-being and quality of life. These models will serve as valuable references for researchers, healthcare professionals, and policymakers who seek to better understand the realities of these families and apply relevant clinical interventions. The structured and modeled program development approach should also enhance the feasibility, adoption, and ultimately the implementation and evaluation of the program, as noted by Kok et al. (2014, 2017): “The Intervention Mapping protocol helps program planners to optimize chances for effectiveness” (Kok et al., 2014) (p. 105).
In conclusion, this protocol represents a significant step toward developing an evidence-based, contextually relevant program that addresses the unique needs of families accompanying children with cancer in remote areas. The integration of family resilience frameworks, stakeholder input, and rigorous evaluation methods ensures that the program is well-positioned to improve the well-being and resilience of these families, ultimately enhancing their ability to cope with the challenges of pediatric cancer.
Author contributions
CS: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. VR: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MS-P: Formal analysis, Project administration, Validation, Visualization, Writing – original draft, Writing – review & editing. JC: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Supervision, Validation, Writing – original draft, Writing – review & editing. CB-L: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing. MK: Writing – review & editing. CL: Conceptualization, Data curation, Formal analysis, Methodology, Validation, Writing – original draft, Writing – review & editing. SB: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. LL: Formal analysis, Project administration, Writing – review & editing. VF: Resources, Writing – review & editing. SD: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This research protocol is mainly funded by LEUCAN.
Acknowledgments
We are grateful for LEUCAN’s financial support, which enables all aspects of our study from its inception through to completion. Additionally, we extend our thanks to the CIUSSS du Saguenay-Lac-St-Jean for agreeing to involve their team in the planning and future execution of the project within their clinical facilities. Their commitment is crucial to our efforts to advance knowledge in this field. We acknowledge the use of ChatGPT 4 for identifying synonyms in English and correcting language errors. We verified the accuracy of all modifications made by this technology. The version and model used were ChatGPT 4, developed by OpenAI. The authors thank also the Réseau québécois de la recherche en soins palliatifs et de fin de vie (RQSPAL) for financially supporting the publication.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Agence de la Santé Publique du Canada (2024). “Outil de données sur le cancer chez les jeunes au Canada” in Centre de surveillance et de recherche appliquée (Ottawa, ON: Infobase Santé).
Aitken, T. J., and Hathaway, G. (1993). Long distance related stressors and coping behaviors in parents of children with cancer. J. Pediatr. Oncol. Nurs. 10, 3–12. doi: 10.1177/104345429301000103
Armstrong, G. T., Kawashima, T., Leisenring, W., Stratton, K., Stovall, M., Hudson, M. M., et al. (2014). Aging and risk of severe, disabling, life-threatening, and fatal events in the childhood cancer survivor study. J. Clin. Oncol. 32, 1218–1227. doi: 10.1200/JCO.2013.51.1055
Bartholomew, L. K., Markham, C. M., Ruiter, R. A. C., Fernandez, M. E., Kok, G., and Parcel, G. S. (2016). Planning Health Promotion Programs: An Intervention Mapping Approach. 4th Edn. San Francisco, CA: Jossey-Bass- A Wiley Imprint, 678.
Bartholomew, L. K., and Mullen, P. D. (2011). Five roles for using theory and evidence in the design and testing of behavior change interventions. J. Public Health Dent. 71, S20–S33. doi: 10.1111/j.1752-7325.2011.00223.x
Bhakta, N., Liu, Q., Yeo, F., Chemaitilly, W., and Hudson, M. M. (2020). The cumulative burden of surviving childhood cancer: An assessment of chronic health problems in the St. Jude Lifetime Cohort Study (SJLIFE). Lancet Oncol. 18, 982–993. doi: 10.1016/S1470-2045(20)30005-6
Bhakta, N., Qi, L., Ness, K. K., Baassiri, M., Eissa, H., Yeo, F., et al. (2017). The cumulative burden of surviving childhood cancer: an initial report from the St Jude Lifetime Cohort Study (SJLIFE). Lancet 390, 2569–2582. doi: 10.1016/S0140-6736(17)31610-0
Carrandi, A., Hu, Y., McGill, K., Wayland, S., Karger, S., and Maple, M. (2024). Operationalizing the Consolidated Framework for Implementation Research to build and support the lived experience workforce in direct health service provision. Health Expect. 27, 1–16. doi: 10.1111/hex.14035
Cohen, J. (1988). Statistical power analysis for the behavioral sciences. 2nd Edn. Hillsdale, New Jersey (NJ), USA: Lawrence Erlbaum Associates.
Corrigan, J. J., and Feig, S. A. (2004). Guidelines for pediatric cancer centers. Pediatrics 113, 1833–1835. doi: 10.1542/peds.113.6.1833
Creswell, J. W. (2013). Qualitative Inquiry and Research Design: Choosing Among Five Approaches. 3rd Edn. Thousand Oaks, CA: Sage, 448.
Damschroder, L. J., Aron, D. C., Keith, R. E., Kirsh, S. R., Alexander, J. A., and Lowery, J. C. (2009). Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement. Sci. 4:50. doi: 10.1186/1748-5908-4-50
Daniel, G., Wakefield, C. E., Ryan, B., Fleming, C., Levett, N., and Cohn, R. J. (2013). Accommodation in pediatric oncology: parental experiences, preferences and unmet needs. Rural Remote Health 13, 1–9. doi: 10.22605/RRH2005
Field, A. (2017). Discovering statistics using IBM SPSS statistics. 5th Edn. London, United Kingdom: Sage Publications.
Fluchel, M. N., Kirchhoff, A. C., Bodson, J., Sweeney, C., Edwards, S. L., Ding, Q., et al. (2014). Geography and the burden of care in pediatric cancers. Pediatr. Blood Cancer 61, 1918–1924. doi: 10.1002/pbc.25170
Gottlieb, L. N. (2013). Strenghts-Based Nursing Care: Health and Healing for Person and Family. New-York, NY: Springer Publishing Company, 413.
Gottlieb, L., and Gottlieb, B. (2017). Strenght-based nursing: A process for implementing a philosophy into practice. J. Fam. Nurs. 23, 319–340. doi: 10.1177/1074840717717731
Grove, S. K., Burns, N., and Gray, J. (2013). The Practice of Nursing Research: Appraisal, Synthesis, and Generation of Evidence. 7th Edn. Saint-Louis, MO: Elsevier, 732.
Hackman, J. R., and Vidmar, N. (1970). Effects of size and task type on group performance and member reactions. Sociometry 33, 37–54. doi: 10.2307/2786271
Hudson, M. M., Ness, K. K., Gurney, J. G., Mulrooney, D. A., Chemaitilly, W., Krull, K. R., et al. (2013). Clinical ascertainment of health outcomes among adults treated for childhood cancer. JAMA 309, 2371–2381. doi: 10.1001/jama.2013.6296
IBM Corporation (2017). IBM SPSS: Statistics for Windows, Version 25.0. Armonk, NY: IBM Corporation.
Johnson, S. K., Halm, M. A., Titler, M. G., Craft, M., Kleiber, C., Montgomery, L. A., et al. (1993). Group functioning of a collaborative family research team. Clin. Nurse Spec. 7, 184–191. doi: 10.1097/00002800-199307000-00007
Kazak, A. E., Abrams, A. N., Banks, J., Christofferson, J., DiDonato, S., Grootenhuis, M. A., et al. (2015). Psychosocial assessment as a standard of care in pediatric cancer. Pediatr. Blood Cancer 62, S426–S459. doi: 10.1002/pbc.25730
Khan, M. S., Al-Jadiry, M. F., Tarek, N., Zamzam, M., Saab, R., Trehan, A., et al. (2022). Pediatric oncology infrastructure and workforce training needs: a report from the Pediatric Oncology East and Mediterranean (POEM) Group. Pediatr. Blood Cancer :e29858. doi: 10.1002/pbc.29190
Kok, G., Bartholomew, L. K., Parcel, G. S., Gottlieb, N. H., and Fernández, M. E. (2014). Finding theory- and evidence-based alternatives to fear appeals: Intervention Mapping. Int. J. Psychol. 49, 98–107. doi: 10.1002/ijop.12001
Kok, G., Peters, L. W. H., and Ruiter, R. A. C. (2017). Planning theory- and evidence-based behavior change interventions: a conceptual review of the intervention mapping protocol. Psicol. Reflex. Crit. 30:19. doi: 10.1186/s41155-017-0072-x
Koumarianou, A., Symeonidi, A. E., Kattamis, A., Linardatou, K., Chrousos, G. P., and Darviri, C. (2021). A review of psychosocial interventions targeting families of children with cancer. Palliat. Support. Care 19, 103–118. doi: 10.1017/S1478951520000449
Masera, G., Cesa Bianchi, M., and Delle, F. A. (2013). The promotion of resilience: the new paradigm in paediatric oncology. Epidemiol. Prev. 37, 278–281.
McCubbin, M., Balling, K., Possin, P., Frierdich, S., and Bryne, B. (2002). Family resiliency in childhood cancer. Fam. Relat. 51, 103–111. doi: 10.1111/j.1741-3729.2002.00103.x
Miles, M. B., Huberman, M. A., and Saldana, J. (2014). Qualitative Data Analysis: A Méthods Sourcebook. 3rd Edn. Thousand Oaks, CA: SAGE Publications, 381.
National Cancer Institute . Late Effects of Treatment for Childhood Cancer (PDQ®)–Health Professional Version [Internet]. (2024). Available at: https://www.cancer.gov/types/childhood-cancers/late-effects-hp-pdq.
Organisation Mondiale de la Santé . Improving outcomes of childhood cancer: Organisation mondiale de la Santé ; (2021). Available at: https://www.who.int/news-room/fact-sheets/detail/childhood-cancer.
Pai, A. L., Patino-Fernandez, A. M., McSherry, M., Beele, D., Alderfer, M. A., Reilly, A. T., et al. (2008). The Psychosocial Assessment Tool (PAT2.0): psychometric properties of a screener for psychosocial distress in families of children newly diagnosed with cancer. J. Pediatr. Psychol. 33, 50–62. doi: 10.1093/jpepsy/jsm053
Paul, V., Inhestern, L., Sigmund, D., Winzig, J., Rutkowski, S., Escherich, G., et al. (2024). Addressing gaps and enhancing experiences in support services for families of pediatric cancer survivors. Pediatr. Res. doi: 10.1038/s41390-024-03320-2
Robison, L. L., and Hudson, M. M. (2014). Survivors of childhood and adolescent cancer: life-long risks and responsibilities. Nat. Rev. Cancer 14, 61–70. doi: 10.1038/nrc3634
Rosenberg, A. R., Bradford, M. C., Junkins, C. C., Taylor, M., Zhou, C., Sherr, N., et al. (2019). Effect of the promoting resilience in stress management intervention for parents of children with cancer (PRISM-P): a randomized clinical trial. JAMA Netw. Open 2:e1911578. doi: 10.1001/jamanetworkopen.2019.11578
Rosenberg, A. R., Bradford, M. C., McCauley, E., Curtis, J. R., Wolfe, J., Baker, K. S., et al. (2018). Promoting resilience in adolescents and young adults with cancer: Results from the PRISM randomized controlled trial. Cancer 124, 3909–3917. doi: 10.1002/cncr.31666
Rosenberg, A. R., Wolfe, J., Bradford, M. C., Shaffer, M. L., Yi-Frazier, J. P., Curtis, J. R., et al. (2014). Resilience and psychosocial outcomes in parents of children with cancer. Pediatr. Blood Cancer 61, 552–557. doi: 10.1002/pbc.24854
Sancassiani, F., Gambino, S., Lindert, J., Sali, L., Pinna, I., Origa, G., et al. (2021). The reliability and test-retest stability of the treatment perception questionnaire (TPQ) in the oncology field: a pilot study. Clin. Pract. Epidemiol. Mental Health 17, 324–330. doi: 10.2174/1745017902117010324
Scott-Findlay, S., and Chalmers, K. (2001). Rural families' perspectives on having a child with cancer. J. Pediatr. Oncol. Nurs. 18, 205–216. doi: 10.1053/jpon.2001.26864
Simard, C. (2023). “L’accompagnent d’un enfant atteint de cancer: une expérience aux multiples contextes pour les familles habitant loin des centres spécialisés” in Enfances, Familles, Générations, 42.
Snaman, J. M., Kaye, E. C., Baker, J. N., and Wolfe, J. (2018). Pediatric palliative oncology: the state of the science and art of caring for children with cancer. Curr. Opin. Pediatr. 30, 40–48. doi: 10.1097/MOP.0000000000000573
Statistique Canada . Population urbaine et rurale, par province et territoire. Ottawa, ON (2013). Available at: http://www.statcan.gc.ca/cgi-bin/sum-som/getcans/cstsaveasflg2.cgi?filename=demo62a-fra.htm&lan=fre (Accessed February 13, 2013).
Tabachnick, B. G., and Fidell, L. S. (2019). Using multivariate statistics. 7th Edn. Boston: Pearson Education.
Tanner, L., Keppner, K., Lesmeister, D., Lyons, K., Rock, K., and Sparrow, J. (2020). Cancer rehabilitation in the pediatric and adolescent/young adult population. Semin. Oncol. Nurs. 36:150984. doi: 10.1016/j.soncn.2019.150984
Toruner, E. K., and Altay, N. (2018). New trends and recent care approaches in pediatric oncology nursing. Asia Pac. J. Oncol. Nurs. 5, 156–164. doi: 10.4103/apjon.apjon_3_18
Van Shoors, M., Caes, L., Lesley, L., Verhofstadt, L. L., Goubert, L., and Alderfer, M. A. (2015). Systematic review: family resilience after pediatric cancer diagnosis. J. Pediatr. Psychol. 40, 856–868. doi: 10.1093/jpepsy/jsv055
Varni, J. W., Limbers, C. A., and Burwinkle, T. M. (2007). How young can children reliably and validly self-report their health-related quality of life?: an analysis of 8,591 children across age subgroups with the PedsQL 4.0 Generic Core Scales. Health Qual. Life Outcomes 5:1. doi: 10.1186/1477-7525-5-1
Walling, E. B., Fiala, M., Connolly, A., Drevenak, A., and Gehlert, S. (2019). Challenges associated with living remotely from a pediatric cancer center: a qualitative study. J. Oncol. Pract. 15, e219–e229. doi: 10.1200/JOP.18.00115
Walsh, F. (2016a). Applying a family resilience framework in training, practice, and research: mastering the art of the possible. Fam. Process 55, 616–632. doi: 10.1111/famp.12260
Wiener, L., Kazak, A. E., Noll, R. B., Patenaude, A. F., and Kupst, M. J. (2015). Interdisciplinary collaboration in standards of psychosocial care. Pediatr. Blood Cancer 62:S425. doi: 10.1002/pbc.25718
Keywords: pediatric oncology, family resilience, remote communities, Canada, intervention mapping
Citation: Simard C, Roberge V, St-Pierre M, Cherblanc J, Bergeron-Leclerc C, Kadri MA, Lacharité C, Bérubé S, Lapointe L, Faucher V and Dufresne SS (2024) Designing a resilience-based intervention program for children with cancer and their families: a study protocol. Front. Psychol. 15:1419192. doi: 10.3389/fpsyg.2024.1419192
Edited by:
Norbert Schäffeler, Tübingen University Hospital, GermanyReviewed by:
Eva-Maria Skoda, LVR University-Hospital Essen, GermanyChristian Heuser, University of Cologne, Germany
Amanda Marin-Chollom, Central Connecticut State University, United States
Copyright © 2024 Simard, Roberge, St-Pierre, Cherblanc, Bergeron-Leclerc, Kadri, Lacharité, Bérubé, Lapointe, Faucher and Dufresne. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chantale Simard, Q2hhbnRhbGUxX1NpbWFyZEB1cWFjLmNh