
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol., 08 January 2024
Sec. Health Psychology
Volume 14 - 2023 | https://doi.org/10.3389/fpsyg.2023.1295031
This article is part of the Research TopicPublic Mental Health in Trauma and WarView all 10 articles
 Josef S. Baumgartner1*
Josef S. Baumgartner1* Antonia Renner1Thomas Wochele-Thoma2Peter Wehle1,3
Antonia Renner1Thomas Wochele-Thoma2Peter Wehle1,3 Corrado Barbui4
Corrado Barbui4 Marianna Purgato4
Marianna Purgato4 Federico Tedeschi4
Federico Tedeschi4 Lorenzo Tarsitani5Valentina Roselli5Ceren Acartürk6
Lorenzo Tarsitani5Valentina Roselli5Ceren Acartürk6 Ersin Uygun7Minna Anttila8
Ersin Uygun7Minna Anttila8 Tella Lantta8
Tella Lantta8 Maritta Välimäki8,9Rachel Churchill10Lauren Walker10,11
Maritta Välimäki8,9Rachel Churchill10Lauren Walker10,11 Marit Sijbrandij12,13
Marit Sijbrandij12,13 Pim Cuijpers12,13Markus Koesters14,15Thomas Klein14,15Ross G. White16Marion C. Aichberger1
Pim Cuijpers12,13Markus Koesters14,15Thomas Klein14,15Ross G. White16Marion C. Aichberger1 Johannes Wancata1
Johannes Wancata1Refugees are at increased risk for developing psychological impairments due to stressors in the pre-, peri- and post-migration periods. There is limited knowledge on how everyday functioning is affected by migration experience. In a secondary analysis of a study in a sample of refugees and asylum seekers, it was examined how aspects of psychological functioning were differentially affected. 1,101 eligible refugees and asylum seekers in Europe and Türkiye were included in a cross-sectional analysis. Gender, age, education, number of relatives and children living nearby, as well as indicators for depressive and posttraumatic symptoms, quality of life, psychological well-being and functioning, and lifetime potentially traumatic events were assessed. Correlations and multiple regression models with World Health Organization Disability Assessment Schedule 2.0 (WHODAS 2.0) 12-item version’s total and six subdomains’ scores (‘mobility’, ‘life activities’, ‘cognition’, ‘participation’, ‘self-care’, ‘getting along’) as dependent variables were calculated. Tests for multicollinearity and Bonferroni correction were applied. Participants reported highest levels of impairment in ‘mobility’ and ‘participation’, followed by ‘life activities’ and ‘cognition’. Depression and posttraumatic symptoms were independently associated with overall psychological functioning and all subdomains. History of violence and abuse seemed to predict higher impairment in ‘participation’, while past events of being close to death were associated with fewer issues with ‘self-care’. Impairment in psychological functioning in asylum seekers and refugees was related to current psychological symptoms. Mobility and participation issues may explain difficulties arising after resettlement in integration and exchange with host communities in new contexts.
Everyday functioning is an essential part of one’s identity and is closely linked to quality of life and general well-being (Doré and Caron, 2017). Contrary to earlier conceptualisations of physical and mental health as the absence of illness, modern frameworks try to consider an individual’s abilities in light of its challenges and resources (Sleijpen et al., 2013). The World Health Organization (WHO) developed the International Classification of Functioning, Disability and Health (ICF) as a tool to describe information on functioning and to measure impairments in functioning in consideration of environmental and societal factors (World Health Organization, 2001). In accordance with the functioning levels of ICF, the WHO distributed the WHO Disability Assessment Schedule (WHODAS) version 2.0 to efficiently assess psychological functioning in general and clinical populations across the globe (Üstün et al., 2010). Psychological functioning is an umbrella term for the ability to interact with one’s surroundings and in different contexts.
Refugees and asylum seekers (RAS) face various pre-, peri- and post-migratory challenges (Laban et al., 2005; Priebe et al., 2016). RAS are often subjected to persecution for political, ethnic, religious or other reasons in their home countries, some witness death, combat, torture, abuse of relatives, or economic hardship and lack of water, food, and other basic needs (Nosè et al., 2020). On hazardous flight routes RAS are frequently exposed to physical harm, sexual violence and life-threatening conditions (Li et al., 2016). Even after resettlement in their host countries continuous stressors remain, including uncertainty about legal status, risk of being detained and deported, and difficulties with social integration, social exclusion, discrimination and economic disadvantages (Laban et al., 2008; Morgan et al., 2017). In a qualitative study, Salvo and de C Williams (2017) investigated how learning the host country’s language affected the lives of RAS. While the impact of learning the language was associated with achievement, aspirations and autonomy, barriers to learning, and a sense of shame due to reduced skills were important mitigators of individual well-being (Salvo and de C Williams, 2017). Furthermore, traumatic life events are associated with common mental disorders such as posttraumatic stress disorder (PTSD), and with reduced functioning, with a more pronounced relationship in women than in men (Robertson et al., 2016). Recent studies confirm the risk of psychological distress, and occurrence of depression and anxiety symptoms in RAS individuals from Ukraine (Buchcik et al., 2023), while identifying several coping and resilience strategies in the context of war as well as risk and protective factors (Oviedo et al., 2022; Rizzi et al., 2023).
However, outcomes may also be very dependent on the different modes of migration, reasons for flight, levels of openness or hostility of the host country society, as well as the legal, socioeconomic and healthcare provisions available in the host countries (Tay et al., 2019).
The aim of this cross-sectional analysis is to contribute to the existing knowledge base relating to risk factors associated with reduced psychological functioning overall and in the six domains of cognition, mobility, self-care, getting along, life activities and participation according to WHODAS 2.0 12-item version in a vulnerable, but clinically healthy population of RAS in high- and middle-income countries. To the best of our knowledge, no studies have yet examined influence factors on the different domains of functioning among RAS. Of particular interest will be which domains of functioning are typically impaired in these populations, whether specific effects of migration- and flight-associated stressors can be identified, and the specific role of traumatic events. Initial expectations were that, even in the absence of overt mental disorders, reduced psychological functioning would still play an important role in refugee mental health.
We performed a secondary analysis of the RE-DEFINE dataset (Purgato et al., 2019, 2021; Acarturk et al., 2022), specifically of baseline data from an intervention study which had been gathered in the period between September 2018 and March 2020.
Recruitments took place in Austria, Finland, Germany, Italy, Türkiye and the United Kingdom. The study population had been highly selected, with inclusion and exclusion criteria rigorously applied in order to test the preventive effects of a psychosocial intervention in a sample of RAS who were in psychological distress, but without diagnosis of a psychiatric disorder. Inclusion criteria were (1) age 18 or above, (2) able to speak and understand Arabic, Dari, or English, (3) being asylum seeker, refugee or person under temporary protection, (4) presence of psychological distress with a score of 3 or more (binary scoring) on the 12-item General Health Questionnaire (GHQ-12), and (5) giving oral and written consent; exclusion criteria were (1) any mental disorder as shown by a positive Mini International Neuropsychiatric Interview (M.I.N.I., Sheehan et al., 1997), (2) acute medical conditions contraindicating participation, (3) clinical evidence of imminent suicide risk or `moderate or high` suicide risk on the M.I.N.I., and (4) clinical evidence of impaired decision-making, and are given also in the RE-DEFINE study protocols (Purgato et al., 2019). Interviews were performed with the help of cultural mediators and involved translators where necessary. Psychological distress, PTSD symptoms, depressive symptoms, psychological well-being and potentially traumatic life events were assessed by using standardized, widely used and feasible measures (see ‘2.3. Measures’). Furthermore, sociodemographic variables (age, gender, years and level of education, number of relatives and children living in the same country) and migration-associated factors (detention, post-migration living difficulties) were gathered during the interviews.
The World Health Organization Disability Assessment Schedule (WHODAS) 2.0 12-item version (short form) is a measurement for deficits in everyday functioning due to health conditions across six domains (Üstün et al., 2010). It is linked to the concepts of the International Classification of Functioning (World Health Organization, 2001) and assesses a time period of 30 days before the interview. The schedule, which was used in translated and validated versions, has shown excellent internal consistency with Cronbach’s alpha up to 0.96, and has been used across different countries and cultures with good discriminative ability and test–retest reliability (Saltychev et al., 2021). Two items each are grouped into the six domains ‘cognition’ (learning a new task, concentrating on doing something for 10 min), ‘mobility’ (standing for long periods, walking a long distance), ‘self-care’ (washing whole body, getting dressed), ‘getting along’ (dealing with people you do not know, maintaining friendships), ‘life activities’ (household responsibilities, day-to-day work), and ‘participation’ (joining community activities, emotionally affected by health problems). In our sample, Cronbach’s alpha for the WHODAS 2.0 was 0.84, and ranging from 0.41 (‘participation’) to 0.90 (‘self-care’) for the subdomains.
The Posttraumatic Symptom Checklist (PCL-5) is based on the Diagnostic and Statistical Manual of Mental Disorders 5th edition (DSM-5)‘s criteria for PTSD (American Psychiatric Association, 2013; Blevins et al., 2015). PCL-5 comprises 20 items out of the diagnostic criteria domains ‘reexperiencing’, ‘avoidance’, ‘negative alterations in cognitions and mood’ and ‘hyperarousal’, and rates them on a scale from zero (‘not at all’) to four (‘extremely’). Recommended cut-offs for probable PTSD diagnosis and indication for treatment range from scores of 31–33 points (Bovin et al., 2016). Internal consistency was measured with a Cronbach’s alpha = 0.91 in this study.
The Patient Health Questionnaire 9-item version (PHQ-9) is a short screening tool for depressive symptoms in adult populations (Kroenke et al., 2001). It rates the nine Diagnostic and Statistical Manual of Mental Disorders 4th edition (DSM-IV)‘s criteria for depression from zero (‘not at all’) to three (‘nearly every day’) (American Psychiatric Association, 1994). The PHQ-9 is a useful tool for measuring depression, with a recommended cut-off of 10 points, and depression severity, with scores of 5, 10, 15, and 20 indicating mild, moderate, moderately severe, and severe depressive symptoms, respectively (Kroenke et al., 2001). Cronbach’s alpha was 0.83 in this study.
The General Health Questionnaire 12-item version (GHQ-12) is a short reliable measurement for psychological distress and signs of depression and anxiety (Goldberg et al., 1997). It includes a four-point Likert scale on each of the 12 items, and is most commonly rated either in a 0–0–1-1 or 0–1–2-3 mode. In order to better assess for severity of distress the second mode was used, with a Cronbach’s alpha of 0.69.
Stressors due to current living conditions in the host country were assessed through 17 items of the Post-Migration Living Difficulties (PMLD) scale, which rates if people were affected by problems in various domains from zero (‘not a problem’) to four (‘a very serious problem’) in the past 12 months (Silove et al., 1997). Cronbach’s alpha in our sample was 0.85.
The 5-item World Health Organization Well-Being Index (WHO-5) is a commonly used short assessment of psychological wellbeing (World Health Organization, Regional Office, 1998). Five positively framed questions on subjective well-being are scored from zero (‘at no time’) to five (‘all of the time’), and generated scores from zero to 25 are elsewhere usually multiplied by four (0–100 final score). It has been applied in many languages and across different settings, and has shown adequate validity as an outcome measure (Cronbach’s alpha in this sample 0.88), with scores of 50 or below indicating poor well-being (12.5 in this study), and as a screening tool for depression (cut-off 28; or 7 in our study) (Topp et al., 2015).
The Harvard Trauma Questionnaire (HTQ) assesses posttraumatic symptoms and life-time traumatic events in refugees (Mollica et al., 1992). Its first part focuses on 16 specific traumatic events and one item ‘other (e.g., domestic violence)’, and had been assessed in a binary yes or no question in this study. In a principal component analysis including a larger sample of refugees and asylum seekers HTQ items had been pooled in three thematic domains ‘lack of basic needs’ (three items, ‘factor 1’), ‘violence and abuse’ (eight items, ‘factor 2’) and ‘being close to death’ (six items, ‘factor 3’) (Barbui et al., 2023). Internal consistency was high with Cronbach’s alpha of 0.87 (subscores’ alphas 0.75–0.80).
Sociodemographic, migration-related factors and results of WHODAS 2.0, GHQ-12, HTQ-I, PCL-5, PHQ-9, PMLD and WHO-5 were analyzed by using descriptive statistics, in absolute numbers and percentages for the categorical variables, and with means and standard deviations for continuous parameters. All parameters are given in gender-disaggregated form in order to take into account gender differences in descriptive statistics. Cross-tabulation for the WHODAS 2.0 subdomains was used to describe the level of functioning in the sample, with mean and standard deviation (SD) at the domain level to sense differences in impairment. Overall WHODAS 2.0 scores were also reported, to see if values are evenly distributed in our sample.
Spearman rank-order correlations between WHODAS 2.0 total scores (0–48) and each domain score separately (0–8) were calculated for all potential factors, in order to detect strong positive or negative relationships. Strengths of correlations were measured with Spearman correlation coefficients rs.
Finally, multivariable linear regression models were performed for WHODAS 2.0 scores and sub-scores separately, with all other variables acting simultaneously as independent variables (SPSS ‘Enter’ command). Non-standardized regression coefficients were calculated, and variance inflation factor (VIF) as a test for multi-collinearity was applied. In order to account for multiple testing, Bonferroni correction (x7) was used, and the significance level of p < 0.05 was adjusted accordingly (p < 0.007).
Sociodemographic characteristics are summarized in Table 1. A total of 1,101 RAS (48.9% female) with a mean age of 31.8 years (SD 9.5; range 18–71 years) were included in the analysis, the majority of which were of Syrian nationality (n = 758; 68.8%) and resettled to Türkiye (n = 642; 58.3%). Male RAS reported considerably more often having been held in detention than female RAS (24.2% vs. 6.3%), were less likely to be living in a marriage or partnership (57.0% vs. 77.7%), and had on average fewer children and relatives living in the close proximity or the same household. Otherwise, men and women were roughly comparable in other sociodemographic variables.
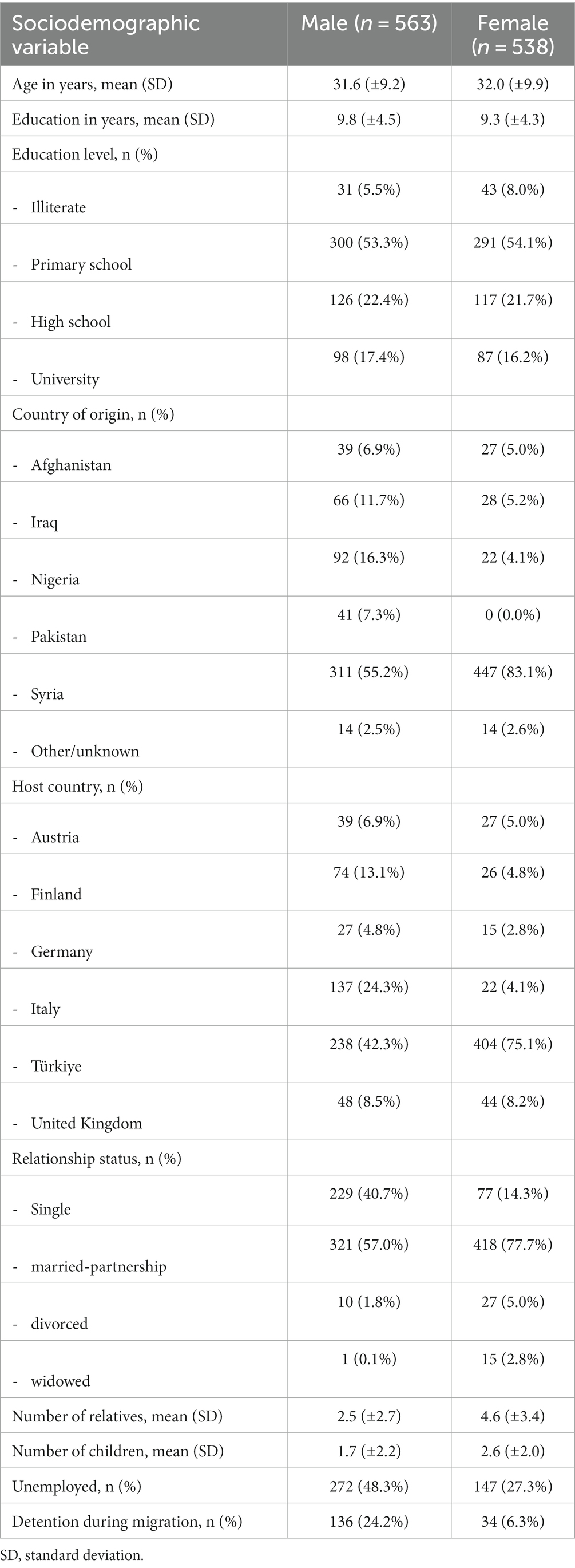
Table 1. Sociodemographics of total sample (n = 1,101).
Presence of psychiatric disorder as assessed by the M.I.N.I. was one of the exclusion criteria, but, based on a GHQ score of 3 or above, those assessed as experiencing clinically significant distress were eligible, and data on a range of depressive symptoms and PTSD symptoms was collected (see Table 2). Men suffered on average more post-migration living difficulties, and reported more lifetime potentially traumatic events, especially those associated with violence and close-to-death experiences. Participants in general showed high psychological distress and reduced quality of life. Accordingly, as shown in Table 3, everyday functioning was mild to moderately impaired in the cohort. The most strongly affected domains of functioning were ‘mobility’ and ‘participation’, followed by ‘life activities’ and ‘cognition’.
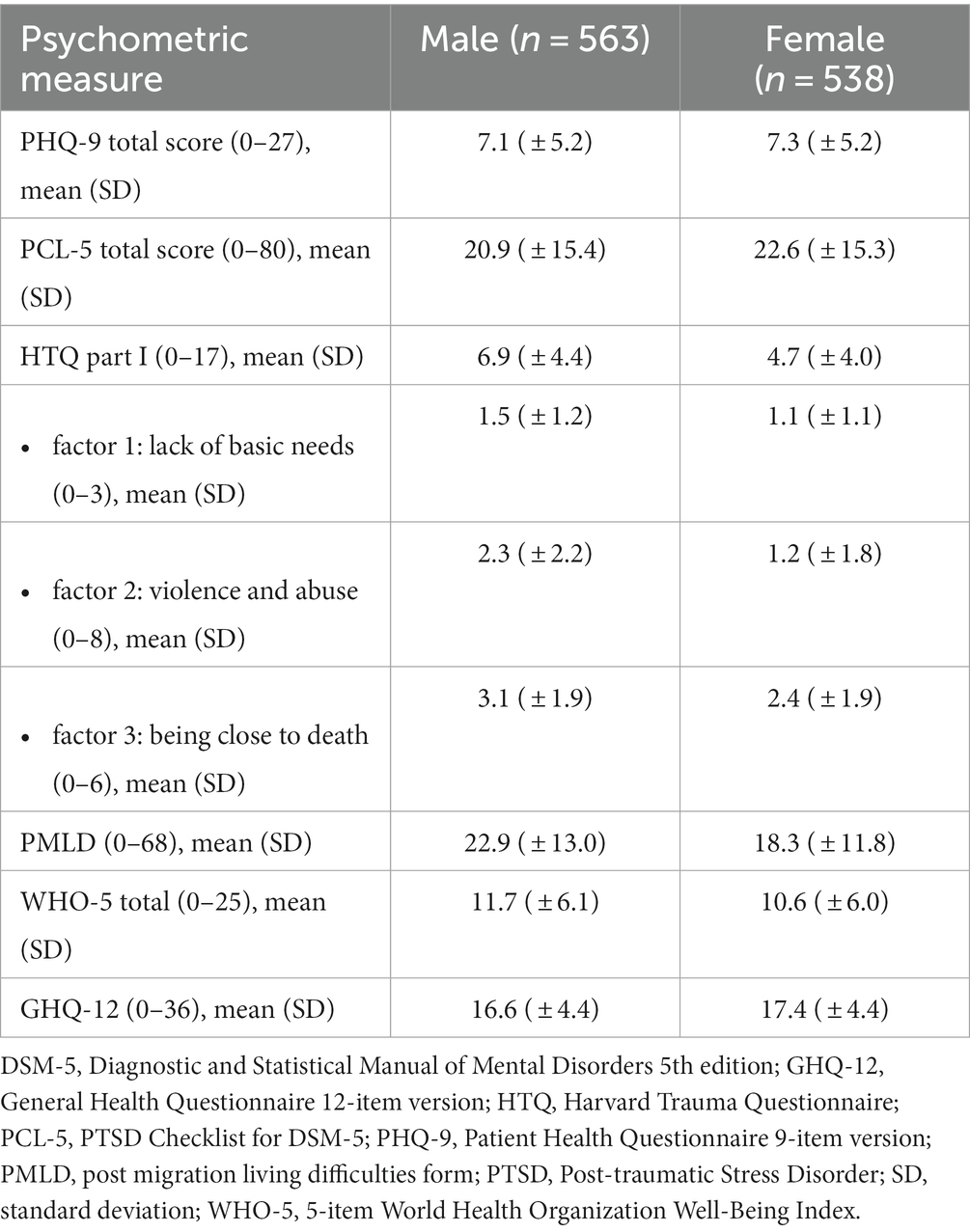
Table 2. Depressive and PTSD symptoms, traumatic events, post-migration living difficulties, quality of life and psychological problems in the sample.
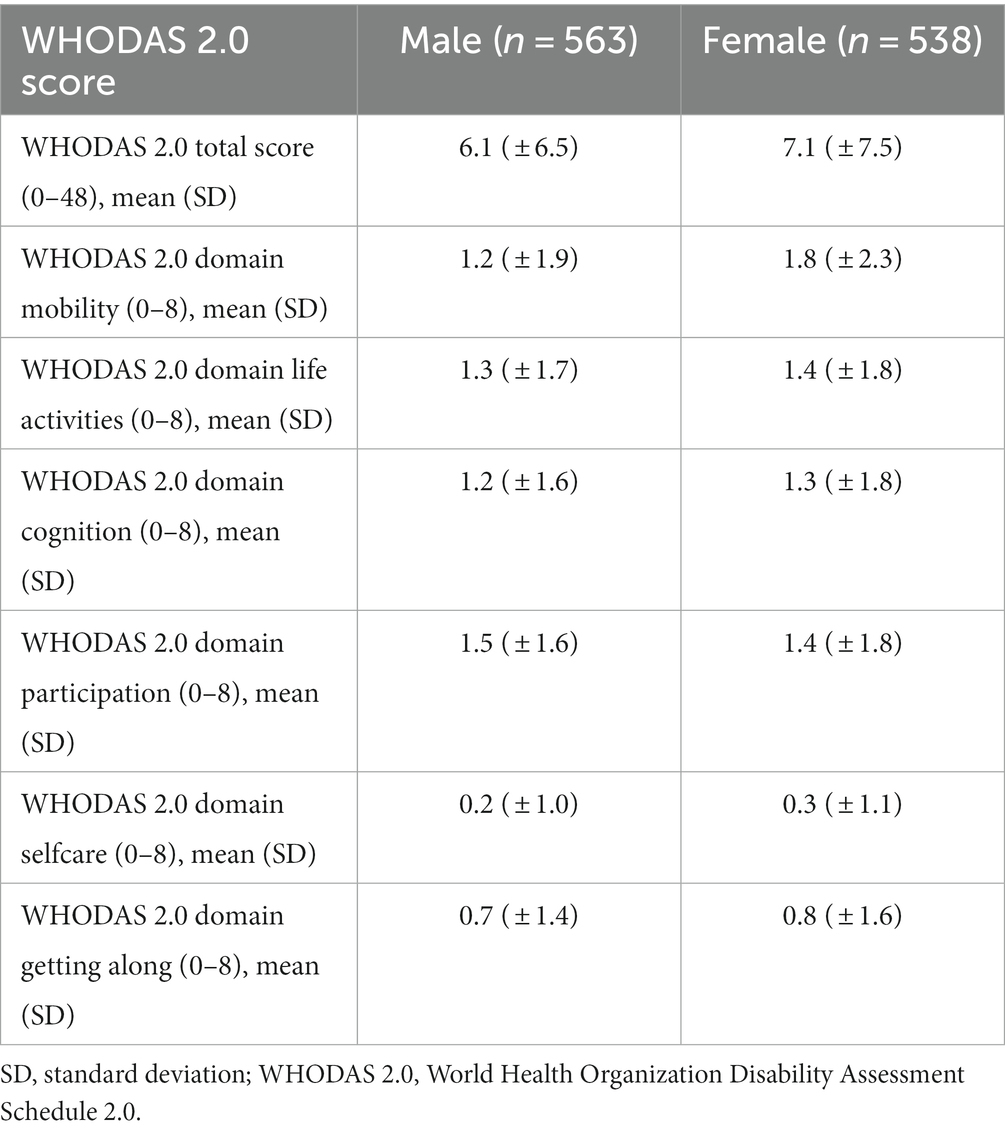
Table 3. 12-item WHODAS 2.0 total and domain scores in the sample.
Spearman rank-order correlations revealed that reduced overall psychological functioning was moderately to strongly associated with PHQ-9 depressive (rs = 0.49) and PCL-5 PTSD (rs = 0.55) symptom scores. Moderate correlations with depressive (PHQ-9) and PTSD (PCL-5) symptoms were also seen for the WHODAS 2.0 domains ‘life activities’ (rs = 0.37 and 0.41), ‘cognition’ (rs = 0.40 and 0.46), ‘participation’ (rs = 0.45 and 0.46), and ‘getting along’ (rs = 0.31 and 0.34). PHQ-9 and PCL-5 scores correlated strongly with each other (rs = 0.68), and both had an inverse relationship to quality of life (rs = 0.41 and 0.34). All bivariate correlations are shown in a table in the appendix (Supplementary Table S1).
The fitted regression models for WHODAS 2.0 total score and domain scores are shown in Table 4. Overall regressions were statistically significant (all p < 0.001), with a variance explained by all predictors simultaneously of around one-third (Nagelkerke’s R2 = 0.368). It was found that older age was significantly associated with more pronounced disability overall (p < 0.001) as well as in the specific domains ‘mobility’ (p < 0.001) and ‘participation’ (p = 0.001). Higher PCL-5 and PHQ-9 scores were associated with worse psychological functioning overall (both p < 0.001) and in every subdomain (all p < 0.001, except PHQ-9 with ‘mobility’ (p = 0.004)). Post-migration living difficulties was associated with worse functioning in ‘cognition’ (p = 0.003). Traumatic life events seemed to have heterogeneous effects on psychological functioning. While ‘violence and abuse’ (HTQ I factor 2) was significantly associated with impairment in ‘participation’ (p = 0.007), ‘being close to death’ (HTQ I factor 3) was non-significantly associated to lower disability overall (p = 0.042), and better ‘self-care’ significantly (p < 0.001). Worse ‘self-care’, on the other hand, was significantly associated with a higher number of children (p < 0.001). The highest VIF was tolerable (VIF = 2.177), hence supporting the assumption of non-multicollinearity of parameters.
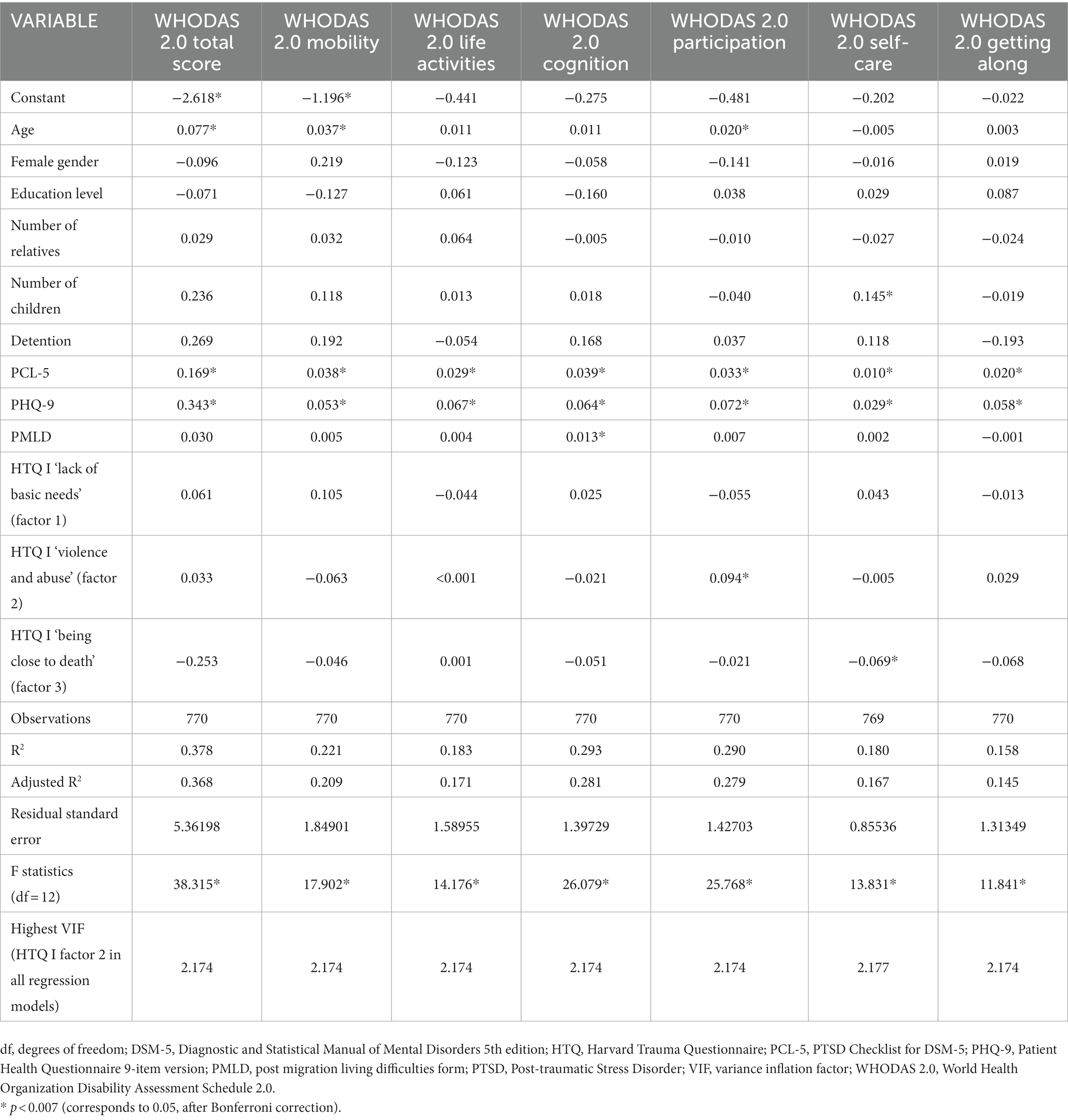
Table 4. Multiple linear regression analyses with WHODAS 2.0 total score and subdomain scores as dependent variables, with non-standardized regression coefficients B for each independent variable, number of observations, R and F statistics and VIF.
This study describes deficits in psychological functioning among a large sample of RAS in high- and middle-income countries in Europe and Türkiye. Functioning is more commonly investigated as a secondary or control variable, but rarely considered as an important primary outcome. It adds value to scientific knowledge in the sense of a differential analysis of psychological functioning in a predominantly Arabic-speaking sample of RAS in European countries including Türkiye. Syria is currently the main origin of RAS worldwide, who are experiencing a high prevalence of mental disorders (Sá et al., 2022), and together with RAS from Ukraine and Afghanistan account for 52% of refugees and persons needing protection worldwide in 2022 (UNHCR, 2023).
An individual’s everyday functioning - i.e. coping with everyday stressors and mastering challenges - is a multi-faceted ability, and there are calls for assessing different domains of functioning rather than an overall functioning as a summative score (Saltychev et al., 2021). These findings support our initial expectation that the various domains of functioning are differentially influenced by pre-, peri- and post-migration parameters. Our sample of RAS exhibits notable impairments in functioning, as the mean overall WHODAS 2.0 scores in the sample lie between the 80th and 90th percentile of population percentiles of the 12-item version (Ustun et al., 2012). Consistent with findings from other studies of RAS, older age is associated with disability, which might be due to the effects of physical aging (Mollica, 1999).
In particular, symptoms of depression and PTSD were linked to worse day-to-day functioning overall and in all functioning subdomains in RAS with psychological distress. The influence of potentially traumatic life events, which correlated poorly with PTSD symptom scores, is more complex. In this study, experiences of deprivation and of violence and abuse were associated with lower functioning, especially when people were asked if they had trouble in joining community activities and if they were emotionally affected by their health problems. Counter-intuitively, experiences of ‘being close to death’, e.g., witnessing murder/combat, were associated with lower WHODAS 2.0 scores, and significantly predicted better functioning in ‘self-care’ (personal hygiene and dressing oneself). A similar result has been found in people who were victims of torture, but with a very small impact (Laban et al., 2008). In this population of non-hospitalized RAS individuals, these results might be explained by a higher level of resilience in those who have managed to cope with such difficulties. Similarly, front line workers in the COVID-19 pandemic who exhibited high trait resilience were tolerating stressors better (Fino et al., 2021). Another mechanism could be seen in accounts of post-traumatic growth (PTG) after traumatic events, where individuals were able to maintain or even exceed their functioning facing adversity (Tedeschi and Calhoun, 2004). For refugees, evidence of PTG was reported in several studies (Sultani et al., 2024).
Generally, it is acknowledged that trauma is a critical harmful agent in many aspects of everyday functioning, which is well documented for different populations of RAS (Khan and Haque, 2021). These findings underline the necessity of recognizing that trauma effects on individual functioning may be multifactorial, and of always considering multiple influencing factors, such as symptoms of PTSD, family support and living conditions (Mollica, 1999). Disability in getting acquainted with living conditions and new people can maintain and even reinforce disadvantages, with consequences of prolonged suffering from mental health disorders (Friis Jørgensen et al., 2017).
Difficulties with living conditions post-migration were associated with worse functioning in concentrating and learning new tasks. Structuring one’s daily routines and being resilient are important assets in organizing one’s own day-to-day life, and difficult living arrangements, such as over-crowding, limited privacy and conflicts in large communal accommodations, may negatively interfere with these (Agbih, 2019). Another finding is that a higher number of children in the same household or living nearby was associated with worse ‘self-care’ and with worse functioning overall, which was previously described (Robertson et al., 2016). On the one hand, this could be explained by limited time resources when caring for under-aged children, and therefore having less time for fulfilling one’s own needs, also considering that finding childcare options for RAS is difficult. On the other hand - with women reporting having more children than men in our sample – this could be a reflection of differences between genders, as the majority of RAS in Türkiye were female, whereas RAS in Western European countries were predominantly male. Another study reported a stronger negative relationship between trauma and functioning for females than for males, which might add to the gender differences (Robertson et al., 2016).
Lastly, the observed association between experiences of violence and abuse, and lower abilities in participating in community activities could stem from certain stressors or definitive life events. Past exposure to traumatic events may lead the individual to be less inclined to want to participate, potentially posing a further barrier toward inclusion into the host society, especially as expectations that RAS should integrate with the community in host countries may further amplify individual stress, potentially leading to social exclusion.
As one strategy to prevent social exclusion, proficiency courses in the host country’s language could be combined with work training, day structure training and opportunities to mingle with local communities. Combined language and work training programs show promising results (Kuschel et al., 2023). Isolated language tandem programs have not been scientifically evaluated in RAS, gender differences must be taken into consideration in these populations. Female RAS’s relationship status and childcare situations have an impact on their language skills, which was not found for male RAS (Bernhard and Bernhard, 2022). Having fewer opportunities to learn than men, female RAS were more efficient in learning (Bernhard and Bernhard, 2022).
Strengths of this study are: firstly, a large sample size of RAS from many countries and settings: secondly, a methodologically exact screening procedure which rendered a comparably homogenous sample of RAS: thirdly, the nationalities included show that the sample was quite representative for current RAS populations in Europe and Türkiye until 2022. However, conclusions cannot be made for the general population of RAS in these regions, as we investigated a non-random sample under psychological distress and interested to receive an intervention. Limiting the study’s findings is foremost that the study was ideated for another type of analysis; in this sample, psychological functioning was primarily assessed as a secondary outcome. Secondly, the cross-sectional methodology does not warrant causality assumptions, and some associations could be explained by reverse causality. Thirdly, we did not assess physical health, which might have been an important predictor of psychological functioning in our sample. Fourthly, questionnaires derived from different versions of the DSM were used, which might limit their comparability. Generated hypotheses have to be reviewed in a longitudinal follow-up study.
This study underlines the need for the consideration of sub-clinical forms of war and trauma-associated disabilities, as patterns of functional impairment are even present in RAS without a clinical diagnosis of a mental health disorder. This finding might be taken into account in the organization of medical and psychosocial assistance to RAS. We hypothesize that reduced everyday functioning of individuals who had to leave their home country due to war, prosecution, and other hardships could hamper their ability to adapt successfully to new contexts, cope with new tasks and recover from their experiences.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by WHO Research Ethics Review Committee and Ethics Committees of all participating sites. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
JB: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. AR: Writing – review & editing, Visualization TW-T: Writing – review & editing. PW: Writing – review & editing. CB: Conceptualization, Funding acquisition, Project administration, Supervision, Writing – review & editing. MP: Writing – review & editing. FT: Data curation, Formal analysis, Supervision, Writing – review & editing. LT: Writing – review & editing. VR: Writing – review & editing. CA: Writing – review & editing. EU: Writing – review & editing. MA: Writing – review & editing. TL: Writing – review & editing. MV: Writing – review & editing. RC: Writing – review & editing. LW: Writing – review & editing. MS: Writing – review & editing. PC: Writing – review & editing. MK: Writing – review & editing. TK: Writing – review & editing. RW: Writing – review & editing. MCA: Conceptualization, Supervision, Writing – review & editing, Methodology, Validation. JW: Writing – review & editing, Conceptualization, Project administration, Supervision.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the European Commission, grant agreement n. 779255 (“RE-DEFINE: Refugee Emergency: DEFining and Implementing Novel Evidence-based psychosocial interventions”).
We thank all the people involved in the RE-DEFINE study for their work.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2023.1295031/full#supplementary-material
Supplementary Table S1 | Spearman correlations.
Acarturk, C., Uygun, E., Ilkkursun, Z., Carswell, K., Tedeschi, F., Batu, M., et al. (2022). Effectiveness of a WHO self-help psychological intervention for preventing mental disorders among Syrian refugees in Turkey: a randomized controlled trial. World Psychiatry 21, 88–95. doi: 10.1002/wps.20939
Agbih, S. (2019). Housing facilities for asylum seekers in Germany: ethical concerns regarding social exclusion, othering and negative effects on health. Eur. J. Pub. Health 29, 174–185. doi: 10.1093/eurpub/ckz185.174
American Psychiatric Association . (1994). Diagnostic and statistical manual of mental disorders. American Psychiatric Publishing, Arlington
American Psychiatric Association . (2013). Diagnostic and statistical manual of mental disorders. American Psychiatric Publishing, Arlington
Barbui, C., Tedeschi, F., Acarturk, C., Anttila, M., Au, T., Baumgartner, J., et al. (2023). Risk factors for mental disorder development in asylum seekers and refugees resettled in Western Europe and Turkey: participant-level analysis of two large prevention studies. Int. J. Soc. Psychiatry 69, 664–674. doi: 10.1177/00207640221132430
Bernhard, S., and Bernhard, S. (2022). Gender differences in second language proficiency—evidence from recent humanitarian migrants in Germany. J. Refug. Stud. 35, 282–309. doi: 10.1093/jrs/feab038
Blevins, C. A., Weathers, F. W., Davis, M. T., Witte, T. K., and Domino, J. L. (2015). The posttraumatic stress disorder checklist for DSM-5 (PCL-5): development and initial psychometric evaluation. J. Trauma. Stress. 28, 489–498. doi: 10.1002/jts.22059
Bovin, M. J., Marx, B. P., Weathers, F. W., Gallagher, M. W., Rodriguez, P., Schnurr, P. P., et al. (2016). Psychometric properties of the PTSD checklist for diagnostic and statistical manual of mental disorders–fifth edition (PCL-5) in veterans. Psychol. Assess. 28, 1379–1391. doi: 10.1037/pas0000254
Buchcik, J., Kovach, V., and Adedeji, A. (2023). Mental health outcomes and quality of life of Ukrainian refugees in Germany. Health Qual. Life Outcomes 21:23. doi: 10.1186/s12955-023-02101-5
Doré, I., and Caron, J. (2017). Mental health: concepts, measures, determinants. Sante Ment. Que. 42, 125–145. doi: 10.7202/1040247ar
Fino, E., Bonfrate, I., Fino, V., Bocus, P., Russo, P. M., and Mazzetti, M. (2021). Harnessing distress to boost growth in frontline healthcare workers during COVID-19 pandemic: the protective role of resilience, emotion regulation and social support. Psychol. Med. 53, 1–3. doi: 10.1017/S0033291721000519
Friis Jørgensen, S., A Auning-Hansen, M., Edward Ottesen Kennair, L., and Elklit, A. (2017). Can disability predict treatment outcome among traumatized refugees? Torture 27, 12–26. doi: 10.7146/torture.v27i2.97208
Goldberg, D. P., Gater, R., Sartorius, N., Ustun, T. B., Piccinelli, M., Gureje, O., et al. (1997). The validity of two versions of the GHQ in the WHO study of mental illness in general health care. Psychol. Med. 27, 191–197. doi: 10.1017/S0033291796004242
Khan, S., and Haque, S. (2021). Trauma, mental health, and everyday functioning among Rohingya refugee people living in short- and long-term resettlements. Soc. Psychiatry Psychiatr. Epidemiol. 56, 497–512. doi: 10.1007/s00127-020-01962-1
Kroenke, K., Spitzer, R. L., and Williams, J. B. W. (2001). The PHQ-9: validity of a brief depression severity measure. J. Gen. Intern. Med. 16, 606–613. doi: 10.1046/j.1525-1497.2001.016009606.x
Kuschel, A., Hansen, N., Heyse, L., and Wittek, R. P. M. (2023). Combining language training and work experience for refugees with low-literacy levels: a mixed-methods case study. J. Int. Migr. Integr. 24, 1635–1661. doi: 10.1007/s12134-023-01028-6
Laban, C. J., Gernaat, H. B. P. E., Komproe, I. H., van der Tweel, I., and de Jong, J. T. (2005). Postmigration living problems and common psychiatric disorders in Iraqi asylum seekers in the Netherlands. J. Nerv. Ment. Dis. 193, 825–832. doi: 10.1097/01.nmd.0000188977.44657.1d
Laban, C. J., Komproe, I. H., Gernaat, H. B. P. E., and de Jong, J. T. V. M. (2008). The impact of a long asylum procedure on quality of life, disability and physical health in Iraqi asylum seekers in the Netherlands. Soc. Psychiatry Psychiatr. Epidemiol. 43, 507–515. doi: 10.1007/s00127-008-0333-1
Li, S. S. Y., Liddell, B. J., and Nickerson, A. (2016). The relationship between post-migration stress and psychological disorders in refugees and asylum seekers. Curr. Psychiatry Rep. 18:82. doi: 10.1007/s11920-016-0723-0
Mollica, R. F. (1999). Disability associated with psychiatric comorbidity and health status in Bosnian refugees living in Croatia. JAMA 282, 433–439. doi: 10.1001/jama.282.5.433
Mollica, R., Caspi-Yavin, Y., Bollini, P., Truong, T., Tor, S., and Lavelle, J. (1992). The Harvard trauma questionnaire. Validating a cross-cultural instrument for measuring torture, trauma, and posttraumatic stress disorder in Indochinese refugees. J. Nerv. Ment. Dis. 180, 111–116. doi: 10.1097/00005053-199202000-00008
Morgan, G., Melluish, S., and Welham, A. (2017). Exploring the relationship between postmigratory stressors and mental health for asylum seekers and refused asylum seekers in the UK. Transcult. Psychiatry 54, 653–674. doi: 10.1177/1363461517737188
Nosè, M., Tarsitani, L., Tedeschi, F., Lotito, C., Massetti, P., Purgato, M., et al. (2020). Association of traumatic events with levels of psychological distress and depressive symptoms in male asylum seekers and refugees resettled in Italy. BMC Psychiatry 20:576. doi: 10.1186/s12888-020-02988-0
Oviedo, L., Seryczyńska, B., Torralba, J., Roszak, P., del Angel, J., Vyshynska, O., et al. (2022). Coping and resilience strategies among Ukraine war refugees. Int. J. Environ. Res. Public Health 19:13094. doi: 10.3390/ijerph192013094
Priebe, S., Giacco, D., and El-Nagib, R. (2016). Public health aspects of mental health among migrants and refugees: a review of the evidence on mental health care for refugees, asylum seekers and irregular migrants in the WHO European Region. WHO Regional Office for Europe. Denmark
Purgato, M., Carswell, K., Acarturk, C., Au, T., Akbai, S., Anttila, M., et al. (2019). Effectiveness and cost-effectiveness of self-help plus (sh+) for preventing mental disorders in refugees and asylum seekers in Europe and Turkey: study protocols for two randomised controlled trials. BMJ Open 9:e030259. doi: 10.1136/bmjopen-2019-030259
Purgato, M., Carswell, K., Tedeschi, F., Acarturk, C., Anttila, M., Au, T., et al. (2021). Effectiveness of self-help plus in preventing mental disorders in refugees and asylum seekers in Western Europe: a multinational randomized controlled trial. Psychother. Psychosom. 90, 403–414. doi: 10.1159/000517504
Rizzi, D., Ciuffo, G., Landoni, M., Mangiagalli, M., and Ionio, C. (2023). Psychological and environmental factors influencing resilience among Ukrainian refugees and internally displaced persons: a systematic review of coping strategies and risk and protective factors. Front. Psychol. 14:1266125. doi: 10.3389/fpsyg.2023.1266125
Robertson, C. L., Savik, K., Mathiason-Moore, M., Mohamed, A., and Hoffman, S. (2016). Modeling psychological functioning in refugees. J. Am. Psychiatr. Nurses Assoc. 22, 225–232. doi: 10.1177/1078390316641489
Sá, F. H. D. L., Waikamp, V., Freitas, L. H. M., and Baeza, F. L. C. (2022). Mental health outcomes in Syrian refugees: a systematic review. Int. J. Soc. Psychiatry 68, 933–953. doi: 10.1177/00207640221099404
Saltychev, M., Katajapuu, N., Bärlund, E., and Laimi, K. (2021). Psychometric properties of 12-item self-administered World Health Organization disability assessment schedule 2.0 (WHODAS 2.0) among general population and people with non-acute physical causes of disability – systematic review. Disabil. Rehabil. 43, 789–794. doi: 10.1080/09638288.2019.1643416
Salvo, T., and de C Williams, A. C. (2017). “If I speak English, what am I? I am full man, me”: emotional impact and barriers for refugees and asylum seekers learning English. Transcult. Psychiatry 54, 733–755. doi: 10.1177/1363461517746315
Sheehan, D., Lecrubier, Y., Harnett Sheehan, K., Janavs, J., Weiller, E., Keskiner, A., et al. (1997). The validity of the Mini international neuropsychiatric interview (MINI) according to the SCID-P and its reliability. Eur. Psychiatry 12, 232–241. doi: 10.1016/S0924-9338(97)83297-X
Silove, D., Sinnerbrink, I., Field, A., Manicavasagar, V., and Steel, Z. (1997). Anxiety, depression and PTSD in asylum-seekers: assocations with pre-migration trauma and post-migration stressors. Br. J. Psychiatry 170, 351–357. doi: 10.1192/bjp.170.4.351
Sleijpen, M., June ter Heide, F. J., Mooren, T., Boeije, H. R., and Kleber, R. J. (2013). Bouncing forward of young refugees: a perspective on resilience research directions. Eur. J. Psychotraumatology 4. doi: 10.3402/ejpt.v4i0.20124
Sultani, G., Heinsch, M., Wilson, J., Pallas, P., Tickner, C., and Kay-Lambkin, F. (2024). ‘Now I have dreams in place of the nightmares’: an updated systematic review of post-traumatic growth among refugee populations. Trauma Violence Abuse 25, 795–812. doi: 10.1177/15248380231163641
Tay, A. K., Rees, S., Miah, M. A. A., Khan, S., Badrudduza, M., Morgan, K., et al. (2019). Functional impairment as a proxy measure indicating high rates of trauma exposure, post-migration living difficulties, common mental disorders, and poor health amongst Rohingya refugees in Malaysia. Transl. Psychiatry 9:213. doi: 10.1038/s41398-019-0537-z
Tedeschi, R. G., and Calhoun, L. G. (2004). Target article: “posttraumatic growth: conceptual foundations and empirical evidence.”. Psychol. Inq. 15, 1–18. doi: 10.1207/s15327965pli1501_01
Topp, C. W., Østergaard, S. D., Søndergaard, S., and Bech, P. (2015). The WHO-5 well-being index: A systematic review of the literature. Psychother. Psychosom. 84, 167–176. doi: 10.1159/000376585
UNHCR . (2023). Global trends. Forced displacement in 2022. Available at: (https://www.unhcr.org/global-trends-report-2022).
Üstün, T. B., Chatterji, S., Kostanjsek, N., Rehm, J., Kennedy, C., Epping-Jordan, J., et al. (2010). Developing the world health organization disability assessment schedule 2.0. Bull. World Health Organ. 88, 815–823. doi: 10.2471/BLT.09.067231
Ustun, T. B., Kostanjesek, N., Chatterji, S., and Rehm, J., World Health Organization. (2012). Measuring health and disability: manual for WHO disability assessment schedule (WHODAS 2.0). World Health Organization, Geneva
World Health Organization . (2001). International classification of functioning, disability and health (ICF). Available at:(https://icd.who.int/dev11/l-icf/en).
Keywords: psychological functioning, refugee mental health, post-migration stressors, trauma, WHODAS 2.0, participation
Citation: Baumgartner JS, Renner A, Wochele-Thoma T, Wehle P, Barbui C, Purgato M, Tedeschi F, Tarsitani L, Roselli V, Acartürk C, Uygun E, Anttila M, Lantta T, Välimäki M, Churchill R, Walker L, Sijbrandij M, Cuijpers P, Koesters M, Klein T, White RG, Aichberger MC and Wancata J (2024) Impairments in psychological functioning in refugees and asylum seekers. Front. Psychol. 14:1295031. doi: 10.3389/fpsyg.2023.1295031
Edited by:
Man Cheung Chung, Zayed University, United Arab EmiratesReviewed by:
Edita Fino, University of Bologna, ItalyCopyright © 2024 Baumgartner, Renner, Wochele-Thoma, Wehle, Barbui, Purgato, Tedeschi, Tarsitani, Roselli, Acartürk, Uygun, Anttila, Lantta, Välimäki, Churchill, Walker, Sijbrandij, Cuijpers, Koesters, Klein, White, Aichberger and Wancata. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Josef S. Baumgartner, am9zZWYuYmF1bWdhcnRuZXJAbWVkdW5pd2llbi5hYy5hdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.