 François Bourgognon1*
François Bourgognon1* Denise Bechet2Cécile Huin-Schohn2Aurélia Strelow3Laëtitia Demarche1Mireille Guillou1
Denise Bechet2Cécile Huin-Schohn2Aurélia Strelow3Laëtitia Demarche1Mireille Guillou1 Virginie Adam1
Virginie Adam1 Estelle Fall3†Abdou Yacoubou Omorou3,4,5†
Estelle Fall3†Abdou Yacoubou Omorou3,4,5†- 1Department of Supportive Care in Oncology, Institut de Cancérologie de Lorraine, Vandæuvre-lès-Nancy, France
- 2Departement of Clinical Research, Institut de Cancérologie de Lorraine, Vandæuvre-lès-Nancy, France
- 3Université de Lorraine, Inserm, INSPIIRE, Nancy, France
- 4CIC-1433 Clinical Epidemiology, Nancy, France
- 5The French National Platform Quality of Life and Cancer, Nancy, France
Propose: This study aimed to propose an innovative, open, and circular program that combines acceptance and commitment therapy (ACT) and mindfulness practices. We assessed its feasibility, acceptability, and first signs of its effect on psychological wellbeing in cancer support treatment.
Methods: A single-center, single-arm, uncontrolled study was performed. Forty adult patients with non-metastatic prostate or breast cancer, newly diagnosed or undergoing treatment (chemotherapy, radiotherapy, hormone therapy), were recruited. Three cycles of three MAEva program sessions (MAEva: Mindfulness meditation, Acceptance, and Commitment to values program) over nine consecutive weeks were proposed. During the total of 12 weeks of follow-up, after attending the first session, patients were free to attend subsequent sessions.
Results: Adherence to the study was high, with participation in an average of 6.8 out of nine sessions. A total of eight patients attended all sessions over the three cycles, and 90% participated in at least one cycle. Furthermore, attendance was associated with a statistically significant improvement in Quality of Life (QoL). Each additional session was associated with a mean increase in overall QoL score of more than one point (β = 1.09 [0.13; 2.04], p = 0.02). The fatigue dimensions decreased with session attendance: physical (β = −2.24 [−3.63; −0.85]), emotional (β = −2.60 [−4.11; −1.09]), and interference with daily life (β = −2.33 [−3.95; −0.72]). The qualitative section demonstrated that patients learned skills and shared their ability to “let go”. Patients rated the degree of importance of the program at 8.36/10 (SD ± 1.64).
Conclusion: This study highlights the feasibility and acceptability of an original program that combines ACT and mindfulness practices in cancer patients. Future studies are required to demonstrate the efficacy of the MAEVA program. The MAEva pilot study is registered with ClinicalTrials.gov under the identifier NCT04751201.
Clinical trial registration: https://classic.clinicaltrials.gov/ct2/show/NCT04751201, identifier [NCT04751201].
Introduction
Cancer is one of the leading causes of morbidity and mortality worldwide, according to the World Health Organization (WHO). Cancer is associated with high levels of distress, particularly anxiety, depression, sleep disturbances, and fatigue (Pitman et al., 2018; Naser et al., 2021). These issues negatively affect patients' Quality of Life (QoL), social relationships, rehabilitation time, medication adherence, and illness behaviors (Artherholt and Fann, 2012; Fann et al., 2012; Grassi, 2020). Cancer patients face significant stressors throughout their care, starting with the wait and announcement of the diagnosis, the therapeutic decision, and the start of treatment. However, clinicians often have few resources to help patients manage stress and improve quality of life (Carlson et al., 2004, 2010; Sellick and Edwardson, 2007). To regulate stress, cancer patients are increasingly turning to complementary medicines and psychological interventions, including mindfulness practices (Huebner et al., 2014; Lyman, 2018; Carlson et al., 2019).
Mindfulness is defined as moment-to-moment awareness with an attitude of non-judgment, acceptance, and openness (Kabat-Zinn, 1990). Mindfulness practices, offered widely in North America and Europe in the form of 8-week programs such as Mindfulness-Based Stress Reduction (MBSR) (Kabat-Zinn, 1990), or Mindfulness-Based Cognitive Therapy (MBCT) (Segal et al., 2002), or Mindfulness-Based Cancer Recovery (MBCR) (Carlson and Speca, 2010), have shown their effectiveness in reducing distress and improving quality of life in cancer patients (Oberoi et al., 2020). For example, a recent meta-analysis of 29 randomized clinical trials of mindfulness-based therapies involving 3,476 cancer patients reported that the interventions reduced anxiety and depression, and improved fatigue, stress, and quality of life (Xunlin et al., 2020). Moreover, in other fields, mindfulness skills have been linked to satisfaction of the three fundamental psychological needs (i.e., autonomy, competence, and relatedness) defined by the self-determination theory (SDT, Ryan and Deci, 2000; Ataşalar and Michou, 2019; Rodríguez-Meirinhos et al., 2021). SDT postulates that satisfaction of one's needs in terms of autonomy (i.e., the feeling of having control of one's life and taking volitional, self-endorsed, and authentic actions), competence (i.e., the feeling of being able to use adaptative learning and having relevant skills to perform chosen actions), and relatedness (i.e., feeling of being included in positive social interactions based on reciprocal feelings of belonging with others) is related to enhanced quality of life and health behaviors (Ryan et al., 2008). In chronic diseases such as HIV, psychological need satisfaction mediated the relationship between mindfulness skills and sleep quality and had an impact on health-related quality of life (Campbell et al., 2019).
Nevertheless, participation in usual mindfulness interventions, such as 8-week programs like MBSR can be difficult, if not impossible, for patients undergoing treatment, because they involve 20–26 h of formal meditation in group sessions of 2.5 h each, plus one full day of practice in silence (6 h), and daily practice of about 45 min at home (Toivonen et al., 2020). Such a high level of requirement is often not compatible with and sometimes contraindicated by the reality of a cancer patient suffering from significant distress or treatment side effects (Creswell, 2017; Taylor et al., 2022).
The proposal of interventions other than the classic 8-week programs, which would be more flexible, open, less formal, and adaptable, is a promising but understudied area (Baminiwatta and Solangaarachchi, 2021; Zhang et al., 2021). Incorporating practices that echo mindfulness, Acceptance and Commitment Therapy (ACT) is a psychotherapy originally developed by Steven C. Hayes and colleagues in the 1980s based on a scientific methodology. It belongs to the Cognitive Behavioral Therapies (CBT) (Hayes et al., 1999). Thanks to various exercises and metaphors, ACT proposes to train mindfulness-related processes without having to use formal learning: acceptance (i.e., willingly accepting the unwanted feelings inevitably elicited by taking difficult actions, particularly those consistent with the patient's hopes, values, and goals), defusion (i.e., stepping back from thoughts that interfere with valued actions and seeing them for what they are), contact with the present moment (i.e., flexibly and purposefully remaining in the present moment by being mindful of thoughts, feelings, bodily sensations, and action potentials, including during distressing experiences), and self-as-context (i.e., keeping balanced and broad perspective on thinking and feeling, such that painful or distressing thoughts and feelings do not automatically trigger maladaptive avoidance behaviors). ACT also offers the opportunity to address two other processes, namely, values (i.e., clarifying fundamental hopes, values, and goals such as being there for one's family, pursuing meaningful work, and so on) and committed action (i.e., cultivating a commitment to doing things in line with identified hopes, values, and goals). Psychological flexibility, defined as the ability to persist in or change behavior when it is in service of valued ends in a particular context, reflects the broader target of the ACT approach (Hayes et al., 2011). The findings of several recent systematic reviews and meta-analyses suggest that ACT is associated with improvements in anxiety, depression, psychological flexibility, and quality of life in patients with cancer (Li et al., 2021; Mathew et al., 2021; Zhang et al., 2023; Jiang et al., 2024). The goal of the present study was to assess the feasibility and acceptability of an original group ACT program with mindfulness practices, to roll the program out on a larger scale. The program called MAEva (M for Meditation, A for Acceptance, and Eva for Commitment to Values) has a very different design from classic mindfulness programs traditionally delivered in 8 weeks. Indeed, the MAEva program is open, circular, and rolling in three sessions, thus enabling a great deal of flexibility in clinical delivery, whereby patients can enter the program at any session (not needing to wait until a group begins), they are invited to participate according to their possibilities, and they can make up for the missed session(s). A proposal such as this would help to address real-world implementation issues in these patients. Therefore, this study tested the feasibility and acceptability of the MAEva program in our center.
Methods
Research design
We performed a prospective, single-center, single-arm study testing the feasibility and impact of the MAEva program on patient-reported outcomes among non-metastatic breast and prostate cancer patients. The study was reviewed and approved by the Ethics Committee “Comité de Protection des Personnes Ile de France X” on 15 March 2021 under the number ID-RCB: 2021-A00601-40. All participants provided written informed consent. The study was conducted between September 2021 and July 2022, and all the participants were recruited in our center.
Participants
A total of 40 patients with non-metastatic breast or prostate cancer were recruited at the Lorraine Institute of Oncology. The inclusion criteria were age 18 years or above, newly diagnosed or undergoing treatment, and able to remain in a seated position for the duration of the sessions (1h30). Although the study was primarily aimed at patients who were in the first phases of treatment (surgery, chemotherapy, radiotherapy), it was also open to patients undergoing hormone therapy. The exclusion criteria were patients currently participating in another meditation program, severe hearing impairment, or severe mental illness.
The program was proposed to patients during consultations by the practitioners (oncologists, nurses, psychologists, etc.). The study was presented to the patients using a brochure. The center's psychiatrist then met with eligible patients, who were given an information leaflet explaining the content of the study. The psychiatrist obtained the patient's written informed consent. Then, the patients were included by the center's psychiatrist who carried out a clinical assessment at the inclusion visit based on a structured interview exploring the main psychiatric disorders [Mini Neuropsychiatric International Interview (MINI)].
Procedure
The MAEva program combines ACT and mindfulness practices, and comprises three group sessions of 1 h 30 min each, following a weekly schedule. Each session addresses a specific theme and contains short meditative practices (10–15 min), as well as sharing times with feedback of experience and theoretical contributions: Session 1: Mindfulness Meditation (targeted processes: contact with the present moment and self-as-context), Session 2: Acceptance (targeted processes: acceptance and defusion), and Session 3: Commitment to Values (targeted processes: values and committed action).
The MAEva program is an open group intervention (i.e., patients can enter the program at any session), and it is circular (i.e., it is possible to do the three sessions in any order and repeat the program to benefit from a training effect). Patients are invited to participate according to their possibilities and without having to commit to carrying out the whole program (i.e., it is fully acceptable for a patient to participate in only one or two of the three sessions of a complete cycle) (Figure 1).
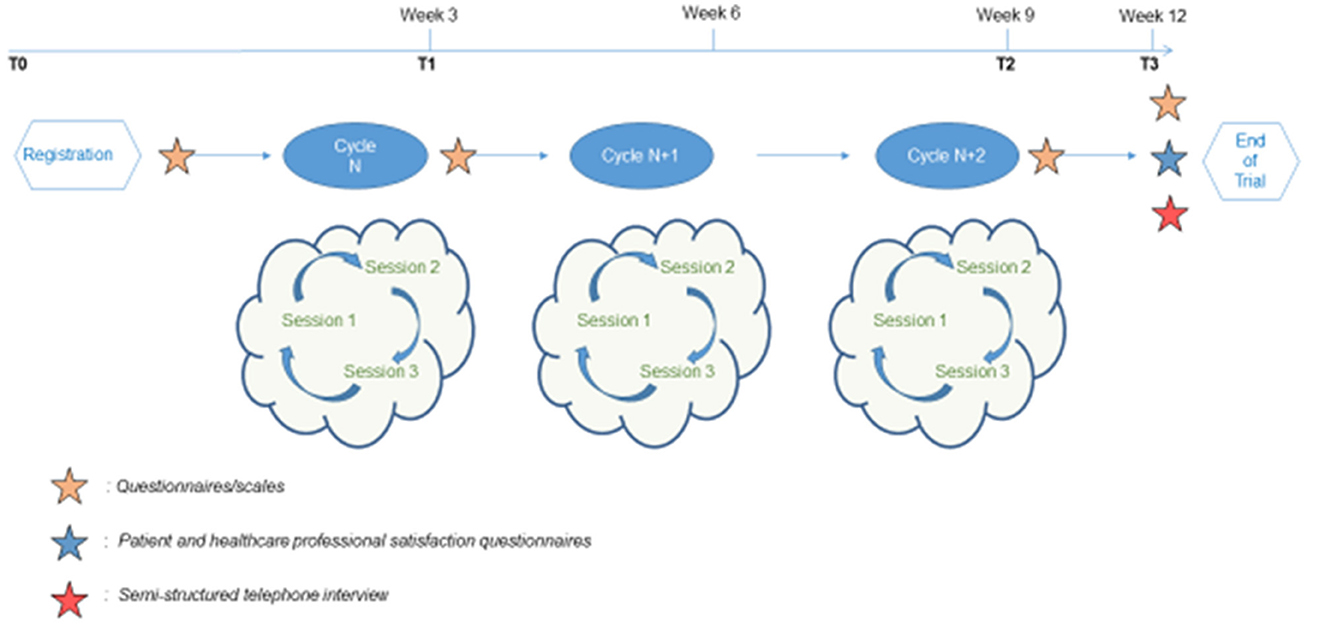
Figure 1. Study process. After enrollment, patient could participate at three cycles of MAEva program within 9 consecutive weeks. Follow-up evaluations are organized in weeks 0, 3, 9, and 12 (or T0, T1, T2, and T3). The MAEva program is an open and circular intervention of three different sessions. Each session addresses a specific theme: Mindfulness meditation, Acceptance and Commitment to values (Session 1, 2 or 3). In this MAEva trial, the maximum duration participation for patient is 12 weeks (graphics program: Microsoft Power Point).
Between sessions, participants were encouraged to engage in daily practice of the ACT therapeutic processes covered. They were also asked to train daily in an original adaptation of the mini-meditation called “three min of breathing space” used in the MBCT program (stop, observe, breathe, expand, and transform reaction into response). Moreover, they were invited to cultivate mindfulness in daily life through informal exercises, that is, to devote oneself attentively to routine activities (e.g., taking a shower, brushing one's teeth, getting dressed, eating, walking, etc.).
The program designer is a psychiatrist, MBCT instructor, ACT therapist, and supervisor.
The facilitators of the sessions were the psychiatrists or psychologists of our center, all trained in ACT, as well as in leading mindfulness sessions, as used in the program. Summary documents were given to the participants at the end of each session, including a summary of the concepts covered during the session and the exercises to practice for the following week. The observation period in this study was 12 weeks for each patient. Moreover, patients could participate in three cycles of the MAEva program over nine consecutive weeks. Follow-up consisted of evaluations scheduled at weeks 0, 3, 9, and 12. In other words, the number of sessions performed per patient could vary from 1 to 9 sessions (one cycle of the MAEva program comprising three sessions; and the cycle repeated three consecutive times).
Outcome criteria
The main outcome of this study was participation rate, defined as the proportion of patients who participated at least once in each of the three sessions of the program (i.e., attended the Meditation session at least once, the Acceptance session at least once and the Commitment to Values session at least once) over the 9 weeks of the program. Other outcomes of this study were to evaluate the benefit of MAEva on wellbeing in terms of QoL, fatigue, anxiety and depression, process and mechanism, as well as adherence to the program.
Measures
Quantitative data
Evaluations were performed at inclusion (T0), week 3 (T1), week 9 (T2), and week 12 (T3), and data were recorded using Cleanweb software (Figure 1). Follow-up at T1 and T2 corresponded to the intervention period, while T3 corresponded to the follow-up evaluation 3 weeks post-intervention. At each follow-up period, an e-mail was automatically sent to patients, inviting them to complete the online questionnaire. Participants who did not have internet access or did not have an e-mail address had the option of completing the questionnaires in paper format.
Sociodemographic (age, sex, marital status, education level, professional situation) and clinical data (body mass index, WHO performance status, localization of cancer, treatment) were collected at enrollment.
Patient-reported outcome measures (PROMs) were assessed using three questionnaires. The Global Health and Quality of life (QoL) scale in cancer patients was assessed using the validated French version of the EORTC QLQC-30 (European Organization for Research and Treatment of Cancer 30-item QoL questionnaire) (Aaronson et al., 1993). It is a cancer-specific QoL self-administered questionnaire with 30 items grouped into five functional dimensions (PF: physical, RF: role, CF: cognitive, EF: emotional, and SF: social), nine symptomatic dimensions (fatigue, pain, nausea and vomiting, dyspnea, sleep disturbance, loss of appetite, constipation, diarrhea, and financial impact), and one global health status (GHS) dimension (example items from the questionnaire: During the past week, have you had pain? Were you limited in doing either your work or other daily activities? Have you had difficulty remembering things? Did you feel irritable? Has your physical condition or medical treatment interfered with your social activities?). The score of each dimension was calculated and normalized on a scale from 0 to 100 (high QoL). Cronbach's alpha value ranged from 0.70 for pain, to 0.88 for fatigue, and to 0.80 for GHS.
Cancer-related fatigue was evaluated using the QLQ-FA12 questionnaire (Weis et al., 2017)—a multidimensional instrument consisting of 12 items—to be used in conjunction with the basic quality-of-life questionnaire (QLQ-C30). This module assesses the physical, cognitive, and emotional aspects of cancer-related fatigue (example items from the questionnaire: During the past week, did you feel sleepy during the day? Did you have trouble thinking clearly? Did you feel discouraged?). Cronbach's alpha value ranged from 0.88 for emotional fatigue to 0.93 for cognitive fatigue.
Anxiety and depression were measured using the 14-item Hospital Anxiety and Depression Scale (HADS) (Zigmond and Snaith, 1983). This scale is frequently used to assess psychosocial outcomes in cancer patients, and its reliability and validity have been confirmed (Zhang et al., 2015; example items from the questionnaire: I feel tense or ‘wound up', I can laugh and see the funny side of things, I get sudden feelings of panic). Each subscale is scored from 0 to 21, with higher scores indicating greater anxiety and depression; 0–7 is generally considered within a normal range. Cronbach's alpha ranged from 0.63 for anxiety to 0.82 for depression.
The number of sessions attended and the topics covered were assessed to calculate participation data. An end-of-study satisfaction questionnaire was given to participants at T3 (week 12) to collect their opinions and feedback about the conduct of the MAEva program. In particular, they were asked to rate the degree of importance that the program had for them on a scale ranging from 0 (not important at all) and 10 (very important), and to explain why. Several other open questions were also included to evaluate the benefits and obstacles of the program. A satisfaction questionnaire was also given to the facilitators of the sessions.
Qualitative data
Qualitative data were collected to evaluate the processes and mechanisms of action involved during the MAEva program using semi-structured telephone interviews conducted at T3 (week 12) with the first 10 participants (Figure 1). An interview guide was developed in advance to specify the various questions to be addressed. The interviews were recorded and then transcribed for qualitative framework analysis.
Data analyses
Sample size and the smallest detectable difference
The inclusion period was 7 months corresponding to a potential inclusion of 40 patients. Thus, the smallest detectable difference (SDD) was calculated with this sample size. Change in anxiety score was used to define the smallest detectable difference (As the program was expected to have the greatest impact on this outcome). The SDD for anxiety was calculated with a 5% type I error and 80% power, assuming a normal distribution of the 12-week change and a standard deviation (SD) of 4.0. In these conditions, this study would be able to detect a minimal change in anxiety score from before to after the intervention of 1.82 points. Knowing that a difference of 1.7 points in the anxiety score was considered the minimum threshold beyond which the difference was clinically relevant (Lemay et al., 2019); this estimated SDD seemed acceptable to us.
Quantitative data
Baseline sociodemographic and clinical characteristics of the study sample were assessed using descriptive statistics (mean ± SD; number (N), and percentage). The scores were calculated for the different dimensions of the PROMs and their change at each follow-up time (weeks 3, 9, and 12) compared to inclusion.
For the main objective of this study, the level of patient participation was assessed for the various sessions offered (total number of sessions, total number of mindfulness meditation sessions, total number of acceptance sessions, and total number of value commitment sessions). Feasibility of the study was defined as participation at least once in each of the three sessions of the program over the 9-week period.
Finally, the association between the level of participation in the sessions and changes in PROMs was analyzed using linear mixed models for repeated measures with the patient as a random effect. The mixed models were first univariate and then multivariate, and they were adjusted for cancer type, WHO status, prior surgery, and receipt of complementary treatment.
Qualitative data
Qualitative data from the semi-structured interviews were analyzed according to the framework analysis approach (Gale et al., 2013). For each interview, the transcript was read several times to become familiar with the discourse of the interviewee. With each interview transcript, informative statements were extracted into units of meaning and categorized into different themes. The 10 interviews were initially categorized into themes corresponding to the 6 ACT processes involved in the intervention (i.e., contact with the present moment, self-as-context, acceptance, defusion, values, and committed action). Then, to include other themes that participants expressed, the coding was expanded using a second codebook based on self-determination theory to identify units of meaning relevant to the three main psychological needs (i.e., autonomy, competence, and relatedness).
Results
Study sample characteristics
All participants were included in the statistical analysis using the intention to treat (ITT) analysis.
Table 1 shows the baseline sociodemographic, clinical, and PROMs data. The study sample was predominantly female (37/40, 92.5%) with an average age of 50.4 years [min = 31 and max = 70]. Approximately, 60% were married, over 90% had a high school diploma or higher education, and 47.5% were intermediate professionals. Clinically, there were 37 cases of breast cancer and three cases of prostate cancer.

Table 1. Baseline sociodemographic, clinical and perceived health of the study sample.
None of the patients included in the study had adhered to a meditation program before inclusion, none were currently on another meditation program (exclusion criteria), and none engaged in regular meditation practice at the time of their inclusion.
Of the participants, 62.5% had undergone surgery and 85% were currently undergoing treatment.
At inclusion, patients had relatively high QoL scores, especially for the physical, psychological, social, and cognitive dimensions. The symptom dimensions of the QLQ-C30 were relatively low. According to the HADS questionnaire scores, more than three-quarters of patients probably (62.5%) or definitely (12.5%) had symptoms of depression, and almost all of the patients (97.8%) probably (43.2%) or definitely (54.1%) had symptoms of anxiety. There was an intermediate level of fatigue measured by the FA-12 questionnaire at inclusion, particularly for physical and emotional fatigue.
Main outcome
Overall, attendance in the MAEva program was excellent, with patients attending an average of 6.8 out of 9 sessions (min = 2, max = 9) (Table 2). A total of 8 of 40 participants (20%) attended all the 9 sessions. The level of participation in the thematic sessions was similar, with 23 (57.5%) attending all the Mindfulness meditation sessions, 18 (45%) attending all the Acceptance sessions, and 17 (42.5%) attending all the Commitment to Values sessions. The feasibility was excellent, with almost 90% of patients attending at least one session of each type.
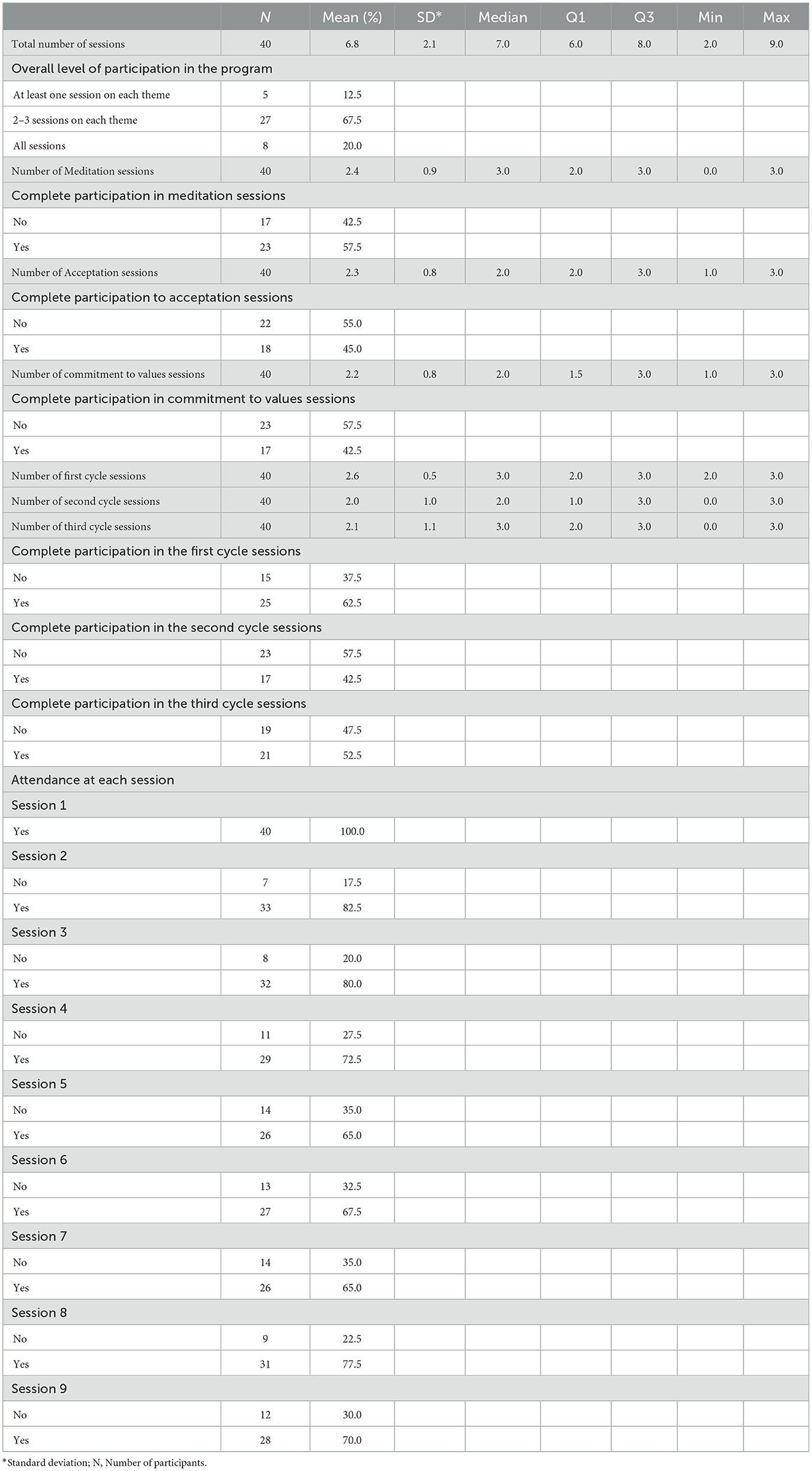
Table 2. Participation in the MAEva program.
Secondary outcomes
Adherence to the program was associated with a statistically significant improvement in QoL, particularly in its functional dimensions (Tables 3, 4). For example, participation in each additional session was associated with a mean increase in overall QoL score of more than one point at each measurement time (β = 1.09 [0.13; 2.04], p = 0.02). The psychological and emotional dimensions were those that were most positively impacted by the sessions with, respectively, β = 2.27 [0.84; 3.71] and β = 2.31 [1.12; 3.51]. Participation level was also associated with a significant improvement in fatigue. The fatigue dimensions decreased with session attendance: physical (β = −2.24 [−3.63; −0.85]), emotional (β = −2.60 [−4.11; −1.09]), and interference with daily life (β = −2.33 [−3.95; −0.72]). Conversely, the nausea and vomiting dimension showed a negative association with presence at the sessions (β = 1.11 [0.45; 1.78]). No statistically significant association was found between the number of sessions and changes in anxiety and depression scores. Finally, on the satisfaction questionnaires, patients reported an average score of the degree of importance that the program had for them of 8.36/10 (SD ± 1.64).
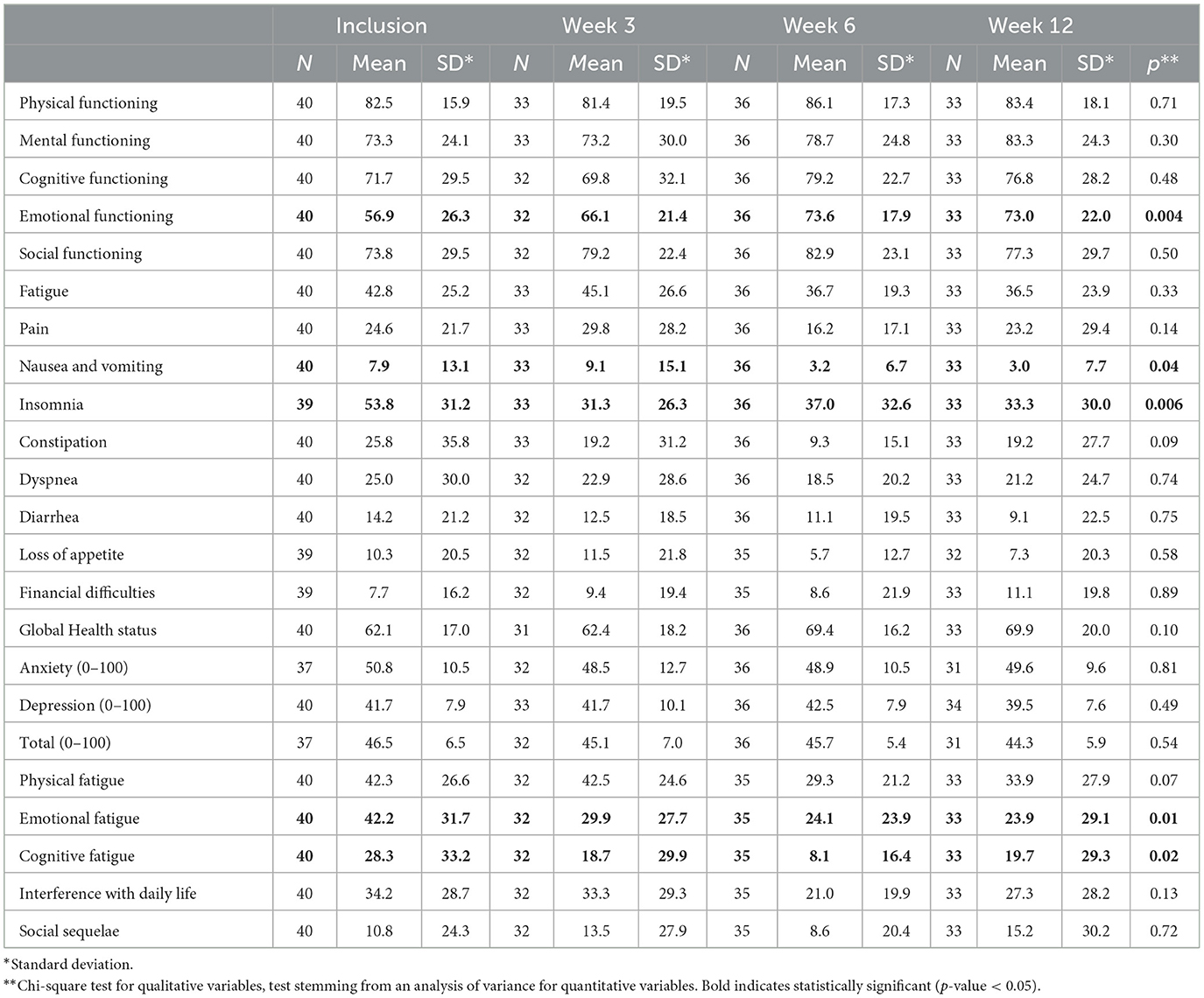
Table 3. Description of changes in quality of life, fatigue, anxiety, and depression during follow-up.
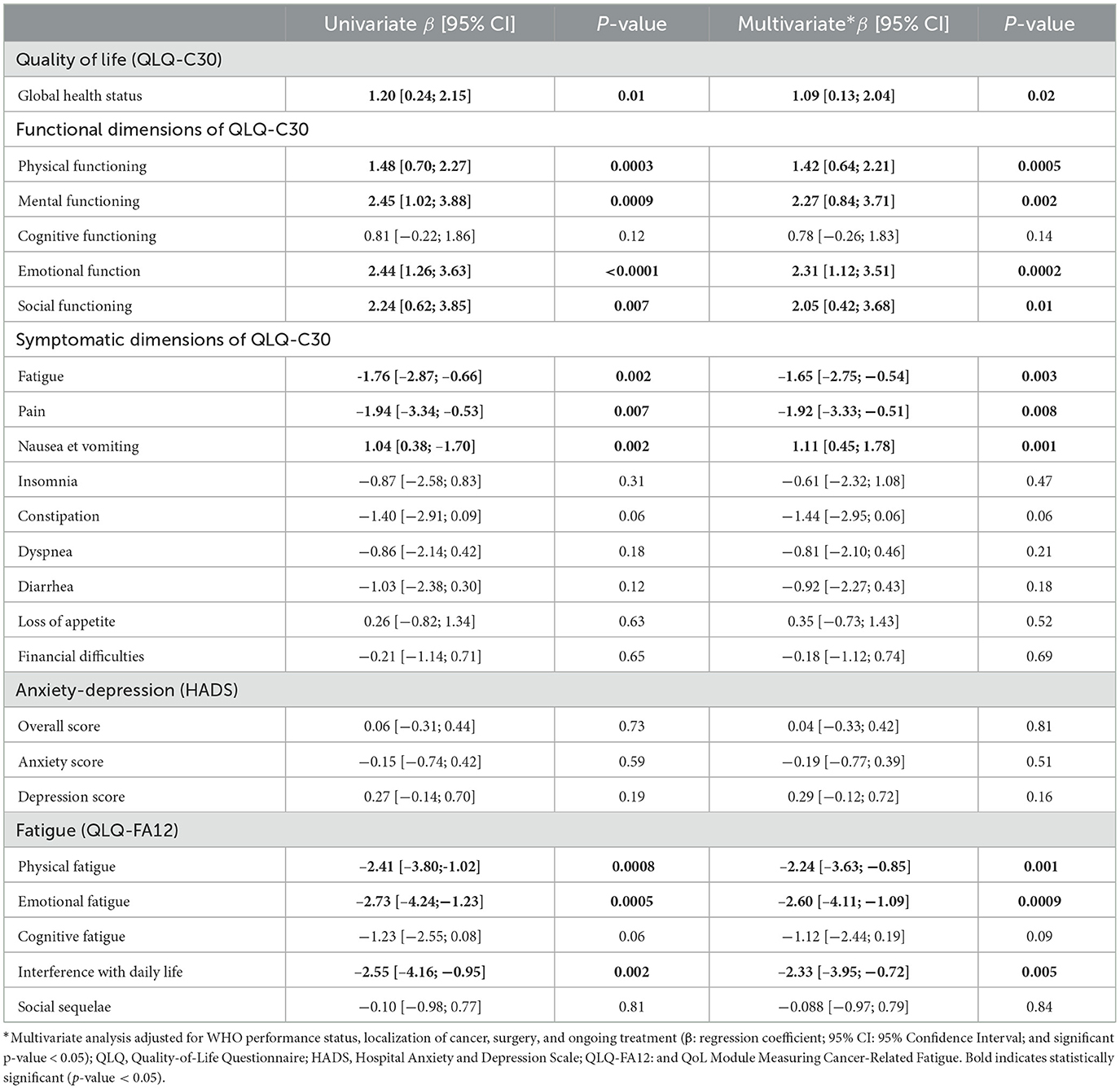
Table 4. Association between level of participation and change in patient-reported outcomes measures.
Post-intervention interview outcomes
Table 5 presents the number of units of meaning relevant to the ACT process. Using the first codebook based on ACT processes, the following themes were extracted: (1) committed action, (2) contact with the present moment, (3) self-as-context, (4) defusion, (5) values, and (6) acceptance. They are presented from the most to the least commonly expressed.
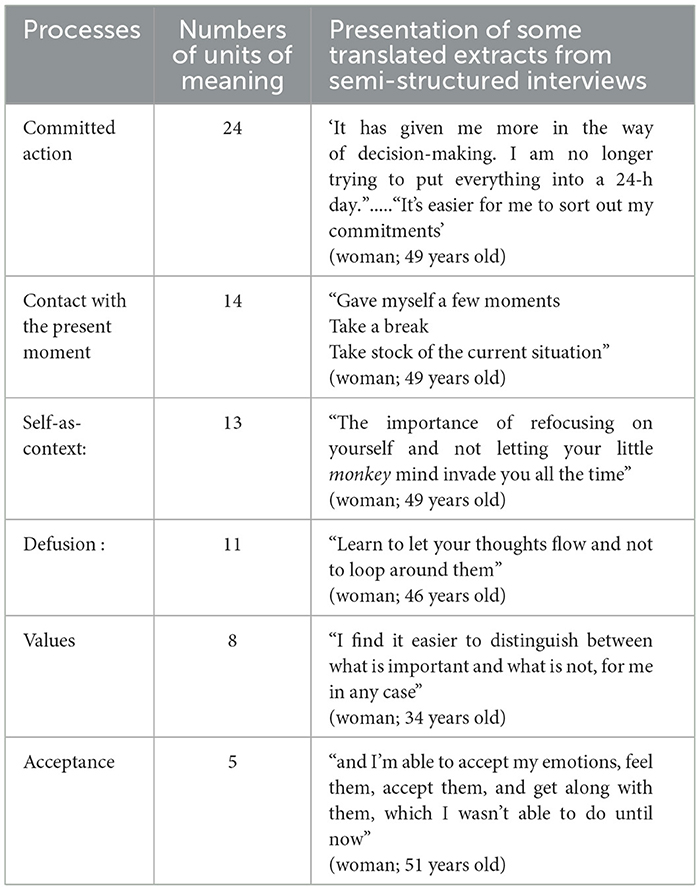
Table 5. Number of units of meaning relevant to the ACT process.
Through their attendance at sessions, application of daily exercises, involvement in long-term practice, and transmission of what they have learned to members of their entourage, participants demonstrated their commitment to applying mindfulness during and after the MAEva program (Committed action). The interview analysis also reveals a strong appropriation of the “being present” process. Thanks to the MAEva program, participants developed some capacities, such as anchoring themselves in the present moment, identifying mind wandering, and focusing on bodily sensations, enabling them to experience the present moment more fully (Contact with the present moment).
Through the participants' discourse, it was also possible to perceive the development of the ability to “let go” during the program, giving them access to another way of experiencing the present moment, more in line with their authentic selves, and by the “self-as-context” perspective (Self-as-context). The regular use of an original adaptation of the mini-meditation called “three minutes of breathing space” used in the MBCT program was reported by the majority of the participants after the program. This underlines the development of the defusion process, which refers to the ability to distance oneself from thoughts and observe them without judgment or an impulse to react (Defusion).
Finally, most participants were receptive to the values process during the sessions of MAEva program, as seen in their words relating their ability to give great meaning to their lives and to identify their sources of reinforcement (Values). Although less represented in participant discourse, the acceptance process was illustrated through recurrent expressions such as “welcome, deal with, not fight against” thoughts and emotions (Acceptance) (Table 5).
Using the second codebook based on basic psychological needs, three themes were extracted: (1) competence need; (2) autonomy need; and (3) relatedness need (Table 6).
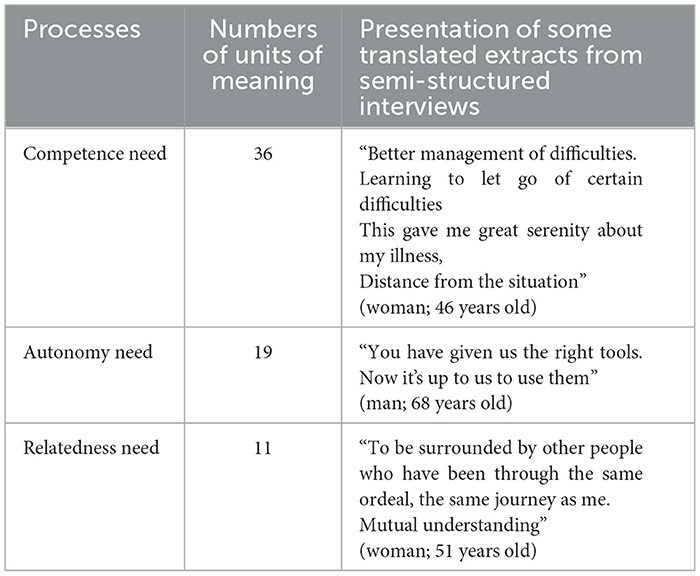
Table 6. Number of units of meaning relevant to three basic psychological needs of self-determination theory.
The Competence need is illustrated in the participant discourse highlighting the ability to autonomously apply the techniques taught in the program. The MAEva program enabled patients to better manage the anxiety and/or pain associated with cancer through their ability to apply the meditative practices, observe their inner processes, learn self-awareness, and thanks to emotions and disease management. The Autonomy need is perceptible in the patients' discourse through their decision to participate in the group sessions and to choose whether to use the techniques learned during the MAEva program. Moreover, this need is also obvious in the way they organize their practice and decide to get involved in other activities. Finally, the need for relatedness is also reinforced, with the importance of belonging to a group, as expressed by more than half the participants (Table 6).
Discussion
This study highlights the feasibility and acceptability of an original program using ACT with mindfulness practices for cancer patients. To obtain a homogeneous population sample, patients with non-metastatic breast or prostate cancer were either recruited, newly diagnosed, or undergoing treatment. Our center is particularly involved in the treatment of breast cancer. Most patients included in this study were women. Conducting this study confirmed to us that the inclusion of women is easier in our center for this type of intervention. As this is a feasibility study, we did not wish to exclude the three patients with prostate cancer from our analyses. Indeed, in our view, the MAEva program seems sufficiently flexible to be offered to a majority of cancer patients, regardless of the location or stage of the disease, which could be the subject of future studies.
The program attendance throughout the observation period was high, and almost all patients received the full intervention (which was defined as participation at least once in each of the three types of sessions of the MAEva program). In line with these results, the MAEva program was appreciated by the patients, and they reported that it had a high degree of importance for them.
Our results indicate that participation in the MAEva program was associated with an improvement in QoL and fatigue. In keeping with a previous study based on mindfulness interventions for chronic disease (Dantzer and Le Barbenchon, 2016), the present study shows a greater improvement in the psychological, emotional, and social dimensions of QoL than in the physical dimensions. The participants also reported a reduction in pain, and in both emotional and physical fatigue, which is a promising result for patients living with cancer. Unexpectedly, participants also reported an increase in nausea and vomiting. This result is probably explained by the stage of diseases of the included patients, most of whom were undergoing chemotherapy at the time of the study. Another possible interpretation is that, by learning mindfulness skills, patients increased their ability to identify their symptoms and pay more attention to their bodies. This ability could be useful to take care of the disease and increase self-care. A trend toward an improvement in anxiety and depression scores was observed, although this result did not reach statistical significance. Therefore, the assessment of quality of life scores seems more relevant to evaluate the impact of the MAEva program (McCloy et al., 2022). This study enabled us to calculate a suitable study sample size for future randomized controlled trials based on this outcome. Furthermore, each thematic session provides similar benefits, underlining the importance of all elements of the program.
The qualitative section shows that the patients learned skills using the ACT and mindfulness practices. More specifically, interviewed participants shared their satisfaction regarding the development of their ability to “let go”, as well as a close connection with an authentic self through their values, and their commitment to daily mindful practices. These new abilities could help them to deal with challenging emotions and thoughts that are unavoidable with a chronic disease like cancer (Pitman et al., 2018). Moreover, the MAEva program provided participants with a greater feeling of autonomy, competence, and connection with other persons living with the same disease. A recent study highlighted the influence of psychological needs, and more particularly the competence need, in predicting physical activity for patients with breast cancer during chemotherapy and recommended that health professionals should pay attention to the satisfaction of these needs (Fu et al., 2022). The qualitative results of the current study also highlight the overlap of ACT processes and their connection with the satisfaction of the three basic psychological needs described in the self-determination theory (Ryan et al., 2008). The participants' discourse illustrates that the MAEva program influenced the development of their intrinsic motivation and promoted their psychological flexibility.
This study extends existing knowledge regarding the potential of using meditation-based interventions for cancer patients in reducing distress and improving QoL. Indeed, this original program, with an open and circular design, was created very differently from the classic mindfulness programs delivered in a closed 8-week format. Engaging in formal meditation training, as offered in the MBSR program, is extremely difficult for cancer patients and sometimes inadvisable. They face significant stressors related to illness, treatment, and fatigue as well as multiple logistical obstacles (Zernicke et al., 2016; Peters et al., 2020). A few studies have highlighted the difficulties cancer patients face in meeting the demands of an 8-week program and the need to adapt interventions to make them less intensive (Eyles et al., 2015; Kubo et al., 2018). In the present study, the participants greatly appreciated the flexibility of the MAEva program (the possibility of missing sessions and making up for them) as well as the characteristics of the practices trained (short meditations [10–15 min], exercises proposing a systematic approach to regulating stress, informal practices, and theoretical contributions).
In addition, during this feasibility study, useful observations were made to assess the relevance of the MAEva program in the patients' real lives. Firstly, the recruitment did not encounter any difficulty, and the enrollment of 40 patients was much faster than expected (few refusals, patients motivated to participate). Secondly, an improvement in QoL was observed, with high levels of satisfaction and no negative consequences. Thirdly, the MAEva program is an intervention suitable for all cancer patients, at all stages of disease. Moreover, its implementation appeared simple and inexpensive to us, although we must consider that our center had psychology professionals trained in ACT and mindfulness available on site, and this may not be the case everywhere (Zhang et al., 2022). Lastly, the MAEva program is a written and structured intervention, and the responsibility for its delivery can be shared between different health professionals, facilitating implementation and maintenance within the hospital. However, it should be noted that the facilitators who took part in this study were all trained in each thematic session of the program. The satisfaction questionnaires completed by the healthcare professionals showed that they were motivated and firmly convinced of the utility of this program, which is an essential condition for the success of such a project (Hutchinson et al., 2021).
Our methods provide a practical strategy for conducting a larger, fully powered clinical trial, and we provide important insights for further work in the future. The question of the effectiveness of the MAEva program could be addressed via a randomized controlled trial, with quality of life as the main outcome for which we can calculate the study sample size. Qualitative analyses also suggest the importance of evaluating the flexibility processes of ACT. This could be done quantitatively in future larger studies using scales such as the Multidimensional Psychological Flexibility Inventory (MPFI) (Grégoire et al., 2020).
Limitations
This study has some limitations. First, it was a single-arm feasibility study, and, thus, the lack of a control group and the small sample size make it impossible to draw firm conclusions regarding the potential efficacy of the intervention on participant-reported outcomes. The observed improvements in QoL and fatigue may simply represent natural improvements. In addition, the discrepancies between the number of men and women, between diagnoses and phases of the treatment, preclude any generalization of the results among cancer patients.
Second, the post-intervention interviews were conducted by a single facilitator, which may leave potential for social desirability bias. Indeed, it is possible that the patients questioned wanted to present themselves in a favorable light. However, the results of the satisfaction questionnaires and the post-intervention interviews concur to indicate that the participants appreciated the MAEva program. It helped them to cultivate presence, acceptance, commitment, and better regulation of stress, providing sufficient justification for further investigation of the effectiveness of this intervention through larger randomized clinical trials.
Conclusion
This feasibility study provides encouraging evidence that an original, open, and circular program of ACT with mindfulness practices is acceptable for breast cancer patients (newly diagnosed or undergoing treatment). Although no causality could be definitively established from this study, our findings encourage the performance of additional randomized control trials, especially given the very low risks associated with the MAEva program. Future larger scale randomized studies involving diverse populations are necessary to establish the efficacy of the MAEva program. Pragmatic trials of this type of intervention within large healthcare systems will help document the effectiveness of implementing structured, low-cost programs that combine ACT and mindfulness practices, which are less demanding than conventional eight-week mindfulness programs, for cancer patients.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Ethics Committee or Comité de Protection des Personnes Ile de France X on 15 March 2021 under the number ID-RCB: 2021-A00601-40. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
FB: Conceptualization, Formal analysis, Investigation, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. DB: Formal analysis, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. CH-S: Conceptualization, Methodology, Writing – review & editing. AS: Formal analysis, Writing – review & editing. LD: Investigation, Writing – review & editing. MG: Investigation, Writing – review & editing. VA: Investigation, Writing – review & editing. EF: Conceptualization, Formal analysis, Validation, Visualization, Writing – original draft, Writing – review & editing. AO: Conceptualization, Formal analysis, Methodology, Software, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This research was funded by the Lorraine Institute of Oncology. This work was supported by the association “Vivre comme avant” – Paris.
Acknowledgments
The authors would like to thank Dr. Lionel Uwer for his active participation in patient recruitment. The authors greatly appreciate the time and effort that the staff of the Clinical Research Center of the Lorraine Institute of Oncology devoted to this work. The authors also appreciate the work of Bérenger MARTIN as data manager from “Unité de Méthodologie en Recherche Clinique Epidémiologie et Santé Publique (uMETh)” - Besançon University.
Conflict of interest
FB is a paid trainer and speaker in mindfulness meditation, acceptance and commitment therapy (ACT). He receives royalties for several books on mindfulness meditation and ACT published by FIRST, Pocket, Humensis, and Ellipses.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Aaronson, N. K., Ahmedzai, S., Bergman, B., Bullinger, M., Cull, A., Duez, N. J., et al. (1993). The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 85, 365–376. doi: 10.1093/jnci/85.5.365
Artherholt, S. B., and Fann, J. R. (2012). Psychosocial care in cancer. Curr. Psychiatry Rep. 14, 23–29. doi: 10.1007/s11920-011-0246-7
Ataşalar, J., and Michou, A. (2019). Coping and mindfulness: mediators between need satisfaction and generalized problematic Internet use. J. Media Psychol. 31, 110–115. doi: 10.1027/1864-1105/a000230
Baminiwatta, A., and Solangaarachchi, I. (2021). Trends and developments in mindfulness research over 55 years: a bibliometric analysis of publications indexed in web of science. Mindfulness 12, 2099–2116. doi: 10.1007/s12671-021-01681-x
Campbell, R., Vansteenkiste, M., Delesie, L., Soenens, B., Tobback, E., Vogelaers, D., et al. (2019). The role of basic psychological need satisfaction, sleep, and mindfulness in the health-related quality of life of people living with HIV. J. Health Psychol. 24, 535–545. doi: 10.1177/1359105316678305
Carlson, L. E., Angen, M., Cullum, J., Goodey, E., Koopmans, J., Lamont, L., et al. (2004). High levels of untreated distress and fatigue in cancer patients. Br. J. Cancer 90, 2297–2304. doi: 10.1038/sj.bjc.6601887
Carlson, L. E., Groff, S. L., Maciejewski, O., and Bultz, B. D. (2010). Screening for distress in lung and breast cancer outpatients: a randomized controlled trial. J. Clini. Oncol. 28, 4884–4891. doi: 10.1200/JCO.2009.27.3698
Carlson, L. E., and Kirsti Toivonen Subnis, U. (2019). Integrative approaches to stress management. Cancer J. 25, 329–336. doi: 10.1097/PPO.0000000000000395
Carlson, L. E., and Speca, M. (2010). Mindfulness-Based Cancer Recovery. Oakland, CA: New Harbinger Publications.
Creswell, J. D. (2017). Mindfulness interventions. Annu. Rev. Psychol. 68, 491–516. doi: 10.1146/annurev-psych-042716-051139
Dantzer, C., and Le Barbenchon, E. (2016). “Méditation de pleine conscience dans la prise en charge de la maladie chronique: état des connaissances, processus et perspectives,” in Introduction à la pleine Conscience. (Malakoff: DUNOD) 89–103. doi: 10.3917/dunod.falle.2016.01.0089
Eyles, C., Leydon, G. M., Hoffman, C. J., Copson, E. R., Prescott, P., Chorozoglou, M., et al. (2015). Mindfulness for the self-management of fatigue, anxiety, and depression in women with metastatic breast cancer: a mixed methods feasibility study. Integr. Cancer Ther. 14, 42–56. doi: 10.1177/1534735414546567
Fann, J. R., Ell, K., and Sharpe, M. (2012). Integrating psychosocial care into cancer services. J. Clini. Oncol. 30, 1178–1186. doi: 10.1200/JCO.2011.39.7398
Fu, Y., Li, K., Zhou, Z., Wei, W., Wang, C., Dong, J., et al. (2022). Integrating self-determination theory and upper limb factors to predict physical activity in patients with breast cancer during chemotherapy. Cancer Nurs. 45, 52–60. doi: 10.1097/NCC.0000000000000951
Gale, N. K., Heath, G., Cameron, E., Rashid, S., and Redwood, S. (2013). Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med. Res. Methodol. 13:117. doi: 10.1186/1471-2288-13-117
Grassi, L. (2020). Psychiatric and psychosocial implications in cancer care: the agenda of psycho-oncology. Epidemiol. Psychiatr. Sci. 29:e89. doi: 10.1017/S2045796019000829
Grégoire, S., Gagnon, J., Lachance, L., Shankland, R., Dionne, F., Kotsou, I., et al. (2020). Validation of the english and french versions of the multidimensional psychological flexibility inventory short form (MPFI-24). J. Cont. Behav. Sci. 18, 99–110. doi: 10.1016/j.jcbs.2020.06.004
Hayes, S., Strosahl, K., and Wilson, K. (2011). Acceptance and Commitment Therapy: the Process and Practice of Mindful Change. New York: Guilford Publications.
Hayes, S. C., Strosahl, K. D., and Wilson, K. G. (1999). Acceptance and Commitment Therapy: An Experiential Approach to Behavior Change. New York: Guilford Publications.
Huebner, J., Prott, F. J., Micke, O., Muecke, R., Senf, B., Dennert, G., et al. (2014). Online survey of cancer patients on complementary and alternative medicine. Oncol. Res. Treatm. 37, 304–308. doi: 10.1159/000362616
Hutchinson, J. K., Jones, F., and Griffith, G. (2021). Group and common factors in mindfulness-based programmes: a selective review and implications for teachers. Mindfulness 12, 1582–1596. doi: 10.1007/s12671-021-01596-7
Jiang, X., Sun, J., Song, R., Wang, Y., Li, J., and Shi, R. (2024). Acceptance and commitment therapy reduces psychological distress in patients with cancer: a systematic review and meta-analysis of randomized controlled trials. Front. Psychol. 14:1253266. doi: 10.3389/fpsyg.2023.1253266
Kabat-Zinn, J. (1990). Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain and Illness. New York, NY: Dell Publishing, 512.
Kubo, A., Altschuler, A., Kurtovich, E., Hendlish, S., Laurent, C. A., Kolevska, T., et al. (2018). A pilot mobile-based mindfulness intervention for cancer patients and their informal caregivers. Mindfulness 9, 1885–1894. doi: 10.1007/s12671-018-0931-2
Lemay, K. R., Tulloch, H. E., Pipe, A. L., and Reed, J. L. (2019). Establishing the minimal clinically important difference for the hospital anxiety and depression scale in patients with cardiovascular disease. J. Cardiopulm. Rehabil. Prev. 39, E6–E11. doi: 10.1097/HCR.0000000000000379
Li, H., Wu, J., Ni, Q., Zhang, J., Wang, Y., and He, G. (2021). Systematic review and meta-analysis of effectiveness of acceptance and commitment therapy in patients with breast cancer. Nurs. Res. 70, E152–E160. doi: 10.1097/NNR.0000000000000499
Lyman, G. H., Greenlee, H., Bohlke, K., Bao, T., DeMichele, A. M., Deng, G. E., et al. (2018). Integrative therapies during and after breast cancer treatment: ASCO endorsement of the SIO clinical practice guideline. J. Clini. Oncol. 36, 2647–2655. doi: 10.1200/JCO.2018.79.2721
Mathew, A., Doorenbos, A. Z., Jang, M. K., and Hershberger, P. E. (2021). Acceptance and commitment therapy in adult cancer survivors: a systematic review and conceptual model. J. Cancer Survivor. 15, 427–451. doi: 10.1007/s11764-020-00938-z
McCloy, K., Hughes, C., Dunwoody, L., Marley, J., and Gracey, J. (2022). Effects of mindfulness-based interventions on fatigue and psychological wellbeing in women with cancer: A systematic review and meta-analysis of randomised control trials. Psychooncology 31, 1821–1834. doi: 10.1002/pon.6046
Naser, A. Y., Hameed, A. N., Mustafa, N., Alwafi, H., Dahmash, E. Z., Alyami, H. S., et al. (2021). Depression and anxiety in patients with cancer: a cross-sectional study. Front. Psychol. 12:585534. doi: 10.3389/fpsyg.2021.585534
Oberoi, S., Yang, J., Woodgate, R. L., Niraula, S., Banerji, S., Israels, S. J, et al. (2020). Association of mindfulness-based interventions with anxiety severity in adults with cancer. JAMA Network Open 3:e2012598. doi: 10.1001/jamanetworkopen.2020.12598
Peters, L., Brederecke, J., Franzke, A., de Zwaan, M., and Zimmermann, T. (2020). Psychological distress in a sample of inpatients with mixed cancer-a cross-sectional study of routine clinical data. Front. Psychol. 11:591771. doi: 10.3389/fpsyg.2020.591771
Pitman, A., Suleman, S., Hyde, N., and Hodgkiss, A. (2018). Depression and anxiety in patients with cancer. BMJ. 361:k1415. doi: 10.1136/bmj.k1415
Rodríguez-Meirinhos, A., Antolín-Suárez, L., and Oliva, A. (2021). Psychological needs in parents and clinically referred adolescents: an integrative model via parenting and parental mindfulness. J. Family Psychol. 35, 906–915. doi: 10.1037/fam0000863
Ryan, R. M., and Deci, E. L. (2000). Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 55, 68–78. doi: 10.1037/0003-066X.55.1.68
Ryan, R. M., Patrick, H., Deci, E. L., and William, G. C. (2008). Facilitating health behaviour change and its maintenance: interventions based on Self-Determination Theory. Eur. Health Psycholo. 10, 2–5.
Segal, Z. V., Williams, J. M. G., and Teasdale, J. D. (2002). Mindfulness-Based Cognitive Therapy for Depression: A New Approach to Preventing Relapse. New York, NY, US: Guilford Press, 351.
Sellick, S. M., and Edwardson, A. D. (2007). Screening new cancer patients for psychological distress using the hospital anxiety and depression scale. Psychooncology 16, 534–542. doi: 10.1002/pon.1085
Taylor, G. B., Vasquez, T. S., Kastrinos, A., Fisher, C. L., Pulg, A., and Bylund, C. L. (2022). The adverse effects of meditation-interventions and mind–body practices: a systematic review. Mindfulness 13, 1839–1856. doi: 10.1007/s12671-022-01915-6
Toivonen, K., Hermann, M., White, J., Speca, M., and Carlson, L. E. (2020). A mixed-method, multi-perspective investigation of barriers to participation in mindfulness-based cancer recovery. Mindfulness 11, 2325–2337. doi: 10.1007/s12671-020-01461-z
Weis, J., Tomaszewski, K. A., Hammerlid, E., Ignacio Arraras, J., Conroy, T., Lanceley, A., et al. (2017). International psychometric validation of an eortc quality of life module measuring cancer related fatigue (EORTC QLQ-FA12). J. Natl. Cancer Inst. 109:5. doi: 10.1093/jnci/djw273
Xunlin, N. G., Lau, Y., and Klainin-Yobas, P. (2020). The effectiveness of mindfulness-based interventions among cancer patients and survivors: a systematic review and meta-analysis. Sup. Care Canc. 28, 1563–1578. doi: 10.1007/s00520-019-05219-9
Zernicke, K. A., Campbell, T. S., Speca, M., McCabe-Ruff, K., Flowers, S., Dirkse, D. A., et al. (2016). The eCALM Trial: eTherapy for cancer applying mindfulness. exploratory analyses of the associations between online mindfulness-based cancer recovery participation and changes in mood, stress symptoms, mindfulness, posttraumatic growth, and spirituality. Mindfulness 7, 1071–1081. doi: 10.1007/s12671-016-0545-5
Zhang, D., Lee, E. K. P., Mak, E. C. W., Ho, C. Y., and Wong, S. Y. S. (2021). Mindfulness-based interventions: an overall review. Br. Med. Bull. 138, 41–57. doi: 10.1093/bmb/ldab005
Zhang, L., Lopes, S., Lavelle, T., Jones, K. O., Chen, L., Jindal, M., et al. (2022). Economic evaluations of mindfulness-based interventions: a systematic review. Mindfulness 13, 2359–2378. doi: 10.1007/s12671-022-01960-1
Zhang, M.-F., Wen, Y.-S., Liu, W.-Y., Peng, L.-F., Wu, X.-D., and Liu, Q.-W. (2015). Effectiveness of mindfulness-based therapy for reducing anxiety and depression in patients with cancer: a meta-analysis. Medicine 94, e0897–e0890. doi: 10.1097/MD.0000000000000897
Zhang, Y., Ding, Y., Chen, X., Li, Y., Li, J., and Hu, X. (2023). Effectiveness of acceptance and commitment therapy on psychological flexibility, fatigue, sleep disturbance, and quality of life of patients with cancer: a meta-analysis of randomized controlled trials. Worldviews Evid. Based Nurs. 20, 582–592. doi: 10.1111/wvn.12652
Keywords: cancer, MAEva program, mindfulness, acceptance and commitment therapy, quality of life, stress
Citation: Bourgognon F, Bechet D, Huin-Schohn C, Strelow A, Demarche L, Guillou M, Adam V, Fall E and Omorou AY (2024) A mixed method feasibility and acceptability study of a flexible intervention based on acceptance and commitment therapy for patients with cancer. Front. Psychol. 15:1409308. doi: 10.3389/fpsyg.2024.1409308
Received: 29 March 2024; Accepted: 18 June 2024;
Published: 03 July 2024.
Edited by:
Sérgio A. Carvalho, University of Coimbra, PortugalReviewed by:
David Gillanders, University of Edinburgh, United KingdomJoana Marta-Simões, University of Coimbra, Portugal
Copyright © 2024 Bourgognon, Bechet, Huin-Schohn, Strelow, Demarche, Guillou, Adam, Fall and Omorou. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: François Bourgognon, Zi5ib3VyZ29nbm9uQG5hbmN5LnVuaWNhbmNlci5mcg==
†These authors have contributed equally to this work and share last authorship