 Dagny Adriaenssen Johannessen
Dagny Adriaenssen Johannessen Stian Overå3
Stian Overå3- 1Department of Social Work, Child Welfare and Social Policy, OsloMet—Oslo Metropolitan University, Oslo, Norway
- 2Blue Cross East, Oslo, Norway
- 3Norwegian National Advisory Unit on Concurrent Substance Abuse and Mental Health Disorders, Innlandet Hospital Trust, Brumunddal, Norway
- 4Section for Clinical Addiction Research, Division of Mental Health and Addiction, Oslo University Hospital, Oslo, Norway
Introduction: Recovery from complex conditions such as gambling disorders (GD) often entail considerable change and require a range of adaptable interventions in the health care system. Outcomes from such avenues to change are influenced by multifarious contextual factors, which are less frequently considered in treatment outcome studies. Accordingly, this scoping review aims to map the level of evidence and explore how contextual factors influence the provision and outcomes of GD interventions.
Methods: A systematic search in selected health and social science research databases yielded a total of 2.464 unique references. The results were screened in three selection steps—titles (n = 2.464), abstracts (n = 284) and full-text (n = 104). The scoping approach was applied to provide a narrative account of the final included references (n = 34).
Results and discussion: Findings suggest that the research on GD treatment is in the early stages of development. Additionally, studies on GD interventions are characterized by cultural biases (Region and ethnicity and Gender perspectives), while three key elements are described as successful avenues to recover from GD (Competence, Perception and Utilization). In line with these findings, proposals for future research and treatment designs are made.
1 Introduction
Behavioral addictions, such as gambling disorders (GDs), are considered complex conditions (Griffiths, 2005; Langham et al., 2015). Approximately 0.1–3% of the population across European countries and around 0.1–6% worldwide experienced harmful consequences from GDs in the past year (Calado and Griffiths, 2016; Health Survey for England 2018, 2019; Pallesen et al., 2023).
Regarding GDs as addictive disorders, the classification of GD in the Diagnostic and Statistical Manual of Mental Disorders (DSM) has undergone significant changes, marking a watershed event in 1980 (Rosenthal, 2020). With the publication of the DSM-III (APA, 1980), GD was first acknowledged as a psychiatric condition. Termed “Pathological Gambling,” it was categorized under “Disorders of Impulse Control Not Elsewhere Classified.” The subsequent edition, DSM-IV (APA, 1994), retained this classification, albeit with more refined diagnostic criteria. A major paradigm shift occurred in DSM-5 (APA, 2013), where GD was reclassified as a “Substance-Related and Addictive Disorder,” reflecting contemporary research that highlighted parallels in brain function, behavioral patterns, and treatment approaches between GD and substance use disorders (Abbott, 2020; Moreira et al., 2023). Similarly, in the International Classification of Diseases (ICD), GD’s recognition as a mental health condition has evolved (Attard-Mallia, 2023). Initially classified under “Habit and Impulse Disorders” in ICD-10 (WHO, 1992), it was repositioned in ICD-11 to “Disorders Due to Addictive Behaviors,” mirroring the DSM-5’s stance (WHO, 2019). This reclassification in both the DSM and ICD marks an important development in acknowledging GD as a complex and significant mental health challenge globally (Johnstone and Regan, 2020; Shaffer et al., 2020).
Gambling disorders are complex in the sense that individuals with the disorder experience negative consequences in multiple concurrent domains of everyday life (Griffiths, 2005; Langham et al., 2015). Negative consequences include psychological distress (Petry, 2005; Lorains et al., 2011; Dowling et al., 2015), interpersonal conflict (Downs and Woolrych, 2010; Goodwin et al., 2017; Roberts et al., 2018) and social consequences, such as financial and housing problems (Grant et al., 2010c; Langham et al., 2015; Sharman et al., 2016; Swanton and Gainsbury, 2020). Studies from Europe (Winkler et al., 2017; Rogers et al., 2019; Hofmarcher et al., 2020), Australia (Productivity Commission, 2001; Victorian Competition and Efficiency Commission, 2012), and the United States (Walker and Sobel, 2016) have also proposed that GD is a public health issue in terms societal costs. Additionally, GDs are associated with various risk factors that contribute to their complex nature, such as younger age, male gender, low socioeconomic status, traumatic experiences, childhood neglect, and exposure to gambling environments (Abbott et al., 2018).
Arguably, the prevalence of GDs worldwide is modest from a population perspective. However, one person’s GD affects several of their significant others in a negative way (Goodwin et al., 2017; Järvinen-Tassopoulos, 2020; Lind et al., 2022), and GD-related repercussions have considerable societal costs (Atherton and Beynon, 2018; Hofmarcher et al., 2020; Kristensen et al., 2022). Taking these aspects together, GDs represent a major concern for individuals, families, and society.
Overcoming GDs often entails considerable personal, relational, and social change (Ashford et al., 2019; Brown and Ashford, 2019). Findings from recent studies on GDs emphasized certain traits as contributing to reduced potency of treatment, including distorted cognition (Rash and Petry, 2014; Mansueto et al., 2019; Yücel et al., 2019), impaired decision-making (Goschke, 2014; Challet-Bouju et al., 2017), impulsiveness and emotional dysregulation (Yau and Potenza, 2015; Anderson et al., 2021; Vintró-Alcaraz et al., 2021). Such traits have been identified as core maintaining factors and described as commonalities across addictive behaviors (e.g., Shaffer et al., 2004, 2018; Griffiths, 2005; Grant et al., 2010b; Mansueto et al., 2019; Yücel et al., 2019).
Most people with addiction-related problems recover without formal support from the health care system (Slutske, 2006; Kelly et al., 2017). However, some seek formal help to overcome their GD, where those with serious issues are more likely to seek formal treatment than those with less severe problems (Wieczorek and Dąbrowska, 2018; Bijker et al., 2022). These courses of change usually require individual tailoring and diversity of interventions and treatment delivery in the health care system (Clark, 2013; Kim and Hodgins, 2018) and have previously been described as complex (Pawson et al., 2004; Clark, 2013; Wong et al., 2013). Outcomes from complex avenues to change are influenced by multifarious factors along the way (Bhaskar et al., 2018; Danermark et al., 2018), including those activated through specific health care interventions. Interventions described as cognitive behavioral (CB) represents the most prevalent approaches for the treatment of GD (Chebli et al., 2016; Challet-Bouju et al., 2017; Petry et al., 2017; Abbott, 2019). These approaches include interventions such as Motivational Interview (MI) (Miller and Rollnick, 2004) and Personalized Normative Feedback (PFI) (Marchica and Derevensky, 2016). Mindfulness-based interventions (Maynard et al., 2018) and pharmacotherapy are also common treatment interventions for GDs (Bartley and Bloch, 2013). These treatment approaches aim to target factors specifically associated with the maintaining of GDs. As exemplified by Yücel et al. (2019), mindfulness or goal-directed strategies intend to readjust maintaining habits and counter compulsion, while contingency management or MI aims to target GD-related reward ideation. Moreover, previous research indicated positive outcomes from treatments addressing specific GD-related factors, including cognitive flexibility, emotional regulation (Sancho et al., 2018), self-awareness and self-management strategies (Marchica and Derevensky, 2016). GD treatment also shows beneficial results related to reduced gambling frequency, expenditure (Yakovenko et al., 2015; Maynard et al., 2018; Peter et al., 2019), and gambling urges (Christensen, 2018).
Although the findings from studies on GD treatment represent important contributions regarding whether GD-specific interventions coincide with beneficial change in certain life domains, less is known about how change is realized. Pawson et al. (2004) described specific interventions in complex avenues of change as “complex systems thrust amidst complex systems.” Accordingly, contextual factors distinctive from the place in which the interventions occur play an essential role in the eventual outcome of complex treatment avenues (Pawson et al., 2004; Bhaskar et al., 2018; Danermark et al., 2018). Contextual factors, such as policies, social equality, healthcare capacity and capability, and local environment factors, determine various aspects of health. As exemplified in previous studies, these contextual factors are associated with health outcomes, including lifestyle diseases, mortality, mental and physical health status, substance use, and criminal behavior (Bleich et al., 2012; Ciccone et al., 2014; Oakes et al., 2015; Vella et al., 2023). Considering GD treatment specifically, influencing contextual factors include political governance (e.g., regulation and access to gambling and treatment services), welfare (e.g., socioeconomic factors, accessibility and quality of support services), social factors (e.g., personal finances, leisure activities, employment, and living conditions), and individual factors (e.g., predispositions) (Abbott et al., 2018). However, these factors are less frequently considered in treatment outcome studies (Pawson et al., 2005; Richardson et al., 2018).
Research on outcomes from GD treatment has evolved gradually since the 80s when CB first was established as “best practice” (Ladouceur et al., 1994; Blaszczynski and Silove, 1995). The potency of a treatment intervention for bringing about change in the real world is termed “treatment effectiveness” (Office of Technology Assessment, 1978). That is, the effectiveness of a treatment is the expectation of a benefit when the typical practitioner provides the treatment in a typical fashion to typical patients in typical clinical settings. If the effectiveness of a new treatment is small or suppressed by the influence of unexplored mediating factors, the treatment does not achieve the status “effective.” The effectiveness relies on high internal validity, which is why mediating or moderating contextual factors are studied. The evaluation guidelines of World Health Organization (WHO, 1975) for testing and development of drugs’ medical use are often adapted. Building on these guidelines, Robey and Schultz (1998) proposed a five-phase model for outcome research, where phase I focuses on researching the therapeutic effect and, if it is present, estimating its magnitude. Phase II studies typically explore the dimensions of therapeutic effects and prepare for conducting a clinical trial. In phase III, clinical trials are conducted. Large sample sizes and conservative tolerance for type I errors are applied. In phase IV, the context is explored, and field research is typical. The fundamental task is to assess the degree to which the effect is realized in day-to-day clinical practice and to what extent different approaches are needed to meet the variations in target populations or contextual factors. Phase V typically focuses on cost–benefit analyses. Still, GD treatment is in its early stages of development and there has been extensive change—societal and technological—since the search for effective GD treatment first commenced. Additionally, compared with substance-related addictions GDs were recently recognized as standalone addictive behavioral diagnoses (APA, 2013; WHO, 2019). As a result, research on the treatment interventions for GDs has developed and increased in recent years.
The primary aim of this review is to broaden the understanding of how specific intervention features catalyze change and to guide future research directions by mapping the current evidence level for GD treatments. Additionally, it seeks to elucidate the role of contextual factors in these complex change processes. To achieve this, the review addresses two critical research questions:
1. What is the status of evidence for GD treatment?
2. How do contextual factors influence the provision and outcomes of interventions targeting emotional regulation or impulsivity in people with GDs?
2 Materials and methods
The review used a scoping approach to provide a narrative account of the initial search results. Scoping is a valid approach to map the main sources of evidence and gain insight to overarching patterns in research fields (Arksey and O'Malley, 2005; Lockwood et al., 2019). The aims of this review were explored by illuminating links between contextual factors and specific GD interventions.
The planning, procedure, and reporting of findings from the present review align with PRISMA extension for scoping reviews (PRISMA-ScR) (Tricco et al., 2018). The review was registered a priori in the International Prospective Register of Systematic Reviews (PROSPERO registration code: 282609).1
2.1 Preliminary scoping
First, the Cochrane Database of Systematic Reviews (CDSR) and Epistemonikos were searched in August 2021 for prior published reviews, and PROSPERO was searched for ongoing reviews with similar overarching aims as the present review. At the time of the search, no such reviews were identified.
As shown in Figure 1, the preliminary scoping was run in databases providing health and social science research: ASSIA (ProQuest), CINAHL (EBSCO), EMBASE (Ovid), MEDLINE (EBSCO), PsycINFO (OVID), and SocINDEX (EBSCO). The scope was conducted during September and October 2021 using a combination of relevant keywords: [(gambl* OR betti* OR wage*) AND (disorder* OR addict* OR dependen* OR excessive)) AND (treat* OR therap* OR rehab* OR recover* OR intervention*].

Figure 1. Screening and selection process.
The search results were screened to identify the intended outcomes of prevailing GD interventions, focus the aims of this review and design a main search strategy. The results from the preliminary scoping were reviewed and discussed between all authors (DJ, SO, and EA), leading to an agreement to address the underlying traits that contribute to the maintenance of GDs. These traits include factors related to GD (e.g., cognitive flexibility, decision-making, impulsiveness, or emotional regulation) that prevailing interventions are designed to address and that are central to program theory. The main search (described in the next section) was adjusted according to findings from the preliminary search by adding keywords related to emotional regulation and impulsiveness to the search string.
2.2 Main search strategy
The main search was conducted in January and February 2022 in the following databases: ASSIA (ProQuest), MEDLINE (Ovid), PsycINFO (OVID), SocINDEX (EBSCO), and PubPsych (see Figure 1). The databases were selected to target the biopsychosocial aspects of GDs (WHO, 1992, 2019; APA, 2013).
The main search string was constructed by combining relevant keywords: (gambl*) AND (problem* OR disorder* OR addict*) AND (therap* OR treatment* OR self-help OR “user driven” OR “health care”) AND (urge* OR emotion* OR affect*). The search strategy was adapted to meet the terms given by each of the respective databases. The complete search strategy is presented in the Supplementary Information SI1.
2.2.1 Inclusion criteria
The criteria of eligibility were informed by the preliminary scoping and aims of the present review. As outlined in Table 1, the inclusion criteria comprised interventions targeting emotional regulation or impulsivity (setting) in people with gambling disorder (population). The outcomes of interest were the influence of contextual factors on the provision and outcomes of such interventions.
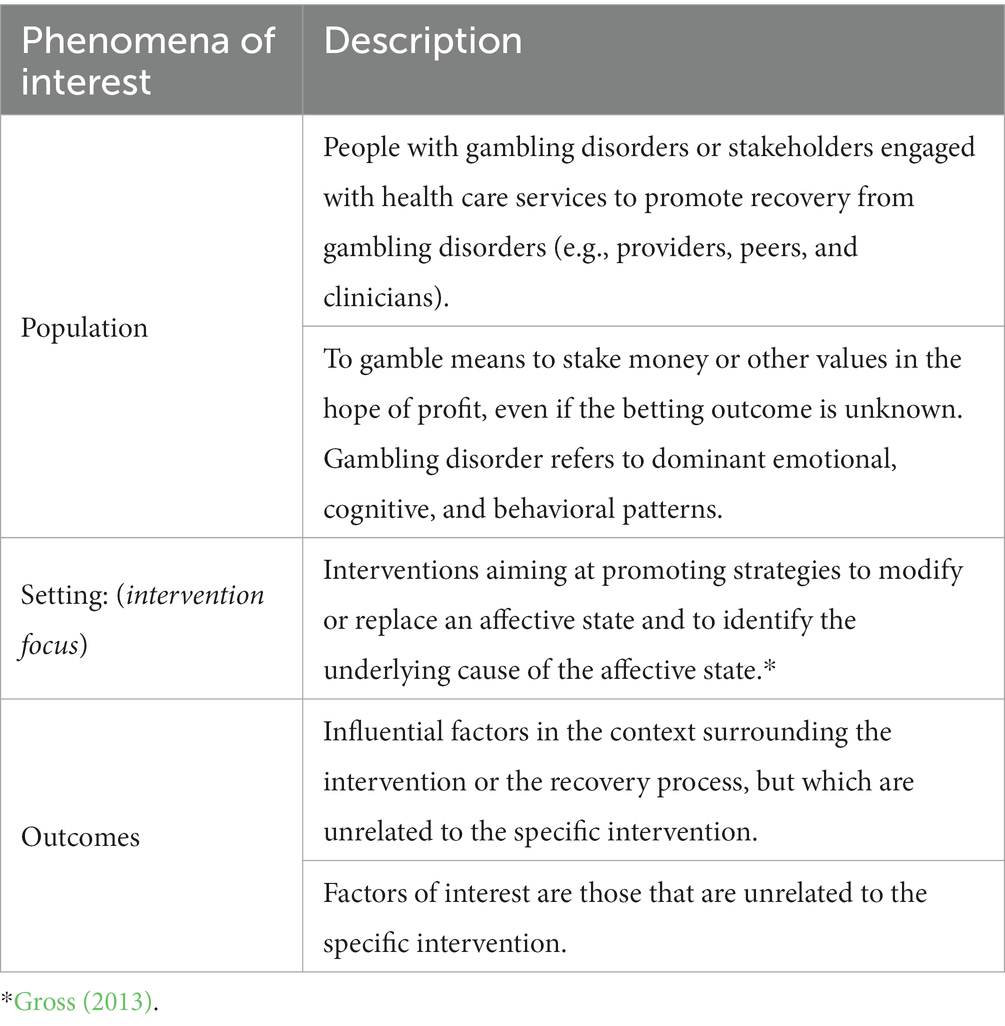
Table 1. Inclusion criteria.
Here, it is relevant to distinguish between context and setting. Context represents an element of the analytical framework and constitutes both observable and unobservable individual, intrapersonal, institutional and intra-structural surrounding traits (Pawson et al., 2004). The setting, on the other hand, refers to the characteristics of the intervention (Greenhalgh and Manzano, 2021). According to the inclusion criteria, interventions targeting emotional regulation or impulsivity were the setting of interest. Therefore, studies reporting the impact of interventions on individuals’ capacity to cope with overwhelming experiences and emotions were included during the screening process, while studies only reporting outcomes, such as gambling frequency or expenditure, were excluded. Also, studies written in other languages than English, studies designated to control for the influence of contextual factors [e.g., Randomized controlled trails (RCT)] and studies published before the year 2010 were excluded (see section 2.2.2 for description).
2.2.2 Screening and selection process
The search was planned by all authors (DJ, SO, and EA) and conducted by DJ. As shown in Figure 1, the main search yielded a total of 3.386 references, including duplicates (n = 922). The results from the main search were screened using three selection steps: (1) titles, (2) abstracts, and (3) full-text publications. The screening and selection process was conducted using Bramer et al. (2017) procedure with EndNote 20.3.
In the first selection step, author DJ applied the inclusion criteria to titles (n = 2.464) and identified these as either Include or Exclude. A subset with a random selection of 20% was screened by the two co-authors to establish reliability.
In the second selection step, authors DJ, SO, and EA applied the inclusion criteria to evaluate references identified as Include (n = 284). Diverging evaluations were resolved by consensus. Based on the authors’ preliminary perceptions during the second selection step (abstracts), further directions of the screening process were discussed and decided on. Looking at the main search results (n = 2.464), most of the identified references were published in 2010 or later (1,952 publications vs. 512 publications before 2010; see Figure 2). Thus, studies published before 2010 and studies that only included diagnostic traits, such as time or money spent for gambling, were excluded. In addition, studies designed to control for the influence of contextual factors (i.e., RCTs) were excluded. These additional eligibility criteria were applied to further screening.

Figure 2. Publications per period.
In the last selection step, all authors (DJ, SO, and EA) evaluated the included full-text publications (n = 104) and identified those as Include (n = 34) and Exclude (n = 70).
2.3 Information extraction
Relevant information was extracted from the finally included references and recorded in a predesigned data extraction form. In addition to the variables author and year of publication, information that was extracted focused on study design, phenomena of interest (e.g., study aims and objectives, operationalization’s, and definition of GD), sample characteristics (e.g., sample size, gender, age, ethnicity, and socio-demographics), intervention (e.g., type of therapeutic approach, context, and mode of delivery, intended outcomes), and findings and explanation of findings. The data extraction form is presented in the Supplementary Information SI2. Information extraction was carried out in two phases. First, DJ, SO, and EA extracted one-third of the information each from the finally included references. Second, DJ, SO, and EA reviewed the extracted information across the included references by each analyzing a set of variables.
2.3.1 Considerations in summarizing the extracted information
The aims of the current review were to map the level of evidence and explore how contextual factors influence the provision and outcomes of interventions targeting emotional regulation or impulsivity in people with GDs. Information extracted from the finally included references (n = 34) was summarized with the purpose of providing a narrative account of findings. Following Arksey and O'Malley (2005), the narrative presentation of findings had two aspects: (1) a descriptive presentation of information extracted from the individual references, and (2) a presentation of patterns across the included references, specifically relevant to the aims of the present review.
Considering the aims, the contextual factors of interest are those present in the surroundings of the place in which GD interventions are provided. While the patterns of interest relate to contextual factors with influential potential on the provision or outcomes of GD interventions. The analyses of the initial search results therefore focused on processes or activities surrounding the specific GD interventions. Contextual factors refer to elements surrounding a health care intervention. As outlined by Pawson et al. (2004) contextual factors with influential potential include individual (i.e., characteristics of the actors that are involved, such as attitudes, expertise, and demographic traits), interpersonal (i.e., characteristics of the interaction between actors that are involved, such as communication, trust, and safety), institutional (i.e., characteristics of the local environment surrounding the change process, such as culture, management, and structure), and intra-structural factors (i.e., characteristics of the broader environment surrounding the change process, such as political or economic governance, welfare system, and regulation and organization of the health care system).
3 Results
3.1 Characteristics of the included studies
The sample sizes of the studies varied widely, with a range of 1–471 participants and a median of 27.5 (see Supplementary Table 1). Of the 34 intervention studies included in our scoping review, 23 were quantitative studies, eight were qualitative studies (case studies and interview studies), and three used mixed method designs. Of the 23 quantitative studies, 17 were categorized as exploratory studies with various pre–post outcome changes. Five studies had experimental designs, including one quasi-controlled study. According to the five-phase model proposed by Robey and Schultz (1998), most of the included studies of treatment interventions for GD fell into phase I or II in that they focused on therapeutic effect or dimensions of therapeutic effect. Here, three out of the 34 studies had medical interventions (Memantine; Grant et al., 2010a; Disulfiram; Mutschler et al., 2010; Naltrexone; Ward et al., 2018). The most reported psychotherapeutic interventions were cognitive behavioral therapy (CBT, n = 10: Castren et al., 2013; Rossini-Dib et al., 2015; Tarrega et al., 2015; Boughton et al., 2016; Smith et al., 2016, 2018; Bouchard et al., 2017; Mallorqui-Bague et al., 2018; Zhuang et al., 2018; Granero et al., 2020), which was delivered either in groups or individually, either face to face (F2F) or digitally. This was followed by motivational interviewing (MI, n = 4: Grant et al., 2011; Parhami et al., 2012; Pasche et al., 2013; Stewart et al., 2016), mindfulness based interventions (n = 3: de Lisle et al., 2011; Shead et al., 2020; van der Tempel et al., 2020), dialectical behavior therapy (DBT, n = 1: Christensen et al., 2013), acceptance and commitment therapy (ACT, n = 1: Nastally and Dixon, 2012), and transcranial magnetic stimulation (TMS, n = 1: Zack et al., 2016). Desensitization techniques or exposure were a part of multiple studies but were also used exclusively in two studies (Giroux et al., 2013; van Minnen et al., 2020). Several studies did not describe the specific content of the treatment (n = 9). Four of the interventions were delivered digitally, and the rest were delivered via F2F methods.
3.2 Cultural biases
A key finding addresses cultural biases with generative potential for the access to knowledge about people with GD. Considering the aims of this review, the cultural biases constitute the influencing contextual factor, while access to culturally adapted knowledge and interventions comprise the outcome of GD interventions.
We identified two cultural biases in the selected studies related to Region and ethnicity and Gender perspectives. The first bias, Region and ethnicity, related to the lack of studies examining non-Western societies and cultural subgroups (e.g., ethnicity, religion, and Indigenous peoples). Three regions were overrepresented in the 34 included studies (see Supplementary Table 1): North America (n = 14), Europe (n = 10), and Australia (n = 7). Most studies were conducted in Canada (n = 10), Australia (n = 7), Spain (n = 5), and the United States (n = 4). In total, three studies were from countries in South America (Brazil), Africa (South Africa), and Asia (China/Hong Kong).
Many studies (n = 19) provided no information about the ethnic composition of the sample. In two studies conducted in Canada, the sample consisted solely of Caucasian males (Stewart et al., 2016) and Caucasian women (Piquette and Norman, 2013). None of these studies included cultural factors in the analyses. Several studies included different ethnic groups (Grant et al., 2011; Christensen et al., 2013; Gomes and Pascual-Leone, 2015; Rossini-Dib et al., 2015; Tarrega et al., 2015; Boughton et al., 2016; Bouchard et al., 2017; van Minnen et al., 2020). However, none of these studies addressed cultural background in the analysis of the results.
We found that cultural factors were given attention in two of the three studies conducted in non-Western countries (Pasche et al., 2013; Zhuang et al., 2018) and in a study that specifically addressed an ethnic minority group (Parhami et al., 2012). A common feature of these studies is that they examined culturally adapted programs. For example, Parhami et al. (2012) investigated the effects of an intervention specifically designed for Chinese immigrants in the United States. However, there were no cross-cultural studies or studies about indigenous peoples in the sample.2
The second bias, Gender perspectives, points to a lack of research examining the impact of gender in the intervention of gambling problems. Most of the studies had samples of both males and females (n = 21). The majority of the gender-mixed studies had more male than female participants (n = 15); five studies had more female than male participants; and one study (Smith et al., 2016) had an equal gender composition. The sample size in these studies ranged from 3 to 471 participants, with an average of 43.5. Finally, one of the articles in the sample (Smith et al., 2018) presented results from three sub studies, two of which had approximately the same gender composition and with the last consisting of only male participants. The majority of the gender-mixed studies did not examine gender differences in the analysis, with Castren et al. (2013) and Rodda et al. (2017) as the only exceptions.
Seven studies used an all-male sample (Tarrega et al., 2015; Stewart et al., 2016; Zack et al., 2016; Mallorqui-Bague et al., 2018; Zhuang et al., 2018; Granero et al., 2020; Melero Ventola et al., 2020), and three studies used an all-female sample (Piquette and Norman, 2013; Boughton et al., 2016; van der Tempel et al., 2020). In the gender-homogeneous studies, the number ranged from 1 to 192 participants, with an average of 42.6. Further, there were two single case studies, one of which involved a 48-year-old man (Mutschler et al., 2010) and one involving a 61-year-old woman (de Lisle et al., 2011).
The gender perspective was not present in any of the studies that exclusively used male samples. In comparison, two of the three studies with only female participants (Piquette and Norman, 2013; van der Tempel et al., 2020) discussed gambling behavior in relation to gender roles in society.
3.3 Three elements in avenues of recovery
An additional key finding addresses the commonalities across successful avenues for change. This finding presents contextual factors with generative potential for the provision of GD interventions. Considering the aims of this review, the structure and organization of health care services constitute the influencing contextual factor, while the three elements represent provision of GD interventions.
Across the included studies, certain features were echoed in the treatment courses identified as successful. These can be summarized in three overarching elements with relevance to recovery from GD: Competence, Perception, and Utilization. The element Competence encompasses insight, awareness or knowledge related to recovery from GD (e.g., understanding emotions, cognition, behavior, coping strategies, literacy, GD-specific factors, and the extent of available help or services). Examples from the included studies contain sharing experience with peers to gain knowledge about GD and learn efficient GD-specific coping strategies (e.g., Piquette and Norman, 2013; Boughton et al., 2016; Syvertsen et al., 2020). Additionally, cognitive flexibility (e.g., Grant et al., 2011; Mallorqui-Bague et al., 2018; Melero Ventola et al., 2020) and enhanced awareness of GD were associated with successful outcomes in terms of a reduced urge to gamble and GD treatment compliance (e.g., Castren et al., 2013; Jara-Rizzo et al., 2019).
The element Perception include opportunities to experience, test and adjust newly acquired understandings. For example, exposure to high-risk situations or distinctive emotional vulnerabilities during treatment sessions may offer opportunities to reevaluate and adjust one’s understanding of trigger traits (Pasche et al., 2013; e.g., Bouchard et al., 2017; van der Tempel et al., 2020). Additionally, testing and practicing coping strategies can provide opportunities to gain personal experiences with one’s coping strategies, and tailor the strategies accordingly (e.g., Grant et al., 2011; Boughton et al., 2016; Melero Ventola et al., 2020).
The third element, Utilization, involve possibilities to integrate new understandings and strategies to cope with triggering emotions, thoughts or experiences into real-life situations. Successful utilization was described as processes in which new coping strategies became embodied and integrated as an individual’s default responses to triggering emotions, thoughts, or situations. The participants from the study of van der Tempel et al. (2020) suggested that “more practice transferring skills from group sessions to home would have been valuable.” Further examples from the included studies are building traits such as abstinence self-efficacy (Gomes and Pascual-Leone, 2015) or confidence (Jackson et al., 2013), and daily practicing (Melero Ventola et al., 2020) or adherence to positive change (de Lisle et al., 2011).
3.4 Summary of key findings
First, the findings show that studies on GD interventions can be characterized by biases related to region, ethnicity, and gender perspectives (Cultural biases). Second, three elements have been identified in avenues to recovery (Competence, Perception, and Utilization). The key findings and relation between them are outlined in Figure 3.
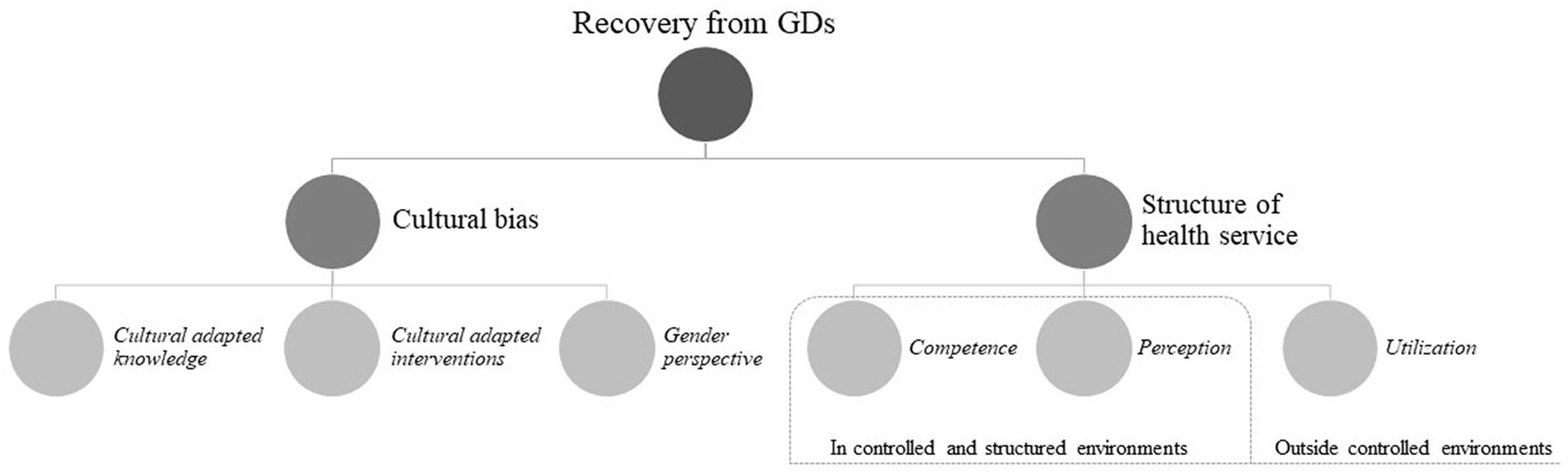
Figure 3. Key context variables for GD recovery.
4 Discussion
The aims of the present scoping review were to map the level of evidence and explore how contextual factors influence the provision and outcomes of interventions targeting emotional regulation or impulsivity in people with GDs.
The research on GD treatment is in the early stages of development, with most studies in the early phases of the five-phase model (Robey and Schultz, 1998). That is, establishing if different treatments influence outcomes and preparing for clinical trials. We propose an exploration of the deserved patterns and trends, and future research with focus on, such as different kinds of gambling, different settings, and cultural variations, for the field to move forward. On the other hand, one might argue that context is a central part of the disorder and, thus, part of the solution or treatment. In this case, one would not wait until phase IV to explore these variables but include them as covariates in early experimental studies, recommending multisite international collaboration.
The two key findings—Cultural biases and Three elements in avenues of recovery—will be discussed in the following sections.
4.1 Cultural biases in knowledge production—implications for practice
As pointed out by De Munck and Bennardo (2019), culture is a term used by many people and in varying ways. Anthropologist Clifford Geertz famously claimed that “man is an animal suspended in webs of significance he himself has spun” (Geertz, 1973). In line with Geertz, we refer to culture as a shared set of thoughts, meanings, norms, attitudes, values, and myths (see also Abbott et al., 2018).
A key finding from the present review is a lack of studies examining non-Western societies and specific cultural subgroups (e.g., ethnicity, religion, and Indigenous peoples). As pointed out by the researchers in the South African study (Pasche et al., 2013)—and still valid today—there is a lack of research on the effectiveness of treatment for GDs in low- and middle-income countries. This bias is unfortunate because research suggested that attitudes toward gambling and treatment can vary considerably by ethnicity and cultural traditions (Williams et al., 2012; Breen and Gainsbury, 2013; Clark, 2013; Kim et al., 2016; Abbott et al., 2018).
Another finding is a lack of research examining the impact of gender in the intervention of gambling problems. Although 25 out of 34 studies included both males and females in the sample, most did not explicitly address gender differences in the analysis. Overall, the gender perspective was the most present in the studies that exclusively used female samples. For example, Piquette and Norman (2013) claimed that most of the research in Western cultures has focused on the situation of American male gamblers and that there is a need for more research on intervention mechanisms that could support female problem gamblers. Similarly, van der Tempel et al. (2020) argued that gender often influences the trajectory of a GD, as several previous studies have also found (e.g., Baxter et al., 2016; Hing et al., 2016; Carneiro et al., 2020; Håkansson and Widinghoff, 2020). In line with these two studies, we argue that future research should integrate a gender perspective to a greater extent. This would allow for more insights into gender-related experiences of gambling, treatment, and GD, as well as how gender intersects with other factors (such as age, social class, and gambling type).
Health care policies and clinical practice are grounded on knowledge about the challenges they aim to solve and characteristics of the population they intend to serve (Brown and Ashford, 2019). The observed cultural bias in gambling research is most likely influenced by a complex interplay of factors. The dominance of English in academic publishing (Politzer-Ahles et al., 2020) and global research funding disparities (Hilbrecht et al., 2020) may play a pivotal role. Variations in cultural norms and gambling regulations across regions may also contribute. For instance, in areas with strict gambling laws, like many Middle Eastern countries, conducting gambling research is likely less feasible (Aldhehayan and Tamvada, 2023; Zeng et al., 2023). Additionally, in less affluent countries, pressing issues like poverty and inadequate healthcare infrastructure are likely to take precedence. A limited or biased knowledge base may have generative potential for provision and, therefore, outcomes of GD interventions, especially for populations for which there is a lack of knowledge about them (Grant and Chamberlain, 2023). To address this bias, a multifaceted approach involving inclusive funding, diverse publication channels, and international collaborations is essential (Hilbrecht et al., 2020). Such efforts could foster a more balanced understanding of GDs. The findings of the present review clearly suggest that there is a need for more attention to the role of cultural factors and gender in future gambling research.
4.2 Inside- or outside-controlled environments—implications for recovery from GD
Change-promoting interventions mostly consist of several phases or steps that may produce the intended outcomes (Pawson et al., 2004). Our findings imply that understanding the traits and behaviors that contribute to GD and having knowledge and experience with resilient coping strategies are important steps for navigating the complex processes of change. Furthermore, an equally important phase of the transformation process is gaining awareness and understanding of the personal triggers related to emotions, thoughts, or situations. These findings are in line with previous research on recovery from GD (see, e.g., Cornil et al., 2018; Oakes et al., 2020; Pickering et al., 2020). Individuals’ reactions to emotions are situational, especially in pressured circumstances, such as unexpected trigger situations (Gross, 2013; Tenenbaum et al., 2013). Trigger situations may impair cognitive function, hence influencing an individual’s capacity to regulate emotions and utilize newly gained knowledge and experiences with resilient coping strategies (Oakes et al., 2020). Emotional regulation includes strategies to modify or replace an affective state and efforts taken to identify the underlying cause of the affective state (Gross, 2013). The understanding of emotions arising in trigger situations affects the reactions to the emotion and, consequently, the actions taken to cope in such circumstances (Tenenbaum et al., 2013). Emotional reactions are influenced by both psychological (e.g., utilization of resilient coping strategies) and contextual (e.g., social support) conditions and vary depending on how triggering the specific situation is (Tenenbaum et al., 2013). In line with this, experiences with successful coping in situations that previously have triggered an unpleasant affective state may change the meaning the individual gives to similar situations (e.g., unmanageable). The new understanding of the situation (e.g., manageable) may facilitate or enable the individual’s ability to cope with similar challenges in the future (Gross, 2013), such as gambling-related trigger situations.
Different interventions are intended to initiate the features and processes described in two of the three elements. Competence contains interventions aiming to increase an individual’s insight, knowledge, and awareness (e.g., psychoeducation, cognitive therapy, conversational group therapy, etc.). Perception comprises interventions intending to enable opportunities to practice new strategies or enhance experience with emotions, thoughts, or situations (e.g., exposure therapy, virtual reality, body-based therapy, etc.). However, it seems that understanding these traits and behaviors and having knowledge of coping strategies alone may not be enough to successfully implement these strategies in the face of unexpected triggers in real-life situations. As the findings reveal, for GD patients to effectively use their knowledge and awareness, they need opportunities that enable the process where newly learned coping strategies are transformed and integrated as the standard response. Such opportunities should be formalized and integrated as services in the health care system.
The features and processes summarized earlier in Utilization are characterized by unplanned or unexpected episodes and situations where the newly gained insight or strategies are put to the test. In considering the prevailing treatment in conventional health care systems, interventions targeting traits embedded in Competence and Perception are planned according to a specific structure and progress in controlled environments (i.e., therapeutic setting, treatment facility, etc.). In contrast, features and processes covered by Utilization are not planned and occur in outside-controlled environments (i.e., in-between therapeutic sessions or after discharge from treatment). This points to a shortcoming of the formal health care system, representing a tendency that may be especially challenging for people recovering from disorders partly triggered by traits or activities that are conventional in most societies, such as gambling. Indeed, gambling is a legal activity in most countries worldwide, and the majority of players gamble with recreational motives (Calado and Griffiths, 2016; Health Survey for England 2018, 2019; Pallesen et al., 2020). Therefore, people who have experienced problems with gambling and have recovered from a GD are dependent on resilient strategies when facing unexpected trigger situations in their everyday lives.
Interventions that promote the features described in the elements Competence and Perception are well established within the formal health care system (see, e.g., Cowlishaw et al., 2012; Abbott, 2019; Bodor et al., 2021). However, treatment success extends beyond a successful outcome at the time of discharge from formal treatment. More specifically, treatment success depends not only on positive results within the treatment context, but also on successful outcomes outside of it. Our findings suggest that this requires insights and experiences gained in the treatment facility or therapeutic setting (i.e., in controlled and structured environments) become internalized and applied in real-life situations outside of the treatment context (i.e., outside-controlled environments). In line with this, we argue that these finding have structural and practical implications for stakeholders that are engaged in with GD services. Interventions promoting the processes described in Utilization may further facilitate avenues for recovery from GD, hence representing an important area for further research and a valuable contribution to the already established interventions in the formal health care system.
4.3 Limitations
Some limitations must be taken into account when considering the findings from the present study. First, this scoping review has applied an explorative approach in designing the search strategy and the analysis of the search results. However, the search strategy was informed by the findings from the preliminary search for treatment studies of prevailing GD interventions. Additionally, the search strategy and summary of the search results were driven by the intent to provide insights with relevance to today’s status in the practice field. Second, an alternative selection of databases, a different selection and combination of text words or studies written in other languages than English would generate other search results. Also, the first screening phase (titles) was primarily conducted by one author that evaluated all titles in the search result, while two authors evaluated 10% each of the titles. This entails a risk that eligible studies were not identified during the systematic search or excluded during the early screening process. However, the objective of scoping reviews is not to provide a complete overview of the existing evidence (Arksey and O'Malley, 2005; Tricco et al., 2018; Lockwood et al., 2019), and missing some studies for inclusion is the rule rather than the exception. Finally, the quality of the research design and data basis of studies were not assessed and, therefore, not considered in the analyses of the final included references. However, as shown in the discussion, the findings from this review are in line with established theories relevant to GD-related factors, as well as previous research findings with relevance to the aims of the current review.
5 Conclusion
The research field on GD treatment is in its infancy, with outcome studies mostly in the early phases of knowledge development. Findings from the current review of studies on treatment for GDs have structural and practical implications for various stakeholders that are engaged with GD research and services to promote recovery from GD. The review has uncovered context variables that must be taken into consideration when designing further research. First, there is a need to consider cultural biases and report on such variables (e.g., ethnicity and gender) to a greater extent. This may enhance knowledge about cultural variations and contribute to developing the availability of interventions adapted to specific minorities within the GD population. Second, health care services should include elements that enhance the competence related to GD and recovery from GD. Health care services should also provide the possibilities to practice newly gained strategies to cope. Finally, health care services should facilitate arenas that enable people in recovery from GDs to transform coping strategies into standard resilient responses when offering novel treatments.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material; further inquiries can be directed to the corresponding author.
Author contributions
DJ, SO, and EA contributed to conceptualization, planning the search strategy, screening and analyzing search results, and writing the manuscript. DJ conducted the systematic search and administrated the collaboration between the authors. All authors contributed to the article and approved the submitted version.
Funding
DJ’s sideline position is financed from private donor funds for a research project on gambling disorder in the non-profit organization Blue Cross Norway. The donors received quarterly progress reports of the overall project and took no other part in the research project or this review.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2024.1247152/full#supplementary-material
Footnotes
1. ^The registration was automatically rejected with the following reason: “To enable PROSPERO to focus on COVID-19 registrations during the 2020 pandemic, this registration record was automatically rejected because it did not meet the acceptance criteria.” Therefore, the record could not be edited and updated consecutively in PROSPERO, and changes made during the review process are thoroughly described throughout the section 2.
2. ^Abbott et al. (2018, p. 72) defined the term as follows: “Indigenous Peoples refers to those who have occupied lands and territories before the arrival of settler societies.”
References
Abbott, M. (2019). Professionally delivered interventions for gambling disorder. Curr. Opin. Psychiatry 32, 313–319. doi: 10.1097/YCO.0000000000000516
Abbott, M. W. (2020). The changing epidemiology of gambling disorder and gambling-related harm: public health implications. Public Health 184, 41–45. doi: 10.1016/j.puhe.2020.04.003
Abbott, M., Binde, P., Clark, L., Hodgins, D., Johnson, M., Manitowabi, D., et al. (2018). Conceptual Framework of Harmful Gambling: An International Collaboration, Third Edition. Guelph, Ontario, Canada: Gambling Research Exchange Ontario (GREO).
Aldhehayan, A., and Tamvada, J. (2023). Religiosity and risk-taking: evidence from Islam. J. Manag. Spiritual. Relig. 20, 473–498. doi: 10.51327/AGLB1237
Anderson, A. C., Youssef, G. J., Robinson, A. H., Lubman, D. I., and Verdejo-Garcia, A. (2021). Cognitive boosting interventions for impulsivity in addiction: a systematic review and meta-analysis of cognitive training, remediation and pharmacological enhancement. Addiction 116, 3304–3319. doi: 10.1111/add.15469
APA (1980). Diagnostic and Statistical Manual of Mental Disorders. Third Edition (DSM-III). 3rd Edn. Washington, D.C: American Psychiatric Pubication.
APA (1994). Diagnostic and Statistical Manual of Mental Disorders. Fourth edition (DSM-IV). 3rd Edn. Washington, D.C: American Psychiatric Pubication.
APA (2013). Diagnostic and Statistical Manual of Mental Disorders (DSM-5®). Washington, DC; London, England: American Psychiatric Pubication.
Arksey, H., and O'Malley, L. (2005). Scoping studies: towards a methodological framework. Int. J. Soc. Res. Methodol. 8, 19–32. doi: 10.1080/1364557032000119616
Ashford, R. D., Brown, A., Brown, T., Callis, J., Cleveland, H. H., Eisenhart, E., et al. (2019). Defining and operationalizing the phenomena of recovery: a working definition from the recovery science research collaborative. Addict. Res. Theory 27, 179–188. doi: 10.1080/16066359.2018.1515352
Atherton, F., and Beynon, C. (2018). Is gambling an emerging public health issue for Wales, UK? J. Public Health 41, 858–863. doi: 10.1093/pubmed/fdy164
Attard-Mallia, T. (2023). Delving into the ICD-11: a review of the chapter on mental, behavioural or neurodevelopmental disorders. Minima Media, 63–78.
Bartley, C. A., and Bloch, M. H. (2013). Meta-analysis: pharmacological treatment of pathological gambling. Expert. Rev. Neurother. 13, 887–894. doi: 10.1586/14737175.2013.814938
Baxter, A., Salmon, C., Dufresne, K., Carasco-Lee, A., and Matheson, F. I. (2016). Gender differences in felt stigma and barriers to help-seeking for problem gambling. Addict. Behav. Rep. 3, 1–8. doi: 10.1016/j.abrep.2015.10.001
Bhaskar, R., Danermark, B., and Price, L. (2018). Interdisciplinarity and Well-Being: A Critical Realist General Theory of Interdisciplinarity. London: Routledge
Bijker, R., Booth, N., Merkouris, S. S., Dowling, N. A., and Rodda, S. N. (2022). Global prevalence of help-seeking for problem gambling: a systematic review and meta-analysis. Addiction 117, 2972–2985. doi: 10.1111/add.15952
Blaszczynski, A., and Silove, D. (1995). Cognitive and behavioral therapies for pathological gambling. J. Gambl. Stud. 11, 195–220. doi: 10.1007/BF02107115
Bleich, S. N., Jarlenski, M. P., Bell, C. N., and LaVeist, T. A. (2012). Health inequalities: trends, Progress, and policy. Annu. Rev. Public Health 33, 7–40. doi: 10.1146/annurev-publhealth-031811-124658
Bodor, D., Ricijaš, N., and Filipčić, I. (2021). Treatment of gambling disorder: review of evidence-based aspects for best practice. Curr. Opin. Psychiatry 34, 508–513. doi: 10.1097/yco.0000000000000728
Bouchard, S., Robillard, G., Giroux, I., Jacques, C., Loranger, C., St-Pierre, M., et al. (2017). Using virtual reality in the treatment of gambling disorder: the development of a new tool for cognitive behavior therapy. Front. Psychol. 8:27. doi: 10.3389/fpsyt.2017.00027
Boughton, R. R., Jindani, F., and Turner, N. E. (2016). Group treatment for women gamblers using web, teleconference and workbook: effectiveness pilot. Int. J. Ment. Heal. Addict. 14, 1074–1095. doi: 10.1007/s11469-016-9700-4
Bramer, W. M., Milic, J., and Mast, F. (2017). Reviewing retrieved references for inclusion in systematic reviews using end note. J. Med. Libr. Assoc. 105, 84–87. doi: 10.5195/jmla.2017.111
Breen, H., and Gainsbury, S. (2013). Aboriginal gambling and problem gambling: a review. Int. J. Ment. Heal. Addict. 11, 75–96. doi: 10.1007/s11469-012-9400-7
Brown, A. M., and Ashford, R. D. (2019). Recovery-informed theory: situating the subjective in the science of substance use disorder recovery. J. Recov. Sci. 1, 1–15. doi: 10.31886/jors.13.2019.38
Calado, F., and Griffiths, M. D. (2016). Problem gambling worldwide: an update and systematic review of empirical research (2000–2015). J. Behav. Addict. 5, 592–613. doi: 10.1556/2006.5.2016.073
Carneiro, E., Tavares, H., Sanches, M., Pinsky, I., Caetano, R., Zaleski, M., et al. (2020). Gender differences in gambling exposure and at-risk gambling behavior. J. Gambl. Stud. 36, 445–457. doi: 10.1007/s10899-019-09884-7
Castren, S., Pankakoski, M., Tamminen, M., Lipsanen, J., Ladouceur, R., and Lahti, T. (2013). Internet-based CBT intervention for gamblers in Finland: experiences from the field. Scand. J. Psychol. 54, 230–235. doi: 10.1111/sjop.12034
Challet-Bouju, G., Bruneau, M., Victorri-Vigneau, C., and Grall-Bronnec, M. (2017). Cognitive remediation interventions for gambling disorder: a systematic review. Front. Psychol. 8:1961. doi: 10.3389/fpsyg.2017.01961
Chebli, J. L., Blaszczynski, A., and Gainsbury, S. M. (2016). Internet-based interventions for addictive Behaviours: a systematic review. J. Gambl. Stud. 32, 1279–1304. doi: 10.1007/s10899-016-9599-5
Christensen, D. R. (2018). A review of opioid-based treatments for gambling disorder: an examination of treatment outcomes, cravings, and individual differences. Int. Gambl. Stud. 18, 286–309. doi: 10.1080/14459795.2018.1470662
Christensen, D. R., Dowling, N. A., Jackson, A. C., Brown, M., Russo, J., Francis, K. L., et al. (2013). A proof of concept for using brief dialectical behavior therapy as a treatment for problem gambling. Behav. Chang. 30, 117–137. doi: 10.1017/bec.2013.10
Ciccone, D. K., Vian, T., Maurer, L., and Bradley, E. H. (2014). Linking governance mechanisms to health outcomes: a review of the literature in low- and middle-income countries. Soc. Sci. Med. 117, 86–95. doi: 10.1016/j.socscimed.2014.07.010
Clark, A. M. (2013). What are the components of complex interventions in healthcare? Theorizing approaches to parts, powers and the whole intervention. Soc. Sci. Med. 93, 185–193. doi: 10.1016/j.socscimed.2012.03.035
Cornil, A., Lopez-Fernandez, O., Devos, G., de Timary, P., Goudriaan, A. E., and Billieux, J. (2018). Exploring gambling craving through the elaborated intrusion theory of desire: a mixed methods approach. Int. Gambl. Stud. 18, 1–21. doi: 10.1080/14459795.2017.1368686
Cowlishaw, S., Merkouris, S., Dowling, N., Anderson, C., Jackson, A., and Thomas, S. (2012). Psychological therapies for pathological and problem gambling. Cochrane Database Syst. Rev. 11. doi: 10.1002/14651858.CD008937.pub2
Danermark, B., Ekström, M., and Karlsson, J.C. (2018). Att Förklara Samhället. Lund: Studentlitteratur
de Lisle, S. M., Dowling, N. A., and Allen, J. S. (2011). Mindfulness-based cognitive therapy for problem gambling. Clin. Case Stud. 10, 210–228. doi: 10.1177/1534650111401016
De Munck, V. C., and Bennardo, G. (2019). Disciplining culture: a sociocognitive approach. Curr. Anthropol. 60, 174–193. doi: 10.1086/702470
Dowling, N. A., Cowlishaw, S., Jackson, A. C., Merkouris, S. S., Francis, K. L., and Christensen, D. R. (2015). The prevalence of comorbid personality disorders in treatment-seeking problem gamblers: a systematic review and Meta-analysis. J. Personal. Disord. 29, 735–754. doi: 10.1521/pedi_2014_28_168
Downs, C., and Woolrych, R. (2010). Gambling and debt: the hidden impacts on family and work life. Community Work Fam. 13, 311–328. doi: 10.1080/13668803.2010.488096
Giroux, I., Faucher-Gravel, A., St-Hilaire, A., Boudreault, C., Jacques, C., and Bouchard, S. (2013). Gambling exposure in virtual reality and modification of urge to gamble. Cyberpsychol. Behav. Soc. Netw. 16, 224–231. doi: 10.1089/cyber.2012.1573
Gomes, K., and Pascual-Leone, A. (2015). A resource model of change: client factors that influence problem gambling treatment outcomes. J. Gambl. Stud. 31, 1651–1669. doi: 10.1007/s10899-014-9493-y
Goodwin, B. C., Browne, M., Rockloff, M., and Rose, J. (2017). A typical problem gambler affects six others. Int. Gambl. Stud. 17, 276–289. doi: 10.1080/14459795.2017.1331252
Goschke, T. (2014). Dysfunctions of decision-making and cognitive control as transdiagnostic mechanisms of mental disorders: advances, gaps, and needs in current research. Int. J. Methods Psychiatr. Res. 23, 41–57. doi: 10.1002/mpr.1410
Granero, R., Valero-Solis, S., Fernandez-Aranda, F., Gomez-Pena, M., Moragas, L., Mena-Moreno, T., et al. (2020). Response trajectories of gambling severity after cognitive behavioral therapy in young-adult pathological gamblers. J. Behav. Addict. 9, 140–152. doi: 10.1556/2006.2020.00008
Grant, J. E., and Chamberlain, S. R. (2023). Gambling disorder in minority ethnic groups. Addict. Behav. 136:107475. doi: 10.1016/j.addbeh.2022.107475
Grant, J. E., Chamberlain, S. R., Odlaug, B. L., Potenza, M. N., and Kim, S. W. (2010a). Memantine shows promise in reducing gambling severity and cognitive inflexibility in pathological gambling: a pilot study. Psychopharmacology 212, 603–612. doi: 10.1007/s00213-010-1994-5
Grant, J. E., Donahue, C. B., Odlaug, B. L., and Kim, S. W. (2011). A 6-month follow-up of imaginal desensitization plus motivational interviewing in the treatment of pathological gambling. Ann. Clin. Psychiatry 23, 3–10.
Grant, J. E., Potenza, M. N., Weinstein, A., and Gorelick, D. A. (2010b). Introduction to behavioral addictions. Am. J. Drug Alcohol Abuse 36, 233–241. doi: 10.3109/00952990.2010.491884
Grant, J. E., Schreiber, L., Odlaug, B. L., and Kim, S. W. (2010c). Pathologic gambling and bankruptcy. Compr. Psychiatry 51, 115–120. doi: 10.1016/j.comppsych.2009.04.002
Greenhalgh, J., and Manzano, A. (2021). Understanding ‘context’ in realist evaluation and synthesis. Int. J. Soc. Res. Methodol. 25, 583–595. doi: 10.1080/13645579.2021.1918484
Griffiths, M. (2005). A 'components' model of addiction within a biopsychosocial framework. J. Subst. Abus. 10, 191–197. doi: 10.1080/14659890500114359
Gross, J. J. (2013). “Emotion regulation: conceptual and empirical foundations” in Handbook of Emotion Regulation. ed. J. J. Gross . 2nd ed (New York, United States: Guilford Publications), 3–20.
Håkansson, A., and Widinghoff, C. (2020). Gender differences in problem gamblers in an online gambling setting. Psychol. Res. Behav. Manag. 13, 681–691. doi: 10.2147/prbm.s248540
Hilbrecht, M., Baxter, D., Abbott, M., Binde, P., Clark, L., Hodgins, D. C., et al. (2020). The conceptual framework of harmful gambling: a revised framework for understanding gambling harm. J. Behav. Addict. 9, 190–205. doi: 10.1556/2006.2020.00024
Hing, N., Russell, A., Tolchard, B., and Nower, L. (2016). Risk factors for gambling problems: an analysis by gender. J. Gambl. Stud. 32, 511–534. doi: 10.1007/s10899-015-9548-8
Hofmarcher, T., Romild, U., Spångberg, J., Persson, U., and Håkansson, A. (2020). The societal costs of problem gambling in Sweden. BMC Public Health 20:1921. doi: 10.1186/s12889-020-10008-9
Jackson, A. C., Francis, K. L., Byrne, G., and Christensen, D. R. (2013). Leisure substitution and problem gambling: report of a proof of concept group intervention. Int. J. Ment. Heal. Addict. 11, 64–74. doi: 10.1007/s11469-012-9399-9
Jara-Rizzo, M. F., Navas, J. F., Steward, T., López-Gómez, M., Jiménez-Murcia, S., Fernández-Aranda, F., et al. (2019). Impulsivity and problem awareness predict therapy compliance and dropout from treatment for gambling disorder. Adicciones 31, 147–159. doi: 10.20882/adicciones.1041
Järvinen-Tassopoulos, J. (2020). The impact of problem gambling: are there enough services available for families with children? Public Health 184, 28–32. doi: 10.1016/j.puhe.2020.03.020
Johnstone, P., and Regan, M. (2020). Gambling harm is everybody's business: a public health approach and call to action. Public Health 184, 63–66. doi: 10.1016/j.puhe.2020.06.010
Kelly, J. F., Bergman, B. G., Hoeppner, B. B., Vilsaint, C., and White, W. L. (2017). Prevalence and pathways of recovery from drug and alcohol problems in the United States population: implications for practice, research, and policy. Drug Alcohol Depend. 181, 162–169. doi: 10.1016/j.drugalcdep.2017.09.028
Kim, J., Ahlgren, M. B., Byun, J.-W., and Malek, K. (2016). Gambling motivations and superstitious beliefs: a cross-cultural study with casino customers. Int. Gambl. Stud. 16, 296–315. doi: 10.1080/14459795.2016.1182569
Kim, H. S., and Hodgins, D. C. (2018). Component model of addiction treatment: a pragmatic transdiagnostic treatment model of behavioral and substance addictions. Front. Psychol. 9:406. doi: 10.3389/fpsyt.2018.00406
Kristensen, J.H.B., Leino, T., and Pallesen, S. (2022). "Den samfunnsøkonomiske kostnaden av problemspilling i Norge." Universitetet i Bergen.
Ladouceur, R., Boisvert, J.-M., and Dumont, J. (1994). Cognitive-behavioral treatment for adolescent pathological gamblers. Behav. Modif. 18, 230–242. doi: 10.1177/01454455940182006
Langham, E., Thorne, H., Browne, M., Donaldson, P., Rose, J., and Rockloff, M. (2015). Understanding gambling related harm: a proposed definition, conceptual framework, and taxonomy of harms. BMC Public Health 16, 1–23. doi: 10.1186/s12889-016-2747-0
Lind, K., Castrén, S., Hagfors, H., and Salonen, A. H. (2022). Harm as reported by affected others: a population-based cross-sectional Finnish gambling 2019 study. Addict. Behav. 129, 1–10. doi: 10.1016/j.addbeh.2022.107263
Lockwood, C., dos Santos, K. B., and Pap, R. (2019). Practical guidance for knowledge synthesis: scoping review methods. Asian Nurs. Res. 13, 287–294. doi: 10.1016/j.anr.2019.11.002
Lorains, F. K., Cowlishaw, S., and Thomas, S. A. (2011). Prevalence of comorbid disorders in problem and pathological gambling: systematic review and meta-analysis of population surveys. Addiction 106, 490–498. doi: 10.1111/j.1360-0443.2010.03300.x
Mallorqui-Bague, N., Mestre-Bach, G., Lozano-Madrid, M., Fernandez-Aranda, F., Granero, R., Vintro-Alcazaz, C., et al. (2018). Trait impulsivity and cognitive domains involving impulsivity and compulsivity as predictors of gambling disorder treatment response. Addict. Behav. 87, 169–176. doi: 10.1016/j.addbeh.2018.07.006
Mansueto, G., Martino, F., Palmieri, S., Scaini, S., Ruggiero, G. M., Sassaroli, S., et al. (2019). Desire thinking across addictive behaviours: a systematic review and meta-analysis. Addict. Behav. 98:106018. doi: 10.1016/j.addbeh.2019.06.007
Marchica, L., and Derevensky, J. L. (2016). Examining personalized feedback interventions for gambling disorders: a systematic review. J. Behav. Addict. 5, 1–10. doi: 10.1556/2006.5.2016.006
Maynard, B. R., Wilson, A. N., Labuzienski, E., and Whiting, S. W. (2018). Mindfulness-based approaches in the treatment of disordered gambling: a systematic review and meta-analysis. Res. Soc. Work. Pract. 28, 348–362. doi: 10.1177/1049731515606977
Melero Ventola, A. R., Yela, J. R., Crego, A., and Cortes-Rodriguez, M. (2020). Effectiveness of a mindfulness-based cognitive therapy group intervention in reducing gambling-related craving. J. Evid. Psychotherap. 20, 107–134. doi: 10.24193/jebp.2020.1.7
Miller, W., and Rollnick, S. (2004). Talking oneself into change: motivational interviewing, stages of change, and therapeutic process. J. Cogn. Psychother. 18, 299–308. doi: 10.1891/088983904780944306
Moreira, D., Azeredo, A., and Dias, P. (2023). Risk factors for gambling disorder: a systematic review. J. Gambl. Stud. 39, 483–511. doi: 10.1007/s10899-023-10195-1
Mutschler, J., Buhler, M., Grosshans, M., Diehl, A., Mann, K., and Kiefer, F. (2010). Disulfiram, an option for the treatment of pathological gambling? Alcohol Alcohol. 45, 214–216. doi: 10.1093/alcalc/agp093
Nastally, B. L., and Dixon, M. R. (2012). The effect of a brief acceptance and commitment therapy intervention on the near-miss effect in problem gamblers. Psychol. Rec. 62, 677–690. doi: 10.1007/BF03395828
Oakes, J. M., Andrade, K. E., Biyoow, I. M., and Cowan, L. T. (2015). Twenty years of neighborhood effect research: an assessment. Curr. Epidemiol. Rep. 2, 80–87. doi: 10.1007/s40471-015-0035-7
Oakes, J., Pols, R., Lawn, S., and Battersby, M. (2020). The "zone": a qualitative exploratory study of an altered state of awareness in electronic gaming machine problem gambling. Int. J. Ment. Heal. Addict. 18, 177–194. doi: 10.1007/s11469-018-9976-7
Office of Technology Assessment (1978). "Assessing the efficacy and safety of medical technologies."
Pallesen, S., Mentzoni, R.A., Syvertsen, A., Kristensen, J.H., Erevik, E.K., and Morken, A.M. (2023). "Omfang av penge-og dataspillproblemer i Norge 2022." Institutt for samfunnspsykologi.
Pallesen, S., Mentzoni, R.A., Torsheim, T., Erevik, E.K., Molde, H., and Morken, A.M. (2020). "Omfang av penge-og dataspillproblemer i Norge 2019." Institutt for samfunnspsykologi.
Parhami, I., Davtian, M., Hanna, K., Calix, I., and Fong, T. W. (2012). The implementation of a telephone-delivered intervention for Asian American disordered gamblers: a pilot study. Asian Am. J. Psychol. 3, 145–159. doi: 10.1037/a0029799
Pasche, S. C., Sinclair, H., Collins, P., Pretorius, A., Grant, J. E., and Stein, D. J. (2013). The effectiveness of a cognitive-behavioral intervention for pathological gambling: a country-wide study. Ann. Clin. Psychiatry 25, 250–256.
Pawson, R., Greenhalgh, T., Harvey, G., and Walshe, K. (2004). Realist synthesis: an introduction. RMP methods paper 2/2004.
Pawson, R., Greenhalgh, T., Harvey, G., and Walshe, K. (2005). Realist review – a new method of systematic review designed for complex policy interventions. J. Health Serv. Res. Policy 10, 21–34. doi: 10.1258/1355819054308530
Peter, S. C., Brett, E. I., Suda, M. T., Leavens, E. L. S., Miller, M. B., Leffingwell, T. R., et al. (2019). A Meta-analysis of brief personalized feedback interventions for problematic gambling. J. Gambl. Stud. 35, 447–464. doi: 10.1007/s10899-018-09818-9
Petry, N. M. (2005) in Pathological Gambling: Etiology, Comorbidity, and Treatment. ed. N. M. Petry (Washington, DC: American Psychological Association), 85–115.
Petry, N. M., Ginley, M. K., and Rash, C. J. (2017). A systematic review of treatments for problem gambling. Psychol. Addict. Behav. 31, 951–961. doi: 10.1037/adb0000290
Pickering, D., Spoelma, M. J., Dawczyk, A., Gainsbury, S. M., and Blaszczynski, A. (2020). What does it mean to recover from a gambling disorder? Perspectives of gambling help service users. Addict. Res. Theory 28, 132–143. doi: 10.1080/16066359.2019.1601178
Piquette, N., and Norman, E. (2013). An all-female problem-gambling counseling treatment: perceptions of effectiveness. J. Groups Addict. Recover. 8, 51–75. doi: 10.1080/1556035X.2013.727736
Politzer-Ahles, S., Girolamo, T., and Ghali, S. (2020). Preliminary evidence of linguistic bias in academic reviewing. J. Engl. Acad. Purp. 47:100895. doi: 10.1016/j.jeap.2020.100895
Productivity Commission (2001). "Australia's gambling industries." University Library of Munich, Germany.
Rash, C. J., and Petry, N. M. (2014). Psychological treatments for gambling disorder. Psychol. Res. Behav. Manag. 7, 285–295. doi: 10.2147/PRBM.S40883
Richardson, G. B., Blount, T. N., and Hanson-Cook, B. S. (2018). Life history theory and recovery from substance use disorder. Rev. Gen. Psychol. 23, 263–274. doi: 10.1037/gpr0000173
Roberts, A., Landon, J., Sharman, S., Hakes, J., Suomi, A., and Cowlishaw, S. (2018). Gambling and physical intimate partner violence: results from the national epidemiologic survey on alcohol and related conditions (NESARC). Am. J. Addict. 27, 7–14. doi: 10.1111/ajad.12656
Robey, R. R., and Schultz, M. C. (1998). A model for conducting clinical-outcome research: an adaptation of the standard protocol for use in aphasiology. Aphasiology 12, 787–810. doi: 10.1080/02687039808249573
Rodda, S. N., Lubman, D. I., Jackson, A. C., and Dowling, N. A. (2017). Improved outcomes following a single session web-based intervention for problem gambling. J. Gambl. Stud. 33, 283–299. doi: 10.1007/s10899-016-9638-2
Rogers, R., Wardle, H., Sharp, C.A., Wood, S., Hughes, K., Davies, T.J., et al. (2019). "Gambling as a Public Health Issue in Wales." Wales: Public Health Wales NHS Trust, Bangor University.
Rosenthal, R. J. (2020). Inclusion of pathological gambling in DSM-III, its classification as a disorder of impulse control, and the role of Robert Custer. Int. Gambl. Stud. 20, 151–170. doi: 10.1080/14459795.2019.1638432
Rossini-Dib, D., Fuentes, D., and Tavares, H. (2015). A naturalistic study of recovering gamblers: what gets better and when they get better. Psychiatry Res. 227, 17–26. doi: 10.1016/j.psychres.2015.03.003
Sancho, M., De Gracia, M., Rodríguez, R. C., Mallorquí-Bagué, N., Sánchez-González, J., Trujols, J., et al. (2018). Mindfulness-based interventions for the treatment of substance and behavioral addictions: a systematic review. Front. Psychol. 9:95. doi: 10.3389/fpsyt.2018.00095
Shaffer, H., Blaszczynski, A., and Ladouceur, R. (2020). Gambling control and public health: Let’s be honest. Int. J. Ment. Heal. Addict. 18, 819–824. doi: 10.1007/s11469-020-00240-0
Shaffer, H. J., LaPlante, D. A., LaBrie, R. A., Kidman, R. C., Donato, A. N., and Stanton, M. V. (2004). Toward a syndrome model of addiction: multiple expressions, common etiology. Harv. Rev. Psychiatry 12, 367–374. doi: 10.1080/10673220490905705
Shaffer, H. J., Tom, M. A., Wiley, R. C., Wong, M. F. Y., Chan, E. M. L., Cheng, G. L. F., et al. (2018). Using the syndrome model of addiction: a preliminary consideration of psychological states and traits. Int. J. Ment. Heal. Addict. 16, 1373–1393. doi: 10.1007/s11469-018-9952-2
Sharman, S., Dreyer, J., Clark, L., and Bowden-Jones, H. (2016). Down and out in London: addictive behaviors in homelessness. J. Behav. Addict. 5, 318–324. doi: 10.1556/2006.5.2016.037
Shead, N. W., Champod, A. S., and Mac Donald, A. (2020). Effect of a brief meditation intervention on gambling cravings and rates of delay discounting. Int. J. Ment. Heal. Addict. 18, 1247–1263. doi: 10.1007/s11469-019-00133-x
Slutske, W. S. (2006). Natural recovery and treatment-seeking in pathological gambling: results of two U.S. National Surveys. Am. J. Psychiatry 163, 297–302. doi: 10.1176/appi.ajp.163.2.297
Smith, D. P., Fairweather-Schmidt, A. K., Harvey, P. W., and Battersby, M. W. (2018). How does routinely delivered cognitive-behavioural therapy for gambling disorder compare to "gold standard" clinical trial? Clin. Psychol. Psychother. 25, 302–310. doi: 10.1002/cpp.2163
Smith, D., Pols, R., Lavis, T., Battersby, M., and Harvey, P. (2016). Experiences and perceptions of problem gamblers on cognitive and exposure therapies when taking part in a randomised controlled trial: a qualitative study. J. Gambl. Stud. 32, 1243–1260. doi: 10.1007/s10899-015-9589-z
Stewart, M. J., Mac Nevin, P. L. D., Hodgins, D. C., Barrett, S. P., Swansburg, J., and Stewart, S. H. (2016). Motivation-matched approach to the treatment of problem gambling: a case series pilot study. J. Gambl. Issues 33, 124–147. doi: 10.4309/jgi.2016.33.8
Swanton, T. B., and Gainsbury, S. M. (2020). Gambling-related consumer credit use and debt problems: a brief review. Curr. Opin. Behav. Sci. 31, 21–31. doi: 10.1016/j.cobeha.2019.09.002
Syvertsen, A., Eilin, K. E., Rune Aune, M., and Pallesen, S. (2020). Gambling addiction Norway – experiences among members of a Norwegian self-help group for problem gambling. Int. Gambl. Stud. 20, 246–261. doi: 10.1080/14459795.2020.1722200
Tarrega, S., Castro-Carreras, L., Fernandez-Aranda, F., Granero, R., Giner-Bartolome, C., Aymami, N., et al. (2015). A serious videogame as an additional therapy tool for training emotional regulation and impulsivity control in severe gambling disorder. Front. Psychol. 6:1721. doi: 10.3389/fpsyg.2015.01721
Tenenbaum, G., Basevitch, I., Gershgoren, L., and Filho, E. (2013). Emotions–decision-making in sport: theoretical conceptualization and experimental evidence. Int. J. Sport Exer. Psychol. 11, 151–168. doi: 10.1080/1612197X.2013.773687
Tricco, A. C., Lillie, E., Zarin, W., O'Brien, K. K., Colquhoun, H., Levac, D., et al. (2018). PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann. Intern. Med. 169, 467–473. doi: 10.7326/M18-0850
van der Tempel, J., McDermott, K., Niepage, M., Afifi, T. O., McMain, S., Jindani, F., et al. (2020). Examining the effects of mindfulness practice and trait mindfulness on gambling symptoms in women with gambling disorder: a feasibility study. Int. Gambl. Stud. 20, 114–134. doi: 10.1080/14459795.2019.1686766
van Minnen, M., Markus, W., and Blaauw, E. (2020). Addiction-focused EMDR therapy in gambling disorder: a multiple baseline study. J. EMDR Pract. Res. 14, 46–59. doi: 10.1891/1933-3196.14.1.46
Vella, S. A., Sutcliffe, J. T., Fernandez, D., Liddelow, C., Aidman, E., Teychenne, M., et al. (2023). Context matters: a review of reviews examining the effects of contextual factors in physical activity interventions on mental health and wellbeing. Ment. Health Phys. Act. 25:100520. doi: 10.1016/j.mhpa.2023.100520
Victorian Competition and Efficiency Commission (2012). "Counting the cost: Inquiry into the costs of problem gambling." State of Victoria.
Vintró-Alcaraz, C., Mestre-Bach, G., Granero, R., Gómez-Peña, M., Moragas, L., Fernández-Aranda, F., et al. (2021). Do emotion regulation and impulsivity differ according to gambling preferences in clinical samples of gamblers? Addict. Behav. 126:107176. doi: 10.1016/j.addbeh.2021.107176
Walker, D. M., and Sobel, R. S. (2016). Social and economic impacts of gambling. Curr. Addict. Rep. 3, 293–298. doi: 10.1007/s40429-016-0109-8
Ward, S., Smith, N., and Bowden-Jones, H. (2018). The use of naltrexone in pathological and problem gambling: a UK case series. J. Behav. Addict. 7, 827–833. doi: 10.1556/2006.7.2018.89
WHO (1992). International statistical classification of diseases and related health problems. World Health Organization.
WHO (2019). International statistical classification of diseases and related health problems. World Health Organization.
Wieczorek, Ł., and Dąbrowska, K. (2018). What makes people with gambling disorder undergo treatment? Patient and professional perspectives. Nordic Stud. Alcohol Drugs 35, 196–214. doi: 10.1177/1455072518772397
Williams, R., West, B., and Simpson, R. (2012). "Prevention of problem gambling: A comprehensive review of the evidence, and identified best practices."
Winkler, P., Bejdová, M., Csémy, L., and Weissová, A. (2017). Social costs of gambling in the Czech Republic 2012. J. Gambl. Stud. 33, 1293–1310. doi: 10.1007/s10899-016-9660-4
Wong, G., Greenhalgh, T., Westhorp, G., Buckingham, J., and Pawson, R. (2013). RAMESES publication standards: realist syntheses. J. Adv. Nurs. 69, 1005–1022. doi: 10.1111/jan.12095
World Health Organization (1975). WHO scientific group on guidelines for evaluation of drugs for use in man. Geneva: World Health Organization.
Yakovenko, I., Quigley, L., Hemmelgarn, B. R., Hodgins, D. C., and Ronksley, P. (2015). The efficacy of motivational interviewing for disordered gambling: systematic review and meta-analysis. Addict. Behav. 43, 72–82. doi: 10.1016/j.addbeh.2014.12.011
Yau, Y. H. C., and Potenza, M. N. (2015). Gambling disorder and other behavioral addictions: recognition and treatment. Harv. Rev. Psychiatry 23, 134–146. doi: 10.1097/HRP.0000000000000051
Yücel, M., Oldenhof, E., Ahmed, S. H., Belin, D., Billieux, J., Bowden-Jones, H., et al. (2019). A transdiagnostic dimensional approach towards a neuropsychological assessment for addiction: an international Delphi consensus study. Addiction 114, 1095–1109. doi: 10.1111/add.14424
Zack, M., Cho, S. S., Parlee, J., Jacobs, M., Li, C., Boileau, I., et al. (2016). Effects of high frequency repeated transcranial magnetic stimulation and continuous theta burst stimulation on gambling reinforcement, delay discounting, and stroop interference in men with pathological gambling. Brain Stimul. 9, 867–875. doi: 10.1016/j.brs.2016.06.003
Zeng, H., Li, X., Zhou, Z., Ma, Y., and Lv, F. (2023). Local gambling culture and corporate tax aggressiveness: a trait activation perspective on informal institutions. Manag. Decis. Econ. 44, 3166–3184. doi: 10.1002/mde.3869
Zhuang, X. Y., Wong, D. F. K., Ng, T. K., Jackson, A. C., Dowling, N. A., and Lo, H. H.-M. (2018). Evaluating the effectiveness of an integrated cognitive-Behavioural intervention (CBI) model for male problem gamblers in Hong Kong: a matched-pair comparison design. J. Gambl. Stud. 34, 969–985. doi: 10.1007/s10899-018-9747-1
Keywords: gambling disorder, treatment, recovery, context factors, scoping review
Citation: Johannessen DA, Overå S and Arnevik EA (2024) The role of contextual factors in avenues to recover from gambling disorder: a scoping review. Front. Psychol. 15:1247152. doi: 10.3389/fpsyg.2024.1247152
Edited by:
Saeed Ahmed, Saint Francis Hospital and Medical Center, United StatesReviewed by:
André Luiz Monezi Andrade, Pontifical Catholic University of Campinas, BrazilLakshit Jain, University of Connecticut Health Center, United States
Souparno Mitra, New York University, United States
Aditi Sharma, The Wright Center, United States
Amit Jagtiani, Burrell Behavioral Health, United States
Copyright © 2024 Johannessen, Overå and Arnevik. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dagny Adriaenssen Johannessen, ZGFnbnlhakBsaXZlLmNvbQ==