
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol., 19 January 2024
Sec. Psycho-Oncology
Volume 14 - 2023 | https://doi.org/10.3389/fpsyg.2023.1251049
This article is part of the Research TopicNeurobiological, Psychological, and Environmental Influences on Parenting and Child Development: An Inclusive and Interdisciplinary PerspectiveView all 11 articles
 Christian Heuser1,2,3*
Christian Heuser1,2,3* Juliane Nora Schneider4
Juliane Nora Schneider4 Lina Heier1,2,3,5,6
Lina Heier1,2,3,5,6 Nicole Ernstmann1,2,3
Nicole Ernstmann1,2,3 Hannah Nakata2,3Andrea Petermann-Meyer3,7Rebecca Bremen3,7
Hannah Nakata2,3Andrea Petermann-Meyer3,7Rebecca Bremen3,7 André Karger3,8
André Karger3,8 Andrea Icks9,10Tim H. Brümmendorf3,7Franziska Geiser3,4
Andrea Icks9,10Tim H. Brümmendorf3,7Franziska Geiser3,4Introduction: Estimated 50,000 minor children in Germany experience a newly diagnosed cancer in one of their parents every year. Family resilience has proven to be an important concept against life crises. However, little research exists regarding family resilience in the context of parental cancer with minor children. Based on the “Family Resilience Framework,” the aim of the study is to investigate the processes of family resilience of affected families. In addition, we explore which combinations of promoting family resilience processes can be characterized.
Methods: As part of the mixed-method quasi-experimental interventional study “F-SCOUT,” a qualitative content analysis was used to analyze the documentation of the “Family-Scouts” (a fixed contact person who advises, accompanies, and supports the families). Documentation was performed by families’ study inclusion (T0), after 3 months (T1) and 9 months (T2) concerning current family situation, organization of everyday life, emotional coping, open communication within the family, and planned tasks.
Results: The N = 73 families had between one and six children. In 58 (79%) families, the mother had cancer. In the course of the analysis, a category system with 10 main categories and 36 subcategories emerged. Family resilience processes were described to different extents. Combinations of categories promoting family resilience were characterized by the use of social resources, flexibility, economic resources, and open communication.
Discussion: The findings are consistent with existing assumptions about family resilience in terms of the importance of social resources, family cohesion, mutual support, flexibility, open communication, and psychological well-being. In contrast to the findings of previous research, spirituality, and collaborative problem-solving indicate less centrality here. In turn, the findings on economic resources and information-seeking provide a valuable addition to the family resilience literature in the context of parental cancer with minor children.
Clinical trial registration: ClinicalTrials.gov, identifier NCT04186923.
According to current estimates, 498,000 people receive a cancer diagnosis in Germany every year (Robert Koch-Institute, 2022a). Many of the patients do not face the diagnosis alone. A 2010 survey from the United States showed that 18% of cancer patients had minor children at initial diagnosis (Weaver et al., 2010). In Germany, 50,000 minor children experience a newly diagnosed parental cancer yearly, according to current estimates (Robert Koch-Institute, 2022b). Parental cancer affects not only the individual but the entire family (Veach and Nicholas, 1998). In addition to the negative impact of the diagnosis on the quality of life (Annunziata et al., 2013; Bellardita et al., 2013), well-being (Heinemann and Simeit, 2017), and mental health (Romer, 2007; Hinz et al., 2010; Nakaya et al., 2010; Götze et al., 2012) of individual family members, the disease affects both family functionality (Kühne et al., 2013) and relationships among family members (Drabe et al., 2013; DellaRipa et al., 2015). Furthermore, parental cancer can be associated with intense stress in children (Faccio et al., 2018). Compared with children in the general population, children of parents with a serious physical illness are about twice as likely to develop psychological symptoms (Romer, 2007). Among the most common of these are anxiety and depressive phenomena, and psychosomatic complaints. In addition, parental cancer can be a potentially traumatic experience for a growing child (Howell et al., 2016).
To support families with parental cancer in developing an adaptive approach to the disease, research has shifted from a deficit to a resource perspective (Buchbinder et al., 2009). The focus is often on resilience as a significant protective factor against stressful life events and crises (Seiler and Jenewein, 2019). The term resilience then primarily refers to “psychological resilience” (Bengel and Lyssenko, 2012; Kurz et al., 2014), which enables individuals to maintain or restore their mental health in the context of adverse circumstances and stresses (Kalisch, 2017). In oncology, research on resilience has focused primarily on individuals, finding positive associations between resilience and general well-being (Bajjani-Gebara et al., 2019) as well as higher quality of life and better mental health (Kurz et al., 2014; Molina et al., 2014; Li et al., 2016) of cancer patients. The concept of “maintaining mental health” in resilience research is often reduced to not developing psychiatric symptoms after confrontation with adversities (Hiebel et al., 2021). A developmental definition describes resilience as a positive adaptation process with the result of maintained or regained psychological and social functioning (Luthar et al., 2000). Masten adds that studying resilience should include a systemic approach, taking into account the networks of relationships and community support (Masten, 2001). Another definition by Yehuda views resilience as a reintegration of self that includes a conscious effort to move forward in an insightful integrated positive manner as a result of lessons learned from an adverse experience (Southwick et al., 2014). When transferring these concepts to family systems, a resilient family may well experience psychological distress, but will find ways to adapt to the new situation, activate networks, and maintain a positive outlook which allows the family members to move on as a family as well as in their individual lives.
Studies examining resilience in a family with parental cancer are scarce (Buchbinder et al., 2009; van Schoors et al., 2015). Family resilience is often operationalized as the healthy and successful functioning of a family following significant stress (Walsh, 2003; van Schoors et al., 2015). Within the family system, this includes dynamic, interactive, and familial processes (Faccio et al., 2018) that promote successful coping (Burgette, 2020) and adaptation to stresses and crises (Luthar et al., 2000; van Schoors et al., 2015). The processes of family resilience enable the family system to recover from crises, buffer stress, reduce the risk of dysfunction, and support optimal adjustment (Walsh, 2003).
In this research, the theoretical basis of understanding family resilience is the “Family Resilience Framework” (Walsh, 2003) which captures effective key family processes in crisis situations. According to Walsh, dynamic and effective family processes and associated interactions are central in the collective coping with a stressful life event like parental cancer (Walsh, 2003). The framework identifies three areas: (1) Family belief systems containing subcategories “Make meaning of adversity,” “Positive outlook” and “transcendence and spirituality”; (2) Family organizational patterns containing “Flexibility,” “Connectedness” and “Social and economic resources”; (3) Family communication / Problem solving containing “Clarity,” “Open emotional expression” and “Collaborative problem-solving.”
It has been emphasized by researchers in the past that families sometimes show remarkable resilience in dealing with the cancer of a family member (Gerhardt et al., 2007; Jantien Vrijmoet-Wiersma et al., 2008; Buchbinder et al., 2009; Chen et al., 2018). However, there is a lack of concrete research on the underlying processes of family resilience in families with parental cancer and minor children. Therefore, the aim of this study is to exploratively examine and describe which processes of family resilience take place in families with parental cancer and minor children. Of particular interest in this context are factors that help families to cope with the crisis. Hence, it will be investigated which, according to Walsh’s model, resilience-promoting (combinations of) family resilience categories can be observed.
The methods section is based on the “Consolidated criteria for reporting qualitative research (COREQ),” a 32-item checklist for interviews and focus groups (Tong et al., 2007), in order to support the validity and reliability of the qualitative content analysis.
This study is part of the larger mixed-method quasi-experimental interventional study “Family-SCOUT” (Comprehensive support for families with parental cancer – Family-SCOUT) supported by the German Innovation Fund and conducted at the Cancer Centers of the University Hospitals of Aachen, Bonn, and Düsseldorf between July 2018 and June 2022. The study followed a convergent-parallel mixed-methods design (O'Cathain et al., 2010). The intervention consisted of active outreaching, cross-sectional and cross-phase support for families with parental cancer and minor children by the so-called “Family-Scouts,” who are a fixed contact person who advises, accompanies, and supports the families concerning organizational, emotional, and communicative purposes and facilitates access to existing support services (Dohmen et al., 2021). The primary study aim was to examine the effectiveness of the intervention. Further information on the study design can be found elsewhere (Dohmen et al., 2021).
Families with parental cancer and minor children were consecutively recruited in the Centers for Integrated Oncology in the German University Hospitals Aachen, Bonn, and Düsseldorf. Inclusion criteria were a confirmed ICD-10 diagnosis of cancer in one parent, custody of at least one minor child (and/or one minor living in the household), age > 18 years, sufficient German language skills, membership of the cancer-diagnosed parent in German statutory health insurance, and written informed consent from at least the cancer diagnosed parent (or the existence of a written procuration for the healthy parent).
Here, data from the Center for Integrated Oncology Bonn is used. In the intervention group, the Family-Scouts accompanied the families throughout the course of the disease (or even after the death of the parental cancer patients). The Family-Scouts collected the data by completing standardized documentation forms (see Supplementary materials) at three time points which corresponded with the quantitative measurement time points: at study inclusion of the whole family (T0 baseline), 3 months (T1) and 9 months (T2) after study inclusion. The standardized documentation forms were completed after an appointment with the families at the appropriate time T0-T2. The duration of the accompaniment by the Family-Scout (=intervention) was individually adapted to the needs of the families. In this study, the targeted period was at least nine months. Termination of contact with the Family-Scouts or withdrawal of consent to the study resulted in a reduced number of completed documentation forms in some families.
The Family-Scouts documented the organizational, emotional, and communicative situation in the families of the intervention group on standardized documentation forms at the three time points T0-T2 (see Supplementary materials) with the help of open text formats or check boxes, e.g., concerning the situation of the families with regard to the disease, family characteristics, household management, care situation of the children, organizational factors, emotional coping with the disease, assessment of the (open) communication in the families, as well as work assignments and action plans to be derived (Dohmen et al., 2021).
VERBI MAXQDA 2020 software was used for analysis. The Family-Scouts documentation sheets were checked for completeness and matched by identification numbers over the three time points for each family. A structuring qualitative content analysis according to Kuckartz was conducted including seven phases (Kuckartz and Rädiker, 2020, 2022): (1) initiating text screening, (2) derivation of deductive main categories, here from the “Family Resilience Framework” (Walsh, 2003), (3) first coding of the whole data with the main categories, (4) coded segments of the main categories were compiled into lists and discussed, (5) coded segments of the main category were deductively [Family Resilience Framework (Walsh, 2003)] and inductively (by means of the data) systematized and differentiated into subcategories leading to a differentiated category system, (6) second coding of the whole data with the differentiated category system, and (7) in-depth analysis of main and subcategories, here concerning which processes of family resilience take place in families documented by the Family-Scouts were observable. Subsequently, it was examined which (combinations of) main and subcategories were coded that theoretically are resilience-promoting (according to Walsh’s model), sometimes with the help of complex code configurations to investigate multidimensional relationships between categories. To increase the validity of the qualitative content analysis, data were analyzed by two researchers (JNS, CH) independently with different professional backgrounds (psychology and sociology) and both with 3–8 years of experience in qualitative research and coding. Regular meetings were held during the coding process to discuss coding segments and category systems. Interrater reliability was based on Cohen’s Kappa calculation for a random sample of 10 families. The agreement was substantial (κ = 0.69).
IBM SPSS version 29 was used to analyze the sociodemographic data (age, number of children, age of parents, sex of the parental cancer patient) of the sample descriptively.
From the N = 78 families in the intervention group in Bonn, data for N = 73 families were available for analysis. Data on age and number of children were available for N = 70 families. The families had one to six children (M = 1.97, SD = 1.12) with an average age of M = 9.44 years (SD = 5.46, range 0–27). Sociodemographic data were available for N = 70 parental cancer patients and N = 57 cancer-free parents. Parental cancer patients were M = 46 years old (SD = 6.53, range 32–64) and cancer-free parents were M = 48 years old (SD = 7.43, range 31–62). In 58 (79%) families, the mother had cancer, in 16 (22%) the father, and in one (1%) family both parents. In 16 (22%) families the parent with cancer died during the approximately 9 months of intervention. In 11 families (15%), the support by the Family-Scouts had a duration shorter than 9 months, because Family-Scouts (in accordance with the families) saw no further need for support. 21 (29%) families broke off contact with the Family-Scouts over the course of the 9 months by no longer responding to their attempts to contact them. For 51 (70%) families three filled out documentation forms (T0, T1, T2) were available. All available and also incomplete documentation forms were analyzed.
In the course of the analysis, a category system with 10 main categories and 36 subcategories emerged. For each main category 0 to 8 subcategories were differentiated. The number of coded segments of the main categories ranged from 4 (Transcendence and Spirituality) to 208 (Social Resources). The complete coding tree is shown in Table 1. The Family Resilience Framework combines economic and social resources into one category. However, based on the data material and the inductive coding it was decided to separate this category into two.
(1) Family belief systems – Make meaning of adversity: The parental cancer disease was not described as meaningful per se to the Family-Scouts. Rather, the illness or the death of a parent was perceived as manageable or normalized.
(2) Family belief systems – Positive outlook: Confidence, hope, courage, and perseverance were demonstrated by many families. One pattern contained the acceptance of the disease and associated physical limitations, while the other pattern consisted in managing ambivalence through phases of repression or denial. For most of the families, psychological and emotional stress, as well as fear, sadness, helplessness, excessive demands, and despair, were evident in the documentation of the Family-Scouts.
(3) Family belief systems – Transcendence and spirituality: In the documentation forms of the Family-Scouts a few text passages associated with transcendence and spirituality were found. No subcategories were developed because there were only four coded segments. Spirituality and transcendence appeared in the form of mostly organizational help from other members of the religious community or social environment.
(4) Family organization patterns – Flexibility: The analysis showed that helpful aspects of flexibility, such as restructuring and adapting to the new situation as well as obtaining information about the disease, were often (inductively) found in the documentation. However, a few families found it difficult to adapt to the new living circumstances or were hardly or only moderately informed.
(5) Family organization patterns – Connectedness: Family connectedness varied greatly among the families. In some families, strong cohesion and/or mutual support was evident for the Family-Scouts. In others, however, there was little cohesion and no or a lack of mutual support. Some family members withdrew from joint family life. In addition, in some families, the parents were separated, and/or there were problems or conflicts in contact with each other.
(6) Family organization patterns – Social resources: There were numerous social resources. Family members and friends helped in the household, took the children to school, or looked after them when the parents did not have time for various reasons (e.g., chemotherapy, work). The professional support system, such as psycho-oncologists, psychotherapists, or the Family-Scouts, was also frequently used. However, there were also families that did not have or use social support.
(7) Family organization patterns – Economic resources: Some families were in sufficient financial positions with parents in steady employment or reporting financial reserves. Other families received financial support from the state or relatives. Unemployment, no financial reserves, or debt was also reported to the Family-Scouts and problematized.
(8) Family communication and problem-solving – Clarity: The family systems differed greatly in how openly they communicated about parental cancer or about other topics in general. The Family-Scouts reported a range from very open communication to intentional concealment.
(9) Family communication and problem-solving – Open emotional expression: The Family-Scouts documented that some families shared their emotions and dealt with each other empathically. In others, however, emotional closeness, control of emotions, or lack of emotional exchange was observed.
(10) Family communication and problem-solving – Collaborative problem-solving: Joint problem-solving was characterized by the joint development of solutions or the collective work on opportunities to solve a problem (e.g., by actively asking for help). In contrast, in families where problems concerning parental couple relationships arose, (couple) conflicts were not managed together and decisions were not made together.
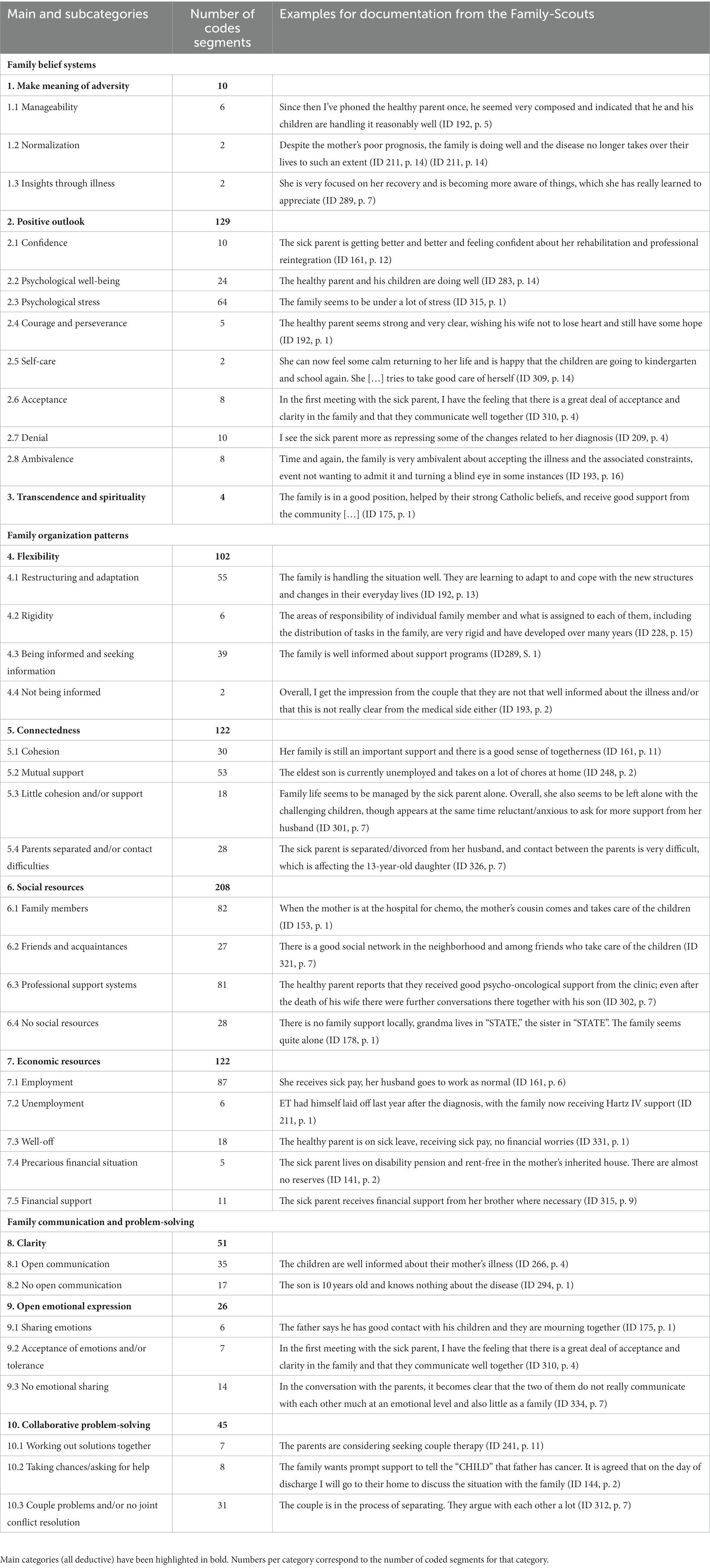
Table 1. Differentiated category system of family resilience of families with parental cancer and minor children (N = 73 families).
In the following, frequently coded combinations of main and subcategories of family resilience are described. Figure 1 shows a concept map of the frequently mentioned categories in the families. The main category with the most mentions was social resources (44 codings), followed by issues related to flexibility (24 codings) and economic resources (21 codings). Some text passages were also identified on positive outlook (14 codings) and family connectedness (13 codings).
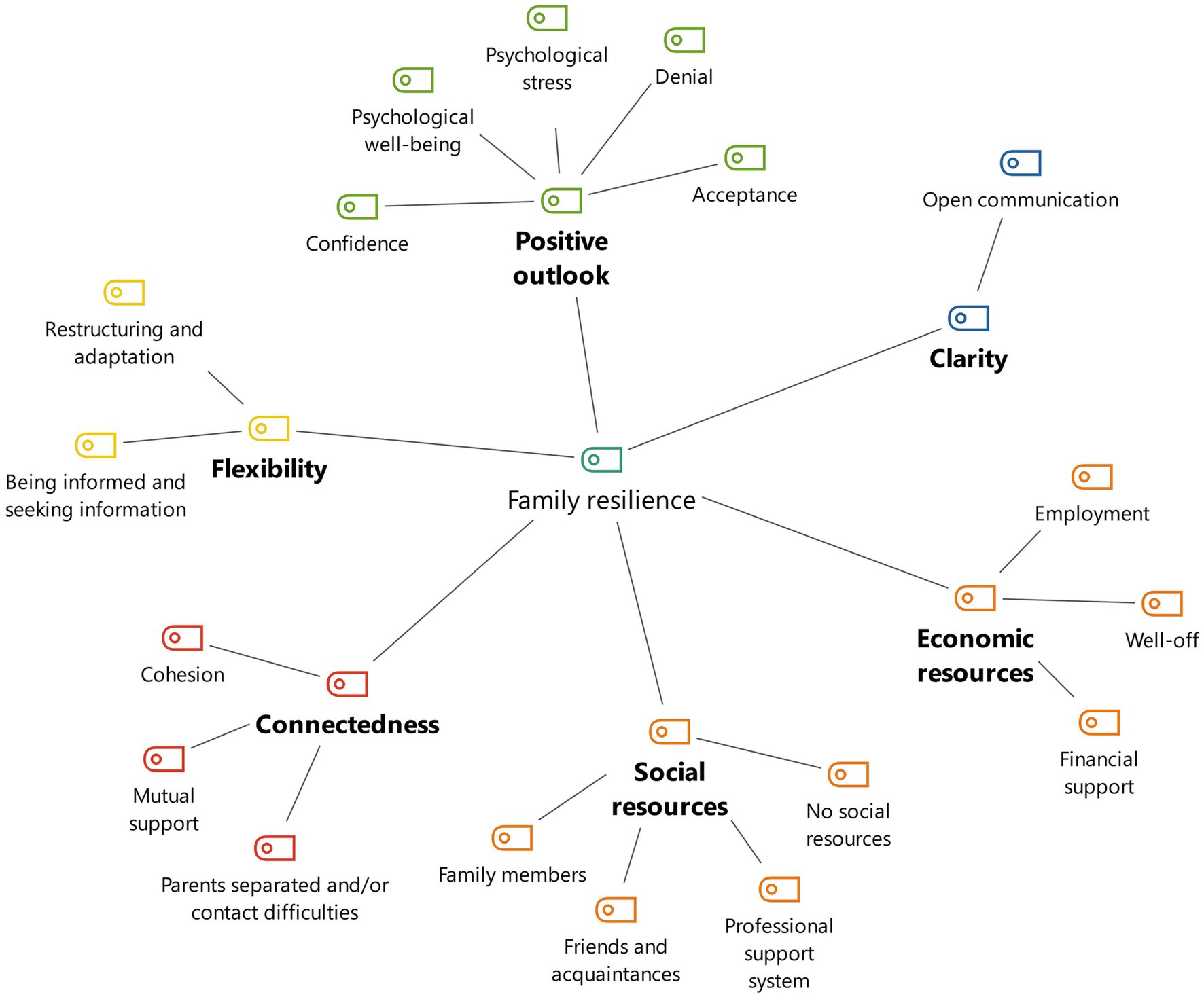
Figure 1. Concept map of the (combination of) family resilience categories that theoretically are resilience-promoting (according to Walsh’s model).
The Family-Scouts observed well-functioning social networks as well as experiencing support from family members (grandparents, aunts, siblings), friends or acquaintances, and professional help systems (Family-Scouts, home help, psycho-oncologists, psycho-therapists). The family members especially helped with child care and household tasks (e.g., shopping, cleaning).
The Family-Scouts observed adaptation to new life circumstances and flexible processes of restructuring everyday life. This included reducing work hours, restructuring daily routines, and also organizational flexibility (e.g., applying for rehabilitation, creating a living will and healthcare proxy, applying for sick pay). Families were also well informed about support services, treatment, and organizational matters or actively got in contact with the Family-Scouts to seek information on these topics. The children searched for information about parental cancer disease.
At least one parent either worked full-time, received sick pay, or was on parental leave. There were no reports of unemployment or financial problems.
The analysis made it clear that there was open communication within the families. The illness or death of a parent was discussed openly, and partners and children were well informed. No concealment or withholding of information was observed.
The aim of the study was to qualitatively investigate resilience in families with parental cancer and minor children as well as family resilience categories that are resilience-promoting. Therefore, deductive [Family Resilience Framework (Walsh, 2003)] and inductive structuring qualitative content analysis (Kuckartz and Rädiker, 2020, 2022) of the Family-Scouts documentation (Dohmen et al., 2021) of supported families was performed. We could identify specific resilience processes described to different extents present within the families. Promoting family resilience processes were identified as a combination of social resources, flexibility, economic resources, and open communication.
Overall, the findings regarding social resources, family cohesion, mutual support, flexibility, open communication, and psychological well-being as potential mechanisms for promoting resilience are consistent with existing assumptions about family resilience (Walsh, 2003; Visser et al., 2004; Black and Lobo, 2008; Choi and Yoo, 2015; Martin et al., 2015; Howard Sharp et al., 2017; Carr and Kellas, 2018). Open communication and psychological well-being that occurred in families in this study was also associated with resilience among family members in the cancer context (Carr and Kellas, 2018; Bajjani-Gebara et al., 2019).
Only few hints on transcendence and spirituality were identified in the Family-Scout documentation forms. This is in contrast to the results of previous research as spirituality was often attributed a central role in the resilience of a family (Black and Lobo, 2008; Martin et al., 2015). However, as spirituality or religiosity is assumed to interact highly with other resilience processes such as social resources (Bengel and Lyssenko, 2012), this could underlie the frequently confirmed positive relationship between spirituality and family resilience. The results of this study showed that spirituality was related to receiving social support, e.g., from the religious community. Furthermore, previous research attributed a key role in family resilience to collaborative problem-solving (Black and Lobo, 2008). In our sample, couple issues without collaborative problem-solving were mentioned frequently, even in families who otherwise showed many resilient processes. This may be due to the special situation of a family with one parent affected by cancer and minor children to care for, where role changes in different areas of life are especially difficult to manage for both parents (Hiltrop et al., 2021). Indeed, literature describing collaborative problem-solving as a core process of resilience has not focused on families affected by cancer (Black and Lobo, 2008).
Extensions of the specific context of this study emerged regarding the importance of economic resources and information-seeking. Literature has shown that satisfaction with the individual economic status contributed to the well-being of family members (McCubbin and McCubbin, 1988). A family’s economic resources may be used up in the course of parental cancer disease (Walsh, 2003) if the parent with primary income is no longer able to work due to the illness or if sick pay is insufficient to provide financial security for the family. Therefore, economic resources are an important consideration in the context of parental cancer with minor children (Phillips et al., 2021). Furthermore, information-seeking has also been found to promote resilience (Rutten et al., 2005). In the context of cancer, seeking disease-related information presumably has a more significant role than in other family crises (Walsh, 2003). This represents a possible explanation for the relevance of information-seeking found in this study through many inductive codings.
Families received social support from family members, friends, and professional support systems. This is consistent with findings in previous literature on the resilience of individuals (Bengel and Lyssenko, 2012) as well as families (Patterson, 2002; Black and Lobo, 2008). Resilient families are able to admit when they need help and turn to their social environment or professional support systems to get it (Walsh, 1998). Flexibility is also considered a widely researched core process of (family) resilience (Walsh, 2003; Black and Lobo, 2008; Martin et al., 2015). This is consistent with findings from this study. Families demonstrated flexible processes of restructuring to changing life circumstances with the cancer disease. Active seeking of information on topics such as diagnosis, treatment, possible support services, and social-legal issues was also observed. Previous literature on this topic has shown that parents of children with cancer demonstrated that they used information-seeking as a problem-focused coping strategy (Rutten et al., 2005). An important aspect of resilience among patients with chronic pain was characterized by a sense of control, which sometimes developed from information-seeking (Rolbiecki et al., 2017). Furthermore, economic security with income in the form of salary, sick pay, or parental benefits was coded as promoting family resilience. Resilience research in the family context has only addressed families’ economic resources to a limited extent, focusing here on the absence rather than the presence of this resource (Conger et al., 1990; Fogel, 2017). The findings of this study argue for not neglecting the importance of economic resources to the family resilience of families with parental cancer and minor children. The role of open communication within families which has been recognized in literature (Choi and Yoo, 2015; Carr and Kellas, 2018) was supported in the present research. Past research showed that open communication in families was characterized by directness, clarity, and honesty (Lindsey and Mize, 2001). In the face of parental cancer, clarification of information about topics such as diagnosis, treatment, side effects, and prognosis is particularly important, as a lack of open communication may cause children to fill existing gaps in knowledge about these topics with anxiety or even feeling guilty (Garmezy et al., 1984; Kühne et al., 2012; Faccio et al., 2018).
In this study, the relevance of the corresponding resilience processes was derived from the number of mentions in the documentation forms of the Family-Scouts (coded segments). It should be noted that some processes can be more easily observed by a person from outside the family (e.g., social and economic resources) and others are more difficult to observe (open expression of emotions within the family, spirituality). The Family-Scouts commented on difficulties in assessing such issues in their documentation forms. Furthermore, processes such as transcendence and spirituality are not consistently defined in the literature (Walach, 2022). Therefore, it can be assumed that the number of mentions in the documentation forms does not automatically indicate the actual relevance of the corresponding resilience processes. One important example of this limitation might be the category “religion and spirituality”: religion and spirituality tend to be private matters in Germany and are rarely addressed in everyday discourse and patient care. This topic could be better explored with qualitative interviews than with routine documentations by the Family-Scouts (social workers).
Social support was possibly asked about more actively, so that only at this point, for example, an involvement in a religious community became clear. Termination of contact with the Family-Scouts or withdrawal of consent to the study resulted in a reduced number of completed documentation forms in some families. However, in order to increase the validity of the qualitative content analysis conducted, the data were analyzed by two researchers with different professional backgrounds (psychology and sociology), and in case of discrepancies an agreement was reached before data analysis. Furthermore, the data are based on documentation within one cancer center in Germany. The generalizability of the results is limited to families with an oncological disease who were treated at this university hospital in Germany. Nevertheless, data on family resilience of families with parental cancer and minor children is very rare, and here, unique data from a new intervention (“F-SCOUT” study) could be qualitatively analyzed with common qualitative methods.
The study showed that Walsh’s framework of family resilience (Walsh, 2003) can be applied to families with parental cancer and minor children and contributes to an improved understanding of how resilience can emerge and be supported in families. The resilience process, i.e., finding a way to adapt positively to the new situation created by the cancer disease (Luthar et al., 2000), and being able to move consciously forward as a family in this situation (Southwick et al., 2014), was connected to social and economic resources, flexibility, and open communication. As changes in resilience could not be analyzed over the three measurement points, future studies can address this research gap. The results also underline the importance of information-seeking as an important process of coping with cancer disease (Rutten et al., 2005). Long-term mental health outcomes might be affected as (family) resilience has been associated with higher subjective well-being (Bajjani-Gebara et al., 2019), stress coping abilities (Patterson, 2002; Connor and Davidson, 2003), and higher quality of life (Kurz et al., 2014; Molina et al., 2014; Li et al., 2016) of cancer patients and their relatives. The findings can also serve as inspiration for future research by providing starting points for the formulation of quantitative hypotheses, e.g., concerning health outcomes for individual family members or on family level. They may provide a basis for the development of a questionnaire assessing resilience in families with parental cancer and minor children. They may also help to adapt previous questionnaires for assessing family resilience (Walsh, 2003; Zhou et al., 2020).
The results provide practical implications for how healthcare providers (HCP) can support families with parental cancer and minor children. HCP should be sensitized for families with parental cancer and minor children in general. Furthermore, as information-seeking is a possible resilience-building process, this is an opportunity for HCP to effectively support families by providing disease-related (evidence-based) information. A focus on families with less developed resilience processes can help identify families at risk early and offer them increased support. Also, potential consequences such as the impact on minor children (Flechtner et al., 2011; Heinemann and Simeit, 2017) could be more specifically regulated in prevention programs as resilience-based interventional studies show positive results in reducing psychopathology in children (Garmezy et al., 1984; Fritz et al., 2018). Within the German healthcare system, the interprofessional care of affected families seems important as resilience has emerged as an important element of psychological care for cancer patients (Molina et al., 2014). Examples include social support from healthcare workers (e.g., Family-Scouts), interventions to promote restructuring and adjustment, and providing information about the disease, its treatment, and possible support services. Family discussions to promote open communication could also help affected families develop an adaptive approach to the disease and its associated challenges (Zomerlei, 2015; Lundquist, 2017). Financially less well-off family systems with a parent with cancer could be strengthened by access to governmental financial assistance. These findings provide insights and support for intervention and prevention approaches to strengthen family resilience in families with parental cancer and minor children.
The study indicates that family resilience processes describe and analyze challenges of families with parental cancer and minor children in a comprehensive and multidimensional way. For HCP this might help to better understand the functioning of families entrusted to their care. For researchers this might help to provide insights and support for intervention and prevention approaches to strengthen family resilience in families with parental cancer and minor children. The findings are consistent with existing assumptions about family resilience (Walsh, 2003; Choi and Yoo, 2015) in terms of the importance of social resources, family cohesion, mutual support, flexibility, open communication, and psychological well-being. In contrast to the results of previous research (Black and Lobo, 2008; Martin et al., 2015), the findings on spirituality and collaborative problem-solving in this study indicate less importance. In turn, the findings on economic resources and information-seeking provide a valuable extension to the literature in the context of families with parental cancer and minor children. Further research on resilience in these families is needed especially to provide guidance for integrating findings into clinical practice (Veach and Nicholas, 1998; Visser et al., 2004; van Schoors et al., 2015).
The raw data supporting the conclusions of this article will be made available by the authors on reasonable request, without undue reservation.
The studies involving humans were approved by the Ethics Committee of the Medical Faculties of the RWTH Aachen University (EK195/18), University of Bonn (267/18) and the Heinrich-Heine University Düsseldorf (2018-215). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by all participants themselves or the participants’ legal guardians/next of kin.
AP-M, NE, TB, FG, AI, and AK contributed to the conception and design of the study. RB, AP-M, CH, LH, HN, AK, and FG organized the database. CH and JS performed the data analysis. CH, JS, LH, NE, HN, AP-M, RB, and FG interpreted the results. CH, JS, and FG wrote the first draft of the manuscript. All authors commented and revised the manuscript critically and contributed to the manuscript revision, read, and approved the submitted version.
The study was supported by the German Innovation Fund from the Federal Joint Committee, grant number 01NVF17043 [Innovationsfonds des Gemeinsamen Bundesausschusses (G-BA), Förderkennzeichen 01NVF17043].
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2023.1251049/full#supplementary-material
Annunziata, M. A., Muzzatti, B., Mella, S., and Bidoli, E. (2013). Fatigue, quality of life, and mood states during chemotherapy in Italian cancer patients. Tumori J. 99, e28–e33. doi: 10.1177/030089161309900129
Bajjani-Gebara, J., Hinds, P., Insel, K., Reed, P., Moore, K., and Badger, T. (2019). Well-being, self-transcendence, and resilience of parental caregivers of children in active Cancer treatment: where do we go from Here? Cancer Nurs. 42, E41–E52. doi: 10.1097/NCC.0000000000000662
Bellardita, L., Rancati, T., Alvisi, M. F., Villani, D., Magnani, T., Marenghi, C., et al. (2013). Predictors of health-related quality of life and adjustment to prostate cancer during active surveillance. Eur. Urol. 64, 30–36. doi: 10.1016/j.eururo.2013.01.009
Bengel, J., and Lyssenko, L. (2012). Resilienz und psychologische Schutzfaktoren im Erwachsenenalter. Stand der Forschung zu psychologischen Schutzfaktoren von gesundheit im Erwachsenenalter. [resilience and psychological protective factors in adulthood. State of research on psychological protective factors of health in adulthood]. Köln: Bundeszentrale für gesundheitliche Aufklärung.
Black, K., and Lobo, M. (2008). A conceptual review of family resilience factors. J. Fam. Nurs. 14, 33–55. doi: 10.1177/1074840707312237
Buchbinder, M., Longhofer, J., and McCue, K. (2009). Family routines and rituals when a parent has cancer. Fam. Syst. Health 27, 213–227. doi: 10.1037/a0017005
Burgette, J. M. (2020). Family resilience and connection is associated with dental caries in US children. JDR Clin. Transl. Res. 7, 61–70. doi: 10.1177/2380084420982250
Carr, K., and Kellas, J. K. (2018). The role of family and marital communication in developing resilience to family-of-origin adversity. J. Fam. Commun. 18, 68–84. doi: 10.1080/15267431.2017.1369415
Chen, C.-M., Du, B.-F., Ho, C.-L., Ou, W.-J., Chang, Y.-C., and Chen, W.-C. (2018). Perceived stress, parent-adolescent/young adult communication, and family resilience among adolescents/young adults who have a parent with cancer in Taiwan: a longitudinal study. Cancer Nurs. 41, 100–108. doi: 10.1097/NCC.0000000000000488
Choi, E. K., and Yoo, I. Y. (2015). Resilience in families of children with down syndrome in Korea. Int. J. Nurs. Pract. 21, 532–541. doi: 10.1111/ijn.12321
Conger, R. D., Elder, G. H., Lorenz, F. O., Conger, K. J., Simons, R. L., Whitbeck, L. B., et al. (1990). Linking economic hardship to marital quality and instability. J. Marriage Fam. 52:643. doi: 10.2307/352931
Connor, K. M., and Davidson, J. R. T. (2003). Development of a new resilience scale: the Connor-Davidson resilience scale (CD-RISC). Depress. Anxiety 18, 76–82. doi: 10.1002/da.10113
DellaRipa, J., Conlon, A., Lyon, D. E., Ameringer, S. A., Lynch Kelly, D., and Menzies, V. (2015). Perceptions of distress in women with ovarian Cancer. Oncol. Nurs. Forum 42, 292–300. doi: 10.1188/15.ONF.292-300
Dohmen, M., Petermann-Meyer, A., Blei, D., Bremen, R., Brock-Midding, E., Brüne, M., et al. (2021). Comprehensive support for families with parental cancer – Family-SCOUT: Study protocol for the evaluation of a complex intervention. Med. Psychol. doi: 10.21203/rs.3.rs-401056/v1
Drabe, N., Wittmann, L., Zwahlen, D., Büchi, S., and Jenewein, J. (2013). Changes in close relationships between cancer patients and their partners. Psycho-Oncology 22, 1344–1352. doi: 10.1002/pon.3144
Faccio, F., Ferrari, F., and Pravettoni, G. (2018). When a parent has cancer: how does it impact on children's psychosocial functioning? A systematic review. Eur. J. Cancer Care 27:e12895. doi: 10.1111/ecc.12895
Flechtner, H. H., Krauel, K., Simon, A., Krause-Hebecker, N., and Romer, G. (2011). Kinder krebskranker Eltern. [children of parents with cancer]. Nervenheilkunde 30, 10–157. doi: 10.1055/s-0038-1627793
Fogel, S. J. (2017). Amid the storm, surviving and thriving. Fam. Soc. 98, 255–257. doi: 10.1606/1044-3894.2017.98.32
Fritz, J., De Graaff, A. M., Caisley, H., van Harmelen, A.-L., and Wilkinson, P. O. (2018). A systematic review of amenable resilience factors that moderate and/or mediate the relationship between childhood adversity and mental health in young people. Front. Psych. 9:230. doi: 10.3389/fpsyt.2018.00230
Garmezy, N., Masten, A. S., and Tellegen, A. (1984). The study of stress and competence in children: a building block for developmental psychopathology. Child Dev. 55, 97–111. doi: 10.2307/1129837
Gerhardt, C. A., Gutzwiller, J., Huiet, K. A., Fischer, S., Noll, R. B., and Vannatta, K. (2007). Parental adjustment to childhood cancer: a replication study. Fam. Syst. Health 25, 263–275. doi: 10.1037/1091-7527.25.3.263
Götze, H., Brähler, E., Romer, G., Bergelt, C., Von Klitzing, K., Herzog, W., et al. (2012). Partnerinnen von Krebspatienten mit minderjährigen Kindern–Psychische Belastung im Vergleich zur Allgemeinbevölkerung und zum krebskranken partner. [female spouses of Cancer patients with minor children–psychological distress in comparison with the general population and the Cancer partner]. Psychother. Psychosom. Med. Psychol. 62, 170–176. doi: 10.1055/s-0032-1306303
Heinemann, C., and Simeit, R. (2017). Psychoedukative Gruppeninterventionen für Familien mit einem krebskranken Elternteil. [psychoeducational group interventions for families with a parent with cancer]. Prax. Kinderpsychol. Kinderpsychiatr. 66, 161–178. doi: 10.13109/prkk.2017.66.3.161
Hiebel, N., Rabe, M., Maus, K., Peusquens, F., Radbruch, L., and Geiser, F. (2021). Resilience in adult health science revisited-a narrative review synthesis of process-oriented approaches. Front. Psychol. 12:659395. doi: 10.3389/fpsyg.2021.659395
Hiltrop, K., Heidkamp, P., Breidenbach, C., Kowalski, C., Streibelt, M., and Ernstmann, N. (2021). Conflicting demands, coping, and adjustment: a grounded theory to understand rehabilitation processes in long-term breast cancer survivors. Psycho-Oncology 30, 1957–1964. doi: 10.1002/pon.5769
Hinz, A., Krauss, O., Hauss, J. P., Höckel, M., Kortmann, R. D., Stolzenburg, J. U., et al. (2010). Anxiety and depression in cancer patients compared with the general population. Eur. J. Cancer Care 19, 522–529. doi: 10.1111/j.1365-2354.2009.01088.x
Howard Sharp, K. M., Willard, V. W., Barnes, S., Tillery, R., Long, A., and Phipps, S. (2017). Emotion socialization in the context of childhood Cancer: perceptions of parental support promotes posttraumatic growth. J. Pediatr. Psychol. 42, jsw062–jsw103. doi: 10.1093/jpepsy/jsw062
Howell, K. H., Barrett-Becker, E. P., Burnside, A. N., Wamser-Nanney, R., Layne, C. M., and Kaplow, J. B. (2016). Children facing parental cancer versus parental death: the buffering effects of positive parenting and emotional expression. J. Child Fam. Stud. 25, 152–164. doi: 10.1007/s10826-015-0198-3
Jantien Vrijmoet-Wiersma, C. M., van Klink, J. M. M., Kolk, A. M., Koopman, H. M., Ball, L. M., and Maarten Egeler, R. (2008). Assessment of parental psychological stress in pediatric cancer: a review. J. Pediatr. Psychol. 33, 694–706. doi: 10.1093/jpepsy/jsn007
Kalisch, R. (2017). Der resiliente Mensch: Wie wir Krisen erleben und bewältigen: Neueste Erkenntnisse aus Hirnforschung und Psychologie: eBook. Berlin: Berlin Verlag.
Kuckartz, U., and Rädiker, S. (2020). Fokussierte Interviewanalyse mit MAXQDA: Schritt für Schritt. Wiesbaden: Springer VS.
Kuckartz, U., and Rädiker, S. (2022). Qualitative Inhaltsanalyse. Methoden, Praxis, Computerunterstützung: Grundlagentexte Methoden. 5th Edn. Weinheim: Beltz Juventa.
Kühne, F., Krattenmacher, T., Beierlein, V., Grimm, J. C., Bergelt, C., Romer, G., et al. (2012). Minor children of palliative patients: a systematic review of psychosocial family interventions. J. Palliat. Med. 15, 931–945. doi: 10.1089/jpm.2011.0380
Kühne, F., Krattenmacher, T., Bergelt, C., Beierlein, V., Herzog, W. V., Klitzing, K., et al. (2013). "there is still so much ahead of us"-family functioning in families of palliative cancer patients. Fam. Syst. Health 31, 181–193. doi: 10.1037/a0032274
Kurz, K., Reißig, A., Strauß, B., and Rosendahl, J. (2014). Geschlechtsunterschiede in der psychischen Belastung von Patienten mit Lungenkarzinom und deren Partnern. [Gender Differences in Mental Distress of Patients with Lung Cancer and their Partners]. Psychother. Med. Psychol. 64, 431–438. doi: 10.1055/s-0034-1375631
Li, M.-Y., Yang, Y.-L., Liu, L., and Wang, L. (2016). Effects of social support, hope and resilience on quality of life among Chinese bladder cancer patients: a cross-sectional study. Health Qual. Life Outcomes 14, 73–79. doi: 10.1186/s12955-016-0481-z
Lindsey, E. W., and Mize, J. (2001). Interparental agreement, parent-child responsiveness, and Children's peer competence. Fam. Relat. 50, 348–354. doi: 10.1111/j.1741-3729.2001.00348.x
Lundquist, M. (2017). Fathers facing advanced cancer: an exploratory study. J. Soc. Work End Life Palliat. Care 13, 266–283. doi: 10.1080/15524256.2017.1403410
Luthar, S. S., Cicchetti, D., and Becker, B. (2000). The construct of resilience: a critical evaluation and guidelines for future work. Child Dev. 71, 543–562. doi: 10.1111/1467-8624.00164
Martin, A. S., Distelberg, B. J., and Elahad, J. A. (2015). The relationship between family resilience and aging successfully. Am. J. Fam. Ther. 43, 163–179. doi: 10.1080/01926187.2014.988593
Masten, A. S. (2001). Ordinary magic: resilience processes in development. Am. Psychol. 56, 227–238. doi: 10.1037//0003-066x.56.3.227
McCubbin, H. I., and McCubbin, M. A. (1988). Typologies of resilient families: emerging roles of social class and ethnicity. Fam. Relat. 37:247. doi: 10.2307/584557
Molina, Y., Jean, C. Y., Martinez-Gutierrez, J., Reding, K. W., Joyce, P., and Rosenberg, A. R. (2014). Resilience among patients across the cancer continuum: diverse perspectives. Clin. J. Oncol. Nurs. 18, 93–101. doi: 10.1188/14.CJON.93-101
Nakaya, N., Saito-Nakaya, K., Bidstrup, P. E., Dalton, S. O., Frederiksen, K., Steding-Jessen, M., et al. (2010). Increased risk of severe depression in male partners of women with breast cancer. Cancer 116, 5527–5534. doi: 10.1002/cncr.25534
O'Cathain, A., Murphy, E., and Nicholl, J. (2010). Three techniques for integrating data in mixed methods studies. BMJ 341:c4587. doi: 10.1136/bmj.c4587
Patterson, J. M. (2002). Integrating family resilience and family stress theory. J. Marriage Fam. 64, 349–360. doi: 10.1111/j.1741-3737.2002.00349.x
Phillips, F., Prezio, E. A., Panisch, L. S., and Jones, B. L. (2021). Factors affecting outcomes following a psychosocial intervention for children when a parent has Cancer. J. Child Life 2:28322. doi: 10.55591/001c.28322
Robert Koch-Institute. (2022a). Cancer in Germany – C00-C97 without C44, [Krebs in Deutschland – C00-C97 ohne C44]. Available at: https://www.krebsdaten.de/Krebs/DE/Content/Publikationen/Krebs_in_Deutschland/kid_2019/kid_2019_c00_97_krebs_gesamt.html (Accessed November 02, 2022)
Robert Koch-Institute. (2022b). How common are cancer diseases in parents of minor children? [Wie häufig sind Krebserkrankungen bei Eltern minderjähriger Kinder?]. Available at: https://www.krebsdaten.de/Krebs/DE/Content/Publikationen/Kurzbeitraege/Archiv2019/2019_3_Kurzbeitraege_Krebskranke_Eltern.html (Accessed November 02, 2022)
Rolbiecki, A., Subramanian, R., Crenshaw, B., Albright, D. L., Perreault, M., and Mehr, D. (2017). A qualitative exploration of resilience among patients living with chronic pain. Traumatology 23, 89–94. doi: 10.1037/trm0000095
Romer, G. (2007). Kinder körperlich kranker Eltern: Psychische Belastungen, Wege der Bewältigung und Perspektiven der seelischen Gesundheitsvorsorge. [children of physically ill parents: mental stress, ways of coping and prospects for mental health care]. Prax. Kinderpsychol. Kinderpsychiatr. 56, 870–890. doi: 10.25656/01:3065
Rutten, L. J. F., Arora, N. K., Bakos, A. D., Aziz, N., and Rowland, J. (2005). Information needs and sources of information among cancer patients: a systematic review of research (1980-2003). Patient Educ. Couns. 57, 250–261. doi: 10.1016/j.pec.2004.06.006
Seiler, A., and Jenewein, J. (2019). Resilience in cancer patients. Front. Psych. 10:208. doi: 10.3389/fpsyt.2019.00208
Southwick, S. M., Bonanno, G. A., Masten, A. S., Panter-Brick, C., and Yehuda, R. (2014). Resilience definitions, theory, and challenges: interdisciplinary perspectives. Eur. J. Psychotraumatol. 5:25338. doi: 10.3402/ejpt.v5.25338
Tong, A., Sainsbury, P., and Craig, J. (2007). Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 19, 349–357. doi: 10.1093/intqhc/mzm042
van Schoors, M., Caes, L., Verhofstadt, L. L., Goubert, L., and Alderfer, M. A. (2015). Systematic review: family resilience after pediatric cancer diagnosis. J. Pediatr. Psychol. 40, 856–868. doi: 10.1093/jpepsy/jsv055
Veach, T. A., and Nicholas, D. R. (1998). Understanding families of adults with cancer: combining the clinical course of cancer and stages of family development. J. Couns. Dev. 76, 144–156. doi: 10.1002/j.1556-6676.1998.tb02387.x
Visser, A., Huizinga, G. A., van der Graaf, W. T. A., Hoekstra, H. J., and Hoekstra-Weebers, J. E. (2004). The impact of parental cancer on children and the family: a review of the literature. Cancer Treat. Rev. 30, 683–694. doi: 10.1016/j.ctrv.2004.06.001
Walach, H. (2022). “Spiritualität: [Spirituality]” in Dorsch Lexikon der Psychologie. ed. M. A. Wirtz (Bern: Hogrefe)
Walsh, F. (2003). Family resilience: a framework for clinical practice. Fam. Process 42, 1–18. doi: 10.1111/j.1545-5300.2003.00001.x
Weaver, K. E., Rowland, J. H., Alfano, C. M., and McNeel, T. S. (2010). Parental cancer and the family: a population-based estimate of the number of US cancer survivors residing with their minor children. Cancer 116, 4395–4401. doi: 10.1002/cncr.25368
Zhou, J., He, B., He, Y., Huang, W., Zhu, H., Zhang, M., et al. (2020). Measurement properties of family resilience assessment questionnaires: a systematic review. Fam. Pract. 37, 581–591. doi: 10.1093/fampra/cmaa027
Keywords: parental cancer, minor children, resilience, family intervention, family-SCOUT, oncology, qualitative research and analysis, health services research
Citation: Heuser C, Schneider JN, Heier L, Ernstmann N, Nakata H, Petermann-Meyer A, Bremen R, Karger A, Icks A, Brümmendorf TH and Geiser F (2024) Family resilience of families with parental cancer and minor children: a qualitative analysis. Front. Psychol. 14:1251049. doi: 10.3389/fpsyg.2023.1251049
Edited by:
Michele Giannotti, University of Trento, ItalyReviewed by:
Amanda Marin-Chollom, Central Connecticut State University, United StatesCopyright © 2024 Heuser, Schneider, Heier, Ernstmann, Nakata, Petermann-Meyer, Bremen, Karger, Icks, Brümmendorf and Geiser. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christian Heuser, Y2hyaXN0aWFuLmhldXNlcjFAdWsta29lbG4uZGU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.