 Alberto Stefana
Alberto Stefana Paolo Fusar-Poli1,2,3
Paolo Fusar-Poli1,2,3 Eduard Vieta
Eduard Vieta Eric A. Youngstrom
Eric A. Youngstrom- 1Department of Brain and Behavioral Sciences, University of Pavia, Pavia, Italy
- 2OASIS Service, South London and Maudsley NHS Foundation Trust, London, United Kingdom
- 3Early Psychosis: Interventions and Clinical-detection (EPIC) Lab, Department of Psychosis Studies, Institute of Psychiatry, Psychology & Neuroscience, King’s College London, London, United Kingdom
- 4Bipolar and Depressive Disorders Unit, Hospital Clinic, IDIBAPS, CIBERSAM, Institute of Neuroscience, University of Barcelona, Barcelona, Catalonia, Spain
- 5Institute for Mental and Behavioral Health Research, Nationwide Children’s Hospital and Department of Psychiatry, The Ohio State University, Columbus, OH, United States
- 6Helping Give Away Psychological Science, Chapel Hill, NC, United States
In this study, we examined how four components of the therapeutic relationship—working alliance, real relationship, and positive and negative affective reactions of the patient toward their therapist—relate to each other and to the psychotherapy session outcome, from the patient’s point of view. Our simple comprised 700 adult patients in individual psychotherapy who were recruited and participated online. They underwent a baseline evaluation of their most recent therapy session, which encompassed a series of validated self-report measures focused on specific elements of the therapeutic relationship. The results revealed that, from the patient’s perspective, working alliance, real relationship, and positive affective reactions toward the therapist were positively correlated with session outcome, while negative affective reactions were negatively correlated. All components predicted session outcome when simultaneously included in a regression model. Collectively, these four components accounted for 30% of the variance in session outcome. Factor analysis revealed four distinct factors, underlying perceptions of the therapeutic relationship. Notably, the bond dimension of the alliance was sufficiently different from the task and goal dimensions, warranting consideration as a distinct construct. These findings, although cross-sectional, lay the groundwork for a more nuanced investigation of multiple dimensions of the therapeutic relationship.
Introduction
The patient–therapist relationship is a fundamental component of psychotherapy (Høglend, 2014; Norcross and Lambert, 2018) and any intervention focused on mental health (San and Arranz, 2023). Meta–analytic estimates show that it accounts for approximately 15% of the total variance in adult psychotherapy outcomes, with the patient contributing 30%, the therapist 7%, and the specific treatment method ranging from 0 to 10% (Norcross and Lambert, 2019; see also Wampold and Imel, 2015). These data underscore the importance of investigating underexplored facets and dynamics of the therapeutic relationship (TR). Some experts advocate a transition from a holistic analysis to a more detailed exploration of its specific elements (Horvath, 2009; Bhatia and Gelso, 2018).
Two models that provide a nuanced understanding of TR are Bruce Wampold’s contextual model of psychotherapy (Wampold and Budge, 2012; Wampold and Imel, 2015) and Charles Gelso’s tripartite model of the TR (Gelso, 2014; Gelso, 2018). The contextual model, also known as the “common factors” model, posits that psychotherapy is based on an initial patient–therapist bond and unfolds through three pathways (Wampold, 2017): (a) The real relationship between the patient and the therapist provides the patient with an empathic and caring connection, beneficial to his/her health. (b) The therapist helps the patient understand the origins of their mental disorder and offers ways to cope and overcome their difficulties, fostering hope that they will be successful in completing therapy tasks and managing their problems. (c) Therapy–specific techniques and strategies can create expectations in the patient and facilitate healthy behavior changes. A psychotherapeutic treatment that incorporates these three pathways to some extent will be effective. The significance of these common factors is well-supported by empirical evidence and is crucial across various therapeutic approaches (Bailey and Ogles, 2023).
Within this metamodel of psychotherapy, a model of the TR can be embedded. The tripartite model identifies three interconnected elements: the real relationship, the working alliance, and the transference–countertransference configuration. Evidence indicates that the tripartite model predicts 27% of the variance in session outcomes, however, factor analysis revealed that items from the four therapeutic relationship measures emerged as four separate factors, albeit with some degree of overlap (Bhatia and Gelso, 2018).
Although individual studies have examined elements of the therapeutic relationship (TR) as components of the therapeutic process, few have explored the interplay between these elements, often relying on the therapist’s perspective. Consequently, patient ratings can provide valuable information to theoretically model the TR. In this context, our research represents an opportunity to enhance the understanding of the TR by integrating patient feedback. Specifically, our objective was to explore a quadripartite model (different from that theorized by Charles Gelso) of the TR from the perspective of patients, encompassing the working alliance, the real relationship, and positive and negative affective reactions toward the therapist. Theoretically, these affective reactions can be seen as a conscious phenotype of what some contemporary psychoanalysts call transference (Westen and Gabbard, 2002; Bradley et al., 2005). Specifically, our exploration focused on three broad domains:
a. The relationship between patient–rated working alliance, real relationship, positive and negative affective reactions, and patient–rated session outcome.
b. The interrelations among the four components of the TR.
c. The grouping of items from the measures of the four components and the factors that emerged from this merged item pool through exploratory factor analysis.
Methods
Dataset
This research report outlines a secondary analysis of baseline data from a longitudinal study, as described in the study protocol by Stefana et al. (2024c). The Institutional Review Board of the University of North Carolina at Chapel Hill (UNC-CH) approved the study (IRB number: 23–0216; approval date: March 6, 2023).
Participants
Participants in the study were 700 adults who underwent individual psychotherapy in the United States. Most participants (70%) received treatment in private practice settings. The remaining participants were distributed among private health institutions (11%), public health institutions (10%), and other settings (9%), such as university counseling centers. The demographic distribution included 81% females (n = 564), with 74% (n = 512) identifying with woman gender. The primary age groups represented were 23–29 years (20%, n = 142) and 30–39 years (28%, n = 193). The majority of ethnicities were Caucasian, comprising 81% (n = 566) of the participants. A predominant proportion, 84% (n = 590), had been diagnosed with at least one psychiatric ailment, with anxiety (66%, n = 464) and unipolar depression (56%, n = 391) being the most prevalent conditions. The patients received different types of psychotherapy. Table 1 details the demographic, contextual, and therapeutic characteristics of the sample. All information, including psychiatric diagnosis, was self-reported.
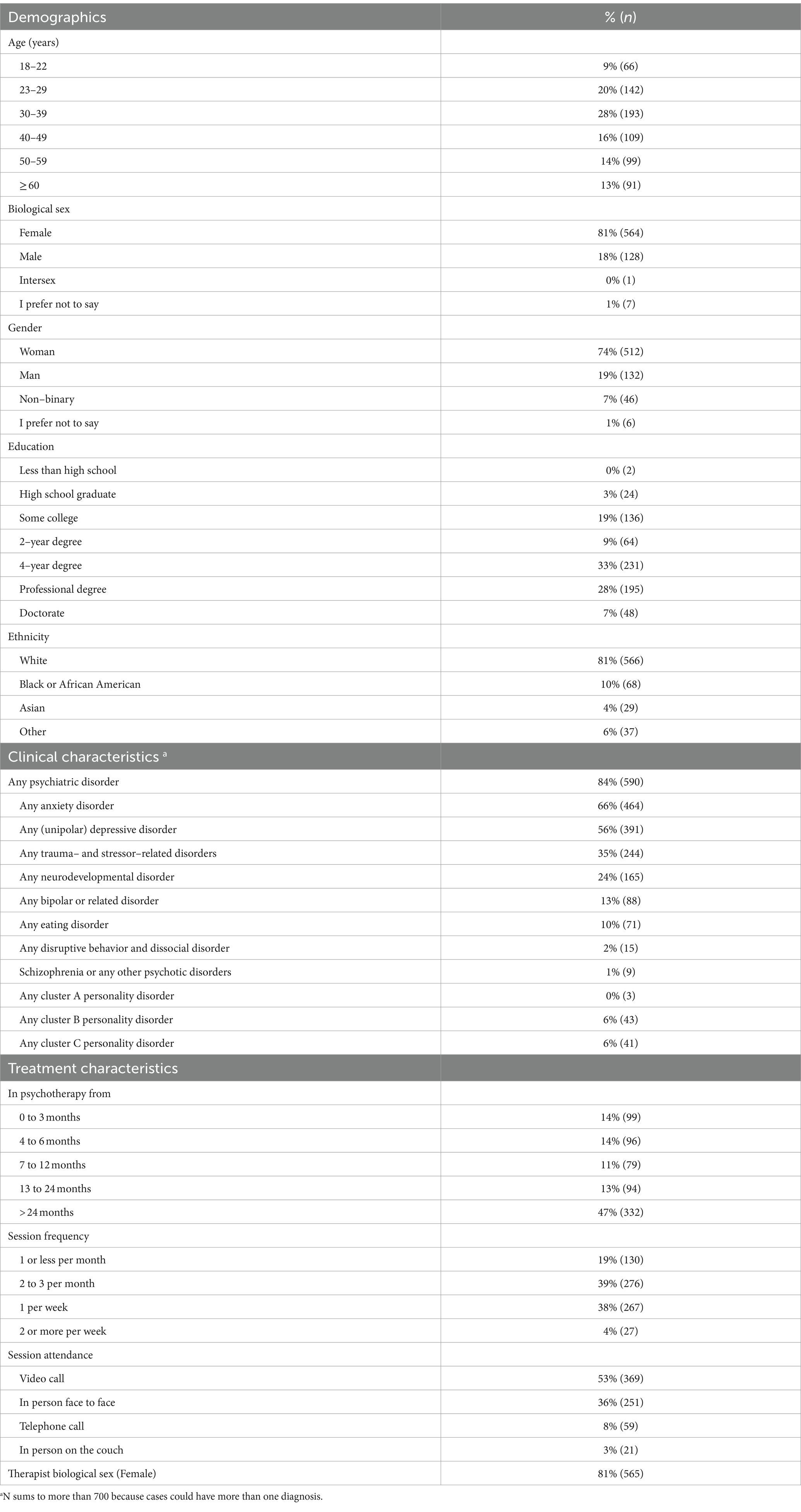
Table 1. Demographics, contextual, and treatment characteristics of participating patients (N = 700).
Measures
Sociodemographic and clinical domain
A sociodemographic and clinical data form was specifically designed for this study to capture the information reported in Table 1.
Therapeutic relationship domain
The Working Alliance Inventory–Short Revised (WAI–SR) (Hatcher and Gillaspy, 2006), a 12–item self–report measure of the working alliance in psychotherapy sessions. WAI–SR is based on Bordin (1979) theory of the working alliance and encompasses three subscales with four items each: agreement on therapy tasks, agreement on therapy goals, and the establishment of an affective bond between the patient and the therapist. The items are rated on a Likert scale ranging from 0 (“Not at all”) to 5 (“Completely”). In this study, the WAI–SR total scale showed an internal consistency Cronbach’s alpha value of 0.95. Furthermore, in previous studies, the WAI–SR has shown good convergent validity, correlated well with other established measures such as the Helping Alliance Questionnaire (r = 0.71) (Munder et al., 2009).
The Real Relationship Inventory–Client–Short Form (RRI–C–SF) (Stefana et al., 2024a) is an 8–item self–report measure of perception of the strength of the real relationship between patient and therapist from the perspective of the former. It contains two subscales of four items each: Realism and Genuineness. Ratings are made on a Likert scale, ranging from 1 (“Strongly disagree”) to 5 (“Strongly agree”). Higher scores indicate a stronger real relationship. In our study, Cronbach’s alpha and the average item correlation for the total scale were, respectively, 0.97 and 0.55. Real relationship has demonstrated strong convergence validity with both the construct of working alliance (r = 0.66 between RRI and total WAI scores) (Vaz et al., 2023) and the patient perceptions of genuineness or congruence (r = 0.71 with the dimension of congruence of the Barrett–Lennard Relationship Inventory) (Kelley et al., 2010).
The in–Session Patient Affective Reactions Questionnaire (SPARQ) (Stefana et al., 2023, 2024b) is an 8–item self–report questionnaire that assesses the perceptions and affective reactions of the patient toward his/her therapist during their individual psychotherapy session. It contains two subscales of four items each: Positive Affect (PA) and Negative Affect (NA). The SPARQ-PA scale captures the perception of a secure and comfortable relationship with his/her therapist from the perspective of the patient. The SPARQ-NA scale captures feelings of shyness, shame, fear of speaking openly, worry about not getting needed help, and a sense of failure due to his/her need for help from the therapist. Items are rated on a Likert scale ranging from 0 (“Not at all true”) to 4 (“Very true”). The two scales provide two distinct scores that cannot be summated with each other. In the current study, the Cronbach alpha values were 0.75 for the NA scale and 0.86 for the PA scale.
Session outcome domain
The Session Evaluation Scale (SES) (Hill and Kellems, 2002; Lent et al., 2006) is a 5–item self–report scale that assesses the perception of the quality of a therapy session. Four of the items are rated on a Likert scale ranging from 1 (“Strongly disagree”) to 5 (“Strongly agree”). These items require respondents to evaluate how pleased they were to have attended the most recent session, how satisfied they were with its outcome, and how helpful and valuable they found the session. An additional item is rated on a scale from 1 (“Very effective”) to 5 (“Ineffective”). The SES score is obtained by summing the values of the five items (after appropriate reversal is applied for two items) and then dividing by five. In our study, the SES showed an internal consistency Cronbach’s alpha value of 0.86.
Statistical analyses
Categorical variables were reported as frequencies, while continuous variables were described using means, standard deviations, and ranges. Pearson’s correlation analyses were used to investigate relationships between the components of the TR, as measured by WAI-SR, RRI-C-SF, and SPARQ-PA and-NA, and session outcomes, as measured by the SES. Then a multiple regression analysis was performed to determine the unique contribution of each component of the TR in predicting the session outcome, with session outcome as the dependent variable and the four components of the TR as independent variables. To explore the interrelations between the four components of the TR, Pearson’s correlation coefficients were calculated. Furthermore, partial correlation analyzes were performed to control for possible confounder variables, which involved calculating correlation coefficients between the variables of interest, with the effect of treatment length partialed out. To examine the underlying structure of the components of the TR when their items were grouped together, exploratory factor analysis (EFA) was performed using a principal-axis factoring method and oblique rotation. The suitability of the data for factor analysis was evaluated using Bartlett’s sphericity test and the Kaiser-Meyer-Olkin test. Various methods, including the Hull method (Lorenzo-Seva et al., 2011), comparison data (Ruscio and Roche, 2012), Horn’s parallel analysis (Horn, 1965), and parallel analysis with principal component analysis and EFA, were employed to determine the optimal number of factors to retain. Items’ loadings were examined with a cutoff set at >0.30 (Raykov and Marcoulides, 2011). All analyzes were performed with R version 4.3.1.
Procedure
Data was collected from September to November 2023 through two online patient registers: Research for Me and ResearchMatch. Research for Me has been developed by the North Carolina Translational and Clinical Sciences Institute, which represents the collaborative efforts of the US National Institutes of Health under the Clinical and Translational Science Awards (CTSA) Program at UNC-CH. Similarly, ResearchMatch (Harris et al., 2012) originates from a collaboration of leading academic institutions, receiving support from the US National Institutes of Health through the CTSA Program. To qualify, participants had to be adults 18 years or older and underwent individual psychotherapeutic treatment. They also needed to be fluent in English and capable of providing informed consent. After consenting, the participants underwent a baseline evaluation of their most recent therapy session. The survey was carried out using Qualtrics software.
Results
Table 2 reports the mean, standard deviation, and item range for each measure of the TR used in this study. The SPARQ-NA exhibited positive skewness. Consequently, a logarithmic transformation was applied to the data and the natural logarithms of the values of the SPARQ-NA variable were used in all subsequent correlation and regression analyzes. The positively skewed distribution of the data for this variable is congruent with how we expect negative emotions toward the therapist to be experienced during sessions by the patients (i.e., rare to have strong negative feelings after most typical sessions). Moreover, despite the skewed distribution, the SPARQ-NA has demonstrated theoretically meaningful correlations with the other variables.
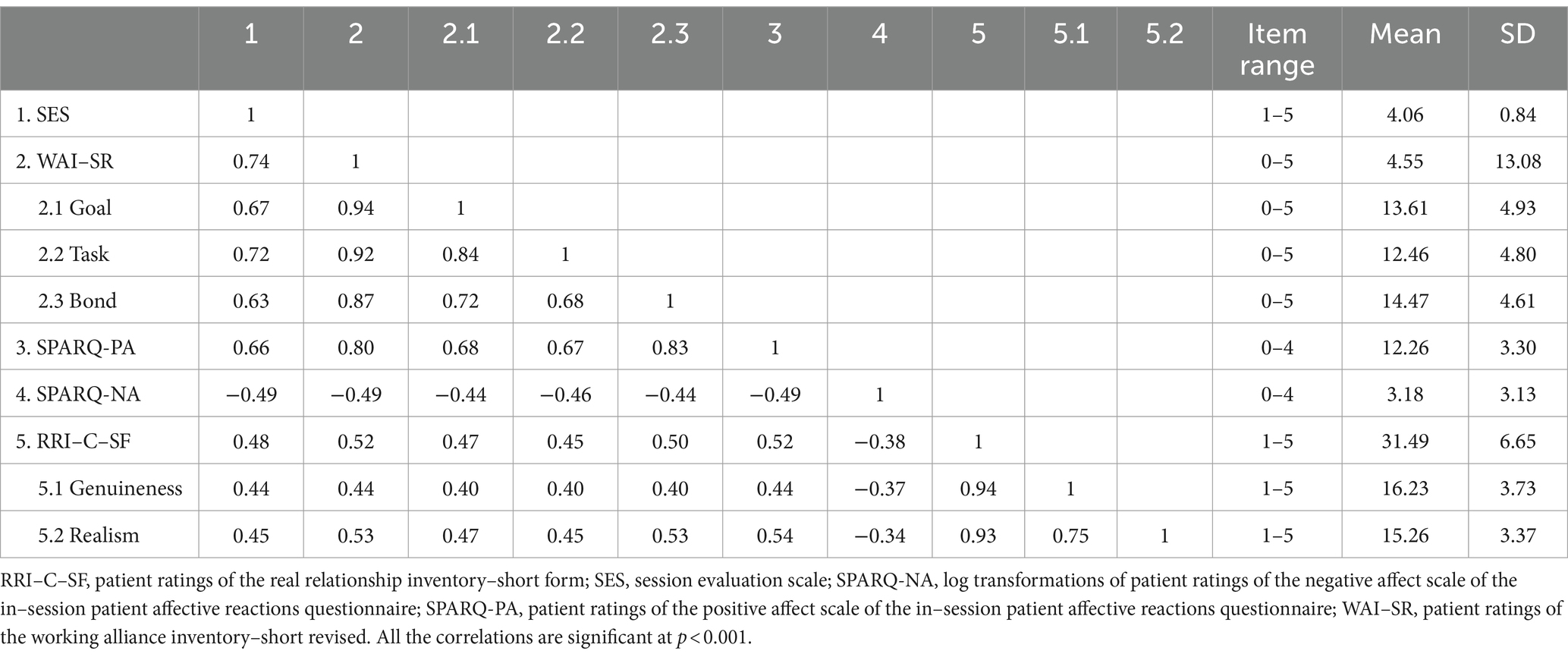
Table 2. Descriptive statistics and correlation matrix for study variables.
Considering the varied settings of the psychotherapy sessions within the sample, items related to the setting of the session (either in–person face–to–face, in–person on the couch, by video call, or over the telephone) were examined for correlations with the components of the TR and the outcome of the session, as reported by the patients. This was to determine any potential associations between the setting of the session and the constructs of the study. The results did not reveal significant correlations between the setting of the session and the relational and outcome measures used in the study. Specifically, the correlation coefficients for the outcome measure (sestot_t0) ranged from −0.07 (telephone call) to 0.03 (in-person face-to-face), and for the relational measures, the correlation coefficients ranged from −0.08 (WAI bond in telephone call) to 0.08 (WAI task in telephone call).
A similar rationale was applied to investigate the impact of session frequency and duration of treatment on elements of TRs and session outcome. Analysis of variance (ANOVA) revealed that there were no significant differences in the means of TR or outcome measures across various session frequencies, namely, once a month or less, two to three times a month, once a week or two or more times a week. On the contrary, significant differences were observed in the means of TR and outcome measures over different durations of treatment. Specifically, WAI–SR, SPARQ-PA, and SES demonstrated significant differences at the 0.01 significance level between patients treated for 0 to 3 months and those treated for over 24 months. Furthermore, SPARQ-PA and SES exhibited significant differences at the 0.01 level between patients treated for 4–6 months and those treated for over 24 months. For all three measures, the trend is toward improvement with longer treatment durations. SPARQ-NA revealed significant differences between patients treated for 0 to 3 months (p < 0.01) or 4 to 6 months (p = 0.02) and those treated for more than 24 months. The trend for SPARQ Negative Affect is towards improvement (reduction in negative affect) with longer treatment durations, especially notable in patients treated for more than 24 months. RRI–C–SF did not show significant differences.
Relationship between measures of therapeutic relationship and session outcome
The outcome of the patient-rated session outcome related positively to the patient-rated working alliance (r = 0.74, p < 0.001), real relationship (r = 0.48, p < 0.001), and positive affective reactions toward the therapist (r = 0.66, p < 0.001), and negatively to the negative affective reactions of the patient toward the therapist (r = −0.49, p < 0.001).
A simultaneous regression (Table 3) was conducted to examine the contributions of the working alliance, the real relationship and negative affective reactions toward the therapist, as perceived by the patients, to the patients’ ratings of session outcome. In this model, session outcome was the dependent variable. The results indicated that these four components together accounted for 30% of the variance in the session outcome (Adj.R2 = 0.58, F = 238, p < 0.001). All predictors in the model had a statistically significant effect on session outcome (see Table 2), with working alliance showing the strongest association (partial r = 0.53, p < 0.001) after adjusting for all other components. To explore the potential impact of the length of treatment, regression analyses were performed with treatment length partialed out. These analyzes showed that the relationships between variables remained significant and showed almost identical correlation values, indicating that the duration of treatment did not play a significant role in the relationships observed in this sample.

Table 3. Simultaneous regression model: therapeutic relationship components predicting session outcome.
Interrelations between the four components of the therapeutic relationship
As hypothesized, there is a positive correlation between the working alliance and the real relationship (r = 0.48, p < 0.001) and the positive affective reactions towards the therapist (r = 0.80, p < 0.001), as well as between these latter two components (r = 0.52, p < 0.001). Furthermore, as hypothesized, the negative affective reactions of the patients towards the therapist were negatively related to both alliance (r = −0.49, p < 0.001), real relationship (r = −0.49, p < 0.001), and positive affective reactions (r = −0.49, p < 0.001).
To account for the significant variability in treatment length within our sample, we performed additional correlation analyses with treatment length partialed out. The results mirrored the original analysis in terms of magnitude and significance, indicating that the duration of treatment does not significantly influence the relationships among the components of the TR examined in this study.
Factoring the model of the therapeutic relationship
The Bartlett test of sphericity (p < 0.001) and the Kaiser–Meyer–Olkin test (0.96) verified the suitability of the data for factor analysis. The Hull method (Lorenzo-Seva et al., 2011) and the parallel analysis with PCA and EFA all suggested retaining four factors. EFA revealed that the four–factor solution explained 64.3% of the variance. The four factors (considering items with factor loadings >0.30) closely resembled the original components: (i) working alliance, (ii) positive and (iii) negative affective reactions toward the therapist, and (iv) real relationship. The first factor emerging from the principal–axis factor analysis included the goal and task items of the working alliance, as well as the item (with a negative loading) “I felt worried my therapist could not help me,” which pertains to the negative affect reaction toward the therapist. The second factor perfectly corresponded to the real relationship. The third factor comprised all items of the positive affective reaction toward the therapist, in addition to the bond item of the working alliance. The fourth and final factor included the four items of the negative affect reaction toward the therapist. Table 4 (Model A) reports item loadings from exploratory factor analysis of combined TR components.
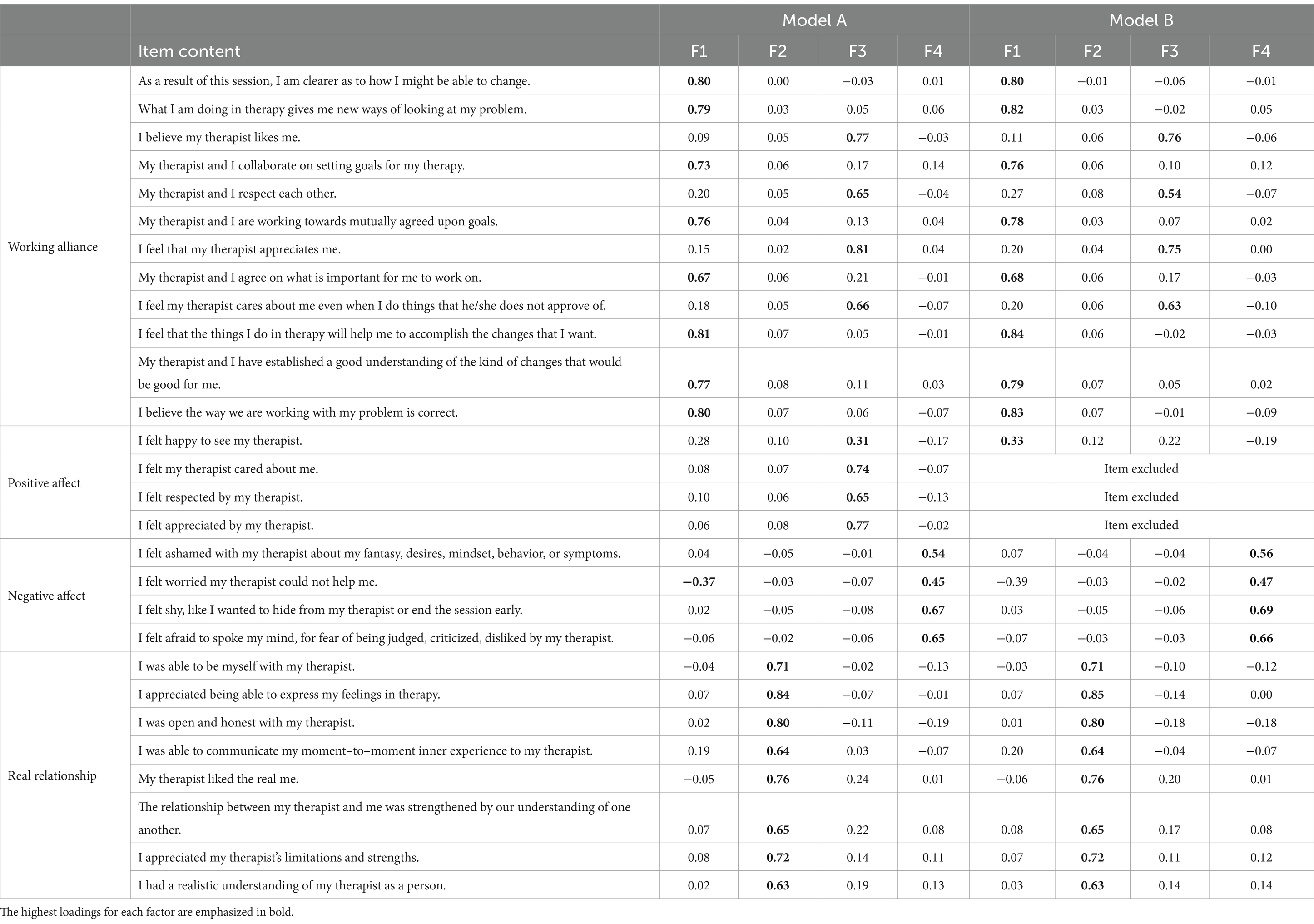
Table 4. Item loadings from exploratory factor analysis of combined therapeutic relationship components.
Since three of the four bond items of the working alliance cover contents similar to three of the four items of positive affective reactions towards the therapist (correlation values were 0.79 for appreciation, 0.72 for respect, and 0.67 for care), we performed sensitivity analyses, conducted a parallel analysis and an exploratory factor analysis with an item pool that excluded the three items of the SPARQ. Analyses indicated four factors with the same pattern of loadings although the fourth factor had fewer items and was borderline in terms of size compared to parallel analysis (Table 4, Model B).
Discussion
This study is among the few to have examined multiple elements of the TR simultaneously, from the patient’s perspective. The working alliance, the real relationship, and the positive and negative affective reactions toward the therapist together accounted for 30% of the variance in the outcomes of the session as rated by the patients. From the patient’s perspective, these four components of the TR were correlated with session outcomes to varying degrees. Moreover, they were found to be interrelated, yet distinctly separate entities. The findings of the present study add to the growing body of literature investigating the value of examining specific components of the TR.
We first investigated how the working alliance, the real relationship, and positive and negative affective reactions were correlated with the session outcome rated by the patients. Consistent with previous findings (Flückiger et al., 2020b), a stronger alliance was associated with a more positive session outcome. The magnitude of this correlation in our sample (r = 0.74) was consistent with that (r = 0.72) detected in a similar study that investigated the TR from the therapist’s perspective (Bhatia and Gelso, 2018). Not surprisingly, it was much stronger than the r = 0.23–31 found in meta-analyses of alliance–treatment outcome associations for adult psychotherapy (Flückiger et al., 2018, 2020a). This difference is explained by the fact that our outcome pertained to the session rather than the treatment outcome, as in the meta-analyses.
Similarly, patients who experienced positive affective reactions toward the therapist tended to perceive the session as of higher quality. The only previous study that has explored the correlation between session outcome (the same inventory used in the present study) and the positive affective response of the patient to the therapist as measured through the SPARQ-PA, showed a r of 0.64 (n = 475) (Stefana et al., 2024d). Furthermore, our finding of a large correlation value (r = 0.66) between the positive affective response and the session outcome is consistent with the correlation between the bond alliance dimension and the session outcome (r = 0.63). This similarity may be attributed to a significant overlap in the content of items measuring the bond dimension of the WAI-SR and the SPARQ-PA.
Patients who perceived a strong real relationship with their therapists were also likely to rate the session positively. This finding (r = 0.48) aligns with previous studies investigating this correlation from patients’ or therapists’ perspectives, which reported correlation coefficients ranging from 0.32 to 0.63 (Bhatia and Gelso, 2018; Marks et al., 2019; Pérez-Rojas and Gelso, 2020). These findings are consistent with existing meta-analytic findings (Gelso et al., 2018), which revealed an r of 0.38.
Lastly, the presence of negative reactions toward the therapist was associated with a lower quality of the session, as the patient rated. A previous study explored the association between SPARQ-NA and session outcomes, revealing similar results (r = −0.51) (Stefana et al., 2024d). Furthermore, the direction of our findings is theoretically meaningful and aligns with previous research on the correlation between therapist-rated session outcome and negative transference (Bhatia and Gelso, 2018). The difference in the magnitude of the correlations (r = −0.49 in our study versus r = 0.25 in previous research) may be explained by the likelihood that negative affective reactions encompass, but are not limited to, negative transference reactions.
In summary, the working alliance, the real relationship, and the positive and negative reactions of the patient toward the therapist are significantly related to the patient’s evaluation of the session outcome. A key finding of our study is that the negative affects experienced by patients toward their therapists during sessions are related to the session outcome with a lower magnitude than the positive affects. This suggests that in-session negative emotional reactions have a lesser impact on session quality compared to positive reactions. The working bond and the real relationship likely act as a buffer against negative affective reactions.
Although the simultaneous regression model primarily highlights the importance of the working alliance, the relevance of other components of the TR should not be prematurely dismissed. The roles of the real relationship, as well as positive and negative in-session reactions toward the therapist, may be better understood in relation to the working alliance. From the patient’s perspective, stronger in-session negative emotions are associated with weaker alliance and real relationship, aligning with the literature that examined negative transference (Marmarosh et al., 2009; Bhatia and Gelso, 2018). The interconnections between these components of the TR represent a potentially fruitful area of research.
In the present study, we made an initial attempt to understand the interconnections among the four elements of the TR by examining how items from the employed measures are grouped from the patient’s perspective. A principal-axis factor analysis revealed four factors that almost exactly corresponded to those posited by the respective measures. It is important to note that the SPARQ-PA and-NA tools use the same item format, and the formats of the other measures are also similar. Items of the bond dimension of the WAI-SR loaded on the same factor as items from the SPARQ-PA, but not on the factor with the RRI-C-SF items. This suggests that the bond of the alliance—an attachment reflecting the feelings and attitudes experienced by members of the therapeutic dyad toward each other (Hatcher and Barends, 2006; Pérez-Rojas et al., 2019)—differs substantially from the task and goal dimensions of the alliance, which are cognitive aspects emphasizing consensus or negotiation about therapy goals and the tasks required to achieve them (Mallinckrodt and Tekie, 2016).
The most significant theoretical (and potentially clinical) implication of this study’s findings pertains to the construct of alliance. Unlike the theory that alliance should be considered as comprising an emotional component (corresponding to the WAI bond dimension) and a cognitive component (corresponding to the WAI goals and tasks dimensions) (Wampold and Flückiger, 2023), we hypothesize that these components can and should be regarded as distinct constructs. This suggests that clinicians cannot simply focus on conveying information clearly and coherently. To increase the persuasive prominence of information, agreement on goals, and assignment of treatment tasks, it is crucial to invest in enhancing the bond dimension of the relationship (which is the patient’s emotional belief that their therapist cares for them, understands them, and will make efforts to support them). However, further research is needed to confirm this hypothesis.
Contrary to what has been theorized in the literature (Gelso, 2011), the working alliance and the real relationship inventory had no items that cross-loaded onto each other’s factors. More broadly, items from the real relationship did not show any non-trivial cross-loading, indicating that the bond dimension of factor 3 may be composed, at least to some extent, of transference and countertransference elements.
In general, factor analysis reveals how items from the four patient-rated TR measures used in this study coalesce into four distinct factors, demonstrating a limited yet theoretically meaningful degree of overlap. Findings offer support for a quadripartite model of integral elements from the patient’s perspective in the TR: the working alliance, real relationship, and positive and negative affective reactions towards the therapist. Theoretically, the positive and negative affective reactions of patients towards their therapist can be conceptualized as two specific patterns of transference (Westen and Gabbard, 2002; Bradley et al., 2005) that manifest within the TR. From a clinical perspective, these results highlight the importance for therapists of adopting a holistic approach that considers all components of the TR to optimize therapy outcomes.
Limitations
The results of the present study should be considered in light of some limitations. First, the ecological validity of this study is limited by its cross-sectional design. The components of the TR can evolve throughout therapy (Gelso et al., 2012). Longitudinal research is necessary to elucidate how these components develop and interact over time. Second, our sample consisted only of self-selected participants who were informed about the general topic of the study: the TR. Consequently, their decision to participate may have been influenced by their personal views or experiences with therapy. Lastly, regarding future research, perspectives from therapists and/or external observers should be incorporated alongside those of the patients to provide a more comprehensive understanding.
Conclusion
The findings of the present study sustain the importance of the relationship in healing. More specifically, they demonstrate that, from the patient’s perspective, the components of a quadripartite model of the TR encompassing the working alliance, real relationship, and positive and negative affective reactions towards the therapist account for a substantial amount of variance in session outcomes as rated by the patients. A deeper understanding of the relationship between the components of the TR and the outcomes of the session (and treatment) outcomes will enable the therapists to focus on those components that can improve or detract from the session outcome, both in terms of quality and effectiveness. Moreover, the results suggest that the affective bond dimension of the working alliance is a distinct construct from the cognitive task and goal dimensions. A crucial clinical takeaway is the importance of establishing and maintaining a positive alliance with patients.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the corresponding author upon reasonable request.
Ethics statement
The Institutional Review Board of the University of North Carolina at Chapel Hill (UNC-CH) approved the study (IRB number: 23–0216; approval date: March 6, 2023). The study was conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AS: Conceptualization, Formal analysis, Funding acquisition, Writing – original draft, Writing – review & editing. PF-P: Funding acquisition, Supervision, Writing – review & editing. EV: Supervision, Writing – review & editing. EY: Funding acquisition, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study has received funding from the European Union’s Horizon 2020 research and innovation program under the Marie Sklodowska-Curie grant agreement No. 101030608.
Conflict of interest
EY has received royalties from the American Psychological Association and Guilford Press, and consulted about psychological assessment with Signant Health. He is the co-founder and Executive Director of Helping Give Away Psychological Science (HGAPS.org). EV has received grants and served as consultant, advisor or CME speaker for the following entities: AB-Biotics, AbbVie, Adamed, Angelini, Biogen, Biohaven, Boehringer-Ingelheim, Celon Pharma, Compass, Dainippon Sumitomo Pharma, Ethypharm, Ferrer, Gedeon Richter, GH Research, Glaxo-Smith Kline, HMNC, Idorsia, Johnson & Johnson, Lundbeck, Medincell, Merck, Newron, Novartis, Orion Corporation, Organon, Otsuka, Roche, Rovi, Sage, Sanofi-Aventis, Sunovion, Takeda, and Viatris, outside the submitted work.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Bailey, R. J., and Ogles, B. M. (2023). Common factors therapy: a principle-based treatment framework : APA Books.
Bhatia, A., and Gelso, C. J. (2018). Therapists’ perspective on the therapeutic relationship: examining a tripartite model. Couns. Psychol. Q. 31, 271–293. doi: 10.1080/09515070.2017.1302409
Bordin, E. S. (1979). The generalizability of the psychoanalytic concept of the working alliance. Psychotherapy 16, 252–260. doi: 10.1037/h0085885
Bradley, R., Heim, A. K., and Westen, D. (2005). Transference patterns in the psychotherapy of personality disorders: empirical investigation. Br. J. Psychiatry 186, 342–349. doi: 10.1192/bjp.186.4.342
Flückiger, C., Del Re, A. C., Wampold, B. E., and Horvath, A. O. (2018). The alliance in adult psychotherapy: a meta-analytic synthesis. Psychotherapy 55, 316–340. doi: 10.1037/pst0000172
Flückiger, C., Del Re, A. C., Wlodasch, D., Horvath, A. O., Solomonov, N., and Wampold, B. E. (2020a). Assessing the alliance–outcome association adjusted for patient characteristics and treatment processes: a meta-analytic summary of direct comparisons. J. Couns. Psychol. 67, 706–711. doi: 10.1037/cou0000424
Flückiger, C., Rubel, J., Del Re, A. C., Horvath, A. O., Wampold, B. E., Crits-Christoph, P., et al. (2020b). The reciprocal relationship between alliance and early treatment symptoms: a two-stage individual participant data meta-analysis. J. Consult. Clin. Psychol. 88, 829–843. doi: 10.1037/ccp0000594
Gelso, C. J. (2011). The real relationship in psychotherapy. Washington: American Psychological Association.
Gelso, C. (2014). A tripartite model of the therapeutic relationship: theory, research, and practice. Psychother. Res. 24, 117–131. doi: 10.1080/10503307.2013.845920
Gelso, C. J. (2018). The therapeutic relationship in psychotherapy practice: an integrative perspective. 1st Edn. Abingdon, Oxon: Routledge.
Gelso, C. J., Kivlighan, D. M., Busa-Knepp, J., Spiegel, E. B., Ain, S., Hummel, A. M., et al. (2012). The unfolding of the real relationship and the outcome of brief psychotherapy. J. Couns. Psychol. 59, 495–506. doi: 10.1037/a0029838
Gelso, C. J., Kivlighan, D. M., and Markin, R. D. (2018). The real relationship and its role in psychotherapy outcome: a meta-analysis. Psychotherapy 55, 434–444. doi: 10.1037/pst0000183
Harris, P. A., Scott, K. W., Lebo, L., Hassan, N., Lightner, C., and Pulley, J. (2012). ResearchMatch: a National Registry to recruit volunteers for clinical research. Acad. Med. 87, 66–73. doi: 10.1097/ACM.0b013e31823ab7d2
Hatcher, R. L., and Barends, A. W. (2006). How a return to theory could help alliance research. Psychother. Theory Res. Pract. Train. 43, 292–299. doi: 10.1037/0033-3204.43.3.292
Hatcher, R. L., and Gillaspy, J. A. (2006). Development and validation of a revised short version of the working alliance inventory. Psychother. Res. 16, 12–25. doi: 10.1080/10503300500352500
Hill, C. E., and Kellems, I. S. (2002). Development and use of the helping skills measure to assess client perceptions of the effects of training and of helping skills in sessions. J. Couns. Psychol. 49, 264–272. doi: 10.1037/0022-0167.49.2.264
Høglend, P. (2014). Exploration of the patient-therapist relationship in psychotherapy. Am. J. Psychiatry 171, 1056–1066. doi: 10.1176/appi.ajp.2014.14010121
Horn, J. L. (1965). A rationale and test for the number of factors in factor analysis. Psychometrika 30, 179–185. doi: 10.1007/BF02289447
Horvath, A. O. (2009). How real is the “real relationship”? Psychother. Res. 19, 273–277. doi: 10.1080/10503300802592506
Kelley, F. A., Gelso, C. J., Fuertes, J. N., Marmarosh, C., and Lanier, S. H. (2010). The real relationship inventory: development and psychometric investigation of the client form. Psychother. Theory Res. Pract. Train. 47, 540–553. doi: 10.1037/a0022082
Lent, R. W., Hoffman, M. A., Hill, C. E., Treistman, D., Mount, M., and Singley, D. (2006). Client-specific counselor self-efficacy in novice counselors: relation to perceptions of session quality. J. Couns. Psychol. 53, 453–463. doi: 10.1037/0022-0167.53.4.453
Lorenzo-Seva, U., Timmerman, M. E., and Kiers, H. A. L. (2011). The Hull method for selecting the number of common factors. Multivar. Behav. Res. 46, 340–364. doi: 10.1080/00273171.2011.564527
Mallinckrodt, B., and Tekie, Y. T. (2016). Item response theory analysis of working Alliance inventory, revised response format, and new brief Alliance inventory. Psychother. Res. 26, 694–718. doi: 10.1080/10503307.2015.1061718
Marks, E. C., Hill, C. E., and Kivlighan, D. M. (2019). Secrets in psychotherapy: for better or worse? J. Couns. Psychol. 66, 70–82. doi: 10.1037/cou0000311
Marmarosh, C. L., Gelso, C. J., Markin, R. D., Majors, R., Mallery, C., and Choi, J. (2009). The real relationship in psychotherapy: relationships to adult attachments, working alliance, transference, and therapy outcome. J. Couns. Psychol. 56, 337–350. doi: 10.1037/a0015169
Munder, T., Wilmers, F., Leonhart, R., Linster, H. W., and Barth, J. (2009). Working Alliance inventory-short revised (WAI-SR): psychometric properties in outpatients and inpatients. Clin. Psychol. Psychother. 17, 231–239. doi: 10.1002/cpp.658
Norcross, J. C., and Lambert, M. J. (2018). Psychotherapy relationships that work III. Psychotherapy 55, 303–315. doi: 10.1037/pst0000193
Norcross, J. C., and Lambert, M. J. (2019). “Evidence-based psychotherapy relationship: the third task force” in Psychotherapy relationships that work. eds. J. C. Norcross and M. J. Lambert (New York: Oxford University Press), 1–23.
Pérez-Rojas, A. E., and Gelso, C. J. (2020). International counseling students: acculturative stress, cultural distance, and the process of counseling with U.S. clients. Couns. Psychol. Q. 33, 352–374. doi: 10.1080/09515070.2018.1553145
Pérez-Rojas, A. E., González, J. M., and Fuertes, J. N. (2019). “The bond of the working alliance” in Working Alliance skills for mental health professionals. eds. A. E. Pérez-Rojas, J. M. González, and J. N. Fuertes (Oxford: Oxford University Press), 11–42.
Raykov, T., and Marcoulides, G. A. (2011). Introduction to psychometric theory. New York: Routledge.
Ruscio, J., and Roche, B. (2012). Determining the number of factors to retain in an exploratory factor analysis using comparison data of known factorial structure. Psychol. Assess. 24, 282–292. doi: 10.1037/a0025697
San, L., and Arranz, B. (2023). Effective patient-physician communication in the era of neuropsychopharmacology. Eur. Neuropsychopharmacol. 71, 1–2. doi: 10.1016/j.euroneuro.2023.02.007
Stefana, A., Fusar-Poli, P., Vieta, E., Gelso, C. J., and Youngstrom, E. A. (2024a). Development and validation of an 8-item version of the real relationship inventory–client form. Psychother. Res. doi: 10.1080/10503307.2024.2320331
Stefana, A., Fusar-Poli, P., Vieta, E., and Youngstrom, E. A. (2024b). Assessing the patient’s affective perception of their psychotherapist: validation of the in-session patient affective reactions questionnaire. Front. Psych. 15:1346760. doi: 10.3389/fpsyt.2024.1346760
Stefana, A., Fusar-Poli, P., Vieta, E., and Youngstrom, E. A. (2024c). Therapeutic relationship elements and therapy session outcomes: protocol for a longitudinal study of the patient’s perspective. Open research. Europe 3. doi: 10.12688/openreseurope.16466.2
Stefana, A., Langfus, J. A., Vieta, E., Fusar-Poli, P., and Youngstrom, E. A. (2023). Development and initial validation of the in-session patient affective reactions questionnaire (SPARQ) and the rift In-session questionnaire (RISQ). J. Clin. Med. 12:5156. doi: 10.3390/jcm12155156
Stefana, A., Vieta, E., Fusar-Poli, P., and Youngstrom, E. A. (2024d). Enhancing psychotherapy outcomes by encouraging patients to regularly self-monitor, reflect on, and share their affective responses toward their therapist: protocol for a randomized controlled trial. JMIR Res. Protocols 13:e55369. doi: 10.2196/55369
Vaz, A. M., Ferreira, L. I., Gelso, C., and Janeiro, L. (2023). The sister concepts of working alliance and real relationship: a meta-analysis. Couns. Psychol. Q. 37, 247–268. doi: 10.1080/09515070.2023.2205103
Wampold, B. E. (2017). “What should we practice?: a contextual model for how psychotherapy works” in The cycle of excellence. eds. T. Rousmaniere, R. Goodyear, S. D. Miller, and B. E. Wampold. 1st ed (Hoboken, NJ: Wiley), 49–65.
Wampold, B. E., and Budge, S. L. (2012). The 2011 Leona Tyler award address: the relationship—and its relationship to the common and specific factors of psychotherapy. Couns. Psychol. 40, 601–623. doi: 10.1177/0011000011432709
Wampold, B. E., and Flückiger, C. (2023). The alliance in mental health care: conceptualization, evidence and clinical applications. World Psychiatry 22, 25–41. doi: 10.1002/wps.21035
Wampold, B. E., and Imel, Z. E. (2015). The great psychotherapy debate: The evidence for what makes psychotherapy work. Second Edn. New York: Routledge.
Keywords: working alliance, real relationship, affective reaction, therapeutic relationship, session outcome, patients’ perspective
Citation: Stefana A, Fusar-Poli P, Vieta E and Youngstrom EA (2024) Patients’ perspective on the therapeutic relationship and session quality: the central role of alliance. Front. Psychol. 15:1367516. doi: 10.3389/fpsyg.2024.1367516
Edited by:
Jenifer L. Vohs, Indiana University School of Medicine, United StatesReviewed by:
Tomasz Prusiński, The Maria Grzegorzewska University, PolandJay A. Hamm, Eskenazi Health, United States
Stefano Barlati, University of Brescia, Italy
Georgius Esswein, Federal University of Health Sciences of Porto Alegre, Brazil
Copyright © 2024 Stefana, Fusar-Poli, Vieta and Youngstrom. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alberto Stefana, YWxiZXJ0by5zdGVmYW5hQGdtYWlsLmNvbQ==