 Ana Carla Cepeda-Lopez1,2*
Ana Carla Cepeda-Lopez1,2* Leticia Solís Domínguez1
Leticia Solís Domínguez1 Sofía Villarreal Zambrano2
Sofía Villarreal Zambrano2 Iris Y. Garza-Rodriguez1
Iris Y. Garza-Rodriguez1 Alejandra Cortes del Valle1
Alejandra Cortes del Valle1 Angélica Quiroga-Garza3
Angélica Quiroga-Garza3- 1Tecnologico de Monterrey, Monterrey, Mexico
- 2Department of Nutrition, Universidad de Monterrey, San Pedro Garza García, Mexico
- 3Department of Psychology, Universidad de Monterrey, San Pedro Garza García, Mexico
Background: To mitigate against the possible adverse effects of stress among nurses due to the COVID-19 outbreak, we designed a 12-week mind–body based online intervention program to promote well-being and prevent stress-related disorders such as burnout. Our study aimed to compare the impact of the intervention on perception of stress, negative emotions, burnout, mindfulness, resilience, and well-being at pretest and 6 months post-intervention and to compare the effect among nurses working at two different hospitals.
Methods: We conducted an uncontrolled trial using a convenience sample of nurses working at two hospitals in Mexico: one designated to treat confirmed COVID-19 patients (COVID-hospital) and the other whose patients had a negative COVID-19 test on admission (Non COVID-hospital). The 12 week online intervention consisted of 36 mind–body based micropractices, with subjective well-being as the primary outcome. Secondary outcomes were health perception, resilience, mindfulness, negative emotions, stress, and burnout.
Results: A pretest survey was completed by 643 nurses. Of the remaining valid responses, 82% were women, with a mean age of 34.8 (SD = 8.95) years old. For the analysis two groups of nurses were sampled by cluster: a COVID-hospital group of 429 (67%) nurses, and a non-COVID Hospital group of 214 (33%) nurses. The proportion lost to follow-up was 71% at postest (n = 188) and 42% at 6 months follow-up (n = 371). At pretest, non-COVID hospital nurses had lower subjective well-being and higher burnout than their COVID hospital counterparts. At postest, non-COVID hospital nurses displayed more negative emotions than their COVID hospital peers. At 6 months post-intervention, nurses experienced improved mindfulness, reduced negative emotions and stress, but a decrease in subjective well-being and resilience. Nurses working at the non-COVID hospital had significantly higher mean scores for burnout than those working at the COVID hospital.
Conclusion: The results of our study suggest that our online mind–body interventions can help to reduce stress and negative emotions, yet the effects on subjective well-being and resilience are uncertain. Further research is needed to gain a better understanding of their potential mechanisms and the associated efforts of such online interventions.
Clinical Trial Registration: ClinicalTrials.gov, NCT05515172.
1. Introduction
Historically nurses have played a critical role in addressing the medical and psychological needs of patients during outbreaks, including coronavirus disease 2019 (COVID-19), severe acute respiratory syndrome (Shih et al., 2009), the Middle East respiratory coronavirus (Choi and Kim, 2016), zika (Wilson and Nguyen, 2017; Dran, 2018), and Ebola virus disease (Kollie et al., 2017; Raven et al., 2018). Before the COVID-19 pandemic, the World Health Organization (WHO) designated 2020 as the International Year of the Nurse and the Midwife (World Health Organization, World Health Day, 2020). The aim was to celebrate these essential healthcare professionals and bring to light the challenges often inherent in the profession to ensure they get the support they need. Nurses are the healthcare team members who spend the most time with patients and report the highest levels of job stress (World Health Organization, 2020). Research in nursing practice during the past decade has shown that long work hours, dealing with pain, loss, and emotional suffering, caring for dying patients and providing support to families is not new nor only due to the COVID-19 pandemic (Lazarus and Folkman, 1984; Andolhe et al., 2015). Facing this critical situation, made nurses more susceptible to distress and burnout (Raudenská et al., 2020).
As the impact of the COVID-19 outbreak began to manifest on patients and healthcare systems, nurses across the world were asked to do the unthinkable, pushing body and mind to the limit (Maben and Bridges, 2020). During this time nurses worldwide were required to work recurrent long hours and draining shifts, sometimes with limited access to personal protective equipment and evolving guidance on how to care for patients infected with the virus. Moreover, nurses faced separation from their families, stigma, fear of being infected, fear of infecting their loved ones, and pain of losing patients and colleagues (El-Hage et al., 2020; Walton et al., 2020). These extreme conditions triggered depression, anxiety, insomnia, phobia, obsessive–compulsive symptoms, and somatization symptoms in nurses worldwide (Cai et al., 2020).
Given the adverse environmental demands related to the COVID-19 outbreak there were significant concerns about nurses’ mental health and psychological adaptation worldwide (Sampaio et al., 2021). A study performed in Mexico showed that many nurses were suffering from psychological disturbances due to the COVID-19 outbreak. The authors showed that 47% of nurses reported moderate–severe traumatic distress response, 42% of nurses reported a high level of emotional exhaustion, and 42% showed moderate–severe psychological distress (Cortés-Álvarez et al., 2020). A stressful situation is one in which the demands of the setting threaten to exceed the resources of the individual (Lazarus and Folkman, 1984). Although stress responses evolved as adaptive processes, Selye observed that severe, prolonged stress responses might lead to tissue damage and disease (Selye, 1956). Environmental demands can overwhelm an individual’s resources, and therefore when high levels of stress are perceived, this can damage health leading to burnout (Montero-Marín et al., 2014). Burnout syndrome is a common psychological phenomenon among nurses characterized by the inability to cope with chronic occupational stress adapt to or protect oneself from it (Maslach et al., 2001; Johnson et al., 2018). This can be the result of too much effort in the workplace with limited opportunities for recovery.
Fundamentally, resilience refers to the ability to maintain or regain mental health successfully despite experiencing adversity (Jackson et al., 2007). Definitions have evolved as scientific knowledge has increased. New perspectives share “a focus on conceptualizing resilience at multiple levels, from the biological to the social and policy level, a focus on the dynamic nature of resilience itself as a fluid, interacting process of adaptation, and a move away from conceptualizing resilience as an individual trait” (Denckla et al., 2020). In line with this conceptualization, existential positive psychology is based on positive change brought upon by personal strength, higher appreciation of life, maintaining hope, existential courage, engagement in meaningful activities, a relationship with others, and the possibility of new opportunities in life (Wong, 2010). It also considers the negative side of life as a counterbalance to the positive (Wong, 2011; Wong, 2020). It establishes that suffering brought on by trauma, death, and disease is inevitable. Nonetheless, adversity functions as promoter of personal and spiritual development achieving post-traumatic growth. This is based on positive change brought upon by personal strength, higher appreciation of life, relationship with others, and the possibility of new opportunities in life (Magne et al., 2021).
Using mind–body interventions has been shown to be key to promoting resilience to chronic stress. Mind–body interventions cover a range of practices that trigger the “relaxation response,” a physiological state of lower sympathetic tone, increased parasympathetic tone, and lower resting heart rate, respiratory rate, and blood pressure (Benson et al., 1974; Cozzolino et al., 2020). For example, the practice of meditation has been shown to physically change regions of the brain, improving information-processing and emotion-regulation abilities (Grossman et al., 2004; Davidson and Lutz, 2008). Research on mindfulness, a psychological construct drawn from the Buddhist tradition, has identified that mindfulness-based programs designed to train individuals to cultivate mindfulness and incorporate its practice into daily life decreases rumination (Kabat-Zinn, 2003). According to Bishop et al. (2004), mindfulness encompasses two components: self-regulation of attention, and adoption of a particular orientation toward one’s experiences. Current conceptualizations point to two primary, essential elements of mindfulness: awareness and nonjudgmental acceptance of one’s moment-to-moment experience. A possible explanation for the roll of mindfulness practices in reducing reactivity to emotional stimuli and enhancing psychological well-being is that it promotes disengagement from perseverative cognitive activities and enhances attentional capacities through gains in working memory. These cognitive gains, in turn, contribute to effective emotion-regulation strategies and the development of skills to deal with negative thoughts and emotions in an adaptive and flexible manner (Bishop et al., 2004). Cognitive reappraisal (i.e., cognitive–behavioral approaches) involves reframing an emotional stimulus to change its emotional impact (Gross, 2015). It has been shown that for individuals who are struggling with acute elevations in psychological distress (the COVID-19 outbreak), reappraisal may be an important first line of defense, whereas acceptance may be beneficial in the longer term, perhaps after more immediate emotional relief has occurred (Troy et al., 2018).
A combination of physical and psychological characteristics, including body chemistry and personality factors, gives individuals the skills to be stress-resilient. Indeed, previous research has demonstrated the positive effects of resilience programs in nurses (Foster et al., 2018; Henshall et al., 2020). Resilience-based interventions, focused on healthcare workers, have emerged during the COVID-19 pandemic using online tools such as video calls and applications. Findings from this study demonstrated that resilience enhancement programs can increase nurses’ levels of resilience and confidence and improve inter-professional relationships (Weiner et al., 2020). Moreover, relaxation exercises such as yoga and qigong practices have been found to be effective in reducing chronic pain or anxiety associated with stressful experiences (Griffith et al., 2008; Zhang et al., 2021). Thus, interventions that combine physical and psychological mind–body practices could be effective in promoting physical and emotional well-being across nurses.
As part of efforts to mitigate against the adverse effects of stress among nurses due to the COVID-19 outbreak, we designed an online mind–body based intervention combining physical and psychological mind–body practices such as mindfulness to mitigate psychological distress associated with the pandemic. Therefore, the current investigation examined whether the 12 weeks mind–body based online intervention could decrease the perception of stress and improve the perception of subjective well-being in nurses working in two different setting during the first wave of the COVID-19 pandemic.
2. Materials and methods
2.1. Study design, setting, and participants
This uncontrolled trial used a convenience sample at two private hospitals in northeast Mexico: a COVID-19 designated hospital that treated confirmed COVID-19 patients (COVID-hospital) and a hospital were patients had to demonstrate a negative COVID-19 test on admission (Non COVID-hospital). Mexico declared a state of emergency due to the COVID-19 pandemic on March 30th, 2020. Our intervention was implemented from April 22nd, 2020, until July 12th, 2020 (12 weeks). During this first wave of the pandemic, we invited nurses to answer a survey and to participate in a 12 weeks-long mind–body based intervention. Figure 1 describes the overlap of the study’s intervention implementation and data acquisition time points with the COVID-19 pandemic. The inclusion criteria for the participants were as follows: (a) nurses who were currently employed in one of the selected private hospitals and (b) nurses who provided informed consent. Participation was voluntary and participants did not receive any compensation.

Figure 1. Participant Timeline.
Study participants were informed about the intervention via word of mouth. The questionnaire links were sent in an institutional email. All participants who agreed to participate in the study signed a consent form before answering the online survey with demographic questions and self-report measures to assess perception of health, subjective well-being, resilience, mindfulness, negative emotions, stress, and burnout. The completion of the online survey took approximately 25 min.
A total of 769 nurses working at two hospitals during the onset of COVID-19 in Mexico were invited to participate in an intervention and to complete a survey at three-time points. A pretest was conducted during the onset of COVID-19 in Mexico, with a response rate of 84%. Subsequently, postest measures were conducted during the peak of the first COVID-19 crisis in Mexico (de México, 2020), with a response rate of 29%. Follow-up measures were conducted 6 months later, when the first COVID-19 vaccines had been made available to health workers in the area and the lowest number of COVID-19 cases in the last year was reported (Gobierno de Nuevo Leon, 2021), with a response rate of 58%. Our analysis comparing the efficacy of the intervention was limited to participants who completed the pre-test and follow-up measures. The study variables questionnaire was designed as an online survey using Google Forms (https://www.google.com/intl/en-GB/forms/about/; Alphabet Co., Mountain View, CA, United States). The Institutional Ethical Committee of the School of Medicine of the Universidad de Monterrey approved the study (CEI-002-20191210).
2.2. Description of the online intervention
A multidisciplinary team of experts, experienced in the practice and teaching of mind–body techniques, developed a 12-week online intervention to address COVID-19-related chronic stress and promote well-being among nurses. This intervention was composed of a toolbox of well-being resources, containing 36 micro-practices. Frontline nurses were incorporated into the research team that developed the study intervention, which was an essential aspect of the project. Informal interviews were conducted with nurses to identify the most effective methods to adapt the intervention to the context. Nurse leaders provided local support by sharing micro-practices three times per week in a group setting, with the practices being done collectively. Since not all micro-practices were going to resonate with every nurse, the goal was that the nursing staff could also access the link with the toolbox of well-being resources using their personal devices (laptops/tablets/smartphones) so they could select those that they wished to engage with at any moment.
The micro-practices were delivered for 12 weeks using a web-based platform administered to nursing staff by the Nurse Manager using a WhatsApp group. Each link presented the following structure: (a) reflection on the micro-practice carried out during the previous week, (b) presentation and explanation of the role of the micro-practice on well-being, (c) a 3-min YouTube video or audio file that participants could watch or listen to, including different techniques to elicit the relaxation response such as mindfulness-based stress reduction, single-focus meditation, self-regulation exercises (i.e., yoga qi-gong), breathing practices (i.e., diaphragmatic breathing), awareness practices (attentiveness to perceptual impressions in one’s environment, as well as internal cues, such as bodily sensations, thoughts, and emotions), spirituality and reframing strategies based of existential positive psychology (realizing connections with the self, finding meaning/purpose through acceptance, courage, letting it go, maintaining calm with whatever comes, and connecting with something greater than oneself), and journaling (Figure 2). Micro-practices were designed to be quick (only required a few seconds to a few minutes to implement) and could be done solo or with others, and almost anywhere. Most of the micro-practices were linked to an existing activity, such as practicing mindfulness when using hand sanitizer. Participants that were particularly at risk for experiencing significant mental distress were identified. They were assigned to a weekly cohesion group directed by a health coach using the Zoom platform. The cohesion group served as a compassionate accompaniment to mitigate acute anguish via Psychological First Aid to increase social engagement and peer support. Additionally, nurses were offered further evaluation with psychological support at the hospital.
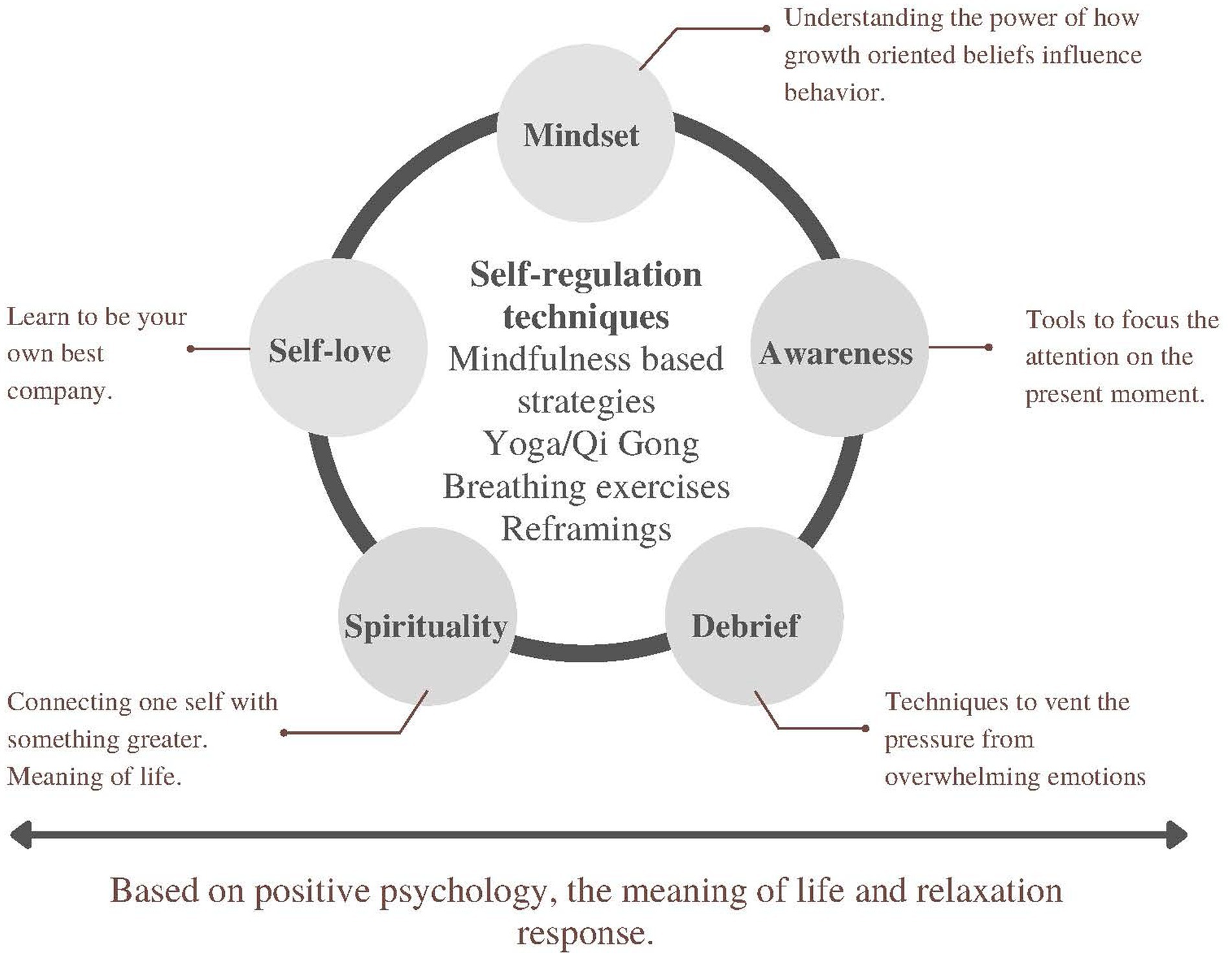
Figure 2. Description of the intervention.
2.3. Quantitative research methods
2.3.1. Demographic data
We assessed demographic data such as age, gender, marital status, hospital, department, education, and children at home/parental status.
2.3.2. Subjective well-being
We used the Spanish translation of the PERMA Profiler developed by Butler and Kern (2016) and translated by Tarragona. The PERMA Profiler measures five domains of flourishing: positive emotion, engagement, relationships, meaning, and accomplishment. Each domain has three items, with the total score from these domains constituting a measure of subjective well-being. Subjective well-being provides a helpful index on how we are doing and how well we live individually. PERMA Profiler also includes additional items that evaluate negative emotion (three items), perceived physical health (three items), and loneliness (one item, excluded from the study). The measure consists of 23 items. Questions are on an 11-point response scale ranging from 0 to 10, with the end points labeled. (Cronbach’s Alpha: Subjective well-being α = 0.886; Health α = 0.856; Negative Emotions α = 0.814).
2.3.3. Resilience
We used the Spanish version (Rodríguez-Rey et al., 2016) of the Brief Resilience Scale (BRS; Smith et al., 2008) aiming to assess individuals’ ability to recover from stressful circumstances. The scale consists of six Likert scale items that range from strongly disagree (Shih et al., 2009) to strongly agree (Raven et al., 2018; Cronbach’s α = 0.612).
2.3.4. Mindfulness, attention, and awareness
We employed the Spanish version (Barajas and Garra, 2014) of the Mindfulness Attention Awareness Scale (MAAS; Brown and Ryan, 2003) which measures characteristics of mindfulness, namely, open, or receptive awareness and attention to the present. The MAAS consists of 15 items where participants establish the frequency, they find themselves in that situation. The answers are recorded using a six-point scale that ranges from almost always (Shih et al., 2009) to almost never (Raven et al., 2018). Higher scores indicate greater mindfulness (Cronbach’s α = 0.912).
2.3.5. Perceived stress
We used the Spanish version (Brito Ortíz et al., 2020) of the Perceived Stress Scale (PSS; Cohen et al., 1983) which measures the degree to which unpredictable or unexpected situations and events in the last month were considered stressful for the participants. The PSS is a 14-item questionnaire with a five-point response scale ranging from 0 (never) to 4 (very often). A higher score indicates higher stress (Cronbach’s α = 0.819).
2.3.6. Burnout
The Burnout Clinical Subtypes Questionnaire (BCSQ-12; Montero-Marín et al., 2011) consists of 12 items equally distributed between the dimensions manifested through the differentiation of three clinical subtypes: (Shih et al., 2009) Frenetic, which is characterized by “overload” and the perception of jeopardizing one’s health to pursue worthwhile results, and is highly associated with exhaustion; (Choi and Kim, 2016) under-challenged, which is characterized by “lack of development,” defined as the perception of a lack of personal growth, together with the desire for a more rewarding occupation that better corresponds to one’s abilities, and is most strongly associated with cynicism; and (Dran, 2018) worn-out, which is characterized by “neglect,” defined as an inattentive and careless response to responsibilities, and is closely associated with inefficacy. The BCSQ-12 provides an approach to burnout, focusing on identifying the type of dissatisfaction and discomfort experienced. Participants had to state their degree of agreement with each affirmation using a seven-point Likert scale from totally disagree (Shih et al., 2009) to totally agree (World Health Organization, World Health Day, 2020; Cronbach’s Alpha: Burnout α = 0.857; Overload α = 0.803; Lack of Development α = 0.801; Negligence α = 0.768).
2.4. Statistical analysis
Computed statistical analysis and visualizations were performed using the statistical packages SPSS (Statistical Package for the Social Sciences; IBM 2017; Version 28). Internal consistency statistics were analyzed for all instruments. Data were checked for a normal distribution. For data that complied with a normal distribution, the mean and standard deviation (SD) are reported. Chi-squared test were used to assess differences in categorical demographic variables between hospitals. Independent samples t tests were used to compare COVID and non-COVID hospitals on all outcome variables at pretest, posttest, and 6-month follow-up. Due to the low response rate at posttest, when testing the intervention we compared pretest and follow-up scores only. Paired-samples t tests were used to assess changes in outcome variables from pretest to follow-up among the 371 participants who completed both surveys. Cohen’s d is reported as an effect size measure. This analysis was repeated for the COVID and non-COVID hospital subsamples. If the data were skewed, the non-parametric Wilcoxon signed-ranks test was used. The alpha level was set to 0.05 for all analyses.
3. Results
From the 769 nurses invited to participate, 643 (84%) completed the pretest survey (83% women, Mage = 34.05, SD = 9.22). For the analysis two groups of nurses were sampled by cluster: COVID-hospital group consisted of 429 (67%) nurses, and non-COVID Hospital group consisted of 214 (33%) nurses. The demographic characteristics are shown in Table 1. Age, having children at home, education, and department were significantly different between groups. At postest measurements, 188 valid responses were obtained (COVID-hospital nurses n = 144; non-COVID Hospital nurses n = 44). The proportion lost to follow-up was 71%. At 6 months post-intervention measurements, 371 valid responses were obtained (COVID-hospital nurses n = 255; non-COVID Hospital nurses n = 116). The proportion lost to follow-up was 42%.
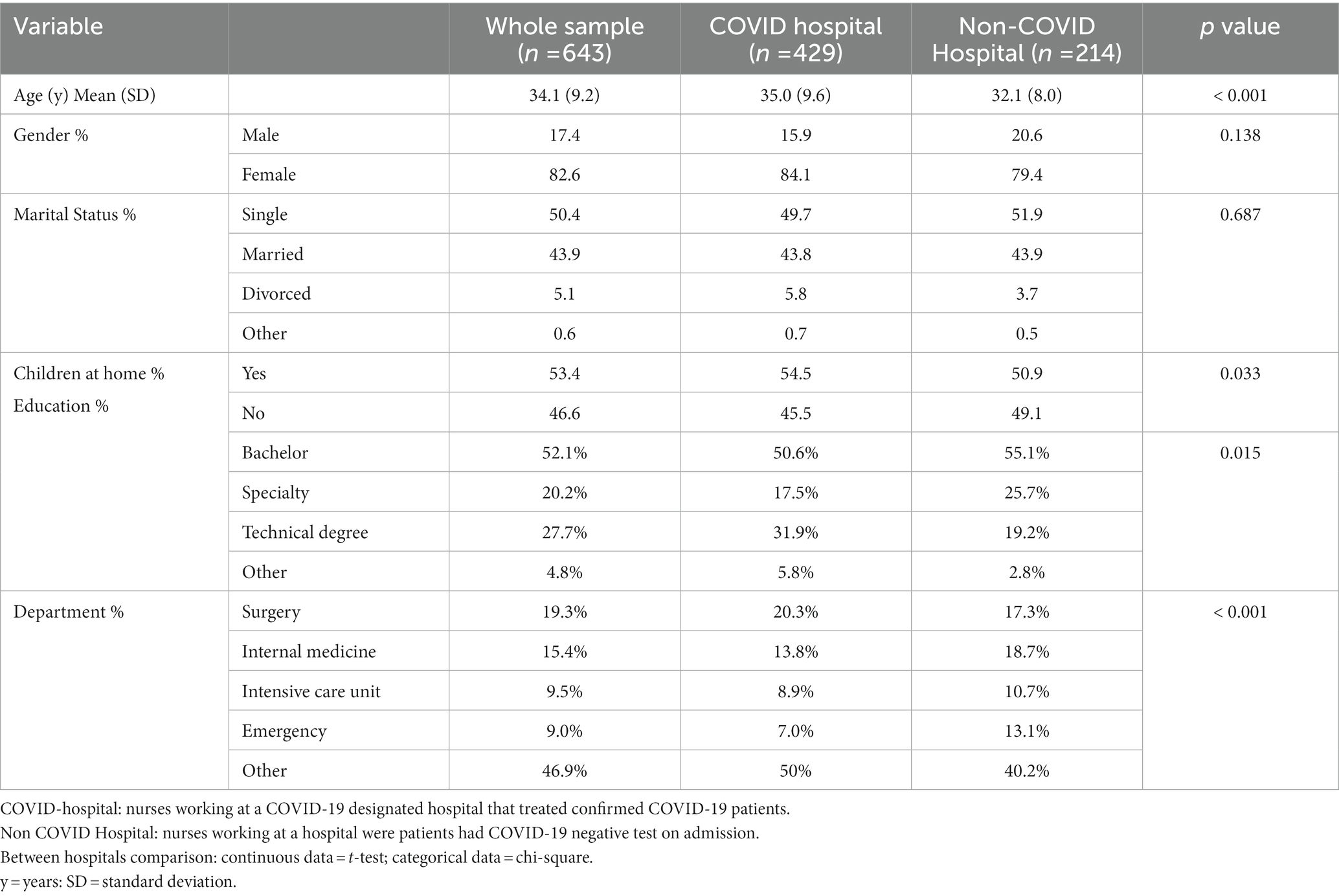
Table 1. Baseline characteristics for the whole sample and stratified by hospital.
Mean scores of perceived health, subjective well-being, resilience, mindfulness, stress, burnout, and negative emotions were assessed at different time points for the entire sample of nurses, and the results were compared between subgroups of COVID and Non-COVID Hospital nurses (Table 2). At pretest, non-COVID hospital nurses had significantly lower mean scores for subjective well-being and higher burnout scores compared to COVID hospital nurses. At postest, the mean score for negative emotions was significantly higher for non-COVID hospital nurses than for COVID hospital nurses. At 6 months follow-up, non-COVID hospital nurses had significantly higher mean scores for burnout than COVID hospital nurses.
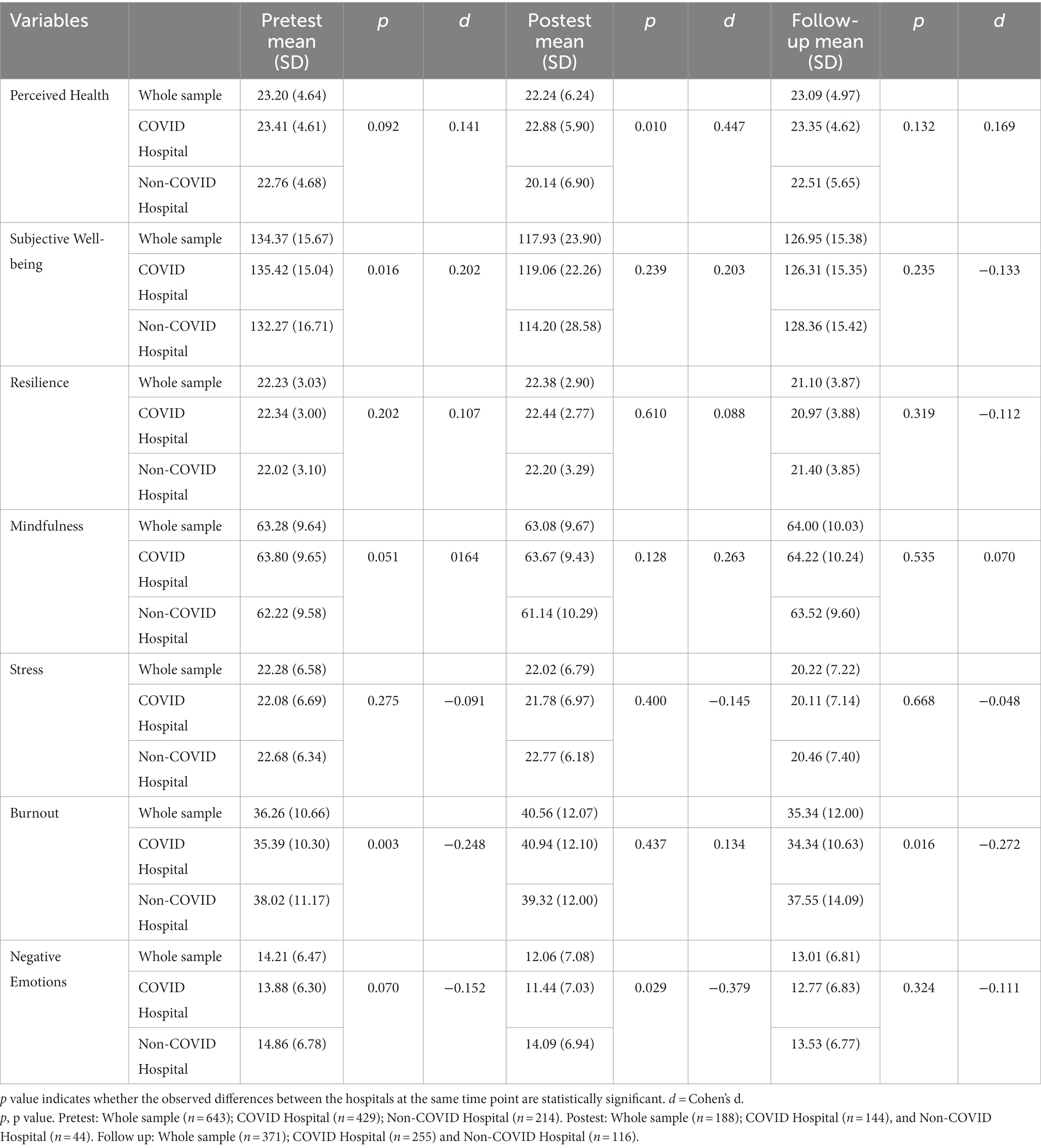
Table 2. Mean scores of perceived health, subjective well-being, resilience, mindfulness, stress, burnout, and negative emotions for the whole sample and divided by COVID Hospital and Non-COVID Hospital nurses at pretest, postest, and 6-month follow-up.
In a subsample of 371 nurses, who completed pre-test and 6 months follow-up surveys, the mean scores of subjective well-being, resilience, stress, and negative emotions significantly decreased from pre-test to 6 months follow-up, while the mean score for mindfulness increased. The mean score for the perception of health and burnout, however, remained stable. A different trend was observed among non-COVID Hospital nurses, where only the mean scores of subjective well-being and stress decreased, while the mean scores of mindfulness, resilience, and negative emotions remained unchanged (Table 3).
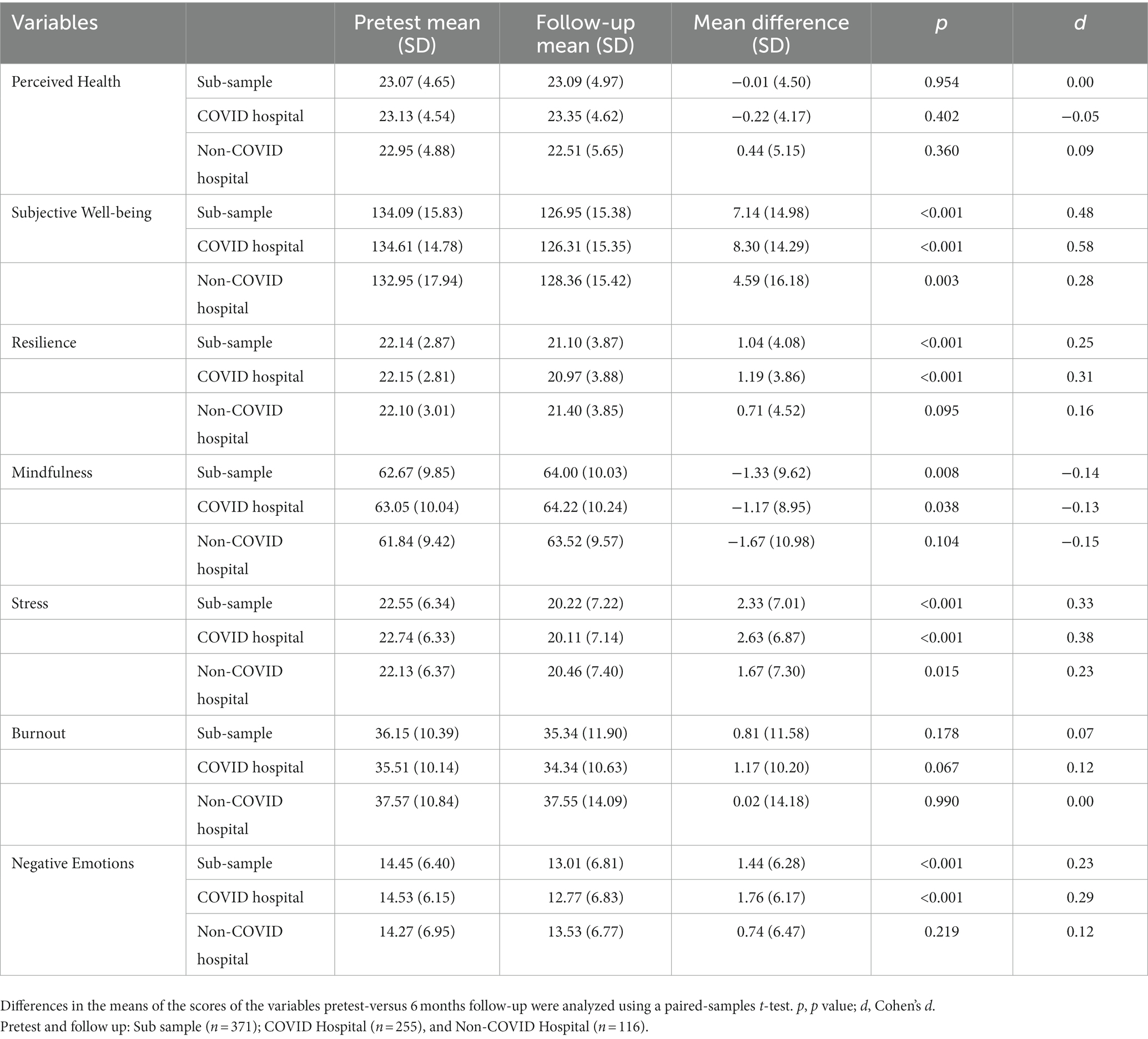
Table 3. Mean scores and mean difference for perceived health, subjective well-being, resilience, mindfulness, stress, burnout and negative emotions at pretest and 6 months follow-up for a sub-sample of nurses who completed both timepoint measures and divided by hospitals.
4. Discussion
The results of our study indicate that an online mind–body based intervention was associated with improved mindfulness and decreased negative emotions and stress among nurses during the first wave of the COVID-19 pandemic. However, this intervention was also associated with a decrease in subjective well-being and resilience. There were no significant changes in burnout and health perception. At 6 months post-intervention, nurses working at the non-COVID hospital had significantly higher mean scores for burnout than those working at the COVID hospital.
After 6 months post-intervention, nurses in both COVID and non-COVID hospitals showed an increase in mindfulness and a decrease in perceived stress and negative emotions. Notably, nurses in the COVID Hospital who had higher levels of mindfulness also presented lower scores in negative emotions compared to those in the non-COVID hospital. Under the Perceived Stress Scale (PSS; Cohen et al., 1983) we measured situations appraised as stressful and recorded as unpredictable, uncontrollable, and overloaded in nurses’ lives; that is, when the individual’s resources to cope with stressors are disabled and a sense of imbalance in control over health, relations, or emotions negatively impacting well-being (Schönfeld et al., 2016; Wersebe et al., 2018; Kun, 2022). Mindfulness practices involve directing one’s awareness to the present moment without judgment, in order to lessen stress and negative emotions when faced with stressful situations (Kabat-Zinn, 2005; Antonova et al., 2021). In this way, it can enable nurses to interpret circumstances as less distressing, which in turn can decrease negative emotions. It is possible that our findings were due to nurses paying more mindful attention to their appraisals of challenging situations, which enabled them to adapt better to stress, resulting in a decrease in negative emotions and an increase in mindfulness (Weinstein et al., 2009). Our results are compatible with well-documented effects on the effectiveness of mindfulness-based interventions for nurses resulting in the reduction of stress (Guillaumie et al., 2017). The beneficial effects of mindfulness on the reduction of stress perception have primarily been reported for face-to-face programs. Recent studies showed that online mindfulness interventions can successfully reduce stress and anxiety while improving emotion regulation in participants (Sanilevici et al., 2021; Ju et al., 2022). Our results could also be explained by the temporal nature of the data collection in the context of the COVID-19 pandemic. Pretest measures were collected 1 month after the official outbreak of the pandemic, which may have caused alarm and elevated levels of stress and negative emotions in nurses. Follow-up data was collected after vaccines became available for health staff Mexico, which may have resulted in a reduction of perceived stress and negative emotions due to a decreased sense of risk. Our findings support the feasibility online mind–body based intervention for the promotion of mindfulness, reduction of stress and negative emotions, especially during difficult times like the COVID-19 pandemic. However, further research is needed to investigate this relationship in a context where the circumstances are not rapidly changing, and with the inclusion of a control group.
Based on our observation of an increase in mindfulness and a decrease in perceived stress and negative emotions, we anticipated that the perception of resilience and well-being would also increase over time. However, this was not the outcome. Nurses decrease in resilience scores could be more directly linked to their incapacity to recover from the health-related outcomes of the COVID-19 crisis. This could be attributed to the fact that the Brief Resilience Scale (Smith et al., 2008) measures an individual’s ability to recover from stress rather than resilience as a personality trait, which is reflected in scales such as the Connor-Davidson Resilience Scale (Connor and Davidson, 2003). Moreover, nurses’ perception of subjective well-being, as measured under the PERMA approach, considers that higher levels of the five components (positive emotions, engagement, relationships, meaning, and achievement) act as a buffer against negative emotions and distress (Seligman, 2018). It is proposed that, despite advances in well-being research, there is a lack of a unifying framework that clarifies dimensions of well-being that can be improved through training. Additionally, research is needed to understand the mechanisms through which these interventions work and to identify any potential hindering intervening factors associated with their use. In order to ensure that these interventions can be used safely and effectively, it is important to conduct further research to answer these questions.
Overall, we found that perception of burnout remained stable over time. We observed that nurses not directly involved in the care of COVID-19 patients had higher scores of negative emotions and burnout compared to those working in COVID hospitals, both at the initial assessment and during the subsequent follow-up assessment, which differed from the findings of previous research (Hu et al., 2020; Sarboozi Hoseinabadi et al., 2020). A possible explanation for this unexpected trend is that nurses at the COVID-hospital were likely more adequately equipped to fulfill their job requirements in comparison to those employed in the non-COVID hospital. Moreover, non-COVID hospitals nurses had increased workload, reassignment to other roles or duties. In a recent study conducted in China during the COVID-19 pandemic, they found that frontline medical staff had a lower frequency of burnout as compared with those working in usual wards. Frontline staff are the individuals on the frontlines of the pandemic, providing direct care to patients with COVID-19, while those in usual wards are providing care to patients with other medical conditions who are not affected by the virus. In that study frontline workers were less worried about becoming infected despite working directly with infected patients (Wu et al., 2020). Another possible explanation is that by directly addressing COVID-19 patients, nurses may have felt a greater sense of control of their situation as well as increasing recognition. Control in the workplace is thought to be a major driver of engagement and important for avoiding burnout (Maslach and Leiter, 2016). Our results confirm that in the face of a crisis, both frontline and usual health staff should be considered when policies and procedures to support the well-being of health care workers are planned.
There are several limitations of this study. An important limitation of our study is the lack of a control group. As the pandemic caused fluctuating conditions for each time period, it cannot be determined whether the differences in nurses’ responses were due to the intervention or the impact of the COVID-19 crisis. Nurses worked at a private institution, limiting the generalization of our findings to nurses working at public healthcare settings in Mexico that may have had different experiences of the COVID-19 outbreak. Given the high rate of attrition, our results should be viewed with caution. Over 70% of nurses did not fill out the post-test, and 42% did not take the 6-month post-intervention survey. This could lead to response bias, as those who did not respond may have been too stressed or we may have only received responses from highly engaged nurses. Finally, we were unable to objectively measure the adherence to the intervention. To gain insight into the implementation of the program, weekly check-ins with nurses’ managers were conducted. Furthermore, we monitored the user count and the view count for the web-based platform where the intervention was conducted. But unfortunately, we were not able to accurately measure the degree to which individual participants engaged with the program or how frequently they practiced.
Despite the limitations noted above, the results of this study indicate that our online mind–body intervention has the potential to enhance mindfulness and lessen stress and negative emotions. However, its influence on the subjective well-being and resilience of hospital staff nurses is uncertain. This paper contributes to the existing literature by providing insight into nurses’ experiences with combined mind–body based interventions, which has been under-researched. Our results may enable future comparative work to further understand what works for these professionals and may enhance evidence-based development of new initiatives to support their well-being. Additionally, our findings suggest that both frontline and usual health care workers should be considered when developing strategies to maintain the health and safety of health care personnel during times of crisis.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by The Institutional Ethical Committee of the School of Medicine of the Universidad de Monterrey approved the study (CEI-002-20191210). The patients/participants provided their written informed consent to participate in this study.
Author contributions
AC-L, AQ-G and AV generated the idea. AC-L designed the intervention. AC-L and SV were responsible for drafting the manuscript. AC-L, SV, AV, IG-R, and LS coordinate the study and participants. AC-L, SV, AV, IG-R, LS, and AQ-G critically revised it for important intellectual content, gave final approval to the finished manuscript, and agreed to be accountable for all aspects of the work. All authors contributed to the article and approved the submitted version.
Acknowledgments
We thank all the study participants for taking the time to answer the questionnaires and participating in the online mind–body based intervention; the nurse department for their support in coordinating the study and the expert volunteers in mind–body techniques: Patricia Montemayor, Claudia Treviño, Graciela Maldonado, Inés Andina, Melva Vela, Rossana De La Garza, and Silvia Fernández for their time in the design and implementation of the intervention. Finally, we thank TecSalud for allowing us to carry out the intervention and collect data at the three time points.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Andolhe, R., Barbosa, R. L., EMD, O., Costa, A. L. S., and Padilha, K. G. (2015). Estresse, coping e burnout da Equipe de Enfermagem de Unidades de Terapia Intensiva: fatores associados. Rev. Esc. Enferm. U.S.P. 49(spe), 58–64. doi: 10.1590/S0080-623420150000700009
Antonova, E., Schlosser, K., Pandey, R., and Kumari, V. (2021). Coping with COVID-19: mindfulness-based approaches for mitigating mental health crisis. Front. Psychol. 12:322. doi: 10.3389/fpsyt.2021.563417
Barajas, S., and Garra, L. (2014). Mindfulness and psychopathology: adaptation of the mindful attention awareness scale (MAAS) in a Spanish sample. Clin. Salud. 25, 49–56. doi: 10.1016/S1130-5274(14)70026-X
Benson, H., Beary, J. F., and Carol, M. P. (1974). The relaxation response. Psychiatry 37, 37–46. doi: 10.1080/00332747.1974.11023785
Bishop, S. R., Lau, M., Shapiro, S., Carlson, L., Anderson, N. D., Carmody, J., et al. (2004). Mindfulness: a proposed operational definition. Clin. Psychol. Sci. Pract. 11, 230–241. doi: 10.1093/clipsy.bph077
Brito Ortíz, J. F., Nava Gómez, M. E., and Juárez, G. A. (2020). Escala de estrés percibido en estudiantes de odontología, enfermería y psicología: validez de constructo. Rev. Concienc. Epg. 4, 42–54. doi: 10.32654/CONCIENCIAEPG.4-2.4
Brown, K. W., and Ryan, R. M. (2003). The benefits of being present: mindfulness and its role in psychological well-being. J. Pers. Soc. Psychol. 84, 822–848. doi: 10.1037/0022-3514.84.4.822
Butler, J., and Kern, M. L. (2016). The PERMA-profiler: a brief multidimensional measure of flourishing. Int. J. Wellbeing 6, 1–48. doi: 10.5502/ijw.v6i3.526
Cai, H., Tu, B., Ma, J., Chen, L., Fu, L., Jiang, Y., et al. (2020). Psychological impacts and coping strategies of front-line medical staff during COVID-19 outbreak in Hunan, China. Med. Sci. Monit. 26:26. doi: 10.12659/MSM.924171
Choi, J. S., and Kim, K. M. (2016). Crisis prevention and management by infection control nurses during the Middle East respiratory coronavirus outbreak in Korea. Am. J. Infect. Control 44, 480–481. doi: 10.1016/j.ajic.2015.10.032
Cohen, S., Kamarck, T., and Mermelstein, R. (1983). A global measure of perceived stress. J. Health Soc. Behav. 24:385. doi: 10.2307/2136404
Connor, K. M., and Davidson, J. R. T. (2003). Development of a new resilience scale: the Connor-Davidson resilience scale (CD-RISC). Depress. Anxiety 18, 76–82. doi: 10.1002/da.10113
Cortés-Álvarez, N. Y., Piñeiro-Lamas, R., and Vuelvas-Olmos, C. R. (2020). Psychological effects and associated factors of COVID-19 in a Mexican sample. Disaster Med. Public Health Prep. 14, 413–424. doi: 10.1017/dmp.2020.215
Cozzolino, M., Girelli, L., Vivo, D. R., Limone, P., and Celia, G. (2020). A mind–body intervention for stress reduction as an adjunct to an information session on stress management in university students. Brain Behav. 10:e01651. doi: 10.1002/brb3.1651
Davidson, R. J., and Lutz, A. (2008). Buddha’s brain: neuroplasticity and meditation [in the spotlight]. IEEE Signal Process. Mag. 25, 176–174. doi: 10.1109/MSP.2008.4431873
de México, G. (2020). COVID-19 Tablero México-CONACYT-CentroGeo-GeoInt-DataLab [Internet]. Available at: https://coronavirus.gob.mx/datos/
Denckla, C. A., Cicchetti, D., Kubzansky, L. D., Seedat, S., Teicher, M. H., Williams, D. R., et al. (2020). Psychological resilience: an update on definitions, a critical appraisal, and research recommendations. Eur. J. Psychotraumatol. 11:1822064. doi: 10.1080/20008198.2020.1822064
Dran, J. (2018). A unique institutional response to the Zika virus epidemic. Obstet. Gynecol. 131, 666–670.
El-Hage, W., Hingray, C., Lemogne, C., Yrondi, A., Brunault, P., Bienvenu, T., et al. (2020). Les professionnels de santé face à la pandémie de la maladie à coronavirus (COVID-19): quels risques pour leur santé mentale? L'Encéphale 46, S73–S80. doi: 10.1016/j.encep.2020.04.008
Foster, K., Cuzzillo, C., and Furness, T. (2018). Strengthening mental health nurses’ resilience through a workplace resilience programme: a qualitative inquiry. J. Psychiatr. Ment. Health Nurs. 25:338. doi: 10.1111/jpm.12467
de Nuevo Leon, G. (2021). Reporta NL la cifra más baja de casos de COVID-19 en 11 meses. Available at: https://www.nl.gob.mx/boletines-comunicados-y-avisos/reporta-nl-la-cifra-mas-baja-de-casos-de-covid-19-en-11-meses
Griffith, J. M., Hasley, J. P., Liu, H., Severn, D. G., Conner, L. H., and Adler, L. E. (2008). Qigong stress reduction in hospital staff. J. Altern. Complement. Med. 14, 939–945. doi: 10.1089/acm.2007.0814
Gross, J. J. (2015). Emotion regulation: current status and future prospects. Psychol. Inq. 26, 1–26. doi: 10.1080/1047840X.2014.940781
Grossman, P., Niemann, L., Schmidt, S., and Walach, H. (2004). Mindfulness-based stress reduction and health benefits. J. Psychosom. Res. 57, 35–43. doi: 10.1016/S0022-3999(03)00573-7
Guillaumie, L., Boiral, O., and Champagne, J. (2017). A mixed-methods systematic review of the effects of mindfulness on nurses. J. Adv. Nurs. 73, 1017–1034. doi: 10.1111/jan.13176
Henshall, C., Davey, Z., and Jackson, D. (2020). The implementation and evaluation of a resilience enhancement programme for nurses working in the forensic setting. Int. J. Ment. Health Nurs. 29, 508–520. doi: 10.1111/inm.12689
Hu, D., Kong, Y., Li, W., Han, Q., Zhang, X., Zhu, L. X., et al. (2020). Frontline nurses’ burnout, anxiety, depression, and fear statuses and their associated factors during the COVID-19 outbreak in Wuhan, China: A large-scale cross-sectional study. EClinicalMedicine :24:100424. doi: 10.1016/j.eclinm.2020.100424
Jackson, D., Firtko, A., and Edenborough, M. (2007). Personal resilience as a strategy for surviving and thriving in the face of workplace adversity: a literature review. J. Adv. Nurs. 60, 1–9. doi: 10.1111/j.1365-2648.2007.04412.x
Johnson, J., Hall, L. H., Berzins, K., Baker, J., Melling, K., and Thompson, C. (2018). Mental healthcare staff well-being and burnout: a narrative review of trends, causes, implications, and recommendations for future interventions. Int. J. Ment. Health Nurs. 27, 20–32. doi: 10.1111/inm.12416
Ju, R., Chiu, W., Zang, Y., Hofmann, S. G., and Liu, X. (2022). Effectiveness and mechanism of a 4-week online self-help mindfulness intervention among individuals with emotional distress during COVID-19 in China. BMC Psychol. 10:149. doi: 10.1186/s40359-022-00831-7
Kabat-Zinn, J. (2003). Mindfulness-based interventions in context: past, present, and future. Clin. Psychol. Sci. Pract. 10, 144–156. doi: 10.1093/clipsy.bpg016
Kabat-Zinn, J. Coming to Our Senses: Healing Ourselves and the World Through Mindfulness. New York, NY: Hyperion; (2005).
Kollie, E., Winslow, B., Pothier, P., and Gaede, D. (2017). Deciding to work during the Ebola outbreak: the voices and experiences of nurses and midwives in Liberia. Int. J. Afr. Nurs. Sci. 7, 75–81. doi: 10.1016/j.ijans.2017.09.002
Kun, A. (2022). “Health, stress, well-being and positive affectivity” in Psychology [Internet]. Typotex Kiadó; 2013 [Cited 2022 August 22]. eds. Tackacs I, Soos J, p. 1–21. Available at: http://www.tankonyvtar.hu/hu/tartalom/tamop412A/2011-0023_Psychology/000000.html
Maben, J., and Bridges, J. (2020). Covid-19: supporting nurses’ psychological and mental health. J. Clin. Nurs. 29, 2742–2750. doi: 10.1111/jocn.15307
Magne, H., Jaafari, N., and Voyer, M. (2021). La croissance post-traumatique: un concept méconnu de la psychiatrie française. L'Encéphale 47, 143–150. doi: 10.1016/j.encep.2020.05.021
Maslach, C., and Leiter, M. P. (2016). Understanding the burnout experience: recent research and its implications for psychiatry. World Psychiatry 15, 103–111. doi: 10.1002/wps.20311
Maslach, C., Schaufeli, W. B., and Leiter, M. P. (2001). Job Burnout. Annu. Rev. Psychol. 52, 397–422. doi: 10.1146/annurev.psych.52.1.397
Montero-Marín, J., Piva Demarzo, M. M., Stapinski, L., Gili, M., and García-Campayo, J. (2014). Perceived stress latent factors and the burnout subtypes: a structural model in dental students. PLoS One 9:e99765. doi: 10.1371/journal.pone.0099765
Montero-Marín, J., Skapinakis, P., Araya, R., Gili, M., and García-Campayo, J. (2011). Towards a brief definition of burnout syndrome by subtypes: development of the “burnout clinical subtypes questionnaire” (BCSQ-12). Health Qual. Life Outcomes 9:74. doi: 10.1186/1477-7525-9-74
Raudenská, J., Steinerová, V., Javůrková, A., Urits, I., Kaye, A. D., Viswanath, O., et al. (2020). Occupational burnout syndrome and post-traumatic stress among healthcare professionals during the novel coronavirus disease 2019 (COVID-19) pandemic. Best Pract. Res. Clin. Anaesthesiol. 34, 553–560. doi: 10.1016/j.bpa.2020.07.008
Raven, J., Wurie, H., and Witter, S. (2018). Health workers’ experiences of coping with the Ebola epidemic in Sierra Leone’s health system: a qualitative study. BMC Health Serv. Res. 18:251. doi: 10.1186/s12913-018-3072-3
Rodríguez-Rey, R., Alonso-Tapia, J., and Hernansaiz-Garrido, H. (2016). Reliability and validity of the brief resilience scale (BRS) Spanish version. Psychol. Assess. 28, e101–e110. doi: 10.1037/pas0000191
Sampaio, F., Sequeira, C., and Teixeira, L. (2021). Impact of COVID-19 outbreak on nurses’ mental health: a prospective cohort study. Environ. Res. 194:110620. doi: 10.1016/j.envres.2020.110620
Sanilevici, M., Reuveni, O., Lev-Ari, S., Golland, Y., and Levit-Binnun, N. (2021). Mindfulness-based stress reduction increases mental wellbeing and emotion regulation during the first wave of the COVID-19 pandemic: a synchronous online intervention study. Front. Psychol. 12:720965. doi: 10.3389/fpsyg.2021.720965
Sarboozi Hoseinabadi, T., Kakhki, S., Teimori, G., and Nayyeri, S. (2020). Burnout and its influencing factors between frontline nurses and nurses from other wards during the outbreak of coronavirus disease-COVID-19-in Iran. Investig. Educ. Enferm. 38:e3. doi: 10.17533/udea.iee.v38n2e03
Schönfeld, P., Brailovskaia, J., Bieda, A., Zhang, X. C., and Margraf, J. (2016). The effects of daily stress on positive and negative mental health: mediation through self-efficacy. Int. J. Clin. Health Psychol. 16, 1–10. doi: 10.1016/j.ijchp.2015.08.005
Seligman, M. (2018). PERMA and the building blocks of well-being. J. Posit. Psychol. 13, 333–335. doi: 10.1080/17439760.2018.1437466
Shih, F. J., Turale, S., Lin, Y. S., Gau, M. L., Kao, C. C., Yang, C. Y., et al. (2009). Surviving a life-threatening crisis: Taiwan’s nurse leaders’ reflections and difficulties fighting the SARS epidemic. J. Clin. Nurs. 18, 3391–3400.
Smith, B. W., Dalen, J., Wiggins, K., Tooley, E., Christopher, P., and Bernard, J. (2008). The brief resilience scale: assessing the ability to bounce back. Int. J. Behav. Med. 15, 194–200. doi: 10.1080/10705500802222972
Troy, A. S., Shallcross, A. J., Brunner, A., Friedman, R., and Jones, M. C. (2018). Cognitive reappraisal and acceptance: effects on emotion, physiology, and perceived cognitive costs. Emotion 18, 58–74. doi: 10.1037/emo0000371
Walton, M., Murray, E., and Christian, M. D. (2020). Mental health care for medical staff and affiliated healthcare workers during the COVID-19 pandemic. Eur. Heart J. Acute Cardiovasc. Care 9, 241–247. doi: 10.1177/2048872620922795
Weiner, L., Berna, F., Nourry, N., Severac, F., Vidailhet, P., and Mengin, A. C. (2020). Efficacy of an online cognitive behavioral therapy program developed for healthcare workers during the COVID-19 pandemic: the REduction of STress (REST) study protocol for a randomized controlled trial. Trials 21:870. doi: 10.1186/s13063-020-04772-7
Weinstein, N., Brown, K. W., and Ryan, R. M. (2009). A multi-method examination of the effects of mindfulness on stress attribution, coping, and emotional well-being. J. Res. Pers. 43, 374–385. doi: 10.1016/j.jrp.2008.12.008
Wersebe, H., Lieb, R., Meyer, A. H., Hofer, P., and Gloster, A. T. (2018). The link between stress, well-being, and psychological flexibility during an acceptance and commitment therapy self-help intervention. Int. J. Clin. Health Psychol. 18, 60–68. doi: 10.1016/j.ijchp.2017.09.002
Wilson, A., and Nguyen, T. N. M. (2017). The Zika virus epidemic: public health roles for nurses. Online J. Issues Nurs. 22:4. doi: 10.3912/OJIN.Vol22No01Man04
Wong, P. T. P. (2010). Meaning therapy: an integrative and positive existential psychotherapy. J. Contemp. Psychother. 40, 85–93. doi: 10.1007/s10879-009-9132-6
Wong, P. T. P. (2011). Positive psychology 2.0: towards a balanced interactive model of the good life. Can. Psychol. 52, 69–81. doi: 10.1037/a0022511
Wong, P. T. P. (2020). Existential positive psychology and integrative meaning therapy. Int. Rev. Psychiatry 32, 565–578. doi: 10.1080/09540261.2020.1814703
World Health Organization State of the world’s nursing 2020: Investing in education, jobs and leadership. Geneva. (2020).
World Health Organization, World Health Day (2020). Year of the nurse and midwife. Available at: https://www.who.int/china/news/detail/07-04-2020-world-health-day-2020-year-of-the-nurse-and-midwife
Wu, Y., Wang, J., Luo, C., Hu, S., Lin, X., Anderson, A. E., et al. (2020). A comparison of burnout frequency among oncology physicians and nurses working on the frontline and usual wards during the COVID-19 epidemic in Wuhan. Chin. J. Pain Symptom Manag. 60, e60–e65. doi: 10.1016/j.jpainsymman.2020.04.008
Keywords: well-being, COVID-19, nurses, mindfulness, negative emotion, mind–body
Citation: Cepeda-Lopez AC, Solís Domínguez L, Villarreal Zambrano S, Garza-Rodriguez IY, del Valle AC and Quiroga-Garza A (2023) A comparative study of well-being, resilience, mindfulness, negative emotions, stress, and burnout among nurses after an online mind–body based intervention during the first COVID-19 pandemic crisis. Front. Psychol. 14:848637. doi: 10.3389/fpsyg.2023.848637
Edited by:
Dan J. Miller, James Cook University, AustraliaReviewed by:
Jose Maria De La Roca-Chiapas, University of Guanajuato, MexicoLuis Felipe Dias Lopes, Federal University of Santa Maria, Brazil
Yuke Tien Fong, Singapore General Hospital, Singapore
Copyright © 2023 Cepeda-Lopez, Solís Domínguez, Villarreal Zambrano, Garza-Rodriguez, del Valle and Quiroga-Garza. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ana Carla Cepeda-Lopez, YW5hY2FybGFjZXBlZGExMUBnbWFpbC5jb20=