 Isabel Martín-Monzón
Isabel Martín-Monzón Laura Amores-Carrera
Laura Amores-Carrera David Sabsevitz
David Sabsevitz Guillaume Herbet
Guillaume Herbet- 1Department of Experimental Psychology, Faculty of Psychology, Campus Santiago Ramón y Cajal, University of Seville, Seville, Spain
- 2Department of Psychiatry and Psychology, Division of Neuropsychology, Mayo Clinic Florida, Jacksonville, FL, United States
- 3Department of Neurosurgery, Gui de Chauliac Hospital, Montpellier, France
- 4Praxiling Lab, UMR5267 CNRS & Paul Valéry University, Bâtiment de Recherche Marc Bloch, Montpellier, France
- 5Department of Medicine, University of Montpellier, Campus ADV, Montpellier, France
- 6Institut Universitaire de France, Paris, France
The right hemisphere of the brain is often referred to as the non-dominant hemisphere. Though this is meant to highlight the specialized role of the left hemisphere in language, the use of this term runs the risk of oversimplifying or minimizing the essential functions of the right hemisphere. There is accumulating evidence from functional MRI, clinical lesion studies, and intraoperative mapping data that implicate the right hemisphere in a diverse array of cognitive functions, including visuospatial functions, attentional processes, and social cognitive functions. Neuropsychological deficits following right hemisphere resections are well-documented, but there is a general paucity of literature focusing on how to best map these functions during awake brain surgery to minimize such deficits. To address this gap in the literature, a systematic review was conducted to examine the cognitive and emotional processes associated with the right hemisphere and the neuropsychological tasks frequently used for mapping the right hemisphere during awake brain tumor surgery. It was found that the most employed tests to assess language and speech functions in patients with lesions in the right cerebral hemisphere were the naming task and the Pyramids and Palm Trees Test (PPTT). Spatial cognition was typically evaluated using the line bisection task, while social cognition was assessed through the Reading the Mind in the Eyes (RME) test. Dual-tasking and the movement of the upper and lower limbs were the most frequently used methods to evaluate motor/sensory functions. Executive functions were typically assessed using the N-back test and Stroop test. To the best of our knowledge, this is the first comprehensive review to help provide guidance on the cognitive functions most at risk and methods to map such functions during right awake brain surgery.
Systematic Review Registration: PROSPERO database [CRD42023483324].
1 Introduction
Direct electrical stimulation (DES) during awake craniotomy for brain tumors has contributed substantially to our understanding of functional neuroanatomy. Nevertheless, most of this work has focused on the dominant hemisphere or left hemisphere functions, mainly speech and language; the right hemisphere, typically referred to as the non-dominant hemisphere, is often considered less eloquent than the left hemisphere, especially in clinical fields. This is highlighted by the preference in many neurosurgical centers to perform left hemisphere resections awake with DES, while right hemisphere resections not involving the sensorimotor cortex are often done under general anesthesia. The view that the right hemisphere is less eloquent than the left hemisphere is challenged by the many lesion and neuroimaging studies (Bartolomeo, 2006; Gianotti, 2012; Robertson, 2014) showing that a variety of functions depend on the integrity of the right hemisphere, including attention, visuospatial, emotional, and social cognitive functions. Further, high rates of cognitive morbidity have been reported after right hemisphere resections (Vilasboas et al., 2017).
Herbet and Duffau (2020) highlighted the critical importance of mapping the right hemisphere as well as the cortico-subcortical distributed networks mediating movement execution and control, visual and spatial cognition, language processing, working memory, and social cognition. This is particularly noteworthy given the observed constraints in neuroplasticity potential within these connections (Herbet et al., 2016). Following their work, different teams around the world have started to introduce new tasks to monitor a variety of cognitive functions, including sensorimotor, language, attention, visuospatial, emotional, and social functions. Duffau and his group have made significant contributions to the literature by extending mapping to the white matter pathways (Duffau et al., 2002) and, in collaboration with neuropsychologists, introduced new cognitive tasks to the operating room, such as the line bisection paradigm (Thiebaut de Schotten et al., 2005).
Intraoperative stimulation mapping is critical in optimizing the extent of resection while sparing cognitive functions and improving patients' quality of life in both left and right hemisphere surgeries (De Witt Hamer et al., 2012; Wijnenga et al., 2018). Areas usually thought of as “noneloquent” can be essential for brain functions, such as the crucial role of both the right inferior frontal gyrus and the right dorsolateral prefrontal cortex in mentalizing (Yordanova et al., 2017), the right dorsolateral prefrontal cortex in nonverbal semantic processing (Herbet et al., 2018), the right fronto-temporo-parietal cortex in attention (Krall et al., 2015), or right-sided speech functions (Vilasboas et al., 2017).
There is little research to guide the selection of tasks to optimally map these functions with DES. To help inform task selection, it is important to summarize the neuropsychological tasks frequently used for mapping the right hemisphere during awake brain tumor surgery and their correlates with neuroanatomy based on a network model. This study seeks to provide a systematic review of the literature on intraoperative protocols used to map the right hemisphere during awake surgery.
2 Methods
Details of the protocol for this systematic review were registered in the PROSPERO database (CRD42023483324).
2.1 Search strategy
A systematic literature review was conducted following the PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-Analyzes) in order to adjust the review methodology to quality criteria (Liberti et al., 2009; Moher et al., 2009). The databases used to search for articles were PubMed, PsycINFO, Scopus, and Cochrane Library. All of these databases were chosen because they contain articles related to neuroscience in general (PubMed, Scopus, Cochrane Library) and specifically psychology (PsycINFO).
The search process was carried out systematically in these databases, with words and Boolean terms: (“awake brain surgery” OR “awake craniotomy” OR “awake brain mapping” OR “intraoperative mapping”) AND (“right hemisphere” OR “non-dominant hemisphere”) AND (“cognitive functions” OR “cognitive processes”) AND “social cognition” in different combinations. The results were limited to articles published in academic journals in the last 19 years (2005–2024) because it is a recent study topic, especially in the field of neurosurgery. The search in the databases was carried out up to March 2024, obtaining a total of 138 articles in PubMed, 110 in Scopus, 102 in PsycINFO, and 99 in Cochrane Library.
After the first screening, 84 duplicate articles were removed, and a total of 294 were excluded by title and abstract to ensure the selection of relevant articles for further evaluation. Each article was carefully reviewed based on the following criteria: relevance to the research topic, clarity of reported outcomes, methodological alignment, and quality of evidence. Specifically, articles that did not directly address awake craniotomy with direct electrical stimulation in adult glioma patients were excluded. Additionally, articles with unclear or ambiguous reported outcomes related to cognitive functions during awake brain surgery were also excluded. Furthermore, articles that did not align with the methodological framework of our study, such as those assessing cognitive processes not pertinent to right hemisphere surgeries, were excluded. The second phase of screening consisted of an exhaustive reading of the 71 full articles in order to check in Section 2 for the most important variables related to our research question: the number of subjects studied, their age, the surgery procedure followed, the pathologies of the participants, and the neuropsychological instruments informed. This first analysis revealed that some articles did not meet the eligibility criteria, and 40 publications were finally discarded due to the omission of relevant data points. Figure 1 shows the complete study selection process, which ended with 31 articles finally chosen for the systematic review. Authors, titles, year, and code per publication are specified in Table 1.
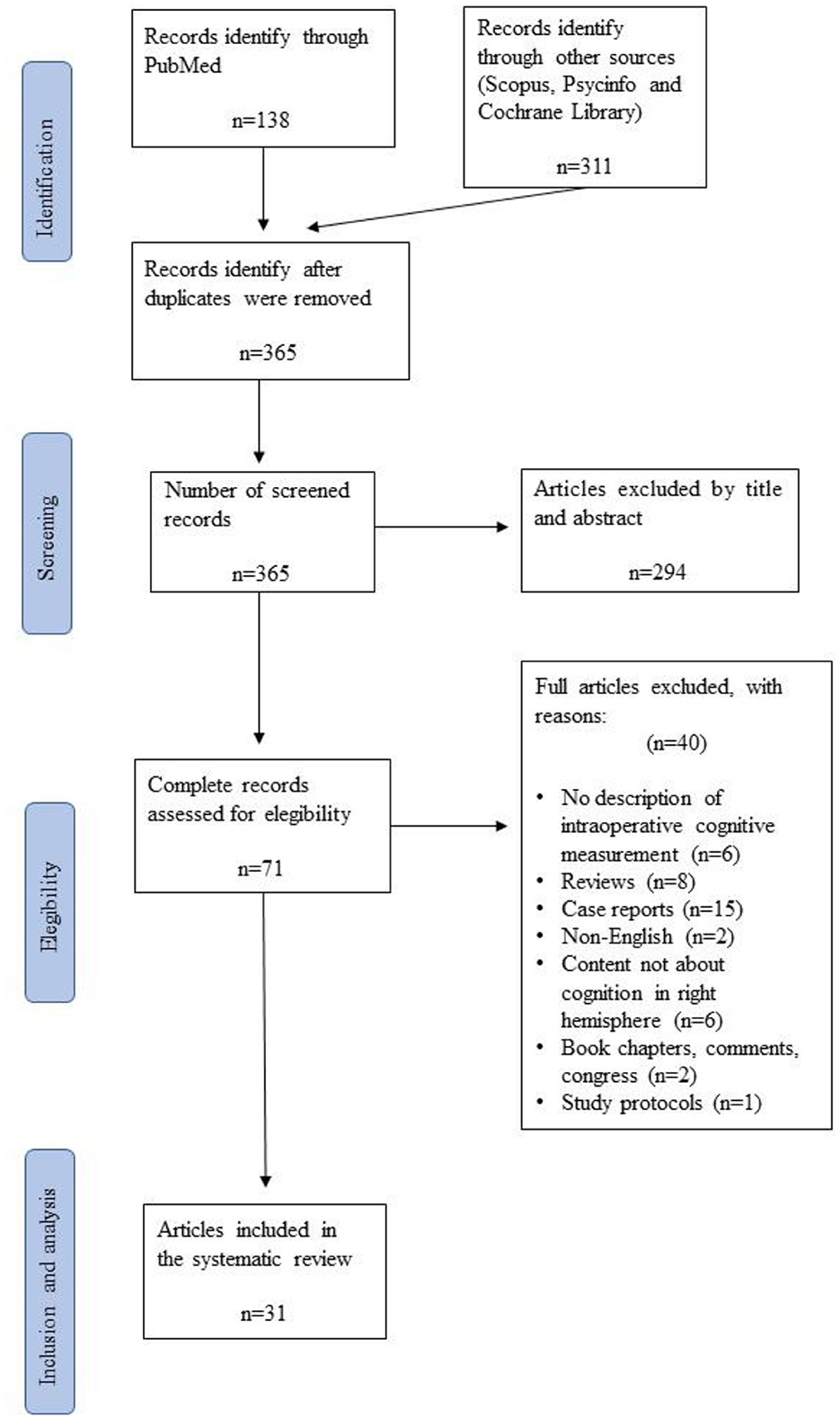
Figure 1. Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flowchart illustrating the search, screening, inclusion, and exclusion process for the present study.
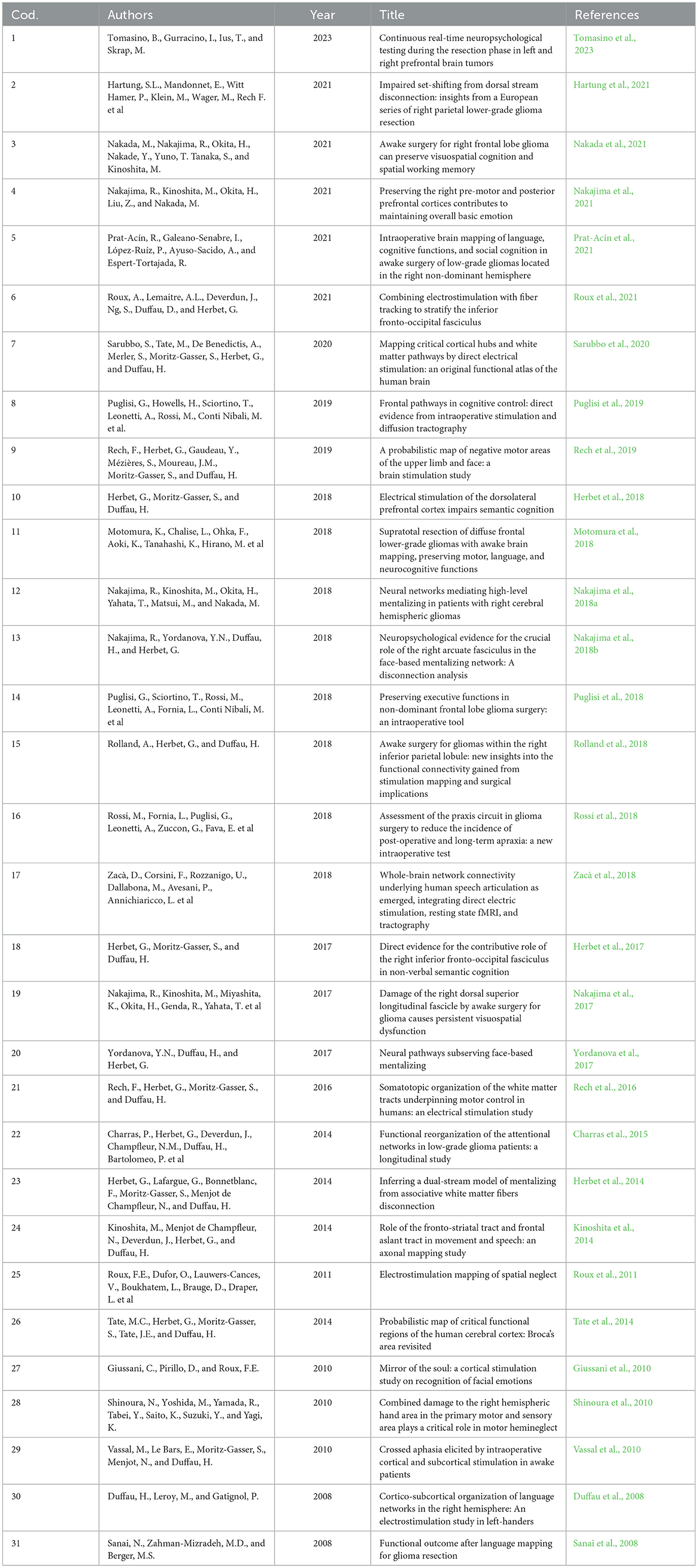
Table 1. Articles considered by code, authors, year and title included in the systematic review.
For the analysis of these articles, a two-phase procedure was conducted. In the first phase, the methodological characteristics of the 31 articles were systematically evaluated, specifying the characteristics of the samples, the histopathology of patients, the location of the lesion within the right hemisphere, the instruments used during intraoperative mapping, how the neuroanatomical data were acquired, and the neuropsychological assessment method used (Table 2). In the second phase, the information presented in the results sections of each article was synthesized (Tables 3, 4).
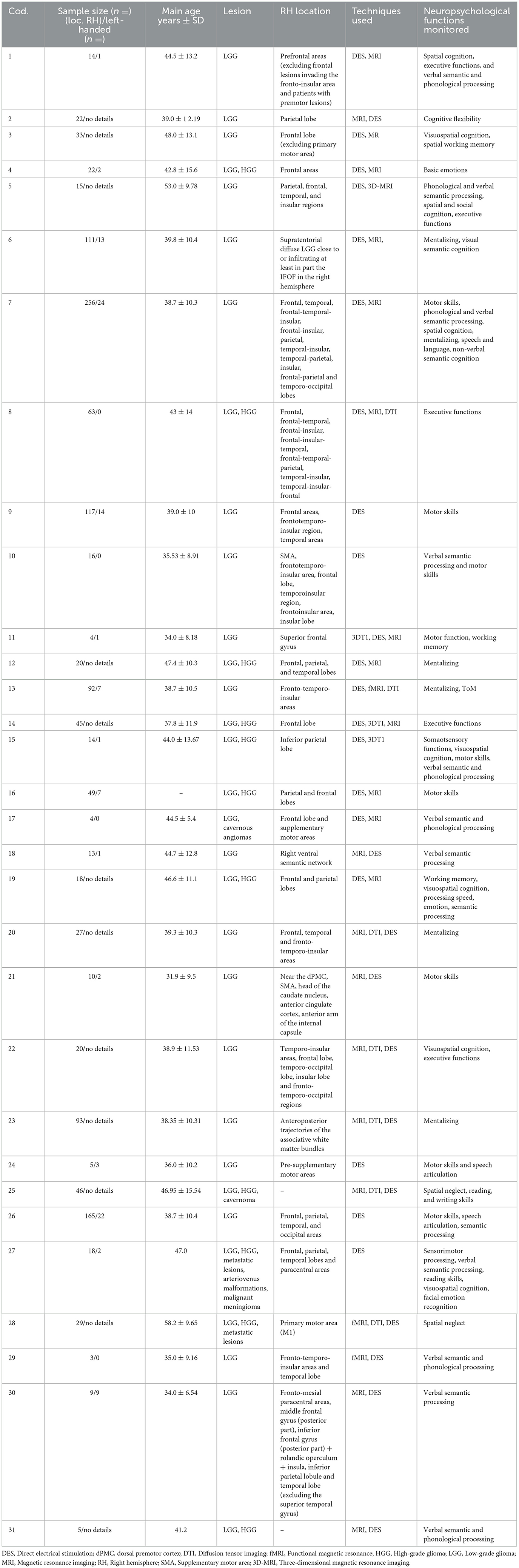
Table 2. Main methodological information of the reviewed articles.
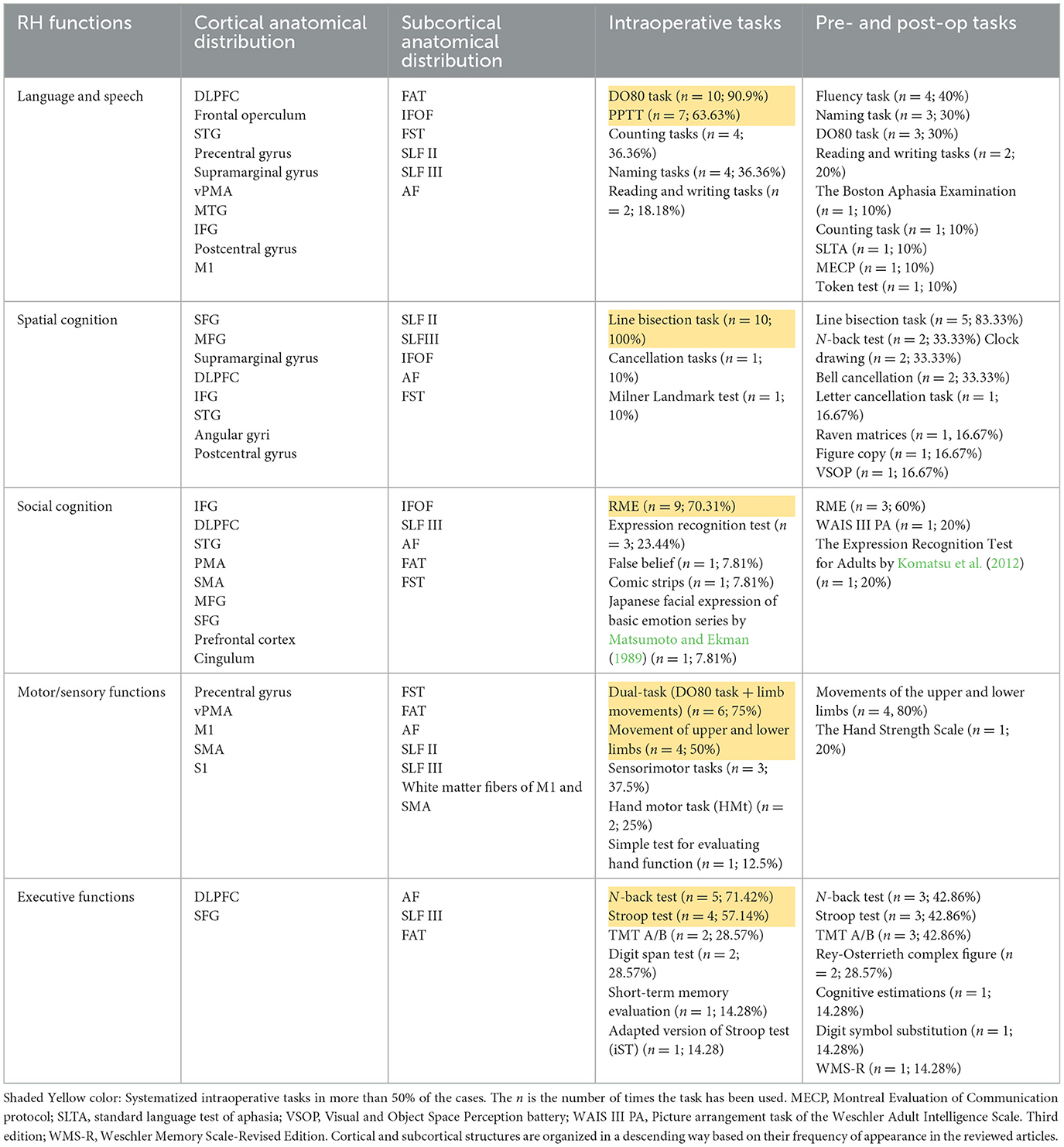
Table 3. Distribution of the brain areas (cortical and subcortical levels) and the percentage of tasks systematically used in each phase (pre-, intra-, and post-operative) per cognitive functions.
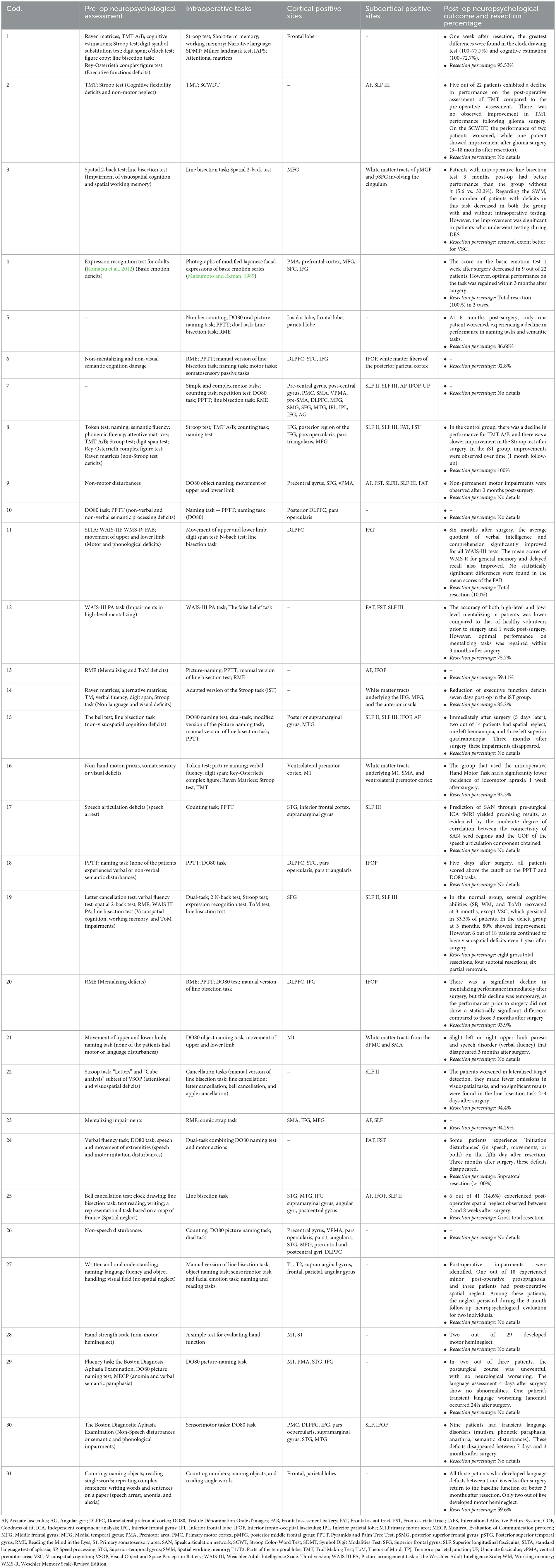
Table 4. Relevant results of the reviewed studies.
2.2 Inclusion and exclusion criteria
The inclusion and exclusion criteria were defined according to the PICO (patient population, intervention, control, outcome) framework criteria. All articles were included that reported on adult patients with gliomas of the right hemisphere (WHO grade I–IV: patient population) who underwent awake craniotomies with DES (intervention) and who produced specific intraoperative cognitive errors (outcome) while stimulating or resecting in a specific reported brain location (outcome). As long as DES was used, studies using additional imaging techniques (e.g., intraoperative Magnetic Resonance Imaging, iMRI; Diffusion Tensor Imaging, DTI; functional Magnetic Resonance Imaging, fMRI) were also included.
Articles were excluded if brain locations or cognitive errors were not reported, not further specified, or not clear. Articles were also excluded if they did not report (original) patient data or intraoperative neuropsychological information on glioma patients or if the article was a book chapter, comment, case report, editorial, or was written in a language other than English. The PRISMA flowchart is shown in Figure 1.
2.3 Data analysis
The different data analyses are explained below.
2.3.1 First analysis: cortical and subcortical distribution of brain functions assessed
The cognitive functions and a percentage of how often these cognitive processes occurred in a specific brain location (cortically and subcortically) were calculated based on the total number of articles that reviewed each cognitive function (e.g., total of speech articulation articles: n = 7, speech arrest in location x: n = 3 =42.85%).
Locations, including the gyrus, cortex, and lobe, were seen as cortical. At the subcortical level, a distinction was made between general subcortical locations (e.g., white matter below primary motor area, M1 and supplementary motor area, SMA) and subcortical tracts (e.g., inferior fronto-occipital fasciculus, IFOF; superior longitudinal fasciculus SLF).
2.3.2 Second analysis: cognitive functions and intraoperative tasks
Individually, for each cognitive function, a percentage of how often an intraoperative task was used was calculated based on the total number of articles that reviewed each cognitive process (e.g., total spatial cognition articles: n = 9, cancellation task performed in n = 1 articles = 11.11%). The level of evidence for each task was also compiled. A high level of evidence was considered for a task when its frequency and percentage of occurrence were equal to or >50%.
2.3.3 Third analysis: pre- and post-operative outcomes
For each cognitive function, a percentage was calculated to indicate how frequently a task was used pre- and post-operatively. This calculation was based on the total number of articles that assessed each cognitive function in the pre- and post-op phases.
2.4 Participant characteristics
In Table 2, the main methodological information is synthesized. In 25 articles (1, 2, 3, 5, 6, 7, 8, 9, 12, 13, 14, 15, 17, 19, 20, 22, 23, 24, 25, 26, 27, 28, 29, 30, and 31), the data were collected in order to study the effects of the transitory disconnection of different brain areas caused by DES and its effects on the cognitive functions (semantic and phonological processing, speech articulation, visuospatial cognition, working memory, and cognitive flexibility) and in six studies (4, 6, 10, 11, 16, and 19) DES caused transient disturbances in socio-cognitive processing [mentalizing, theory of mind, (ToM), and basic emotion deficits].
The sample size in Table 2 indicates the number of subjects who had a lesion within the right hemisphere. The total number of participants included in this review is 1,358; although most studies had a sample of fewer than 50 participants, five studies include less than six patients (11, 17, 24, 25, and 31), and only six publications evaluated 92 to 245 cases (6, 7, 9, 13, 23, and 26). The mean age of the participants ranges from 34.0 to 58.2 (range: 18–63 years). Left-handed participants were also considered in this study. Only five out of 31 articles selected for the present systematic review showed a left-handed sample size >3 (6, 9, 16, 26, and 30). Articles 10, 17, and 29 only include right-handed patients in their studies, and 11 articles (2, 3, 5, 12, 19, 20,22, 23, 25, 28, and 31) did not report the handedness of the subjects.
The location of the lesion within the right hemisphere was specified in 12 studies (37.03%) (3, 6, 10, 11, 14, 15, 16, 17, 18, 21, 23, 24, 28, and 30). Two articles (23 and 29) did not report the location, and 13 (1, 2, 4, 5, 9, 12, 13, 19, 20, 22, 26, 27, and 29) only showed the cerebral lobe and lobule regions where the glioma was located (frontal, parietal, temporal, insular, and occipital lobes).
The main lesion located in the right hemisphere was the diffuse low-grade glioma (LGG; WHO grade II). In addition to LGG, high-grade gliomas (HGG; WHO III and IV) were found in 33.33% (n = 11), and other lesions such as cavernous angiomas (17), cavernomas (25), metastatic lesions (27, 28), arteriovenous malformations (27), and meningiomas (27, 28) were described (n = 4; 14.81%).
Finally, all the studies used DES intraoperatively. Neuroimaging techniques such as MRI, fMRI, or 3D-MRI were used to analyze both the location and size of the lesion prior to surgery, as well as examine the volume of tissue resected after surgery. No MRI imaging techniques were conducted in four studies (9, 10, 26, and 27). Diffusion tensor imaging techniques were combined with MRI studies in ten articles (7, 8, 11, 13, 14, 17, 22, 24, 25, and 28) to track the main bundles of white matter tracts pre-operatively.
3 Results
This review article presents an in-depth analysis of the 31 articles included in Table 1. In the search for which cognitive and emotional processes have been related to positive cortical-subcortical sites when right brain surgery has been performed, as well as which neuropsychological tasks are more sensitive to assess high-order cognitive processing during surgery (Figure 2), we performed a systematic analysis of 1. neuropsychological functions assessed during pre-, intra- and post- right awake surgery; 2. type of tasks employed during right awake surgery; and 3. Pre- and post-surgical neuropsychological outcomes (Table 4). Figure 1 presents the highlights of this literature review.
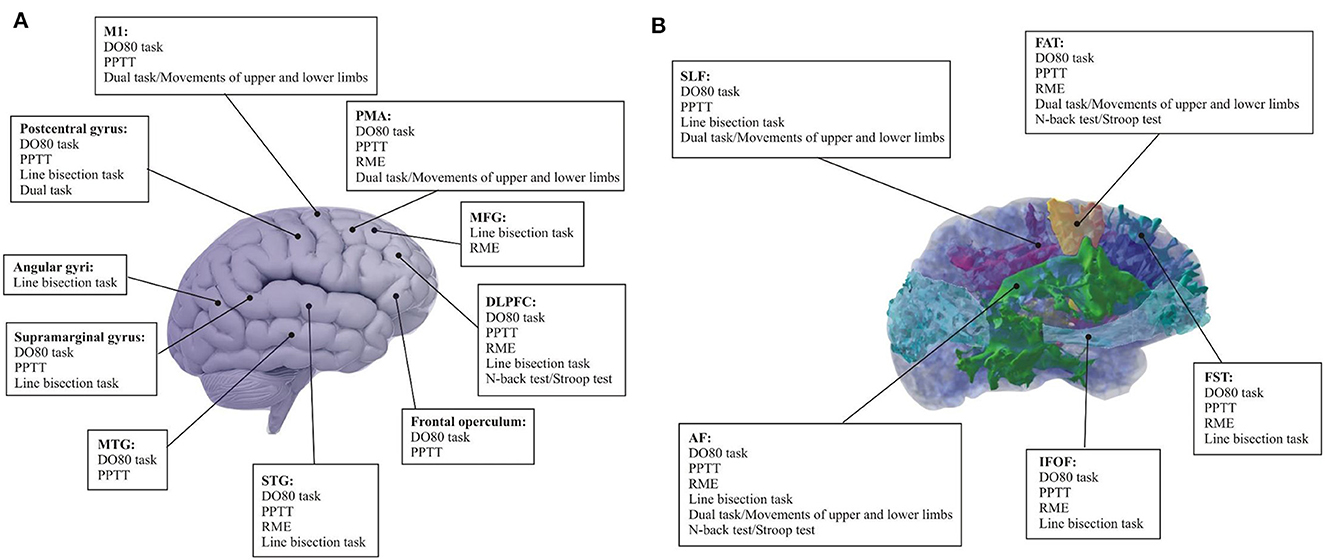
Figure 2. Summary of the neuropsychologically validated tasks frequently used and neural networks mediating cognitive and social function provided by cortico-subcortical electrical mapping. It shows cortical (A) and subcortical (B) visual representation. Note that only neuropsychological tasks with a high level of evidence (>50%) are indicated. D080 task (90.9%); PPTT (63.63%); Line bisection task (100%); RME (70.31%); Dual-task (75%); Movements of upper and lower limbs (50%); N-back test (71.42%); Stroop test (50%). AF, Arcuate fasciculus; DLPFC, Dorsolateral prefrontal cortex; DO80 task, Dénomination orale d'images test; FAT, Frontal aslant tract; FST, Fronto-striatal tract; IFOF, Inferior fronto-occipital fasciculus; MFG, Middle frontal gyrus; MTG, Middle temporal gyrus; M1, Primary motor cortex; PMA, Premotor area; PPTT, Pyramids and Palm Tree Test; RME, Reading the Mind in the Eyes; SLF, Superior longitudinal fasciculus; STG, Superior temporal Gyrus.
3.1 First analysis: cortical and subcortical distribution of brain functions assessed
As shown in Table 3, the 31 articles selected for this systematic review comprehensively explore different neurocognitive functions that were assessed during DES in right awake surgery patients. The included studies predominantly assessed essential cognitive domains, including language, spatial cognition, social cognition, motor/sensory functions, and executive functions. The relationship between these cognitive functions and cortical and subcortical brain regions was analyzed.
3.1.1 Language and speech
Language and speech functions were assessed in 12 of the 31 articles selected for the present systematic review (41.34%).
Speech arrest disturbances were described cortically in seven articles (53.84%): Ventral premotor area (vPMA) (n = 4; 57.14%), the precentral gyrus (n = 4; 57.14%), frontal operculum (pars opercularis and triangularis; n = 3; 42.85%), supramarginal gyrus (n = 3; 42.85%), medial temporal gyrus (MTG) (n = 2; 42.85%), inferior temporal gyrus (IFG) (n = 2; 42.85%), dorsolateral prefrontal cortex (DLPFC) (n = 2; 14.28%), superior temporal gyrus (STG) (n = 1; 14.28%), and primary motor area (M1) (n = 1; 14.28%). Five (7, 8, 9, 24, 30) of the seven articles showed the results of DES at the subcortical level: superior longitudinal fasciculus II (SLF II) (n = 4; 80%), superior longitudinal fasciculus (SLF III) (n = 3; 60%), frontal aslant tract (FAT) (n = 1; 33.33%), fronto-striatal tract (FST) (n = 1; 100%), arcuate fasciculus (AF) (n = 1; 33.33%), and IFOF (n = 1; 33.33%).
Verbal and non-verbal semantic cognition were also analyzed (n = 7; 58.33%). The cortical regions involved in semantic cognition were as follows: DLPFC (n = 5; 83.33%), STG (n = 3; 50%), frontal operculum (n = 2; 33.33%), MTG (n = 1; 16.67%), middle frontal gyrus (MFG) (n = 1; 16.67%), and IFG (n = 1; 16.67%). The subcortical areas related to semantic cognition were only described in four of the six articles (6, 9, 14, 26). The main white matter tract involved in this language component was the SLF III (n = 3; 75%) and IFOF (n = 2; 50%). FAT (n = 1; 25%) and was also found. Article 6 only reported that semantic cognition deficits appeared when DES was applied to the white matter tracts of the posterior parietal lobe. It should be noted that one article did not specify the positive language-related sites (1), and another one (5) showed that language disturbances were observed after the electrical stimulation of the insular and frontal lobes.
3.1.2 Spatial cognition
Spatial cognition was analyzed in 10 articles of a total of 31 (34.48%). Two studies (13 and 20) assessed this neurocognitive function, but as part of the awake brain surgery routine. Eight out of the ten articles provided results about the intraoperative findings at the cortical level: MFG (n = 2; 20%), superior frontal gyrus (SFG) (n = 2; 20%), supramarginal gyrus (n = 2; 20%), the postcentral gyrus (n = 2; 20%), STG (n = 2; 20%), DLPFC (n = 1; 10%), IFG (n = 1; 10%), MTG (n = 1; 10%), SFG (n = 1; 10%), inferior parietal lobe (IPL) (n = 1; 10%), and the angular gyri (n = 1; 10%). The subcortical positive sites were located mainly in SLF II and III (n = 10; 100%). Other significant white matter tracts involved in this cognitive process were IFOF (n = 2; 20%), FAT (n = 1; 10%), and AF (n = 1; 10%).
3.1.3 Social cognition
Eight out of 31 articles selected (27.59%) showed mentalizing and emotional processing deficits during DES over the following cortical sites: IFG (n = 6; 100%), premotor area (PMA) (n = 2; 33.33%); DLPFC (n = 2; 33.33%), STG (n = 2; 33.33%), SFG (n = 2; 33.33%), MFG (n = 1; 16.67%); SMA (n = 1; 16.67%); cingulum (n = 1; 16.67%), and prefrontal cortex (n = 1; 16.67%). These percentages have been calculated considering the number of studies in which the cortical areas were mentioned (n = 6). The subcortical mapping was described in five articles (6, 12, 13, 18, and 21): IFOF (n = 3; 60%); SLF III (n = 2; 40%); AF (n = 2; 40%); FAT (n = 1; 20%), and FST (n = 1; 20%).
3.1.4 Motor/sensory functions
Motor/sensory functions were evaluated in eight articles. Nevertheless, only five (9, 17, 21, 24, and 28) out of 31 reported results about intraoperative brain mapping (n = 5; 17.24%). The other three articles (11, 15, 19) carried out the assessment of these brain functions to avoid potential motor interferences in the cognitive processes they aimed to evaluate. Three studies (9, 21, 28) described the cortical brain mapping: M1 (n = 2; 66,67%), vPMA (n = 1; 33.33%), premotor cortex (PMC) (n = 1; 33.33%), SMA (n = 1; 33.33%), primary somatosensory area (S1) (n = 1; 33.33%), and precentral gyrus (n = 1; 33.33%); and all the articles described the subcortical brain mapping: FST (n = 2; 50%), FAT (n = 2; 50%), SLF (n = 2; 50%), AF (n = 1; 25%). One out of 4 (17) studies revised for the motor/sensory functions showed that motor skills were observed over the sensorimotor cortex during DES. No description of critical cortical or subcortical regions involved in this cognitive function was analyzed.
3.1.5 Executive functions
Inhibition and working memory (executive functions) were found in 6 out of 31 articles (1, 2, 3, 8, 11, and 9) selected for the systematic review (20.69%). The cortical positive sites were: DLPFC (n = 1; 16.67%%) and SFG (n = 1; 16.67%); IFG (n = 1; 16.67%); and MFG (n = 1; 16.67%). At the subcortical level, FAT (n = 2; 33.33%) and SLF II and III (n = 2; 33.33%) were described. It should be noted that one article (1) suggested a non-specific brain mapping during DES.
3.2 Second analysis: cognitive functions and intraoperative tasks
The intraoperative findings at the cortical and subcortical levels for each of the cognitive functions assessed were made possible using different neuropsychological tasks (Tables 3, 4).
3.2.1 Language and speech
A strong level of evidence showed that the main tasks used to assess semantic cognition and speech articulation intraoperatively were the Dénomination orale d'images test (DO80) (n = 10; 90.9%) and Pyramids and Palm Tree Test (PPTT) (n = 7; 63.63%). Other tasks were used. Nonetheless, their level of evidence was under 50%: naming task (n = 4; 36.36%), counting task (n = 2; 1.82%), and reading and writing tasks (n = 1; 0.9%).
3.2.2 Spatial cognition
The line bisection test was the gold standard task used to evaluate spatial cognition (n = 10; 100%). A lesser level of evidence was found using cancellation tasks (n = 1; 10%) and Milner landmark test (n = 1; 10%).
3.2.3 Social cognition
Mentalizing and emotional processing were mainly assessed by Reading the Mind in the Eyes (RME) (n = 9). This test showed the strongest level of evidence (70.31%). The expression recognition test (n = 3; 23.44%), the false belief (n = 1; 7.81%), comic strips (n = 1; 7.81%), and the Japanese facial expression of basic emotions series by Matsumoto and Ekman (1989) (n = 1; 7.81%) were also described in the reviewed articles. Notice that the latter task was used in one article (4) rather than RME. The authors argued that cultural biases influenced the interpretation of Western emotional gestures by the Asian participants in the study.
3.2.4 Motor/sensory functions
The dual task (naming task + limb movements) showed a high level of evidence (75%) due to this task being performed in all articles that evaluated cognitive processes. Additionally, the movements of the upper and lower limbs (n = 4; 50%) showed a good level of evidence. A low level of evidence was found in sensorimotor tasks (n = 3; 37.5%). Finally, one article (28) provided the use of a simple test to evaluate hand function (n = 1; 12.5%), and another one (16) carried out intraoperatively a Hand Movement Task (HMt) (n = 1; 12.5%)
3.2.5 Executive functions
The N-back test (n = 5; 71.42%) and Stroop test (n = 4; 57.14) showed a good level of evidence. In a low level of evidence, the digit span (n = 2; 28.57%), Trail Making Test A/B (TMT A/B) (n = 2; 28.57%), short-term memory test (n = 1; 14.28%), and adapted version of the Stroop test (iST) (n = 1; 14.28) were employed.
3.3 Third analysis: pre- and post-operative outcomes
In this section, the post-operative results are examined in relation to the baseline of each pre-operative case.
3.3.1 Language and speech
Fourteen of the 31 selected articles for the systematic review included an assessment of semantic cognition and speech/language functions (n = 14; 48.27%) pre-operatively. Of these 14 articles, 11 described the pre-operative tasks used, and these included: fluency task (n = 4; 28.57%); naming task (n = 4; 28.57%); DO80 task (n = 3; 21.43%); reading and writing tasks (n = 2; 14.28%); the Boston Diagnostic Aphasia Examination (BDAE) (n = 1; 7.14%); counting task (n = 1; 7.14%); standard language test of aphasia (SLTA) (n = 1; 7.14%), and Montreal Evaluation of Communication protocol (MECP) (n = 1; 7.14%). Two articles (six and 13) reported semantic cognition and speech articulation disturbance (speech arrest) before surgery.
One article (7) did not describe the pre- and post-surgical examination. Similarly, one article (19) did not describe the pre-surgical examination. However, language post-op results were shared in article 19, with one patient showing a decline in naming and semantic tasks post-operatively. Articles 21 and 23 also described post-op decline in their sample. In article 21, there was a slight decline in verbal fluency tasks during the post-op assessment. In article 23, some patients experienced speech initiation disturbances post-op comparable to their original presentation during the days prior to surgery. Despite the initial worsening, all patients regained their linguistic skills at long-term follow-up (3 and 6 months post-op).
Transient language disorders such as mutism, phonetic paraphasia, anarthria, and semantic disturbances were observed in one article (30). While all patients who were normal pre-surgical developed speech or semantic language disturbance 24 hours after resection. These language disturbances disappeared by 7 days post-op. Three out of 13 articles (11, 18, 31) showed improvements in language tasks in comparison with the pre-op assessment between 1 week and 6 months post-op. Two studies (17 and 29) that reported speech arrest, anomia, and verbal semantic paraphasia pre-operatively experienced an improvement in language tasks immediately after surgery. Articles 6, 10, and 26 did not describe postsurgical outcomes, and article 27 did not examine the results of post-op language testing.
In addition to this information, it is important to note that five of the 13 (5, 6, 11, 24, and 31) articles that analyzed language pre and post-operatively reported results about the percentage of the brain tissue resected during the surgical procedure. In articles 11 and 24, a supratotal resection (> 100%) was performed. A gross resection was carried out in articles 5 and 6 (86.6 and 92.8%, respectively). In article 31, only 59.6% of the tumor was removed.
3.3.2 Spatial cognition
Seven out of 31 articles performed spatial cognitive testing pre-operatively (25.93%). Three articles (3, 19, and 22) showed visuospatial and attentional deficits in the pre-operative period; two studies (14 and 16) reported non-spatial cognition impairments prior to surgery, and one (1) did not describe the results of the pre-op assessment in spatial cognition.
Among studies that reported on spatial cognitive testing, the most used task was the line bisection task (n = 5; 71.43%). To a lesser degree, clock drawing (n = 2; 28.57%) and bell cancellation (n = 2; 28.57%) were used. Only one article described the use of the letter cancellation task (n = 1; 14.28%), Raven Matrices (n = 1; 14.28%), figure copy (n = 1; 14.28%), and Visual Object and Space Perception Battery (VSOP) (n = 1; 14.28%).
The post-operative evaluation results were systematically described in all studies. Articles 3 and 19 described significant improvement pre- to post-operatively in visuospatial cognition tasks (Table 4). Improvement in line bisection was noted 3 months after surgery. Similar results were obtained in article 22, with improvement in spatial cognition tests reported.
Article 1 did not report any information about pre-operative neuropsychological outcomes, but the post-operative results were described. One week after the resection, there was a slight decline in performance on the clock drawing task (100–77.7%). This decline was also observed in articles 15 and 27. However, these disturbances were transient and resolved 3 months after the resection.
The extent of resection was described in five out of six articles that assessed spatial cognition pre- and post-operatively. The percentage of tissue resection was more than 90% in articles 1 (95.53%) and 22 (94.4%). Articles 19 and 25 only reported the type of resection (gross, subtotal, or partial resection).
3.3.3 Social cognition
Social cognition was analyzed pre-operatively in seven of the 31 (n = 7; 25.92%) articles selected. Articles 12, 13, 20, and 23 showed pre-operative impairments in mentalizing, and one article (4) found basic emotion deficits prior to surgery. Only one study (6) did not report mentalizing disturbances. Five out of the 31 articles that assessed social cognition detailed the measures used. RME was the gold standard test used to evaluate this cognitive process (n = 3; 60%). Other tasks described included picture arrangement tasks from the Weschler Adult Intelligence Scale (WAIS-III PA) (n = 1; 20%) and the Expression Recognition Test for Adults by Komatsu et al. (2012) (n = 1; 20%).
The post-operative outcome was described in three of the articles reviewed. Four studies (11, 13, 19, and 23) did not report information about the neuropsychological follow-up. In articles 12 and 20, similar impairments in mentalizing pre- and 24 h to 1 week post-operatively were noted. Article 4 reported similar results. Nonetheless, all the disturbances exhibited in articles 12, 20, and 4 were transient, with improvements seen by 3 months post-op.
Regarding the extent of resection, one article (4) described a complete resection (100%) in two patients, and two articles (20 and 22) reported the removal of more than 90% of the tumor (93.3 and 94.29%, respectively). Article 12 reported 75.7% of the tumor resected, and article 13 noted 59.11% extent of resection.
3.3.4 Motor/sensory functions
Motor/sensory functions were assessed pre-operatively in 18.52% (n = 6) of the articles reviewed in the present study. Two articles (11 and 24) reported motor impairment pre-operatively, while four articles (9, 16, 21, and 28) did not report any motor disturbances prior to surgery. Four out of six articles described the tasks used, which included the movement of the upper and lower limbs (n = 4; 80%) and the Hand Strength Scale (n = 1; 20%), and only one article (16) did not report the tasks used pre-operatively.
The post-operative outcome was described in all articles except article 11. All studies reported transient motor disturbances, including paresis; one article (16) described a significantly lower incidence of ideomotor apraxia 1 week post-op. Even in studies (9, 21, and 28) in which the pre-operative assessment did not describe motor impairments, temporary deficits were noted immediately after surgery. Nevertheless, these disturbances disappeared between 3 and 6 months post-op.
Only three studies (11, 16, and 24) reported the extent of resection (>93%) (see Language section and Table 4 for more information about articles 11 and 24).
3.3.5 Executive functions
Executive functions, such as inhibition and working memory, were evaluated prior to surgery in 27.59% (n = 9) of the articles reviewed. One out of four studies (4) described cognitive flexibility deficits. One other article (1) reported more general executive function impairments, and article 14 described the absence of language and visual deficits. Articles 11 and 22 did not report executive function results pre-operatively.
The tasks used during the pre-operative phase were described in all the studies. The most used task was the N-back test, administered in four out of nine articles (50%). The Stroop test and the TMT were employed in 37.5 % (n = 3) of the articles. Digit symbol substitution (n = 2; 25%), digit span test (n = 2; 25%), Rey-Osterrieth complex figure (n = 2; 25%), cognitive estimations (n = 1; 12.5%), and the Weschler Memory Scale-Revised Edition (WMS-R) (n = 1; 12.5%) were used, but to a lesser degree.
Post-operative neuropsychological assessment was carried out in four articles. Only one study (22) did not report results on executive functions. One study (11) described an improvement in the mean scores of the WMS-R during the post-op phase (6 months after surgery), and another article (14) reported a reduction of executive function deficits 7 days post-op. Three studies (1, 2, 8) showed a decline in executive functions after surgery. One article (1) reported a worsening in cognitive estimations. In an article (2), 22.72% of patients exhibited a decrement in TMT. Similarly, 9.09% of patients showed worse performance on the Stroop test immediately after surgery. However, recovery was seen at 3 and 18 months post-op. Article 8 reported a worsening in Stroop performance with improvement by 1 month post-surgery.
Three articles (11, 14, and 22) showed resection data (>85%) (see Table 4 for more information).
4 Discussion
This study examines the neuropsychological assessment tools used to map right hemisphere functions during awake brain surgery over the past 15 years. It emphasizes the need for carefully chosen tasks for intraoperative assessment of right hemisphere functions and systematic use of pre- and post-operative assessments to enhance the understanding of cognitive and emotional processes related to right cortical-subcortical structures. The study contributes to a deeper appreciation of the functional anatomy of the right hemisphere for neurosurgeons and neuropsychologists participating in awake brain surgeries. What follows is a discussion of the most common functions evaluated and tasks used during right hemisphere resections.
4.1 Language and speech
Language and speech are by far the most tested cognitive domains in awake brain surgery. Almost 50% of the studies included in this review describe a test or test paradigm for the assessment of language and speech functions within the right hemisphere. Simple tasks like counting and more complex assessments such as semantic associations or translation skills are employed to monitor speech processing and language functions. Standardized neuropsychological tests, including DO80 (Deloche and Hannequin, 1997), are commonly used. The DO80 task, especially, exhibits strong evidence (81.81%) at the intraoperative level, effectively assessing a range of language disorders. For intraoperative assessment of verbal and non-verbal semantic cognition, PPTT is frequently employed (54.54%). In the study conducted by Herbet et al. (2018), PPTT was used in addition to the DO80 task. They wanted to analyze semantic paraphasia because the main aim of their study was to investigate the contribution of prefrontal structures to semantic processing but not to other language-related processes. Employing only the DO80 task was not enough to describe the semantic processing. Consequently, a combination of DO80 and PPTT is proposed as the gold neuropsychological standard to assess key language processes.
While language processing in the left hemisphere is well-established, the role of the right hemisphere remains debated. Evidence suggests the right hemisphere is involved in core language functions, challenging traditional views. The revisited model of language processing, proposed by Herbet and Duffau (2020), identifies a dual route: the dorsal phonological stream and the ventral semantic route. The dorsal stream comprises deep and superficial components. The deep component corresponds to the connections between the posterior temporal structures (MTG and ITG) and the IFG (mostly the frontal operculum), but also the most ventral part of DLPFC (Martino et al., 2010) by the AF white matter fibers. The superficial component of the dorsal route is underlain by the lateral part of the SLF III for articulatory processing. These cortical-subcortical positive sites are described by two articles: Herbet et al. (2018) for verbal semantic processing in the left hemisphere and for non-verbal semantics in the left and right hemispheres, and Zacà et al. (2018) for speech articulation. The cortical mapping results showed semantic paraphasia, phonological paraphasia, and speech arrest, respectively, during the intraoperative electrical stimulation of the right hemisphere. Nevertheless, these results were found in a much lower proportion in comparison with the data obtained in the left hemisphere. Of note, the FAT is also involved in speech initiation as well as in speech control (Dick et al., 2019). One article selected for the current systematic review (Kinoshita et al., 2014) is consistent with this fact. The authors describe FAT as a core of speech control due to the appearance of “speech initiation disturbances” during DES.
The ventral route, involving the IFOF, the inferior longitudinal fasciculus (ILF), and the uncinate fasciculus (UF), plays a role in verbal and non-verbal semantic processing. One article used in this systematic review (Herbet et al., 2017) agrees with these neuroanatomical findings within the right hemisphere. In this study, the authors found direct evidence for the role of the right IFOF in non-verbal semantic cognition, assessed by means of the PPTT. This finding confirms the homotypic organization of the non-verbal semantic network at the white matter level, consistent with the proposition made by Herbet et al. (2018) at the cortical level.
Language and speech disorders may arise post-operatively, emphasizing the need for language mapping in both hemispheres to prevent lasting impairments. The complexity of the brain's language network necessitates comprehensive assessment and mapping to ensure optimal outcomes.
4.2 Spatial cognition
Attention plays an important role in our daily lives, and the asymmetries of attentional networks that favor the right hemisphere (RH) are significant (Nobre, 2001; Corbetta and Shulman, 2002; Mandonnet and Herbet, 2021). Thus, dysfunction in these networks within the RH can lead to serious consequences. Impairments in attentional processes can impact many cognitive functions and behaviors, affecting an individual's ability to focus, perceive, and respond. Visual neglect is the dramatic clinical consequence of attention network dysfunction.
Spatial neglect or attentional disturbances are commonly assessed by several tests that can be broadly categorized into visuo-perceptual tests, visuo-graphic tests, and representational tests (Bartolomeo and Mandonnet, 2021). All these tasks were conducted in the articles reviewed in the present study. Even though it is remarkable that this cognitive domain is tested, sometimes with just one test (for example, only cancellation tasks), the line bisection task could be considered the gold standard test used to assess spatial cognition due to its level of evidence (100%). Consequently, this finding strongly reinforces the recommendation to include the line bisection task as part of the monitoring process during right parietal lobe surgeries.
Line bisection cortical positive sites seem to be highly variable from one patient to another, and when pooling all data from the literature, there is currently no more specific localization than the whole right parietal lobe (Bartolomeo and Mandonnet, 2021). Despite these findings, we found in the reviewed articles other positive cortical sites out from the parietal lobe, such as the precentral gyrus, the supramarginal gyrus, and motor areas. At the white matter level, electrostimulation studies have yielded consistent evidence suggesting the critical role of frontoparietal connections, supported by the SLF II and arcuate fasciculus pathways, in spatial awareness (Thiebaut de Schotten et al., 2005; Roux et al., 2011; Vallar et al., 2014). Several reports also observed a contribution from the IFOF (Herbet et al., 2017). These latter findings are consistent with the results obtained by the intraoperative stimulation of these white matter fibers performed in the spatial cognition articles selected for the present systematic review.
Other tasks beyond the line bisection task have been proposed as useful for mapping the networks involved in spatial attention, particularly cancellation-like tasks. While the line bisection task primarily evaluates the perceptual aspect of neglect, typically associated with parietal lesions, the cancellation task demands intentional exploration and attention orientation toward the contralesional space, a cognitive process rooted in the dorsal attention network (DAN), notably the eye field network. However, it is worth noting that a comprehensive lesion mapping study involving a cohort of patients with lower-grade glioma revealed that, despite resections targeting the medial eye field areas and their underlying connectivity or areas close to the frontal eye field, resulting in visuo-exploratory neglect, the deficit was transient (Herbet and Duffau, 2019). Since spatial cognition mapping with a cancellation task was not conducted in these areas, it raises questions about the additional utility of such tasks alongside the line bisection task.
4.3 Social cognition
Social cognition is thought to be supported by three anatomically separated but functionally interactive networks—the face perception network, the ‘mirror' neuron network, and mentalizing network (Keysers and Gazzola, 2007; Lieberman, 2007; Grill-Spector and Weiner, 2014; Pan et al., 2018; Wang et al., 2018). Mentalizing (or theory of mind) is fundamentally defined as the distinctively human tendency to attribute mental states (e.g., intentions, motives, and beliefs) to others based on observable behaviors and contextual information (Premack and Woodruff, 1978; Brothers, 1990). Mentalizing allows one to understand and anticipate others' behaviors and attitudes and to adjust one's own behavior in return.
Mentalizing is mainly assessed by the Read the Mind in the Eyes (RME; Baron-Cohen et al., 2001) test. The articles in the current systematic review relied heavily on this task, and they provided a high level of evidence (62.5%) supporting the importance of its use intraoperatively. RME should not be considered as a unique assessment of this cognitive function but rather a preferential gauge of social cognition.
The cortical areas involved in mentalizing-related processes include the dorsal and ventral aspects of the medial prefrontal cortex and the posterior cingulate cortex along with the precuneus (medially); the temporoparietal junction along with the posterior superior temporal sulcus, the IFG (laterally); and the temporal pole and its neighboring amygdala (less centrally) (Frith and Frith, 2003; Amodio and Frith, 2006; Carrington and Bailey, 2009; Van Overwalle and Baetens, 2009; Schurz et al., 2014). Likewise, it has been observed the important risk of generating long-term deficits in social cognition if there is a structural disconnection of the temporo-occipital areas and their connections via the ILF (Berro et al., 2021; Ekert et al., 2024). The white matter connections of the mentalizing system are, to date, understudied. However, a handle of studies has suggested that the white matter tracts that play a central role are the SLF/AF, the IFOF, and the cingulum (Herbet et al., 2014, 2016; Yordanova et al., 2017; Nakajima et al., 2018a,b; Roux et al., 2021). For example, Yordanova et al. (2017) explained that, cortically, the mapping results not only confirmed the involvement of the posterior part of the inferior frontal gyrus but also unveiled a pivotal role of the posterior dorsolateral prefrontal cortex, along with, to a lesser extent, the superior temporal gyrus (posterior part). Critically, numerous sites were also identified in the white matter underneath the dorsolateral prefrontal cortex and the middle and superior temporal gyri. The disconnection analyses performed on the axonal stimulation dataset demonstrated that fibers of the IFOF and the SLF/AF had the highest probabilities of being disconnected during subcortical stimulation. Additionally, Nakajima et al. (2018a,b), besides identifying positive cortical sites (IFG and SFG), found that not only the SLF/AF and IFOF are important in this process of social cognition. They found that FST and FAT have a significant contribution to specific aspects of mentalizing.
Some studies related to social cognition described deficits after the resection phase (Herbet et al., 2014; Yordanova et al., 2017; Roux et al., 2021). Although neuro-oncological studies suggest that surgical resections do not have a persistent detrimental effect on social cognition abilities, lesion mapping studies provide different results by showing degraded performances in social cognition abilities a few months after surgery. This discrepancy in results could be attributed to the fact that neuro-oncological studies typically do not employ a comprehensive array of neuroanatomical analyses (Nakajima et al., 2021).
4.4 Motor/sensory functions
Preventing motor impairments is one of the foremost considerations in brain tumor surgery, especially when the tumor is in proximity to the primary motor cortex and its associated descending nerve fibers. Consequently, cortical and subcortical brain mapping is often used to guide resection (Bello et al., 2021).
Tests for motor or sensory functions are less frequently mentioned. Many studies report that they monitor sensorimotor functions, but this is mostly done by asking a patient to report any sensations or movements (Rech et al., 2016, 2019; Motomura et al., 2018), and no specific task or paradigm is administered. Motor functions are also often monitored by motor-evoked potentials. Shinoura et al. (2010) and Rossi et al. (2018) describe the recently developed Hand Manipulation-Task (hMT), which requires the patient to perform a rotational movement on a tool shaped like a screwdriver. Many of the studies in this systematic review employed a dual task (75%), or in some of the articles, the neuropsychologist asked the patients to move the upper and lower limbs (50%). This renders these tasks the primary ones used in monitoring motor functions during right awake surgery. From a surgical viewpoint, specific patterns of positive or negative motor phenomena (both behavioral and EMG) are associated with different cortical-subcortical brain areas. Intraoperative DES applied over M1 causes negative responses. Additionally, the same negative responses were obtained after electrical stimulation of the dorsal premotor cortex (dPMC).
The SMA is linked to IFG and the ventral section of the precentral gyrus via the frontal aslant tract (FAT). Furthermore, the SMA, along with the dPMC and the ventral premotor cortex (vMPC), connects to the caudate nucleus through the fronto-striatal tract (FST) (Bello et al., 2021). The studies conducted by Kinoshita et al. (2014) and Rech et al. (2016) agree with these facts. In these articles, patients showed slight left or right paresis and “initiation disturbances” during DES applied over FAT and FST of the right hemisphere.
In most of the studies reviewed, the motor deficits were not permanent and tended to recover during the first 3 months (Shinoura et al., 2010; Kinoshita et al., 2014; Rech et al., 2016).
4.5 Executive functions
Executive functions (EFs), also known as executive control or cognitive control, encompass a set of top-down mental processes essential for concentration and attention, problem-solving, or behavioral control. There is general agreement that there are three core EFs (Miyake et al., 2000; Lehto et al., 2003): inhibition, working memory, and cognitive flexibility (also called set shifting).
The most studied EFs in the current systematic review are working memory and inhibitory control. Therefore, we will only describe the most significant findings related to these executive functions. In clinical settings, diverse tests address inhibitory mechanisms: go-on-go task or the stop-signal reaction-time task (Diamond, 2013; Motomura et al., 2018). However, the most used task is the N-back test. In the present systematic review, this task was employed to assess working memory in 57.14% of studies. The N-back test and the Stroop test have a good level of evidence. It could be interesting to add these tasks in the intraoperative protocol to evaluate working memory during right awake surgeries.
From a surgical viewpoint, intraoperative electrical stimulation has revealed some of the different networks sustaining these complex functions. In inhibitory control, the DLPFC seems to be crucial in the modulation of these processes. Motomura et al. (2018) obtained consistent results with this hypothesis in their study. In addition to this cortical region, they found the same disturbances during electrical stimulation of SFG. At the subcortical level, the right FAT could play a role in inhibitory control due to these white fibbers allowing the connection between the IFC and pre-SMA (Dick et al., 2019). Motomura et al. (2018) and Puglisi et al. (2019) agree with this fact. They found that the white matter direct stimulation highlighted the involvement of FAT in inhibitory control. Additionally, the involvement of SLF and AF in inhibitory control and cognitive flexibility seems to be clear. The study conducted by Hartung et al. (2021) confirmed that the right SLF and AF contributed to impairments in set-shifting and inhibition.
The current literature provides some evidence of long-lasting surgical deficits related to EFs. This fact indicates the necessity of assessing these high-order functions pre-, intra-, and post-operatively to avoid the high impact disturbances in the patient's quality of life.
4.6 Pre-, intra-, and post-operative neuropsychological assessment
The findings of the present systematic review underscore the critical importance of neuropsychological assessment before, during, and after awake craniotomy. Pre-operative evaluation establishes the patient's baseline neuropsychological profile, determining suitability for awake brain craniotomy and guiding intraoperative tasks (Hande et al., 2021). During surgery, neuropsychological tasks aid in directing the resection of brain tissue damage to optimize oncological outcomes (Kelm et al., 2017; Herbet and Duffau, 2020). The reviewed studies revealed resection percentages ranging from 70 to 100%, emphasizing the need to understand the networks involved in cognitive and emotional processing. Intraoperative neuropsychological assessments enable personalized resections within individual functional limits, fostering the development of functional neuro-oncology and connectome-based neurosurgery. Brain lesions can significantly impact functional connectivity, and disruptions in anatomical connectivity are well-documented (He et al., 2007; Griffis et al., 2019). The meta-networking approach, exploring how functional networks communicate and reconfigure in response to behavioral demands, offers a novel perspective (Herbet and Duffau, 2020). This approach may guide the selection of rehabilitation strategies to enhance between-network communication, leading to improved post-operative performance and a higher quality of life for patients.
4.7 Refining functional mapping of the right hemisphere
To refine the functional mapping of the right hemisphere during awake brain surgery, several strategies can be implemented to enhance the assessment of cognitive functions and improve the understanding of brain organization. Applying a comprehensive neuropsychological examination allows for a detailed evaluation of various cognitive domains, including visuospatial abilities, language processing, memory, social cognition, and sensory/motor functions (Strauss et al., 2006). By employing a wide range of standardized neuropsychological tests tailored to specific cognitive functions, clinicians can obtain a more nuanced understanding of the patient's cognitive profile and identify areas of potential functional impairment. Additionally, conducting longitudinal studies to assess functional recovery post-surgery can help identify which functions may not fully recover. Through the assessment of cognitive outcomes at various time intervals, researchers can ascertain the trajectory of recovery across different cognitive domains and obtain insights into the long-term effects of surgery on cognitive function. This longitudinal approach can inform treatment planning and rehabilitation strategies for patients with persistent cognitive deficits (Sala-Lonch et al., 2015; Gondar et al., 2021). Similarly, adapting tasks for mapping uncompensated functions in the right hemisphere is crucial for accurately identifying areas of cognitive vulnerability. Designing tasks that specifically target cognitive functions known to be challenging for the right hemisphere and incorporating sensitive measures of cognitive performance can effectively identify critical brain regions and assess functional integrity (Kelm et al., 2017; Herbet and Duffau, 2020). Tailoring tasks to probe specific cognitive processes enhances the accuracy of functional mapping and improves the identification of areas requiring preservation during surgery (Bates et al., 2003; Trimble et al., 2015). By incorporating these strategies into the assessment and mapping of right hemisphere functions during awake brain surgery, clinicians and researchers can refine their understanding of cognitive organization in the brain, heighten surgical outcomes, and enhance the quality of care for patients undergoing complex neurosurgical procedures.
4.8 Strengths and limitations of the study
The study exhibits notable strengths alongside certain limitations. It features a rigorous and comprehensive systematic search process, utilizing specific search terms and Boolean operators across multiple databases to identify relevant articles. This approach enhances the overall reliability of the literature review. Additionally, the study conducts in-depth analyses of selected articles, focusing on key variables related to cognitive and emotional functions during awake brain surgery, contributing to a thorough understanding of the research question. It also focuses on various cognitive functions, such as visuospatial abilities, language processing, memory, social cognition, and sensory/motor processes during awake brain surgery, allowing for a nuanced exploration of specific cognitive domains. Furthermore, it proposes a valuable protocol for assessing cognitive and emotional functions during awake brain surgeries, outlining six crucial tasks designed to evaluate different cognitive processes. This protocol can act as a foundational resource for guiding future research endeavors in this area. Moreover, the analysis of neural correlates associated with different cognitive functions assessed during awake brain surgery adds another layer of depth to the study, providing valuable insights into the underlying neural basis of cognitive processes within the unique context of brain surgery.
Despite these strengths, it is important to recognize the limitations of the study. Potential selection bias, which arises from a narrow focus on patient populations (adults with gliomas in the right hemisphere) who underwent awake craniotomies with direct electrical stimulation (DES), could restrict the applicability of the results to a wider population undergoing brain surgery. Methodological differences among the studies included variations in sample sizes, handedness, the use of diverse cognitive tasks, and the stimulation sites not specified in most of the selected articles, introducing complexities that could impact the comparability and integration of results. Additionally, inter-individual variability in plasticity potential, topographical bias due to neuroplasticity, and heterogeneity in glioma pathology (low-grade glioma vs. high-grade glioma) underscore the need for caution in interpreting results, considering individual differences, validating task sensitivity, addressing neuroplastic changes, and accounting for tumor characteristics. Understanding these limitations is essential for refining mapping techniques, optimizing patient outcomes, and advancing our understanding of brain plasticity in neurosurgical contexts.
In summary, considering both the advantages and drawbacks highlighted in this systematic review, clinicians and researchers can approach a more nuanced understanding of the insights regarding the right hemisphere awake brain surgery and its cognitive functions. This comprehension can then steer forthcoming research endeavors and enhancements in methodology within this domain.
5 Conclusions
This review examines visuospatial, language, memory, social cognition, and sensory/motor processes, along with corresponding neural structures, assessed during right awake craniotomy with direct electrical stimulation (DES) in adult glioma patients over the past 15 years. Analyzing high-impact journals, the present study challenges traditional views by revealing mirror brain circuits in the right hemisphere, emphasizing a distributed yet specialized network perspective. Dynamic interactions among these circuits lead to varied outcomes and neuroplastic phenomena, underscoring the importance of understanding the right hemisphere's functional anatomy in tumor surgery.
This systematic review proposes a protocol for assessing cognitive and emotional functions during right awake brain surgeries, identifying crucial tasks (DO80, PPTT, line bisection task, dual task, movements of the upper and lower limbs, RME, Stroop test, and N-back test) for language, spatial cognition, social cognition, motor/sensory functions, and executive functions. Implementing these tasks in a right hemisphere craniotomy protocol is deemed essential to prevent intraoperative injuries and post-operative effects, ensuring a comprehensive evaluation. These findings contribute to a better understanding of neuropsychological assessment within brain plasticity, emphasizing the need for careful task selection during intraoperative processes to prevent cognitive and emotional deficits and enhance patients' quality of life post-tumor resection.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
IM-M: Conceptualization, Formal analysis, Investigation, Supervision, Validation, Writing – original draft, Writing – review & editing. LA-C: Data curation, Formal analysis, Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing. DS: Writing – review & editing. GH: Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Amodio, D. M., and Frith, C. D. (2006). Meeting of minds: the medial frontal cortex and social cognition. Nat. Rev. Neurosci. 7, 268–277. doi: 10.1038/nrn1884
Baron-Cohen, S., Wheelwright, S., Hill, J., Raste, Y., and Plumb, I. (2001). The “Reading the Mind in the Eyes” Test revised version: a study with normal adults, and adults with Asperger syndrome or high-functioning autism. J. Child Psychol. Psychiatry 42, 241–251. doi: 10.1111/1469-7610.00715
Bartolomeo, P. (2006). A parietofrontal network for spatial awareness in the right hemisphere of the human brain. Arch. Neurol. 63, 1238–1241. doi: 10.1001/archneur.63.9.1238
Bartolomeo, P., and Mandonnet, E. (2021). “Spatial cognition,” in Intraoperative Mapping of Cognitive Networks: Which Tasks for Which Locations. 1st Edn, eds. E. Mandonnet, and G. Herbet (Montpellier: Springer International Publishing).
Bates, E., Wilson, S. M., Saygin, A. P., Dick, F., Sereno, M. I., Knight, R. T., et al. (2003). Voxel-based lesion–symptom mapping. Nat. Neurosci. 6, 448–450. doi: 10.1038/nn1050
Bello, L., Freyshclag, C. F., and Rech, F. (2021). “Motor control,” in Intraoperative Mapping of Cognitive Networks: Which Tasks for Which Locations, 1st Edn, eds. E. Mandonnet, and G. Herbet (Montpellier: Springer International Publishing).
Berro, D. H., Herbet, G., and Duffau, H. (2021). New insights into the anatomo-functional architecture of the right sagittal stratum and its surrounding pathways: an axonal electrostimulation mapping study. Brain Struct. Funct. 226, 425–441. doi: 10.1007/s00429-020-02186-4
Brothers, L. (1990). The social brain: a project for integrating primate behavior and neurophysiology in a new domain. Concepts Neurosci. 1, 27–61.
Carrington, S. J., and Bailey, A. J. (2009). Are there theory of mind regions in the brain? A review of the neuroimaging literature. Hum. Brain Mapp. 30, 2313–2335. doi: 10.1002/hbm.20671
Charras, P., Herbet, G., Deverdun, J., Menjot de Champfleur, N., Duffau, H., Bartolomeo, P., et al. (2015). Functional reorganization of the attentional networks in low-grade glioma patients: a longitudinal study. Cortex 63, 27–41. doi: 10.1016/j.cortex.2014.08.010
Corbetta, M., and Shulman, G. L. (2002). Control of goal-directed and stimulus-driven attention in the brain. Nat. Rev. Neurosci. 3, 201–215. doi: 10.1038/nrn755
De Witt Hamer, P. C., Robles, S. G., Zwinderman, A. H., Duffau, H., and Berger, M. S. (2012). Impact of intraoperative stimulation brain mapping on glioma surgery outcome: a meta-analysis. J. Clin. Oncol. 30, 2559–2565. doi: 10.1200/JCO.2011.38.4818
Deloche, G., and Hannequin, D. (1997). Test de dénomination orale d'images: DO 80. Paris: Éditions du Centre de psychologie appliquée.
Diamond, A. (2013). Executive functions. Annu. Rev. Psychol. 64, 135–168. doi: 10.1146/annurev-psych-113011-143750
Dick, A. S., Garic, D., Graziano, P., and Tremblay, P. (2019). The frontal aslant tract (FAT) and its role in speech, language and executive function. Cortex 111, 148–163. doi: 10.1016/j.cortex.2018.10.015
Duffau, H., Capelle, L., Sichez, N., Denvil, D., Lopes, M., Sichez, J.-P., et al. (2002). Intraoperative mapping of the subcortical language pathways using direct stimulations. An anatomo-functional study. Brain 125(Pt 1), 199–214. doi: 10.1093/brain/awf016
Duffau, H., Leroy, M., and Gatignol, P. (2008). Cortico-subcortical organization of language networks in the right hemisphere: an electrostimulation study in left-handers. Neuropsychologia 46, 3197–3209. doi: 10.1016/j.neuropsychologia.2008.07.017
Ekert, J. O., Sabsevitz, D. S., Martin Del Campo, I., Goyal, A., Gillespe, C. S., Middlebrooks, E. H., et al (2024). Awake brain mapping paradigms for the nondominant hemisphere gliomas. Neurosurg Focus. 56, E7. doi: 10.3171/2023.11.FOCUS23610
Frith, U., and Frith, C. D. (2003). Development and neurophysiology of mentalizing. Philos. Trans. R. Soc. Lond. Ser. B Biol. Sci. 358, 459–473. doi: 10.1098/rstb.2002.1218
Gianotti, G. (2012). Unconscious processing of emotions and the right hemisphere. Neuropsychologia 50, 205–218. doi: 10.1016/j.neuropsychologia.2011.12.005
Giussani, C., Pirillo, D., and Roux, F. E. (2010). Mirror of the soul: a cortical stimulation study on recognition of facial emotions. J. Neurosurg. 112, 520–527. doi: 10.3171/2009.5.JNS081522
Gondar, R., Patet, G., Schaller, K., and Meling, T. R. (2021). Meningiomas and cognitive impairment after treatment: a systematic and narrative review. Cancers 13:1846. doi: 10.3390/cancers13081846
Griffis, J. C., Metcalf, N. V., Corbetta, M., and Shulman, G. L. (2019). Structural disconnections explain brain network dysfunction after stroke. bioRxiv 28, 2527–2540.e9. doi: 10.1016/j.celrep.2019.07.100
Grill-Spector, K., and Weiner, K. S. (2014). The functional architecture of the ventral temporal cortex and its role in categorization. Nat. Rev. Neurosci. 15, 536–548. doi: 10.1038/nrn3747
Hande, V. H., Gunasekaran, H., Hedge, S., Shashidhar, A., and Arimappamagan, A. (2021). Role of the clinical neuropsychologists in awake-craniotomy. Neurol. India 69, 711–716. doi: 10.4103/0028-3886.319237
Hartung, S. L., Mandonnet, E., de Witt Hamer, P., Klein, M., Wager, M., Rech, F., et al. (2021). Impaired set-shifting from dorsal stream disconnection: insights from a European series of right parietal lower-grade glioma resection. Cancers 13:3337. doi: 10.3390/cancers13133337
He, B. J., Snyder, A. Z., Vincent, J. L., Epstein, A., Shulman, G. L., and Corbetta, M. (2007). Breakdown of functional connectivity in frontoparietal networks underlies behavioral deficits in spatial neglect. Neuron 53, 905–918. doi: 10.1016/j.neuron.2007.02.013
Herbet, G., and Duffau, H. (2019). “Awake craniotomy and bedside cognitive mapping in neurosurgery,” in Neurosurgical Neuropsychology, eds. C. M. Pearson, E. Ecklund-Johnson, and S. D. Gale (New York, NY: Elsevier), chapt. 7, 113–138.
Herbet, G., and Duffau, H. (2020). Revisiting the functional anatomy of the human brain: toward a meta-networking theory of cerebral functions. Physiol. Rev. 100, 1181–1228. doi: 10.1152/physrev.00033.2019
Herbet, G., Lafargue, G., Bonnetblanc, F., Moritz-Gasser, S., Menjot de Champfleur, N., and Duffau, H. (2014). Inferring a dual-stream model of mentalizing from associative white matter fibers disconnection. Brain 137(Pt 3), 944–959. doi: 10.1093/brain/awt370
Herbet, G., Maheu, M., Costi, E., Gilles, L., and Duffau, H. (2016). Mapping neuroplastic potential in brain-damaged patients. Brain 139 (Pt3), 829–844. doi: 10.1093/brain/awv394
Herbet, G., Moritz-Gasser, S., and Duffau, H. (2017). Direct evidence for the contribute role of the right inferior fronto-occipital fasciculus in non-verbal semantic cognition. Brain Struct. Funct. 222, 1597–1610. doi: 10.1007/s00429-016-1294-x
Herbet, G., Moritz-Gasser, S., and Duffau, H. (2018). Electrical stimulation of the dorsolateral prefrontal cortex impairs semantic cognition. Neurology 90, e1077–e1084. doi: 10.1212/WNL.0000000000005174
Kelm, A., Sollman, N., Ille, S., Meyer, B., Ringel, F., and Krieg, S. M. (2017). Resection gliomas with and without neuropsychological support during awake craniotomy-effects on surgery and clinical outcome. Front. Oncol. 7:176. doi: 10.3389/fonc.2017.00176
Keysers, C., and Gazzola, V. (2007). Integrating simulation and theory of mind: from self to social cognition. Trends Cogn. Sci. 11, 194–196. doi: 10.1016/j.tics.2007.02.002
Kinoshita, M., Menjot de Champfleur, N., Deverdun, J., Moritz-Gasser, S., Herbet, G., and Duffau, H. (2014). Role of fronto-striatal tract and frontal aslant tract in movement and speech: an axonal mapping study. Brain Struct. Funct. 220, 3399–3412. doi: 10.1007/s00429-014-0863-0
Komatsu, S., Nakamura, T., and Hakoda, Y. (2012). Expression Recognition Test for Adults. Hukuoka: Toyo Physical.
Krall, S. C., Rottschy, C., Oberwelland, E., Bzdok, D., Fox, P. T., Eickhoff, S. B., et al. (2015). The role of the right temporoparietal junction in attention and social interaction as revealed by ALE meta-analysis. Brain Struct. Funct. 220, 587–604. doi: 10.1007/s00429-014-0803-z
Lehto, J. E., Juujärvi, P., Kooistra, L., and Pulkkinen, L. (2003). Dimensions of executive functioning: evidence from children. Br. J. Dev. Psychol. 21, 59–80. doi: 10.1348/026151003321164627
Liberti, A., Altman, D. G., Tetzlaff, J., Mulrow, C., Gøtzche, P. C., Loannidis, J. P. A., et al (2009). The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 6:e1000100. doi: 10.1371/journal.pmed.1000100
Lieberman, M. D. (2007). Social cognitive neuroscience: a review of core processes. Annu. Rev. Psychol. 58, 259–289. doi: 10.1146/annurev.psych.58.110405.085654
Mandonnet, E., and Herbet, G., (eds.). (2021). Intraoperative Mapping of Cognitive Networks: Which Tasks for Which Locations. 1st Edition. Montpellier: Springer International Publishing.
Martino, J., Brogna, C., Robles, S. G., Vergani, F., and Duffau, H. (2010). Anatomic dissection of the inferior fronto-occipital fasciculus revisited in the lights of brain stimulation data. Cortex 46, 691–699. doi: 10.1016/j.cortex.2009.07.015
Matsumoto, D., and Ekman, P. (1989). American-Japanese cultural differences in judgments of facial expressions of emotion. Motiv. Emot. 13, 143–157.
Miyake, A., Friedman, N. P., Emerson, M. J., Witzki, A. H., Howeter, A. H., and Wager, T. D. (2000). The unity and diversity of executive functions and their contributions to complex “Frontal Lobe” tasks: a latent variable analysis. Cogn. Psychol. 41, 49–100. doi: 10.1006/cogp.1999.0734
Moher, D., Liberti, A., Tetzlaff, J., Altman, D. G., and The PRISMA Group (2009). Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 6:e1000097. doi: 10.1371/journal.pmed.1000097
Motomura, K., Chalise, L., Ohka, F., Aoki, K., Tanahashi, K., Hirano, M., et al. (2018). Supratotal resection of diffuse frontal lower grade gliomas with awake brain mapping, preserving motor, language, and neurocognitive functions. World Neurosurg. 119, 30–39. doi: 10.1016/j.wneu.2018.07.193
Nakada, M., Nakajima, R., Okita, H., Nakade, Y., Yuno, T., Tanaka, S., et al. (2021). Awake surgery for right frontal lobe glioma can preserve visuospatial cognition and spatial working memory. J. Neurooncol. 151, 221–230. doi: 10.1007/s11060-020-03656-9
Nakajima, R., Kinoshita, M., Miyashita, K., Okita, H., Genda, R., Yahata, T., et al. (2017). Damage of the right dorsal superior longitudinal fascicle by awake surgery for glioma causes persistent visuospatial dysfunction. Sci. Rep. 7:17158. doi: 10.1038/s41598-017-17461-4
Nakajima, R., Kinoshita, M., Okita, H., Liu, Z., and Nakada, M. (2021). Preserving right pre-motor and posterior prefrontal cortices contribute to maintaining overall basic emotions. Front. Hum. Neurosci. 15:612890. doi: 10.3389/fnhum.2021.612890
Nakajima, R., Kinoshita, M., Okita, H., Yahata, T., Matsui, M., and Nakada, M. (2018a). Neural networks mediating high-level mentalizing in patients with right cerebral hemispheric gliomas. Front. Behav. Neurosci. 12:33. doi: 10.3389/fnbeh.2018.00033
Nakajima, R., Yordanova, Y., Duffau, H., and Herbet, G. (2018b). Neuropsychological evidence for the crucial role of the right arcuate fasciculus in face-based mentalizing network: a disconnection analysis. Neuropsychologia 115, 179–187. doi: 10.1016/j.neuropsychologia.2018.01.024
Nobre, A. C. (2001). The attentive homunculus: now you see it, now you don't. Neurosci. Biobehav. Rev. 25, 477–496. doi: 10.1016/S0149-7634(01)00028-8
Pan, J., Zhan, L., Hu, C., Yang, J., Wang, C., Gu, L, et al. (2018). Emotion regulation and complex brain networks: association between expressive suppression and efficiency in the fronto-parietal network and default-mode network. Front. Hum. Neurosci. 12:70. doi: 10.3389/fnhum.2018.00070
Prat-Acín, R., Galeano-Senabre, I., López-Ruiz, P., Ayuso-Sacido, A., and Espert-Tortajada, R. (2021). Intraoperative brain mapping of language, cognitive functions, and social cognition in awake surgery of low-grade gliomas located in the right non-dominant hemisphere. Clin. Neurol. Neurosurg. 200:106363. doi: 10.1016/j.clineuro.2020.106363
Premack, D., and Woodruff, G. (1978). Does a chimpanzee have a theory of mind. Behav. Brain Sci. 1, 515–526. doi: 10.1017/S0140525X00076512
Puglisi, G., Howells, H., Sciortino, T., Leonetti, A., Rossi, M., Conti Nibali, M., et al (2019). Frontal pathways in cognitive control: direct evidence from intraoperative stimulation and diffusion tractography. Brain 142, 2451–2465. doi: 10.1093/brain/awz178
Puglisi, G., Sciortino, T., Rossi, M., Leonetti, A., Fornia, L., Conti Nibali, M., et al (2018). Preserving executive functions in nondominant frontal lobe glioma surgery: an intraoperative tool. J. Neurosurg. 131, 474–480. doi: 10.3171/2018.4.JNS18393
Rech, F., Herbet, G., Gaudeau, Y., Mézières, S., Moureau, J. M., Moritz-Gasser, S., et al. (2019). A probabilistic map of negative motor areas of the upper limb and face: a brain stimulation study. Brain 142, 952–965. doi: 10.1093/brain/awz021
Rech, F., Herbet, G., Moritz-Gasser, S., and Duffau, H. (2016). Somatotopic organization of the white matter tracts underpinning motor control in humans: an electrical stimulation study. Brain Struct. Funct. 221, 3743–3753. doi: 10.1007/s00429-015-1129-1
Robertson, I. H. (2014). Right hemisphere role in cognitive reserve. Neurobiol. Aging 35, 1375–1385. doi: 10.1016/j.neurobiolaging.2013.11.028
Rolland, A., Herbet, G., and Duffau, H. (2018). Awake surgery for gliomas within the right inferior parietal lobule: new insights into the functional connectivity gained from stimulation mapping and surgical implications. World Neurosurg. 112, e393–e406. doi: 10.1016/j.wneu.2018.01.053
Rossi, M., Fornia, L., Puglisi, G., Leonetti, A., Zuccon, G., Fava, E., et al (2018). Assessment of the praxis circuit in glioma surgery to reduce the incidence of postoperative and long-term apraxia: a new intraoperative test. J. Neurosurg. 130, 17–27. doi: 10.3171/2017.7.JNS17357
Roux, A., Lemaitre, A. L., Deverdun, J., Ng, S., Duffau, H., and Herbet, G. (2021). Combining electrostimulation with fiber tracking to stratify the inferior fronto-occipital fasciculus. Front. Neurosci. 15:683348. doi: 10.3389/fnins.2021.683348
Roux, F. E., Dufor, O., Lauwers-Cances, V., Boukhatem, L., Brauge, D., Draper, L., et al. (2011). Electrostimulation mapping of spatial neglect. Neurosurgery 69, 1218–1231. doi: 10.1227/NEU.0b013e31822aefd2
Sala-Lonch, R., Bartrés-Faz, D., and Junqué, C. (2015). Reorganization of brain networks in aging: a review of functional connectivity studies. Front. Psychol. 6:663. doi: 10.3389/fpsyg.2015.00663
Sanai, N., Mirzadeh, Z., and Berger, M. S. (2008). Functional outcome after language mapping for glioma resection. N. Engl. J. Med. 358, 18–27. doi: 10.1056/NEJMoa067819
Sarubbo, S., Tate, M., De Benedictis, A., Merler, S., Moritz-Gasser, S., Herbet, G., et al. (2020). Mapping critical cortical hubs and white matter pathways by direct electrical stimulation: an original functional atlas of the human brain. Neuroimage 205:116237. doi: 10.1016/j.neuroimage.2019.116237
Schurz, M., Radua, J., Aichhorn, M., Richlan, F., and Perner, J. (2014). Fractionating theory of mind: a meta-analysis of functional brain imaging studies. Neurosci. Biobehav. Rev. 42, 9–34. doi: 10.1016/j.neubiorev.2014.01.009
Shinoura, N., Yoshida, M., Yamada, R., Tabei, Y., Saito, K., Suzuki, Y., et al. (2010). Combined damage to the right hemispheric hand area in the primary motor and sensory area plays a critical role in motor hemineglect. Eur. Neurol. 63, 17–23. doi: 10.1159/000258636
Strauss, E., Sherman, E. M. S., and Spreen, O. (2006). A Compendium of Neuropsychological Tests: Administration, Norms, and Commentary, 3rd Edn. Oxford: Oxford University Press.
Tate, M. C., Herbet, G., Moritz-Gasser, S., Tate, J. E., and Duffau, H. (2014). Probabilistic map of critical functional regions of the human cerebral cortex: Broca's area revisited. Brain 137(Pt 10), 2773–2782. doi: 10.1093/brain/awu168
Thiebaut de Schotten, M., Urbanski, M., Duffau, H., Volle, E., Lévy, R., Dubois, B., et al. (2005). Direct evidence for a parietal-frontal pathway subserving spatial awareness in humans. Science 309, 2226–2228. doi: 10.1126/science.1116251
Tomasino, B., Guarracino, I., Lus, T., and Skrap, M. (2023). Continuous real-time neuropsychological testing during resection phase in left and right prefrontal brain tumors. Curr. Oncol. 30, 2007–2020. doi: 10.3390/curroncol30020156
Trimble, G., McStravick, C., Farling, P., Megaw, K., McKinstry, S., Smyth, G., et al. (2015). Awake craniotomy for glioma resection: technical aspects and initial results in a single institution. Br. J. Neurosurg., 29, 836–842. doi: 10.3109/02688697.2015.1054354
Vallar, G., Bello, L., Bricolo, E., Castellano, A., Casarotti, A., Falini, A., et al. (2014). Cerebral correlates of visuospatial neglect: a direct cerebral stimulation study. Hum. Brain Mapp. 35, 1334–1350. doi: 10.1002/hbm.22257
Van Overwalle, F., and Baetens, K. (2009). Understanding others' actions and goals by mirror and mentalizing systems: a meta-analysis. Neuroimage 48, 564–584. doi: 10.1016/j.neuroimage.2009.06.009
Vassal, M., Le Bars, E., Moritz-Gasser, S., Menjot, N., and Duffau, H. (2010). Crossed aphasia elicited by intraoperative cortical and subcortical stimulation in awake patients. J. Neurosurg. 113, 1251–1258. doi: 10.3171/2010.6.JNS10719
Vilasboas, T., Herbet, G., and Duffau, H. (2017). Challenging the myth of the right nondominant hemisphere: Lessons from corticosubcortical stimulation mapping in awake surgery and surgical implications. World Neurosurg. 103, 449–456. doi: 10.1016/j.wneu.2017.04.021
Wang, Y., Metoki, A., Alm, K. H., and Olson, I. R. (2018). White matter pathways and social cognition. Neurosci. Biobehav. Rev. 90, 350–370. doi: 10.1016/j.neubiorev.2018.04.015
Wijnenga, M. M. J., French, P. J., Dubbink, H. J., Dinjens, W. N. M., Atmodimedjo, P. N., Kros, J. M., et al. (2018). The impact of surgery in molecularly defined low-grade glioma: an integrated clinical, radiological, and molecular analysis. Neuro Oncol. 20, 103–112. doi: 10.1093/neuonc/nox176
Yordanova, Y., Duffau, H., and Herbet, G. (2017). Neural pathways subserving face-based mentalizing. Brain Struct. Funct. 222, 3087–3105. doi: 10.1007/s00429-017-1388-0
Zacà, D., Corisni, F., Rozzanigo, U., Dallabona, M., Avesani, P., Annicchiarico, L., et al. (2018). Whole-brain network connectivity underlying the human speech articulation as emerged integrating direct electric stimulation, resting state fMRI and tractography. Front. Human Neurosci. 12:405. doi: 10.3389/fnhum.2018.00405
Keywords: right hemisphere, awake surgery, direct electrical stimulation, cognitive mapping, neuropsychological protocol, intraoperative brain mapping, connectome
Citation: Martín-Monzón I, Amores-Carrera L, Sabsevitz D and Herbet G (2024) Intraoperative mapping of the right hemisphere: a systematic review of protocols that evaluate cognitive and social cognitive functions. Front. Psychol. 15:1415523. doi: 10.3389/fpsyg.2024.1415523
Received: 10 April 2024; Accepted: 03 June 2024;
Published: 20 June 2024.
Edited by:
Sara Bottiroli, University of Pavia, ItalyReviewed by:
Luca Zigiotto, Santa Chiara Hospital, ItalyAkira Midorikawa, Chuo University, Japan
Analía Arévalo, University of Sao Paulo Medical School, Brazil
Francesco Latini, Uppsala University, Sweden
Copyright © 2024 Martín-Monzón, Amores-Carrera, Sabsevitz and Herbet. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Isabel Martín-Monzón, aXNhYmVsbWFydGluQHVzLmVz