
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol. , 05 February 2024
Sec. Quantitative Psychology and Measurement
Volume 15 - 2024 | https://doi.org/10.3389/fpsyg.2024.1289158
This article is part of the Research Topic Psychometrics in Psychiatry 2022: Adolescent and Young Adult Psychiatry View all 7 articles
 Meinou H. C. Theunissen1*
Meinou H. C. Theunissen1* Marianne S. de Wolff1
Marianne S. de Wolff1 Iris Eekhout1
Iris Eekhout1 Coryke van Vulpen2
Coryke van Vulpen2 Sijmen A. Reijneveld1,3
Sijmen A. Reijneveld1,3Aim: The Strengths and Difficulties Questionnaire self-report (SDQ-SR) is a valid instrument for detection of emotional and behavioral problems. The aim of this study was to compare the psychometric properties of the SDQ-SR for low and higher educated adolescents, and to explore its suitability.
Methods: We included 426 adolescents. We compared internal consistency for low-educated, i.e., at maximum pre-vocational secondary education, and higher educated adolescents and assessed whether the five-factor structure of the SDQ holds across educational levels. We also interviewed 24 low-educated adolescents, and 17 professionals.
Results: On most SDQ subscales the low-educated adolescents had more problematic mean scores than the higher educated adolescents. Findings on the invariance factor analyses were inconsistent, with some measures showing a bad fit of the five factor model, and this occurring relatively more for the low-educated adolescents. Professionals and adolescents reported that the SDQ included difficult wordings.
Discussion: Our findings imply that the scale structure of the SDQ-SR is slightly poorer for low educated adolescents. Given this caveat, psychometric properties of the SDQ-SR are generally sufficient for use, regardless of educational level.
About 10% to 25% of adolescents has symptoms of mental health problems, such as low self-esteem, depressive thoughts, and impulsive or maladaptive behaviors (Leaf et al., 1996; Kieling et al., 2011; UNICEF, 2020; The Lancet Regional Health-Europe, 2022). The COVID-19 pandemic has posed additional challenges to the mental health of adolescents by lock down measures and school closures, this may have increased the prevalence of mental health disorders (The Lancet Regional Health-Europe, 2022). These emotional and behavioral problems (EBPs) can negatively impact an adolescent’s development, and can result in lower educational attainment (Veldman et al., 2014), and in persistent serious mental health problems during the life course (Tremblay et al., 2005; Jaspers et al., 2012). Early identification and treatment of EBPs can improve prognosis (Geeraert et al., 2004; Cuijpers et al., 2005; Lavigne et al., 2016).
Community pediatric services play a major role in the early identification of EBPs in children and adolescents. Validated short questionnaires have been shown to improve identification (Theunissen et al., 2019). The Strengths and Difficulties Questionnaire (SDQ) is a short screening instrument widely used to identify EBPs in adolescents, including the support of early identification of EBPs in care settings (Goodman, 1997). The SDQ can be completed by adolescents themselves (aged 11–16) as well as by parents and/or teachers (for children/adolescents aged 4–16). The Self Report (SR) has been shown to be valid as tool for early identification of EBPs in adolescents in a community setting (Goodman, 2001; Muris et al., 2003; van Widenfelt et al., 2003; Van Roy et al., 2008; Kim et al., 2015; Theunissen et al., 2019).
However, an important concern from professionals using the SDQ-SR is that adolescents may not understand the questions correctly, because of the difficulty of many terms used in the SDQ-SR. This can particularly affect responses of low educated adolescents, whose literacy capacities are more limited. Evidence on this issue is lacking, as most studies on the validity of the SDQ-SR have either been performed among higher educated adolescents (Van Roy et al., 2008; Theunissen et al., 2019), or did not differentiate by educational level.
More evidence is needed to confirm that the SDQ-SR measures EBPs in the same way across educational levels. This evidence is even more vital because of the relatively high vulnerability to mental health problems of low educated adolescents (Kaptein et al., 2008; Joffe and Black, 2012). In particular it should be clear whether the SDQ-SR measures the same construct in low and higher educated adolescents. The SDQ consist of a five factor structure: emotional symptoms, conduct problems, hyperactiviy-inattention, peer problems and pro-social behavior (Goodman, 2001). This five factor structure in the SDQ SR has been confirmed in some previous studies in community settings (Koskelainen et al., 2000; van de Looij-Jansen et al., 2011), but not in other studies (Van Roy et al., 2008; Vugteveen et al., 2020). The SDQ should be measurement invariant across educational levels, to guarantee that the SDQ scores of low and higher educated adolescents refer to similar EBPs. Moreover, for optimal use both low educated adolescents and community pediatric professionals should agree on the suitability of the SDQ.
Therefore, aim of the present study was first to compare the psychometric properties of the SDQ-SR (internal consistency and scale structure) between low and higher educated adolescents, and more specifically, whether the five-factor structure of the SDQ-SR is invariant by educational levels. Second, we explored the suitability of the SDQ-SR according to low educated adolescents, and community pediatric professionals.
We obtained quantitative and qualitative (interview) data. We also obtained written informed consent for participation in the study from all participating adolescents and from parents of adolescents under the age of 16 years. Ethical approval for this study was granted by the ethics committee of the Heymans Institute for Psychological Research of the University of Groningen in the Netherlands.
For the quantitative study we obtained data about the psychometric properties from adolescents at schools, using two samples.
1. National sample: Our first sample included adolescents aged 12–17 years from a national cross-sectional norming study for an intelligence test. Data were gathered in 2016 and 2017 via public schools as part of a norming study for an intelligence test. These schools were located over the whole of the Netherlands equally distributed over rural and urban areas. The sample consisted of 426 adolescents. We included only adolescents with complete data on SDQ-SR and level of education (n = 385; 89 low- and 296 higher-educated).
2. School sample—low educated adolescents: A second sample included adolescents involved in a newly designed cross-sectional study in three public pre-vocational secondary education schools located in the middle and west of the Netherlands, in 2017 and 2018. The sample consisted of 41 low educated adolescents.
In total, 426 Dutch adolescents (130 low educated and 296 higher educated) participated.
All adolescents completed the SDQ-SR designed for the 11- to 17-year age range, either at class level or with one-on-one supervision by a test leader. The SDQ-SR consists of 25 items related to children’s strengths and difficulties. Each item is scored on a 3-point scale (0 = not true, 1 = somewhat true, and 2 = certainly true). The SDQ-SR consists of five subscales with each five items: four subscales on difficulties—Emotional symptoms, Conduct problems, Hyperactivity-inattention, and Peer problems,—and one on strengths: Pro-social behavior. An SDQ Total Difficulties Score (TDS) can be calculated by adding up the scores on the first four subscales.
Level of education was determined based on the type of school that adolescents attended and divided into two groups: low (at maximum pre-vocational secondary education) and higher educated adolescents (low general secondary education, higher general secondary education, and pre-university education); 20.9% of all adolescents in the Netherlands attend low-level education (Central Bureau of Statistics, 2021).
First, we assessed the background characteristics of the sample. Second, we assessed the psychometric properties of the SDQ-SR and compared these between low and higher educated adolescents. We computed the internal consistency (Cronbach’s alphas) of the SDQ-SR (sub)scales (an alpha of >0.70 is considered acceptable) (Streiner, 2003) and the mean values of the SDQ-SR (sub)scales. We tested differences between the two educational levels regarding mean SDQ values using independent sample T-tests. Third, we assessed whether the five-factor structure of the SDQ-SR was invariant across the two education subgroups, by performing multigroup structural equation modeling. Finally, we examined the fit between the scale structure and the observed data for each group (low educated, higher educated, and total group) with confirmatory factor analyses (CFA). The measurement invariance between the groups was evaluated by sequentially testing for invariance in the factor structure (i.e., configural invariance), invariance of the factor loadings (i.e., metric invariance), invariance of the factor intercepts (i.e., scalar invariance), and invariance of the factor intercept means (i.e., residual invariance). Measurement invariance is evaluated by testing the significance of the X2 change between two nested models sequentially and allow a CFI change of −0.01 paired with RMSE change of 0.015 (Chen, 2007). The recommended sample size for a CFA is to have at least 100 respondents per group for a multi-group CFA (Kline, 2005). In this study 130 low educated and 296 higher educated completed the SDQ-SR. For the multigroup structural equation and the CFA analyses (single group) we used the following routine measures: root mean square error of approximation (RMSEA) (approximate fit <0.08, and good fit when the RMSEA was <0.05) (Browne and Cudeck, 1993), Standardised Root Mean Residual (SRMR) (good fit for values <0.08), Tucker-Lewis index (TLI), and the Comparative Fit Index (CFI) (TLI and CFI acceptable model fit for values >0.90, and good model fit with values >0.95) (Hu and Bentler, 1999). Items with regression weights <0.30 were considered not to be a fit. Analyses were conducted with SPSS 25 and Lavaan, R Package for Structural Equation Modeling (Rosseel, 2012).
For the qualitative study we obtained data from adolescents and from community pediatric professionals.
1. Adolescent sample—low educated adolescents: The sample consisted of 24 adolescents from three pre-vocational secondary education schools.
2. Professional sample—community pediatric physicians and nurses: The second sample consisted of 17 nurses and physicians employed at six community pediatric organizations across the Netherlands. They all used the SDQ-SR as part of their initial assessment of emotional and behavioral problems among adolescents.
Adolescents were interviewed at school by a researcher. They were asked to complete the SDQ-SR out loud. Next, to assess uncertainties we used the method of cognitive debriefing (McColl et al., 2003; García, 2011) whereby adolescents report in their own words what they think to be the meaning of each item of the SDQ-SR. This method is similar to the Teach Back method that is often used in care settings (Yen and Leasure, 2019). At the end, they were asked to mention striking issues and/or difficulties experienced when completing the SDQ-SR. The researcher registered words and items of the SDQ that were perceived as difficult to understand, and reported the adolescents’ general comments about the suitability of the SDQ.
We conducted two (online) focus group interviews with community pediatric professionals (total n = 17) about the suitability of the SDQ-SR among adolescents. The interviews were chaired by a researcher. Lead questions related first to the validity of the SDQ-SR, i.e., how often adolescents’ problems were not detected (missed) using the SDQ-SR, or detected falsely. Second, questions related to the strong and weak points of the SDQ-SR. Finally, we addressed the conditions required for successful implementation of the SDQ-SR.
Table 1 shows the demographic characteristics of low and higher educated adolescents. Compared to the low-educated adolescents, the group of higher educated adolescents included relatively more older adolescents (15–17 years) and more girls. However, differences between the two subsamples with regard to adolescent gender and age were small (Cohen effect sizes w: 0.16–0.31).
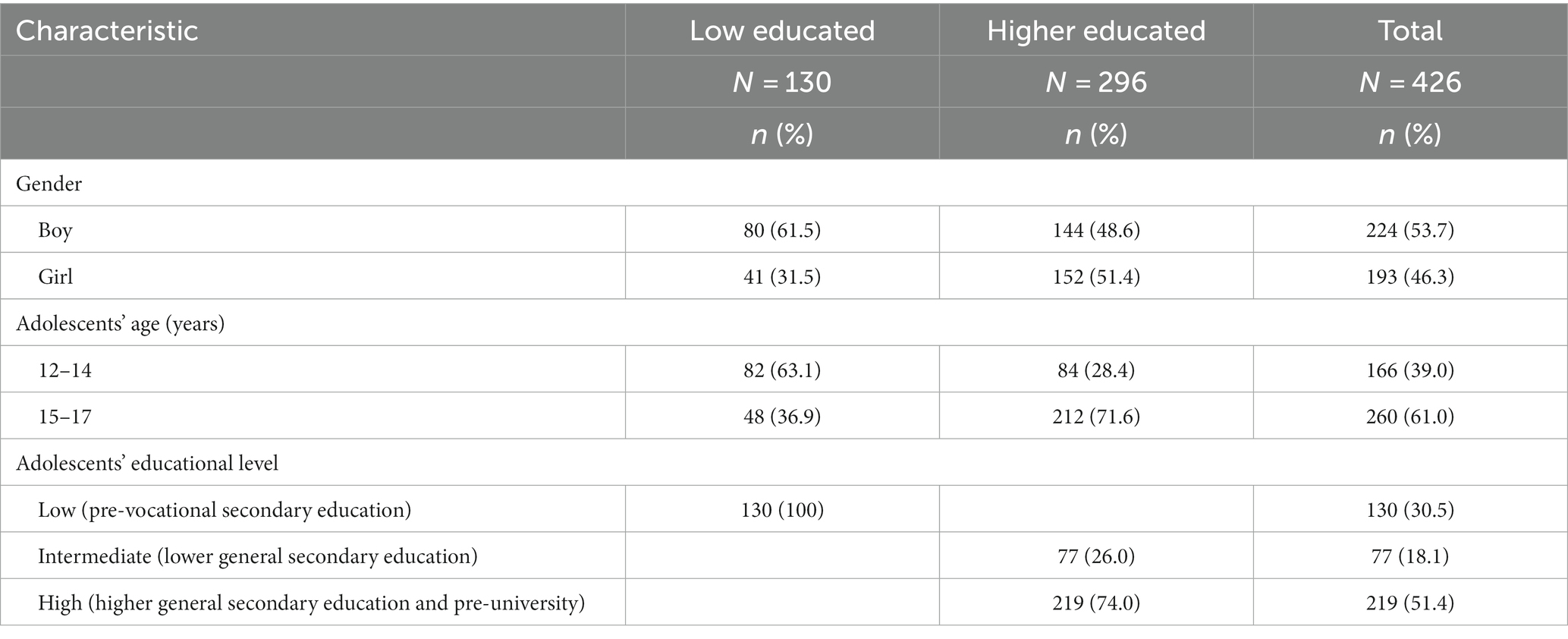
Table 1. Demographic characteristics of participating adolescents, and differences between low and higher educated adolescents.
Table 2 shows the Cronbach’s alphas and the mean scores on the SDQ-subscales and TDS for low and higher educated adolescents. The Cronbach’s alphas for the low educated adolescents varied between 0.41 and 0.57, and for the higher educated adolescents between 0.36 and 0.76, with those for total scores being very similar. Comparison of the scores on the SDQ-subscales and TDS in low and higher educated adolescents showed that low educated adolescents had significantly higher mean scores on the TDS and on the subscales Conduct problems, Hyperactivity and Peer problems, i.e., had more problems. For Prosocial we found lower mean scores for low educated adolescents than for higher educated adolescents, i.e., low-educated adolescents had fewer strengths at average.
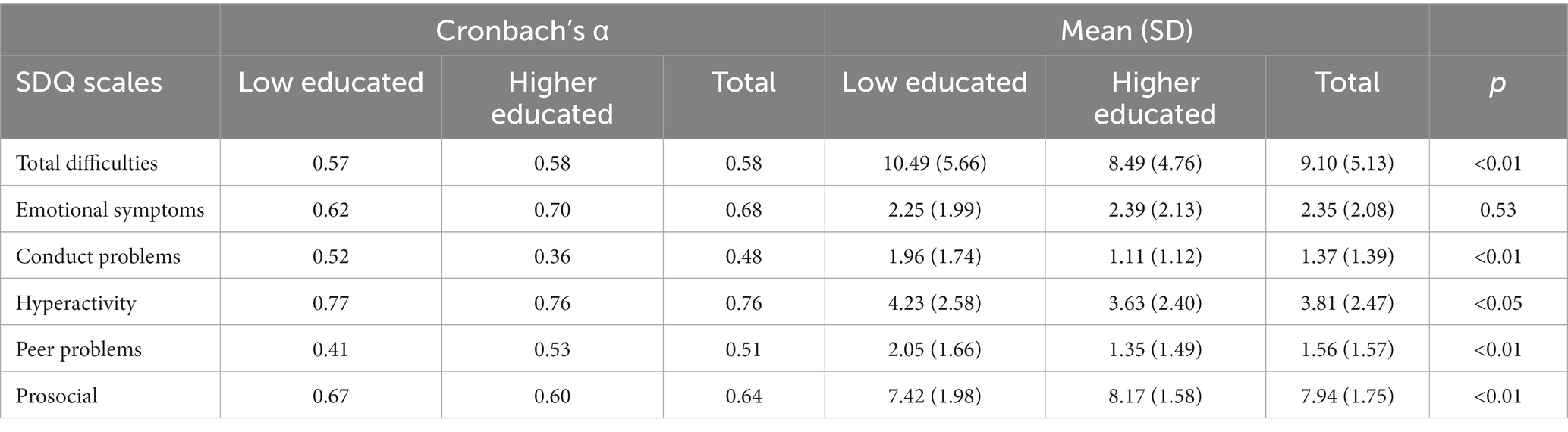
Table 2. Internal consistency, SDQ mean scores and standard deviations (SD) for SDQ subscales in adolescents with low and higher education.
Table 3 shows the multi-group and single group invariance indices of the five factor structure for the two educational groups. Results of the multi-group analyses showed the CFI and TLI to be <0.90, suggesting a bad fit (Table 3). The other goodness-of-fit indices showed adequate fit (RMSEA and SRMR <0.08). We present only the configural model (i.e., with the factor loadings were estimated freely within each education subgroup) because subsequent models impose more restrictions regarding the factor structure, and did not lead to improvement of indices. In other words, the X2 changes in the sequential models for measurement invariance, indicated significant worse fit when more parameters were fixed.
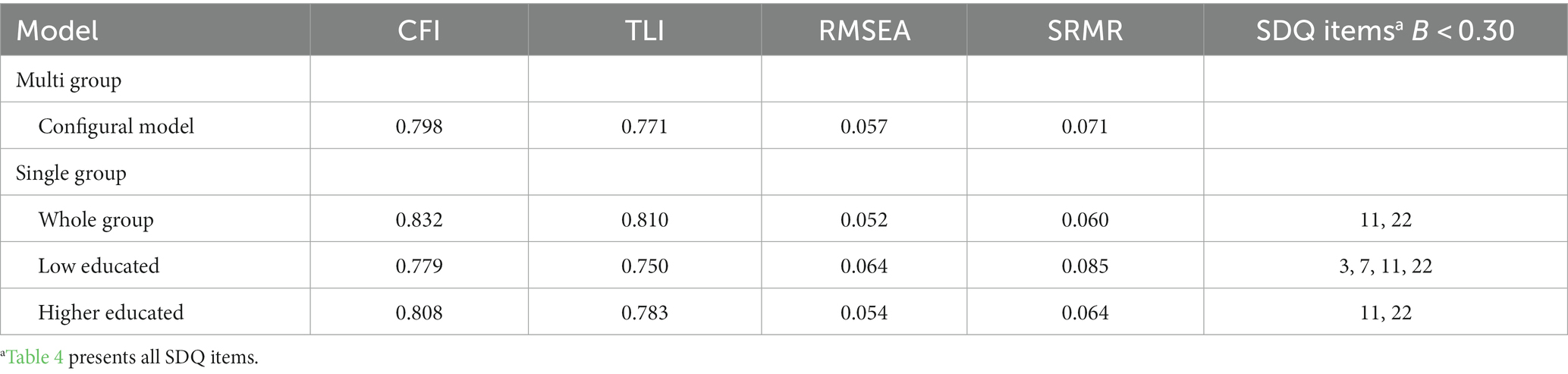
Table 3. Findings on model fit for the measurement invariance analyses of the SDQ self-report across low and higher educated adolescents.
The single group analyses CFA showed that for all groups (total, low- and higher educated adolescents) the CFI and TLI are <0.90, suggesting a bad fit. The other goodness-of-fit indices showed adequate fit of the five factor model (RMSEA and SRMR <0.08) for all groups. Except for the lower educated group, the RSMSEA approaches 0.08, but was slightly higher (0.085) indicating an inadequate fit. Furthermore, the RMSEA in the whole and higher educated group approaches the 0.05 (0.052 and 0.054, respectively), suggesting a good fit. In sum, the single (total, lower and higher educated groups) and multi-group analyses showed an (almost) acceptable fit for two routine measures of invariance (RMSEA and SRMR) and insufficient fit for two other measures (CFI and TLI). Based on these inconsistent findings, there is a slight indication of measurement variance by educational level, because a bad fit of the five factor model occurs more frequently among lower educated adolescents. However, for both groups variance indices were close to the criterion value.
Two items had regression weights <0.30 (item 11, “I have one good friend or more” and item 22, “I take things that are not mine from home, school or elsewhere”) in all groups. The low educated group also had regression weights <0.30 for item 3, “I get a lot of headaches, stomach aches or sickness” and item 7, “I usually do as I am told”.
We explored the opinions of low educated adolescents and of community pediatric physicians and nurses regarding the suitability of the SDQ-SR. Table 4 shows the difficult to understand words and items of the SDQ-SR as indicated by low educated adolescents and by professionals. According to the adolescents, seven words were particularly difficult to understand. These were Dutch translations of the words/expressions: “restless,” “angry,” “worried,” “down-hearted,” “cheating,” “pick on me” and “taking things that are not mine.” Furthermore, some adolescents reported difficulties with items comprising two sentences, such as items 1, 5, 12, 24, and 25. The general comment was that the Dutch translation of the SDQ-SR is too proper or ‘formal’, resulting in difficult language. The adolescents recommended shortening the number of words in each sentence, and using more understandable words.
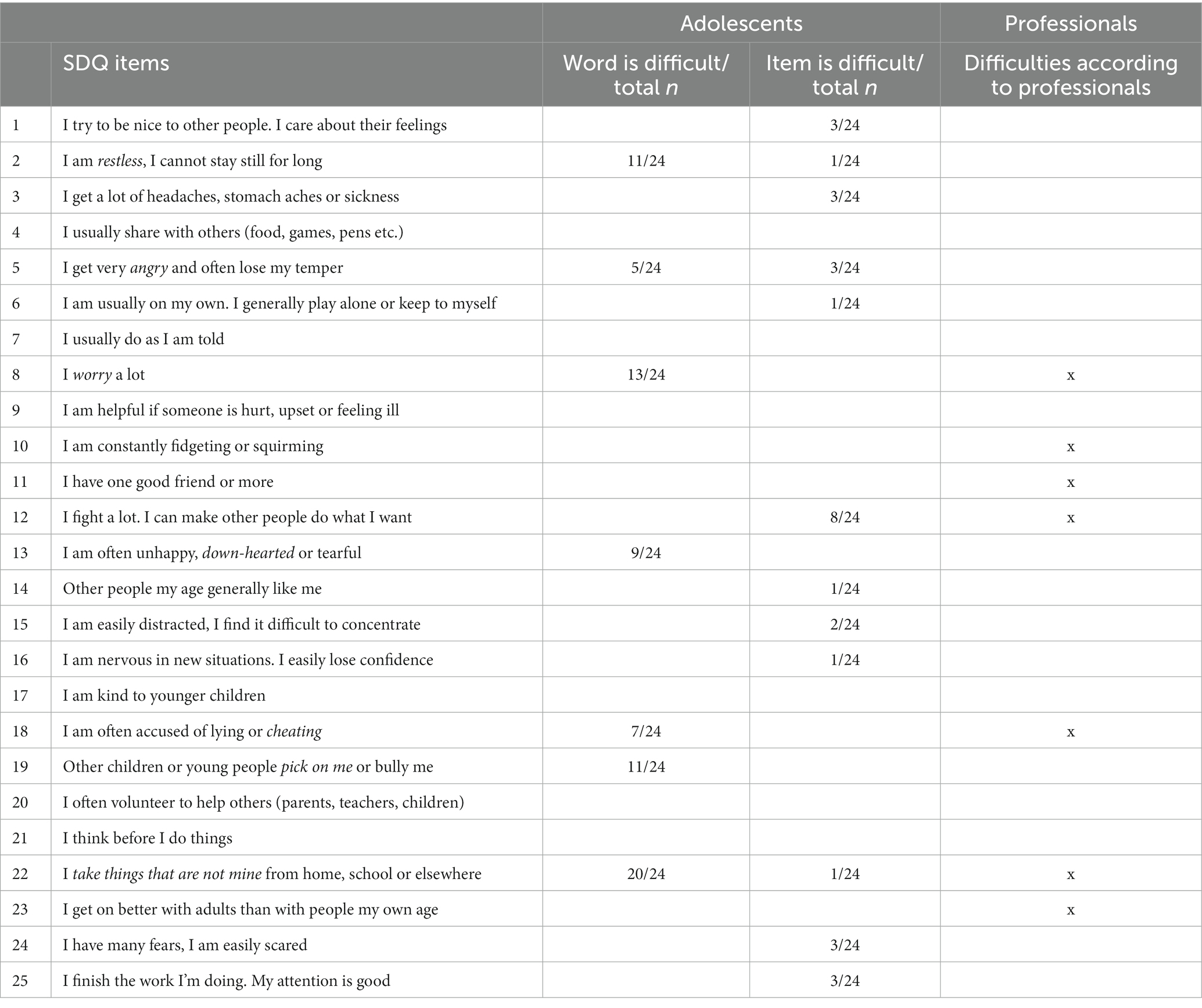
Table 4. Difficult to understand SDQ words and items as reported by low educated adolescents and community pediatric professionals.
Professionals reported having perceived the SDQ-SR to be a valid instrument; the outcome of the SDQ-SR often matched their own assessment regarding adolescents’ EBPs. However, they found that the SDQ-SR sometimes falsely identified EBPs. A reason may be that some higher educated adolescents are very critical leading to falsely elevated SDQ-SR scores. Professionals further indicated as weakness of the SDQ-SR that adolescents—regardless of their educational level—experience difficulties with items comprising two sentences. Items found difficult to understand were 8, 10, 11, 12, 18, 22, and 23. Professionals also indicated that the use of the SDQ-SR among adolescents may sometimes lead to socially desirable answers.
A strong point of the SDQ-SR reported by professionals is that it offers a good overall impression of the child’s emotional and behavioral health. More specifically, they mentioned some items to be particularly informative: items 13: ‘I am often unhappy, down-hearted or tearful’, and 19: ‘Other children or young people pick on me or bully me’. However, when asked about the conditions necessary for successful implementation of the SDQ-SR, professionals reported that although the SDQ-SR provides a good overall impression of the child’s EBPs, it includes many outdated and difficult words. They recommended to reformulate the SDQ-SR in simpler language and to provide a training for professionals on using the SDQ, e.g., via an e-learning module.
We found that the internal consistencies of the SDQ-SR subscales were comparable for low and higher educated adolescents, and that mean SDQ TDS scores were higher, i.e., more problematic, for low educated adolescents, as could be expected. For the five-factor structure of the SDQ-SR we found that some measures indicated a slightly invariance by educational level (two out of four measures), while other measures (two out of four) indicated a slightly variance by educational level. The misfit of factor structure occurred relatively more for the low educated adolescents compared to the higher educated or whole group adolescents. Regarding the suitability of the SDQ-SR, professionals perceived the SDQ-SR as a valid instrument, offering a good overview of the child’s wellbeing. However, low educated adolescents and professionals reported that the SDQ-SR includes several hard to understand words. Moreover, they reported difficulties with SDQ-SR items consisting of two sentences.
The internal consistency of the SDQ-SR was similar for low and higher educated adolescents but generally relatively poor for some subscales, and for the overall scale. The poor internal consistency of the overall scale contrasts with some previous studies reporting higher Cronbach’s alphas for the SDQ-SR TDS (i.e., 0.75), but is generally consistent with previous studies for some of the other SDQ subscales (Vogels et al., 2009; Theunissen et al., 2013, 2019). Similarly, Vugteveen et al. (2019) found internal consistencies for some SDQ-SR subscales to be insufficient, but to have adequate criterion validity despite. That is rather unexpected as consistency typically is a prerequisite for validity (Moss, 1994). An explanation may be that the various items all measure components relevant for the criterion even though not being related to one unique part. This can then yield a valid subscale even though this not consistently measures one concept.
For the five-factor structure of the SDQ-SR we found some variance by educational level; the scale structure of the SDQ-SR is slightly poorer for low educated adolescents. Nevertheless, the CFA outcomes show that the SDQ-SR performed moderately at conceptual level for both educational groups. Both educational groups have variance indices that are close to the criterion value and the SDQ-SR is therefore sufficient for use regardless educational level. The finding that the SDQ performs moderately at conceptual level is in line with other research (Goodman et al., 2010; Stone et al., 2010; Theunissen et al., 2019). These studies did not differentiate by educational level.
Professionals and low educated adolescents had concerns regarding the suitability of wordings and items of the SDQ-SR, but these findings did not align with our finding of moderate psychometric performance at the conceptual level. More specifically, the items detected by the CFA analysis as having a poor fit were other ones than those mentioned by professionals and adolescents as difficult to understand. An explanation may be that CFA identifies items that do not fit well with the proposed factor structure, which may be rather independent from the difficulty of the wording of an SDQ-SR item. This wording of the items apparently does not have a major influence on the fit with the proposed factor structure.
We further found difficulties in the Dutch translation of the SDQ-SR with some items comprising two sentences and difficult words. Such difficulties are likely to hold for other languages too, and seem to relate partially to outdating of words. For example, the SDQ-SR in English also comprises two sentences such as item 12 “I fight a lot. I can make other people do what I want”. Similarly outdated words are likely to occur in other language-version of the SDQ-SR as this has not been updated in any way since its introduction in 1997, neither in English nor in other languages. The wording of the SDQ-SR thus requires attention, for the Dutch version and also for other languages, in particular with regard to low educated adolescents.
Our study had several strengths, such as its community-based nature and its use of a combination of quantitative and qualitative data to answer the research questions. However, a limitation may be that we used a relatively small sample, of in total 426 adolescents, in the CFA analyses. However, this still exceeds the recommended minimum sample size for a CFA of 100 respondents per group for a multi-group CFA (Kline, 2005). Another limitation may be that we restricted the interviews to low educated adolescents regarding their perception of the suitability of the SDQ and did not include higher educated adolescents. Higher educated adolescents may have similar difficulties with items comprising two sentences, as indicated by the professionals that participated in this study, so this requires further study.
The scale structure of the SDQ-SR is somewhat poorer for low educated adolescents. Given this caveat, psychometric properties of the SDQ-SR are generally sufficient for use among low and higher educational groups. However, the scale structure of the SDQ-SR could be improved, for both educational groups.
Our findings also indicate a need to improve the wording of the SDQ-SR, as clearly expressed by both professionals and adolescents. Adolescents, particularly low educated ones, experience difficulties with the outdated and difficult words, and with items comprising two sentences. This study investigated the experiences difficulties with the wording of the SDQ among professionals and low-educated adolescents. Given the challenges that we found, further research is needed on this issue among higher educated adolescents. These difficulties with the wording of the SDQ are likely to hold for other languages as well, but this deserves further study.
Early detection of EBPs only has value when it is followed by early treatment in improving the prognosis for EBPs. Mental health promotion programmes in schools specifically aim to teach young people social and emotional skills such as self-awareness and resilience. An example of a potentially effective mental health programme in schools is the Social, Personal and Health Education (SPHE) with an aim to promote physical, mental, and emotional wellbeing (Dowling et al., 2019; The Lancet Regional Health-Europe, 2022). The availability and implementation of clinical guidelines are important for providing high-quality primary adolescent health care (Kocken et al., 2022).
Our study generally yielded reassuring findings regarding the applicability of the SDQ-SR for low educated adolescents compared to higher educated ones. The psychometric properties of the SDQ-SR are sufficient for use among low and higher educated adolescents, but can be improved in both groups by revising SDQ-SR’s wording as well as its scale structure.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by the Institutional Review Board (or Ethics Committee) of the Heymans Institute for Psychological Research of the University of Groningen in the Netherlands. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
MT: Writing – original draft. MW: Writing – review & editing. IE: Methodology, Writing – review & editing. CV: Writing – review & editing. SR: Writing – original draft.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The original research received financial support from the Netherlands Organization for Health Research and Development (ZonMw 729300105). No honorarium, grant, or other form of payment was given to anyone to produce the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Browne, M. W., and Cudeck, R. Alternative ways of assessing model fit. Newbury Park, CA: Sage Publications; (1993).
Central Bureau of Statistics. (2021). Secondary education; students, education type, grade, age [dataset]. Available at: https://opendata.cbs.nl/statline/#/CBS/nl/dataset/80041ned/table?ts=1617091245255 (Accessed April 18, 2021)
Chen, F. F. (2007). Sensitivity of goodness of fit indexes to lack of measurement invariance. Struct. Equ. Model. Multidiscip. J. 14, 464–504. doi: 10.1080/10705510701301834
Cuijpers, P., Van Straten, A., and Smit, F. (2005). Preventing the incidence of new cases of mental disorders: a meta-analytic review. J. Nerv. Ment. Dis. 193, 119–125. doi: 10.1097/01.nmd.0000152810.76190.a6
Dowling, K., Simpkin, A. J., and Barry, M. M. (2019). A cluster randomized-controlled trial of the mind out social and emotional learning program for disadvantaged post-primary school students. J. Youth Adolesc. 48, 1245–1263. doi: 10.1007/s10964-019-00987-3
García, A. A. (2011). Cognitive interviews to test and refine questionnaires. Public Health Nurs. 28, 444–450. doi: 10.1111/j.1525-1446.2010.00938.x
Geeraert, L., Noortgate van den, W., Grietens, H., and Onghena, P. (2004). The effects of early prevention programs for families with young children at risk for physical child abuse and neglect: a meta-analysis. Child Maltreat. 9, 277–291. doi: 10.1177/1077559504264265
Goodman, R. (1997). The strengths and difficulties questionnaire: a research note. J. Child Psychol. Psychiatry 38, 581–586. doi: 10.1111/j.1469-7610.1997.tb01545.x
Goodman, R. (2001). Psychometric properties of the strengths and difficulties questionnaire. J. Am. Acad. Child Adolesc. Psychiatry 40, 1337–1345. doi: 10.1097/00004583-200111000-00015
Goodman, A., Lamping, D. L., and Ploubidis, G. B. (2010). When to use broader internalising and externalising subscales instead of the hypothesised five subscales on the strengths and difficulties questionnaire (SDQ): data from British parents, teachers and children. J. Abnorm. Child Psychol. 38, 1179–1191. doi: 10.1007/s10802-010-9434-x
Hu, L. T., and Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 6, 1–55. doi: 10.1080/10705519909540118
Jaspers, M., de Winter, A. F., Huisman, M., Verhulst, F. C., Ormel, J., Stewart, R. E., et al. (2012). Trajectories of psychosocial problems in adolescents predicted by findings from early well-child assessments. J. Adolesc. Health 51, 475–483. doi: 10.1016/j.jadohealth.2012.02.007
Joffe, V. L., and Black, E. (2012). Social, emotional, and behavioral functioning of secondary school students with low academic and language performance: perspectives from students, teachers, and parents. Lang. Speech Hear. Serv. Sch. 43, 461–473. doi: 10.1044/0161-1461(2012/11-0088)
Kaptein, S., Jansen, D. E. M. C., Vogels, A. G. C., and Reijneveld, S. A. (2008). Mental health problems in children with intellectual disability: use of the strengths and difficulties questionnaire. J. Intellect. Disabil. Res. 52, 125–131. doi: 10.1111/j.1365-2788.2007.00978.x
Kieling, C., Baker-Henningham, H., Belfer, M., Conti, G., Ertem, I., Omigbodun, O., et al. (2011). Child and adolescent mental health worldwide: evidence for action. Lancet 378, 1515–1525. doi: 10.1016/S0140-6736(11)60827-1
Kim, M. H., Ahn, J. S., and Min, S. (2015). Psychometric properties of the self-report version of the strengths and difficulties questionnaire in Korea. Psychiatry Investig. 12, 491–499. doi: 10.4306/pi.2015.12.4.491
Kline, R. B. Principles and practice of structural equation modeling (2nd ed.). New York: Guilford; (2005).
Kocken, P. L., van Kesteren, N. M. C., van Zoonen, R., and Reijneveld, S. A. (2022). Availability and implementation of guidelines in European child primary health care: how can we improve? Eur. J. Pub. Health 32, 670–676. doi: 10.1093/eurpub/ckac114
Koskelainen, M., Sourander, A., and Kaljonen, A. (2000). The strengths and difficulties questionnaire among Finnish school-aged children and adolescents. Eur. Child Adolesc. Psychiatry 9, 277–284. doi: 10.1007/s007870070031
Lavigne, J. V., Meyers, K. M., and Feldman, M. (2016). Systematic review: classification accuracy of behavioral screening measures for use in integrated primary care settings. J. Pediatr. Psychol. 41, 1091–1109. doi: 10.1093/jpepsy/jsw049
Leaf, P. J., Alegria, M., Cohen, P., Goodman, S. H., Horwitz, S. M., Hoven, C. W., et al. (1996). Mental health service use in the community and schools: results from the four-community MECA study. Methods for the epidemiology of child and adolescent mental disorders study. J. Am. Acad. Child Adolesc. Psychiatry 35, 889–897. doi: 10.1097/00004583-199607000-00014
McColl, E., Meadows, K., and Barofsky, I. (2003). Cognitive aspects of survey methodology and quality of life assessment. Qual. Life Res. 12, 217–218. doi: 10.1023/A:1023233432721
Moss, P. A. (1994). Can there be validity without reliability. Educ. Res. 23:5. doi: 10.2307/1176218
Muris, P., Meesters, C., and van den Berg, F. (2003). The strengths and difficulties questionnaire (SDQ). Eur. Child Adolesc. Psychiatry 12, 1–8. doi: 10.1007/s00787-003-0298-2
Rosseel, Y. (2012). Lavaan: an R package for structural equation modeling. J. Stat. Softw. 48, 1–36. doi: 10.18637/jss.v048.i02
Stone, L. L., Otten, R., Engels, R. C., Vermulst, A. A., and Janssens, J. M. (2010). Psychometric properties of the parent and teacher versions of the strengths and difficulties questionnaire for 4-to 12-year-olds: a review. Clin. Child. Fam. Psychol. Rev. 13, 254–274. doi: 10.1007/s10567-010-0071-2
Streiner, D. L. (2003). Starting at the beginning: an introduction to coefficient alpha and internal consistency. J. Pers. Assess. 80, 99–103. doi: 10.1207/S15327752JPA8001_18
The Lancet Regional Health-Europe (2022). Protecting the mental health of youth. Lancet Reg Health Eur. 12:100306. doi: 10.1016/j.lanepe.2021.100306
Theunissen, M. H. C., de Wolff, M. S., and Reijneveld, S. A. (2019). The strengths and difficulties questionnaire self-report: a valid instrument for the identification of emotional and behavioral problems. Acad. Pediatr. 19, 471–476. doi: 10.1016/j.acap.2018.12.008
Theunissen, M. H. C., Vogels, A. G. C., de Wolff, M. S., and Reijneveld, S. A. (2013). Characteristics of the strengths and difficulties questionnaire in preschool children. Pediatrics 131, e446–e454. doi: 10.1542/peds.2012-0089
Tremblay, R. E., Nagin, D. S., Seguin, J. R., Zoccolillo, M., Zelazo, P. D., Boivin, M., et al. (2005). Physical aggression during early childhood: trajectories and predictors. Can. Child Adolesc. Psychiatr. Rev. 14, 3–9. doi: 10.1542/peds.114.1.e43
van de Looij-Jansen, P. M., Goedhart, A. W., de Wilde, E. J., and Treffers, P. D. (2011). Confirmatory factor analysis and factorial invariance analysis of the adolescent self-report strengths and difficulties questionnaire: how important are method effects and minor factors? Br. J. Clin. Psychol. 50, 127–144. doi: 10.1348/014466510X498174
Van Roy, B., Veenstra, M., and Clench-Aas, J. (2008). Construct validity of the five-factor strengths and difficulties questionnaire (SDQ) in pre-, early, and late adolescence. J. Child Psychol. Psychiatry 49, 1304–1312. doi: 10.1111/j.1469-7610.2008.01942.x
van Widenfelt, B. M., Goedhart, A. W., Treffers, P. D., and Goodman, R. (2003). Dutch version of the strengths and difficulties questionnaire (SDQ). Eur. Child Adolesc. Psychiatry 12, 281–289. doi: 10.1007/s00787-003-0341-3
Veldman, K., Bültmann, U., Stewart, R. E., Ormel, J., Verhulst, F. C., and Reijneveld, S. A. (2014). Mental health problems and educational attainment in adolescence: 9-year follow-up of the TRAILS study. PLoS One 9:e101751. doi: 10.1371/journal.pone.0101751
Vogels, A. G., Crone, M. R., Hoekstra, F., and Reijneveld, S. A. (2009). Comparing three short questionnaires to detect psychosocial dysfunction among primary school children: a randomized method. BMC Public Health 9:489. doi: 10.1186/1471-2458-9-489
Vugteveen, J., de Bildt, A., Serra, M., de Wolff, M. S., and Timmerman, M. E. (2020). Psychometric properties of the Dutch strengths and difficulties questionnaire (SDQ) in adolescent community and clinical populations. Assessment 27, 1476–1489. doi: 10.1177/1073191118804082
Vugteveen, J., de Bildt, A., Theunissen, M., Reijneveld, M., and Timmerman, M. (2019). Validity aspects of the strengths and difficulties questionnaire (SDQ) adolescent self-report and parent-report versions among Dutch adolescents. Assessment 28, 601–616. doi: 10.1177/1073191119858416
Keywords: SDQ, screening, adolescents, education level, community
Citation: Theunissen MHC, de Wolff MS, Eekhout I, van Vulpen C and Reijneveld SA (2024) A study on the applicability of the Strengths and Difficulties Questionnaire among low- and higher-educated adolescents. Front. Psychol. 15:1289158. doi: 10.3389/fpsyg.2024.1289158
Edited by:
Tjhin Wiguna, University of Indonesia, IndonesiaReviewed by:
Kusuma Minayati, University of Indonesia, IndonesiaCopyright © 2024 Theunissen, de Wolff, Eekhout, van Vulpen and Reijneveld. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Meinou H. C. Theunissen, bWVpbm91LnRoZXVuaXNzZW5AdG5vLm5s
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.