
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol., 04 April 2024
Sec. Health Psychology
Volume 15 - 2024 | https://doi.org/10.3389/fpsyg.2024.1361767
 Julia Finsel1
Julia Finsel1 Angela Rosenbohm1
Angela Rosenbohm1 Raphael S. Peter2Hansjörg Bäzner3Axel Börtlein3Silke Dempewolf4Martin Schabet4Martin Hecht5Andreas Kohler6Christian Opherk6Andrea Nägele7
Raphael S. Peter2Hansjörg Bäzner3Axel Börtlein3Silke Dempewolf4Martin Schabet4Martin Hecht5Andreas Kohler6Christian Opherk6Andrea Nägele7 Norbert Sommer7Alfred Lindner8
Norbert Sommer7Alfred Lindner8 Dietrich Rothenbacher2
Dietrich Rothenbacher2 Albert C. Ludolph1,9
Albert C. Ludolph1,9 Gabriele Nagel2†
Gabriele Nagel2† Dorothée E. Lulé1*† on behalf of the ALS Registry Swabia Study Group
Dorothée E. Lulé1*† on behalf of the ALS Registry Swabia Study GroupBackground: Amyotrophic lateral sclerosis (ALS) is a fatal disorder, which imposes a severe emotional burden on patients. Appropriate coping mechanisms may alleviate this burden and facilitate wellbeing, with social support known to be a successful coping strategy. This observational study aimed to determine the interplay of general coping traits of hope for success and fear of failure, coping behavior of social activity, and patients' wellbeing.
Methods: In this cross-sectional study, patients with ALS from a clinical-epidemiological registry in Southwestern Germany were interviewed regarding coping traits (achievement-motivated behavior: hope for success and fear of failure), coping behavior of social activity, and psychosocial adjustment, determined using measures of depressiveness, anxiety [both measured by Hospital Anxiety and Depression Scale (HADS)], and quality of life [Anamnestic Comparative Self-Assessment (ACSA)]. Demographics, clinical [ALS Functional Rating Scale revised version (ALSFRS-R)], and survival data were recorded.
Results: A total of 868 patients [60.70% male patients, mean age: 64.70 (±10.83) years, mean ALSFRS-R: 37.36 ± 7.07] were interviewed. Anxiety in patients was found to be associated with a high fear of failure. In contrast, a generally positive attitude in patients exemplified in high hopes for success was associated with better wellbeing. Finally, coping behavior of social activity explained up to 65% of the variance of depressiveness among the patients with ALS.
Conclusion: In this study, we present evidence that the wellbeing of patients with ALS is not an immediate fatalistic consequence of physical degradation but rather determined by coping traits and behavior, which may be trained to substantially increase the wellbeing of patients with ALS.
Amyotrophic lateral sclerosis (ALS) is the most frequent adult-onset motor neuron disease with typical onset after 60 years of age, characterized by progressive physical, respiratory, and swallowing impairments. The median survival after disease onset ranges from 2 to 4 years (Chiò et al., 2009). During the disease course, patients have to deal with severe restrictions in daily life, intensive use of medical services, and physical dependency on others (Oliver et al., 2016), resulting in a tremendous emotional burden (McLeod and Clarke, 2007). Patients often experience heightened levels of depressiveness and anxiety in the initial phase of ALS and shortly after diagnosis (Kurt et al., 2007; Vázquez Medrano et al., 2020). However, a majority of patients may gain satisfactory wellbeing in the long course (Rabkin et al., 2000), despite increasing physical disability, even when reaching the locked-in state (Kuzma-Kozakiewicz et al., 2019). This aspect indicates that patients develop highly individualized coping strategies to preserve their psychological wellbeing.
This coping process depends on several intrinsic and extrinsic factors, of which the physical state is only one among many (Nelson et al., 2003). In general, coping can be categorized into coping strategies and coping styles (Lazarus and Folkman, 1984). Coping strategies involve distinct behavioral actions during a patient's stress episode (Lazarus and Folkman, 1984; Rabari et al., 2023). Most studies regarding coping in ALS focus on coping strategies (Matuz et al., 2010, 2015; Montel et al., 2012; Tramonti et al., 2012; Jakobsson Larsson et al., 2016; Leandro et al., 2022), with “seeking social support” being the primary coping strategy in the sense of efforts to seek information, emotional support, or instrumental support (Matuz et al., 2010; Leandro et al., 2022). Coping strategies are plentiful, but it has been theorized that individuals usually react to stressful situations in a certain way, based on a specific coping style (Roth and Cohen, 1986). Coping styles, or traits, are related to general personality traits and the result of previous experience (Lazarus and Folkman, 1984). Additionally, these styles are usually divided into the tendencies of approach and avoidance (Roth and Cohen, 1986). However, limited knowledge exists regarding coping traits according to personality traits in ALS, apart from an elevated anxiety trait being associated with decreased quality of life (QoL) (Siciliano et al., 2019). The specific personality traits of patients with ALS suggest a strong desire to excel in tasks and a high aim for achievement, compared to healthy controls (Parkin Kullmann et al., 2018). However, the extent to which coping traits affect the wellbeing of patients with ALS remains extensively unexplored, prompting us to address this gap.
A concept used to quantify these coping traits is the achievement-motivated behavior (AMB) (Atkinson, 1957). AMB reflects the general tendency of individuals to evaluate their behavior in situations where they perceive the potential to improve the outcomes (Atkinson, 1957). Achievement motive splits into approach (hope of success) and avoidance (fear of failure) tendencies (Atkinson, 1957; Heckhausen, 1963, 1991). The difference between hope of success and fear of failure serves as a predictor for the overall strength of individual's motives for achievements. These motives are regarded as a personality trait and are triggered by social incentives, such as external expectations (Atkinson, 1957). In ALS, the debilitating condition limits options to fulfill external expectations (e.g., lack of gratification in a job as most have to retire following the diagnosis), resulting in patient's mastery is primarily driven by their inner achievement motive. However, there is limited knowledge on how this inner achievement motive, as an indicator of coping traits, interacts with the successful psychosocial adaptation of patients affected by ALS.
The objective of this study was to characterize the potentially protective effect of general coping traits and current social behavior on the wellbeing of patients with ALS. To exclude selection bias stemming from highly motivated patients, we included a large cross-sectional sample of patients from the ALS registry Swabia in Southwestern Germany (Nagel et al., 2013), which is now among the most prominent European ALS registries and covers a majority (82%) of patients in this area.
This study is conducted as a cross-sectional and observational investigation and is part of the ALS registry Swabia in Southwestern Germany (Nagel et al., 2013), a clinical-epidemiological registry established in October 2010. Total ethical approvals were obtained from the ethical committees of the University of Ulm (No. 11/10), the medical association of the state of “Baden-Wuerttemberg” (Landesärztekammer, No. B-F-2010-062), and the medical association of the state of “Bayern” (No. 7/11300). All participants gave verbal and written informed consent prior to inclusion in the study. The study protocol with recruitment procedures, inclusion criteria, and details on the standardized data collection sheet have been previously published (Nagel et al., 2013; Rosenbohm et al., 2017). The relevant measures for this particular study are reported in detail under the Measures section. All patients underwent a neurological examination conducted by the collaborating neurologists. Additional clinical information and neuropsychological data were collected by neuropsychologists and trained study nurses using the standardized data collection sheet (Nagel et al., 2013). In a case-control study, healthy controls were interviewed who were matched for age, living area, and sex, for further details please see Nagel et al. (2013).
A total of 868 patients with ALS were interviewed (Table 1) (Nagel et al., 2013; Rosenbohm et al., 2017). The diagnosis was verified and classified according to the revised El Escorial criteria (Brooks et al., 2000; Ludolph et al., 2015). The mean age at the time of interview was 64.70 (± 10.83) years. The physical function was determined using the ALS functional rating scale revised version (ALSFRS-R) (Cedarbaum et al., 1999), ranging from 0 (no residual volitional motor control) to 48 points (full motor control). Patients exhibited moderate physical impairments (ALSFRS-R mean = 37.36 ± 7.07) with a mean bulbar involvement of 9.84 (±2.76; max. 12), a mean spinal involvement of 16.66 (±5.37; max. 24), and a mean respiratory involvement of 10.81 (±2.03; max. 12). Mean disease duration from symptom onset to interview was 14.68 (±11.44) months, indicating an early phase of the disease course. The progression rate (calculated as 48 minus current ALSFRS-R divided by months since symptom onset) ranged from moderate to fast (Kollewe et al., 2008) (mean = 1.07 loss of ALSFRS-R score per month ±1.13; Table 1). Patients' vital status was annually verified through record linkage with the central registration database and requests in the regional registration offices of Baden Württemberg and Bavaria. The censoring date for the survival analyses was October 30, 2021. In total, 604 (69%) died with the mean survival rate of 32.74 (±18.14) months after onset. A total of 788 healthy controls were interviewed in the case-control study (Nagel et al., 2013).
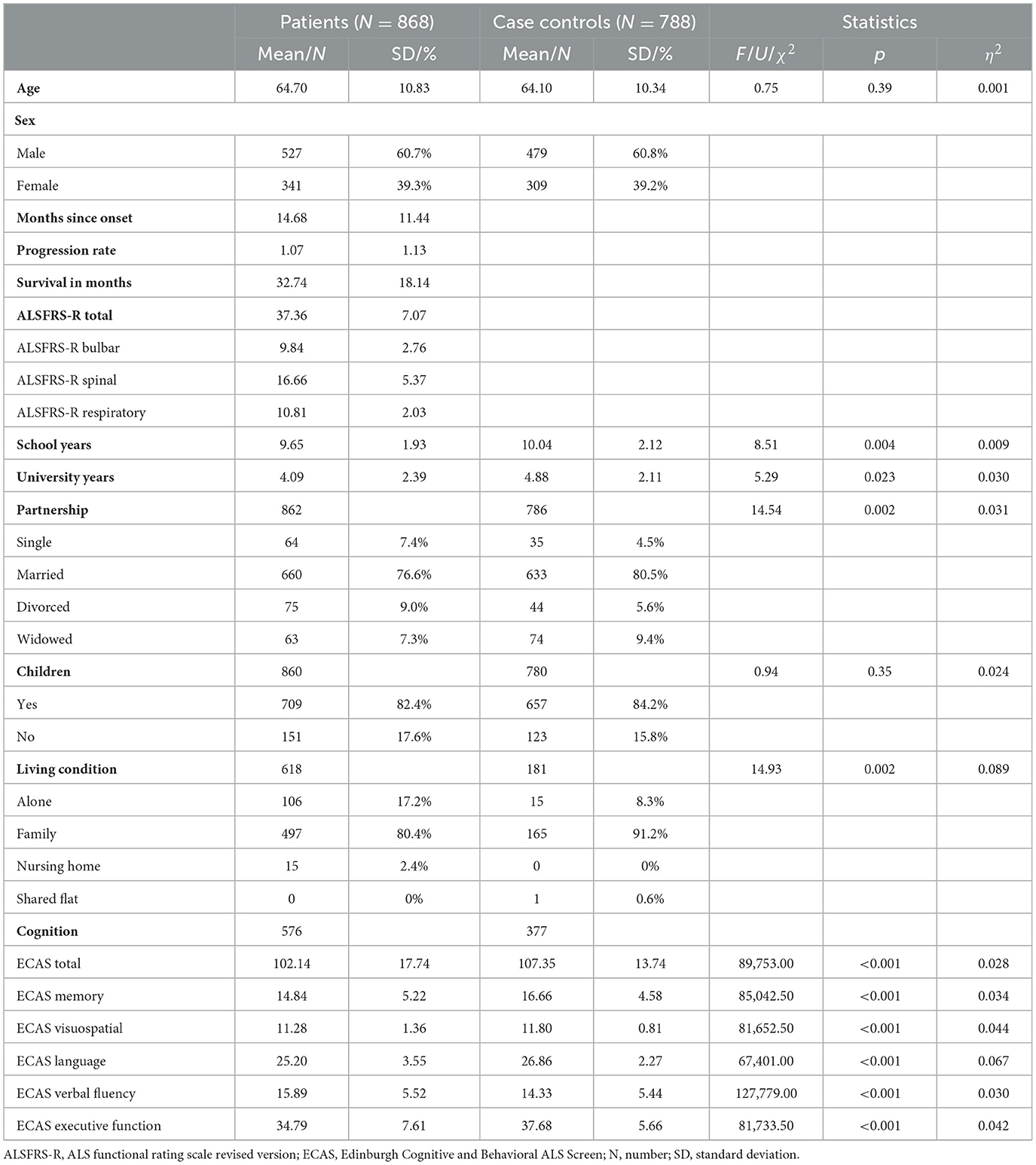
Table 1. Characteristics of ALS cases and healthy case controls.
The Edinburgh Cognitive and Behavioral ALS Screen (ECAS) (Abrahams et al., 2014; Lulé et al., 2015) is a specifically designed cognitive and behavioral instrument for patients with ALS to examine language, verbal fluency, executive functioning, memory, and visuospatial functioning. The concurrent validity of the German version with similar instruments is moderate to high (r = 0.46–0.58), showing high specificity (75%−100%), medium sensitivity (33%−50%), and moderate to high inter-rater reliability (Cohen's kappa value = 0.4–0.9) depending on the cognitive domain (Lulé et al., 2015).
A total of 576 patients were physically capable of completing the ECAS, while 377 controls were tested with the ECAS. Additionally, behavioral data were collected for 523 patients with interviews of caregivers (all first-degree relatives).
Coping traits regarding hope for success and fear of failure were determined using the short version of the Achievement Motive Scale (AMS) (Gjesme and Nygard, 1970; Lang and Fries, 2006), which consists of a 10-item scale with respective ratings ranging from 4 = strongly agree to 1 = strongly disagree. The achievement motive is determined according to either the component of hope for success (five items) or fear of failure (five items). The difference between both scales serves as a measure of the individual level of achievement motive. The reported internal consistency is Cronbach's alpha = 0.71–0.86, and the validity coefficient ranges between 0.51 and 0.79 (Lang and Fries, 2006).
Wellbeing was determined by measures of affective state (depressiveness and anxiety) and quality of life (QoL). Depressiveness and anxiety were examined using the self-reporting Hospital Anxiety and Depression Scale (HADS) (Herrmann-Lingen et al., 2011), with each scored between 0 and 21. Scores ranging between 11 and 21 indicated probable cases of clinically significant depressiveness and anxiety, respectively. Cronbach's alpha is reported as 0.67 to 0.93, sensitivity and specificity are both at 80%, and correlation with similar instruments is reported to be between 0.48 and 0.83 (Bjelland et al., 2002).
QoL was assessed with the Anamnestic Comparative Self-Assessment (ACSA) (Bernheim and Buyse, 1983; Bernheim, 1999). ACSA is a single-item instrument developed in clinical settings to assess subjective wellbeing. Participants were asked to define the periods of their best and worst QoL throughout their lifetime and to rate their current level (−5 = as bad as possible to +5 = as good as possible) according to the anchors of best and worst periods. Correlations with conventional happiness questions have been reported to range between 0.43 and 0.67 (Bernheim et al., 2006; Verhofstadt et al., 2019), while correlation with a multi-item life satisfaction instrument was reported as 0.59 (Bernheim et al., 2006). In patients with cancer, concurrent validity was further suggested by significant correlations between ACSA and the gravity of the disease, physical performance status, and response to treatment (Bernheim and Buyse, 1983).
Current behavior regarding social activity was defined according to the frequency of activities with family members and close friends (1 = less than once a month to 5 = on a daily base). Demographics such as the living situation (alone/with partner or family/others), partnership (single/married or partner/divorced/widowed), and the number of children were taken into consideration. Furthermore, participation in voluntary or club activities (yes/no) and hours dedicated to such activities were recorded. Club membership in Germany is the membership in an organization of society with specific goals, including clubs of physical activities, but also clubs of traditions (civic and home associations), clubs of specific hobbies (gardening, philately, animal breeding, etc.), clubs of music, clubs of environment and nature conservation, clubs for support groups (unemployment, alcoholism, patients with specific diseases or their caregivers, etc.), clubs of charity, clubs of worldview, and clubs of that particular in fundraising (for kindergartens, schools, theaters, individual education, etc.) (Müller-Jentsch, 2008).
Statistical analyses were conducted using IBM® SPSS version 25.0. All quantitative, continuous data are given as mean and SD. Categorical data are described as absolute frequencies and ratios. Due to the large sample size of N > 100 participants, normality distribution can be assumed (Lumley et al., 2002), and ANOVA, being robust to possible violations of non-normality (Blanca et al., 2017), was used to compare patients with controls for coping traits, current coping behavior, demographics (age, school years, years of university studies), and wellbeing. According to the Levene test, homogeneity of variances was present for all variables except for some subscores of the ECAS, so group comparisons for cognitive status were conducted using the Mann–Whitney-U tests. The chi-square test was conducted to compare partnership, number of children, and living conditions. Regression models and curve fit were conducted with independent variables for general coping traits of achievement motives (hope for success, fear of failure, total score) and current coping behavior (activity in voluntary work, club membership and with family members, demographics); dependent variable was defined as wellbeing (anxiety and depressiveness measured with HADS, subjective measure of global of life with ACSA). Due to large sample size, only predictors with p < 0.001 are considered significant. Regarding effect sizes, η2 = 0.01 indicates a small effect, η2 = 0.06 indicates a medium effect, and η2 = 0.14 indicates a large effect. All statistical tests, apart from the regression model, were two-sided, and the significance level was set at p = 0.05.
Compared to healthy controls, patients with ALS showed no significant differences with regard to demographics, apart from fewer university years, being single with a small effect size, and having more patients living alone with a medium effect size (Table 1).
A total of 90 (15.6%) patients exhibited mild cognitive impairments according to age and education-adjusted cut-offs (Loose et al., 2016). A total of 26 (6.9%) controls were found to have cognitive impairments according to the cut-offs mentioned above. Patients differed significantly from controls in all ECAS subscores (Table 1).
Apathy (N = 131, 25%) was the most common behavioral change in patients, followed by loss of social interest (N = 73, 14%), loss of compassion (N = 56, 11%), hyperorality (N = 40, 8%), stereotyped behavior (N = 28, 5%), which were subsumed under five behavioral domains (disinhibition, apathy, loss of sympathy, stereotyped behavior, and hyperorality); however, none of the participants fulfilled criteria of behavioral variant FTD according to Strong et al. (2017).
Patients with ALS showed reduced wellbeing, as evidenced by significantly higher anxiety and depressiveness scores (incidence of clinically relevant depression 4.6 vs. 28.2%, and anxiety 4.4 vs. 24.5%) and a lower subjective QoL. For both groups, wellbeing was in a neutral to positive range (mean 0.19 ± 2.37 vs. mean 2.34 ± 1.59; Table 2).
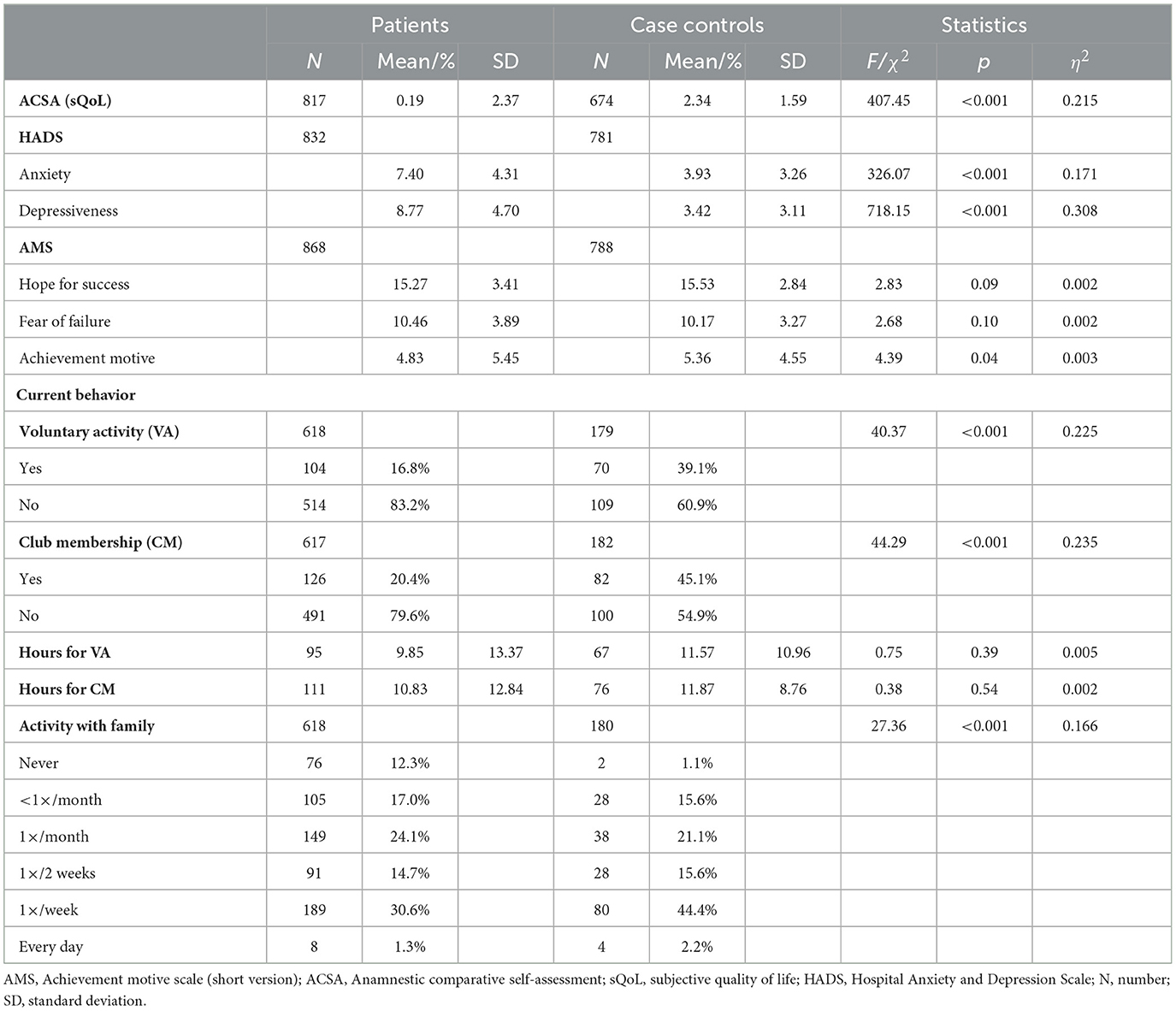
Table 2. Comparison of patients with ALS and healthy case-controls on general traits, wellbeing and current behavior.
Regarding coping traits, no significant group differences were found for the total achievement motive score, hope for success, or fear of failure.
Current coping behavior with regard to social activity was significantly different since patients spent less time with their families. Patients reported engaging in fewer social activities such as a club member or doing voluntary activity; the hourly effort for these activities was similar between both groups (Table 2).
The prediction model of psychosocial adaptation can be found in Figure 1. The most substantial effect was observed for anxiety (R2 = 0.173, F = 38.85, p < 0.001), which was predicted by fear of failure (B = 0.433 p < 0.001), explaining 43% of the variance, and hope for success, explaining 15% of the variance (B = 0.148, p = 0.007). Depressiveness was also predicted by coping traits of hope for success, explaining 30% of the variance (R2 = 0.146, F = 34.107, p < 0.001; B = −0.300, p < 0.001), and fear of failure accounting for 23% of the variance (B = 0.230, p < 0.001). Additionally, depressiveness was predicted by current coping behaviors of social activity (B = −0.647, p < 0.001), explaining 65% of the variance. Finally, QoL was determined by coping traits (R2 = 0.062, F = 12.252, p < 0.001), hope for success explained 7% (B = 0.073, p = 0.015) and fear of failure explained 10% (B = −0.099, p < 0.001). The current behavior of family activities explained 21% of the variance in QoL (B = 0.209, p = 0.004). A summary of the relationships between coping traits and coping behavior with wellbeing is shown in Table 3.
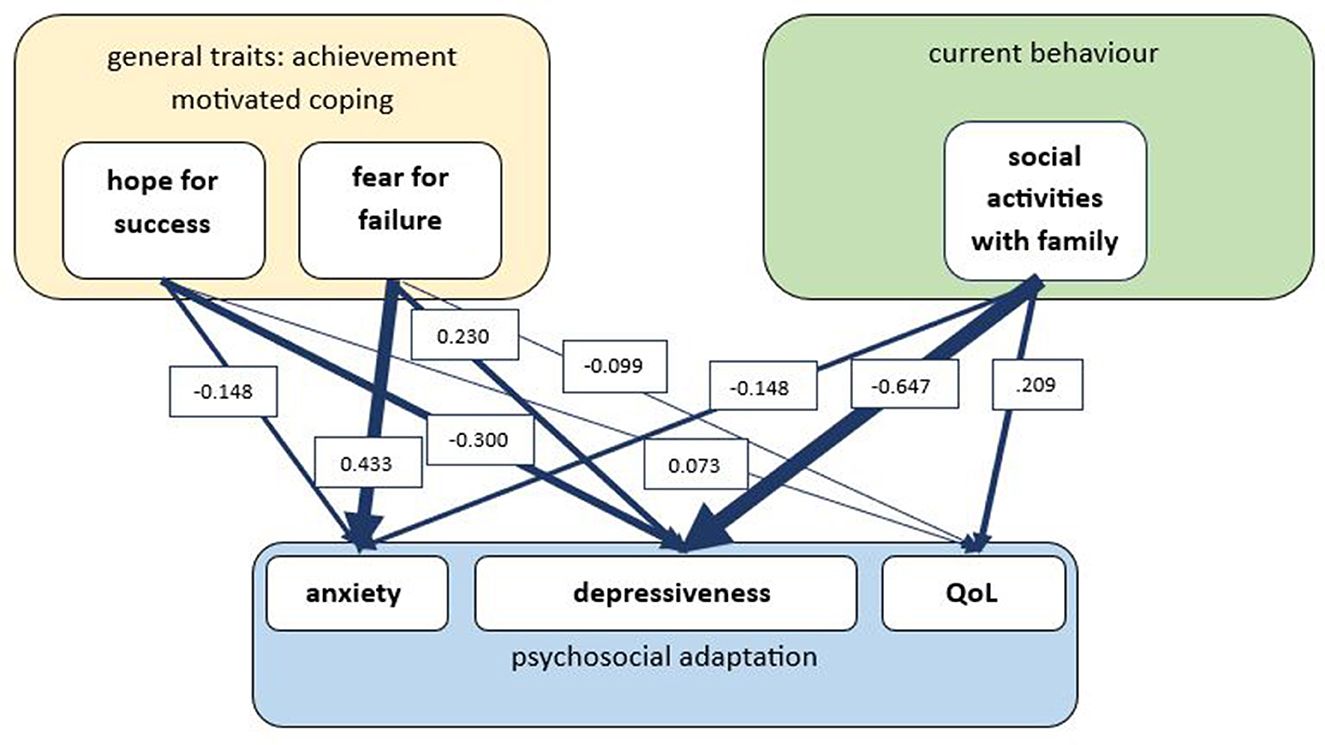
Figure 1. Prediction model of psychosocial adaptation. General traits of achievement motives are defined by hope of success and fear of failure (measured with Achievement Motive Scale, AMS); current behavior is defined by social activities with family members; psychosocial adaptation is defined by anxiety and depressiveness (measured with Hospital Anxiety and Depression Scale, HADS) and subjective quality of life (measured with Amnestic Comparative Self-Assessment, ACSA). Regression analysis with B-values indicating explained variance; due to large sample size, only predictors with p < 0.001 are considered significant.
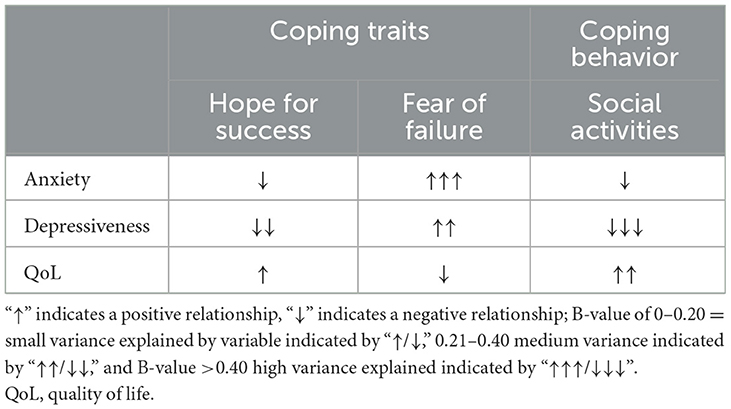
Table 3. Effect of coping traits and coping behavior on wellbeing.
None of the other factors (demographics, voluntary/club activity) were found to be significant predictors of wellbeing.
The Southwestern German ALS registry served as a platform for exploring the potentially protective effect of general coping traits and current social behavior on the wellbeing of patients with ALS. We present evidence that coping traits and behavior essentially predict psychosocial adaptation and, thus, wellbeing of patients with ALS. Subsequently, general traits of achievement motives predicted wellbeing similar to current behaviors of social participation. This study expands the current evidence on coping with ALS, which was primarily focused on researching coping strategies rather than traits (Matuz et al., 2010), and adds achievement motives as a potential element of the coping process to preserve wellbeing despite ALS. Furthermore, our results are in line with the model of coping proposed by Lazarus and Folkman (1984), wherein achievement motives as part of personality traits may influence of selection and implementation of coping behaviors (Lazarus and Folkman, 1984; Connor-Smith and Flachsbart, 2007). The link between personality and implemented coping strategies while dealing with severe diseases has also been demonstrated recently in patients with cancer (Rabari et al., 2023); however, the relationship between personality traits and coping strategies appears to vary across different population samples (Connor-Smith and Flachsbart, 2007).
The study provides evidence that the coping trait of hope for success has a positive effect on the wellbeing of patients with ALS, as measured by affective state and quality of life. Conversely, the effect of fear of failure is linked with increased anxiety and depressiveness. ALS is inherently associated with several losses in different contextual situations, which may not only include the loss of their physical strength and autonomy and possible dependence on the assistance of others for daily care and on medical devices for survival (The EFNS Task Force on Diagnosis and Management of Amyotrophic Lateral Sclerosis et al., 2012; Lulé et al., 2018) but may also include loss of the employment, leading to financial security and professional expression. Eventually, patients with ALS often confront the fact that they will be losing life itself within a short time frame. The patients who have always been anxious and afraid of losing, expressed in fear of failure, may suffer even more in the face of the multiple changes imposed on them in the context of ALS. Patients with a high fear of failure may feel less sense of control and may tend to use less problem-focused strategies. However, understanding of control and problem-focused strategies are both correlated with better wellbeing of patients with ALS (King et al., 2009; Matuz et al., 2015; Jakobsson Larsson et al., 2016). On the other hand, the patients who have a positive attitude, as expressed in hope for success, find it easier to cope with the devastating condition according the hereby presented data. This aspect aligns with earlier findings, wherein patients with ALS who exhibit positive action and positive thinking tend to experience fewer depressive symptoms (Jakobsson Larsson et al., 2016).
Our study revealed a general lower wellbeing of patients with ALS compared to controls, characterized by lower subjective QoL and higher rates of anxiety and depressiveness, highlighting the negative effects of the disease. Shortly after diagnosis, many patients show a reactive episode of low wellbeing, as indicated by increased depressiveness and low QoL (Vázquez Medrano et al., 2020). Our study population was in rather early disease stage. Additionally, the study population exhibited a rather high progression rate, which is known to be associated with low wellbeing (Lulé et al., 2013). However, psychosocial adaptation is possible in the course of ALS, despite the severity of the medical condition and the emotional burden it imposes. This phenomenon is a general one observed in severe diseases with different etiologies, subsumed under the wellbeing paradox (Herschbach, 2002). However, this adaptation is only achievable if certain prerequisites are fulfilled. According to the data presented, these prerequisites include extrinsic (current coping behavior, here measured with social activity) and intrinsic factors related to general coping traits. While we found no differences in general coping traits between patients with ALS and controls, patients reported less social activity compared to controls. This is unfortunate, since coping strategies of “seeking social support” have been shown to be the most successful coping strategy in ALS (Matuz et al., 2010, 2015; Tramonti et al., 2012; Leandro et al., 2022) and family members were named to be most helpful regarding coping (Hecht et al., 2002). Our data support this concept to be valid: social activities with family members explained up to 65% of the variance in depressiveness in patients with ALS and to a lesser degree of quality of life and anxiety. This effect can be easily modulated by families and friends and yielded by palliative care teams by providing social inclusion and participation of patients in social activities. Especially for those patients living in nursing homes, where home residents are most of their time unoccupied and with little interaction (Hoel et al., 2022), social activities, the quality of life may be endangered. Thus, it is of utmost importance to monitor the wellbeing and coping of patients with ALS from early on and during the course of the disease.
This work presents no causality but correlations. Therefore, causal conclusions about the relationship between coping traits, coping behaviors and wellbeing of patients with ALS cannot be drawn. Patients who are depressed may as well be the ones with reduced social activities. Additionally, the affective state could be modulating the tendency for hope for success or fear of failure. Longitudinal studies are needed to strengthen the evidence for the proposed relationships. To better understand the relationship between the achievement motives and actual coping strategies used, future studies should incorporate an instrument to assess coping behavior in more detail, such as the Coping Inventory for Stressful Situations (Endler and Parker, 1994) or the MND Coping Scale (Lee et al., 2001). Furthermore, our study used self-reporting instruments, which could be prone to biases, such as social-desirable responding. Another limitation of our study might be that patients with high achievement motives may be willing to participate in studies despite severe physical restrictions. Patients with high social support may be overrepresented, as a family member may support study inclusion. As a result, most studies including patients with ALS in advanced stages may report a high wellbeing despite severe physical function loss due to successful coping strategies of the participants (and sufficient social resources). Additionally, 18% of patients presented with mild cognitive impairments according to age- and education-adjusted cut-off scores for ECAS, which may interfere with wellbeing. However, none of the patients presented with dementia, and according to previous research, it can be expected that mild impairments do not reduce patient's general decision capacity (Böhm et al., 2016). Finally, we hereby present cross-sectional data, which provide a snapshot in time with no indication of dynamics in the course of the disease. It is not entirely clear yet whether coping behavior differs during the disease course (Jakobsson Larsson et al., 2016), and different coping strategies appear to have different effects on wellbeing during the disease course (Matuz et al., 2015). Future research needs to investigate longitudinal changes in wellbeing during the disease course. Additionally, in our study, none of the demographic factors played a role regarding wellbeing; however, there may be possible associations between wellbeing and other aspects of personality (Abdullahi et al., 2020; Anglim et al., 2020), cultural background (Ciećwierska et al., 2023a,b), or spirituality (Bernard et al., 2017; Ciećwierska et al., 2023b), which should be included in further research.
We present evidence from a large registry, indicating that patients with high self-attributed motives experience fewer coping difficulties in adapting to the changed circumstances associated with ALS, likely due to their intrinsic achievement motive. Additionally, anxiousness was closely related to fear of failure in general, while hope for success was associated with higher wellbeing. Active social participation showed a strong correlation with reduced depressiveness. These findings suggest that not only wellbeing but also coping traits and coping behavior should be monitored in patients dealing with ALS. This understanding about the coping process could be used for individual psychological counseling and intervention. Professional counseling and psychosocial intervention may improve adaptive coping behavior and wellbeing of patients (Kurt et al., 2007). Appropriate palliative care management can be enhanced by including regular social activities as a non-medicinal therapy, thereby preserving wellbeing even in the end-of-life stages of ALS.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by the Ethical Committees of University of Ulm (No. 11/10), the medical association of the state of “Baden-Wuerttemberg” (Landesärztekammer, No. B-F-2010-062), and the medical association of the state of “Bayern” (No. 7/11300). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
JF: Conceptualization, Formal analysis, Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing. AR: Conceptualization, Data curation, Writing – review & editing, Methodology. RP: Conceptualization, Methodology, Writing – review & editing. HB: Conceptualization, Data curation, Writing – review & editing. AB: Conceptualization, Data curation, Writing – review & editing. SD: Conceptualization, Data curation, Writing – review & editing. MS: Conceptualization, Data curation, Writing – review & editing. MH: Conceptualization, Data curation, Writing – review & editing. AK: Conceptualization, Data curation, Writing – review & editing. CO: Conceptualization, Data curation, Writing – review & editing. AN: Conceptualization, Data curation, Writing – review & editing. NS: Conceptualization, Data curation, Writing – review & editing. AL: Conceptualization, Data curation, Writing – review & editing. DR: Conceptualization, Methodology, Writing – review & editing. ACL: Conceptualization, Funding acquisition, Methodology, Project administration, Supervision, Writing – review & editing. GN: Project administration, Supervision, Writing – review & editing, Conceptualization, Methodology. DL: Conceptualization, Data curation, Formal analysis, Funding acquisition, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing.
Following cooperating partners provided data for the ALS Registry Swabia:
Andres F., Department of Neurology, Kreiskliniken Reutlingen; Arnold G., Department of Neurology, Klinikum Sindelfingen-Boeblingen; Asshauer I., Department of Psychiatry and Psychotherapy, Klinikum Friedrichshafen; Baier H., Department of Epileptology, ZFP Suedwuerttemberg; Beattie J., Department of Neurology, Ostalb-Klinikum Aalen; Becker T., Department of Psychiatry and Psychotherapy, BKH Guenzburg; Behne F., Department of Epileptology, ZFP Suedwuerttemberg; Bengel D., Department of Neurology, Oberschwabenklinik Ravensburg; Bracknies, V., Department of Neurology, Dietenbronn; Broer R., Department of Psychiatry and Psychotherapy, Weinsberg, Klinikum am Weissenhof; Burkhard, A., Department of Neurology, Klinikum Günzburg; Connemann B., Department of Psychiatry and Psychotherapy III, University of Ulm; Dettmers C., Schmieder Kliniken Konstanz; Dieterich M., Department of Neurology, LMU München; Etzersdorfer E., Department of Psychiatry and Psychotherapy, Furtbachkrankenhaus Stuttgart; Freund, W., Praxis Biberach; Gersner T., Department of Psychiatry and Psychotherapy, ZfP Zwiefalten; Gold H.-J., Department of Neurology, Klinikum am Gesundbrunnen Heilbronn; Hacke, W., Department of Neurology, University of Heidelberg; Haman G., Department of Neurology, Klinikum Günzburg; Heimbach B., Department of Neurology, University of Freiburg; Hemmer B., Department of Neurology, TU Muenchen; Hendrich C., Department of Neurology, Klinikum Friedrichshafen; Herting B., Department of Neurology, Diakonie-Klinikum Schwaebisch Hall; Huber R., Department of Neurology, Klinikum Friedrichshafen; Huber-Hartmann K., Department of Neurology, Kliniken Landkreis Heidenheim; Huelser P.-J., Department of Neurology, Fachklinik Wangen; Juettler E., Department of Neurology, Ostalb-Klinikum Aalen; Kammerer-Ciernioch J., Department of Psychiatry and Psychotherapy, Weinsberg, Klinikum am Weissenhof; Kaspar A., Department of Neurology, Oberschwabenklinik Ravensburg; Kern R., Department of Neurology, Klinikum Kempten; Kimmig H., Department of Neurology, Kliniken Schwenningen; Klebe, S., Department of Neurology, University of Würzburg; Kloetzsch C., Bodensee Klinikum, Schmieder Kliniken Allensbach; Klopstock, T., Department of Neurology, LMU München; Kuethmann A., Department of Psychiatry and Psychotherapy, Bezirkskrankenhaus Memmingen; Lewis D., Department of Neurology, Marienhospital Stuttgart; Lichy C., Department of Neurology, Klinikum Memmingen; Maeurer M., Department of Neurology, Caritas Krankenhaus Bad Mergentheim; Maier-Janson W., Praxis Ravensburg; Mertrikat J., Department of Neurology, Bundeswehrkrankenhaus Ulm; Meudt O., Department of Neurology, Klinikum Memmingen; Meyer A., Department of Neurology, Weissenau; Mueller vom Hagen J., Department of Neurology, Universitaetsklinikum Tuebingen; Naumann M., Department of Neurology and Neurophysiology, Klinikum Augsburg; Neher K.-D., Department of Neurology, Vinzenz von Paul Hospital, Rottweil; Neuhaus O., Department of Neurology, Kliniken Landkreis Sigmaringen; Neusch C., Praxis EMSA Singen; Niehaus L., Department of Neurology, Winnenden; Raape J., ZFP Suedwuerttemberg, Neurologie Weissenau; Ratzka P., Department of Neurology and Neurophysiology, Klinikum Augsburg; Rettenmayr C., Department of Neurology, Klinikum Esslingen; Riepe M. W., Department of Gerontopsychiatry, BKH Guenzburg; Rothmeier J., ZFP Suedwuerttemberg, Neurologie Weissenau; Sabolek M., Department of Neurology, Biberach; Schell C., Department of Neurology, Kreiskliniken Reutlingen; Schlipf T., Department of Psychiatry and Psychotherapy, Klinikum Schloss Winnenden; Schmauss M., Department of Psychiatry and Psychotherapy, Bezirkskrankenhaus Augsburg; Schoels L., Department of Neurology, Universitaetsklinikum Tuebingen; Schuetz K., Department of Neurology, Kliniken Schwenningen; Schweigert B., Department of Neurology, Caritas Krankenhaus, Bad Mergentheim; Sperber W., Department of Neurology, Kliniken Esslingen; Steber C., Department of Psychiatry and Psychotherapy, Bezirkskrankenhaus Augsburg; Steber R., Department of Psychiatry and Psychotherapy, Bezirkskrankenhaus Memmingen; Stroick M., Department of Neurology, Klinikum Memmingen; Trottenberg T., Department of Neurology, Winnenden; Tumani H., Department of Neurology, Dietenbronn; Wahl C., Department of Neurology, Klinikum Kempten; Weber F., Department of Neurology, Bundeswehrkrankenhaus Ulm; Weiler M., Department of Neuology, University of Heidelberg; Weiller C., Department of Neurology, University of Freiburg; Wessig C., Department of Neurology, University of Wuerzburg; Winkler A., Department of Neurology, TU Muenchen.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by the German Research Council (Deutsche Forschungsgemeinschaft, DFG Grant Number LU 336/15-1). This work was additionally funded by the Bundesministerium für Bildung und Forschung (FTLDc O1GI1007A, MND-Net 01GM1103A; “NEEDSinALS” 01ED1405; PaCeMed 01DS18031), the Kompetenznetzwerk Präventivmedizin Baden-Württemberg (K.N.K.B.008.04), and the Deutsches Zentrum für Neurodegenerative Erkrankungen (DZNE). The funding sources played no role in the preparation of this manuscript.
We thank all the patients and caregivers that participated in the study. We thank the study nurses I. Kraft-Oberbeck, N. Lämmle, and I. Dobias for their excellent field work and the medical documentation team T. Brehme, S. Enderle, G. Feike, and B. Och for their excellent technical support.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abdullahi, A. M., Orji, R., Rabiu, A. M., and Kawu, A. A. (2020). Personality and subjective well-being: towards personalized persuasive interventions for health and well-being. Online J. Public Health Inform. 12:e1. doi: 10.5210/ojphi.v12i1.10335
Abrahams, S., Newton, J., Niven, E., Foley, J., and Bak, T. H. (2014). Screening for cognition and behaviour changes in ALS. Amyotroph. Lateral Scler. Frontotemporal Degener. 15, 9–14. doi: 10.3109/21678421.2013.805784
Anglim, J., Horwood, S., Smillie, L., Marrero, R. J., and Wood, J. (2020). Predicting psychological and subjective well-being from personality: a meta-analysis. Psychol. Bull. 146, 279–323. doi: 10.31234/osf.io/gupxj
Atkinson, J. W. (1957). Motivational determinants of risk-taking behavior. Psychol. Rev. 64, 359–372. doi: 10.1037/h0043445
Bernard, M., Strasser, F., Gamondi, C., Braunschweig, G., Forster, M., Kaspers-Elekes, K., et al. (2017). Relationship between spirituality, meaning in life, psychological distress, wish for hastened death, and their influence on quality of life in palliative care patients. J. Pain Symptom Manage. 54, 514–522. doi: 10.1016/j.jpainsymman.2017.07.019
Bernheim, J. L. (1999). How to get serious answers to the serious question: ‘How have you been?': subjective Quality of Life (QOL) as an individual experiential emergent construct. Bioethics 13, 272–287. doi: 10.1111/1467-8519.00156
Bernheim, J. L., and Buyse, M. (1983). The anamnestic comparative self-assessment for measuring the subjective quality of life of cancer patients. J. Psychosoc. Oncol. 1, 25–38. doi: 10.1300/J077v01n04_03
Bernheim, J. L., Theuns, P., Mazaheri, M., Hofmans, J., Fliege, H., Rose, M., et al. (2006). The potential of anamnestic comparative self-assessment (ACSA) to reduce bias in the measurement of subjective well-being. J. Happiness Stud. 7, 227–250. doi: 10.1007/s10902-005-4755-0
Bjelland, I., Dahl, A. A., Haug, T. T., and Neckelmann, D. (2002). The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J. Psychosom. Res. 52, 69–77. doi: 10.1016/S0022-3999(01)00296-3
Blanca, M. J., Alarcón, R., Arnau, J., Bono, R., and Bendayan, R. (2017). Non-normal data: is ANOVA still a valid option? Psicothema 29, 552–557. doi: 10.7334/psicothema2016.383
Böhm, S., Aho-Özhan, H. E. A., Keller, J., Dorst, J., Uttner, I., Ludolph, A. C., et al. (2016). Medical decisions are independent of cognitive impairment in amyotrophic lateral sclerosis. Neurology 87, 1737–1738. doi: 10.1212/WNL.0000000000003232
Brooks, B. R., Miller, R. G., Swash, M., Munsat, T. L., and World Federation of Neurology Research Group on Motor Neuron Diseases. (2000). El Escorial revisited: revised criteria for the diagnosis of amyotrophic lateral sclerosis. Amyotroph. Lateral Scler. Other Motor Neuron Disord. 1, 293–299. doi: 10.1080/146608200300079536
Cedarbaum, J. M., Stambler, N., Malta, E., Fuller, C., Hilt, D., Thurmond, B., et al. (1999). The ALSFRS-R: a revised ALS functional rating scale that incorporates assessments of respiratory function. J. Neurol. Sci. 169, 13–21. doi: 10.1016/S0022-510X(99)00210-5
Chiò, A., Logroscino, G., Hardiman, O., Swingler, R., Mitchell, D., Beghi, E., et al. (2009). Prognostic factors in ALS: a critical review. Amyotroph. Lateral Scler. 10, 310–323. doi: 10.3109/17482960802566824
Ciećwierska, K., Lulé, D., Bielecki, M., Helczyk, O., Maksymowicz-Sliwińska, A., Finsel, J., et al. (2023a). Quality of life and depression in patients with amyotrophic lateral sclerosis - does the country of origin matter? BMC Palliat. Care 22:72. doi: 10.1186/s12904-023-01189-2
Ciećwierska, K., Lulé, D., Helczyk, O., Nieporecki, K., Bielecki, M., Baader, S., et al. (2023b). Religiosity in patients with amyotrophic lateral sclerosis, a cross-country comparison. Qual. Life Res. 32, 2235–2246. doi: 10.1007/s11136-023-03383-4
Connor-Smith, J. K., and Flachsbart, C. (2007). Relations between personality and coping: a meta-analysis. J. Pers. Soc. Psychol. 93, 1080–1107. doi: 10.1037/0022-3514.93.6.1080
Endler, N. S., and Parker, J. D. A. (1994). Assessment of multidimensional coping: task, emotion, and avoidance strategies. Psychol. Assess. 6, 50–60. doi: 10.1037/1040-3590.6.1.50
Gjesme, T., and Nygard, R. (1970). Achievement-Related Motives: Theoretical Considerations and Construction of a Measuring Instrument. Oslo: University of Oslo.
Hecht, M., Hillemacher, T., Gräsel, E., Tigges, S., Winterholler, M., Heuss, D., et al. (2002). Subjective experience and coping in ALS. Amyotroph. Lateral Scler. Other Motor Neuron Disord. 3, 225–231. doi: 10.1080/146608202760839009
Heckhausen, H. (1963). Hoffnung und Furcht in der Leistungsmotivation. Meisenheim am Glan: Hain, 406.
Heckhausen, H. (1991). Motivation and Action (Transl. by P. K. Leppmann). New York, NY: Springer-Verlag Publishing, 504. doi: 10.1007/978-3-642-75961-1
Herrmann-Lingen, C., Buss, U., and Snaith, R. P. (2011). HADS-D Manual : Deutsche Adaptation der Hospital Anxiety and Depression Scale (HADS) von R.P. Snaith und A.S. Zigmond. New York, NY: Huber.
Herschbach, P. (2002). The ‘Well-being paradox' in quality-of-life research. Psychother. Psychosom. Med. Psychol. 52, 141–150. doi: 10.1055/s-2002-24953
Hoel, V., Seibert, K., Domhoff, D., Preuß, B., Heinze, F., Rothgang, H., et al. (2022). Social health among german nursing home residents with dementia during the COVID-19 pandemic, and the role of technology to promote social participation. Int. J. Environ. Res. Public Health. 19:1956. doi: 10.3390/ijerph19041956
Jakobsson Larsson, B., Nordin, K., and Nygren, I. (2016). Coping with amyotrophic lateral sclerosis; from diagnosis and during disease progression. J. Neurol. Sci. 361, 235–242. doi: 10.1016/j.jns.2015.12.042
King, S. J., Duke, M. M., and O'Connor, B. A. (2009). Living with amyotrophic lateral sclerosis/motor neurone disease (ALS/MND): decision-making about ‘ongoing change and adaptation'. J. Clin. Nurs. 18, 745–754. doi: 10.1111/j.1365-2702.2008.02671.x
Kollewe, K., Mauss, U., Krampfl, K., Petri, S., Dengler, R., Mohammadi, B., et al. (2008). ALSFRS-R score and its ratio: a useful predictor for ALS-progression. J. Neurol. Sci. 275, 69–73. doi: 10.1016/j.jns.2008.07.016
Kurt, A., Nijboer, F., Matuz, T., and Kübler, A. (2007). Depression and anxiety in individuals with amyotrophic lateral sclerosis: epidemiology and management. CNS Drugs. 21, 279–291. doi: 10.2165/00023210-200721040-00003
Kuzma-Kozakiewicz, M., Andersen, P. M., Ciecwierska, K., Vázquez, C., Helczyk, O., Loose, M., et al. (2019). An observational study on quality of life and preferences to sustain life in locked-in state. Neurology 93, e938–e945. doi: 10.1212/WNL.0000000000008064
Lang, J. W. B., and Fries, S. A. (2006). Revised 10-item version of the achievement motives scale. Eur. J. Psychol. Assess. 22, 216–224. doi: 10.1027/1015-5759.22.3.216
Lazarus, R., and Folkman, S. (1984). Stress, Appraisal, and Coping. Berlin: Springer Publishing Company, 460.
Leandro, G. S., Dourado Júnior, M. E. T., Santana, G. C., and Dantas, L. S. X. (2022). Coping strategies among amyotrophic lateral sclerosis (ALS) patients: an integrative review. J. Neurol. 269, 693–702. doi: 10.1007/s00415-021-10472-2
Lee, J. N., Rigby, S. A., Burchardt, F., Thornton, E. W., Dougan, C., Young, C. A., et al. (2001). Quality of life issues in motor neurone disease: the development and validation of a coping strategies questionnaire, the MND Coping Scale. J. Neurol. Sci. 191, 79–85. doi: 10.1016/S0022-510X(01)00619-0
Loose, M., Burkhardt, C., Aho-Özhan, H., Keller, J., Abdulla, S., Böhm, S., et al. (2016). Age and education-matched cut-off scores for the revised German/Swiss-German version of ECAS. Amyotroph. Lateral Scler. Frontotemporal Degener. 17, 374–376. doi: 10.3109/21678421.2016.1162814
Ludolph, A., Drory, V., Hardiman, O., Nakano, I., Ravits, J., Robberecht, W., et al. (2015). A revision of the El Escorial criteria - 2015. Amyotroph. Lateral Scler. Frontotemporal Degener. 16, 291–292. doi: 10.3109/21678421.2015.1049183
Lulé, D., Burkhardt, C., Abdulla, S., Böhm, S., Kollewe, K., Uttner, I., et al. (2015). The Edinburgh Cognitive and behavioural amyotrophic lateral sclerosis screen: a cross-sectional comparison of established screening tools in a German-Swiss population. Amyotroph. Lateral Scler. Frontotemporal Degener. 16, 16–23. doi: 10.3109/21678421.2014.959451
Lulé, D., Ehlich, B., Lang, D., Sorg, S., Heimrath, J., Kübler, A., et al. (2013). Quality of life in fatal disease: the flawed judgement of the social environment. J. Neurol. 260, 2836–2843. doi: 10.1007/s00415-013-7068-y
Lulé, D., Ludolph, A. C., and Kübler, A. (2018). “Psychological morbidity in amyotrophic lateral sclerosis - depression, anxiety, hopelessness,” in Amyotrophic Lateral Sclerosis: Understanding and Optimizing Quality of Life and Psychological Well-Being, eds F. Pagnini, and Z. Simmons (Oxford: Oxford University Press), 33. doi: 10.1093/med/9780198757726.003.0003
Lumley, T., Diehr, P., Emerson, S., and Chen, L. (2002). The importance of the normality assumption in large public health data sets. Annu. Rev. Public Health 23, 151–169. doi: 10.1146/annurev.publhealth.23.100901.140546
Matuz, T., Birbaumer, N., Hautzinger, M., and Kubler, A. (2010). Coping with amyotrophic lateral sclerosis: an integrative view. J. Neurol. Neurosurg. Psychiatry 81, 893–898. doi: 10.1136/jnnp.2009.201285
Matuz, T., Birbaumer, N., Hautzinger, M., and Kübler, A. (2015). Psychosocial adjustment to ALS: a longitudinal study. Front. Psychol. 6:1197. doi: 10.3389/fpsyg.2015.01197
McLeod, J. E., and Clarke, D. M. (2007). A review of psychosocial aspects of motor neurone disease. J. Neurol. Sci. 258, 4–10. doi: 10.1016/j.jns.2007.03.001
Montel, S., Albertini, L., Desnuelle, C., and Spitz, E. (2012). The impact of active coping strategies on survival in ALS: the first pilot study. Amyotroph. Lateral Scler. 13, 599–601. doi: 10.3109/17482968.2012.711835
Müller-Jentsch, W. (2008). Der Verein – ein blinder Fleck der Organisationssoziologie. Berl. J. Soziol. 18, 476–502. doi: 10.1007/s11609-008-0020-9
Nagel, G., Ünal, H., Rosenbohm, A., Ludolph, A. C., Rothenbacher, D, and The ALS Registry Study Group (2013). Implementation of a population-based epidemiological rare disease registry: study protocol of the amyotrophic lateral sclerosis (ALS) - registry Swabia. BMC Neurol. 13:22. doi: 10.1186/1471-2377-13-22
Nelson, N. D., Trail, M., Van, J. N., Appel, S. H., and Lai, E. C. (2003). Quality of life in patients with amyotrophic lateral sclerosis: perceptions, coping resources, and illness characteristics. J. Palliat. Med. 6, 417–424. doi: 10.1089/109662103322144736
Oliver, D. J., Borasio, G. D., Caraceni, A., de Visser, M., Grisold, W., Lorenzl, S., et al. (2016). A consensus review on the development of palliative care for patients with chronic and progressive neurological disease. Eur. J. Neurol. 23, 30–38. doi: 10.1111/ene.12889
Parkin Kullmann, J. A., Hayes, S., and Pamphlett, R. (2018). Are people with amyotrophic lateral sclerosis (ALS) particularly nice? An international online case–control study of the Big Five personality factors. Brain Behav. 8:e01119. doi: 10.1002/brb3.1119
Rabari, F., Rezaei, F., Mirzai, F., and Sedighi, F. (2023). Investigating the role of coping strategies, personality traits and mindfulness with self-care in leukemia patients. J. Assess. Res. Appl. Couns. 5, 51–59. doi: 10.61838/kman.jarac.5.4.7
Rabkin, J. G., Wagner, G. J., and Del Bene, M. (2000). Resilience and distress among amyotrophic lateral sclerosis patients and caregivers. Psychosom. Med. 62, 271–279. doi: 10.1097/00006842-200003000-00020
Rosenbohm, A., Peter, R. S., Erhardt, S., Lulé, D., Rothenbacher, D., Ludolph, A. C., et al. (2017). Epidemiology of amyotrophic lateral sclerosis in Southern Germany. J. Neurol. 264, 749–757. doi: 10.1007/s00415-017-8413-3
Roth, S., and Cohen, L. J. (1986). Approach, avoidance, and coping with stress. Am. Psychol. 41, 813–819. doi: 10.1037/0003-066X.41.7.813
Siciliano, M., Trojano, L., Trojsi, F., Monsurrò, M. R., Tedeschi, G., Santangelo, G., et al. (2019). Assessing anxiety and its correlates in amyotrophic lateral sclerosis: the state-trait anxiety inventory. Muscle Nerve 60, 47–55. doi: 10.1002/mus.26475
Strong, M. J., Abrahams, S., Goldstein, L. H., Woolley, S., Mclaughlin, P., Snowden, J., et al. (2017). Amyotrophic lateral sclerosis - frontotemporal spectrum disorder (ALS-FTSD): revised diagnostic criteria. Amyotroph. Lateral Scler. Frontotemporal Degener. 18, 153–174. doi: 10.1080/21678421.2016.1267768
The EFNS Task Force on Diagnosis Management of Amyotrophic Lateral Sclerosis, Andersen, P. M., Abrahams, S., Borasio, G. D., de Carvalho, M., and Chio, A.. (2012). EFNS guidelines on the Clinical Management of Amyotrophic Lateral Sclerosis (MALS) – revised report of an EFNS task force. Eur. J. Neurol. 19, 360–375. doi: 10.1111/j.1468-1331.2011.03501.x
Tramonti, F., Bongioanni, P., Fanciullacci, C., and Rossi, B. (2012). Balancing between autonomy and support: coping strategies by patients with amyotrophic lateral sclerosis. J. Neurol. Sci. 320, 106–109. doi: 10.1016/j.jns.2012.07.006
Vázquez Medrano, C. R., Aho-Özhan, H. E. A., Weiland, U., Uttner, I., Ludolph, A. C., Lulé, D., et al. (2020). Disease progression but not physical state per se determines mental wellbeing in ALS. J. Neurol. 267, 3593–3601. doi: 10.1007/s00415-020-10027-x
Keywords: amyotrophic lateral sclerosis, coping, psychosocial adaptation, quality of life, depressiveness, wellbeing
Citation: Finsel J, Rosenbohm A, Peter RS, Bäzner H, Börtlein A, Dempewolf S, Schabet M, Hecht M, Kohler A, Opherk C, Nägele A, Sommer N, Lindner A, Rothenbacher D, Ludolph AC, Nagel G and Lulé DE (2024) Coping as a resource to allow for psychosocial adjustment in fatal disease: results from patients with amyotrophic lateral sclerosis. Front. Psychol. 15:1361767. doi: 10.3389/fpsyg.2024.1361767
Received: 28 December 2023; Accepted: 11 March 2024;
Published: 04 April 2024.
Edited by:
Morteza Taheri, University of Tehran, IranReviewed by:
Khadijeh Irandoust, Imam Khomeini International University, IranCopyright © 2024 Finsel, Rosenbohm, Peter, Bäzner, Börtlein, Dempewolf, Schabet, Hecht, Kohler, Opherk, Nägele, Sommer, Lindner, Rothenbacher, Ludolph, Nagel and Lulé. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dorothée E. Lulé, ZG9yb3RoZWUubHVsZUB1bmktdWxtLmRl
†These authors share senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.