 Rebeca Robles1*
Rebeca Robles1* Sara Infante2
Sara Infante2 Miriam Feria2Iván Arango2Elsa Tirado2Andrés Rodríguez-Delgado2
Miriam Feria2Iván Arango2Elsa Tirado2Andrés Rodríguez-Delgado2 Edgar Miranda2
Edgar Miranda2 Ana Fresán3Claudia Becerra2
Ana Fresán3Claudia Becerra2 Raul Escamilla2Eduardo Angel Madrigal de León4
Raul Escamilla2Eduardo Angel Madrigal de León4- 1Global Mental Health Research Center, Ramón de la Fuente Muñiz National Institute of Psychiatry, Mexico City, Mexico
- 2Directorate of Clinical Services, Ramón de la Fuente Muñiz National Institute of Psychiatry, Mexico City, Mexico
- 3Laboratory of Clinical Epidemiology, Subdirectorate of Clinical Research, Ramón de la Fuente Muñiz National Institute of Psychiatry, Mexico City, Mexico
- 4General Directorate Ramón de la Fuente Muñiz National Institute of Psychiatry, Mexico City, Mexico
Introduction: Despite the propagation of virtual mental health services for vulnerable groups during COVID-19 pandemic, the implementation and evaluation of remote evidence-based practices (EBP) to manage them in low- and middle-income countries remains scarce. In the current study, we describe and evaluate the implementation process and clinical impact of brief, remote, manualized EBP for crisis intervention and suicide risk management among healthcare workers attending patients with COVID-19 (COVID-19-HCWs) in Mexico.
Methods: The implementation process comprised community engagement of volunteer mental health specialists, creation of new clinical teams with different disciplines and skills, intervention systematization through manuals and education through 4-h remote training as main strategies. Mexican COVID-19-HCWs who had used a free 24-h helpline rated their pre- and post-intervention emotional distress. Therapists recorded patients’ pre-intervention diagnosis, severity, and suicide risk, the techniques used in each case, and their post-treatment perception of COVID-19-HCWs’ improvement at the end of the intervention.
Results: All techniques included in the intervention manual were employed at least in one case (n = 51). At the beginning of the intervention, 65.9% of the COVID-19-HCWs were considered moderately ill or worse according to Clinical Global Impression-Severity (CGI-S) scores, whereas at the end, 79.4% of them were perceived as much or very much improved according to CGI-Improvement scores (CGI-I), and their emotional distress had been significantly reduced (p < 0.001).
Discussion: This prospective study provides evidence that implementation of remote EBP is feasible and useful to reduce emotional distress and suicide risk among COVID-19-HCWs from a middle-income country. However, this study was limited by lack of a control group, improvement ratings provided by therapists and non-anonymous satisfaction ratings.
Introduction
Healthcare workers attending patients with COVID-19 (COVID-19-HCWs) constituted one of the known vulnerable groups in terms of mental health problems (MHP) and suicide risk (Adhanom, 2020). Thus, in parallel with universal suicide prevention strategies designed for the entire population (Mann and Currier, 2011), selective interventions for this (and other vulnerable groups) had to be provided, including mental disorders and suicide risk assessment (Gunnell et al., 2020) as well as indicated evidence-based practices (EBP) targeting those experiencing emotional crises and suicidal risk.
Main examples of EPB for these purposes include psychological first aid (American Psychiatric Association, 1954; Vernberg et al., 2008; Corey et al., 2021), pharmacotherapy for mental disorders (Brent, 2016), brief cognitive-behavioral therapy (CBT) (DeCou et al., 2019), and safety planning (Stanley and Brown, 2012). which had to be adapted to ensure their safe implementation in the context of such highly contagious virus by increasing the development and use of helplines, telemedicine and other digital methods (Gunnell et al., 2020).
The propagation of remote mental health services during COVID-19 might expand access to mental health care during and beyond the pandemic (Wind et al., 2020; Zhou et al., 2020), which is unfortunately low among healthcare students and professionals, even among those with substantial risk factors for suicide (Givens and Tjia, 2002). Barriers to using face-to-face mental health services, which are often offered in institutions where healthcare students and professionals work, include lack of time and fear of documentation in academic or professional records. Such barriers might be solved through remote interventions (e.g., hotlines) not associated with these institutions.
Scientific evidence demonstrates that EBP have effectively been applied remotely to reduce distress and suicide risk in general population and in HCWs (Berrouiguet et al., 2018; Pospos et al., 2018; Reinhardt et al., 2019). According to a systematic review of studies carried out prior to the pandemic, Pospos et al. (2018), showed that web-based tools and mobile applications that incorporate techniques usually employed as part of psychological first aid and suicide prevention (e.g., deep breathing, cognitive-behavioral techniques to cope with unpleasant thoughts and emotions, development of a customized safety plan and grounding exercises), are useful to improve healthcare student’s and professional’s coping, thus mitigating psychological distress and suicide risk.
However, it is still necessary to increase research efforts on which methods are useful for achieving their effective implementation (adoption by clinicians) in the contexts in which they are applied (Wasserman et al., 2020) when significant changes in clinicians’ routine delivery methods (remote vs. face-to-face), and patients (HCW-COVID-19) are in place.
In line with this, according to the emerging field of implementation science of EBP—as opposed to the sciences for their development through clinical trials—, research in this field should be oriented toward understanding the methods for promoting their incorporation into clinical practice (Berrouiguet et al., 2018). Therefore, implementation studies typically focus on the impact of specific strategies on the rates and quality of use of EBP, the proportion of patients who attend a minimum number of treatment sessions, and the adaptations required to improve the implementation process.
The present study sets forth the results of the evaluation of the implementation process and clinical impact of remote EBP designed to address emotional crises and suicide risk in Mexican COVID-19-HCWs, as part of a country-level strategy coordinated by the Mexican Ministry of Health (through its National Institute of Psychiatry), in collaboration with the National Autonomous University of Mexico (UNAM) since the beginning of the COVID-19 pandemic in the country.
Specific objectives include describing: (1) COVID-19-HCWs’ help-seeking process (including their sociodemographic and professional profile, sources of referral and reasons for consultation), (2) COVID-19-HCWs’ MHP and suicide risk according to service providers, (3) the EBP most frequently used by providers (and the reasons for adopting them), (4) the clinical utility of the intervention according to providers (by comparing their perception of the severity of COVID-19-HCWs’ MHP at the start of the intervention with COVID-19-HCWs’ improvement at the end of it), and (5) the acceptability and clinical utility of the intervention according to users (by comparing COVID-19-HCWs’ pre-post perception of emotional distress).
Materials and methods
Participants: clinicians, and patients
A total of 18 clinicians voluntarily participated; 5 were psychiatrists attending cases with suicide risk and/or in need for pharmacotherapy in addition to psychological techniques; and 13 were psychologists with at least a master’s degree. The sample of patients comprised 51 Mexican COVID-19-HCWs over 18 years old who voluntarily agreed to participate in the study, be assessed by a mental health specialist before and after the intervention, and attended at least one intervention session, from April 17 to December 15, 2020, the period encompassing the clusters of cases scenario (when a country experiences cases clusters in time, geographic location, or common exposure; World Health Organization, 2020) and the community transmission scenario (when a country experiences larger outbreaks of local transmission; World Health Organization, 2020), including the first COVID-19 peak in Mexico.
Variables and measures
Sociodemographic, professional, and COVID-19-related variables were evaluated using self-report questions on subjects’ sex, age, marital status, education, profession, personal COVID-19 status, and the COVID-19 status of friends and relatives.
Contact, reason for consultation, and emotional distress
Each subject was asked how they had found out about the free 24-h helpline and the reason for their call. The answers to these open-ended questions were recorded in a previously designed format for patients seeking psychological crisis intervention and suicide risk management. They were subsequently coded for analysis. Emotional distress was assessed at the beginning and end of the intervention through the following sentence: “Which number best describes how much emotional distress you are experiencing right now, on a scale of 0 to 10?” (Almanza-Muñoz et al., 2008).
Diagnostic impression and overall clinical impression
Each mental health professional recorded their diagnostic impression and assessed the severity of the symptoms reported during the psychological crisis using the Clinical Global Impression (CGI)-Severity Scale (CGI-S), rated on a 7-point Likert scale ranging from 1 (normal) to 7 (among the most severely ill patients). At the end of the intervention, the CGI-Improvement Scale (CGI-I) was assessed. CGI-I scores range from 1 (very much improved) to 7 (very much worse) (Guy, 1976).
Suicide risk assessment
The level of suicide risk (mild, moderate, high) was assessed in keeping with the risk of suicide module of the Mini-International Neuropsychiatric Interview (MINI) (Sheehan et al., 1997; Ferrando et al., 1998), comprising six items with a yes/no answer. In addition, the type of intervention required was determined by the total number of the ten risk factors included in the SAD Persons scale (0–4 = ambulatory treatment, 5–19 = hospitalization) (Patterson et al., 1983; Comité de Consenso de Catalunya en Terapéutica de los Trastornos Mentales, 2005; Gobierno de Canarias, 2008).
Clinicians’ adoption of EBP
To determine the level of adoption of the manual and the need to incorporate new techniques, clinicians were asked to record the techniques used and the reasons for their use in every session and case in an ad hoc form designed for the study.
Acceptability of the Intervention was evaluated using three questions; two regarding the level of patients´ satisfaction with the contents and intervention modality (remote), and the degree of complexity of the intervention, to be answered on a 5-point Likert scale, where 0 = not at all satisfied/complex, 1 = not very satisfied/complex, 2 = moderately satisfied/complex, 3 = very satisfied/complex, and 4 = fully satisfied/complex. At the end, a dichotomous question (yes/no) was included on whether subjects would recommend the intervention to other health workers coping with COVID-19.
Procedures
Main implementation strategies and outcomes
Implementation strategies included community engagement (Pinto et al., 2021) of volunteer mental health specialists willing to attend COVID-19-HCWs (psychiatrists and psychologists from de National Institute of Psychiatry with extensive experience treating emotional crises and/or psychiatric urgencies), in order to warrantee the availability of sufficient professional resources and the creation of new clinical teams with different disciplines and skills (Powell et al., 2015); intervention systematization through manuals and education through 4-h. online training session (Powell et al., 2015) in order to strength their skills to implement remote EBP to address emotional crises and suicide risk; and allow better assessment of implementation and clinical outcomes (Pinto, 2013).
Training session’s topics, teaching strategies and time employed to each topic were: 1) Use of the intervention manuals (described below) through conference and group discussion on the application of each strategy to case vignettes (of HCWs in emotional crises and/or with suicide risk during the pandemic) during two hours, 2) Process for referring patients to a psychiatrist, different virtual clinics and services if needed, though conference and exemplification during 30 min, and 3) Administration of the instruments and recording the data for the study (including the additional techniques they considered necessary for each case), through conference, groups exercises applying instruments to case vignettes and recording data in corresponding Excel formats, during 90 min. At the end of the online training session on intervention and evaluation methods, a case vignette was presented to determine interrater reliability between clinicians in the assessment of the patients´ initial severity, suicide risk and improvement after intervention. The Fleiss’ kappa coefficient was determined with values over 0.80 obtained in all cases, reflecting an adequate level of agreement between clinicians.
The main expected implementation outcome was a high level of adoption of EBPs by clinicians. Secondly, we expected high patient satisfaction and significant clinical utility of the intervention. Thus, to be part of the study’s sample, the record of the techniques employed during intervention sessions must be totally complete, and the evaluations of patients´ clinical improvement and treatment satisfaction were not mandatory.
Remote recruitment, evaluation, and intervention
Mexican COVID-19-HCWs were invited to use the free 24-h helpline to cope with emotional crises and/or suicidal thoughts through several sources, including a brief online evaluation and referral to treatment tool (at the national COVID-19 website: coronavirus.gob.mx), which automatically delivered personal feedback after completion of valid, reliable scales, including specific contact information on virtual clinics and other specialized services, if required, (2) the coordinators or therapists of other national virtual clinics for COVID-19-HCWs, (3) the National Institute of Psychiatry’s website and social networks, (4) press conferences and remote meetings with COVID-19-HCWs and COVID-19 health care center authorities (mainly at congresses and academic sessions), and (5) posters at the entrance to the COVID-19 zones of COVID-19 health care centers.
The free 24-h helpline for managing emotional crises and/or suicidal thoughts was answered by one of the participating clinicians. All of them were equipped with a mobile phone to answer the helpline according to a scheduled agenda of days and hours to be covered by each one to cover the service 24 h. Then, clinicians and patients decided together the best way to communicate remotely, whether it was the phone or a session using a virtual platform (for example, Zoom).
Sociodemographic, professional, COVID-19-related variables, source of referral, reasons for consultation and emotional distress were registered at the beginning of the intervention, prioritizing the attention of the patients. At the end of first session, clinicians registered their diagnostic and overall clinical impression, as well as patients´ suicide risk.
Crisis intervention was delivered according to the operational manual for remote psychosocial care during the COVID-19 pandemic in Mexico (Álvarez et al., 2020), which include a detailed description of a psychological intervention in emergencies based on Crisis Intervention Model and Cognitive Behavioral Therapy. Table 1 includes a description of the content and adaptations for COVID-19 pandemic in each manual. Suicide risk was handled using Dialectic Behavioral Therapy techniques (such as TIPP and mindfulness skills), according Linehan’s (2014) DBT Skills training manual.
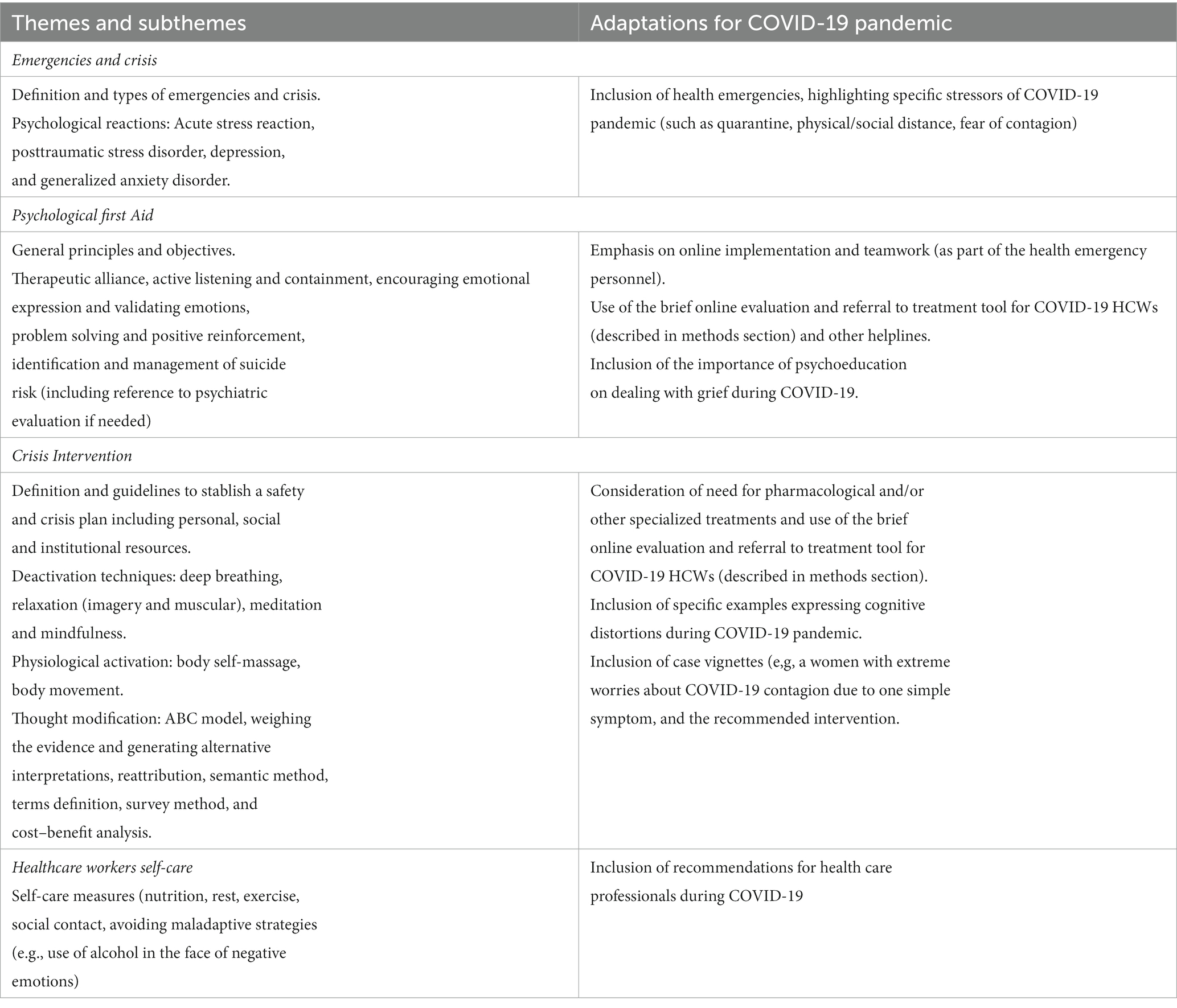
Table 1. Manual for crisis intervention (Álvarez et al., 2020): content and adaptations for COVID-19 pandemic.
However, therapists could use the techniques of their choice for each case, regardless of whether they were included in the intervention manuals, including pharmacotherapy for MHP, and hospitalization for severe cases. At the end of each session, clinicians recorded the techniques used and the reasons for their use, as well as new important information for case management if they considered it necessary (e.g., antecedents of mental health problems and psychological/pharmacological treatments, comorbidity, etc.). At the end of the intervention, clinicians registered patients´ global improvement and patients´ acceptability of the intervention.
Data analyses
All analyses were performed using SPSS-X v.21.0. All descriptive information was determined by frequencies and percentages for categorical variables and means and standard deviation for continuous variables.
Demographics, professional, COVID-19-related variables, reason for consultation (including suicide risk), diagnostic impression and CGI scores among HCWs were described as well as the frequency and percentage of sessions and the use of the techniques included in the intervention manual and the additional ones. We also recorded subjects’ degree of satisfaction with the contents and modality of the intervention, and perception of its complexity.
Emotional distress before and after the intervention (in those who finished the intervention and completed both evaluations) was compared using repeated-measures Student’s t-tests with a prefixed alpha value of p < 0.05. Cohen’s d for t-tests were obtained to determine the effect sizes of the comparisons.
Finally, a content analysis was conducted by categorizing the meanings (Kvale, 1996) of the reasons for the use of additional techniques, to reveal the reason for their use by the therapist.
Results
A total of 234 HCWs was attended in the virtual clinic for crisis intervention and suicide risk management during the period of the study. 183 HCWs were excluded from the study’s sample given the reports of their evaluations were not delivered by the treating psychotherapist given they did not have time to complete the records (in 150 cases) or patients did not accept to complete the evaluations for the study (n = 33). Reports of the remaining 51 HCWs were provided for the present study: 66.7% (n = 34) was women and the remaining 33.3% (n = 17) men, with a mean age of 36.4 (S.D. = 8.5, range 21–60) years. All of them began treatment but three (5.9%) dropped out (two after the first session and one after the fourth session), meaning that 48 (94.1%) completed the intervention. Of the latter, 51.0% (n = 25) failed to complete the questionnaire on the acceptability of the intervention arguing they did not have time to do so. Table 2 shows the main demographic, professional and COVID-19-related variables of the sample. None of the participants was receiving other types of mental health care during the study.
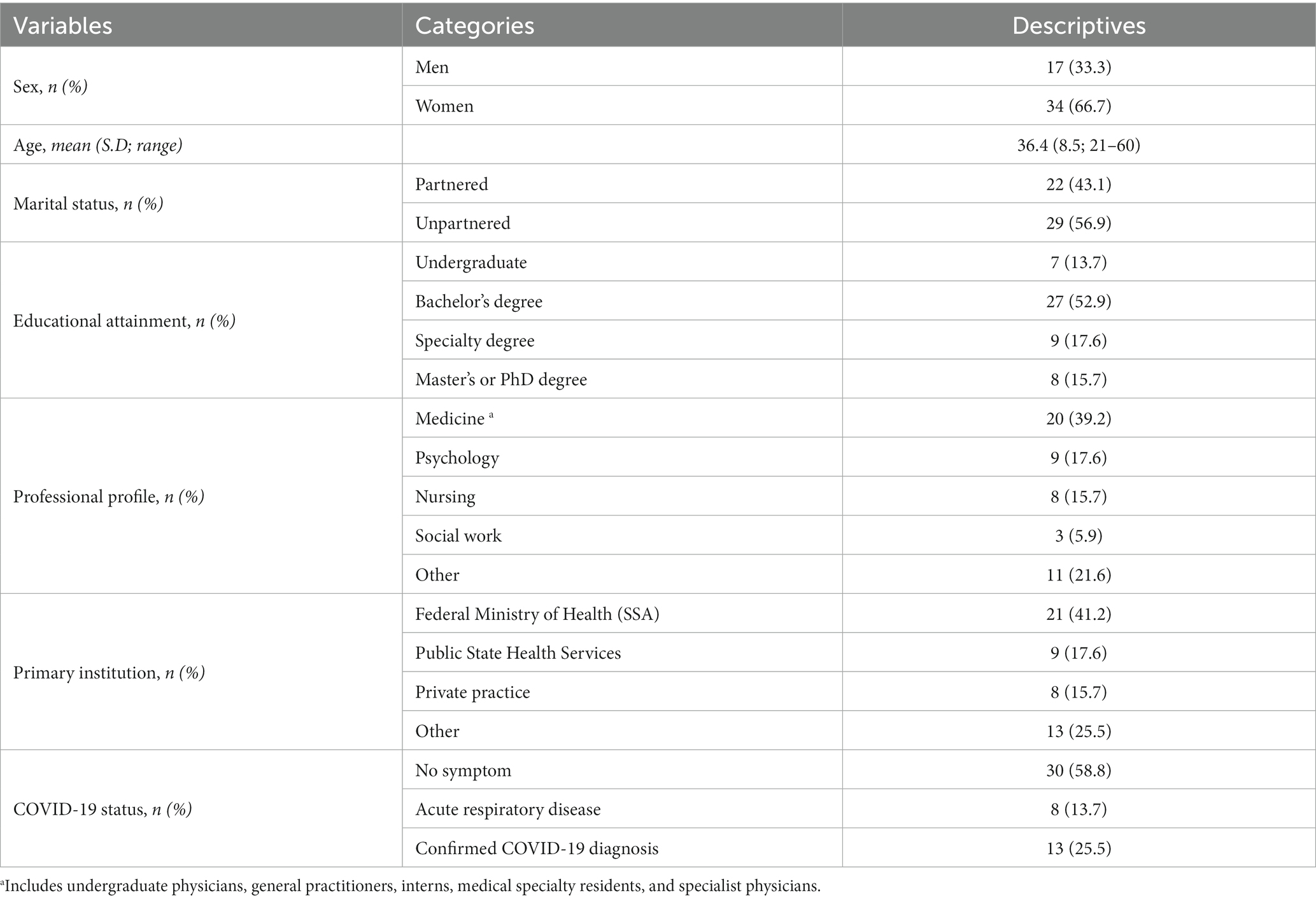
Table 2. Demographic, professional and COVID-19-related variables (n = 51).
As can be seen in Table 3, the most frequent source of referral to the helpline was another HCW. The main reasons for consultation included having tested positive for COVID-19 (n = 10, 21.3%) or the suspicion or fear of having COVID-19 (n = 9, 19.1%), as well as experiencing the death of close friends or loved ones from COVID-19 (n = 10, 21.3%). According to the mental health professionals answering the helpline, more than 60 % of the sample presented some form of depression (with or without anxiety symptoms), while nearly 30 % were at risk of suicide.
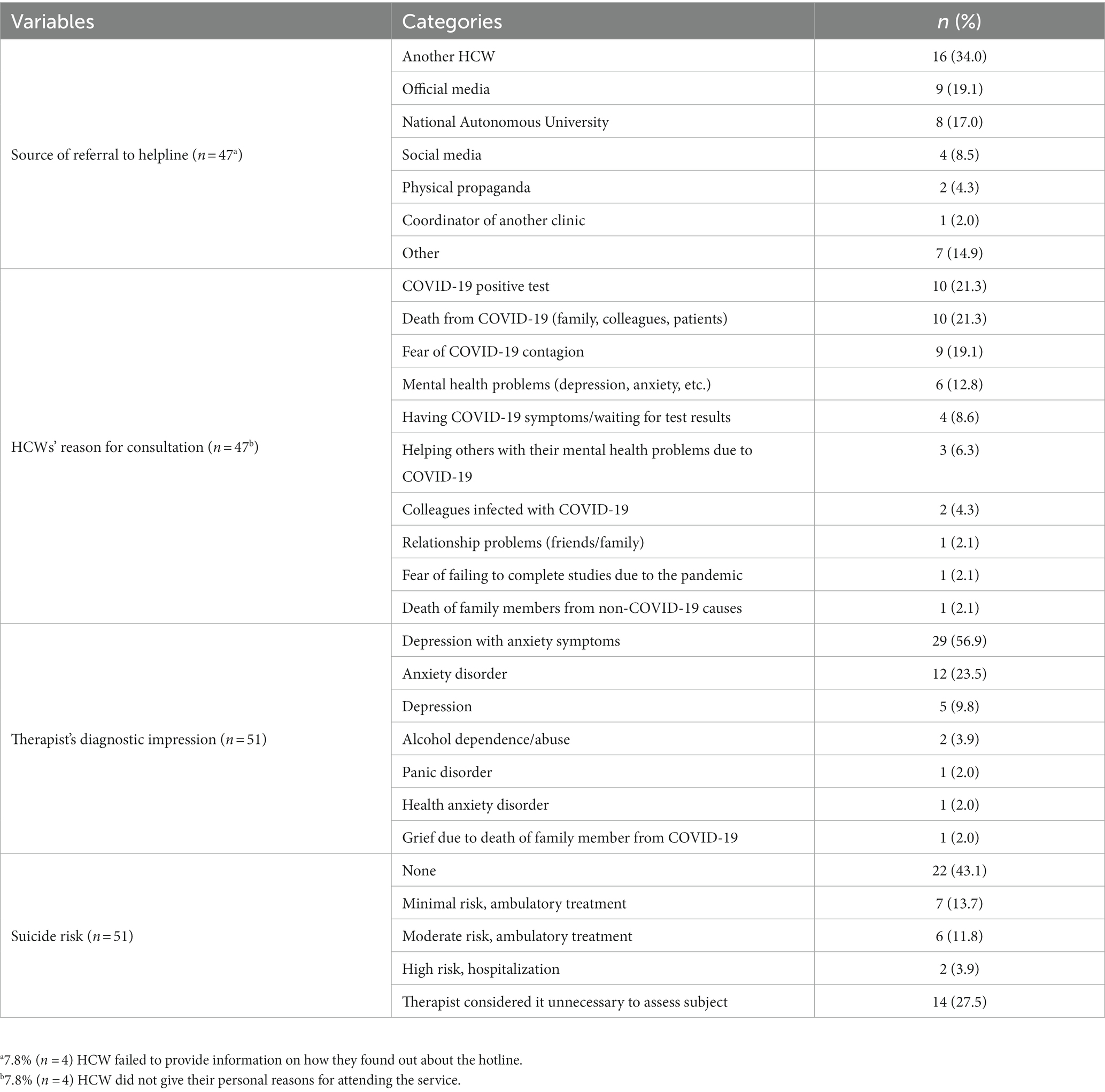
Table 3. Source of referral to helpline, reason for consultation, diagnostic impression, and suicide risk.
Intervention techniques
The number of sessions and techniques used for the subjects was reported, including those who dropped out of treatment. The average number of intervention sessions was 3.5 (S.D. = 2.5, range = 1–12); initial sessions were longer than follow up sessions (60 to 90 min vs. 40 to 60 min). Table 4 presents the frequency of use of the intervention techniques, comprising those contained in the manual, as well as those not included in it yet considered necessary for the cases under treatment by the therapist. Table 4 also shows the reasons for the use of these additional techniques, which are classified into three main categories: 1) Psychopharmacology, 2) Self-disclosure and 3) Use of metaphors.
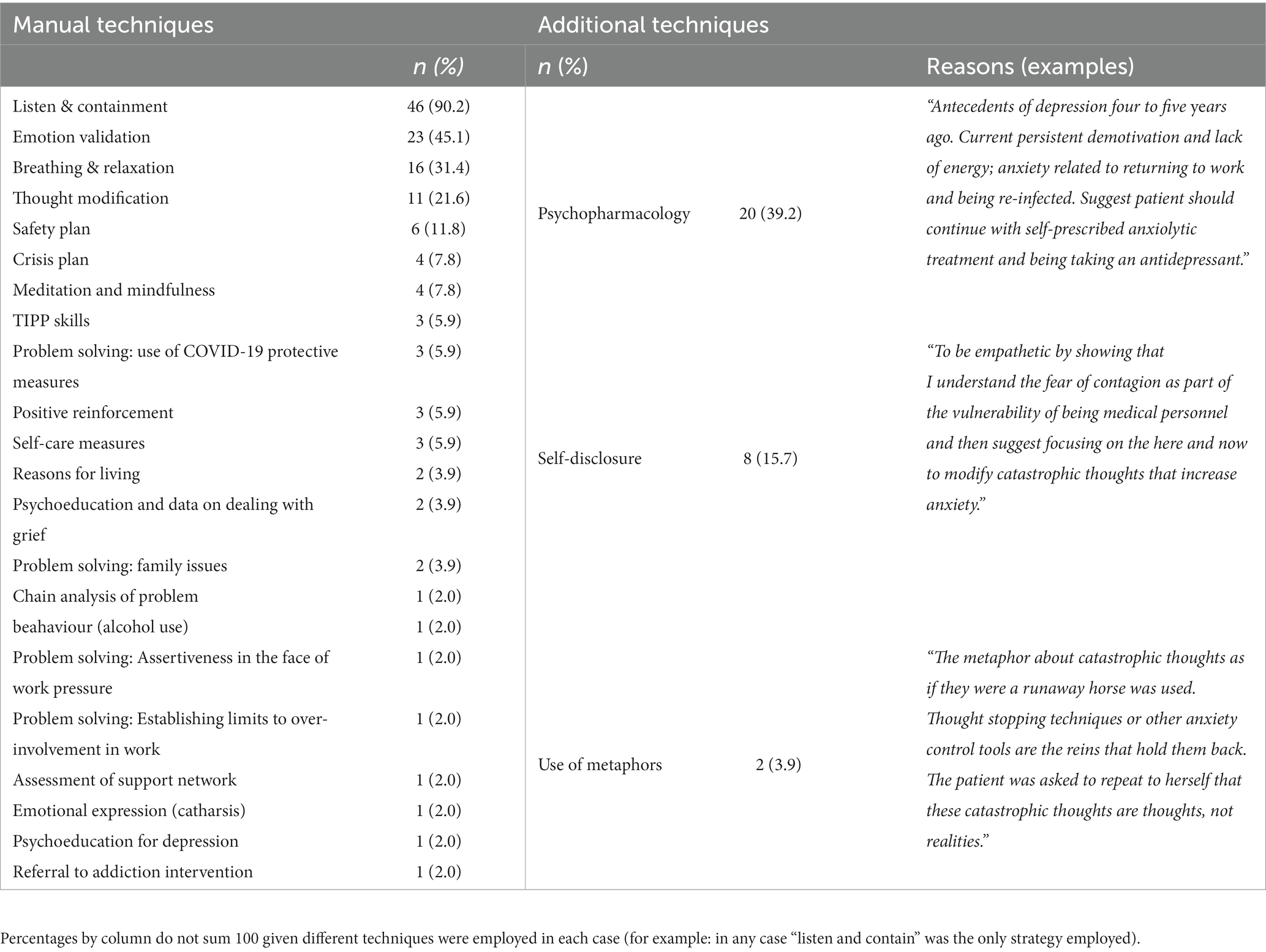
Table 4. Type, frequency of intervention techniques throughout sessions, reasons for use of additional techniques (n = 51), CGI and emotional distress assessment.
Clinical utility of the intervention
The CGI assessment at the beginning and end of the intervention and the comparison of the emotional distress experienced are included in Table 5. As can be seen, at the beginning of the intervention, more than half of the HCWs were classified as moderately ill, whereas by the end of the intervention, 79.4% were considered “very much” or “much” improved by the treating mental health professional. Seven women (23.3% of the total female participants) were classified as moderately to severely ill, while all men were assessed with lower illness severity (borderline moderately ill, to moderately ill), which is in line with women’s initial report of higher distress than men. However, at the end of the intervention, no differences in the distress experienced by sex were founded. Congruently, both women and men reported a significant reduction in emotional distress after the intervention, with “large” effect sizes according to Cohen’s d coefficients (Cohen, 1992). Interestingly, higher proportion of men reported being significantly improved (according to CGI-I scale) at the end of the intervention.
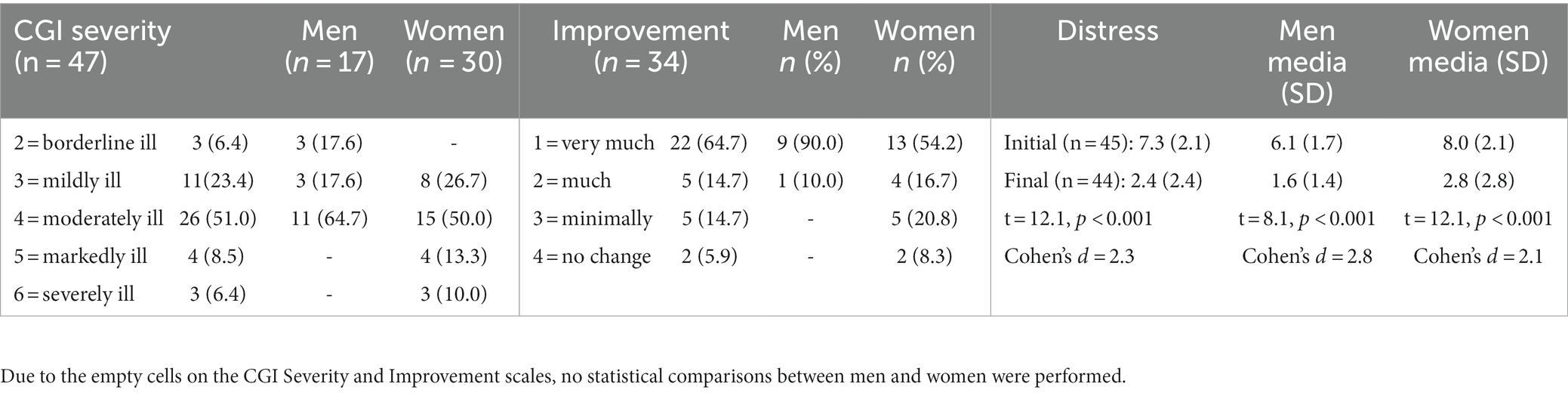
Table 5. Severity of mental health condition at the start of the intervention, improvement at the end of the intervention and HCWs’ pre-post perception of emotional distress: data from the total sample and by sex.
Acceptability of the intervention
Of the 48 HCWs who completed the intervention, a subsample of 26 reported their level of satisfaction with and perception of the complexity of the intervention. All of them (100%) stated that they were “totally satisfied” with the contents of the intervention. Moreover, the majority (n = 17, 65.4% of the subsample) answered that the intervention was “not complex” (followed by 19.2% (n = 5) who considered it “not very complex” and only 7.7% (n = 2) reported that it was “very complex.” All the subjects reported that they would recommend it to their colleagues. Almost all the HCWs were “totally satisfied” (n = 24, 92.3% of the subsample) or “very satisfied (n = 2, 7.7%) with the remote modality of the intervention.
Discussion
Present implementation study carried out a preliminary or basic evaluation of the utility of community engagement (Pinto et al., 2021), creation of new clinical teams, intervention systematization and education (Powell et al., 2015) as the implementation strategies to achieve clinicians´ adoption of remote EBP to address emotional crises and suicide risk, and therefore some indicators of significant clinical improvements and high levels of satisfaction with the intervention among a sample of COVID-19-HCWs in a middle income country (Mexico).
According to our results, these implementation strategies were useful to attain high rates of use of EBP, referred in implementation science as adoption level (Proctor et al., 2011). All techniques included in the intervention manual were employed at least in one of the 51 cases included in the study, particularly listening and providing containment (as a psychological first aid employed to help COVID-19-HCWs feel calm), which were adopted by clinicians to treat 90% of COVID-19-HCWs. This figure is in line with Buselli et al. (2020) previous report on the high perception (around 70%) of CBT techniques´ appropriates for the psychological care of Italian COVID-19-HCWs.
Moreover, the evaluation of the EBP´ level of adoption allows the exploration of specific techniques that are considered necessary to add by participating therapists (Proctor et al., 2011), which was expected given the need for psychological techniques to address patients in extraordinary stressful circumstances (Chen et al., 2020). In general terms, the manualized intervention might be improved by the addition of EBP considered relevant for this specific population and context (COVID-19-HCWs) by the mental health specialists providing treatment, including: a) pharmacological prescription and follow-up, which was recorded as a procedure in approximately 40 % of the sessions for treating moderate to severe MHP; and b) two psychological techniques that seems to be essential tools to treat people suffering significant stressors outside their control (e.g., regular direct contact with COVID-19 patients that increases their risk of contagion):
1) Therapist’s “self-disclosure” of personal worries and feelings of vulnerability to COVID-19 as a health professional. By cautiously modeling openness and sharing intense feelings, therapists can use self-disclosure to enhance patients’ perception of their warmth and connection with them, and elicit more self-disclosure and positive responses on the part of the patient (Henretty and Levitt (2010), dispelling the widespread myth about the inherent difficulty of establishing a therapeutic alliance in non-face-to-face interventions (Berger, 2017).
2) The “use of metaphors,” specially to encourage patients to employe the techniques to manage maladaptive thoughts and emotions (see an example of a therapist-generated metaphor that can be part of a stock of metaphors for this in Table 4). The use of metaphors has demonstrated to be an effective conceptual and clinical strategy to facilitate therapeutic communication (Stine, 2005), information processing (Otto, 2000) and constructive change (Lenrow, 1966), and has been referred to as one of the most important therapeutic tools (Törneke, 2017) available to psychotherapists from different therapeutic orientations, including CBT.
Besides, a significant clinical improvement (as a measure of intervention’s effectiveness) was registered in all COVID-19-HCWs, and nearly 80% managed to improve after the intervention (even though more than 65% were moderately to severely ill at the beginning of the intervention). Additionally, a subset of patients who provided reports on acceptance were “totally satisfied” with the contents of the intervention and would recommend it to their colleagues (referred in implementation science as acceptability level) (Proctor et al., 2011).
In sum, our results indicate that the brief, remote, evidence-based intervention was a feasible and acceptable manner to attend emotional distress in Mexican COVID-19-HCWs, and 79.4% of participants demonstrated a significant improvement. These findings are congruent with previous reports on the effectivity of remote crisis intervention (Berrouiguet et al., 2018; Reinhardt et al., 2019) and the utility of helplines providing psychological first aid to first respondents during emergencies (Pekevski, 2013).
Other interesting results regards to COVID-19-HCWs’ help-seeking process during emotional crises and suicide risk, which might help to understand the type of vulnerable HCWs that could be attending helplines in future emergencies, as well as the efforts needed to increase the use of mental health services among other vulnerable subgroups of HCWs. First, most of those seeking help were women and COVID-19-HCWs associated with the medical profession. Gender differences may be due to the well-known greater tendency to seek and receive mental health care in women than men (Oliver et al., 2005) and the higher prevalence of anxious, depressive and stress-related MHP in women than men (Seedat et al., 2009); and differences between the type of HCWs could be explained given in Mexico (Robles et al., 2021a), as in other countries (Vizheh et al., 2020), those with a medical profession had higher frequencies of all MHP than psychologists, nurses and social workers.
Second, the main source of referral to the helpline was another HCW, which adds to evidence on the increased receipt of mental health care among healthcare professionals when it is suggested by someone in their social network (Dew et al., 1991), and the utility of informing key people—such as human resource colleagues and managers—about the signs of MHP and suicide risk and the services available to individuals requiring them) (World Health Organization, 2014). An example of an effective method to do so in general population that might be useful for this purpose in the future is the Mental Health First Aid (MHFA) Training and Research Program (for a description see: Kitchener and Jorm, 2008).
Third, the most important reason for COVID-19-HCWs to seek help and attend the intervention was testing positive for COVID-19, which has been reported as one of the main predictive factors of MHP among Mexican COVID-19-HCWs (Robles et al., 2021b). Along these same lines, one of the most frequently reported measures required to cope with COVID-19 by COVID-19-HCWs was biosafety equipment (Chen et al., 2020).
Fourth, according to the participating clinicians, a high proportion of COVID-19-HCWs seeking help presented some form of depression (with or without anxiety symptoms) and nearly a third part were at risk of suicide. This is in congruence with previous reports on mental health problems in COVID-19-HCWs. In Mexico, for example, according to Robles et al. (2021a,b) depression was one of the main common mental disorders among COVID-19-HCWs since the cluster of cases to the commentary transmission scenarios of the pandemic. Moreover, those with depression and alcohol abuse or dependence were at moderate suicide risk (vs. minimal or none), which highlight the need for monitoring of HCWs with this comorbidity.
This study has several and significant limitations. First, its hybrid effectiveness-implementation design (Curran et al., 2012) without a control group provides only preliminary evidence regarding the utility of the EBP implementation strategies and of the interventions themselves, which must be confirmed through controlled randomized clinical trials for better comparison and interpretation of their effects. Additionally, the absence of a follow-up evaluation prevents determining result’s maintenance in the long-term, and therefore is highly recommended in future studies on the field.
Another limitation is that, given the recruitment and sample selection method (of volunteer COVID-19-HCWs who engage in remote crisis intervention and/or suicide management), the results regarding MHP and suicide risk among COVID-19-HCWs should not be taken as estimates of prevalence or other epidemiological parameters. Moreover, an examination of whether the patterns of COVID-19-HCWs’ help-seeking during emotional crises and periods of suicide risk noted in this study apply across cultures and languages is warranted to make generalized conclusions in this regard.
Additionally, use of techniques and CGI ratings was reported by therapists rather that unbiased observers/raters, self-reported patients´ stress was based only on one item, and ratings of patients´ satisfaction with the intervention were asked directly by therapists, which might increase patients´ social desirability. Further assessments solving these limitations would improve the clarity of the effects of the intervention.
Conclusion
The present study add evidence regarding the utility and acceptability of brief and remote crisis intervention and suicide risk management. Importantly, this evidence is produced among one highly vulnerable group in the context of a sanitarian emergency (COVID-19) and among inhabitants from middle-income countries, where scare information about the feasibility and effectivity of psychological interventions has been a constant (even more in the case of remote treatments). More women (than men), medicine undergraduate and graduate professionals (than other HCWs), moderately or more depressed seek this type of interventions, which substantially improve their mental health in nearly 80 % of the cases.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found at: https://1drv.ms/f/s!AmLeJVltqurSgQJjOeerQliEDMHB?e=KOBYfk.
Ethics statement
The study involved humans and was approved by Ramón de la Fuente Muñiz National Institute of Psychiatry Research Ethics Committee. The study was conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
RR: conceptualization, methodology, formal analysis, supervision, and writing – original draft. IS and FM: project administration, investigation, data curation, and writing – review & editing. AI, TE, R-DA, and MiE: investigation and writing – review & editing. FA: formal analysis, validation, and writing – review & editing. BC and ER: investigation, validation, and writing – review & editing. MAe: investigation, resources, and software. All authors contributed to the article and approved the submitted version.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We would like to thank Silvia Morales-Chainé, Juan-Manuel Quijada, Diana Tejadilla, Lorena Rodríguez Bores, Evalinda Barrón, Fátima Moneta and José Javier Mendoza for supporting the development of this Project nationwide.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Adhanom, G. T. (2020). Addressing mental health needs: an integral part of COVID-19 response. World Psychiatry 19, 129–130. doi: 10.1002/wps.20768
Almanza-Muñoz, J. J., Juárez, I. R., and Pérez, S. (2008). Traducción, adaptación y validación del Termómetro de Distrés en una muestra de pacientes mexicanos con cáncer. [Translation, adaptation and validation of the Distress Thermometer in a sample of Mexican cancer patients]. Revista Sanidad Militar. 62, 209–217.
Álvarez, J., Andrade, C., Vieyra, V., Esquivias, H., Merlín, I., Neria, R., et al. (2020). “Manual operativo del Curso Emergente para la Brigada de Atención Psicoemocional y Psicosocial a distancia durante la pandemia de la COVID- 19 en México” in Operational manual of the emerging course for the remote psycho-emotional and psychosocial care brigade during the COVID-19 pandemic in Mexico (Mexico City: Instituto Nacional de Psiquiatría Ramón de la Fuente Muñiz)
American Psychiatric Association . (1954). Psychological first aid in community disasters. Washington D.C.: American Psychiatric Association.
Berger, T. (2017). The therapeutic alliance in internet interventions: a narrative review and suggestions for future research. Psychother. Res. 27, 511–524. doi: 10.1080/10503307.2015.1119908
Berrouiguet, S., Larsen, M. E., Mesmeur, C., Gravey, M., Billot, R., Walter, M., et al. (2018). Toward mhealth brief contact interventions in suicide prevention: case series from the suicide intervention assisted by messages (SIAM) randomized controlled trial. JMIR Mhealth Uhealth 6:e8. doi: 10.2196/mhealth.7780
Brent, D. A. (2016). Antidepressants and suicidality. Psychiatr. Clin. N. Am. 39, 503–512. doi: 10.1016/j.psc.2016.04.002
Buselli, R., Baldanzi, S., Corsi, M., Chiumiento, M., Del Lupo, E., Carmassi, C., et al. (2020). Psychological care of health workers during the COVID-19 outbreak in Italy: preliminary report of an occupational health department (AOUP) responsible for monitoring hospital staff condition. Sustainability. 12:5039. doi: 10.3390/su12125039
Chen, Q., Liang, M., Li, Y., Guo, J., Fei, D., Wang, L., et al. (2020). Mental health care for medical staff in China during the COVID-19 outbreak. Lancet Psychiatry 7, e15–e16. doi: 10.1016/S2215-0366(20)30078-X
Comité de Consenso de Catalunya en Terapéutica de los Trastornos Mentales . (2005). Recomendaciones terapéuticas en los trastornos mentales: Conducta suicida. [Therapeutic recommendations in mental disorders: Suicidal behavior]. Mexico City: Ars Medica.
Corey, J., Vallières, F., Frawley, T., De Brún, A., Davidson, S., and Gilmore, B. (2021). A rapid realist review of group psychological first aid for humanitarian workers and volunteers. Int. J. Environ. Res. Public Health 18:1452. doi: 10.3390/ijerph18041452
Curran, G. M., Bauer, M., Mittman, B., Pyne, J. M., and Stetler, C. (2012). Effectiveness-implementation hybrid designs: combining elements of clinical effectiveness and implementation research to enhance public health impact. Med. Care 50, 217–226. doi: 10.1097/MLR.0b013e3182408812
DeCou, C. R., Comtois, K. A., and Landes, S. J. (2019). Dialectical behavior therapy is effective for the treatment of suicidal behavior: a meta-analysis. Behav. Ther. 50, 60–72. doi: 10.1016/j.beth.2018.03.009
Dew, M. A., Bromet, E. J., Schulberg, H. C., Parkinson, D., and Curtis, E. C. (1991). Factors affecting service utilization for depression in a white-collar population. Soc. Psychiatry Psychiatr. Epidemiol. 26, 230–237. doi: 10.1007/BF00788971
Ferrando, L., Bobes, J., Gilbert, J., Soto, M., and Soto, O. (1998). M.I.N.I. Mini international neuropsychiatric interview. Versión en español 5.0.0. DSM-IV. Madrid: Instituto IAP.
Givens, J. L., and Tjia, J. (2002). Depressed medical Students' use of mental health services and barriers to use. Acad. Med. 77, 918–921. doi: 10.1097/00001888-200209000-00024
Gobierno de Canarias (2008). “Consejería de Sanidad. Salud Mental en Atención Primaria” in Recomendaciones Para el abordaje de los trastornos más prevalentes: Conducta suicida. [recommendations for the approach of the most prevalent disorders: Suicidal behavior] (Canarias: Gobierno de Canarias)
Gunnell, D., Appleby, L., Arensman, E., Hawton, K., John, A., Kapur, N., et al. (2020). Suicide risk and prevention during the COVID-19 pandemic. Lancet Psychiatry 7, 468–471. doi: 10.1016/S2215-0366(20)30171-1
Guy, W. (1976). ECDEU assessment manual for psychopharmacology. Rockville: National Institute of Mental Health.
Henretty, J. R., and Levitt, H. M. (2010). The role of therapist self-disclosure in psychotherapy: a qualitative review. Clin. Psychol. Rev. 30, 63–77. doi: 10.1016/j.cpr.2009.09.004
Kitchener, B. A., and Jorm, A. F. (2008). Mental health first aid: an international programme for early intervention. Early Interv. Psychiatry 2, 55–61. doi: 10.1111/j.1751-7893.2007.00056.x
Kvale, S. (1996). Interviews. An introduction to qualitative research interviewing. Michigan: Sage Publications.
Lenrow, P. B. (1966). Use of metaphor in facilitating constructive behavior change. Psychol. Psychother. Theory Res. Pract. 3, 145–148. doi: 10.1037/h0087921
Mann, J. J., and Currier, D. (2011). “Evidence-based suicide prevention strategies” in Evidence-based practice in suicidology: A source book. eds. M. Pompili and T. Tatarelli (Cambridge, MA: Hogrefe Publishing), 67–87.
Oliver, M. I., Pearson, N., Coe, N., and Gunnell, D. (2005). Help-seeking behavior in men and women with common mental health problems: cross-sectional study. BJPsych. 186, 297–301. doi: 10.1192/bjp.186.4.297
Otto, M. W. (2000). Stories and metaphors in cognitive-behavior therapy. Cogn. Behav. Pract. 7, 166–172. doi: 10.1016/S1077-7229(00)80027-9
Patterson, W. M., Dohn, H. H., Bird, J., and Patterson, G. A. (1983). Evaluation of suicidal patients: the SAD PERSONS scale. Psychosomatics 24, 343–349. doi: 10.1016/S0033-3182(83)73213-5
Pekevski, J. (2013). First responders and psychological first aid. J Emerg Manag. 11, 39–48. doi: 10.5055/jem.2013.0126
Pinto, R. M. (2013). What makes or breaks provider–researcher collaborations in HIV research? A mixed method analysis of providers’ willingness to partner. Health Educ. Behav. 40, 223–230. doi: 10.1177/1090198112447616
Pinto, R. M., Park, S. E., Miles, R., and Ni Ong, P. (2021). Community engagement in dissemination and implementation models: a narrative review. Implement Res Pract. 2, 263348952098530–263348952098518. doi: 10.1177/2633489520985305
Pospos, S., Young, I. T., Downs, N., Iglewicz, A., Depp, C., Chen, J. Y., et al. (2018). Web-based tools and mobile applications to mitigate burnout, depression, and suicidality among healthcare students and professionals: a systematic review. Acad. Psychiatry 42, 109–120. doi: 10.1007/s40596-017-0868-0
Powell, B. J., Waltz, T. J., Chinman, M. J., Damschroeder, L. J., Smith, J. L., Matthieu, M. M., et al. (2015). A refined compilation of implementation strategies: result from the expert recommendations for implementing change (ERIC) project. Implement. Sci. 10:21. doi: 10.1186/s13012-015-0209-1
Proctor, E., Silmere, H., Raghavan, R., Hovmand, P., Aarons, G., Bunger, A., et al. (2011). Outcomes for implementation research: conceptual distinctions, measurement challenges, and research agenda. Admin. Pol. Ment. Health 38, 65–76. doi: 10.1007/s10488-010-0319-7
Reinhardt, I., Gouzoulis-Mayfrank, E., and Zielasek, J. (2019). Use of telepsychiatry in emergency and crisis intervention: current evidence. Curr. Psychiatry Rep. 21:63. doi: 10.1007/s11920-019-1054-8
Robles, R., Morales-Chainé, S., Bosch, A., Astudillo-García, C., Feria, M., Infante, S., et al. (2021a). Mental health problems among Covid-19 frontline healthcare workers and the other country-level epidemics: the case of Mexico. Int. J. Environ. Res. Public Health 19:421. doi: 10.3390/ijerph19010421
Robles, R., Rodríguez, E., Vega-Ramírez, H., Álvarez-Icaza, D., Madrigal, E., Durand, S., et al. (2021b). Mental health problems among healthcare workers involved with the COVID-19 outbreak. Braz J Psychiatry. 43, 494–503. doi: 10.1590/1516-4446-2020-1346
Seedat, S., Scott, K. M., and Angermeyer, M. C. (2009). Cross-national associations between gender and mental disorders in the World Health Organization world mental health surveys. Arc Gen Psychiatr. 66, 785–795. doi: 10.1001/archgenpsychiatry.2009.36
Sheehan, D. V., Lecrubier, Y., Harnett-Sheehan, K., Janavs, J., Weiller, E., Keskiner, A., et al. (1997). The validity of the Mini international neuropsychiatric interview (MINI) according to the SCID-P and its re-liability. Eur. Psychiatry 12, 232–241. doi: 10.1016/S0924-9338(97)83297-X
Stanley, B., and Brown, G. K. (2012). Safety planning intervention: a brief intervention to mitigate suicide risk. Cogn. Behav. Pract. 19, 256–264. doi: 10.1016/j.cbpra.2011.01.001
Stine, J. J. (2005). The use of metaphors in the Service of the Therapeutic Alliance and Therapeutic Communication. J. Am. Acad. Psychoanal. Dyn. Psychiatry 33, 531–545. doi: 10.1521/jaap.2005.33.3.531
Törneke, N. (2017). Metaphor in practice: A Professional’s guide to using the science of language in psychotherapy. Oakland, California: New Harbinger Publications.
Vernberg, E. M., Steinberg, A. M., Jacobs, A. K., Brymer, M., Watson, P. J., Layne, C. M., et al. (2008). Innovations in disaster mental health: psychological first aid. Prof Psychol Res Pr. 39, 381–388. doi: 10.1037/a0012663
Vizheh, M., Qorbani, M., Arzaghi, S. M., Muhidin, S., Javanmard, Z., and Esmaeli, M. (2020). The mental health of healthcare workers in the COVID-19 pandemic: a systematic review. J. Diabetes Metab. Disord. 19, 1967–1978. doi: 10.1007/s40200-020-00643-9
Wasserman, D., Iosue, M., Wuestefeld, A., and Carli, V. (2020). Adaptation of evidence-based suicide prevention strategies during and after the COVID-19 pandemic. World Psychiatry 19, 294–306. doi: 10.1002/wps.20801
Wind, T. R., Rijkeboer, M., Andersson, G., and Riper, H. (2020). The COVID-19 pandemic: the ‘black swan’ for mental health care and a turning point for e-health. Internet Interv. 20:100317. doi: 10.1016/j.invent.2020.100317
World Health Organization . (2014). Preventing suicide: a global imperative. Geneva: World Health Organization.
World Health Organization . (2020). Critical preparedness, readiness and response actions for COVID-19. Interim guidance. World Health Organization. Geneva
Keywords: crisis intervention, suicide, healthcare workers, COVID-19, e-mental health, implementation science
Citation: Robles R, Infante S, Feria M, Arango I, Tirado E, Rodríguez-Delgado A, Miranda E, Fresán A, Becerra C, Escamilla R and Madrigal de León EA (2023) Remote crisis intervention and suicide risk management in COVID-19 frontline healthcare workers. Front. Psychol. 14:1253179. doi: 10.3389/fpsyg.2023.1253179
Edited by:
Brooke Schneider, University Medical Center Hamburg-Eppendorf, GermanyReviewed by:
Massimo Tusconi, University of Cagliari, ItalyPaolo Meneguzzo, University of Padua, Italy
Copyright © 2023 Robles, Infante, Feria, Arango, Tirado, Rodríguez-Delgado, Miranda, Fresán, Becerra, Escamilla and Madrigal de León. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rebeca Robles, cmViZXJvYmxlc0BpbXAuZWR1Lm14; cmViZXJvYmxlc0Bob3RtYWlsLmNvbQ==