 Élise Mamimoué1,2*†
Élise Mamimoué1,2*† Christophe Gauld1,2†
Christophe Gauld1,2†- 1Department of Child Psychiatry, Hospices Civiles de Lyon, Université de Lyon, Bron, France
- 2Institut des Sciences Cognitives, UMR 5229 CNRS, Bron, France
Objective: The impact of social relationships on autistic adolescents has been recently studied. However, the link between social relationships and depression in autistic adolescents seem underrepresented in the scientific literature. Especially no specific assessment tool has been developed to evaluate depression in autistic adolescents. The aim of this narrative review is to raise the impact of social relationships on depression in autistic adolescents. We aim to propose lines of thought on the creation of a sensitive tool for identifying depression in this population.
Methods: We conducted two types of searches for articles and reviews on PubMed, Embase, and Cochrane. First, regarding social relationships, we searched the following terms: [(“adolesc*” OR “youth”) AND (“ASD” OR “autis*”) AND (“social communication” OR “peer relationship”) AND (“depress*”)]. Secondly, regarding assessment tool, we searched the following terms: [(“tool” OR “assess*”) AND (“depress*”) AND (“ASD” OR “Autis*)”].
Results: Social impact, verbal skills, and good social motivation are risk factors of depression in autistic adolescents. Social impairment during childhood is related to peer victimization and is a risk factor for depression. There is no specific tool to measure depression in autistic adolescents.
Conclusion: No specific tool based on social relationships was developed to evaluate depression in autistic adolescents. Depression in autistic adolescents needs to be assessed considering the social and pragmatic specificities of autism. Social communication and difficulties in peer relationships may be evaluated in specific assessment tools based on social relationships for depression in autistic adolescents.
Introduction
Autism is defined by impairments in communication and social interactions and restricted behaviors, interests, or activities (APA, 2013). Among autistic adolescents, 11–54% have major depressive disorder (hereinafter referred to as “depression”), and 13–79% have anxiety symptoms (Schwartzman and Corbett, 2020) and in the autistic pediatric population, depression rates variate from 0 to 83.3% (Stewart et al., 2022). Adolescence is a period at high risk of depression due to the characteristic hormonal and social changes as well as the increased academic challenges in this period (Hudson et al., 2019). However, in autistic adolescents, the mutual influences of peer relationships, depressive symptoms, and communication skills, weighted by autistic phenotype, seem difficult to determine.
Social communication difficulties is a core autistic symptom, and in autistic adolescents, social competence and quality of life are widely accepted to be improved by social skills groups (Reichow et al., 2013). Autistic behavioral phenotypes and the diversity of communication skills may be masked by depressive symptoms (Ghaziuddin et al., 2002; M. E. Stewart et al., 2006). Recognizing depressive symptoms in autistic adolescents, especially without language, is clinically difficult.
Several studies have evaluated the impact of social communication on the symptoms of depression in autistic young people as a part of their research. However, we did not identify any literature review specifically studying the impact of social relationships on depression in autistic adolescents. In the same way, we did not find any tool to assess depression in autistic adolescents while considering social communication and difficulties.
In this narrative review, we discuss the impact of social interaction on depression in autistic adolescents. Then, we highlight the lack of a specific diagnostic tool based on social communication for depression in this population.
Materials and methods
This narrative review is based on scientific literature identified without time limit and until August 2023 and is conducted according to the Scale for the Assessment of Narrative Review Articles (SANRA) (Baethge et al., 2019). Our aims are: (1) to describe the link between depression and social relations for autistic adolescents; (2) to analyze studies that have been working on a tool to evaluate depression in youth with autim (3) to sustain the proposal of a specific tool assessing depression in autistic adolescents based on social relationships, and communication difficulties. We used two search strategies to identify relevant studies.
First, research databases PubMed, Embase, and Cochrane were conducted with the following terms in Title, Abstract and Keywords [(“adolesc*” OR “youth”) AND (“ASD” OR “autis*”) AND (“social com*” OR “peer relation*”) AND (“depress*”)]. Then, secondly, we analyzed articles that researched depression assessment tool in autistic adolescents. For the assessment part, we searched the following terms: [(“tool” OR “assess*”) AND (“depress*”) AND (“ASD” OR “Autis*)”]. We did this work separately, then regrouped our research and analyzed only the publications meeting the inclusion criteria. We considered review, communication, and original research. Duplicate records and research that did not focus on term words and aims were eliminated. We focused on articles that investigated the link between social communication, peer relationships and depression in autistic adolescents.
Results
Depression and social relationships in depression in autistic adolescents
In autism, mood disorder can have various forms of verbal and non-verbal expression. For instance, it can manifest as moral distress, impaired social communication, or even behavioral problems. The overlap between these clinical manifestations, specific to autistic adolescents with depressive symptoms, can be particularly difficult to untangle (Ghaziuddin et al., 2002; M. E. Stewart et al., 2006). As reported in the scientific literature (Muskett et al., 2019; Pezzimenti et al., 2019), the appearance of (or the increase in) repetitive or stereotypical behaviors, self-harm, and conduct difficulties incline clinicians to suspect depressive disorder in autistic adolescents with minimal verbal language. However, beyond autistic traits and genetic vulnerabilities of depression, several studies have shown increased depression among autistic adolescents.
In a non-systematic review, DeFilippis and collaborators (DeFilippis, 2018) pointed out the higher rate of depression in autistic children, relative to neurotypical people, and presented the impact of social communication impairment and negative life events on autistic youth with depression. In the same way, the finding of Pouw and collaborators shows that, unlike in neurotypical development individuals, negative friendships and victimization predicted depression in 52% of autistic adolescents (Pouw et al., 2013). This study also showed that individuals presenting avoidant strategies to manage stressful situations in the autistic group had fewer depressive symptoms. The authors considered these avoidant behaviors as adaptive coping strategies.
Hedley & Young (Hedley and Young, 2006) were the first to show correlation between social comparison and depression, especially perceived group membership in adolescent with autism. Rai and collaborators (Rai et al., 2018) showed that autistic adolescents who experienced social difficulties at age 7 and were bullied at age 10 had an increased risk of depression at age 18, relative to autistic adolescents, or neurotypical children who did not report these difficulties. The authors explained that social communication difficulties caused bullying and indirectly induced depression in autistic adolescents. These results were confirmed by a study of 176 autistic adolescents, which also found that social communication difficulties induced peer victimization and, thus, could lead to depression in this population (Greenlee et al., 2020).
Finally, the social impact of peers on the variability of expression of depressive symptoms in autism was further described in a review studying different factors (Pezzimenti et al., 2019): an average or high IQ, social motivation, and life stress such as bullying are risk factors of depression in autistic adolescent. The authors suggested that a good understanding of their social condition and their social particularities might induce depressive symptoms.
Based on this scientific literature, we hypothesize that social environment and peer relationships, need to be considered in the diagnosis of depressive disorder in autistic adolescents. In this way, in Figure 1, we propose to exemplify the different influences of depression, behavioral phenotypes, peer relationships, and communication skills on autistic adolescents, taking the example of social loss as an environmental trigger of depression. We considered verbal language in the expression of depression, based on Greenlee et al. study. Greenle and collaborators (Greenlee et al., 2020) found that language impacts the difficulties of diagnosing depression in autistic adolescents. Autistic adolescents with verbal difficulties showed behavioral difficulties that may induce a lower rate of diagnosed depression in this population rather than the rate of behavioral difficulties.
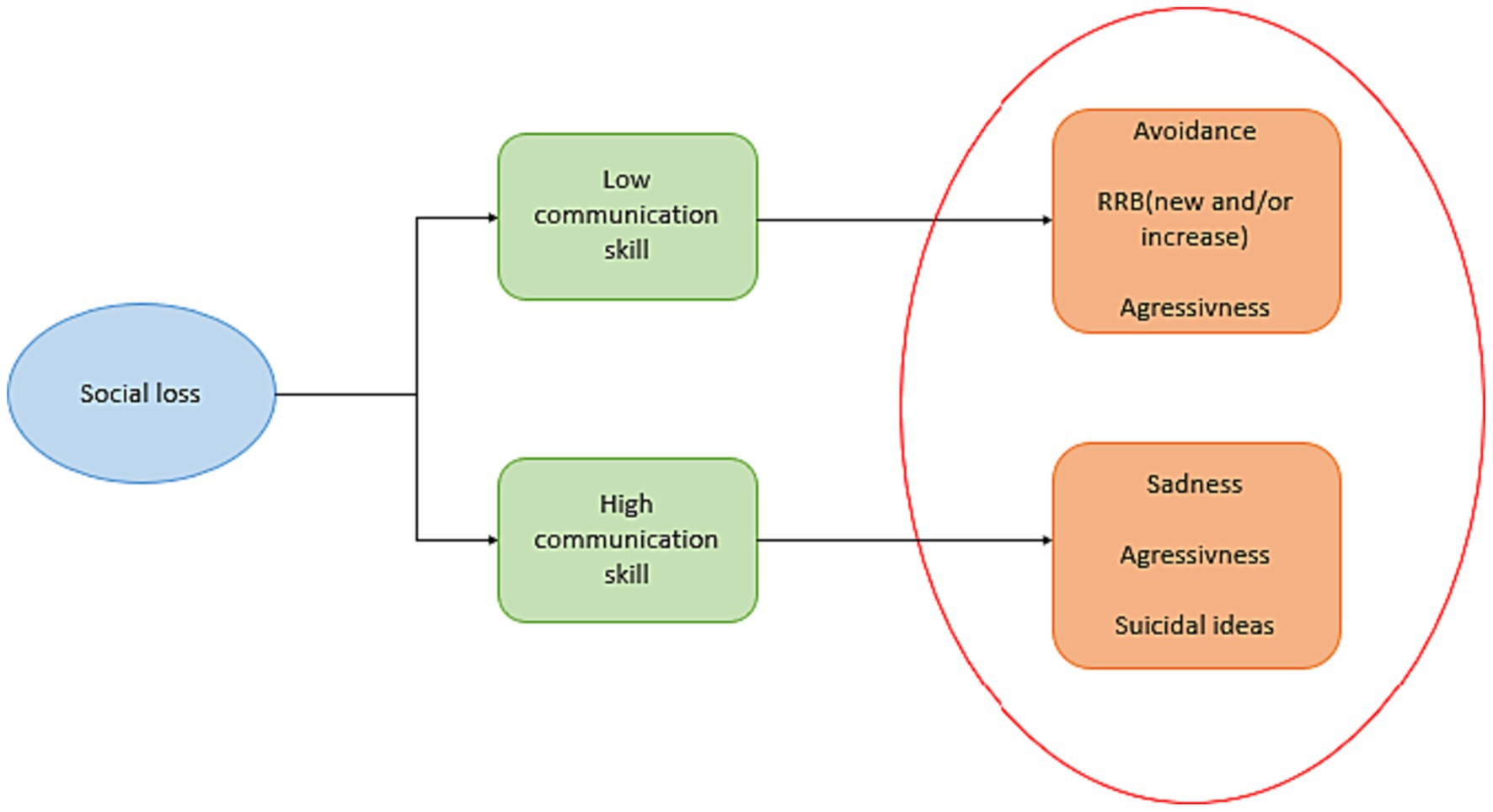
Figure 1. Impact of social loss on depressive symptoms of autistic adolescents according to their communication competence. There is a difference in depressive symptoms. Due to communication difficulties, autistic adolescents with communication difficulties express less sadness and suicidal ideas but show a behavioral response of avoidance or repetitive restrictive behavior (RRB) than autistic adolescents without communication difficulties. However (hetero- or auto-) aggressiveness manifests in both phenotypes.
Finding a good assessment tool based on social items for depression in autistic adolescents
There is currently no specific tool based on social items for assessing depression among autistic adolescents. Indeed, standardized tools used on autistic adolescents focused on depressive symptoms were the Children’s Depression Rating Scale-Revised (CDRS-R) (Mayes et al., 2010), the Children’s Depression Inventory (CDI) (Kovacs, 2011), the Beck Depression Inventory (Kovacs, 2011), the Depression Anxiety Stress Scales (Lovibond and Lovibond, 1995), the Revised Child Anxiety and Depression Scale (RCADS) (Chorpita et al., 2000), the Short Mood and Feelings Questionnaire (SMFQ) (Sharp et al., 2006) and the criteria of the Diagnostic and Statistical Manual of Mental Disorders-5th edition (DSM-5) (APA, 2013). One of the major disadvantages of these scales is their lack of specificity regarding (adolescents with) ASD(Towbin et al., 2005).
A systematic review found only two studies that examined the psychometric properties of depression in autistic children, using two scales: the CDI and the RCADS (Kim, 2021). These assessment tools had lower sensitivity and specificity when used in autistic children relative to neurotypical children. In parallel, Ozsvadjian and collaborators proposed the Children’s Automatic Thoughts Scale (CATS) (Schniering and Rapee, 2002) for assessed depression in autistic young (Ozsivadjian et al., 2014).
To our knowledge, only three studies looked at the development of a specific scale for assessing depression in autistic adolescents. First, Leyfer et al. (2006) proposed the semi-structured Autism Comorbidity Interview–present and lifetime version (ACI-PL), based on the Kiddie Schedule for Affective Disorders and Schizophrenia (KSADS) (Kaufman et al., 1997). The authors screened responses to specify if individuals felt guilty, worthless, or how they understood separation anxiety. They also considered subsyndromal disorder due to the communication or cognitive impairment of some autistic adolescents. This study considered the point of view of autistic adolescents and, more precisely, how they phenomenologically understood their symptoms. KSADS did not evaluate communication impairment, peer relations impact, or bullying. Secondly, a pilot study using the PHQ-9 (for parents and as a self-questionnaire – validated in the TD population) evaluated depression in autistic youth (Pilunthanakul et al., 2021). The authors included youth aged 10–18 years diagnosed with autism and ensured the presence in their sample of children with depression. They used the Mini-Kids, a structured diagnostic interview for DSM-5 in children and adolescents (Sheehan et al., 2010), to evaluate “comorbid disorders.” Unfortunately, the study showed that the tool had lower sensitivity and specificity in autistic adolescents relative to the control population. A high level of depressive symptoms and suicidality was found in autistic adolescents. The authors also discussed the impact of social communication and victimization of autistic youth on their depressive symptoms, but they did not consider social communication and victimization for their assessment tool. Finally, a third study evaluated how the environment can predict depressive symptoms in autistic adolescents (Dallman et al., 2021). The authors used the CDI (self and parental report), the Positive and Negative Affect Scale (PANAS) Children’s Version, Short Form (Ebesutani et al., 2012) and the Ecological Momentary Assessment (EMA) (Shiffman et al., 2008)to evaluate depression in this population. The authors focused on momentary affects and trait factors on the population.
Discussion
We have seen that a recent literature highlighted the impact of social relationships on the depressive symptoms of autistic adolescents (Pouw et al., 2013; DeFilippis, 2018; Rai et al., 2018; Greenlee et al., 2020). Loneliness and bullying are depressive symptom triggers related to social rejection, i.e., a loss of social ties (Pezzimenti et al., 2019), potentially impacting adult life (Lyznicki et al., 2004; Gray et al., 2012). The use of more sensitive and standardized psychometric tools for assessing depressive disorders in autistic adolescents could be of interest to clinicians and could give them a better view of the status of depression in autistic adolescents. However, none of these previous scales was based on communication and social interaction difficulties. Moreover, most of the assessing tools assessing depression in autism are self-report questionnaires. Autism being characterized by pragmatics difficulties, it is uncertain that autistic adolescents understand these self-questionnaires as well as the neurotypical population (Cassidy et al., 2021). This point shows the importance of an adapted tool for the autistic population w to assess depression based on social impairments.
The use of several scales aiming to evaluate social communication in austim, such as the Social Communication Questionnaire (Chandler et al., 2007), the Social Reciprocity Scale (Bruni, 2014), or the Children’s Communication Checklist (Bishop, 1998), could be of great interest. Social items seem to be important pillars in evaluating depression in autistic adolescents. However, to this date, none of these scales is adapted to depressive symptoms (Towbin et al., 2005).
Our study has limitations. First, the method of analysis and research follow the rules of a necessarily imperfect narrative review, which can lead to a risk of missing key references and induced biases in the analysis. However, we follow the systematic SANRA guidelines for this kind of review. Secondly, we found few studies with large samples (Lerner et al., 2018; Rai et al., 2018; Pilunthanakul et al., 2021), which may also induce a sample bias. Furthermore, most of the studies were not international, which did not allow to evaluate the impact of culture on the depressive symptoms. Thirdly, we only focused on the relation between peer relationships and their impact on depression in autistic adolescents. In this way, we are not exhaustive concerning global mental states, or therapies for depression in this population. Finally, we only considered scales that clearly diagnosed depression understood as a disorder (and not, for instance, anxiety, understood as a co-occurring).
Conclusion and futures directions
Depression in autistic adolescents can be difficult to assess due to the complexity of the neurological difference, and also due to the lack of specific assessment tools based on the specific characteristics of this population (i.e., its different degrees of communication and social impairments). However, scientific literature shows the impact of communication and peer relationships on the depressive symptoms of autistic adolescents. Based on the absence of systematized scale built to assess the communicational and social impact on depressive symptoms in autistic adolescents, we propose in Table 1 five recommendations for future research to develop such a tool for this population, considering communication and peer relationships.
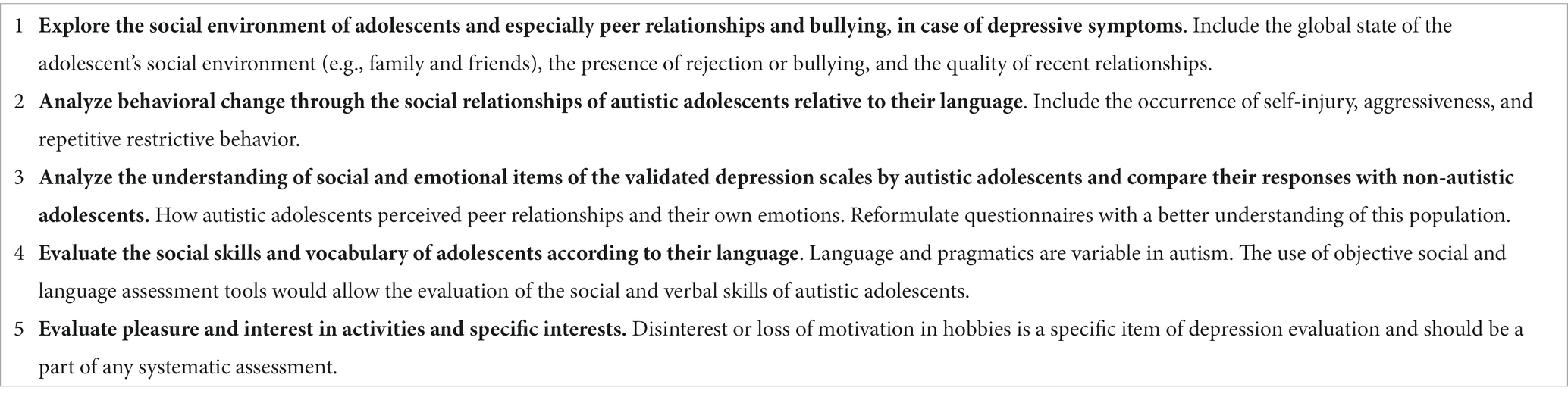
Table 1. Five recommendations to sustain the development of a specific assessment tool for depressive disorders in autistic adolescents based on communicational and social impacts.
Author contributions
ÉM: Conceptualization, Investigation, Methodology, Resources, Validation, Writing – original draft, Writing – review & editing. CG: Investigation, Methodology, Resources, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Baethge, C., Goldbeck-Wood, S., and Mertens, S. (2019). SANRA—a scale for the quality assessment of narrative review articles. Res. Integ. Peer Rev. 4:5. doi: 10.1186/s41073-019-0064-8
Bishop, D. V. M. (1998). Development of the Children’s communication checklist (CCC): a method for assessing qualitative aspects of communicative impairment in children. J. Child Psychol. Psychiatry 39, 879–891. doi: 10.1111/1469-7610.00388
Bruni, T. P. (2014). Test review: social responsiveness scale–second edition (SRS-2). J. Psychoeduc. Assess. 32, 365–369. doi: 10.1177/0734282913517525
Cassidy, S. A., Bradley, L., Cogger-Ward, H., and Rodgers, J. (2021). Development and validation of the suicidal behaviours questionnaire - autism Spectrum conditions in a community sample of autistic, possibly autistic and non-autistic adults. Mol. Autism. 12:46. doi: 10.1186/s13229-021-00449-3
Chandler, S., Charman, T., Baird, G., Simonoff, E., Loucas, T., Meldrum, D., et al. (2007). Validation of the social communication questionnaire in a population cohort of children with autism Spectrum disorders. J. Am. Acad. Child Adolesc. Psychiatr. 46, 1324–1332. doi: 10.1097/chi.0b013e31812f7d8d
Chorpita, B. F., Yim, L., Moffitt, C., Umemoto, L. A., and Francis, S. E. (2000). Assessment of symptoms of DSM-IV anxiety and depression in children: a revised child anxiety and depression scale. Behav. Res. Ther. 38, 835–855. doi: 10.1016/s0005-7967(99)00130-8
Dallman, A. R., Bailliard, A., and Harrop, C. (2021). Identifying predictors of momentary negative affect and depression severity in adolescents with autism: an exploratory ecological momentary assessment study. J. Autism Dev. Disord. 52, 291–303. doi: 10.1007/s10803-021-04935-8
DeFilippis, M. (2018). Depression in children and adolescents with autism Spectrum disorder. Children 5:112. doi: 10.3390/children5090112
APA (2013). Diagnostic and statistical manual of mental disorders: DSM-5™, 5th Ed. Arlington, VA, US: American Psychiatric Publishing, Inc.
Ebesutani, C., Regan, J., Smith, A., Reise, S., Higa-McMillan, C., and Chorpita, B. (2012). The 10-item positive and negative affect schedule for children, child and parent shortened versions: application of item response theory for more efficient assessment. J. Psychopathol. Behav. Assess. 34, 191–203. doi: 10.1007/s10862-011-9273-2
Ghaziuddin, M., Ghaziuddin, N., and Greden, J. F. (2002). Depression in persons with autism: implications for research and clinical care. J. Autism Dev. Disord. 32, 299–306. doi: 10.1023/A:1016330802348
Gray, K., Keating, C., Taffe, J., Brereton, A., Einfeld, S., and Tonge, B. (2012). Trajectory of behavior and emotional problems in autism. Am. J. Intellect. Dev. Disabil. 117, 121–133. doi: 10.1352/1944-7588-117-2.121
Greenlee, J. L., Winter, M. A., and Johnson, M. (2020). Depression symptoms in adolescents with autism Spectrum disorder: a contextual approach to mental health comorbidities. J. Adolesc. 85, 120–125. doi: 10.1016/j.adolescence.2020.10.005
Hedley, D., and Young, R. (2006). Social comparison processes and depressive symptoms in children and adolescents with Asperger syndrome. Autism 10, 139–153. doi: 10.1177/1362361306062020
Hudson, C. C., Hall, L., and Harkness, K. L. (2019). Prevalence of depressive disorders in individuals with autism Spectrum disorder: a meta-analysis | SpringerLink. J. Abnorm. Child Psychol. 47, 165–175. doi: 10.1007/s10802-018-0402-1
Kaufman, J., Birmaher, B., Brent, D., Rao, U., Flynn, C., Moreci, P., et al. (1997). Schedule for affective disorders and schizophrenia for school-age children-present and lifetime version (K-SADS-PL): initial reliability and validity data. J. Am. Acad. Child Adolesc. Psychiatry 36, 980–988. doi: 10.1097/00004583-199707000-00021
Kim, S. Y. (2021). Depression in Young autistic people: a scoping review. Res. Autism Spectr. Disord. 17:101841. doi: 10.1016/j.rasd.2021.101841
Kovacs, Maria. (2011). Children’s depression inventory (CDI2): Technical manual (2nd Edn.). North Tonawanda, NY: Multi-Health Systems, Inc.
Lerner, M. D., Mazefsky, C. A., Weber, R. J., Transue, E., Siegel, M., Gadow, K. D., et al. (2018). Verbal ability and psychiatric symptoms in clinically referred inpatient and outpatient youth with ASD. J. Autism Dev. Disord. 48, 3689–3701. doi: 10.1007/s10803-017-3344-5
Leyfer, O. T., Folstein, S. E., Bacalman, S., Davis, N. O., Dinh, E., Morgan, J., et al. (2006). Comorbid psychiatric disorders in children with autism: interview development and rates of disorders. J. Autism Dev. Disord. 36, 849–861. doi: 10.1007/s10803-006-0123-0
Lovibond, S. H., and Lovibond, P. F. (1995). Depression anxiety stress scales. APA PsycTests. 1995, 335–343. doi: 10.1037/2Ft01004-000
Lyznicki, J. M., McCaffree, M. A., and Robinowitz, C. B. (2004). Childhood bullying: implications for physicians. Am. Fam. Physician 70, 1723–1730.
Mayes, T., Bernstein, I., Haley, C., Kennard, B., and Emslie, G. (2010). Psychometric properties of the Children’s depression rating scale-revised in adolescents. J. Child Adolesc. Psychopharmacol. 20, 513–516. doi: 10.1089/cap.2010.0063
Muskett, A., Capriola-Hall, N. N., Ryan Radtke, S., Factor, R., and Scarpa, A. (2019). Repetitive behaviors in autism Spectrum disorder: associations with depression and anxiety symptoms. Res. Autism Spectr. Disord. 68:101449. doi: 10.1016/j.rasd.2019.101449
Ozsivadjian, A., Hibberd, C., and Hollocks, M. J. (2014). Brief report: the use of self-report measures in Young people with autism Spectrum disorder to access symptoms of anxiety, depression and negative thoughts. J. Autism Dev. Disord. 44, 969–974. doi: 10.1007/s10803-013-1937-1
Pezzimenti, F., Han, G. T., Vasa, R. A., and Gotham, K. (2019). Depression in youth with autism Spectrum disorder. Child Adolesc. Psychiatr. Clin. N. Am. 28, 397–409. doi: 10.1016/j.chc.2019.02.009
Pilunthanakul, T., Goh, T. J., Fung, D. S. S., Sultana, R., Allen, J. C., and Sung, M. (2021). Validity of the patient health questionnaire 9-item in autistic youths: a pilot study. BMC Psychiatry 21, 1–11. doi: 10.1186/s12888-021-03556-w
Pouw, L. B. C., Rieffe, C., Stockmann, L., and Gadow, K. D. (2013). The link between emotion regulation, social functioning, and depression in boys with ASD. Res. Autism Spectr. Disord. 7, 549–556. doi: 10.1016/j.rasd.2013.01.002
Rai, D., Culpin, I., Heuvelman, H., Magnusson, C. M. K., Carpenter, P., Jones, H. J., et al. (2018). Association of Autistic Traits with Depression from Childhood to age 18 years. JAMA Psychiatry 75, 835–843. doi: 10.1001/jamapsychiatry.2018.1323
Reichow, B., Steiner, A. M., and Volkmar, F. (2013). Cochrane review: social skills groups for people aged 6 to 21 with autism Spectrum disorders (ASD). Evidence-Based Child Health 8, 266–315. doi: 10.1002/ebch.1903
Schniering, C. A., and Rapee, R. M. (2002). Development and validation of a measure of Children’s automatic thoughts: the Children’s automatic thoughts scale. Behav. Res. Ther. 40, 1091–1109. doi: 10.1016/S0005-7967(02)00022-0
Schwartzman, J. M., and Corbett, B. A. (2020). Higher depressive symptoms in early adolescents with autism Spectrum disorder by self- and parent-report compared to typically-developing peers. Res. Autism Spectr. Disord. 77:101613. doi: 10.1016/j.rasd.2020.101613
Sharp, C., Goodyer, I. M., and Croudace, T. J. (2006). The short mood and feelings questionnaire (SMFQ): a unidimensional item response theory and categorical data Factor analysis of self-report ratings from a community sample of 7-through 11-year-old children. J. Abnorm. Child Psychol. 34, 365–377. doi: 10.1007/s10802-006-9027-x
Sheehan, D. V., Sheehan, K. H., Douglas Shytle, R., Janavs, J., Bannon, Y., Rogers, J. E., et al. (2010). Reliability and validity of the Mini international neuropsychiatric interview for children and adolescents (MINI-KID). J. Clin. Psychiatry 71, 313–326. doi: 10.4088/JCP.09m05305whi
Shiffman, S., Stone, A. A., and Hufford, M. R. (2008). Ecological momentary assessment. Annu. Rev. Clin. Psychol. 4, 1–32. doi: 10.1146/annurev.clinpsy.3.022806.091415
Stewart, M. E., Barnard, L., Pearson, J., Hasan, R., and O’Brien, G. (2006). Presentation of depression in autism and Asperger syndrome. Autism 10, 103–116. doi: 10.1177/1362361306062013
Stewart, T. M., Martin, K., Fazi, M., Oldridge, J., Piper, A., and Rhodes, S. M. (2022). A systematic review of the rates of depression in autistic children and adolescents without intellectual disability. Psychol. Psychother. 95, 313–344. doi: 10.1111/papt.12366
Keywords: adolescent, assessment, autism spectrum disorder, major depressive disorder, social relationship
Citation: Mamimoué & and Gauld C (2024) The importance of social relationships in depression in autistic adolescents: a narrative-review. Front. Psychol. 15:1335882. doi: 10.3389/fpsyg.2024.1335882
Edited by:
Alessandra Maria Passarotti, University of Illinois Chicago, United StatesReviewed by:
Nicole Dargue, Griffith University, AustraliaCopyright © 2024 Mamimoué and Gauld. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Élise Mamimoué, ZWxpc2UubWFtaW1vdWVAY2h1LWx5b24uZnI=
†These authors have contributed equally to this work and share first authorship