 Zihao Zeng
Zihao Zeng Karen Holtmaat
Karen Holtmaat Sander L. Koole
Sander L. Koole
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Psychol., 24 June 2024
Sec. Psycho-Oncology
Volume 15 - 2024 | https://doi.org/10.3389/fpsyg.2024.1390692
Caregivers make a vital contribution to the emotional wellbeing of cancer survivors (Fong et al., 2017; Li et al., 2018; Harms et al., 2019). A recent systematic review comprising 86 studies with over 69,000 cancer survivors revealed that various forms of interpersonal emotion regulation by caregivers, such as providing emotional support or giving a warm embrace, are positively associated with a broad spectrum of mental health indicators, including less distress, anxiety, and depression, along with a better quality of life and overall wellbeing (Zeng et al., under review).1 Though this is a sizable body of evidence, this finding tacitly adopts the cancer survivor's perspective as the recipient of social-emotional support. Consequently, the perspective of caregivers in regulating survivors' and their own emotions remains understudied. Similar to survivors, caregivers have to cope with fear and uncertainty about the future. They may be confronted with complicated caregiving tasks and long-lasting role changes in the relationship (LeSeure and Chongkham-Ang, 2015). In the present study, we have addressed some of the psychological complexities in interpersonal emotion regulation by caregivers of cancer survivors.
Improving the wellbeing of cancer survivors is a central concern for caregivers, often achieved by fostering pleasant, or hedonic, emotions—relieving the cancer survivor's suffering and improving their good spirits. However, there are situations where promoting others' broader wellbeing may be accompanied by momentary discomfort (Niven et al., 2009). In such cases, caregivers may intentionally lead the survivor to feel worse. Zaki (2020) has characterized the latter form of interpersonal emotion regulation as paternalistic because regulators assume they know what is best for the person whose emotions they are trying to influence.
Zaki (2020) has further distinguished empathically based altruistic motives, often accompanied by feelings of love or companionship, as drivers of interpersonal emotion regulation. Although altruism is an important source of motivation in caring for cancer survivors, caregivers also have their own needs. The task of caring for a cancer survivor is emotionally taxing and often carried out over the years (Kim and Given, 2008; Kent et al., 2016; Üzar-Özçetin and Dursun, 2020). Additionally, caregivers often have to grapple with their own emotional vulnerabilities, such as sadness or existential fears. Such self-serving motivations can be legitimate but may conflict with the immediate interests of cancer survivors. The latter, paternalistic and self-centric aspects of interpersonal emotion regulation have, to date, received little attention in research on care for cancer survivors.
Similar to survivor-centric (altruistic) motivations for interpersonal emotion regulation, caregiver-centric (self-serving) motivations may target both the hedonic and counter-hedonic emotional states of cancer survivors. To serve their own emotional needs, caregivers sometimes evoke positive and sometimes negative emotions in cancer survivors. When we combine caregivers' motivations with the target emotions of cancer survivors, four caregiver orientations emerge. The resulting model of interpersonal emotion regulation by caregivers for cancer survivors is summarized in Table 1. Notably, these orientations are ideal types that are separated only for analytical purposes. In real-life situations, altruistic and self-serving motives can be expected to co-occur, and changes in situational demands may prompt caregivers to shift between hedonic and counter-hedonic regulation. In everyday life, caregivers' behavior is thus likely to be a blend of these different orientations.
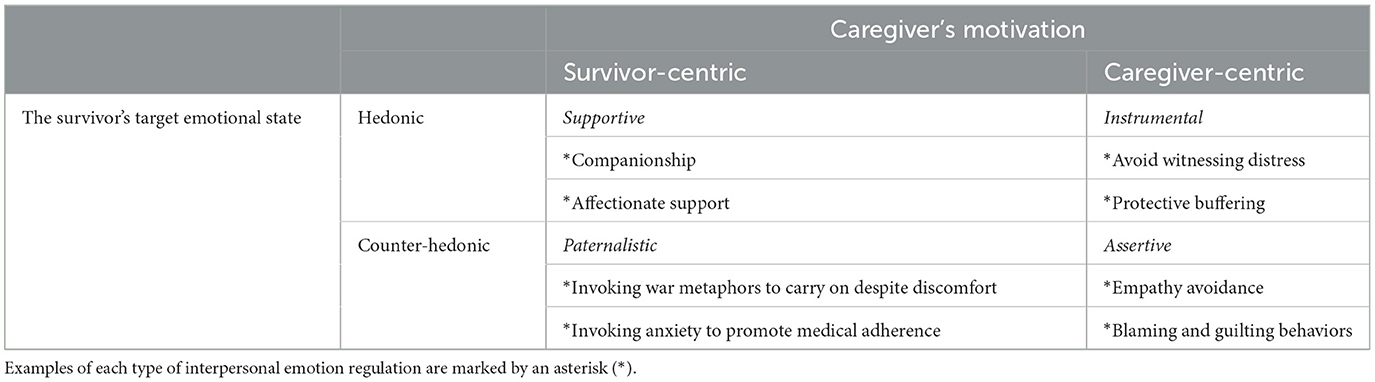
Table 1. A 2 × 2 model of interpersonal emotion regulation by caregivers to cancer survivors.
The 2 × 2 model depicted in Table 1 is novel and thus still awaits systematic empirical testing. Nonetheless, in the following sections, we demonstrate the utility of the model by considering how it may also serve as an integrative framework for existing research findings.
Survivor-centric interpersonal emotion regulation is often aimed at making cancer survivors feel better. This form of supportive regulation has, to date, been the main focus of research on interpersonal emotion regulation among cancer survivors (Zeng et al., under review) (see text footnote 1). As shown in the top left quadrant of Table 1, examples include offering companionship (Thomas et al., 2002) and affectionate support, i.e., physical demonstrations of love and care (Alison Payne et al., 2008). Although these supportive strategies are important and highly meaningful, not all survivor-centric interpersonal emotion regulations are aimed at promoting more positive hedonic states in cancer survivors.
More specifically, the paternalistic type of interpersonal emotion regulation seeks to evoke more negative emotions. Caregivers do not do this because they want to make cancer survivors suffer, but rather because they believe that certain negative emotions may have instrumental benefits for cancer survivors. As depicted in the bottom left quadrant of Table 1, one negative emotion that caregivers may strive to promote in cancer survivors is anger. For instance, it is well documented that many caregivers use war metaphors to describe living and coping with cancer (Penson et al., 2004; Semino et al., 2018). To carry on, caregivers may encourage survivors to disregard inconveniences in the present and to firmly focus on fighting and getting through this period. While cancer survivors are often put off by war metaphors (Semino et al., 2018), caregivers might still want to use them because they believe that anger and aggressiveness can mobilize survivors' energies in facing challenges.
Another negative emotion that caregivers may sometimes seek to induce in cancer survivors is (mild) anxiety. Anxiety is known to promote watchfulness (Derakshan and Eysenck, 2009). Consequently, when cancer survivors are not sufficiently watchful, caregivers might attempt to instill mild levels of anxiety in cancer survivors to ensure that the latter engage in necessary preventive behaviors, such as regular check-ups and medication adherence (Oliveria et al., 2013; Seibel et al., 2023). A qualitative study among 25 German survivors after curative lung cancer treatment and 17 caregivers on cancer follow-up perceptions revealed that many caregivers encourage cancer survivors to undergo regular health checks, even when these evoke “Scanxiety” among cancer survivors (Seibel et al., 2023). Overall, though research on these topics is scarce, some initial evidence that caregivers engage in paternalistic forms of interpersonal emotion regulation are available.
There is a large body of research on caregiver burdens (Liu et al., 2020). Nonetheless, caregiver-centric motives for interpersonal emotion regulation have, to date, not received much attention. In general, well-adjusted relationships always involve a joint consideration of one's own and others' interests (Helgeson and Fritz, 2000; Oakley, 2013). It is in the best interest of both the survivors and caregiver, particularly in the long run, that caregivers appropriately attend to their own emotional needs (Lambert et al., 2012; Girgis et al., 2013; Sklenarova et al., 2015). Addressing caregiver-centric motivations is therefore potentially useful in maintaining high-quality care for cancer survivors.
Caregiver-centric interpersonal emotion regulation may be aimed at enhancing positive emotions in cancer survivors. For instance, caregivers may sometimes find it hard to witness cancer survivors' emotional distress and may, at least from time to time, want to avoid being confronted with it. The self-serving motivation to escape survivors' distress is psychologically distinct from the altruistic motive to alleviate another person's suffering (Batson et al., 1987). Caregivers may thus seek to provide emotional comfort to cancer survivors in order to they feel better themselves. As noted in the lower right quadrant of Table 1, one example of such instrumental regulation is protective buffering, defined as “withholding or denying cancer-related thoughts and concerns from one's partner, hiding dispiriting information, and acquiescing to avoid conflict” (Langer et al., 2009, p. 4312). Although protective buffering might superficially appear altruistic, it is often used by caregivers to protect themselves from personal negative feelings from upsetting the cancer survivor (Langer et al., 2009). Unfortunately, this instrumental form of interpersonal emotion regulation may unintentionally increase the psychological distance between the caregiver and cancer survivor (Winterheld, 2017).
Finally, the assertive type of interpersonal emotion regulation aims to induce counter-hedonic emotional states in cancer survivors to enhance the feelings of the caregiver. Because it may cause emotional discomfort among cancer survivors, the assertive type is probably the most controversial form of interpersonal emotion regulation. However, there are situations where assertive regulation is at least somewhat legitimate. Caring for cancer survivors imposes significant burdens on caregivers, especially when this responsibility extends over an extended period, which is increasingly common (Kim and Given, 2008; Guerra-Martín et al., 2023). To be able to carry these burdens, caregivers must address their own needs, even if, at least in the short run, this causes emotional discomfort for cancer survivors. Two illustrative examples of the assertive type are shown on the lower right side of Table 1.
One form of assertive interpersonal emotion regulation may be empathy fatigue, a phenomenon in which caregivers experience a gradual decline in empathy toward cancer survivors (see also Cavanagh et al., 2020; Shi et al., 2022). A study of 117 cancer healthcare professionals in Ireland indicates that over a quarter of cancer care professionals report a certain level of empathy fatigue (Hunt et al., 2019). Empathy fatigue may be a protective mechanism that prevents emotional exhaustion in caregivers (Lelorain et al., 2012; see also Tops et al., 2015). Another instance of assertive interpersonal emotion regulation may occur when caregivers engage in guilting and blaming behaviors toward cancer survivors. A study involving 304 Canadian dyads of lung cancer survivors and caregivers observed that caregivers were more inclined to blame survivors, especially if they continued to smoke (Lobchuk et al., 2012). Such blaming tendencies may negatively impact the quality of caregiving but may still serve an adaptive role, perhaps by allowing caregivers and cancer survivors to achieve a more balanced give-and-take in their relationship (Taurisano et al., 2023).
Caring for cancer survivors is a complex task with multiple psychological facets. In this study, we have proposed a 2 × 2 model of interpersonal emotion regulation by caregivers for cancer survivors. The model considers how caregivers may not only seek to make cancer survivors feel better but also, at times, may actively strive to make cancer survivors feel worse, even when caregivers have cancer survivors' best interests at heart. Moreover, caregivers may sometimes regulate cancer survivors' emotional states for reasons that are at least somewhat self-serving rather than purely altruistic. Interpersonal emotion regulation by caregivers can thus be supportive (survivor-centric hedonic), paternalistic (survivor-centric counter-hedonic), instrumental (caregiver-centric hedonic), or assertive (survivor-centric counter-hedonic).
Each of these four types of interpersonal emotion regulation entails trade-offs between specific psychological costs and benefits. For instance, the supportive type may allow cancer survivors to feel better but may also create undesirable emotional dependencies (Helgeson and Fritz, 2000). The paternalistic type may promote cancer survivors' long-term interests but may also lead cancer survivors to experience some amount of emotional discomfort (Seibel et al., 2023). The instrumental type may prevent immediate emotional distress in cancer survivors but often creates more psychological distance between cancer survivors and caregivers (Langer et al., 2009). In addition, the assertive type may prevent exhaustion among caregivers but tends to come at the expense of cancer survivors' immediate emotional needs (Chen et al., 2023). These trade-offs merit attention in the future research. Furthermore, it would be insightful to know whether and how caregivers can flexibly switch between or combine the four types of interpersonal emotion regulation. Such flexibility may be vital for the mental health and wellbeing of caregivers and cancer survivors (Kashdan and Rottenberg, 2010).
Our selective review of the literature found preliminary empirical support for the types of processes that are postulated by the 2 × 2 model of interpersonal emotion regulation by caregivers for cancer survivors. Nevertheless, it is important to keep in mind that the relevant empirical studies were not specifically designed to test the 2 × 2 model. The contribution of the present article is, therefore, primarily conceptual. Future research is needed to examine the 2 × 2 model across diverse caregiving contexts and cultural backgrounds to verify its applicability and robustness.
Psychological care for cancer survivors is challenging. To meet this challenge, it is vital to consider not only the perspective of survivors but also that of caregivers. Addressing both perspectives may promote understanding between caregivers and cancer survivors, fostering the development of more mutually beneficial relationships.
ZZ: Conceptualization, Funding acquisition, Resources, Writing – original draft. KH: Supervision, Validation, Writing – review & editing. SK: Funding acquisition, Supervision, Visualization, Writing – review & editing, Conceptualization.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This article was facilitated by a scholarship of the Chinese Scholarship Council (202206720004) and Postgraduate Scientific Research Innovation Project of Hunan Province (CX20230459) to ZZ and NWO Open Competition Grant 406.18.GO.024 to SK.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. ^Zeng, Z., Holtmaat, K., Jia, X., Burchell, G. L., Verdonck-de Leeuw, I. M., and Koole, S. L. (under review). Interpersonal Emotion Regulation and Mental Health Among Cancer Survivors: A Systematic Review.
Alison Payne, S., Seymour, J. E., Chapman, A., and Holloway, M. (2008). Older Chinese people's views on food: implications for supportive cancer care. Ethn. Health 13, 497–514. doi: 10.1080/13557850802023133
Batson, C. D., Fultz, J., and Schoenrade, P. A. (1987). Distress and empathy: two qualitatively distinct vicarious emotions with different motivational consequences. J. Pers. 55, 19–39. doi: 10.1111/j.1467-6494.1987.tb00426.x
Cavanagh, N., Cockett, G., Heinrich, C., Doig, L., Fiest, K., Guichon, J. R., et al. (2020). Compassion fatigue in healthcare providers: a systematic review and meta-analysis. Nurs. Ethics 27, 639–665. doi: 10.1177/0969733019889400
Chen, X., Wang, Z., Zhou, J., and Li, Q. (2023). A scoping literature review of factors influencing cancer patients' self-perceived burden. Eur. J. Oncol. Nurs. 68:102462. doi: 10.1016/j.ejon.2023.102462
Derakshan, N., and Eysenck, M. W. (2009). Anxiety, processing efficiency, and cognitive performance: New developments from attentional control theory. Eur. Psychol. 14, 168–176. doi: 10.1027/1016-9040.14.2.168
Fong, A. J., Scarapicchia, T. M., McDonough, M. H., Wrosch, C., and Sabiston, C. M. (2017). Changes in social support predict emotional well-being in breast cancer survivors. Psycho-oncology 26, 664–671. doi: 10.1002/pon.4064
Girgis, A., Lambert, S. D., McElduff, P., Bonevski, B., Lecathelinais, C., Boyes, A., et al. (2013). Some things change, some things stay the same: a longitudinal analysis of cancer caregivers' unmet supportive care needs. Psycho-oncology 22, 1557–1564. doi: 10.1002/pon.3166
Guerra-Martín, M. D., Casado-Espinosa, M. D. R., Gavira-López, Y., Holgado-Castro, C., López-Latorre, I., and Borrallo-Riego, Á. (2023). Quality of life in caregivers of cancer patients: a literature review. Int. J. Environm. Res. Public Health 20:1570. doi: 10.3390/ijerph20021570
Harms, C. A., Cohen, L., Pooley, J. A., Chambers, S. K., Galvão, D. A., and Newton, R. U. (2019). Quality of life and psychological distress in cancer survivors: the role of psycho-social resources for resilience. Psycho-oncology 28, 271–277. doi: 10.1002/pon.4934
Helgeson, V. S., and Fritz, H. L. (2000). The implications of unmitigated agency and unmitigated communion for domains of problem behavior. J. Pers. 68, 1031–1105 doi: 10.1111/1467-6494.00125
Hunt, P., Denieffe, S., and Gooney, M. (2019). Running on empathy: Relationship of empathy to compassion satisfaction and compassion fatigue in cancer healthcare professionals. Eur. J. Cancer Care 28:e13124. doi: 10.1111/ecc.13124
Kashdan, T. B., and Rottenberg, J. (2010). Psychological flexibility as a fundamental aspect of health. Clin. Psychol. Rev. 30, 865–878. doi: 10.1016/j.cpr.2010.03.001
Kent, E. E., Rowland, J. H., Northouse, L., Litzelman, K., Chou, W. Y. S., Shelburne, N., et al. (2016). Caring for caregivers and patients: research and clinical priorities for informal cancer caregiving. Cancer 122, 1987–1995. doi: 10.1002/cncr.29939
Kim, Y., and Given, B. A. (2008). Quality of life of family caregivers of cancer survivors: across the trajectory of the illness. Cancer 112, 2556–2568. doi: 10.1002/cncr.23449
Lambert, S. D., Harrison, J. D., Smith, E., Bonevski, B., Carey, M., Lawsin, C., et al. (2012). The unmet needs of partners and caregivers of adults diagnosed with cancer: a systematic review. BMJ Support. Palliat. Care.2, 224–300 doi: 10.1136/bmjspcare-2012-000226
Langer, S. L., Brown, J. D., and Syrjala, K. L. (2009). Intrapersonal and interpersonal consequences of protective buffering among cancer patients and caregivers. Cancer 115, 4311–4325. doi: 10.1002/cncr.24586
Lelorain, S., Brédart, A., Dolbeault, S., and Sultan, S. (2012). A systematic review of the associations between empathy measures and patient outcomes in cancer care. Psycho-Oncology 21, 1255–1264. doi: 10.1002/pon.2115
LeSeure, P., and Chongkham-Ang, S. (2015). The experience of caregivers living with cancer patients: a systematic review and meta-synthesis. J. Pers. Med. 5, 406–439. doi: 10.3390/jpm5040406
Li, Y., Wang, K., Yin, Y., Li, Y., and Li, S. (2018). Relationships between family resilience, breast cancer survivors' individual resilience, and caregiver burden: a cross-sectional study. Int. J. Nurs. Stud. 88, 79–84. doi: 10.1016/j.ijnurstu.2018.08.011
Liu, Z., Heffernan, C., and Tan, J. (2020). Caregiver burden: a concept analysis. Int. J. Nurs. Sci. 7, 438–445. doi: 10.1016/j.ijnss.2020.07.012
Lobchuk, M. M., McClement, S. E., McPherson, C. J., and Math, M. C. M. (2012). Impact of patient smoking behavior on empathic helping by family caregivers in lung cancer. Oncol. Nurs. Forum 39, e112–e121. doi: 10.1188/12.ONF.E112-E121
Niven, K., Totterdell, P., and Holman, D. (2009). A classification of controlled interpersonal affect regulation strategies. Emotion 9, 498–509. doi: 10.1037/a0015962
Oakley, A. (2013). “Interviewing women: a contradiction in terms,” in Doing Feminist Research (London: Routledge), 30–61.
Oliveria, S. A., Shuk, E., Hay, J. L., Heneghan, M., Goulart, J. M., Panageas, K., et al. (2013). Melanoma survivors: health behaviors, surveillance, psychosocial factors, and family concerns. Psycho-oncology 22, 106–116. doi: 10.1002/pon.2059
Penson, R. T., Schapira, L., Daniels, K. J., Chabner, B. A., and Lynch, T. J. (2004). Cancer as metaphor. Oncologist 9, 708–716. doi: 10.1634/theoncologist.9-6-708
Seibel, K., Sauer, B., Wagner, B., and Becker, G. (2023). “Scanxiety” and a sense of control: the perspective of lung cancer survivors and their caregivers on follow-up-a qualitative study. BMC Psychol. 11:119. doi: 10.1186/s40359-023-01151-0
Semino, E., Demjén, Z., and Demmen, J. (2018). An integrated approach to metaphor and framing in cognition, discourse, and practice, with an application to metaphors for cancer. Appl. Linguist. 39, 625–645.
Shi, H., Shan, B., Zheng, J., Zhang, Y., Zhang, J., and Hu, X. (2022). Grief as a mediator of the relationship between empathy and compassion fatigue. Psycho-oncology 31, 840–847. doi: 10.1002/pon.5875
Sklenarova, H., Krümpelmann, A., Haun, M. W., Friederich, H. C., Huber, J., Thomas, M., et al. (2015). When do we need to care about the caregiver? Supportive care needs, anxiety, and depression among informal caregivers of patients with cancer and cancer survivors. Cancer 121, 1513–1519. doi: 10.1002/cncr.29223
Taurisano, P., De Feudis, R. L., Graziano, G., Marzano, N., Curci, A., Fidanzio, A., et al. (2023). Patient-caregiver relationship in cancer fatigue and distress. A dyadic approach. Current Psychol. 42, 28167–28179. doi: 10.1007/s12144-022-03860-y
Thomas, C., Morris, S. M., and Harman, J. C. (2002). Companions through cancer: the care given by informal carers in cancer contexts. Soc. Sci. Med. 54, 529–544. doi: 10.1016/S0277-9536(01)00048-X
Tops, M., Schlinkert, C., Tjew-A-Sin, M., Samur, D., and Koole, S. L. (2015). “Protective inhibition of self-regulation and motivation: extending a classic Pavlovian principle to social and personality functioning,” in Handbook of Biobehavioral Approaches to Self-Regulation, eds. G. H. E. Gendolla, M. Tops, and S. L. Koole (Cham: Springer Science + Business Media), 69–85.
Üzar-Özçetin, Y. S., and Dursun, S. I. (2020). Quality of life, caregiver burden, and resilience among the family caregivers of cancer survivors. Eur. J. Oncol. Nurs. 48:101832. doi: 10.1016/j.ejon.2020.101832
Winterheld, H. A. (2017). Hiding feelings for whose sake? Attachment avoidance, relationship connectedness, and protective buffering intentions. Emotion 17, 965–980. doi: 10.1037/emo0000291
Keywords: psychological care, cancer survivors, paternalistic, assertive, instrumental, supportive, interpersonal emotion regulation
Citation: Zeng Z, Holtmaat K and Koole SL (2024) Psychological care for cancer survivors: a 2 × 2 model of interpersonal emotion regulation by caregivers. Front. Psychol. 15:1390692. doi: 10.3389/fpsyg.2024.1390692
Received: 23 February 2024; Accepted: 05 June 2024;
Published: 24 June 2024.
Edited by:
Rocio Guil, University of Cádiz, SpainReviewed by:
Kayi Ntinda, University of Eswatini, EswatiniCopyright © 2024 Zeng, Holtmaat and Koole. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zihao Zeng, ei56aWhhb0B2dS5ubA==
†ORCID: Zihao Zeng orcid.org/0000-0001-6503-6897
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.