 Shai Shorer
Shai Shorer Michael Weinberg
Michael Weinberg Lihi Cohen3
Lihi Cohen3 Miri Cohen
Miri Cohen- 1School of Social Work, Faculty of Social Welfare and Health Sciences, University of Haifa, Haifa, Israel
- 2B’Shvil, Yahud, Israel
- 3Psychology Department, University of Haifa, Haifa, Israel
Combat soldiers are exposed to various potentially traumatic events and face high risk of developing military-related psychopathology, such as depression, posttraumatic stress and grief (PTSS). However, a strong body of research shows that resilience is the default in the aftermath of trauma and indeed, many veterans do not develop high symptomatic levels. To explicate this inconsistency, the current study examined the associations among PTSS, resilience, and patterns of emotional-approach coping. A sample of 595 male combat veterans filled out questionnaires on trauma exposure, PTSS, depressive symptoms, resilience, and emotional-approach coping. Their data were analyzed using structural equation modeling path analysis. Participants reported high exposure to potentially traumatic events during service. Mean scores were high for resilience and relatively low for PTSS and depressive symptoms; 13% had a clinical level of posttraumatic stress disorder. Structural equation modeling revealed that emotional-approach coping strategies mediated the relationship between resilience and PTSS. However, emotional expression was associated with lower PTSS levels, whereas emotional processing was associated with higher PTSS levels. These results suggest that although emotional-approach coping was related to higher resilience, emotional expression (an intrapersonal coping strategy) might have a more positive effect than self-oriented emotional coping strategies. Providing veterans with supportive opportunities and a wider repertoire of emotional coping skills might enhance their well-being, reduce postservice emotional distress while not harming veterans’ resilience levels.
1 Introduction
Exposure to potentially traumatic events (PTEs) and their aftermath is often an inevitable part of combat service for many soldiers and veterans around the world (Korte et al., 2020). Soldiers exposed to combat are at high risk of developing posttraumatic stress symptoms (PTSS) and presenting various levels of posttraumatic stress disorder (PTSD). Prevalence rates of PTSD in veterans have been reported as varying from relatively low (1.09%) to very high (34.84%), depending on demographic, social, life experience, and exposure-related factors (Xue et al., 2015) and the veterans’ homecoming conditions (Boscarino et al., 2018). Given this wide range, Fulton et al. (2015) performed a meta-analysis and found that 23% of American soldiers who participated in recent military campaigns experienced substantial PTSD levels. Although these estimations vary based on the choice of estimation tools and cohort (Hoge et al., 2014), they still reflect a major condition that affects a large part of the veteran population. Moreover, prior research reported that exposure to military trauma was associated with other emotional disorders, such as depression (Yancey et al., 2023), which affects an estimated 9–16% of American veterans (Karstoft et al., 2020; Inoue et al., 2023). Similar rates were reported among veterans of other countries, such as Australia (Carra et al., 2022), Canada (Thompson et al., 2019), and Israel (Shorer et al., 2023).
It is well established that the substantial presence of PTSS among military veterans has multiple causes related to precursor factors, the nature of the traumatic exposure, and its aftermath (Korte et al., 2020). Military-related PTEs are often characterized by unique and high-level exposure, such as facing ongoing danger or witnessing injuries and death of friends. Exposure to PTEs during military service is also unique due to postservice factors, such as confusion of self-identity between being a soldier and a citizen; dominance of masculine characteristics that demand repressing of emotions, most notably weakness and vulnerability (Mobbs and Bonanno, 2018); and experiences of loneliness, isolation, separation from loved ones, and living for long periods in uncertain and unpredictable conditions (Solomon, 2020). However, the inconsistency of this high risk of developing PTSS and the fact that most veterans do not develop military-related psychopathology (Porter et al., 2017) demand further study (Bonanno, 2021).
Aiming to fill this gap, the current research examined the relationships among the personal resource of resilience (Connor and Davidson, 2003), considered a pretraumatic factor; emotional-approach patterns (Stanton et al., 2000a), a peri- and posttraumatic factor; and PTSS and depression, being the consequences of the complex dynamics of these factors.
Resilience is considered to be a personal resource related to better psychological reactions to stressful life events (Bonanno, 2021). Although definitions of resilience as a psychological construct vary (Denckla et al., 2020), scholars generally agree that resilience is not a stable characteristic. Rather, it reflects the dynamics of different peritraumatic factors that comprise and shape the process of coping with the aftermath of traumatic exposure (Bonanno, 2021). It consists of a combination of psychological, physiological, and behavioral characteristics that enable individuals to resist, cope with, and recover in the face of adverse life experiences (Masten and Powell, 2003). Based on the accumulated body of research in this field, researchers have suggested that resilience can be taught and practiced. It is the product of an ongoing process of individual’s evaluation of the situation they face, choosing resilience-enhancing coping strategies among those available, implementing them, and constantly evaluating their effect to make necessary adjustments to improve their coping (Bonnano et al., 2023). This approach considers resilience as a state of mind that can and should be constantly used. It can be evaluated at a specific point in time (Connor and Davidson, 2003), and research has shown high levels of resilience among veterans associated with relatively low levels of PTSD (compared to the general population), despite experiencing multiple PTEs during military service (Galatzer-Levy et al., 2018). Studies have repeatedly examined this relationship, highlighting the notion that PTSS, resilience, and growth often coexist (Zerach et al., 2013). For example, research with a nationally representative sample of U.S. veterans found that most participants presented moderate to high levels of resilience, along with relatively low levels of PTSD (Fogle et al., 2020). This comprehensive study described various important relations among veterans’ active coping methods, distress, and well-being. The study concluded that veterans who were more involved in therapy and social interactions, accepted their emotional and behavioral challenges, and engaged in efforts to solve them presented lower distress over time. Resilience, as a personal resource, was shown to be related to use of more efficient coping strategies in the face of stressors (Bonnano et al., 2023). Moreover, difficulty with emotional clarity (e.g., understanding one’s emotions) and lack of emotional regulation strategies were found to be prominent in the development of PTSD and depression symptoms, two common emotional reactions following traumatic injury (Korte et al., 2020). Notably, lack of emotional clarity was associated with PTSD symptoms of hyperarousal and negative alterations in mood and cognition, overall PTSD symptom severity, and depression levels (Timmer-Murillo et al., 2023). PTSS and depression often co-occur and have been found to evolve in tandem (Armenta et al., 2019). The current study further explored these trajectories.
Theoretical models of coping with stressful situations define coping as the behavioral and cognitive means that individuals use to deal with stressors (Lazarus and Folkman, 1984), and it has been classified into different modes (e.g., problem-focused and emotion-focused coping). In recent years, leading stress and coping researchers have proposed the emotional-approach coping classification (Stanton and Low, 2012). The concept of emotional-approach coping was developed in response to Lazarus and Folkman’s conceptualization of emotion-focused coping (Biggs et al., 2017). A major critique of their model is that it aggregates diverse strategies and does not distinguish between ineffective strategies of disengagement and avoidance, which usually increase emotional distress, and other efficient emotion-focused strategies, such as emotional processing and expression (Stanton et al., 2000a; Carver and Connor-Smith, 2010).
Emotional-approach coping involves processing and expressing emotions in response to stressful life experiences or exposure to adversities (Stanton et al., 2000a). This process is commonly divided into two strategies: emotional processing, which consists of attempts to acknowledge, explore, and understand emotions; and emotional expression, which involves verbal or nonverbal efforts to express or share emotional experiences. Previous studies reported that emotional-approach coping, combining emotional expression and processing, was associated with lower psychopathological symptoms and better adjustment to stressful situations (Stanton and Low, 2012; Juth et al., 2015; Hoyt et al., 2020). Nevertheless, studies also showed distinctive associations of emotional expression and processing with psychological factors. For example, emotional expression was associated with lower distress indexes, whereas diverse results were reported regarding the effect of emotional processing. Scholars suggested that whereas emotional expression helps relieve emotional load and is often related to other people, emotional processing may involve personal ruminations on negative cognitions and emotions (Stanton et al., 2000a; Marroquin et al., 2016). However, the effect of emotional expression and processing may depend on time, gender, and situation (Stanton and Low, 2012; Juth et al., 2015; Hoyt et al., 2020).
Only a few studies have examined the effect of emotional-approach coping on PTSS and emotional distress among trauma-exposed individuals (Hassija et al., 2012; Fishbein et al., 2022). The current study aimed to fill this theoretical gap. In a study with cancer survivors, emotional-approach coping was associated with lower cancer-related trauma symptoms and mediated the effect of acceptance and commitment therapy on decreased symptoms (Fishbein et al., 2022). Another study, involving 209 trauma-exposed U.S. veterans, found that emotional expression was associated with lower PTSD and depression symptoms, whereas emotional processing was not (Hassija et al., 2012).
A study examining the complex relations between resilience and emotional-approach coping found that individuals who shared more of their experiences tended to express higher emotional resilience and have lower rates of PTSD symptoms and emotional distress (Yeung and Chow, 2019). Moreover, resilience was found to moderate the relations among combat exposure, intrusive ruminations, and PTSD levels at various levels of trauma exposure (Blackburn and Owens, 2016). Yet veterans may refrain from sharing their distress or seeking help for emotional issues. In other words, they tend to make partial use of their potential resilience resources (Lahad, 2017; Mobbs and Bonanno, 2018). This trend might be the consequence of shame regarding their combat experience and how they cope with its aftermath, because the military’s masculine and stoic social norms discourage the expression of emotions perceived as weakness (Gaudet et al., 2015).
Israeli citizens are obliged to complete army service of 2–3 years at age 18 (Knesset, 1986), and male Israeli veterans usually continue to serve in the reserve forces until age 40 (Knesset, 2008). Due to this state’s ongoing struggle for security and its small size, Israeli veterans are at risk of multiple PTEs and retraumatization (Solomon, 2020). A recent report indicated about 5,700 of Israel’s emotionally injured veterans were recognized by the Ministry of Defense’s Rehabilitation Wing as dealing with PTSD (Yechimovitch-Cohen, 2022). However, this rate is expected to grow due to the state’s recent violent conflicts (Ministry of Health, 2023). Because about 100,000 soldiers are recruited and discharged each year, this figure probably underestimates the number of Israeli veterans experiencing substantial levels of PTSS.
The current study examined the relationships among resilience, emotional-approach coping strategies, and PTSS and depressive symptoms among Israeli veterans. Specifically, we examined the associations between resilience and levels of PTSS and depression, along with the mediating role of emotional-approach coping strategies (emotional expression and processing) in the association of these factors. The cohort of this study was a unique nonclinical group of people with prior PTEs who were still at risk of exposure to additional PTEs (because most of them served as reservists); they were in touch with both their natural support systems and a military-related, assumedly supportive environment (peer combatants).
2 Materials and methods
The study was approved by the affiliated faculty’s board of ethics (No. 266/21).
2.1 Participants and procedure
The current paper presents the results of the first wave of a longitudinal study on the impact of military service on Israeli combat veterans who participated in a nature-assisted group intervention for processing military-related PTEs called B’Shvil. B’Shvil is a nonprofit organization that aims to help Israeli veterans who served in military units of all forces to process their combat experience, address difficulties in the bidirectional transition between army and civilian life, and facilitate postservice psychological growth (Shorer et al., 2023). Teams of veterans (e.g., squads, companies, platoons) voluntarily participate in this intervention, usually around 5–10 years after their release from mandatory service (and the continuation of reserve service). The group intervention is usually operated as a 10-day retreat in nature settings (to learn more about this intervention, please refer to https://www.bshvil.org/english). Overall, including personal and group meetings before and after the retreat, participants are followed by B’Shvil facilitators for 6 months. A few main therapeutic components are highlighted in this recreational intervention: mind–body relations in the face of trauma; personal and group psychological resilience; and nature’s healing power.
The full research project will examine participants’ condition at three points: before the intervention, after the invention, and at follow-up. Participants completed informed consent forms and self-reported questionnaires at the beginning of the group intervention.
The study sample consisted of 595 male veterans who served in various combat units and military forces (e.g., infantry, armory, navy, air force). Overall, 1,033 veterans participated in the intervention between February 2021 and October 2022 (when data were collected). In this sample, 640 (62%) participants filled out the study questionnaire; 17 participants were excluded because they did not complete the questionnaire. Although women comprise about 40% of Israeli military personnel and 19% of them serve as combatants (Shafran Gittleman, 2020), only a dozen women participated in these groups and only six of them completed the questionnaire. Hence, their data were excluded from the current study. An a priori sample size calculation for SEM: Statistical Equation Modeling (Soper, 2024) indicated that a sample of 400 participants is needed to detect an effect size of 0.10 with desired power of 0.80, seven observed variables (including controlling for confounding variables), and one latent variable.
Table 1 shows the demographic characteristics of the participants. Their mean age was 32.9 (SD = 6.4); 36% were single and the rest were either married or in a relationship; and 97% were engaged in either a full-time job or academic studies. Most participants (93%) reported exposure to PTEs, and 11% were injured during their army service.
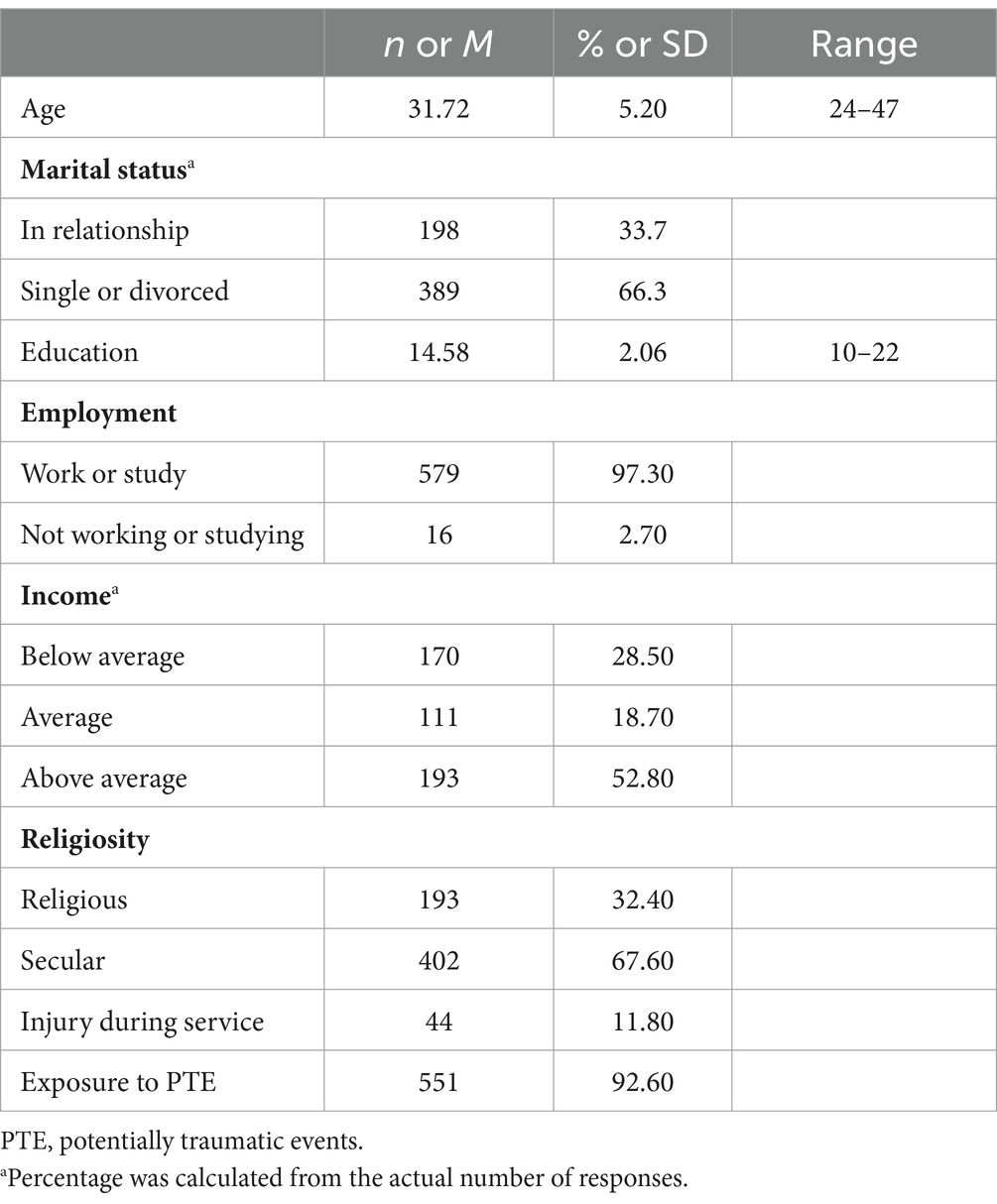
Table 1. Participants’ demographic data.
2.2 Measures
Demographic data and army service details were collected, including what roles participants held during their army service (active combat, supporting active combat, etc.).
Trauma exposure was examined using Life Events Checklist for DSM-5 (Weathers et al., 2013), which was shortened to fit this study population. Six items were eliminated to avoid redundancy. These items related to occupational and recreational injuries, risk of toxification, nonspecific sexual abuse, captivity, exposure to general human suffering, and exposure to sudden death. The final list of events included exposure to combat, other military-related threats to their life or military-related physical injury, civil violence that included trauma, terror attack, car accident, life-threatening natural disaster, life-threatening illness, and other types of traumatic events.
PTSS was evaluated using the Hebrew version of the PTSD Checklist for DSM-5 (PCL-5; Weathers et al., 2013; translated by the Israeli Ministry of Defense). This 20-item questionnaire features a 5-point Likert scale ranging from 0 (not at all) to 4 (extremely) regarding experiences of PTSD symptoms during the last month. For example: “In the past month, how much were you bothered by: Repeated, disturbing, and unwanted memories of the stressful experience?” Participants’ scores were calculated as a combination of their total score (range: 0–80) and whether they currently experienced symptoms in four PTSD clusters. This questionnaire was found to have high internal reliability (Blevins et al., 2015). Initial research suggested a cutoff score of 31–33 as indicative of probable PTSD across samples (National Center for PTSD, n.d.). Correlations between the subscales ranged from 0.71 to 0.93. In the current study, Cronbach’s alpha was 0.96.
Depressive symptoms were evaluated using the 6-item depression subscale of the Brief Symptom Inventory-18 (Derogatis, 2001). Participants were asked to rate certain feelings during the previous 7 days on a 5-point scale from 0 (not at all) to 4 (extremely). The inventory has been translated into Hebrew and is widely used. A mean score was calculated. In the current study, internal reliability (Cronbach’s alpha) for the 18-item questionnaire was 0.95; for the six depression items, it was also 0.95.
Resilience is a multidimensional, context-related, complex phenomenon. Hence, its assessment is complicated and context related (Satapathy et al., 2022). In the current research, resilience was evaluated using the Connor-Davidson Resilience Scale (Campbell-Sills and Stein, 2007), a widely validated and used self-report questionnaire that evaluates perceptions of self-efficacy and adaptability in the face of stressful situations. This tool features 10 personal resilience statements evaluated on a 5-point Likert scale from 0 (not at all) to 4 (strongly agree) regarding the prior month. For example: “I am able to handle anything that happens in my life.” A sum score was calculated (range = 0–40). This tool was chosen because it examines the relevant resilience characteristics of adult participants, was previously used to evaluate veteran populations (e.g., Green et al., 2014; Hughes et al., 2018), and was found to have good internal reliability of 0.86 (Smith et al., 2019). In the current study, Cronbach’s alpha was 0.89.
Emotional-approach coping, consisting of emotional processing and emotional expression subscales (Stanton et al., 2000a,b), was used to evaluate participants’ emotional coping mechanisms. We used a short version of this tool—five items from the emotional expression subscale (e.g., “I allow myself to express my feelings”) and eight items from the emotional processing subscale (e.g., “I take time to understand what I really feel”). Participants rated their answers on a 5-point Likert scale (1 = not at all, 5 = very much). A sum score was calculated for each subscale (range: 8–40). We used a Hebrew translation of this questionnaire (Cohen and Numa, 2011). This tool was found to have good internal reliability in previous studies (e.g., Cohen and Numa, 2011; Marroquin et al., 2016). Internal reliability for emotional processing and emotional expression was 0.72 and 0.82, respectively (Stanton et al., 2000b). In the current study, Cronbach’s alpha was 0.94 for emotional processing and 0.93 for emotional expression.
2.3 Statistical analysis
Data were collected using the Qualtrics platform and later organized for statistical analysis using SPSS 27.0. Descriptive statistics and preliminary analyses were performed in SPSS. The research model was processed using a structural equation modeling path analysis with IBM AMOS 27.0, with the goal of assessing direct and indirect pathways from resilience to PTSS. The placement of the variables in the path analysis was based on the stress and coping model (Lazarus and Folkman, 1984), suggesting that the effect of resilience as a personal resource on psychological outcomes of stressful encounters is mediated via coping strategies. Six cases of missing education data were imputed using variable means. Model fit was assessed using the following indexes: chi-square and normed chi-square tests to assess the model’s overall fit and parsimony; comparative fit index (CFI), Tucker-Lewis Index (TLI), and normed fit index (NFI), which are incremental fit indexes; and root mean-square error of approximation (RMSEA) and its confidence interval (CI), which measures the discrepancy per degree of freedom and indicates the model’s absolute fit. To increase understanding of the mediation paths, the unstandardized indirect and total effects of the specific paths were evaluated using bootstrapping (5,000 bootstrap samples) via the user-defined estimands option.
3 Results
Table 2 shows means, standard deviations, and correlations between the study variables. Mean levels of PTSS were low but ranged widely, from 0 to 70. In addition, 66% of the participants reported very low PTSD levels (PCL ≤ 15), 21% described low to subthreshold PTSD levels (15 ≤ PCL ≤ 33), and a small yet substantial minority (13%) described clinical PTSD levels (PCL > 33). Levels of depressive symptoms were also low. Moreover, participants reported high levels of resilience, although scores varied from 0 to 40. Mean levels of emotional processing were high and substantially higher than levels of emotional expression. PTSS and depression were negatively associated with resilience. Emotional expression and emotional processing were positively associated with resilience. However, only emotional expression, which involves verbal or nonverbal efforts to express and share emotional experiences, was significantly and negatively associated with PTSS and depression. On the other hand, emotional processing, which consists of attempts to acknowledge, explore, and understand emotions, was not significantly associated with PTSS or depression.
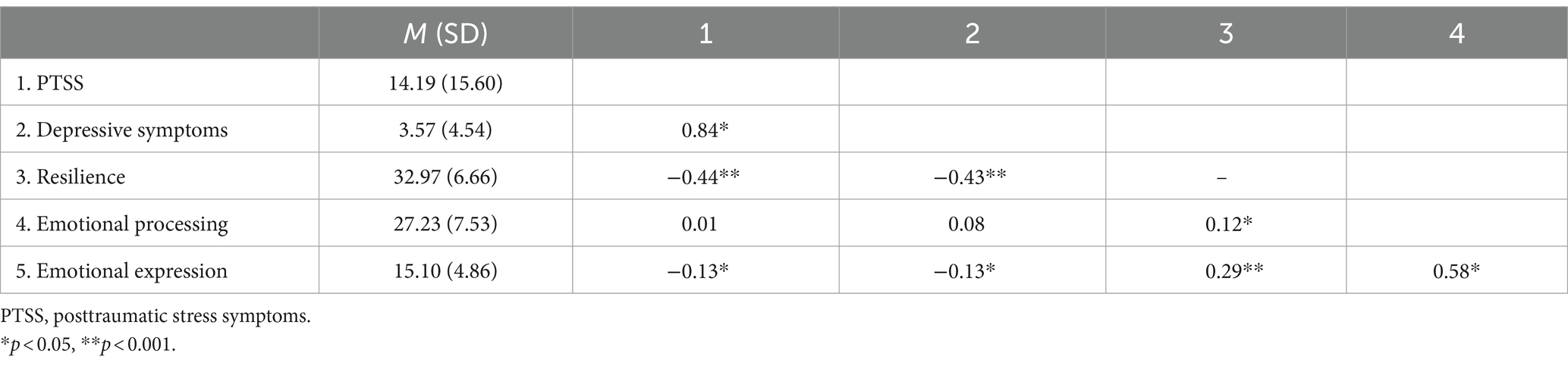
Table 2. Means, standard deviations, and Pearson correlations of the study variables.
Due to the high association between PTSS and depression and their similar associations with the other study variables, the consequent analysis was conducted only with PTSS. Prior to assessment of the direct and indirect associations among resilience, emotional-approach coping, and PTSS via path analysis, we examined what background variables should be controlled. Physical injury that occurred during army service, exposure to PTEs, and years of education were significantly associated with levels of PTSS. However, all injured participants also reported exposure to PTEs; therefore, exposure and education variables were added to the study model. The study model was examined with path analysis (Figure 1), in which emotional processing and expression were defined as mediators of resilience and PTSS, whereas injury and education were control variables. The fit indexes of the model were good: χ2(7) = 5.11, p = 0.65; NFI = 0.99, CFI = 1.00, TLI = 1.01, RMSEA = 0.00, 95% CI [0.00, 0.04]. The model showed that after controlling for exposure to PTEs and years of education (which were associated with PTSS), resilience was directly and negatively associated with PTSS (direct effect: b = −0.79, SE = 0.09, 95% CI [−1.06, −0.54]; total effect: b = −0.35, SE = 0.04, 95% CI [−0.42, −0.26]). Emotional expression and emotional processing were also directly associated with PTSS, showing a negative effect for emotional expression (b = −0.21, SE = 0.16, 95% CI [−0.31, −0.12]) and a positive effect for emotional processing (b = 0.25, SE = 0.10, 95% CI [1.00, 0.37]). Further analysis using bootstrapping indicated that the indirect and total effects for both paths between resilience and PTSS were significant (Table 3).
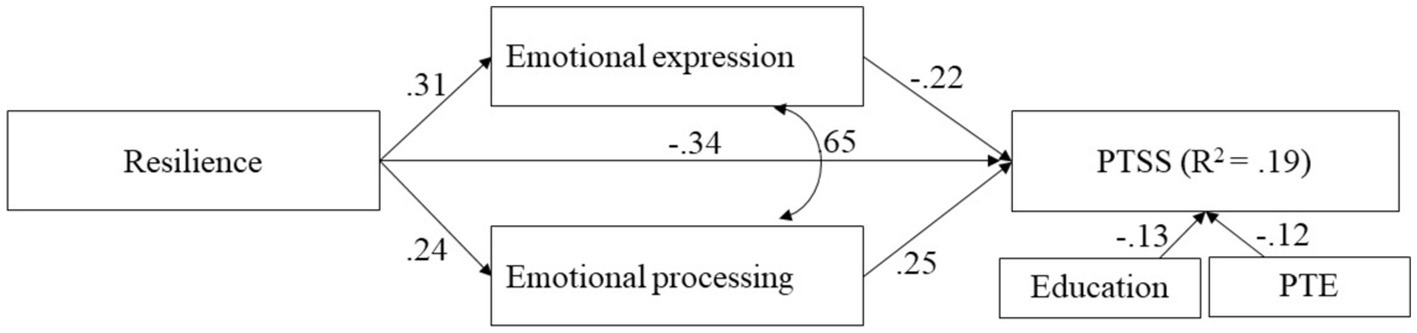
Figure 1. Path analysis for direct and mediated associations between resilience and PTSS. Path analysis for resilience, emotional expression, and processing and PTSS. Model also includes education and PTE as controls. Standardized estimates are shown. PTSS, posttraumatic stress symptoms; PTE, potentially traumatic events (p < 0.001).
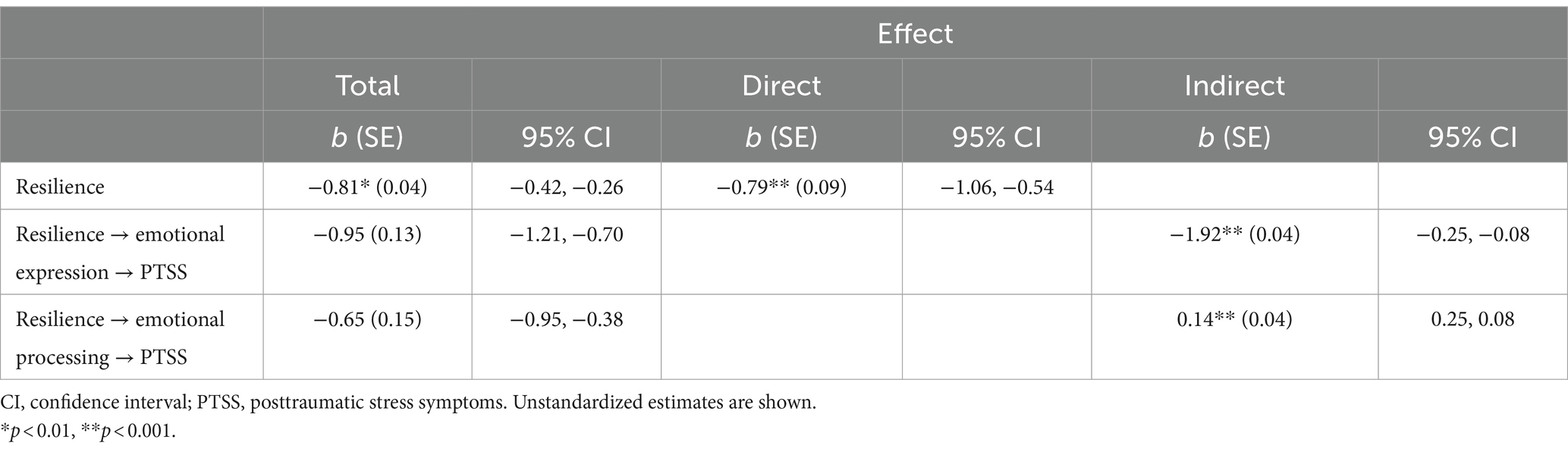
Table 3. Summary of total, direct, and indirect effects of resilience on PTSS.
4 Discussion
The present study found low levels of PTSS and depression and high levels of resilience among veterans, along with strong negative associations between resilience and symptoms. Moreover, these associations were mediated by emotional-approach coping. However, a distinct mediating role of each coping strategy emerged: Although both emotional expression and processing were associated with higher resilience, emotional expression mediated a positive association between resilience and PTSS, whereas emotional processing mediated a negative association with PTSS.
Like in previous studies (Fogle et al., 2020), veterans’ resilience levels were found to be relatively high and their PTSS and depression levels were generally low. Because Israel constantly deals with security threats, health care experts have highlighted the importance of the ecological construct of Israeli resilience. Composed of four major systems (micro or individual, meso or family, exo or society, and macro or state), resilience in Israel exists during times of routine life and emergency—and equally importantly, in the periods between the two (Nuttman-Shwartz and Green, 2021). The relations among these resilience levels are apparently relatively strong and stable in Israel, as described by experts who have highlighted Israeli’s “sense of mission” and “connectedness to others” as main resources that maintain their “inner strength, coping skills, and hope” (Corzine et al., 2017, p. 5). The findings of the current research are in line with this approach. Also, the strong association between PTSS and depression accords with previous studies (Armenta et al., 2019), suggesting that PTSD does not cover all manifestations of postservice distress and despite its centrality in the trauma discourse, represents only part of veterans’ posttraumatic emotional burden. The relations between PTSD and posttraumatic depression are complex and deserve further longitudinal research.
The current study was the first to examine the role of emotional-approach coping in relation to resilience and veterans’ PTSS. Structural equation modeling revealed that although both emotional-approach coping strategies were associated with higher resilience, they showed an inverse mediation effect. Emotional expression was negatively associated with PTSS, indicating that higher resilience was related to lower PTSS when connected with higher emotional expression (Van Voorhees et al., 2018; Fogle et al., 2020). This finding suggests that more use of emotional expression might enable emotions to be seen and shared with others, hence promoting relief (Stanton et al., 2000a). In line with Stanton et al.’s (2000a) findings, the analysis revealed that emotional processing was positively related to resilience but also higher PTSS. This finding suggests that higher involvement in emotional processing might increase PTSS among veterans, because it may represent a ruminative component.
Previous studies presented relations between the use of emotional-approach coping and lower levels of psychological symptoms regarding several stressful conditions, mostly concerning physical illness and physical pains (Austenfeld and Stanton, 2004; Jensen-Johansen et al., 2013; Batenburg and Das, 2014; Yeung and Chow, 2019). However, the clinical presentation of this trend seems to be more complex, with some research highlighting the fact that emotional processing’s effect may vary depending on the time since the traumatic or stressful event and how long this coping method is used (Stanton and Low, 2012; Juth et al., 2015). Similar to the present study’s findings, Hoyt et al. (2020) found that among older people, only emotional expression was related to better and more stable health outcomes over time, whereas emotional processing was related to increased depression in times of stress. Also, in support of the present study, only processing was found to be related to increased negative cognition and emotions (Watkins, 2004). These findings raise the questions of how, when, and for whom emotional-approach coping may be beneficial and whether it can be harmful in certain circumstances. A possible explanation for the sometimes-negative impact of intensive use of emotional processing is that it may foster rumination through the tendency to focus on negative emotions in a repeated manner, amplifying the consequences of those negative emotions. Rumination was found to be associated with increased symptoms of depression and anxiety and the onset of major depressive episodes (Nolen-Hoeksema and Davis, 1999; Vine et al., 2019). However, due to the correlational nature of the results, it may be that individuals with higher PTSS are more involved in emotional processing that encourages rumination.
Furthermore, veterans who presented high levels of emotional processing alongside high levels of resilience might experience resilience as a double-edged sword (Adler and Sowden, 2018). In other words, it seems that although these resilient veterans managed to process their emotions in a more thorough way alone, they were also vulnerable. Paradoxically, the ability to process distress alone can impair the possibility of reducing that distress. This finding is an example of veterans’ radical implementation of the army’s values and culture, which encourage its members to embrace selflessness and personal courage (Adler and Sowden, 2018), which might be interpreted as contradictory to turning to others for help.
Our research contributes to the understanding of this complexity by shedding light on how these processes occur among veterans who deal with military-related traumatic stress, which is characterized by substantial avoidance of emotional sharing stemming from the nature of the trauma and the atmosphere of military service (Solomon, 2020). Because combat soldiers usually seek to live up to masculine codes of behavior and face negative stigma when these codes are not respected (O’Loughlin et al., 2020), sharing of emotions and emotional expressions of feelings seen as “soft” and “weak” is usually difficult. Understanding the nuances of this trend among veterans is of great importance, especially in light of the gap between different types of intimacy they represent. Although soldiers and veterans tend to maintain very intimate relationships with their fellow squad members, which is expressed in the ability to share significant and powerful emotional experiences related to combat and service, they often simultaneously have difficulty sharing personal feelings or moments of emotional weakness and hardship arising from these same experiences.
The fact that emotional expression mediated PTSS for veterans with high resilience levels in this study might indicate the need to encourage veterans to share their hardships via social interaction. It also supports the important role of family members and close others in such sharing initiatives, because they may foster this positive trend and help break the loneliness cycle that sometimes traps trauma victims (Shorer et al., 2024).
4.1 Limitations
Our study has several methodological limitations. The research sample consisted of participants who applied to a program aiming to process combat experiences. It is reasonable to believe that they were more oriented toward emotional processing or expression of feelings than veterans who did not participate in such an intervention. Hence, our sample might be somewhat imbalanced. However, the large sample included full squads and companies from various army units. This means that people of varied backgrounds and many veterans who were not “emotionally oriented” participated in this intervention and study, and their standpoints might have balanced the sample.
Due to the cross-sectional design, the assessment of both resilience and PTSS levels should be interpreted cautiously, because the levels of these factors may change during post-trauma recovery and developmental stages (Masten, 2015). Moreover, as multilayered phenomena, both conditions should be further studied through the use of varied assessment tools and longitudinal research designs. Based on a limited cross-sectional design and only one resilience assessment tool, our study could not offer any causal interpretations or further explore distinct associations between specific resilience features and PTSS. Accordingly, this study does not permit causal inferences, and further studies using longitudinal design are encouraged. We recommend that future work on emotional-approach coping explore the relations between different emotional involvement and coping mechanisms among various trauma-exposed populations, along with studying the point at which emotional processing coping may become negative.
Despite the high rates of female soldiers in the Israeli military (Israel Defense Forces, 2013), few of them turn to military-experience processing programs, and units that use this psychological source are usually male dominated. One possible explanation for this is that female soldiers are expected to adopt “manly” trends during their service; hence, they learn to hide their emotions. Because emotional processing is the opposite of this, they might be confused by this ambiguous message (Harel-Shalev and Daphna-Tekoah, 2020). Because the current research dealt with male veterans only, its conclusions should not be generalized to female veteran populations.
4.2 Clinical applications
The results of the current study suggest that although resilience is a major factor in facing the effects of psychological trauma, its implementation and manifestations depend on individual coping skills. Common coping strategies should be examined in relation to the context in which they are implemented. Promoting resilience among veterans should encourage emotional expressions, and not limited to cognitive or emotional processing only. Interventions to promote the use of this strategy may include initiating social relationships, teaching stress management, and the restructuring of cognitive standpoints toward emotions (Van Voorhees et al., 2018). According to our findings, supporting emotional expression might reduce postservice emotional distress while not harming veterans’ resilience levels.
5 Conclusion
This study explored associations among veterans’ resilience levels, emotional coping mechanisms, and PTSS levels. The findings highlight the importance of emotional expressions of trauma-related reactions to enhance veterans’ well-being. Further investigation of trauma survivors’ specific emotional coping mechanisms is needed.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, upon contacting the corresponding author.
Ethics statement
The studies involving humans were approved by Board of Ethics, Faculty of Social Welfare and Health Sciences, University of Haifa, Israel. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
SS: Conceptualization, Investigation, Project administration, Writing – original draft, Writing – review & editing. MW: Conceptualization, Data curation, Investigation, Methodology, Writing – review & editing. LC: Data curation, Investigation, Writing – review & editing. DM: Conceptualization, Writing – review & editing. MC: Conceptualization, Data curation, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
DM serves as the clinical director of B’Shvil, a non-governmental organization which provides veterans with Nature-Assisted group interventions for processing post military-related stress.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Adler, A. B., and Sowden, W. J. (2018). “Resilience in the military: the double-edged sword of military culture” in Military and veteran mental health: A comprehensive guide. eds. L. W. Roberts and C. H. Warner (New York, NY: Springer), 43–54.
Armenta, R. F., Walter, K. H., Geronimo-Hara, T. R., Porter, B., Stander, V. A., LeardMann, C. A., et al. (2019). Longitudinal trajectories of comorbid PTSD and depression symptoms among U.S. service members and veterans. BMC Psychiatry 19:396. doi: 10.1186/s12888-019-2375-1
Austenfeld, J. L., and Stanton, A. L. (2004). Coping through emotional approach: a new look at emotion, coping, and health-related outcomes. J. Pers. 72, 1335–1364. doi: 10.1111/j.1467-6494.2004.00299.x
Batenburg, A., and Das, E. (2014). Emotional approach coping and the effects of online peer-led support group participation among patients with breast cancer: a longitudinal study. J. Med. Internet Res. 16:e256. doi: 10.2196/jmir.3517
Biggs, A., Brough, P., and Drummond, S. (2017). “Lazarus and Folkman’s psychological stress and coping theory” in The handbook of stress and health: A guide to research and practice. eds. C. L. Cooper and J. C. Quick (New York, NY: Wiley), 349–364.
Blackburn, L., and Owens, G. P. (2016). Rumination, resilience, and posttraumatic stress disorder symptom severity among veterans of Iraq and Afghanistan. J. Aggress. Maltreat. Trauma 25, 197–209. doi: 10.1080/10926771.2015.1107174
Blevins, C. A., Weathers, F. W., Davis, M. T., Witte, T. K., and Domino, J. L. (2015). The posttraumatic stress disorder checklist for DSM-5 (PCL-5): development and initial psychometric evaluation. J. Trauma. Stress. 28, 489–498. doi: 10.1002/jts.22059
Bonanno, G. A. (2021). The resilience paradox. Eur. J. Psychotraumatol. 12:1942642. doi: 10.1080/20008198.2021.1942642
Bonnano, G. A., Chen, S., and Galatzer-Levy, I. R. (2023). Resilience to potential trauma and adversity through regulatory flexibility. Nat. Rev. Psychol. 2, 663–675. doi: 10.1038/s44159-023-00233-5
Boscarino, J. A., Adams, R. E., Urosevich, T. G., Hoffman, S. N., Kirchner, H. L., Boscarino, J. J., et al. (2018). Mental health impact of homecoming experience among 1730 formerly deployed veterans from the Vietnam war to current conflicts: results from the veterans’ health study. J. Nerv. Ment. Dis. 206, 757–764. doi: 10.1097/NMD.0000000000000879
Campbell-Sills, L., and Stein, M. B. (2007). Psychometric analysis and refinement of the Connor-davidson resilience scale (CD-RISC): validation of a 10-item measure of resilience. J. Trauma. Stress. 20, 1019–1028. doi: 10.1002/jts.20271
Carra, K., Curtin, M., Fortune, T., and Gordon, B. (2022). Service and demographic factors, health, trauma exposure, and participation are associated with adjustment for former Australian defense force members. Mil. Psychol. 35, 480–492. doi: 10.1080/08995605.2022.2120312
Carver, C. S., and Connor-Smith, J. (2010). Personality and coping. Annu. Rev. Psychol. 61, 679–704. doi: 10.1146/annurev.psych.093008.100352
Cohen, M., and Numa, M. (2011). Posttraumatic growth in breast cancer survivors: a comparison of volunteers and non-volunteers. Psycho-Oncology 20, 69–76. doi: 10.1002/pon.1709
Connor, K. M., and Davidson, J. R. (2003). Development of a new resilience scale: the Connor-Davidson resilience scale (CD-RISC). Depress. Anxiety 18, 76–82. doi: 10.1002/da.10113
Corzine, E., Figley, C. R., Marks, R. E., Cannon, C., Lattone, V., and Weatherly, C. (2017). Identifying resilience axioms: Israeli experts on trauma resilience. Traumatology 23, 4–9. doi: 10.1037/trm0000094
Denckla, C. A., Cicchetti, D., Kubzansky, L. D., Seedat, S., Teicher, M. H., Williams, D. R., et al. (2020). Psychological resilience: an update on definitions, a critical appraisal, and research recommendations. Eur. J. Psychotraumatol. 11:1822064. doi: 10.1080/20008198.2020.1822064
Derogatis, L. R. (2001). BSI-18: Administration, scoring and procedures manual. Piscataway, NJ: National Computer Systems.
Fishbein, J. N., Judd, C. M., Genung, S., Stanton, A. L., and Arch, J. J. (2022). Intervention and mediation effects of target processes in a randomized controlled trial of acceptance and commitment therapy for anxious cancer survivors in community oncology clinics. Behav. Res. Ther. 153:104103. doi: 10.1016/j.brat.2022.104103
Fogle, B. M., Tsai, J., Mota, N., Harpaz-Rotem, I., Krystal, J. H., Southwick, S. M., et al. (2020). The National Health and resilience in veterans study: a narrative review and future directions. Front. Psych. 11:538218. doi: 10.3389/fpsyt.2020.538218
Fulton, J. J., Calhoun, P. S., Wagner, H. R., Schry, A. R., Hair, L. P., Feeling, N., et al. (2015). The prevalence of posttraumatic stress disorder in operation enduring freedom/operation Iraqi freedom (OEF/OIF) veterans: a meta-analysis. J. Anxiety Disord. 31, 98–107. doi: 10.1016/j.janxdis.2015.02.003
Galatzer-Levy, I. R., Huang, S. H., and Bonanno, G. A. (2018). Trajectories of resilience and dysfunction following potential trauma: a review and statistical evaluation. Clin. Psychol. Rev. 63, 41–55. doi: 10.1016/j.cpr.2018.05.008
Gaudet, C. M., Sowers, K. M., Nugent, W. R., and Boriskin, J. A. (2015). A review of PTSD and shame in military veterans. J. Hum. Behav. Soc. Environ. 26, 56–68. doi: 10.1080/10911359.2015.1059168
Green, K. T., Hayward, L. C., Williams, A. M., Dennis, P. A., Bryan, B. C., Taber, K. H., et al. (2014). Examining the factor structure of the Connor-Davidson resilience scale (CD-RISC) in a post-9/11 U.S. military veteran sample. Assessment 21, 443–451. doi: 10.1177/1073191114524014
Harel-Shalev, A., and Daphna-Tekoah, S. (2020). Breaking the binaries in security studies: A gendered analysis of women in combat. New York, NY: Oxford University Press.
Hassija, C. M., Luterek, J. A., Naragon-Gainey, K., Moore, S. A., and Simpson, T. (2012). Impact of emotional approach coping and hope on PTSD and depression symptoms in a trauma exposed sample of veterans receiving outpatient VA mental health care services. Anxiety Stress Coping 25, 559–573. doi: 10.1080/10615806.2011.621948
Hoge, C. W., Grossman, S. H., Auchterlonie, J. L., Riviere, L. A., Milliken, C. S., and Wilk, J. E. (2014). PTSD treatment for soldiers after combat deployment: low utilization of mental health care and reasons for dropout. Psych. Serv. 65, 997–1004. doi: 10.1176/appi.ps.201300307
Hoyt, M. A., Wang, A. W., Boggero, I. A., Eisenlohr-Moul, T. A., Stanton, A. L., and Segerstrom, S. C. (2020). Emotional approach coping in older adults as predictor of physical and mental health. Psychol. Aging 35, 591–603. doi: 10.1037/pag0000463
Hughes, J. M., Ulmer, C. S., Hastings, S. N., Gierisch, J. M., and Mid-Atlantic VA MIRECC WorkgroupHoward, M. O. (2018). Sleep, resilience, and psychological distress in United States military veterans. Mil. Psychol. 30, 404–414. doi: 10.1080/08995605.2018.1478551
Inoue, C., Shawler, E., Jordan, C. H., and Jackson, C. A. (2023). Veteran and military mental health issues. Treasure Island, FL: StatPearls.
Israel Defense Forces. (2013). IDF leads the way in gender integration. Available at: https://www.idf.il/en/mini-sites/international-cooperation/idf-leads-the-way-in-gender-integration/ (Accessed February 28, 2024).
Jensen-Johansen, M. B., Christensen, S., Valdimarsdottir, H., Zakowski, S., Jensen, A. B., Bovbjerg, D. H., et al. (2013). Effects of an expressive writing intervention on cancer-related distress in Danish breast cancer survivors - results from a nationwide randomized clinical trial. Psycho-Oncology 22, 1492–1500. doi: 10.1002/pon.3193
Juth, V., Dickerson, S. S., Zoccola, P. M., and Lam, S. (2015). Understanding the utility of emotional approach coping: evidence from a laboratory stressor and daily life. Anxiety Stress Coping 28, 50–70. doi: 10.1080/10615806.2014.921912
Karstoft, K. I., Nielsen, A. B. S., Armour, C., Vedtofte, M. S., and Andersen, S. B. (2020). Trajectories of depression symptoms from pre- to post- deployment: does previous trauma predict symptom increase? J. Affect. Disord. 266, 120–127. doi: 10.1016/j.jad.2020.01.112
Knesset. (1986). Security service law: combined version. Available at: https://m.knesset.gov.il/Activity/committees/ForeignAffairs/LegislationDocs/SecurityService21_4.pdf (accessed December 5, 2023).
Knesset. (2008). Reservist law. Available at: https://main.knesset.gov.il/activity/legislation/laws/pages/lawprimary.aspx?t=lawlaws&st=lawlaws&lawitemid=2001396 (Accessed December 5, 2023).
Korte, K. J., Jiang, T., Koenen, K. C., and Gradus, J. (2020). “Trauma and PTSD: epidemiology, comorbidity, and clinical presentation in adults” in Effective treatments for PTSD. eds. D. Forbes, J. I. Bisson, C. M. Monson, and L. Berliner. 3rd ed (New York, NY: Guilford Press).
Lahad, M. (2017). From victim to victor: the development of the BASIC PH model of coping and resiliency. Traumatology 23, 27–34. doi: 10.1037/trm0000105
Marroquin, B., Czamanski-Cohen, J., Weihs, K. L., and Stanton, A. L. (2016). Implicit loneliness, emotion regulation, and depressive symptoms in breast cancer survivors. J. Behav. Med. 39, 832–844. doi: 10.1007/s10865-016-9751-9
Masten, A. S. (2015). Pathways to integrated resilience science. Psych. Inquiry 26, 187–196. doi: 10.1080/1047840X.2015.1012041
Masten, A., and Powell, J. (2003). “A resilience framework for research, policy, and practice” in Resilience and vulnerability: Adaptation in the context of childhood adversities. ed. S. Luthar (Cambridge: Cambridge University Press), 1–26.
Ministry of Health. (2023). The state of Israel is coping with a mass casualty incident, one of the largest that we have faced, both physically, emotionally and nationally. Available at: https://www.gov.il/en/departments/news/22102023-03 (Accessed December 5, 2023).
Mobbs, M. C., and Bonanno, G. A. (2018). Beyond war and PTSD: the crucial role of transition stress in the lives of military veterans. Clin. Psychol. Rev. 59, 137–144. doi: 10.1016/j.cpr.2017.11.007
National Center for PTSD. (n.d.). Using the PTSD checklist for DSM-5 (PCL-5). Available at: https://www.ptsd.va.gov/professional/assessment/documents/using-PCL5.pdf (Accessed December 5, 2023).
Nolen-Hoeksema, S., and Davis, C. G. (1999). Thanks for sharing that: ruminators and their social support networks. J. Pers. Soc. Psychol. 77, 801–814. doi: 10.1037/0022-3514.77.4.801
Nuttman-Shwartz, O., and Green, O. (2021). Resilience truths: trauma resilience workers’ points of view toward resilience in continuous traumatic situations. Int. J. Stress Manage. 28, 1–10. doi: 10.1037/str0000223
O’Loughlin, J. I., Cox, D. W., Ogrodniczuk, J. S., and Castro, C. A. (2020). The association between traditional masculinity ideology and predictors of military to civilian transition among veteran men. J. Mens Stud. 28, 318–338. doi: 10.1177/1060826520911658
Porter, B., Bonanno, G. A., Frasco, M. A., Dursa, E. K., and Boyko, E. J. (2017). Prospective post-traumatic stress disorder symptom trajectories in active duty and separated military personnel. J. Psychiatry Res. 89, 55–64. doi: 10.1016/j.jpsychires.2017.01.016
Satapathy, S., Dang, S., Sagar, R., and Dwivedi, S. N. (2022). Resilience in children and adolescents survived psychologically traumatic life events: a critical review of application of resilience assessment tools for clinical referral and intervention. Trauma Viol. Abuse 23, 288–300. doi: 10.1177/1524838020939126
Shafran Gittleman, I. (2020). Women in the IDF and the joint service order. Jerusalem: The Israeli Institute for Democracy.
Shorer, S., Cohen, L., Cohen, M., Marom, D., and Weinberg, M. (2023). Resilience, emotional approach coping and post-traumatic stress in Israeli veterans. In: Symposium presentation, 44th STAR conference, Faro, Portugal, July 2023.
Shorer, S., Weinberg, M., Koko, Y., and Marom, D. (2024). “My scar”: posttraumatic loneliness as a source of pain and resource for coping. Qual. Health Res. doi: 10.1177/10497323241226599
Smith, K. J., Emerson, D. J., Haight, T. D., Mauldin, S., and Wood, B. G. (2019). An examination of the psychometric properties of the Connor-Davidson resilience Scale-10 (CD-RISC10) among accounting and business students. J. Account. Educ. 47, 48–62. doi: 10.1016/j.jaccedu.2019.01.002
Solomon, Z. (2020). From the frontline to the homefront: the experience of Israeli veterans. Front. Psych. 11:589391. doi: 10.3389/fpsyt.2020.589391
Soper, D. S. (2024). A-priori sample size calculator for structural equation models [software]. Available at: https://www.danielsoper.com/statcalc (Accessed March 24, 2024)].
Stanton, A. L., Danoff-Burg, S., Cameron, C. L., Bishop, M., Collins, C. A., Kirk, S. B., et al. (2000a). Emotionally expressive coping predicts psychological and physical adjustment to breast cancer. J. Consult. Clin. Psychol. 68, 875–882. doi: 10.1037/0022-006x.68.5.875
Stanton, A. L., Kirk, S. B., Cameron, C. L., and Danoff-Burg, S. D. (2000b). Coping through emotional approach: scale construction and validation. J. Pers. Soc. Psycol. 78, 1150–1169. doi: 10.1037/0022-3514.78.6.1150
Stanton, A. L., and Low, C. A. (2012). Dispositional and stressor-related emotion regulation in the context of a chronic, life-limiting stressor. J. Pers. 80, 287–311. doi: 10.1111/j.1467-6494.2011.00732.x
Thompson, J. M., Dursun, S., VanTil, L., Heber, A., Kitchen, P., de Boer, C., et al. (2019). Group identity, difficult adjustment to civilian life, and suicidal ideation in Canadian armed forces veterans: life after service studies 2016. J. Mil. Veteran Fam. Health 5, 100–114. doi: 10.3138/jmvfh.2018-0038
Timmer-Murillo, S., Schramm, A. T., Geier, T. J., Mcleod, E., Larson, C. L., and deRoon-Cassini, T. A. (2023). Facets of emotion dysregulation differentially predict depression and PTSD symptom severity following traumatic injury. Eur. J. Psychotraumatol. 14:2193524. doi: 10.1080/20008066.2023.2193524
Van Voorhees, E. E., Wagner, H. R., Beckham, J. C., Bradford, D. W., Neal, L. C., Penk, W. E., et al. (2018). Effects of social support and resilient coping on violent behavior in military veterans. Psychol. Serv. 15, 181–190. doi: 10.1037/ser0000187
Vine, V., Bernstein, E. E., and Nolen-Hoeksema, S. (2019). Less is more? Effects of exhaustive vs. minimal emotion labelling on emotion regulation strategy planning. Cogn. Emot. 33, 855–862. doi: 10.1080/02699931.2018.1486286
Watkins, E. (2004). Adaptive and maladaptive ruminative self-focus during emotional processing. Behav. Res. Ther. 42, 1037–1052. doi: 10.1016/j.brat.2004.01.009
Weathers, F. W., Blake, D. D., Schnurr, P. P., Kaloupek, D. G., Marx, B. P., and Keane, T. M. (2013). The life events checklist for DSM-5 (LEC-5). Available at: https://www.ptsd.va.gov/professional/assessment/te-easures/life_events_checklist.asp (Accessed December 5, 2023).
Xue, C., Ge, Y., Tang, B., Liu, Y., Kang, P., Wang, M., et al. (2015). A meta-analysis of risk factors for combat-related PTSD among military personnel and veterans. PLoS One 10:e0120270. doi: 10.1371/journal.pone.0120270
Yancey, J. R., Carson, C. N., McGlade, E. C., and Yurgelun-Todd, D. A. (2023). A literature review of mental health symptom outcomes in U.S. veterans and servicemembers following combat exposure and military sexual trauma. Trauma Viol. Abuse. 25, 1431–1447. doi: 10.1177/15248380231178764
Yechimovitch-Cohen, N. (2022). Data on recognition of disability due to post-traumatic stress disorder following the military service. Jerusalem: Knesset Research and Information Center.
Yeung, N. C., and Chow, T. S. (2019). Coping with my own way: mediating roles of emotional expression and social support seeking in the associations between individual differences and posttraumatic growth. Health Psychol. 6, 1–8. doi: 10.1177/2055102919846596
Keywords: combat, coping, emotional approach coping, posttraumatic stress, resilience, veterans
Citation: Shorer S, Weinberg M, Cohen L, Marom D and Cohen M (2024) Emotional processing is not enough: relations among resilience, emotional approach coping, and posttraumatic stress symptoms among combat veterans. Front. Psychol. 15:1354669. doi: 10.3389/fpsyg.2024.1354669
Edited by:
Mahire Olcay Çam, Ege University, TürkiyeReviewed by:
Małgorzata Pięta-Lendzion, University of Warsaw, PolandSeema Bhatnagar, Children's Hospital of Philadelphia, United States
Richard Adams, Kent State University, United States
Copyright © 2024 Shorer, Weinberg, Cohen, Marom and Cohen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shai Shorer, c2hvcmVyc2hAZ21haWwuY29t